
Abstract
Background:
Athletes sustaining Lisfranc joint instability after a low-energy injury often undergo surgical fixation. Limited studies report validated patient-reported outcome measures (PROMs) for this specific patient population. Our purpose was to report PROMs of athletes experiencing instability after a low-energy Lisfranc injury and undergoing surgical fixation.
Methods:
Twenty-nine athletes (23 competitive, 6 recreational) sustained an unstable Lisfranc injury (14 acute, 15 chronic) and met our inclusion criteria. Injuries were classified as acute if surgically managed within 6 weeks. All athletes completed validated PROMs pre- and postoperatively. The cohort underwent various open reduction internal fixation methods. We evaluated outcomes with the Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL) and sports subscales.
Results:
Fourteen of 29 (48%) athletes reported PROMs at ≥2 years with a median follow-up time of 44.5 months. Substantial improvement for both FAAM ADL (50% vs 93%; P < .001) and sports (14.1% vs 80%; P = .002) subscales were found, when comparing preoperative to postoperative scores at ≥2 years.
Conclusion:
This study provides outcomes information for the young athletic population that were treated operatively for low-energy Lisfranc injury with apparent joint instability. Based on the FAAM sports subscale, these patients on average improved between their 6-month evaluation and their final ≥2 years but still scored 80% of the possible 100%, which indicates continued but “slight” difficulty with lower extremity function.
Level of Evidence:
Level IV, case series.
Introduction
The Lisfranc or tarsometatarsal joint (TMTJ) complex is named after Dr Jacques Lisfranc de St Martin of France 8 and is composed of bones, reinforcing tendons, and dorsal, intermediate, and volar ligamentous layers. 31 Over the last decade, Lisfranc injuries were among the most common severe foot injuries observed in elite athletes 2 and have been reported in several sports (eg, ballet, 12 football,9,18 equestrianism, 1 and women’s gymnastics). 4 Although several mechanisms of low-energy Lisfranc injuries have been reported,6,9,23,24,30 Shapiro et al described a forced plantar flexion and abduction moment with the foot in contact with the ground in an equinus position. 24 Ligamentous injury in this population can lead to midfoot instability and inability to return to sport without surgical intervention. 23 To that end, surgical fixation of unstable Lisfranc injuries is the accepted standard. 11
Several studies reported outcomes for athletic patients with unstable Lisfranc injuries receiving various fixation techniques, including primary arthrodesis,5,13 transarticular screws, 10 dorsal plating, 10 percutaneous reduction,7,27,28 hamstring autografts, 19 suture-buttons, 3 or a combination of techniques. 5 Despite this, however, limited studies exist that report validated patient-reported outcome measures (PROMs) for this injury and patient population.
The purpose of this study is to report validated PROMs for both recreational and competitive athletes undergoing surgical fixation of unstable low-energy Lisfranc injuries. 22
Methods
The study was approved by our institutional review board (IRB 20020136). An institution-based registry with foot and ankle patient data that was prospectively collected was queried for patients who underwent surgical fixation of Lisfranc injuries between January 2015 and August 2019 by multiple authors (C.L.B., N.A.J., and C.O.). Patients were included in the study if they had sustained a low-energy mechanism of injury, had Lisfranc joint instability (eg, hypermobile first ray, difficulty bearing weight, or more than 2-mm Lisfranc interval diastasis on weightbearing radiographic imaging), 11 identified as a competitive (ie, for an organized team) or recreational (ie, for personal satisfaction) athlete, underwent open reduction and internal fixation (ORIF) for tarsometatarsal dislocation (Current Procedural Terminology code 28615) by a single surgeon (the senior author, M.V.H.), and completed validated PROMs pre- and postoperatively (Figure 1). Twenty-nine patients met our inclusion criteria. Injuries managed within 6 weeks were defined as acute injuries and after 6 weeks as chronic. 5
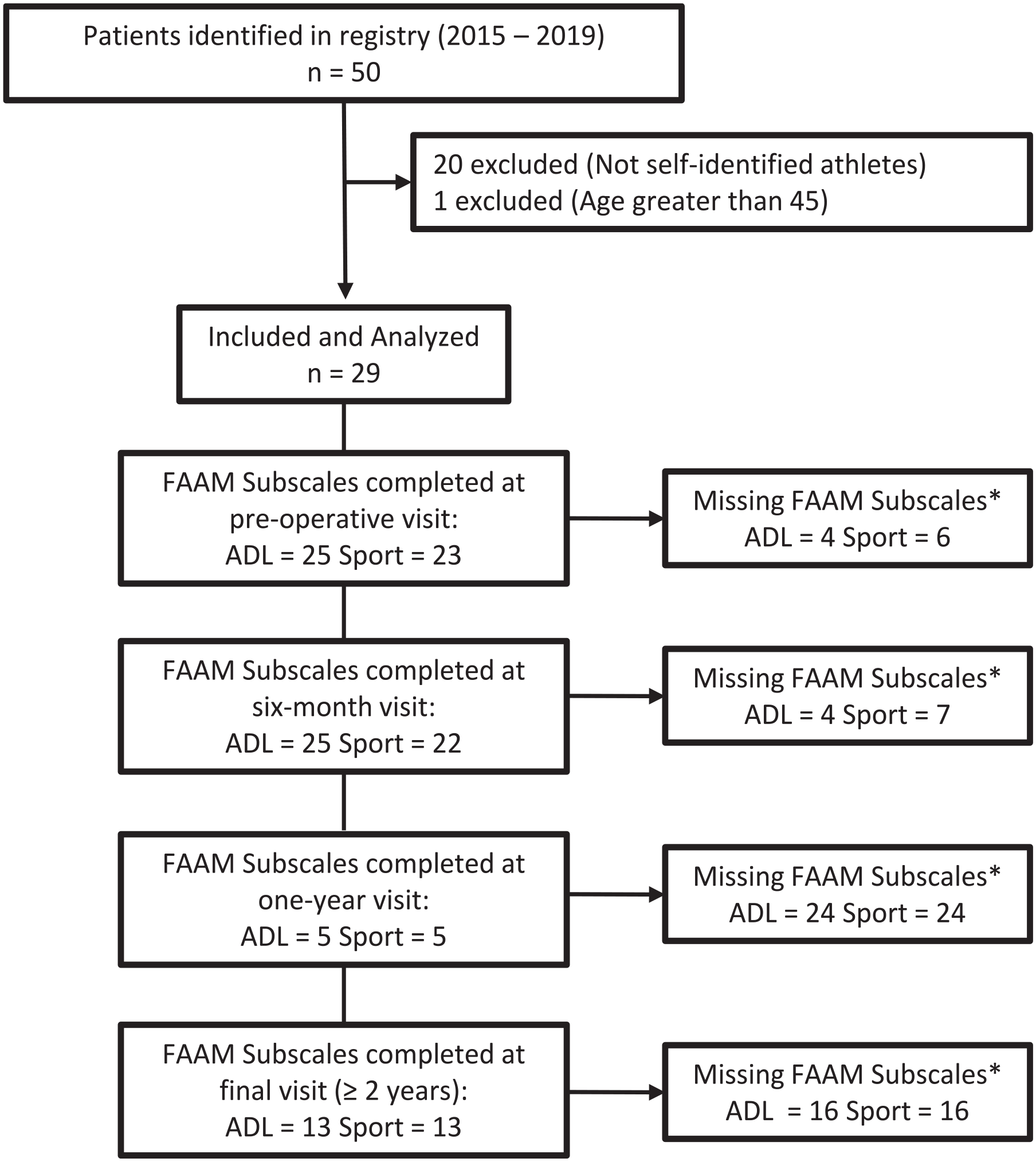
Patient selection flow chart.
Functional Evaluation
The senior author’s practice is located within a tertiary hospital service line. To that end, all patients were evaluated by other providers and met criteria for Lisfranc instability previously described. 11 Joint instability was evaluated by the senior author both in clinic and intraoperatively. Patients with midfoot pain, swelling, plantar ecchymosis, or difficulty bearing weight were sent for weightbearing imaging. Anterior to posterior (AP), lateral, and oblique radiographs were reviewed for joint instability (eg, more than 2-mm Lisfranc interval diastasis on AP radiograph). 21 Some patients were referred to the senior author’s clinic with advanced imaging (eg, magnetic resonance imaging) prior to clinical examination.
The Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL) and FAAM sports subscales were PROMs used to measure outcomes.15,16 They were selected as the main outcomes criteria because they are specific for foot and ankle disorders and are validated instruments for outcome evaluation. 15 The FAAM ADL and FAAM sports subscales consist of 21 and 8 questions, respectively, that provide an understanding of the patient’s current level of function. The overall FAAM scoring range is 0% to 100%, with a higher percentage indicating a better outcome. 25 Patients were asked to completed PROMs at each clinic visit. Authors involved with data analysis (C.L.B., N.A.J., and C.O.) were not directly involved in the surgical procedures.
Surgical Technique
A single dorsal incision between the first and second columns was used for exposure and reduction; fixation generally proceeded from proximal to distal and from medial to lateral. Care was taken to protect branches of the superficial peroneal nerve that cross the extensor hallucis longus, as well as the neurovascular bundle just lateral to the extensor hallucis longus. An incision in the interval between the extensor hallucis longus and extensor hallucis brevis then facilitated examination of the intercuneiform joints. Thereafter, the dorsal Lisfranc joint capsules were examined for evidence of injury and stressed with dorsal-plantar translation to confirm instability. Various fixation techniques were used in the current study and varied based on the exact injury pattern; this was at the discretion of the senior author (M.V.H.) who was the sole surgeon (eg, dorsal plate with transarticular screws, suture-button, and isolated transarticular screws) (Figures 2 and 3).

Fixation devices used to anatomically reduce Lisfranc joint: (A) Dorsal locking plate with both a Lisfranc and intercuneiform screw. (B) Isolated suture-button. (C) Isolated Lisfranc and intercuneiform screws.

Pre- and postoperative images of a 19-year-old male patient who sustained an unstable right Lisfranc injury at practice. He underwent open reduction and internal fixation with dorsal bridge plate and transarticular screws. (A) Diastasis between the medial cuneiform and the base of the second metatarsal. (B) Complete disruption of the Lisfranc ligament between medial cuneiform and second metatarsal. (C) Postreduction films.
Postoperative Management
All patients were placed into a posterior plaster U splint for 2 weeks. At their first postoperative visit, patients were transitioned into a short-leg nonweightbearing cast for 8 weeks. Afterward, patients began progressing to weightbearing with a CAM boot for 8 weeks. Once weightbearing, formal physical therapy focused on gait correction and edema control, followed by progression to sport-specific training and, ultimately, return to play.
Statistical Analysis
All statistical analysis was performed with Stata/SE 17.0 (StataCorp LLC, College Station, TX). For the 29 patients included in our analysis, PROMs were obtained for the following time points: preoperative visit, 6 months, 1 year, and/or ≥2 years. A Shapiro-Wilk test was conducted to assess all data for normality. The nonparametric Wilcoxon signed-rank tests were performed between preoperative and follow-up visits to determine statistical significance at 6 months, 1 year, and latest follow-up visit ≥2 years postoperatively. 29 The significance level for all PROM comparisons was set at 95%, and statistical significance was accepted at a P value <.05. As mentioned above, clinical significance was determined using FAAM subscales.
Results
Functional Outcomes
Twenty-nine patients were identified and included in this study (16 females and 13 males). Patient demographics are shown in Table 1. All patients completed a preoperative survey, 28 (97%) patients completed a 6-month postoperative PROM survey, and 6 (21%) patients completed a 1-year postoperative PROM. Fourteen (48%) patients completed a PROM survey at the latest postoperative follow-up at ≥2 years. Median follow-up was 12 (interquartile range [IQR], 35) months for all patients and 44.5 (IQR, 14.5) months for patients with PROMs ≥2 years. Of the 29 surgeries, 55% (16 of 29) of patients received both a dorsal locking plate and transarticular screws, 24% (7 of 29) received a suture-button, 21% (6 of 29) received isolated transarticular screws.
Patient Characteristics of Athletes Undergoing Open Reduction Internal Fixation for Lisfranc Instability (N = 29)

Abbreviations: DP, dorsal plate; TA, transarticular.
When comparing FAAM ADL pre- and postoperative scores for all patients, there were statistically significant improvements at the 6-month (50 vs 89.1; P < .001), 1-year (50 vs 95.2; P = .03), and final visit at or greater than 2 years (50 vs 93; P = .002). For the FAAM sports subscale, there were statistically significant improvements at the 6-month (14.1 vs 59.4; P = .002) and final visit at ≥2 years (14.1 vs 80; P = .002). FAAM scores over time are demonstrated in Table 2. When comparing preoperative and final postoperative FAAM subscales for athletes undergoing the most frequently used fixation technique—dorsal bridge plate and transarticular screw fixation, there was a statistically significant improvement in both FAAM ADL (48.3 vs 94; P = .02) and sport (9.4 vs 79; P = 0.02) subscales (Table 3). There were various types of athletes who underwent this fixation method. All reported improved functional outcomes (Table 4).
Functional Outcomes After Lisfranc Fixation Using FAAM Subscales.

Abbreviations: ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure; Postop., postoperative; Preop., preoperative.
P value compared with respective preoperative visit subscale score.
Functional outcomes of athletes after Lisfranc fixation with dorsal bridge plate and transarticular screw fixation.
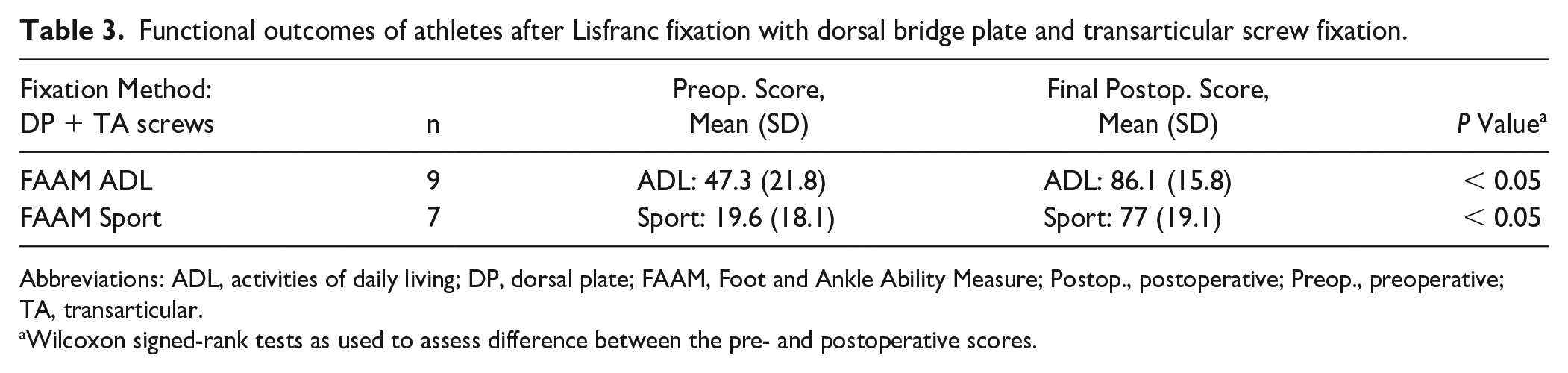
Abbreviations: ADL, activities of daily living; DP, dorsal plate; FAAM, Foot and Ankle Ability Measure; Postop., postoperative; Preop., preoperative; TA, transarticular.
Wilcoxon signed-rank tests as used to assess difference between the pre- and postoperative scores.
Functional Outcomes of Various Athletes After Lisfranc Fixation With Dorsal Plate + Transarticular Screws.

Abbreviations: ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure; Postop., postoperative; Preop., preoperative.
Competitive (C) vs recreational (R). All final FAAM scores were recorded >24 months after surgery. Only 9 of 16 patients who underwent this fixation method reported.
All patients treated with dorsal plate fixation underwent removal of hardware at a median time after fixation of 131 (IQR, 26) days. One patient underwent an additional removal of hardware because of a broken screw that caused discomfort. No patients were diagnosed with a deep vein thrombosis or a superficial or deep infection. No other complications were noted.
Discussion
This study reported validated PROMs for a small cohort of athletes who underwent ORIF for low-energy Lisfranc instability. As expected, FAAM ADL and sports subscales were significantly improved for the 14 athletes with a final postoperative visit >2 years. The FAAM ADL and sports subscales are among the most used foot and ankle PROMs, 14 and several studies support the validity and reliability of these measures for foot injuries.15,16 These PROMs can be used to assess the effectiveness of surgical intervention and also help track patient-reported physical function over time. 15 The current study revealed good outcomes with ORIF as a surgical intervention for low-energy Lisfranc injuries in a small athletic cohort.
Of the studies reporting functional outcomes after ORIF for low-energy Lisfranc injuries in the athletic population,3,5,7,10,13,17,19,20,26,28 Cochran et al 5 was to our knowledge the only to report validated PROMs. The authors compared outcomes of young active military personnel who underwent either an ORIF with bridge plating and/or transarticular screws or primary arthrodesis after low-energy Lisfranc injuries. For the 18 patients who underwent ORIF, the FAAM ADL and sports subscales were 84.7 and 70.4, respectively, at final follow-up of an average of 35 months. No difference was detected between the ORIF and arthrodesis groups.
The strengths of our study include prospectively collected data, a narrowly defined cohort, follow-up duration for a subset of the original patients, and use of validated PROMs. There are, however, notable and important limitations. Patients without outcome data were excluded. Additionally, there was a drop-off in the number of participants who provided PROM data at the 1-year follow-up time point, as well as only 45% of the original participants at the 2-year time point, and this is a significant limitation that must be considered. Next, the method of surgical fixation was varied in our cohort, but the method of treatment for Lisfranc injuries, particularly in the athletic patient population, is not standardized and was based on the degree of injury. Although all patients self-identified as athletes (recreational vs competitive), we did not specify athletic position or level of play or follow specifically each patient’s return to play. Being that our median latest follow-up timeframe for 14 of 29 patients was 44.5 (IQR, 14.5) months, this study does not offer long-term functional outcomes and the potential for late complications that may arise. Furthermore, we did not specifically determine return to performance for each patient or have a control group of non-injured subjects.
In conclusion, this study reports PROMs for the young athletic population that sustained an unstable low-energy Lisfranc injury and underwent surgical fixation. As best we can tell from our midterm follow-up of a small subgroup, these findings did not deteriorate at a median follow-up of 44.5 months. And for those that we do have final follow-up, their average functional scores reveal generally modest activity limitations.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of Pittsburgh (IRB 20020136).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.