
Abstract
Background:
Limited literature examines the relationship between surgical outcomes in chronic foot and ankle conditions and concurrent psychiatric care. The present study aimed to investigate patient-reported and surgical outcomes of patients treated for a psychiatric disorder undergoing first metatarsophalangeal (MTP) fusion for hallux rigidus. We hypothesized that patients on psychotropic medications would have greater subjective pain preoperatively and less improvement in physical and mental functionality postoperatively when compared with nonmedicated patients.
Methods:
A single-center, retrospective review of prospectively collected data was conducted on 92 patients undergoing first MTP fusion with a preoperative diagnosis of hallux rigidus from 2015 to 2019. At their preoperative, 6-month postoperative, and 1-year postoperative visits, patients were administered visual analog pain scale (VAS) and 36-Item Short Form Health Survey (SF-36) functionality surveys. Patients were subsequently identified by chronic use of psychotropic medication preoperatively and grouped for analysis (MED, n = 42; NO MED, n = 50).
Results:
Postoperative mean VAS pain scores were lower for all studied patients at 6 months (VAS = 1.6 ± 2.3) and 1 year postoperatively (VAS = 1.1± 1.8) relative to the preoperative visit (VAS = 4.7 ± 2.8) (P ≤ .0001 and P ≤ .0001, respectively). No differences in mean VAS pain scores nor SF-36 physical component summary scores were detected at preoperative, 6-month, or 1-year visits between NO MED and MED groups. Mean SF-36 mental component summary scores for those in the MED group were lower at preoperative (NO MED = 83.8, MED = 71.8, P = .006) and 6-month postoperative (NO MED = 86.1, MED = 72.7, P = .037) visits than those in the NO MED group, a trend not observed at the 1-year postoperative mark (NO MED = 84.1, MED = 76.8, P = .228). There were no observed differences in operative time (P = .219), tourniquet time (P = .359), nor time to full weightbearing (P = .512) between MED and NO MED groups. Additionally, no differences in postoperative complication rates were observed between groups.
Conclusion:
In patients treated with psychotropically active medications with hallux rigidus, MTP Fusion appears to be a reasonable treatment choice with similar outcomes for patients requiring psychotropically active medications to the outcomes of those patients not requiring psychotropically active medications.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Psychiatric comorbidities have been shown to significantly impact disease course, leading to increasingly complicated hospitalizations and worse overall patient outcomes.4,5,9 Diagnoses of major depressive disorder (MDD) are particularly common—with a prevalence of 16.6%—and have increased significantly since 2005.12,28,31 As might be expected, the prescription of selective serotonin reuptake inhibitors has accordingly risen during this time.17,23,27 MDD and other psychiatric diagnoses (ie, anxiety disorder, schizophrenia) are known to lower patients pain threshold and pain tolerance, complicating their postoperative course.3,14,16,33 Pain management in orthopaedic surgery is paramount in restoring mobility and reaching treatment goals, making a solid understanding of psychiatric conditions in the operative setting vitally important.1,4,11,20
Difficulties associated with treating patients carrying psychiatric diagnoses are pervasive and well documented in the surgical setting. Diagnoses of depression and anxiety have been associated with longer hospitalizations and increased total costs of care after surgery.5,29 Similarly, selective serotonin reuptake inhibitor (SSRI) and other psychotropic medication use have been specifically linked to potential increased peri- and postoperative bleeding risk, 24 as well as increased length of postoperative hospitalization and readmission rates.2,4,6,10 In the orthopaedic setting, adverse pain outcomes following orthopaedic trauma have been observed in patients with depression and anxiety, finding that patients are at significantly increased risk of developing chronic pain disorders.8,32 Even with these known disparities in orthopaedic results and a patient population at high risk for psychiatric comorbidity, sparse literature exists examining the relationship between surgical outcomes in chronic foot and ankle conditions and concurrent psychiatric care.20,26
Pathologies of the first toe can cause patients significant physical and psychological distress. The deformities associated with these diagnoses can be mobility limiting and negatively impact body image—for instance, the severity of hallux valgus deformity has been associated with increased depressive symptoms preoperatively. 18 It has also been shown that delaying surgical management of symptomatic hallux valgus deformities has deleterious effects on postoperative outcomes. 30 The psychological effects stemming from pain and deformity associated with advanced hallux rigidus are less well studied, but still likely prevalent and significant. Positive results in the surgical fixation of both hallux rigidus and hallux valgus are well documented across age groups.7,19 Metatarsophalangeal (MTP) fusion is a reliable method for the treatment of hallux rigidus and is associated with high patient satisfaction and improved functionality. 7 Nevertheless, the effects of psychiatric disorders on surgical outcomes in this population are not well understood. It has recently been shown that patients with hallux valgus with significant depressive symptoms have worse overall outcomes and decreased satisfaction with surgical correction of their deformities. 25 However, no study has addressed outcomes in patients with depressive symptoms undergoing first-metatarsophalangeal (MTP) fusion for hallux rigidus, nor—more broadly—outcomes of patients treated for a psychiatric disorder undergoing first-MTP fusion.
Therefore, the purpose of this study was to observe the association between psychotropic medication use in patients with diagnoses of hallux rigidus undergoing first MTP fusion and differences in patient-reported pain scores, physical and mental functionality scores, comorbidities, and postoperative complications. We hypothesized that patients taking psychotropic medications in the pre- and postoperative period would have significantly worse VAS and SF-36 scores at preoperative time points and have less improvement in physical and mental functionality at postoperative time points.
Methods
Study Design
A retrospective review of prospectively collected data was designed to assess all patients undergoing first MTP fusion with a preoperative diagnosis of hallux rigidus by a single, foot and ankle fellowship–trained orthopaedic surgeon (J.B.) from August 1, 2015, to July 1, 2019. After institutional review board approval was obtained, patients were consented for the study at the time of their presentation to clinic. Any patient that was seen for a preoperative clinic visit, subsequently underwent first-MTP fusion for hallux rigidus, and had 1 year of follow-up, were included in the study. Pregnant women, children, prisoners, and other vulnerable populations were excluded. Patient demographic data, including age and sex, the number of affected toes, and psychotropic medication use were noted at the initial visit through review of the electronic medical record and from the patient’s self-reporting (Table 1). Patients were considered to be taking a psychotropic medication if they endorsed on clinic intake that they were actively taking medications prescribed in a primary care or psychiatry setting for the treatment of an underlying psychiatric comorbidity. Medical comorbidities, procedure characteristics, and operative characteristics were subsequently collected from review of the electronic medical record (Table 2). At their preoperative and postoperative clinical visits, patients were administered a visual analog pain scale (VAS) and 36-Item Short Form Health Survey (SF-36) functionality surveys. The SF-36 survey is broken into mental and physical component summary scores (MCS and PCS, respectively). Patients were subsequently grouped for analysis based on chronic use of a psychotropic medication preoperatively (Table 3). Postoperative VAS pain was defined as the primary outcome measure of the study, with SF-36 composite and subsection scores as secondary outcomes. Postoperative complications were considered to be superficial wound infections requiring antibiotics, deep wound infections requiring washout, and need for revision. These data were obtained through review of the electronic medical record.
Patient Demographics.

Abbreviations: BMI, body mass index; CAD, coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; PAD, peripheral artery disease.
Boldface indicates statistical significance (P < .05).
Operative Procedures.

Abbreviations: MTP, metatarsophalangeal; PIP, proximal interphalangeal.
Boldface indicates statistical significance (P < .05).
List of Psychoactive Medications.

Surgical Technique
According to established surgical technique, the hallux MTP joint was fused using a dorsal plate (Stryker Anchorage without CP technology) and compression screw construct. 15 Patients were placed in a postoperative hard-sole shoe and were immediately allowed to bear weight through their heel postoperatively. They were seen in clinic for a wound check and suture removal at 2 weeks postoperatively. Heel-only weightbearing status in a hard-sole shoe was maintained until the 6-week postoperative visit when they were transitioned to full weightbearing in a postoperative shoe. They were subsequently weaned to normal weightbearing in a supportive athletic shoe over the next 2 weeks, with subsequent follow-up at 12 weeks with radiographic evaluation of their fusion.
Statistics
For all statistical tests, assumptions of α < .05 and β = .8 were made. Patient demographic data were collected and analyzed with descriptive statistics. Normality of these data was assessed with a Shapiro-Wilk test. For normally distributed data, VAS pain, and SF-36 component scores were compared between psychotropic medication cohorts using the independent sample t test whereas non-normal comparisons were made with the Mann-Whitney U test. Fisher exact and Pearson χ2 tests were used to assess categorical data. Post hoc power analysis was conducted using OpenEpi: Open Source Epidemiologic Statistics for Public Health version 3.1 (https://www.openepi.com/Menu/OE_Menu.htm). All other analyses were conducted with SPSS software version 27.0 (IBM Corporation, Armonk, NY).
Results
Over the study duration, 92 total patients underwent surgical correction of the first MTP for hallux rigidus, consented to participate in the study, and had postoperative follow-up. The average age of the patients in our cohort was 63.3 (range, 39 - 83), with 85.9% of the population being female. Patients were separated into groups based on whether or not they were actively taking a psychotropic mediation (MED, n = 42) or not taking a psychotropic medication (NO MED, n = 50) at the time of surgery and immediate follow-up. Psychotropic medications are displayed in Table 3. Aside from a difference in the propensity of hypertension between MED and NO MED groups (P = .043), no differences in patient comorbidities were observed between groups. Mean time to final follow-up was 1.1 ± 0.7 and 1.1 ± 0.6 years in the NO MED and MED groups, respectively (P = .957) (Table 4). The remaining patient demographic data are displayed in Table 1. Operative procedures are displayed in Table 2. Notably, patients in the NO MED group underwent more Hoffmann head resections than the MED group (P = .035). No other differences in operative procedures were observed between groups.
Surgical Outcomes.

Grouped patient reported outcomes are displayed in Table 5. VAS pain scores were significantly lower for the group as a whole at 6 months and 1 year postoperatively relative to the preoperative visit (P ≤ .0001 and P ≤ .0001, respectively). Significant increases in SF-36 PCS scores were seen relative to preoperative visits at the 6-month and 1-year postoperative visits (P = .015, P = .020). No significant changes in SF-36 MCS scores were observed at 6 months or 1 year postoperatively relative to preoperative scores (P = .789, P = .591). No differences in mean VAS pain scores were detected at preoperative (P = .539), 6-month (P = .412), or 1-year (P = .265) visits between NO MED and MED groups (Figure 1). Similarly, no differences in SF-36 PCS scores were detected at preoperative (P = .148), 6-month (P = .316), or 1-year (P = .143) postoperative visits between cohorts (Figure 2). Mean SF-36 MCS scores for those in the MED group were lower at preoperative (P = .006) and 6-month postoperative (P = .037) visits than those in the NO MED group (Figure 3). However, no difference in mean mental component score was observed between groups at the 1-year postoperative visit (P = .228). Mean pain and functionality scores in both cohorts improved similarly over time. There were no observed differences in the preoperative to 6-month nor in the preoperative to 1-year postoperative VAS, SF-36 PCS, and SF-36 MCS scores between cohorts (Table 6).
Patient-Reported Outcomes.

Abbreviations: MCS, mental component summary; PCS, physical component summary; SF-36, 36-Item Short Form Health Survey; VAS, visual analog scale.
Boldface indicates statistical significance (**P < .01. *P < .05).
Change in Patient-Reported Outcomes.

Abbreviations: MCS, mental component summary; PCS, physical component summary; SF-36, 36-Item Short Form Health Survey; VAS, visual analog scale.

Visual analog scale pain score in NO MED vs MED groups at preoperative (P = .539), 6-month postoperative (P = .412), and 1-year postoperative (P = .265) time points. Number displayed inside bar indicates mean.
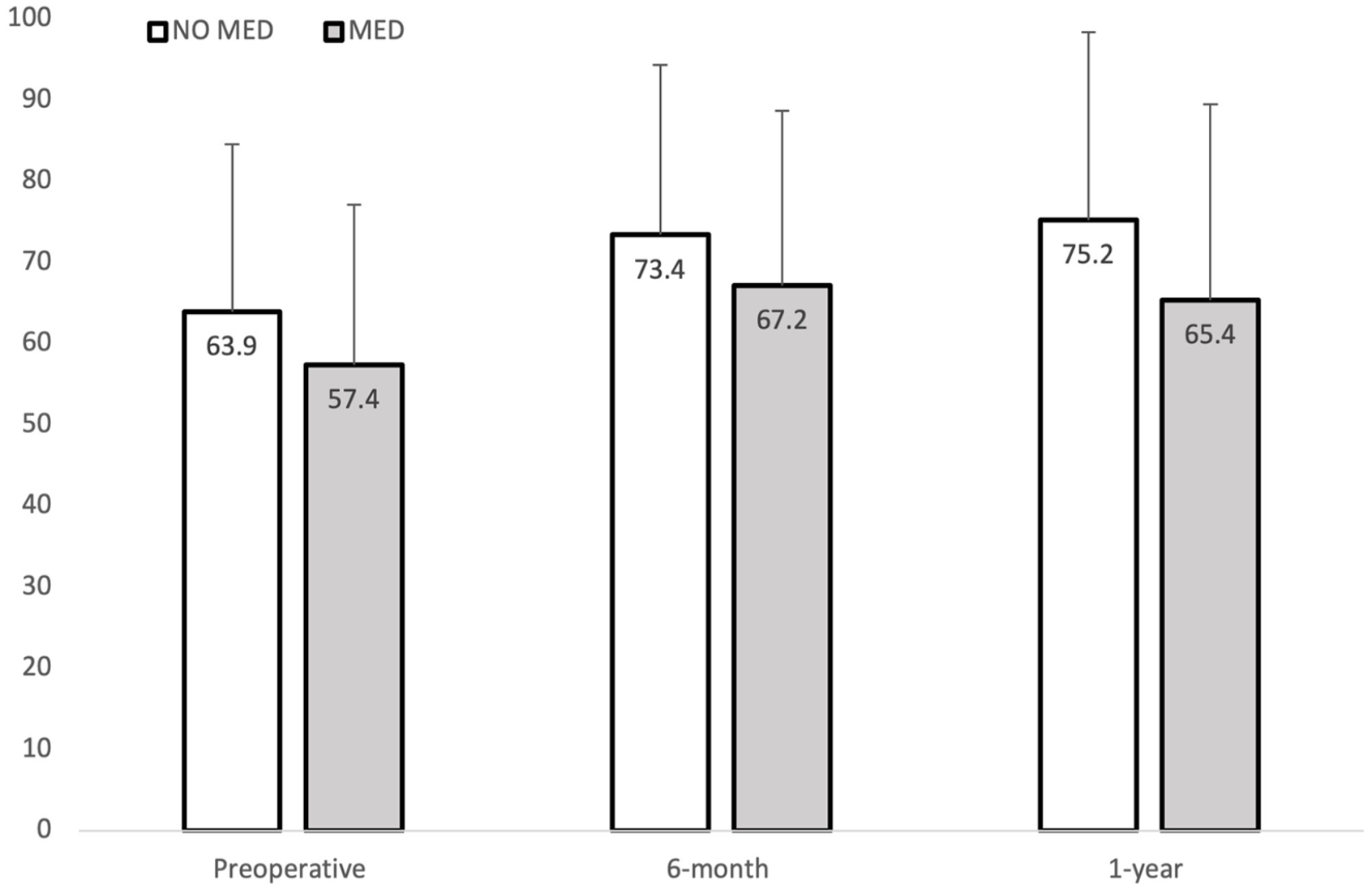
SF-36 physical component summary score in NO MED vs MED groups at preoperative (P = .148), 6-month postoperative (P = .316), and 1-year postoperative (P = .143) time points. Number displayed inside bar indicates mean. SF-36, 36-Item Short Form Health Survey.
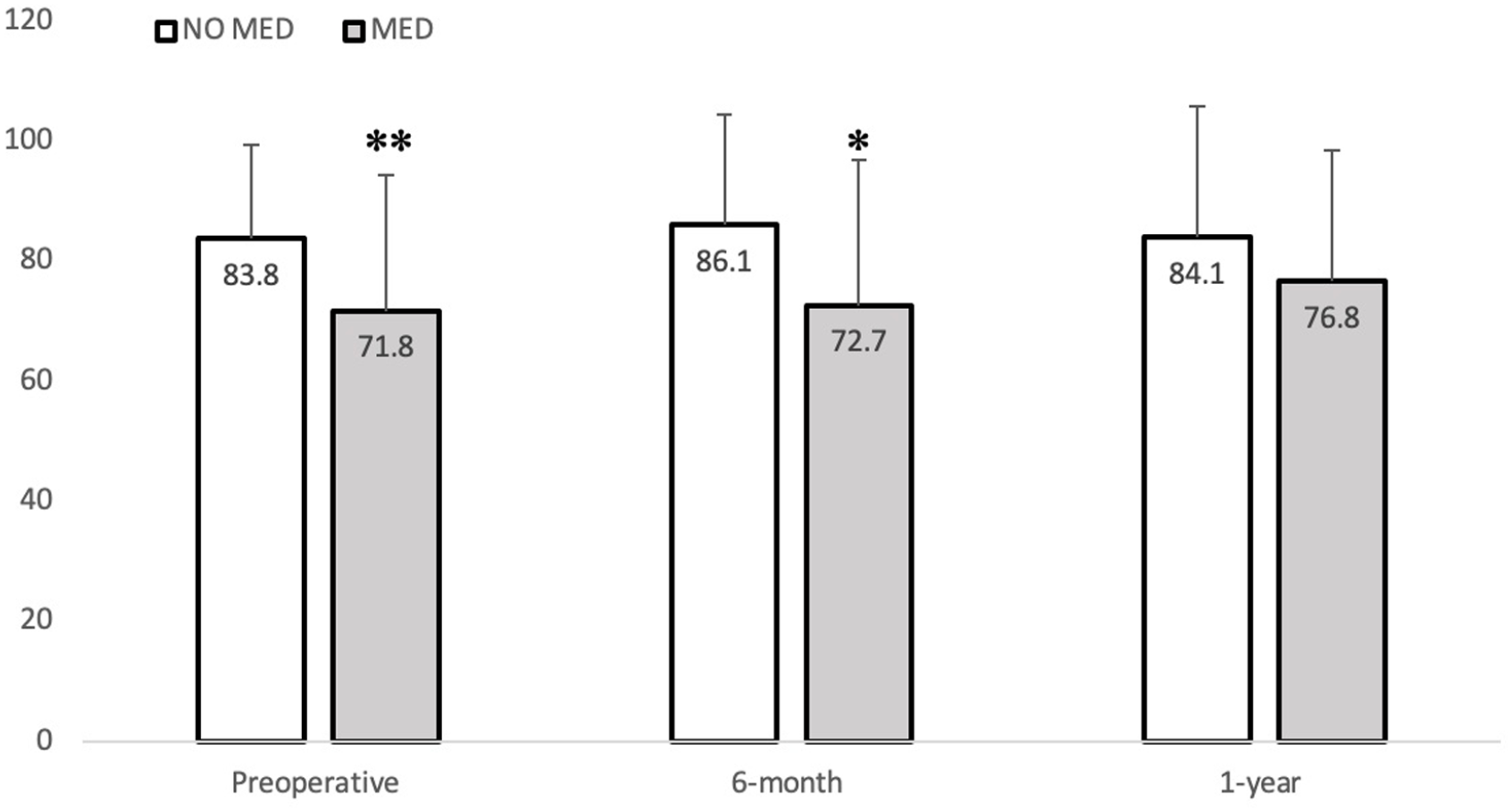
SF-36 mental component summary score in NO MED vs MED groups at preoperative (P = .006), 6-month postoperative (P = .037), and 1-year postoperative (P = .228) time points. Number inside bar indicates mean. SF-36, 36-Item Short Form Health Survey
Surgical outcome data are displayed in Table 4. There were no observed differences in operative time (P = .219), tourniquet time (P = .359), nor time to full weightbearing (P = .512) between MED and NO MED groups. The most common complication for all patients was postoperative wound infection requiring antibiotics (10.9%), followed by symptomatic recurrence requiring a revision operation (6.5%). No differences in postoperative complication rates were observed between MED and NO MED groups.
Discussion
There are known associations in the surgical setting of longer hospitalizations, adverse pain outcomes, and chronic pain disorders in patients carrying psychiatric diagnoses.5,8,29,32 This study sought to evaluate an association between use of psychotropic medications and MTP fusion surgical outcome using patient-reported pain scores, physical and mental functionality scores, comorbidities, and postoperative complications. Our data rejects our hypothesis by demonstrating there was no significant difference in VAS or SF-36 PCS between MED and NO MED groups at the preoperative time point. Additionally, our data show improvement in patient SF-36 MCS in the MED group such that the statistically significant lower scores first observed at the preoperative time point are no longer observed at the 1-year postoperative visit.
In the grouped analysis, both the VAS and SF-36 PCS were significantly lower at 6 months and 1 year postoperatively when compared to preoperative values, providing support for the physical benefits of MTP fusion in hallux rigidus. In contrast, SF-36 MCS were not significantly different at either 6 months or 1 year postoperatively relative to preoperative values for the group analysis. However, preoperatively and at 6 months postoperatively the MED group scored significantly lower on the SF-36 MCS than the NO MED group. At 1 year postoperatively, the difference between the MED and NO MED group was no longer detected, suggesting that the surgery may provide patients on psychotropic medications benefits beyond correction of the big toe. Of note, SSRIs have been reported to potentially cause increased peri and postoperative bleeding. 24 However, our findings indicate that on all studied accounts there was no significant difference in surgical outcome or complication rates between MED and NO MED groups, suggesting that patient use of psychotropic medication does not increase the risk for adverse events following surgical correction with MTP fusion.
To our knowledge, this is the first study looking specifically at psychotropic medication effects on outcomes after MTP fusion for hallux rigidus; however, this has been studied across other foot and ankle pathologies. The influence of depression on MTP fusion outcomes for patients with hallux valgus has previously been studied by Shakked et al. 25 In a series of 239 patients undergoing MTP fusion, 36 met depressive symptom criteria by SF-12 MCS scoring. Those patients displaying depressive symptoms tended to have lower, but nonsignificantly different, VAS (preoperative: not depressed = 6.6, depressed = 7.0; postoperative: not depressed = 4.1, depressed = 3.0) or SF-12 scores (preoperative MCS: not depressed = 57.8, depressed = 38.5; postoperative MCS: not depressed = 56.1, depressed = 49.3; preoperative PCS: not depressed = 45.3, depressed = 41.0; postoperative PCS: not depressed = 47.6, depressed = 44.1) at pre- and postoperative time points. Like the present study, those patients endorsed comparable postoperative satisfaction and symptom improvement to patients without depressive symptoms 1 year after surgery. Additionally, Maidman et al 20 looked at psychotropic medication’s influence on outcomes after hammertoe reconstruction. In their series of 116 patients, 36% of which were on psychotropic medications, there were no differences in pre- and postoperative VAS and PCS scores between medicated and nonmedicated groups (preoperative VAS: nonmedicated = 4.3, medicated = 4.6; postoperative VAS: nonmedicated = 1.5, medicated = 1.8; preoperative PCS: nonmedicated = 62.5, medicated = 54.6; postoperative PCS: nonmedicated = 73.1, medicated = 65.4). They did find lower pre- and postoperative SF-36 MCS scores in medicated patients (preoperative MCS: nonmedicated = 85.5, medicated = 72.9, P = .001; postoperative MCS: nonmedicated = 87.5, medicated = 78.1, P = .006). Interestingly, they also found a significant increase in superficial wound infection in the medicated group, diagnosed simply by clinical history and physical examination. They concluded, similar to our findings, that patients taking psychotropic medications equally benefited from forefoot surgery compared with their nonmedicated peers.
However, the results from our study differ from findings of depressions influence on postoperative outcomes in other pathologies of the foot and ankle. Mulligan et al 22 have previously reported that depressive symptoms in patients undergoing ankle and hindfoot reconstruction had significantly increased overall pain and narcotic usage postoperatively. Similarly, Kim et al 13 found that patients with depressive symptoms undergoing ankle arthroplasty had significantly greater pain and lower functional scores at final postoperative follow-ups, though no differences were observed preoperatively. Notably, all 3 of the aforementioned studies, including the present, used different surrogates for grouping patients with depression or psychiatric conditions, which ultimately may lead to these contradicting observations.
The present study has many strengths, including the use of validated patient outcome measures to detect surgical intervention effectiveness. Patient-reported outcomes were collected prospectively at the time of routine clinic visits to minimize recall bias, and then analyzed retrospectively. Additionally, all surgeries were performed by the same single surgeon, so all patients, regardless of age, followed the same postoperative restrictions and therapeutic protocols. This study also has limitations inherent to its design that must be noted. Although analyzing data from the work of a single surgeon limits the difference in surgical technique, and postoperative management, it drastically limits the generalizability of the data toward a large multispecialty group. Additionally, it should be noted that the nonstatistically significant comparisons of VAS and SF-36 PCS and MCS were found to be underpowered by post hoc power analysis (β = .103, β = .31, and β = .227, respectively). However, based on the range of our findings, it is unlikely any detected differences between groups would be clinically significant based on previous minimally clinically important difference calculations in VAS and SF-36 for first MTP fusion to treat hallux rigidus. 21 We also acknowledge that some patients underwent simultaneous procedures in addition to first MTP fusion and that these procedures could cause more pain and complications; however, we believe this is an accurate representation of patients undergoing first MTP fusion. Finally, because of EMR constraints, we were unable to determine the precise diagnosis for psychotropic medication use and therefore used medication use alone to stratify groups.
Conclusions
In conclusion, this prospective study of patients with hallux rigidus undergoing MTP fusion aimed to assess the impact of psychiatric diagnoses on surgical complications and patient-reported physical and mental surgical outcomes. Compared to patients taking no psychotropic medications, psychotropically medicated patients had significantly lower mental status scores preoperatively and at 6 months postoperatively following MTP fusion for hallux rigidus, but this difference was undetectable at 1 year postoperation. Additionally, there was no difference in complication rates between cohorts. This study provides evidence that patients treated with psychoactive medications could benefit similarly from MTP fusion correction of hallux rigidus as those without.
Footnotes
Ethical Approval
Ethics approval for this study was obtained from Emory University Institutional Review Board (STUDY00000652).
Declaration of Conflicting Interests
The author(s) declared no following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.