
Abstract
Background:
Tibiotalocalcaneal arthrodesis is a well-established procedure to treat some hindfoot diseases. Currently, the most used implants are retrograde intramedullary nails and locking plates combined with lag screws, but there are few articles comparing differences regarding the complications.
Methods:
We have retrospectively analyzed the medical records and the radiographs of patients older than 18 years who underwent this procedure in our service between 2005 and 2019 through retrograde intramedullary nails or lateral locking plates and compression screws with at least 12 months of follow-up and with no history of osteomyelitis in these bones.
Results:
We evaluated a total of 67 patients; of these, 48 received retrograde intramedullary nail implants and 19 received locking plates and compression screws. The overall mean age was 48 years; the median follow-up time was 64.3 months. The complication rate was 60.4% for the intramedullary nail procedure and 52.6% for the locking plate combined with compression screws procedure.
Conclusion:
No significant differences were found in the complication rates between the 2 implants.
Level of Evidence:
Level V, Case series
Keywords
Introduction
Tibiotalocalcaneal arthrodesis (TTCA) may be indicated in patients with advanced arthrosis of the ankle and subtalar joints, primary or secondary to several processes, such as Charcot arthropathy, avascular necrosis of the talus, neuromuscular disorders, rheumatoid arthritis, posttraumatic degeneration, congenital deformities, failure of arthroplasty, or ankle arthrodesis.2,13
Obtaining a stable fixation in this type of arthrodesis is challenging because complications such as nonunion, hardware failure, and infection are not rare. Many patients, who undergo this type of procedure, often have poor bone mineral quality, inflammatory arthropathy, bone fragmentation, or some type of neuropathy, which increases the importance of obtaining adequate fixation.1,12
In addition to biomechanical stability, factors that may contribute to good results after this arthrodesis includes proper hindfoot alignment, preservation of adjacent soft tissues and blood supply, and the ease of execution of the fixation technique. Currently, this type of fixation can be performed through isolated screws, blade plates, retrograde intramedullary nails, or locking plates associated with compression screws, the latter 2 being the most used.2,12
The clinical results of TTCA fixed with a nail or with a locking plate combined with a compression screw were demonstrated through retrospective evaluation and presented similar postoperative clinical outcomes and complication rates.10,21
The scarcity of clinical studies combined with the extensive experience of our service in using fixation techniques with compression screws and plates or retrograde intramedullary nails inspired this study, whose objective was to compare the main clinical and radiographic complications in patients subjected to TTCA through these procedures.
Patients and Methods
After approval by the research and ethics committee, we evaluated the patients subjected to TTCA by ankle and foot surgeons in our service from January 2005 to July 2019.
We analyzed the surgical records of the Foot and Ankle Group to search for operated cases, and then the data were collected through the physical and electronic medical records, including all clinical notes, surgical reports, and radiographic images.
Inclusion criteria:
Patients with hindfoot arthrosis or deformity who failed conservative treatment and who underwent TTCA with a retrograde intramedullary nail or lateral locking plate associated with compression screws in our service from January 2005 to July 2019
Patients aged 18 years or older
Exclusion criteria:
Patients with incomplete data in the medical records
Patients who did not complete the minimum follow-up time of 12 months
History of previous surgery for tibiotalar or subtalar arthrodesis
History of astragalectomy
Patients with a history of local osteomyelitis prior to treatment
The sample evaluated using the collected data included demographic data of the patients, such as age, sex, the underlying cause that led to the indication of the procedure, as well as the presence of smoking and comorbidities. We analyzed the consolidation of arthrodesis through radiographic evaluation with identification of bone bridges and/or continuity between the arthrodesis bones in orthogonal images in 50% of the local surface area, time of arthrodesis consolidation, presence complications, such as superficial and deep infection, loosening or breaking of the synthesis, residual deformity, and need for surgical revision; this was done by a board-certified foot and ankle surgeon.16,18,20
Statistical Analyses
We analyzed the results in the software IBM SPSS Statistics for Windows, version 24.0 (IBM Corp, Armonk, NY). We used chi-square for the categorical variables. And to see if the continuous data were parametric or nonparametric, we performed a Shapiro-Wilk test; if parametric, it was analyzed with the t test, and if not, with the Mann-Whitney test. Data weer considered statistically relevant when P ≤ .05.
Operative Technique
We positioned the patient in lateral decubitus, with a tourniquet positioned proximally to the thigh. The surgical drape allowed visualization of the entire leg starting from the knee to control the foot and ankle rotation during arthrodesis. We chose a lateral, transmalleolar approach by resecting the distal portion of the fibula and using it as a graft.
After osteotomy in the fibula, we obtained complete access to the ankle and subtalar joints. The joints were prepared under direct visualization by resecting the cartilage of both surfaces with osteotomes, followed by bone perforations with Kirschner 2.0 wires.
The ankle and hindfoot were positioned with 90 degrees of dorsiflexion in correlation to the tibia, 5 degrees of the calcaneus valgus, external rotation of 10 to 15 degrees, provisionally fixating with Kirshner 2.0 wires, taking care not to be in the possible path of the screws or nail.
Retrograde Intramedullary Nail
The incision of the entry point was made longitudinally, from 3 to 5 cm, and aligned with the tibial axis in the sagittal plane. Depending on the brand, the retrograde intramedullary nail (RIMN) could be straight or have a valgus angulation. If the RIMN is straight, we aligned the incision with the coronal plane’s tibial axis. In the case of an RIMN with valgus angulation, the incision is made laterally to the tibial axis in the coronal plane. The entry point in the sagittal plane was collinear with the tibial axis and, depending on the RIMN model used, was also in the coronal plane.
After passing the guide wire, the channel was milled to a diameter 1.0 to 1.5 mm larger than the RIMN, and we introduced it. Maintaining the parameters of dorsiflexion and external rotation, the RIMN was locked with one distal posteroanterior screw in the calcaneus, another in the talus, and one proximal screw.
At the end of the procedure, we performed hemostasis, cleaning, placement of the vacuum drain, layered suture, dressing, and analgesic short-leg splint (Figure 1).

Consolidation radiograph of the retrograde intramedullary nail: (A) anteroposterior weightbearing ankle view, (B) lateral weightbearing ankle view, and (C) anteroposterior weightbearing foot view.
Locking Plate and Compression Screws
The definitive stabilization began with the fixation of cannulated screws with partial thread 7.0 with a lag function. One screw was from the posterior region of the calcaneus to the body of the talus, and another was from the posterolateral region of the tibia to the anteromedial talus. Another option was using a single 7.0-mm screw entering the posterior and plantar region of the calcaneus toward the anterior tibia, compressing both joints.
We placed a plate on the lateral side for the neutralization function. The plate used was a 4.5-mm locking compression plate of the proximal humerus put in reverse. There were 3 bicortical screws in the tibia and 4 distributed between the calcaneus and talus (Figure 2).

Consolidation radiograph of the locking plate and compression screws: (A) anteroposterior weightbearing ankle view, (B) lateral weightbearing ankle view, and (C) anteroposterior weightbearing foot view.
Postoperative management
The postoperative management was the same for both techniques. We kept the patients with a short-leg splint for 1 week, then replaced it with a removable short-leg orthosis. Removed the lateral suture at approximately 14 days and the plantar suture at 21 days when the load protected by the orthosis was released and started the transition, with the help of the physiotherapy, from a partial to a full weightbearing according to the patient pain and tolerance.
In the first month, the outpatient follow-up was weekly, with radiographs with ankle and foot load at the end of this period. The patient returned with new radiographs at 2, 4, 6, and 12 months. We removed the orthosis when radiographic signs of consolidation appeared on the radiographs and allowed the use of shoes with firm soles.
Results
We analyzed a total of 67 patients (36 male and 31 female) who underwent TTCA in this period: 48 (72%) with RIMN and 19 (28%) with locking plate and compression screws (LPCS). The mean overall age was 48.0 years (19.33-80.95). The median follow-up was 64.3 months (1.8 -169.0). The most common comorbidities were rheumatoid arthritis. Patients with diabetes mellitus were subjected only to the RIMN technique (Table 1). The indications for surgery were sequelae from trauma, neuromuscular diseases, rheumatic diseases, neuropathies, congenital diseases, stage 4 flatfoot, and others (Table 2).
Patient Epidemiology.

Abbreviations: LPCS, locking plate and compression screws; RIMN, retrograde intramedullary nail.
p is the statistic comparative between the groups.
Patient Surgery Indication.

Abbreviations: LPCS, locking plate and compression screws; RIMN, retrograde intramedullary nail.
p is the statistic comparative between the groups.
Among those who underwent fixation with RIMN, 60.4% had some type of postoperative complication, which included 1 or more of the following: infection, nonunion, residual deformity, or problems with the implant; we did not have any below-the-knee amputation in these patients. Among those who used LPCS, 52.6% had some postoperative complications (Table 3).
Complications by Each Technique.
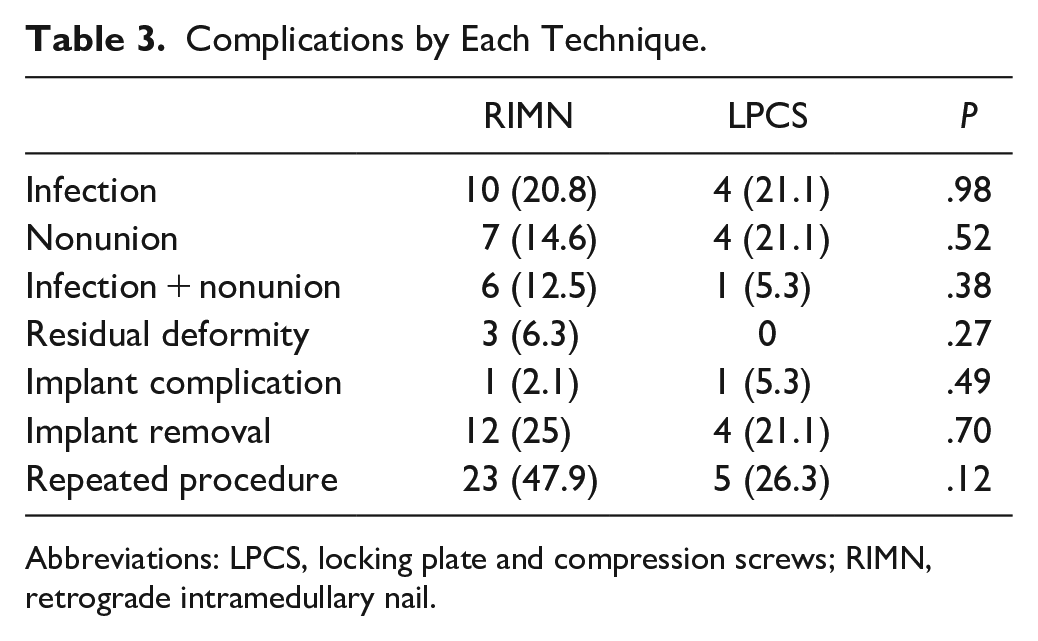
Abbreviations: LPCS, locking plate and compression screws; RIMN, retrograde intramedullary nail.
Forty-seven of the 67 patients developed arthrodesis consolidation after performing the initial procedure. The union rate of the group with RIMN fixation was 68.8% compared to 73.7% in the LPCS group (P = .69). All nonunion occurred at the tibiotalar joint (Figure 3).

(A) Tibiotalar nonunion with RIMN. (B) Tibiotalar nonunion with LPCS. LPCS, locking plate and compression screws; RIMN, retrograde intramedullary nail.
Among the patients who consolidated, 73.9% of patients who used RIMN as a fixation method consolidated in the first 4 months, whereas the remaining 26.1% of consolidation cases occurred between months 4 and 12 after the procedure. Among the patients who consolidated using LPCS and compression screws, 92.90% occurred in the first 4 months (P = .15).
Symptomatic nonunion requiring revision arthrodesis was present in 38.46% of the patients who did not consolidate with RIMN and 40% on LPCS, these data were not statistically significant. In all cases, we debrided the nonunion, performed additional grafting, and revised the hardware.
Each group had 1 episode of superficial wound infection and was treated with local care and oral antibiotics. There were 4 episodes of deep infection in the LPCS group, whereas 17 episodes were in the RIMN. Both groups were treated with surgical cleaning, debridement, and intravenous antibiotics, combined or not with implant removal.
Our hardware complication consisted of 2 cases of loosening with implant migration, 1 in each group. Furthermore, for the residual deformity, the patient had a final alignment different from 0 to 5 degrees in valgus, and in 3 of these cases, the patient needed a new surgery, with 1 being a partial hardware removal and the other 2 underwent osteotomies to realign the ankle. One-quarter of the RIMN patients had the implant removed and 21% of the LPCS group also needed this procedure; there was no statistical difference. Forty-eight percent of the RIMN was submitted to a repeated procedure and 26% of the LCPS (P = .12).
When comparing the risk of complications within patients with comorbidities, the fact that the patient had comorbidity previous to the surgery presented as the only factor with statistical significance in increasing the chance of the complication (P = .03). Neither diabetes mellitus, smoking, nor the indication showed significance when comparing the risk of complication (P > .05).
Discussion
Comparing tibiotalocalcaneal arthrodesis performed with different fixation strategies is challenging, but we sought to compare the methods most commonly used to assist in decision making when any of them could be performed. Occasionally, the choice of the implant can be dictated by previous approaches, preexisting synthesis material, or deformity, but increased complications with any of the techniques could indicate one method as better than the other. Our study revealed that both techniques have a similar complication rate. This finding is consistent with most of the comparative literature on these methods, which fails to show significantly whether one method is better than the other.10,21
Several factors have been associated with poor outcomes for patients in this type of procedure, including age and smoking, but without statistical evidence. 15 The only proven factors that increased complication rates were poorly controlled diabetes and chronic kidney disease.4,7,9,14 When comparing the risk of complications, the only factor that proved statistical significance in our cohort was the presence of comorbidity, without specifying which one. We observed that in our sample, patients with more associated comorbidities or with diabetes belonged to the group that used the RIMN technique and identified a higher rate of complications in this technique than LPCS, but without statistical or clinical significance. Our group tends to use RIMN in patients with a higher risk of soft tissue injury, which may be a bias that determined this difference.
The median patient follow-up time in this study was 64.3 months, which differs from most of the articles available in the literature, where the majority have a mean follow-up time between 12 and 36 months.2,5,6,8 -11,14,15,17,21
The literature shows a difference between the consolidation time of RIMN compared to LPCS, and on average, RIMN consolidates in 3-4 months, whereas LPCS takes 4-6 months to consolidate.3,10,12,21 In our sample, we observed the opposite, with RIMN showing a longer consolidation time than LPCS, but we did not find statistical significance. When we analyzed only the RIMN for tibiotalocalcaneal fusion, we found some questions in the literature about the shape (curve × straight line) and whether to perform compression. Thomas et al 19 reported that one of the advantages of the newer RIMN is the ability to compress the arthrodesis with screws instead of compressing it only manually during the intraoperative period. In turn, Steele et al 17 reported that the change from a straight RIMN to a 5-degree curve allows the RIMN to pass through the joints’ load center, allowing better alignment. More than 1 RIMN type was used in our patients, most without compression. We believe this may be one of the factors that contributed to a later consolidation compared with LPCS.
The nonunion rates evidenced in the literature are quite variable, and the comparison with other studies, even with similar surgical techniques, is difficult because of the definition of union (radiographic or clinical), inclusion or exclusion of medical comorbidities, and complexity of the indication. However, our consolidation rates of 70.1% agree with studies with a similar profile of patients and surgical technique, such as the study by Mulligan et al. 10
The types of pseudarthrosis can be divided into tibiotalar, subtalar, of both joints, and tibiocalcaneal pseudarthrosis in the sequelae of astragalectomy.3,5 -7,10,11 There is no consensus on which joint suffers the most from this problem or a significant change depending on the implant and surgical technique. In our patients, we also found no significant difference between the techniques, suggesting that one leads to more joint nonunion than the other. It is noteworthy that we did not see any subtalar nonunion in our study.
Another important complication is postoperative infection, which affects 34.3% of the patients and may be associated with or even cause nonunion. This value is consistent with what the literature shows, with values ranging from 15% to 36%.3,5,6,8,10,11,18,19,21 Notably, these higher values were founded in studies that analyzed fixation using RIMN. Our studied sample showed similar rates of infection between the groups. Considering that we opted for the RIMN technique in more severely ill patients due to fear of dehiscence and exposure to the implants may show that this was a fair possibility.
This study has weaknesses in that it is retrospective, patients were not randomly allocated, 4 different surgeons performed the procedures, and implants from different manufacturers were used. Strengths were sample size, follow-up time, and group homogeneity.
Conclusion
In our study, the complication rates and types between RIMN and LPCS were not significantly different. Prospective studies with well-defined methodologies may be needed to define for which pathologies one technique would be superior to another.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from USP - Hospital das Clínicas da Faculdade de Medicina da Universidade (number 04921118.1.0000.0068).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.