
Abstract
Background:
Ankle fractures involving the posterior malleolus (PM) tend to result in inferior clinical outcomes compared to other ankle fractures. However, it is unclear which specific risk factors and fracture characteristics are associated with negative outcomes in these fractures. The aim of this study was to identify risk factors for poor postoperative patient-reported outcomes in patients with fractures involving the PM.
Methods:
This retrospective cohort study included patients who sustained ankle fractures involving the PM between March 2016 and July 2020 and had preoperative computed tomography (CT) scans. In total, 122 patients were included for analysis. One patient (0.8%) had an isolated PM fracture, 19 (15.6%) had bimalleolar ankle fractures involving the PM, and 102 (83.6%) had trimalleolar fractures. Fracture characteristics including the Lauge-Hansen (LH) and Haraguchi classifications and posterior malleolar fragment size were collected from preoperative CT scans. Patient Reported Outcome Measurement Information System (PROMIS) scores were collected preoperatively and at a minimum of 1 year postoperatively. The association between various demographic and fracture characteristics with postoperative PROMIS scores was assessed.
Results:
Involvement of more malleoli was associated with worse PROMIS Physical Function (P = .04), Global Physical Health (P = .04), and Global Mental Health (P < .001), and Depression scores (P = .001). Elevated BMI was also associated with worse PROMIS Physical Function (P = .0025), Pain Interference (P = .0013), and Global Physical Health (P = .012) scores. Time to surgery, fragment size, Haraguchi classification, and LH classification were not associated with PROMIS scores.
Conclusion:
In this cohort, we found that trimalleolar ankle fractures were associated with inferior PROMIS outcomes compared with bimalleolar ankle fractures involving the PM in multiple domains.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Fractures of the posterior malleolus (PM) occur in 7% to 44% of ankle fractures, and it is generally accepted that PM involvement in ankle fractures tends to result in inferior clinical outcomes compared to other fracture types, even when the fragment is operatively fixed.3,16,17,24,35 The PM serves as a key stabilizer in resisting posterior translation at the ankle, as it is the attachment site of the posterior inferior tibiofibular ligament.9,26,31
Despite their poor prognosis, numerous aspects of PM fractures have yet to be explored in the literature, ranging from optimal surgical management to risk factors for poor patient outcomes. Historically, posterior malleolar fragment size has driven the decision for operative vs nonoperative treatment, and was suggested as a prognostic factor in these fractures.17,20,21,32 Conversely, more recent studies suggest that the morphology of the fracture, using the Haraguchi classification, may have a greater impact on clinical outcomes than the fragment size—however, it is unclear if this method has utility for assessing severity and determining treatment.1,8,12 Additionally, a variety of demographic and perioperative factors may have an association with outcomes of PM fractures but have yet to be studied.
The difficulty in establishing risk factors for poor patient-reported outcomes in posterior malleolar fractures may be attributed to 3 main factors. First, fracture size and pattern based on plain radiographs may not reflect the actual injury pattern due to rotation or superimposition. Second, variability in treatment protocols, patient demographic factors, and surgical practice between authors limit the ability to compare outcomes and determine consistent risk factors.16,28 Finally, multiple outcome score metrics, not all of which are validated, have been used in evaluating outcomes which capture different aspects of patient function.4,8,12
Understanding the risk factors associated with poor outcomes in PM fractures is important for conveying prognosis to patients and for determining optimal management. The Patient Reported Outcome Measurement Information System (PROMIS) has been increasingly utilized in foot and ankle surgery research and is validated for use with foot and ankle patients and in lower extremity fracture follow-up.15,18,30 To date, no studies have investigated the association between fracture severity, articular involvement, morphology, and operative fixation of PM fragments on PROMIS outcomes.
The aim of this study was to identify risk factors for poor postoperative PROMIS outcomes in patients with fractures involving the PM (ie, isolated PM fracture, bimalleolar ankle fracture, or trimalleolar ankle fracture) with or without operative fixation of the PM fragment. To achieve our study aim, we analyzed preoperative CT scans to evaluate the fracture pattern and fragment size along with other patient demographic factors, which have been suggested as factors associated with patient outcomes. We hypothesized that articular involvement, fracture morphology, and fracture type (unimalleolar, bimalleolar, or trimalleolar), along with known demographic factors such as body mass index (BMI) and age, would be associated with postoperative PROMIS outcomes.
Methods
Patient Cohort
This was a retrospective analysis of prospectively collected data from patients treated at our institution for a rotational ankle fracture involving the PM (including isolated PM, bimalleolar, and trimalleolar fractures) between March 2016 and July 2020. In this study, a bimalleolar fracture was defined as a fracture of the PM and medial malleolus, or PM and fibula. The protocol was approved by the research steering committee that oversees the institutional Foot and Ankle Registry, which was used to identify eligible patients. Patients were included if they sustained a fracture of the PM and if they completed both preoperative and minimum 1-year postoperative patient-reported outcome questionnaires. In total, 265 consecutive patients were identified, representing 9 foot and ankle fellowship-trained orthopaedic surgeons. One hundred patients without preoperative CT scan, and 42 without postoperative PROMIS scores were excluded, leaving 122 patients in the final cohort. Demographic data including BMI, gender, age, and time to surgery, were recorded from the medical record.
Fracture Characteristics
Fracture characteristics were reviewed on preoperative radiographs and computed tomography (CT) scans by a fellowship-trained foot and ankle surgeon. All fractures were classified using the Lauge-Hansen classification system (supination–external rotation, SER; pronation–external rotation, PER; supination-adduction, SA; pronation-abduction, PA) and LH stages (stage I, II, III, or IV) on standard anteroposterior (AP), lateral, and oblique radiographs.19,38 In addition, PM fractures were classified using the Haraguchi classification system (Type 1, posterolateral; Type 2, medial-extension; Type 3, small-shell) using CT scans.19,38 The size of the PM fragment was defined as an overall percentage of the distal articular tibial surface. This was measured using sagittal plane CT scans, which were available for all 122 patients (Figure 1). All parameters were digitally measured using a metric software system (IDS7, Sectra, Sweden).

Preoperative sagittal computed tomographic (CT) scan demonstrating percentage articular involvement of the posterior fracture fragment.
Patient-Reported Outcomes
Patient-reported functional outcomes were prospectively collected through the Foot and Ankle Registry at our institution. PROMIS surveys, which have been validated for use in foot and ankle research,13,15 were administered preoperatively just prior to surgery, and at latest available follow-up, at a minimum of 1 year postoperatively. T scores were recorded for the Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression domains. Average time to survey follow-up was 17.19 (range, 12-28.6) months.
Surgical Technique and Postoperative Protocol
The decision to fix the PM was made at the surgeon’s discretion. General criteria for operative fixation of the PM included (1) posterior dislocation, (2) concern for syndesmotic instability, and (3) concern for a large fragment affecting the articular surface with the potential to lead to significant arthritis. For operative fixation of the PM, the patient was placed in a prone or lateral position. A long posterolateral incision between the fibula and the Achilles tendon was made, and the posterior compartment was dissected first. This posterior approach has been shown to have similar outcomes to a traditional, indirect approach to fixation of the posterior malleolus. 25 The fibula was then reduced and fixed using a plate and screws. Next, the PM was reduced and fixed with a plate and screws. The patient was then turned supine. A medial incision was made for reduction and fixation of the medial malleolus if this was necessary. Finally, the syndesmosis was checked for stability and fixed using screws or a suture button device if instability was present. When no operative fixation of the PM was chosen, the patient was placed in a supine position for reduction and fixation of the medial and lateral malleoli. The posterolateral incision along with any others necessary for the procedure were then closed.
Postoperatively, patients were nonweightbearing for 6-8 weeks. Patients wore a postoperative splint for 2 weeks following surgery and were then transitioned to a controlled ankle motion (CAM) walker boot for another 4-6 weeks in order to begin range of motion exercises while remaining nonweightbearing. Over the following 4-6 weeks, patients progressively increased weightbearing.
Statistical Analysis
Descriptive analyses for BMI, gender, age, time to surgery from injury, articular surface involvement percentage, malleolar fracture type, Haraguchi classification, and postoperative PROMIS scores were calculated. The assumption of normality for continuous variables was evaluated using Shapiro-Wilk tests. Shapiro-Wilk tests demonstrated that the primary outcomes of the study, the postoperative PROMIS scores, were non-normally distributed for PROMIS Physical Function (W = 0.97, P < .001), Pain Interference (W = .90, P < .001), Pain Intensity (W = .89, P < .001), Global Physical Health (W = .96, P < .001); Global Mental Health (W = .96, P < .001), and Depression (W = .95, P < .001). For this exploratory analysis to identify risk factors for worse PROMIS outcomes, ordinary least squares regressions were utilized with BMI, age, gender, time from injury to surgery, malleolar fracture type (isolated PM vs bimalleolar vs trimalleolar), Haraguchi classification, LH classification, concomitant syndesmosis fixation, and articular surface involvement percentage as predictors, and postoperative PROMIS scores as outcome variables. Wilcoxon signed-rank test was used to test for association between the presence of fracture-dislocation of the tibiotalar joint on initial presentation and postoperative PROMIS scores. A subgroup analysis was performed to assess whether articular involvement (≥25% vs <25%) was associated with PROMIS scores in subgroups with operatively fixed PM and nonfixed PM using ordinary least squares regression analysis, since this percentage has been historically used as a threshold for operative treatment.16,22 Another subgroup analysis was performed to assess whether operative fixation was associated with PROMIS scores in subgoups based on fragment size (≥25% and <25%) using ordinary least squares regression. P values of less than .05 were considered statistically significant. All analysis was conducted using RStudio (Boston, MA).
Results
Demographics and Fracture Characteristics
Average age at the time of surgery was 48.7 (range, 14-88) years, average BMI was 26.8, and 76 patients (62.3%) were female (Table 1). Of the 122 patients, 72 (59%) had operative fixation of the PM, and 50 (41%) were treated nonoperatively. Average percentage of articular involvement of the PM fragment was 15.1%. One patient (0.8%) had an isolated PM fracture, 19 (15.6%) had bimalleolar ankle fractures involving the PM, and 102 (83.6%) had trimalleolar fractures. Thirty-four of the patients had fracture-dislocations of the tibiotalar joint on initial presentation that were reduced in the emergency department. None of the patients in this cohort required external fixation for their ankle fractures. The distribution of Lauge-Hansen and Haraguchi classifications of the fractures in the study cohort are tabulated in Table 1. 12 Thirty-seven (30.3%) patients underwent syndesmotic fixation at the time of surgery, and 12 (9.8%) underwent concomitant deltoid reconstruction.
Demographics and Fracture Characteristics (Total N = 122).

Abbreviations: PA, pronation-abduction; PER, supination-adduction; PM, posterior malleolus; SA, pronation-abduction; SER, supination-external rotation.
Patient-Reported Outcomes
Demographic predictors of postoperative PROMIS scores are found in Table 2. Elevated BMI was found to be significantly associated with lower postoperative PROMIS Physical function (P = .0025), higher Pain Interference (P = .013), and lower Global Physical Health (P = .012) scores, indicating more severe functional disability and greater pain. BMI was not a significant predictor for Pain Intensity (P = .09), Global Health Mental (P = .71), or Depression (P = .33) scores. Time to surgery was not found to be significantly associated with any of the postoperative PROMIS domains (P > .05).
Results of OLS Regression Analyses to Determine Associations of Demographics and Fracture Characteristics With Postoperative PROMIS Scores. a

Abbreviations: LH, Lauge-Hansen; OLS, ordinary least squares; PM, posterior malleolus; PROMIS, Patient Reported Outcomes Measurement Information System.
Data are reported as estimates and P values of OLS regression analyses. Significant predictors are bolded. A P value of less than .05 was considered statistically significant.
Fracture characteristics and operative factors associated with postoperative PROMIS scores are found in Table 2. Significant associations were found between malleolar fracture type and postoperative PROMIS Physical Function (P = .04), Global Physical Health (P = .04), and Global Mental Health (P < .001) scores, with increasing malleolar involvement being associated with lower Physical Function, lower Global Physical Health, and lower Global Mental Health scores. Haraguchi classification scores and LH classification were not associated with any postoperative PROMIS score domains. Additionally, the percentage of articular involvement and presence of syndesmosis fixation were not significantly associated with any postoperative PROMIS outcomes. The presence of fracture-dislocation on initial presentation was also not significantly associated with postoperative PROMIS scores in the Physical Function (P = .67), Pain Interference (P = .42), Pain Intensity (P = .76), Global Physical Health (P = .41), Global Mental Health (P = .80), and Depression (P = .84) domains.
Subgroup Analyses
In the subgroup of articular involvement greater than 25%, operative fixation of the fracture was associated with lower postoperative PROMIS Pain Interference (P = .0037), lower Pain Intensity (P = .032), greater Global Physical Health (P = .046), and lower Depression (P = .020). Operative fixation was not associated with postoperative PROMIS Physical Function (P = .095) or Global Mental Health (P = .28) in the >25% articular involvement subgroup (Table 3). There were no significant differences in PROMIS scores based on operative fixation vs nonoperative fixation in the <25% articular involvement subgroup (Table 3).
Effect of Operative Fixation on Postoperative PROMIS Scores in Subgroups of Less Than and Greater Than 25% Articular Involvement. a

Abbreviation: PROMIS, Patient Reported Outcomes Measurement Information System.
Data are reported as mean (SD), estimates, and P values from ordinary least squares regression analysis. Significant predictors are bolded. P values less than .05 were considered statistically significant.
No significant differences were found based on amount of articular involvement (≥25% vs <25%) in the operatively fixed subgroup (Table 4). However, in the nonfixation subgroup, articular involvement greater than 25% was associated with greater PROMIS Pain Interference scores (P = .014), greater Pain Intensity scores (P = .012), and lower Global Physical Health scores (P = .044). Articular involvement was not associated with postoperative PROMIS physical function scores (P = .11), Global Mental Health scores (P = .066), or Depression scores (P = .12) in the nonfixed subgroup (Table 4).
Effect of Articular Involvement on Postoperative PROMIS Scores in Operatively Fixed and Nonoperatively Fixed PM Subgroups. a
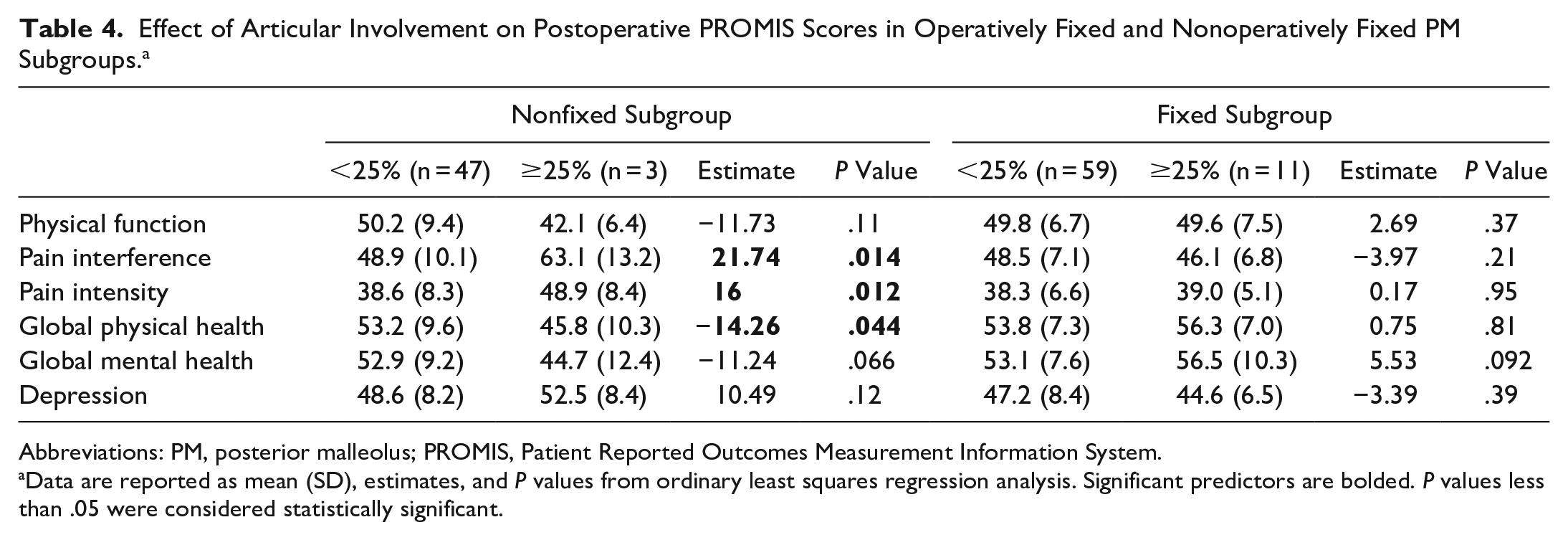
Abbreviations: PM, posterior malleolus; PROMIS, Patient Reported Outcomes Measurement Information System.
Data are reported as mean (SD), estimates, and P values from ordinary least squares regression analysis. Significant predictors are bolded. P values less than .05 were considered statistically significant.
Complications and Removal of Hardware
There were no cases of postoperative infection or delayed wound healing in this cohort of patients. Forty-one patients underwent subsequent removal of hardware at an average of 8.6 months after index surgery. Syndesmosis hardware was removed in 29 cases, medial malleolar hardware was removed in 17 cases, fibular hardware was removed in 17 cases, and posterior malleolar hardware was removed in 3 cases.
Discussion
In this study, we demonstrate that fracture severity at the time of injury is associated with postoperative PROMIS scores in patients with PM fractures. Although trimalleolar involvement and elevated BMI were associated with worse postoperative functional outcomes, no associations with PROMIS outcomes were found for fracture morphology, fracture mechanism, articular involvement, or operative fixation.
Trimalleolar involvement of the ankle fracture was significantly associated with poor PROMIS outcomes in multiple PROMIS domains in our study. Because we only had 1 patient with an isolated PM fracture in this cohort, the association we found predominately reflects differences between the bimalleolar (n = 19) and trimalleolar (n = 102) fractures involving the PM. Trimalleolar fractures tend to occur in more severe fracture mechanisms with higher rotational force, resulting in more soft tissue damage. 3 Additionally, more dissection during operation along with stricter immobilization may lead to increased stiffness and scar formation postoperatively. Previous studies have demonstrated worse subjective outcomes in trimalleolar fractures when compared to bimalleolar and unimalleolar fractures,20,21 but few studies have evaluated these differences using validated patient-reported outcome measures. A recent study by Hong et al 14 found that there were no differences in functional outcomes measured by Olerud and Molander scores between bimalleolar and trimalleolar fractures at 2 years postoperatively in their cohort of 47 ankle fracture patients. However, their small sample size of trimalleolar ankle fractures (n = 31), and the use of a different functional outcome score limits our ability to compare results directly. Gilley et al also found a nonnormal distribution of postoperative PROMIS Physical Function scores across fracture subtypes, with worse PROMIS Physical Function scores in patients with bimalleolar and trimalleolar involvement, when compared to isolated medial, lateral, and posterior malleolar fractures. 11 Our results support that trimalleolar fractures are associated with worse patient-reported outcomes as measured by PROMIS. However, it is important to consider that our sample size of 19 patients in the bimalleolar ankle fracture group is small compared to our larger sample size of trimalleolar fractures, which may decrease the strength of this finding.
BMI was the most common risk factor associated with negative outcomes in multiple PROMIS domains, including Physical Function, Pain Interference, and Global Physical Health. A multitude of factors may explain this relationship, such as increased compressive force on the fracture site leading to a more severe fracture, presence of comorbid metabolic issues associated with obesity, and increased risk of infections, wound complications, and poor healing. 2 However, there were no cases of infection or wound complications in this cohort of patients, suggesting that BMI itself may be influencing outcomes. This finding is in agreement with the trend of increased BMI being predictive of lower PROMIS Physical Function scores after orthopaedic injuries and ankle fractures in general.5-7,33 It is also possible that patients with higher BMI may have worse preoperative PROMIS Physical Function and Global Physical Health scores prior to the injury that can influence the postoperative results, so this limitation must be taken into account. Despite this, patients with higher BMI still had worse postoperative Pain Interference scores, which are likely not affected by BMI preinjury. Although we did not find a specific BMI cutoff where outcomes were worse, based on these previous studies, obese patients with BMI >30 may be at risk for poor outcomes.6,7,33
An association between fracture morphology (specifically, Haraguchi classification) and patient-reported outcomes have been suggested.1,12,27 Blom et al 1 found that Haraguchi type 2 fractures, involving medial extension of the fracture line, had poorer Foot and Ankle Outcome Scores at 2-year follow-up. Similarly, Raeder et al demonstrated that type 2 PM fractures had poorer American Orthopaedic Foot & Ankle Society ankle-hindfoot scores at 6 weeks and 6 months after injury. 27 In contrast to these previously reported findings, we demonstrate that Haraguchi classification was not a significant predictor of poor 1-year outcomes in any PROMIS domain. This contrast in results may be attributed to differences between PROMIS, Foot and Ankle Outcome Score, and American Orthopaedic Foot & Ankle Society ankle-hindfoot score questionnaires that may capture different aspects of a patient’s disability after ankle fracture. The PROMIS questionnaire may be too global to demonstrate differences between these types of ankle fractures. Further studies investigating the effect of Haraguchi classification on PROMIS outcomes are necessary to support these results and evaluate the utility of PROMIS in PM fracture studies.
Similarly, fracture mechanism based on the Lauge-Hansen (LH) classification was not associated with postoperative PROMIS scores. The limitations of the LH classification system have been described in many previous studies, as it has been documented to have poor interobserver reliability, and it does not reliably predict injury to the surrounding ligaments, which is important in determining fracture stability.8,10,22,23,29,34 Therefore, its utility in predicting clinical outcomes of ankle fractures is limited, and it may be helpful to include other radiographic classifications when evaluating these injuries. 34
The traditionally accepted cutoff for surgical treatment of a PM fracture was an injury that, on radiographic examination, involved more than 25% of the articular surface.20,22 Later research suggested that this may not be the case, 7 and van den Bekerom et al 36 concluded that there is a lack of high-level evidence to support this 25% cut-off in determining surgical treatment. Our results partially corroborate these findings, as a treatment threshold of 25% resulted in no significant differences in patient-reported outcomes in the operatively fixed subgroup. Conversely, other factors such as the presence of dislocation or postoperative step-off and gapping may be more important than fracture size with regard to postoperative outcomes in patients with operatively fixed PM.8,37 However, in the nonfixed subgroup, patients with >25% articular involvement had worse Pain Interference, Pain Intensity, and Global Physical Health outcomes. Although this analysis is exploratory in nature and likely limited by sample size, it suggests worse outcomes in patients with nonfixed PM and greater articular involvement. Future studies with fully powered samples are necessary to further explore these findings.
Additional subgroup analysis demonstrated that operative fixation of the PM fragment did not result in better outcomes compared to nonfixed fractures in the subgroup of patients with articular involvement <25%. However, in patients with articular involvement >25%, presence of operative fixation resulted in better PROMIS Pain Interference, Pain Intensity, Global Physical Health, and Depression scores, suggesting that operative fixation of the PM may still be beneficial in cases with greater articular involvement. As previously stated, these results are limited by a small sample size in each subgroup, and have limited implications on surgical decision making of fixing the PM, because the present study included multiple surgeons who used their own discretion and experience to decide whether to fix the PM fragment. There are many confounding factors that can also explain these outcomes; for example, increased preoperative step-off or more severe deformity may influence the surgeon’s decision to operate on the fragment. Additionally, the posterolateral approach for fixation of all PM fractures may have influenced the operative results, as this approach may not be the routine approach used by most orthopaedic institutions, possibly decreasing the generalizability of our findings.
This study has several limitations. Because of the retrospective nature of this study, the decision to initially treat the PM fracture with surgical fixation was made at the surgeons’ discretion. However, inclusion of multiple surgeons in the study may reduce any particular bias toward a certain criterion for fixing the PM and may make the results more applicable to a wider range of surgeons. Additionally, although we found that the presence of syndesmosis fixation was not associated with postoperative PROMIS scores, subsequent surgery to remove hardware from the syndesmosis may affect outcomes. This study may be underpowered to detect a true difference in operative vs nonoperative patient-reported outcomes. Specifically, the small sample size in the nonsurgical subgroup may present a power limitation in the subgroup analysis. Patient enrollment was based on sampling by convenience, in which all eligible patients that met the inclusion and exclusion criteria during the study period were included. Additionally, postoperative reduction status was not objectively evaluated in this study, and postoperative CT scans were not analyzed because it was not routine postoperative standard of care for patients without symptoms. Finally, all radiographic criteria and classifications were evaluated by a single rater.
Conclusion
In this retrospective analysis of our cohort of patients with PM fractures, trimalleolar fractures were associated with poor postoperative patient-reported outcomes. However, an association was not found for Haraguchi type, LH classification, or PM fragment size. The results of the current study suggest that, in the short term, patients with a higher BMI and trimalleolar involvement may benefit from education on the prognosis of their fracture and a clear setting of expectations.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Foot and Ankle Registry Steering Committee of the authors’ institution (IRB 2013-038).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.