
Abstract
Background:
Physical therapy (PT) following total ankle replacement (TAR) is often considered, but guidelines for its use are not standardized. Although patient factors may dictate recommendations, this retrospective cohort study aims to characterize baseline utilization practices to set the stage for establishing generalizable recommendations.
Methods:
TAR patients were identified from the 2010-2019 M91 Ortho PearlDiver data set based on administrative coding. Patient factors were extracted, including age, sex, Elixhauser Comorbidity Index (ECI), region of the country in which patients’ surgery was performed (Midwest, Northeast, South, West), and insurance plan (commercial, Medicaid, Medicare). The incidence, timing, and frequency of home or outpatient PT utilization in the 90 days following TAR were identified. Inpatient PT was not captured. Univariate and multivariate logistic regression analyses allowed identification of predictive factors for PT utilization.
Results:
Of 5412 TAR patients identified, postoperative PT services were used by 2453 (45.3%). Most PT was outpatient (38.3% of the study population) compared to home (4.1% of the study population). Weekly utilization of PT was greatest in the first week following surgery (17.7% of PT visits) and thereafter followed a roughly bell-shaped curve, with utilization greatest at 7 weeks following surgery (14.9% of PT visits).
Independent predictors of PT utilization following TAR included having surgery performed in the Midwest (relative to the South, OR 1.37, P < .0001), Northeast (OR 1.20, P = .0217), or West (OR 1.26, P < .0021) and having commercial (relative to Medicare, OR 1.87, P < .0001) or Medicaid insurance (OR 1.46, P = .0239).
Conclusion:
Of 5412 TAR patients, 42.5% used PT within 90 days of surgery. PT utilization was highest in the first and seventh weeks following surgery, and demographic predictors of PT use were defined. Through identification of timing and predictors of PT utilization following TAR, PT care pathways may be better defined.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Containing costs and improving efficiency while optimizing patient care is an increasingly important focus in health care, and much research is being done with the goal of establishing best practices to ensure consistent care delivery.12,23 Physical therapy (PT) following procedures such as total ankle replacement (TAR) is an area where guidance is limited, and inconsistency is anticipated.
PT is common in many areas of orthopaedics to improve mobility, optimize motion, and limit contractures.7,12,16,21 Despite this, different areas of orthopaedics have shown variability in the application of PT services.
For example, previous studies have demonstrated significant variation in postoperative PT use following anterior cruciate ligament reconstruction, despite it being associated with improved outcomes.1,4,25 In fact, PT utilization was variable based on patient characteristics such as age, sex, or insurance coverage.1,19 One study found that compliance with defined rehabilitation protocols following anterior crucial ligament reconstruction was significantly associated with return to preinjury functional levels. 4
Similarly, PT plays several essential roles in the patient recovery process following TAR, including limiting edema, promoting wound healing, preventing thrombotic events, reducing muscular hypotrophy, as well as improving mobility and balance.17,18 Given these benefits, PT is an important component of effective care pathways following TAR.
Despite the importance of PT following TAR, guidelines for its use are discordant, with no current consensus on postoperative rehabilitation protocols currently existing.14,18 No major orthopaedic surgery society currently provides detailed recommendations for PT utilization following TAR. Different health systems and orthopaedic practices recommend varied physical therapy protocols for TAR patients. Centers vary on when to start therapy as well as the number of visits.13,24 Potentially, understanding the current state of PT across varied centers could help set the stage for general guidelines for PT use in this setting.
The present study, therefore, aims to describe trends in home and outpatient PT utilization following TAR across the United States using a national administrative database. Specifically, it seeks to define the timing, service location, and predictive factors for postoperative PT use, which can provide foundational understanding to guide efficient, consistent delivery of care.
Methods
Database and Cohort
This retrospective cohort study was performed using data abstracted from the 2010-2019 PearlDiver (Colorado Springs, CO) M91Ortho data set. The M91Ortho data set is a large health administrative database containing Health Insurance Portability and Accountability Act (HIPAA)–compliant data covering nearly 91 million orthopaedic patients in the United States. Given that all data within PearlDiver is deidentified and aggregated, our institutional review board (IRB) exempts studies using this database exemption from review.
Patients who underwent TAR were identified using Current Procedural Terminology (CPT) code 27702 (total ankle reconstruction with implant). Only patients with at least 90 days of follow-up following TAR in the data set were included in the study.
After patient identification, several cohort characteristics were tabulated, including average age, sex, average Elixhauser Comorbidity Index (ECI, a measure of patient comorbidity based on ICD diagnosis codes), region of the country (according to US Census Bureau definitions) in which TAR was performed (West, South, Midwest, Northeast), and patient insurance plan (Commercial, Medicaid, Medicare).
Physical Therapy Utilization Following TAR
Physical therapy (PT) utilization in the 90 days after TAR was abstracted by using home and outpatient Current Procedural Terminology codes. Inpatient PT utilization was not captured. Using these data, the daily number of PT utilization events was determined for each day in the 90 days following TAR and subsequently used to determine weekly and total number of PT visits in the 90 days following TAR. Baseline weekly PT utilization was determined by calculating the average weekly incidence of PT utilization in the cohort for the 13 weeks prior to TAR.
Implant Survival
Patients who underwent ankle joint revision following TAR were identified by CPT-27703. Identification of these patients was used to evaluate for differences in 5-year implant survival between patients who did and did not undergo PT following TAR.
Data Analysis
Univariate analysis was used to compare demographic factors of patients who did and did not receive PT in the 90 days following TAR. Patient sex, region of the country in which TAR was performed, and insurance plan were compared between the 2 groups using Pearson chi-squared test. Patient age and ECI of patients in the 2 cohorts were compared with Welch T test.
Multivariate logistic regression was then performed to determine independent predictors of PT utilization following TAR. Odds ratios (ORs) and 95% CIs were calculated for each patient demographic factor analyzed and compared to referent categories.
By separating patients who received PT following TAR at home or in an outpatient setting, univariate and multivariate analyses were used to compare these 2 subcohorts in a fashion similar to PT vs no PT. For this analysis, categories were made exclusive, with any patient who received home PT following TAR being excluded from the cohort designated as having received outpatient PT only. The percentage of patients who had home PT who went on to have outpatient PT in the 90 days following TAR was also determined.
Kaplan-Meier analysis was used to compare the survival of TAR implants between patients who did and did not receive PT following surgery up to 5 years following their procedure. A log-rank test was performed to evaluate for any significant difference in 5-year survival between the 2 groups.
PearlDiver’s in-built statistical analysis software was used to conduct all statistical analyses, with statistical significance being reached at P <.05. Prim9 (GraphPad Softwares, San Diego, CA) and Microsoft Excel (Microsoft Corporation, Redmond, WA) were used to create all figures.
Results
Study Cohort and Incidence of Physical Therapy Utilization
In total, 6282 TAR patients were identified. Of this population, 312 (4.96%) were excluded because of less than 90-day postoperative follow-up in the PearlDiver database; 551 (8.77%) were excluded because of having a trauma, neoplasm, or infection diagnosis in the 90 days prior to TAR; and 7 (1.11%) were excluded for being <18 years of age. As such, the final cohort for the present study contained 5412 TAR patients, of which 2453 (45.3%) underwent at least 1 PT session in the 90 days following TAR.
The occurrence of PT in the 90 days (13 weeks) following TAR, as well as the weekly distribution of PT utilization, is shown in Figure 1. Of all PT occurrences in the 90 days following TAR, 31.2% took place in the first week following surgery. PT utilization dropped steeply in the second week following surgery (2.35% of the study cohort), with a subsequent gradual increase through week 7 following surgery (13.7%). After week 7, weekly PT utilization again dropped through the 13th week following surgery (1.95%).
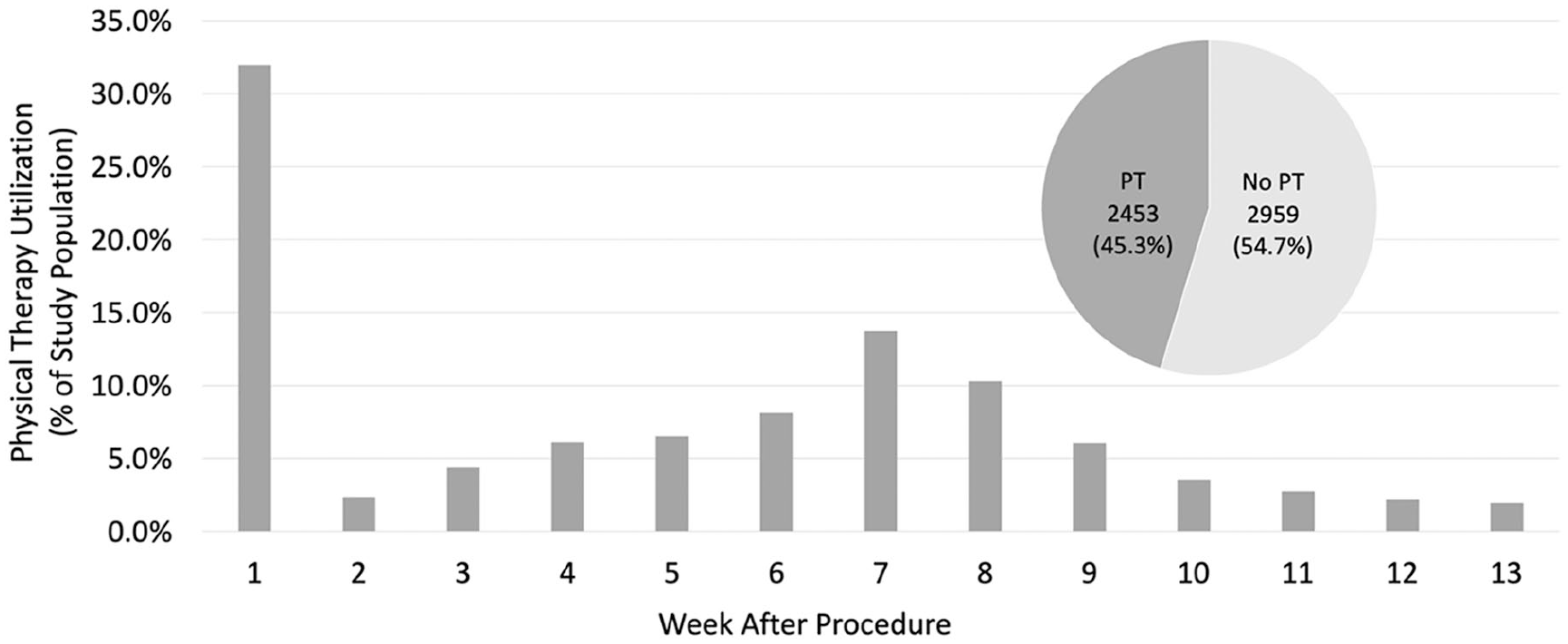
Weekly physical therapy visits after total ankle arthroplasty surgery. PT, physical therapy.
Factors Associated With PT Utilization Following TAR
Demographics of patients who did and did not receive PT following TAR are depicted in Table 1 (2959 and 2453 patients, respectively). On univariate analysis, those who went to PT in the postoperative period were slightly older, sicker, and from different regions of the country and with different insurance (P < .0001 for each).
Demographics of Patients Not Utilizing and Utilizing Physical Therapy Following Total Ankle Replacement. a

Abbreviations: ECI, Elixhauser Comorbidity Index; PT, physical therapy (includes both home and outpatient therapy).
Unless otherwise noted, values are n (%). Statistical significance was established at P <.05 (indicated in bold).
Multivariate analysis revealed no difference between those who did vs did not receive PT with regard to age, sex, or comorbidity status (Table 2). However, having PT following TAR was independently associated with having TAR performed in the Midwestern, Northeast, or Western United States (odds ratios [ORs] compared to South were 1.37, P < .0001; 1.20, P = .217; and 1.26, P = .0021, respectively). Furthermore, those with Commercial and Medicaid insurance were more likely to receive PT following TAR (compared to Medicare patients OR 1.87, P < .0001, and 1.46, P = .0239, respectively).
Multivariate Analysis of Predictive Factors for PT Utilization (N = 6282).
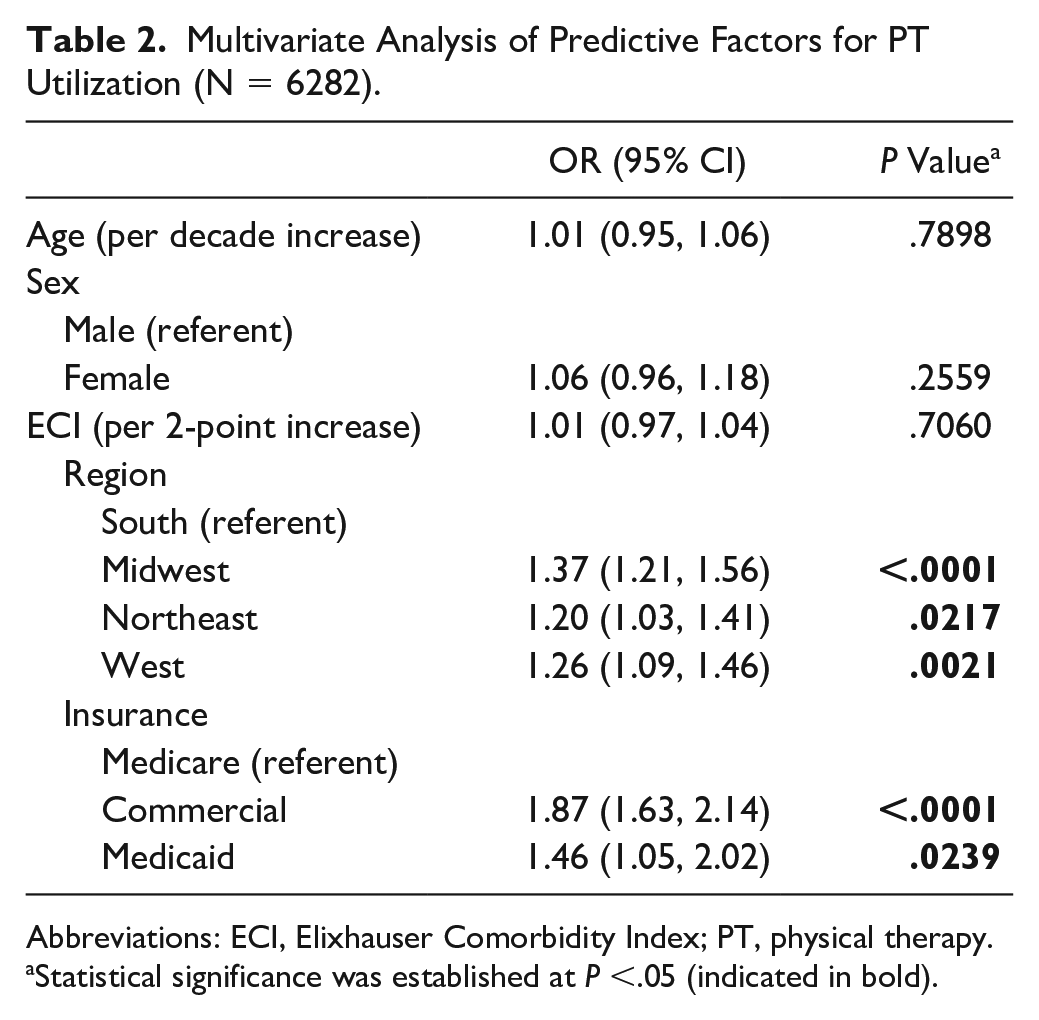
Abbreviations: ECI, Elixhauser Comorbidity Index; PT, physical therapy.
Statistical significance was established at P <.05 (indicated in bold).
Factors Associated With Home vs Outpatient PT Following TAR
Patients receiving PT at home vs outpatient were then subcharacterized (Table 3). Most PT visits were outpatient (n = 2074) vs at home (n = 224). Overall, 42.9% of patients who had home PT subsequently had outpatient PT within 90 days of TAA and could have been counted in both subgroups. Those receiving home PT were more likely to be female (P < .001) and from certain parts of the country (P = .0014).
Demographics of Patients Who Performed Physical Therapy at Home or in an Outpatient Center Following Total Ankle Replacement. a

Abbreviation: PT, physical therapy.
Unless otherwise noted, values are n (%). Statistical significance was established at P <.05 (indicated in bold).
Multivariate analysis revealed that getting PT at home vs outpatient was independently associated with older age (per decade increase, OR 1.61, P < .0001), female sex (compared to male, OR 2.05, P < .0001), higher ECI (per 2-point increase, OR 1.22, P < .0001), having TAR performed in the northeastern United States (compared to South, OR 1.74, P = .0031), and having commercial insurance (compared to Medicare, OR 2.46, P < .0001) (Table 4).
Multivariate Analysis of Predictive Factors for Home PT Utilization vs Outpatient PT (N = 6282).

Abbreviations: ECI, Elixhauser Comorbidity Index; PT, physical therapy.
Statistical significance was established at P <.05 (indicated in bold).
TAR Implant Survival
To get a sense of the potential long-term impact of PT on TAR implant survival, 5-year survival of TAR implant to revision of those with vs without 90-day postoperative PT are shown in Figure 2. Five-year survival (standard error) for patients who received PT following TAR was 95.6% (0.52%), compared with 95.4% (0.48%) among patients who did not undergo PT following surgery. Rank log test revealed no statistically significant difference in implant survival between the 2 groups.

Survival of implant following total ankle replacement. PT, physical therapy.
Discussion
Total ankle replacement is increasingly considered. 10 However, there is variation in the postoperative management of these patients, and a better understanding of aspects of their care might help establish improved care pathways. To that end, the present study found that following TAR, 45.5% received physical therapy, highlighting the previously reported lack of consistency in postoperative rehabilitation. 14
Of those who received postoperative PT, the greatest use was in the first week, and then there was a bell-shaped distribution of visits from weeks 2 to 13, peaking at week 7. The early peak is expected to be for general mobilization and initiation of ankle motion, as some have advocated. 6 The subsequent bell-shaped distribution is interpreted as the implementation of further exercises that have been advocated for week 2,3,5,20 week 4,8,9,11 or week 6.1,2,15
By multivariate analysis, those who used PT were of different geographies in the United States (more in the Midwest, Northeast, and West) or of varying insurance (more for commercial or Medicaid). Previous literature has demonstrated geographic variation 10 and patient insurance status 22 as significant predictors of utilization of and outcomes following total ankle replacement. The fact that these, and not patient factors, were the significant determinants of using PT suggests that patient-specific factors are not the primary determinants at present and that more uniform best practices should be established consistent care plans.
In terms of where PT was provided, the majority was delivered as outpatient, as opposed to at home. Although there were some geographic and insurance differences for this by multivariate analysis, the difference in patient demographics (age, sex, and ECI) suggests more patient-specific and functional considerations.
The TAR implant surgical analysis did not show a difference between those who did and did not receive PT in the postoperative period. However, this is a relatively crude assessment and does not differentiate functional differences.
As with other national database studies, the current study is limited by the administrative nature of the data. However, the occurrence or not of PT is expected to be a well-recorded event. Additionally, individual factors leading to decisions to use or not use PT could not be assessed. Further, functional outcomes could not be determined.
In summary, PT was inconsistently used following TAR in the sizeable national cohort presented here. Given the size and diversity of the patient population analyzed, the results of the present study are presumably of high generalizability. Of the postoperative PT, most was outpatient, and patient factors other than geography and insurance were not the differentiator of use. Current practice patterns are defined and seem to highlight the need to strive for more consistent protocols.
Footnotes
Ethical Approval
Ethical approval for this study was waived by Yale Institutional Review Board because this work does not involve human subjects.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Philip P. Ratnasamy, BS, reports grants or contracts from National Institutes of Health Award 2T35HL007649-36. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health award 2T35HL007649-36 was used to support the completion of this study.