
Abstract
Background:
Intramedullary nailing of the fibula (FN) is a method of fixation that has proven to be useful for treating distal fibular fractures (DFs). FN minimizes soft tissue complications and provides similar stability to plating, with fewer hardware-related symptoms. Nevertheless, FN has been associated with syndesmotic malreduction and the incapacity of restoring length and rotation of the fibula. We aimed to evaluate the fibular position and syndesmotic reduction after fixation with FN compared with the uninjured ankle in the immediate postoperative period.
Methods:
Prospective cohort study. Patients with DF fractures treated with IN between January 2017 and January 2020 were included. Immediate postoperative bilateral ankle CT was obtained in all cases. Fibular rotation, length, and translation as well as syndesmotic diastasis were measured on both ankles and compared by 3 independent observers.
Results:
Twenty-eight patients were included (16 women). The mean age was 46 years (range 16-91). Fracture type distribution according to AO/ASIF classification included 19 patients with 44.B (67.9%), 8 patients with 44.C (28.6%), and 1 patient with a 44.A fracture (3.6%). No significant differences were identified considering fibular rotation (P = .661), syndesmotic diastasis (P = .147), and fibular length (P = .115) between the injured and uninjured ankle. Fibular translation had statistical differences (P = .01) compared with the uninjured ankle. The intraclass correlation coefficient showed an excellent concordance between observers except for fibular translation on the injured ankle.
Conclusion:
In this cohort, fixation of DF fractures with FN allows restoration of anatomical parameters of the ankle in terms of fibular rotation, length, and syndesmotic diastasis. However, fibular translation had significant differences compared with the uninjured ankle based on bilateral CT scan evaluation.
Level of Evidence:
Level II, prospective cohort study.
Introduction
Ankle fractures are one of the most common injuries in orthopaedic practice, and their incidence is expected to increase mainly because of the growing number of people participating in sports activities and a progressively aging population sustaining osteoporotic fractures.14,38 For decades, open reduction and fibular plating have been the gold standard of treatment of ankle fractures with distal fibular involvement.3,11 Nevertheless, intramedullary nailing of the fibula has gained popularity in recent years, with the advent of anatomical and stable implants being at least equivalent from a mechanical point of view to traditional lag screw and plate constructs.9,33,36 Moreover, the clinical and functional results regarding the use of this type of device have been promising in comparison to the standard methods of fixation.7,18,43
Intramedullary nailing of the fibula is a minimally invasive treatment that is especially useful in diabetic and elderly patients because of the higher complication and hardware removal rate associated with open approaches in these populations.2,23,34 Multiple studies had reported on clinical, functional, and cost-effectiveness results regarding fibular nailing in these groups of patients.4,10,28,42 However, results on the restoration of anatomical parameters after fibular nailing in ankle fractures have been scarce. This is mainly because the objective of using these devices is not the anatomical reduction of the fracture site but rather obtaining relative stability allowing the reestablishment of fibular length, alignment, and rotation. In this context, in diabetic and elderly patients it is privileged to avoid soft tissue complications by apparently accepting malreduction on the fracture site. Under this assumption, a higher risk of osteoarthritis due to the latter may be acceptable in lower-demand patients.
First- and second-generation fibular nails did not achieve optimal control of rotation and length nor allowed fixation of the syndesmosis.6,17 Third-generation locked devices not only allow syndesmotic fixation but also rely on tibiofibular fixation to increase rotational and axial stability.6,8,16 The quality of reduction of the syndesmosis in ankle fractures stabilized with traditional plating has been widely studied as it plays an essential role to restore normal ankle mechanics and preventing secondary degenerative changes.12,26,30,39,41 Nevertheless, to our knowledge syndesmotic reduction after intramedullary fixation of distal fibular fractures has not been previously studied.
The aim of this study was to assess the capacity of a third-generation fibular nail to restore the anatomic parameters of the fibula in terms of length and rotation as well as an anatomic syndesmotic reduction compared to the uninjured ankle. As the indication of intramedullary fixation increases in high-demand and younger patients with ankle fractures, these results may be helpful to support shifting the standard of care in this population.
Patients and Methods
A prospective IRB-approved study was conducted between January 2017 and January 2020 including consecutive ankle fractures treated with fibular intramedullary nailing in a level 1 trauma center. All procedures were performed by 4 fellowship-trained foot and ankle orthopaedic surgeons. The decision to use fibular nailing was made at the discretion of the surgeon considering potential soft tissue complications influenced by the patient’s age, medical comorbidities, skin condition, and fracture comminution. Exclusion criteria included open fractures, fibular fractures in the context of distal tibia or pilon fractures, previous ipsilateral or contralateral ankle fractures, neuroarthropathy injuries, and bilateral ankle fractures.
Surgical Technique
Patients were positioned supine with a bump under the ipsilateral hip to allow adequate internal rotation of the ankle during the procedure. General or regional anesthesia was used associated with a thigh tourniquet. Fracture reduction was performed under fluoroscopic assistance using pointed reduction forceps percutaneously (Figure 1). If closed reduction was successful both on frontal and lateral planes, the surgeon would proceed with the installation of a fibular nail. A third-generation nonproximally locked Acumed fibular nail (Acumed LLC, Hillsboro, Oregon) was used in all patients using minimally invasive approaches. In cases where closed reduction was not satisfactory, a 1-cm lateral mini-open incision was made to rule out any interposed tissues preventing reduction. In the event of persistent fluoroscopic malreduction, conversion to an open procedure and fixation were performed using conventional plating.
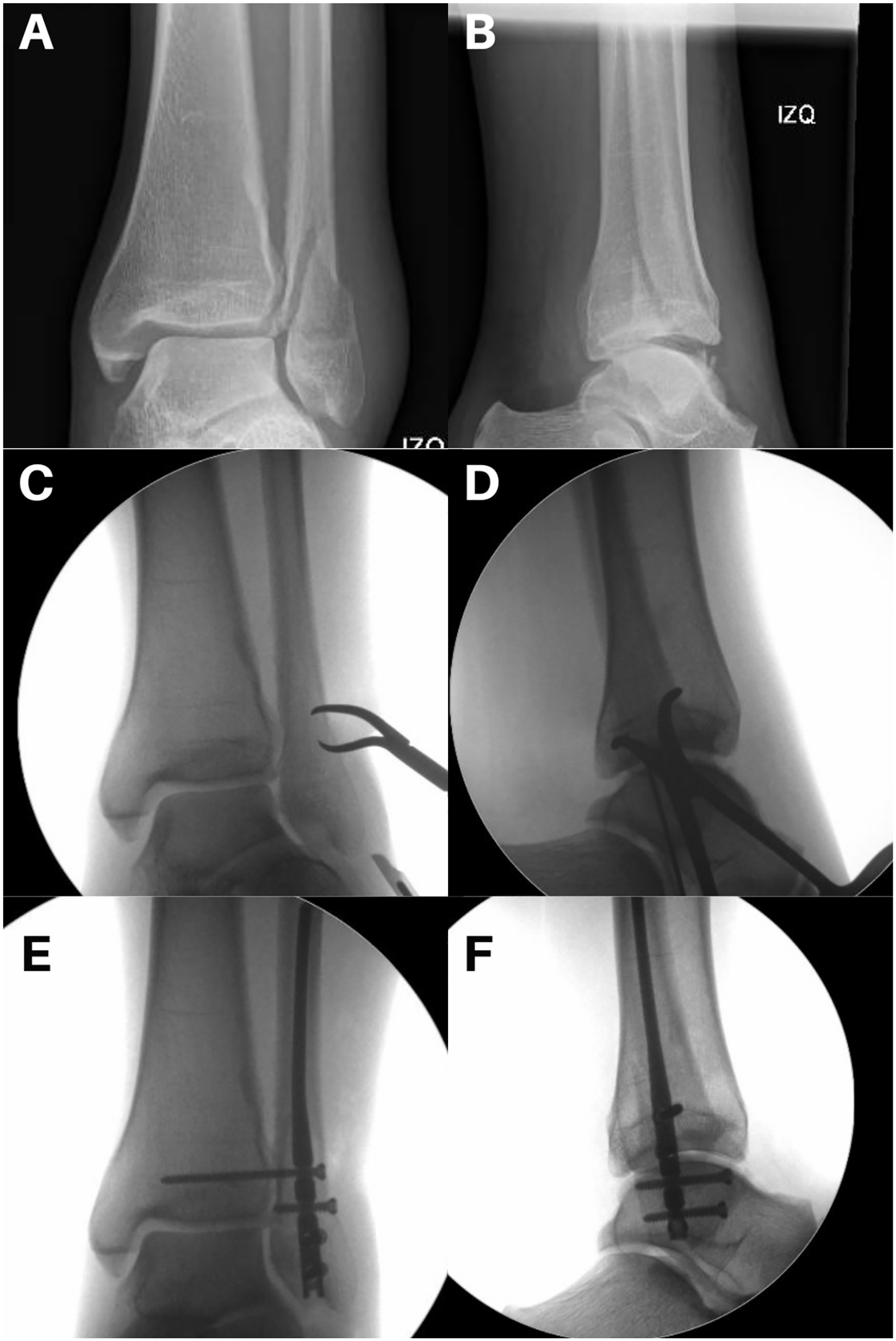
Fibular nailing of displaced malleolar fracture. (A, B) Anteroposterior and lateral radiograph of a Weber B ankle fracture. (C, D) Percutaneous reduction using clamps before nail installation. (E, F) Final intraoperative result.
Syndesmotic stability was tested once the fibular nail was fixed distally using the external rotation stress test under fluoroscopy with the ankle locked in a neutral position as in these patients, we delay complete weightbearing for up to 6 weeks. Regardless of the syndesmotic stress result, all patients had syndesmotic fixation using only manual reduction with 1 or 2 positional screws with the ankle in neutral position, as this particular fibular nail design requires tibiofibular fixation for maintaining reduction and augmenting the stability of the construct. The use of 1 or 2 positional screws was decided according to the intraoperative assessment of bone density, preferring the use of 2 screws in patients with osteopenia or osteoporosis. After syndesmotic reduction, a comparative talar tilt test was performed to assess for deltoid instability. In cases with widening or persistent opening of the medial clear space, a deltoid ligament direct repair was performed using 1 or two 3.5-mm anchors.
Imaging Technique and Evaluation
Immediate postoperative bilateral ankle computed tomography (CT) was obtained in all cases within the first 48 hours after surgery. Images were acquired on a Siemens Definition Dual Energy, Double tube (Siemens Medical, Malvern, PA), 128-channel equipment with minimum slices of 0.6 mm with both ankles in 90 degrees neutral dorsiflexion.
Fibular rotation, diastasis, translation, and length were measured in a radiology workstation, using Phillips VUE PACS Software version 12.1.5 (Philips Medical System, Bothell, WA). Two independent musculoskeletal radiologists and 1 fellowship-trained foot and ankle surgeon performed all radiologic measurements on both ankles. These were made at the widest part of the tibial plafond, 1 cm proximal to the joint line in the axial cuts and at the level of the maximum length of the fibula in the coronal view (Figure 2).

Postoperative bilateral computed tomographic scan imaging. (A) Coronal views. (B) Axial views. A slight anterior translation and overcompression is noted.
The parameters were measured using the postoperative distal tibiofibular reduction protocol described by Prior and colleagues. 29 The method consists of a primary line A that unites the middle point of 2 lines crossing the longest diameter both on the tibia and the fibula in the axial cut (Figure 3A). Tibiofibular diastasis was measured along with line A between the medial cortex of the tibia and the lateral cortex of the fibula (Figure 3B).

Diastasis and anteroposterior translation measurements. (A) Line A unites the middle point of the 2 lines crossing the longest diameter both on the tibia and the fibula. (B) Tibiofibular diastasis was measured along with line A between the medial cortex of the tibia and the lateral cortex of the fibula. (C) Line B is drawn parallel to line A along with the most anterior point of the tibial cortex. Line C is drawn along the most lateral point of the anterior and posterior colliculi of the tibia. Anteroposterior translation (APT) corresponds to the distance between the most anterior aspect of the fibula and line B, parallel to line C. Redrawn from Prior CP, Widnall JC, Rehman AK, Weller DM, Wood EV. A simplified, validated protocol for measuring fibular reduction on ankle CT. Foot Ankle Surg. 2017;23(1):53-56.
A second line (line B) is drawn parallel to line A along with the most anterior point of the tibial cortex. Next, line C is drawn along the most lateral point of the anterior and posterior colliculi of the tibia. Anteroposterior translation (APT) corresponds to the distance between the most anterior aspect of the fibula and line B, parallel to line C (Figure 3C).
Fibular length was measured in the coronal cut using a line drawn following the anatomical axis of the fibula (line D) and a second line perpendicular to line D at the level of the most lateral region of the tibial plafond (line E). Fibular length corresponds to the distance between the tip of the fibula and line E (Figure 4A).

Fibular length and rotation measurements. (A) Line D is drawn following the anatomical axis of the fibula and a second line perpendicular to line D at the level of the most lateral region of the tibial plafond (line E). Fibular length corresponds to the distance between the tip of the fibula and line E. (B) Fibular rotation was determined using the angle conformed by the line that unites the anterolateral and posterolateral distal tibia tuberosities and the line that unites the anterior and posterior fibular tuberosities. Redrawn from Prior CP, Widnall JC, Rehman AK, Weller DM, Wood EV. A simplified, validated protocol for measuring fibular reduction on ankle CT. Foot Ankle Surg. 2017;23(1):53-56.
Fibular rotation was determined relative to the tibial incisura using the angle conformed by the line that unites the anterolateral and posterolateral distal tibia tuberosities and the line that unites the anterior and posterior fibular tuberosities as described by Dikos et al (Figure 4B). 13
Statistical Analysis
Patient characteristics were summarized with frequencies and percentages for categorical variables and mean with SD for continuous variables. Shapiro Wilks test was used to assess normality in continuous variables distribution. The primary outcome measures (rotation, diastasis, translation, and fibular length) were analyzed with paired t-test samples to assess group differences between the injured and uninjured ankles. Statistical significance was set for P value <.5. SPSS 24.0 (SPSS Inc, IBM, Chicago, IL) was used for statistical analysis.
Sample size calculation was conducted with an estimated moderate effect size of 0.5, for fibular translation as the main variable for the primary outcome (matched pairs t test for group differences assessment), indicating that 27 subjects would be needed to achieve 80% power with an α level of 0.05 through G*power software (latest version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany).
Intraclass correlation coefficient (ICC) was used to assess observers’ level of agreement (2-way mixed effects, absolute agreement, multiple raters).20,32 Poor correlation was considered with coefficients <0.5; moderate in the range of 0.5 to 0.75, good between 0.75 and 0.9, and excellent for values >0.9.
Results
Twenty-eight patients (16 women) were included in this study with a mean age of 46 years (range: 16-91). Demographic data, patient characteristics, and fracture classification are summarized in Table 1.
Patient and Fracture Characteristics.

Abbreviations: AO, Arbeitsgemeinschaft für Osteosynthesefragen; OTA, Orthopaedic Trauma Association; PABD, pronation-abduction; PER, pronation-eversion (external rotation); SAAD, supination-adduction; SER, supination-eversion (external rotation).
The mean fibular rotation in the injured and noninjured ankle was 9.7 (SD 4.9) and 10.1 (SD 3.6) degrees respectively, this difference not being statistically significant (P = .661). Regarding syndesmotic diastasis, the mean values were 2.5 mm (SD 1.0) on the injured side and 2.3 mm (SD 0.9) on the uninjured side (P = .147). The mean postoperative fibular length in the fractured ankle was 24.6 mm (SD 3.0) and 25.4 mm (SD 3.3) in the uninjured ankle (P = .115). On the other hand, there was a significant difference (P = . 01) in the postoperative fibular anteroposterior translation between the injured and uninjured ankle, being 9.6 (SD 1.4) and 10.3 (SD 1.3) mm, respectively. CT scan measurements are summarized in Table 2.
Comparison of Anatomical Parameters in the Injured and Uninjured Ankles. a
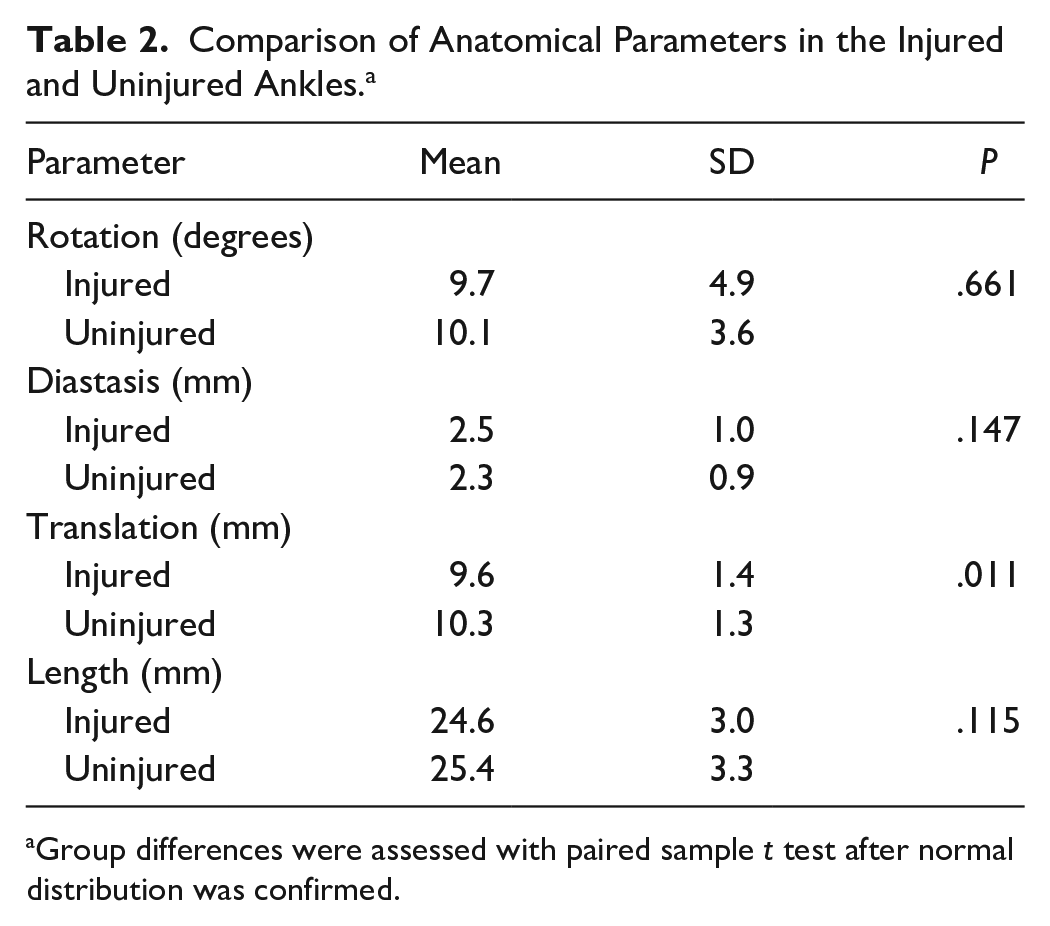
Group differences were assessed with paired sample t test after normal distribution was confirmed.
The ICC analysis showed adequate concordance between the 3 observers except for fibular translation in the injured ankle (ICC 0.623), which was considered to have only moderate concordance in the Poor-Good agreement level range (Table 3).
Interobserver Correlation.

Abbreviation: ICC, intraclass correlation coefficient.
Discussion
Malreduction of both the fibula and the distal tibiofibular syndesmosis after surgical management of ankle fractures has been recognized as a factor of poor prognosis and premature articular degeneration.30,35,37,40 Therefore, assessment of the restoration of anatomical parameters by means of plain radiography and CT scan evaluation has been widely studied but mostly on patients treated with plate osteosynthesis.1,11,19,25 Limitations of both standard fluoroscopy and radiographs in detecting malreduction of the syndesmosis have made CT scanning the standard for postoperative evaluation of fibular malreduction.22,24,29 Furthermore, based on the potential morphologic variations among different individuals, current recommendations establish the use of bilateral CT scans to avoid relying only on quantitative measures and parameters.13,25 To our knowledge, this is the first study to assess the restoration of the anatomical parameters of the fibula and syndesmosis after intramedullary nailing using bilateral CT scanning.
Our results suggest an anatomical restoration of fibular and syndesmotic parameters of the fractured ankle regarding rotation, diastasis and length compared to the uninjured ankle. Nevertheless, we found significant differences when comparing fibular anteroposterior translation between both ankles. We hypothesize 2 potential explanations for this difference. First, and as previously stated, the moderate agreement between our observers regarding the measurement of translation in the injured ankle cannot be ruled out as a feasible explanation, particularly in cases of trimalleolar fractures. Secondly, the device used in all patients relies on the use of 1 or 2 syndesmotic screws for maintaining proximal fixation even in patients without syndesmotic injury as it lacks a proximal blocking system. These design concerns can have a role as syndesmotic malreduction, induced by screw mispositioning, has been reported in fractures treated with plating and rigid fixation of the syndesmosis in up to 52% using CT scan evaluation. 15 Furthermore, Sagi and colleagues reported a malreduction rate of 39.7% in 68 patients treated with rigid fixation for syndesmotic injuries using postoperative bilateral CT scan evaluation. 30 The most common cause of malreduction in their study was widening secondary to lateralization and translation in the anteroposterior plane.
We included only previously validated measurements with adequate interobserver and intraobserver reliability for fibular rotation, diastasis, anteroposterior translation, and length.22,29 Evaluation of concordance between the 3 observers in this study was catalogued between good and excellent for all measurements except for the anteroposterior translation of the injured ankle, which was defined only as moderate (ICC = 0.623). This result contradicts the interobserver agreement reported by the authors describing this method in normal CT scans (ICC = 0.958) and for the same observers in this study for the uninjured ankle (ICC = 0.838). 29 Our explanation is that the determination of line C, which connects the most lateral parts of the anterior and posterior tibial colliculi, could be influenced by residual displacement or rotation of a posterolateral fragment in trimalleolar fractures, thus determining a variable and unreliable anteroposterior translation measurement. This limitation has been previously reported, and considering the fact that trimalleolar fractures represented 23% of our study population, it cannot be ruled out as the cause of poor agreement. 29
New designs of intramedullary implants include improvements in relation to proximal fixation, such as retractable talons or proximal blocking screws.5,6 These implants could reduce the use of rigid fixation in fractures without syndesmotic injury, therefore reducing the probability of anteroposterior malreduction. Furthermore, even in the presence of syndesmotic disruption, some fourth-generation implants allow the use of flexible syndesmotic fixation devices. Flexible fixation has been reported to have a lower syndesmotic malreduction rate when used with traditional plating.21,31 Future studies should focus on comparing the influence of these innovations on fibular and syndesmotic reduction.
Potential limitations of our study include the lack of a control group to evaluate the restoration of fibular and syndesmotic parameters in patients treated with traditional plates. However, these patients are expected to regain fibula length and rotation as a result of anatomic reduction using open approaches and direct visualization of the fracture site.
This protocol did not include weightbearing CT imaging as our evaluation was performed in the immediate postoperative period when the patient usually cannot fully weightbear. Consequently, it is unknown if the obtained reduction parameters are maintained under physiological loads. Even though secondary loss of reduction or loosening could occur when loading is initiated, this could be related to patient compliance or poor bone quality and have no relation to the ability of the nail to restore anatomical parameters intraoperatively.
Anatomical asymmetry in the same patient was not considered in our study design but could potentially limit the clinical application of our results. A recent study by Kubik et al 22 compared 213 bilateral lower limb CT scans of uninjured ankles, concluding that 35% of uninjured syndesmosis would be classified as malreduced by current diagnostic standards. Nonetheless, the CT scans belonged to patients studied for femoracetabular impingement and they were obtained with variable degrees of plantar flexion of the ankle, which has been related to variability in distal tibiofibular relationships. 30 On the contrary, Patel and colleagues reported no differences between uninjured left and right ankles after performing bilateral weightbearing CT imaging in 100 patients, limiting the variability associated with the degree of ankle plantar flexion. 27
Conclusion
According to our results, the use of intramedullary nailing for the management of distal fibular fractures restores the anatomical parameters of the fibula and tibiofibular relationship in terms of rotation, diastasis, and fibular length compared to the uninjured ankle. Nonetheless, postoperative fibular anteroposterior translation had significant differences in comparison to the contralateral ankle. This may be the result of the use of rigid fixation of the syndesmosis that is inherent to the nail design or a limitation of the CT evaluation method previously described for the assessment of syndesmotic malreduction in the anteroposterior axis.
Further long-term comparative studies are needed to determine if the restoration of anatomical parameters, obtained with the fibular nail in this study, diminishes the incidence of posttraumatic osteoarthritis similarly to open reduction and conventional plating. New intramedullary nail designs allowing the use of flexible syndesmotic fixation may improve tibiofibular malreduction related to the rigid fixation used in our group of patients.
Footnotes
Ethical Approval
Ethical approval for this study was waived by Comite de Etica de Investigacion Clinica las Condes (date 7/21/2020, ID034723).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.