
Abstract

Introduction
Fracture nonunions are a complex and challenging problem accounting for significant patient morbidity and financial cost.1,2,6 -8 There is a paucity of data regarding treatment of lesser toe intra-articular proximal phalanx fractures of the metatarsophalangeal joint (MTPJ).4,5 We present a case, surgical technique, and patient-reported outcome measures (PROMs) concerning a lesser toe intra-articular proximal phalanx fracture nonunion of the MTPJ.
Case Report
A 61-year-old woman presented as a second opinion for a second toe injury 3 months following an acute trauma. The mechanism of injury was described as a rotating force while pivoting on a standing plantarflexed foot. She was treated nonoperatively in a boot for 3 months without improvement and complained of impaired ambulation and activities of daily living. Radiographs demonstrated a displaced intra-articular proximal phalanx fracture of the second toe with incomplete radiographic healing and minimal callus formation (Figure 1). On physical examination, the patient exhibited an antalgic gait, second MTPJ tenderness to palpation, and pain with weightbearing and varus stressing of the joint. No plantar plate instability was noted on Lachman examination. Her lower extremities were well perfused with intact pedal pulses, warm toes, and brisk capillary refill.

Anteroposterior (AP) plain radiographs of the foot at 3½ months following initial injury demonstrating minimal healing of the second toe proximal phalanx fracture with intra-articular extension.
Medical history was significant for peripheral vascular disease successfully treated with aorta-bifemoral bypass grafting. Potential contributing comorbidities included a 20-pack-year smoking history with 7 years nicotine cessation and a nonfunctional kidney (creatinine ratio 1.1). No history of nonsteroidal anti-inflammatory use, endocrine abnormalities, or immunosuppression. Laboratory results were negative for infectious and metabolic abnormalities. A vascular surgery evaluation revealed normal ankle brachial index ultrasonography and no concern for vascular insufficiency. Computed tomography (CT) confirmed an intra-articular nonunion affecting approximately 30% of the plantarmedial joint surface (Figure 2).

Preoperative coronal and axial computed tomographic scan images demonstrating a second toe proximal phalanx intra-articular nonunion affecting approximately 30% of the plantarmedial joint surface.
With continued symptoms, lack of biologic nonunion etiology, and no fracture healing progression by 6 months, the patient elected to pursue surgery. Surgical technique referenced described treatment of hand intra-articular proximal phalanx fracture nonunions. 6 Under general anesthesia, the extremity was prepped and draped in sterile fashion, and a nonsterile thigh tourniquet was applied. A longitudinal incision was centered dorsally over the second MTPJ. The interval between the short and long extensor tendons was used with sharp dissection and capsulotomy of the second MTPJ. Full-thickness periosteal flaps were elevated with the capsule, exposing the MTPJ and nonunion fracture site (Figure 3). Homan retractors were inserted medial and lateral, and the toe was plantarflexed to expose the joint surface. The fracture nonunion was grossly unstable with collateral ligament and plantar plate insertions left intact. The fibrous nonunion was retracted with a dental pick and debrided back to viable bone with the use of small curettes. A 0.045 K-wire was used to perforate the bone at the nonunion site. A calcaneal cancellous autograft plug was harvested using a 6.5-mm trephine from a separate incision at the anterior border of the heel. 3 The bone graft was stripped of soft tissue attachments, morselized, and placed at the nonunion site. A pointed reduction clamp and dental pick were used to reduce the nonunion fragment and apply compression. Direct visualization of the joint confirmed appropriate reduction. Two 1.5-mm interfragmentary screws were placed across the nonunion site via a lag by technique method. The nonunion repair and hardware placement was assessed directly and fluoroscopically (Figure 4). The repair site was clinically stressed and showed no instability in varus, valgus, or Lachman. The wounds were copiously irrigated with saline, and the capsular and periosteal flaps were repaired with No. 3-0 Monocryl sutures. The skin was closed with No. 3-0 Monocryl sutures subcutaneously and No. 3-0 nylon sutures through skin in simple fashion. No transarticular pin was placed across the MTPJ as it remained stable following capsular repair.

Exposed second metatarsophalangeal joint after dissection and capsulotomy demonstrating an unstable second proximal phalanx intra-articular nonunion.

Exposed second metatarsophalangeal joint following calcaneal autograft, anatomic reduction, and fixation with two 1.5-mm interfragmentary screws.
The patient was placed into a hard-sole shoe weightbearing through the heel for the first 6 weeks with progression to full weightbearing in a regular shoe by 3 months. Repeat radiographs and CT scans were obtained at 3- and 6-month visits demonstrating anatomic articular alignment and osseous union without hardware complication (Figure 5). Her preoperative pain of 7/10 improved to 2/10 at 3 months and to 0/10 at 6 months. She resumed normal activity without pain by her 6-month follow-up.

Six-month postoperative anteroposterior plain radiograph and coronal/axial computed tomographic images of the foot demonstrating anatomic reduction, complete osseous union, and intact hardware.
Pre- and postoperative (3- and 6-month) PROMs were performed. The Foot and Ankle Disability Index (FADI) showed improved postoperative scores compared with the preoperative (Figure 6). The Foot and Ankle Outcome Score (FAOS) exhibited improvement in all categories and regained range of motion (ROM) at 6 months (Figures 7 and 8). The Patient Reported Outcome Measurement Information System (PROMIS) for physical function improved to normal limits at 6 months postoperatively (Figure 9).

Foot and Ankle Disability Index (FADI) scores preoperative (47.1), 12-week postoperative (74), and 6 month postoperative (96.2).

Foot and Ankle Outcome Score (FAOS) preoperative, 12-week postoperative, and 6-month postoperative demonstrated increased total score (58%, 80%, 96%), return of preoperative motion, improved pain (64%, 81%, 97%), improved function in daily living (59%, 99%, 100%), improved function in sports and recreation (15%, 40%, 80%), and improved quality of life (31%, 56%, 94%), respectively.
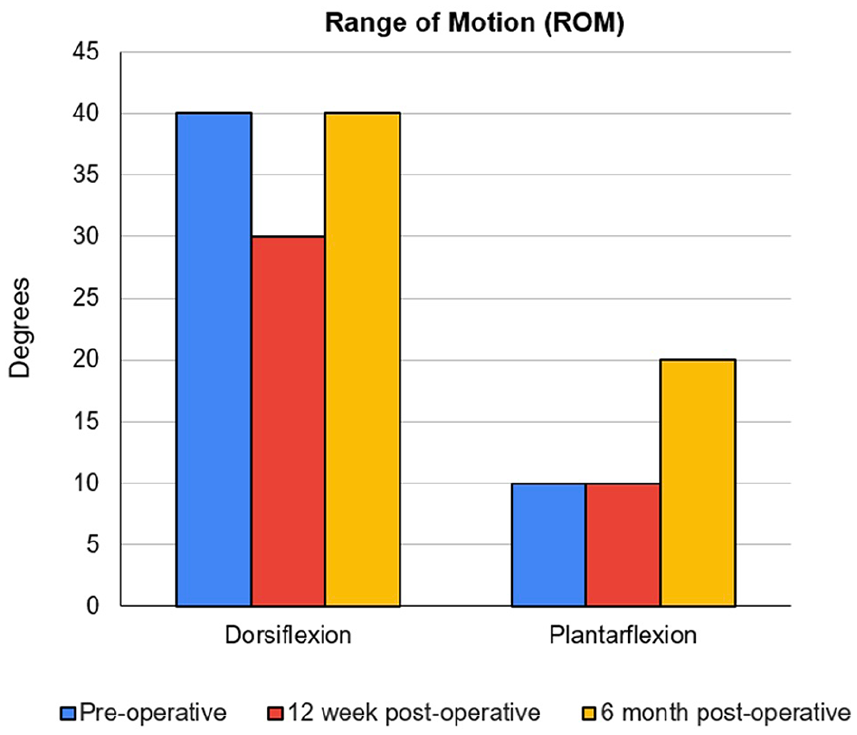
Second metatarsal preoperative, 12-week postoperative, and 6-month postoperative range of motion (ROM).
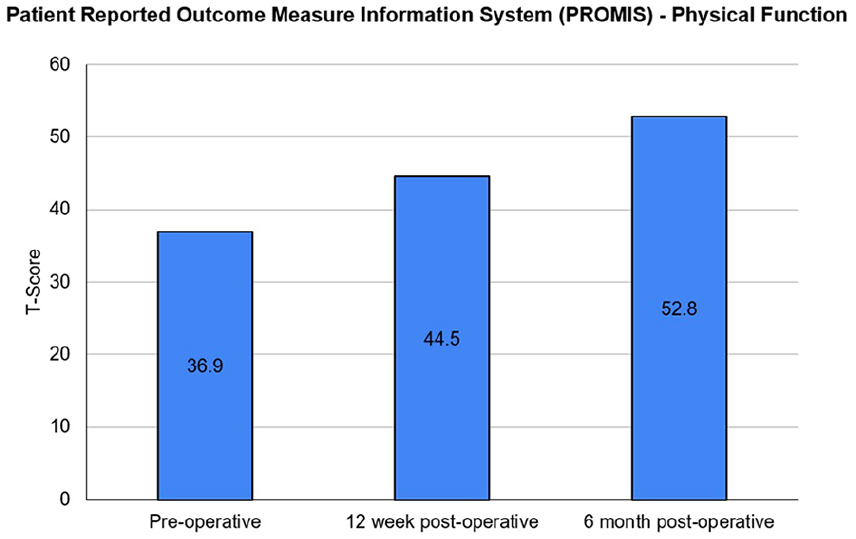
PROMIS scores related to physical function improved from preoperative (36.9), to 12-week postoperative (44.5), to 6-month postoperative (52.8) follow-up. The 6-month postoperative score was within the normal limit threshold (>45).
Discussion
Fracture nonunions are a complex and challenging problem accounting for significant patient morbidity and financial cost.1,2,6 -8 To our knowledge, there are no prior case reports describing evaluation and surgical repair of an intra-articular proximal phalanx fracture of the MTPJ in the foot. Nonunion risk assessment in foot and ankle surgery continues to be of interest with discrepancies on what qualifies as a fracture nonunion. 8 The Food and Drug Administration defines fracture nonunion as failed bone healing 9 months from initial injury without signs of radiographic healing within a 3-month span. 1 Risk factors for nonunion include environmental, injury mechanism and severity, and treatment modalities.1,6 -8 Comprehensive and patient-specific evaluations are necessary to identify risk factors contributing to fracture nonunion. Should nonoperative treatment fail to unite fractures, surgical intervention may be indicated. Intra-articular nonunion can cause severe joint stiffness and arthrosis, making surgical restoration of anatomy imperative. 6 There are variations in surgical technique when treating nonunions; however, autologous bone graft with anatomic reduction to promote primary bone healing remains the criterion standard. 3
Summary/Conclusion
We report a case of an intra-articular fracture nonunion to the second toe proximal phalanx MTPJ that successfully underwent surgical repair. Following treatment and described surgical technique, the patient had improved PROMs and returned to preinjury activities by 6-month follow-up with no pain. Further research is necessary to evaluate intra-articular fractures of the lesser toe proximal phalanx MTPJ, risk factors for nonunion development, and surgical outcomes in the event of nonunion.
Footnotes
Acknowledgements
The work of this project remained internal among the authors; therefore, they have no acknowledgements to make.
Ethical Approval
Ethical approval was not sought out for the present study because written informed consent was obtained from the patient for publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.