
Abstract
Background:
Central talar fractures are rare and often associated with impaired functional outcome. Despite recent advances in diagnosis and management of talus fractures, complications rates remain high and functional outcome is generally poor. This study aims to provide an overview of complication rates and functional outcome following operative treatment of talar neck and body fractures. This may help in clinical decision making by improving patients’ expectation management and tailored treatment strategies.
Methods:
A systematic review of the literature was conducted of studies published from January 2000 to July 2021 reporting functional outcome and/or complications following operative treatment of talar neck, body, or combined neck and body fractures. Keywords used were (Talar fracture) or (Talus fracture). Data on complication rates and functional outcome was extracted from selected articles.
Results:
A total of 28 articles were included in our analysis reporting 1086 operative treated talar fractures (755 neck [70%], 227 body fractures [21%], and 104 combined body and neck fractures [9%]). The mean follow-up was 48 (range 4-192) months. Complications occurred frequently with; 6% surgical site infection, 8% nonunion, 29% avascular necrosis, 64% osteoarthritis, and in 16% a secondary arthrodesis was necessary. A wide variety in functional outcome was reported; however, there seems to be a correlation between fracture classification and postoperative complications.
Conclusion:
Operative treatment of central talar fractures is associated with a high incidence of early and late complications and often leads to an impaired functional outcome. Standardization of talar fracture classification and scoring systems in combination with large sample-sized prospective studies are warranted to detect further predictive factors influencing tailormade treatment strategies and patient expectation management.
Level of Evidence:
Level III, Systematic review of case series and case-control studies.
Introduction
Talar fractures are rare and often associated with prolonged morbidity. The incidence has increased over the last decades, currently accounting for approximately 0.3% to 2% of all fractures.2,10,36 Despite recent advances in diagnosis and management of talus fractures, complication rates remain high, and functional outcome is generally poor. 32 The latter is often due to the complex articular nature of the talus and impaired blood supply following injury.16,35
The talus is divided into 3 anatomic regions: the talar head, neck, and body. 30 About two-thirds of the talus is covered with cartilage, leaving only the area around the talar neck and the posterior aspect of the body for periosteal blood supply. The talar body articulates with the calcaneus on the caudal site. The medial and lateral surfaces of the body articulate with the medial malleolus (of the tibia) and lateral malleolus (of the fibula), respectively. The cranial side of the talar body articulates with the distal tibia. Between the head and the body is the neck of the talus, without an articular surface or cartilage.
The blood supply of the talus arises from extra- and intraosseous sources. The main branches that supply blood for the talus are the tarsal canal (a branch of the posterior tibial artery) and the sinus tarsi artery (branch of the perforating peroneal artery). The tarsal canal artery supplies most of the talar body, whereas the talar neck is mainly supplied by the sinus tarsi artery. Extensive intraosseous anastomoses are present throughout the talus and are responsible for the survival of the talus in severe injuries. Initial fracture displacement, the timing of reduction, and soft tissue damage are factors that can potentially affect the integrity of the talar blood supply. 27
Differentiating between talar neck or body fractures can be challenging. Inokuchi et al 18 described the anatomical border, where fractures can be more clearly distinguished on the inferior surface of the talus than on the superior surface. Hereto, fractures that pass from the medial entrance through the lateral entrance of the tarsal sinus on the inferior surface should be diagnosed as neck fractures, and fractures that pass through the lateral border of the posterior subtalar joint should be diagnosed as body fractures.
Different classifications for the talar neck fracture have been introduced. The Hawkins classification is used most frequently. In 1970, Hawkins 17 classified talar neck fractures into 3 types. In 1978, Canale and Kelly 9 modified this classification by adding a fourth type. Modified Hawkins type I fractures are nondisplaced, with preservation of the talar neck vasculature. Type II fractures are displaced with associated subluxation or dislocation of the subtalar joint, whereas the tibiotalar and talonavicular joints remain in proper alignment. Vallier et al 42 shed new light on the Hawkins type II fractures, separating Hawkins type II fractures into those without (type IIA) and those with (type IIB) subtalar dislocation. This could help to predict the development of avascular necrosis (AVN). Type III fractures have displacement with subluxation or dislocation of the subtalar and tibiotalar joints and are characterized by a normal alignment of the talonavicular joint; however, this pattern of malalignment may be associated with injury to the posterior tibial neurovascular bundle. Type IV fractures demonstrate dislocation or subluxation of the subtalar, tibiotalar, and talonavicular joints and thereby the most severe type. Talar body and neck fractures can be classified by use of the Marti-Weber classification. Type I fractures are classified as distal talar neck and talar head fractures with osteochondral flakes. Type II fractures are nondisplaced talar neck and body fractures, type III fractures are displaced fractures of the talar neck and body, and type IV fractures are characterized by proximal talar neck fractures with corpus tali dislocated out of the intermalleolar space or comminuted fractures. 25 Sneppen et al 37 classified talar body fractures into 6 types: type A compression fracture, type B coronal shearing fracture, type C sagittal shearing fracture, type D fracture of the posterior process, type E fracture of the lateral process, and type F crush fracture.
Currently, the appropriate approach and fixation methods for talar neck and/or body fractures are still under constant discussion. 16 Hence, there is a growing understanding that displaced fractures of the talus neck and/or body should be managed by open anatomic reduction and stable fixation, thereby minimizing the risk of complications and poor functional outcomes, 30 whereas nonsurgical treatment should only be reserved for nondisplaced fractures.
This study aims to provide a systematic review of the literature on complication rates and functional outcome following operative treatment of talar neck and body fractures. This may help in clinical decision making by improving patients’ expectation management and tailored treatment strategies.
Methods
A systematic review of the literature was performed of the following databases using the OVID search engine: MEDLINE, EMBASE, and CENTRAL databases (2000–July 2021). Because of the recent advances in therapeutic strategies of talar fractures, we chose to compare the results of the last 20 years. The initial review was performed in March 2021 and was updated in July 2021. The search strategy for each database is outlined in Figure 1.

PRISM flowchart diagram of included articles.
Inclusion criteria for selecting articles to be included in the review:
Studies involving fractures of the talar neck and/or body in adult (>17-year-old) patients
Studies published between 2000 and 2021
Exclusion criteria included the following:
Studies that included <10 patients
Non–English-language studies
Inability to isolate results
Mean follow-up of <3 months
When the full article was not provided
Two authors performed the systematic review independently (Posthuma and Wijers). Results from all databases were combined, and duplicate titles were removed. Two reviewers assessed the articles at each stage of the filtering process (titles, abstracts, and full-length manuscripts). At all but the final stage, disagreement led to inclusion. At the final stage of selection, disagreement was resolved by consulting a third independent reviewer (Schepers) to provide consensus on the inclusion. After full-length articles to be included were selected, 2 authors performed data extraction using a data extraction form (Posthuma and Wijers).
Variables
The year of publication, type of study, number of patients, gender, age, mechanism of injury, type of fracture (anatomy), treatment, postoperative protocol, primary outcome, complications, and duration of follow-up was noted for systematic analysis of the available evidence.
Complications
Complications were defined as surgical site infection (SSI), nonunion, osteoarthritis, AVN, secondary arthrodesis, or other surgical intervention, as described by the authors of the studied publications.
Functional Outcomes
Several validated functional outcome scores were used such as the Foot Function Index (FFI), the American Orthopaedic Foot & Ankle Society Hindfoot score (AOFAS), the Weber functional outcome score, and the musculoskeletal function assessment (MFA).
The FFI consists of 23 items grouped into 3 subscales: pain, disability, and activity limitations. 8 The American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score is a functional outcome score out of 100 points in domains such as pain (45 points), function (40), and alignment (15 points). Based on the total score, patients were divided in groups according to the literature: a score of 90 to 100 was graded as an excellent result, 75 to 89 as good, 50 to 74 as fair, and less than 49 points was graded as a failure or poor outcome. 20 The Weber functional outcome score is based on the evaluation of 4 categories: pain, gait, activity, and radiographic findings. In all subgroups, 0 is a perfect result and 4 is defined as poor. The latter defines a score of 0-3 as excellent, 4-7 good, 8-12 fair, and 13-16 as poor. The musculoskeletal function assessment (MFA) score is a health status instrument with 100 self-reported health items, with the best score of 0. 12 The Hawkins score consists of 3 parts: pain, the presence of a limp, and range of motion of the ankle. 17
Results
After final selection, 28 full-length articles were included (Figure 1). Most studies were retrospective case series (86%), whereas only 1 prospective study was selected. 3
A total of 755 talar neck, 227 talar body, and 104 combined talar neck and body fractures were reviewed. In the included studies, predominantly male patients were identified. The mean follow-up was 48 months (range 4-192). Further baseline characteristics of selected studies are presented in Table 1.1,3-7,11,13-15,19,23,24,28,29,31,33,34,38-42,43,45 -47
Baseline Characteristics of Operative Treatment of Talar Neck and/or Body Fractures

Abbreviations: CC, case control study; CS, case series; PS, prospective study; NR, not registered; RS, retrospective study.
Complications
Postoperative complications were divided into early and late complications. Postoperative SSI within 90 days was found in 6% (61/944). Late complications included nonunion in 8% (48/636), AVN in 29% (279/966), secondary arthrodesis in 16% (124/800), and osteoarthritis in 64% (514/804). More detailed information is presented in Tables 2 and 3.
Early and Late Complications After Operative Treatment of Talar Neck and/or Body Fractures Sorted by Study.

Abbreviations: AVN, avascular necrosis; NR, not registered; SSI, surgical site infection.
Early and late complications after operative treatment of talar neck and/or body fractures sorted by fracture location.

Abbreviations: AVN, avascular necrosis; SSI, surgical site infections.
Functional Outcome
Different functional outcome scores were used in the reviewed articles. The most frequently used outcome score was the AOFAS score in 15 of 21 articles (71%). In addition, other functional outcome scores were used, such as FFI, 4 of 21 (19%); MFA, 2 of 21 (10%); Hawkins, 2 of 21 (10%); and Weber, 1 of 21 (5%). More detailed information is presented in Table 4.
Functional Outcomes After Operative Treatment of Talar Neck and/or Body Fractures.
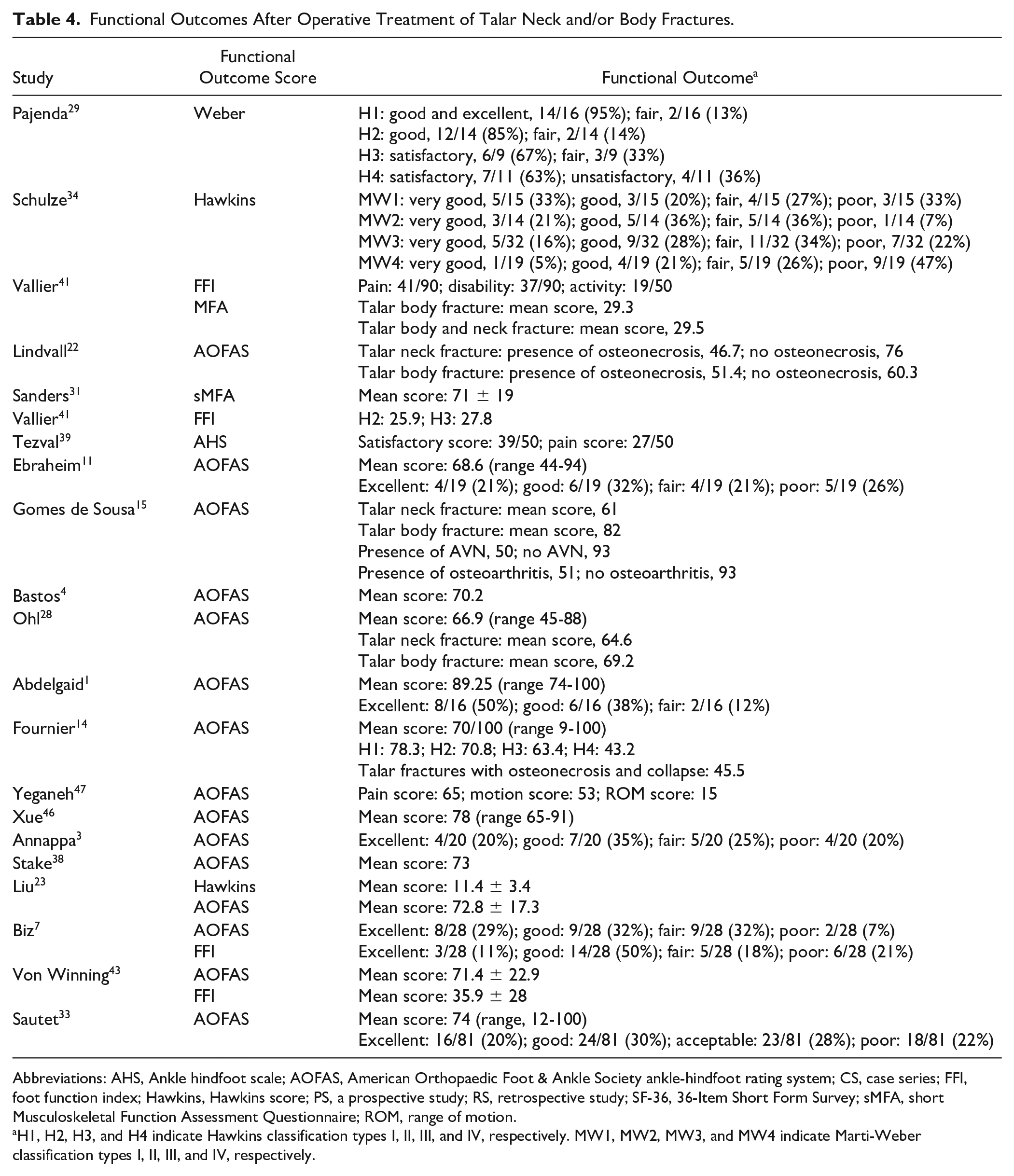
Abbreviations: AHS, Ankle hindfoot scale; AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot rating system; CS, case series; FFI, foot function index; Hawkins, Hawkins score; PS, a prospective study; RS, retrospective study; SF-36, 36-Item Short Form Survey; sMFA, short Musculoskeletal Function Assessment Questionnaire; ROM, range of motion.
H1, H2, H3, and H4 indicate Hawkins classification types I, II, III, and IV, respectively. MW1, MW2, MW3, and MW4 indicate Marti-Weber classification types I, II, III, and IV, respectively.
Discussion
Operative treatment of central talar fractures is associated with a high incidence of early and late complications and often leads to an impaired functional outcome. Almost all articles were of low evidence (Level IV). Given the low incidence of this type of fracture, large volume prospective studies are hard to conduct. One prospective study was identified by Annappa et al 3 describing 20 operatively treated talar neck fractures that were prospectively followed up. Overall, results of articles were challenging to compare, given the heterogeneity of articles, especially given the various classification and functional outcome scores.
Subgroup Incidence
In our evaluation, 755 neck (70%), 227 body (21%), and 104 combined body and neck fractures (9%) were included, suggesting that the talar neck is more prone to traumatic injury than the body. A possible explanation for this is that the short and broad talar neck has a relatively weak cortex. 21 Another explanation can be found in the trauma mechanism. Fractures of the talar neck occur with forced dorsiflexion of the ankle in the setting of a high-energy axial load. The dense cortical bone of the anterior tibia is driven inferiorly and encounters the less-dense bone of the talar neck. 44
Classification
Our study shows that the Hawkins classification for talar neck fractures and Marti-Weber for body and neck fractures are the most commonly used classification. These classifications are widely accepted and should be used as a standard to improve the comparability of future studies.
Complications and Functional Outcome
Complication rates were high, ranging between 6% SSI up to 64% osteoarthritis, following operative treatment of talar fractures. AVN occurred more often in cases of a combined neck-body fracture, than in cases of isolated body or neck fractures. 14 As expected, there seems to be a trend of increased complication rates with a longer follow-up period. Fournier et al 14 described an AVN rate of 34% following operative treatment of 114 talar neck and body fractures after a follow-up of 111 months, whereas only 7% AVN was observed in 81 talar neck and body fractures after 12 months by others. 33 In addition, up to 75% osteoarthritis after 111 months as observed by Fournier et al, 14 compared to 29% after a follow-up of 16 months as described by Bellamy et al. 5 Therefore, in patients suffering from a talar fracture, long and intensive follow-up is warranted for timely recognition of early and late complications. Especially given the correlation between the presence of complications and impaired functional outcome.14,15,22 Lindvall et al 22 described an AOFAS score of 76 after operative treatment of talar neck fractures in the absence of AVN, whereas patients suffering from AVN reported a lower functional outcome score of 46.7. The same trend (but less pronounced) was seen in the talar body fractures (AOFAS score in absence of AVN 60.3 and presence of AVN 51.4). 38 The latter was also observed concerning AVN, where the AOFAS score on talar neck and/or body fractures was 93 in patients without AVN and functional outcome score was 50 in patients with AVN. 15 One explanation might be that postoperative follow-up differs considerably between studies, varying from standardized CT scans to articles in which follow-up imaging was not described. To compare studies in the future, we advocate for standardization of talar fracture follow-up with targeted imaging and functional outcomes scores, to improve the comparability of future studies. Given that the AOFAS score is the most commonly used, we consider this as the most appropriate score for future evaluation. In addition, specific gradings systems are available to rate the severity of subtalar arthritis, such as the Kellgren and Lawrence grading scale and the Paley gradings system. 26
Preoperative Classification and Postoperative Functional Outcome
Several studies revealed that poor outcome was correlated with fracture severity.11,14,29,33,41 Evaluating functional outcome in relation to the fracture classification, we observed a trend toward an impaired functional outcome in Hawkins type III and IV and MW type III and IV. Pajenda et al 29 described good and excellent results in 95% and 85% of the operatively treated Hawkins type I and II fractures, respectively. Only 67% and 63% of the patients having Hawkins III and IV fractures had satisfactory functional outcome scores. None of the patients scored an excellent or good outcome. In addition to this, 53% of the MW I and 57% of MW II fractures led to very good or good functional outcomes, which was only found in 44% and 26% of the MW III and IV fractures. 34 A possible explanation might be that a higher classification is most likely due to higher-energy trauma, which in turn is often associated with severe soft tissue and cartilage damage.
Anatomic reduction is a strong predictive factor for postoperative function. 33 Studies showed that poor reduction was associated with impaired functional outcome. 22 Given that comminuted and dislocated fractures might be a challenge to reduce toward an anatomic reduction, one may assume that more severe-type talar fractures are associated with impaired functional outcome. Another explanation might be that late complications rise on the severity of the fracture. For instance, in Hawkins type III fractures, all 3 major arterial sources to the talus are commonly injured, resulting in a high risk of AVN. Type IV fractures demonstrate dislocation or subluxation of the subtalar, tibiotalar, and talonavicular joints. In addition to the vascular disruption seen in type III injuries, disruption of blood supply to the head and neck fragments may be seen with this injury as well.
Talar Body vs Talar Neck vs Combined Talar Neck and Body Fractures
There were very few articles comparing differences in functional outcome between groups of talar neck, talar body, and combined talar neck and body fractures. In the studies we evaluated, there was no clear difference in functional outcome when comparing talar body, neck, and combined body and neck fractures. Vallier et al 41 described an MFA score after operative treatment of talar body fractures of 29.3 points and talar body and neck fractures of 29.5 points. The mean standardized MFA score for all patients in this series was 29.4, which was significantly higher than the reported mean reference value for patients with hindfoot injuries of 22.1 (P < .001). When comparing talar neck and talar body fractures, articles published conflicting results. Studies are hard to compare given lacking data and a variety of scoring systems for functional outcomes. Therefore, it remains unknown if talar neck, talar body, or combined talar neck and body are related to different functional outcomes. Comparable functional outcome after operative treatment of talar neck and talar body fractures was described by Ohl et al 28 (talar neck fractures: AOFAS score 64.6 vs talar body fractures: AOFAS score 69.2). Lindvall et al 22 showed that AOFAS scores upon talar neck fractures were better when compared to talar body fractures (talar neck: 76 vs talar body: 60.1). Interestingly, the opposite was found by Gomes de Sousa et al 15 describing an AOFAS score for talar neck fractures of 61 and after talar body fractures of 82.
The authors believe that functional outcomes are more dependent on the preoperative classification (eg, amount of dislocation and comminution) than the exact location of the fracture. In addition, the presence of postoperative complications (eg, AVN or osteoarthritis) seems to be a strong predictor, as described earlier. Furthermore, we focused only on talar fractures and did not describe concomitant injuries. Talar fractures are frequently caused by high-velocity trauma, so associated injuries are expected and can affect the different functional outcome.
Conclusion
Operative treatment of central talar fractures is associated with a high incidence of early and late complications and often leads to an impaired functional outcome. Large sample-sized prospective studies are warranted to detect further predictive factors influencing the currently unsatisfactory clinical outcome of patients. Standardization of talar fracture classification and scoring systems would improve the comparability of future studies. the AOFAS score is the most commonly used functional outcome score and should be considered to use in future studies, to make the comparison between studies possible. Nevertheless, there seems to be a trend toward a more impaired functional outcome and increased postoperative complications with increased severity of talar fractures. In addition, our studies showed an overview of commonly reported complications on operative treatment of talar body and/or neck fractures, which makes tailormade treatment strategies and patient expectation management more accurate.
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because the systematic review consists of published papers that contained data sets with patients who were properly anonymized.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.