
Abstract

Introduction
The normal anatomic lateral ankle consists of the peroneus brevis, which originates from the distal fibula and intermuscular septum, and the peroneus longus, which originates from the proximal two-thirds of the lateral fibula, the intermuscular septum, and at times the lateral condyle of the tibia. 2 These tendons are both enclosed in a single synovial sheath that begins 4 cm proximal to and ends 1 cm distal to the tip of the lateral malleolus. Once the tendons are distal to the retromalleolar groove, they separate and become enclosed in their own synovial sheaths. 2 This case report describes an anatomical variant of the lateral ankle that may be a rare cause of pain that has not been previously described. The patient was treated successfully with surgical release of bilateral accessory peroneus brevis compartments, debridement of a low-lying peroneus brevis muscle belly, and left peroneus quartus excision.
Case Report
The patient is a 17-year-old girl who presented with bilateral foot and ankle pain, left more severe than the right. She had a history of painful bilateral congenital pes planus, which was managed unsuccessfully with years of physical therapy and orthotics. Her past surgical history included bilateral calcaneonavicular coalition excision, left lateral column lengthening, and left Achilles tendon lengthening. Despite these interventions, she complained of debilitating bilateral lateral ankle pain.
On physical examination of the left ankle, she had lateral ankle tenderness. Ankle range of motion was 0 degrees dorsiflexion to 40 degrees plantarflexion with no ankle instability, and subtalar motion was 5 degrees eversion to 25 degrees inversion. Motor examination showed 4/5 strength on eversion and plantarflexion, and the sensory examination was intact in all distributions. She had pain with resisted eversion. Anteroposterior, lateral, and oblique weightbearing radiographs of the left ankle and foot (Figure 1) revealed a narrow joint space at the calcaneonavicular joint without sclerosis or osteophytes. A 3-tesla (T) magnetic resonance imaging (MRI) scan of the left ankle showed a possible split tear of the peroneus brevis tendon and postoperative surgical changes secondary to gastrocnemius lengthening. Because non-operative management was exhausted, she agreed to proceed with surgical management of the peroneal tendons. Intraoperatively, the superior peroneal retinaculum (SPR) was identified and split longitudinally, revealing the peroneus longus tendon. The peroneus brevis muscle was found to be in a separate compartment deep to the longus. This compartment was completely released, decompressing the peroneus brevis. In addition, there was a low-lying muscle belly of the peroneus brevis that was debrided. An aberrant peroneus quartus muscle belly and tendon within the compartment was also present and excised.

Preoperative lateral, anterior-posterior, and oblique weightbearing radiographs of the left foot.
Two weeks postoperatively, the patient had no symptoms and reported she was pain-free for the first time since childhood. She was advanced to weightbearing as tolerated and began physical therapy that encompassed a treatment plan of physical medicine modalities, patient education, range of motion, flexibility, strengthening, and home exercises. At 5 weeks postoperatively, eversion strength increased slightly to 4+/5 and range of motion increased to 5 degrees of dorsiflexion, 45 degrees of plantar flexion, 28 degrees of inversion, and 0 degrees of eversion. At 10 weeks postoperatively, she had completed physical therapy and was asymptomatic.
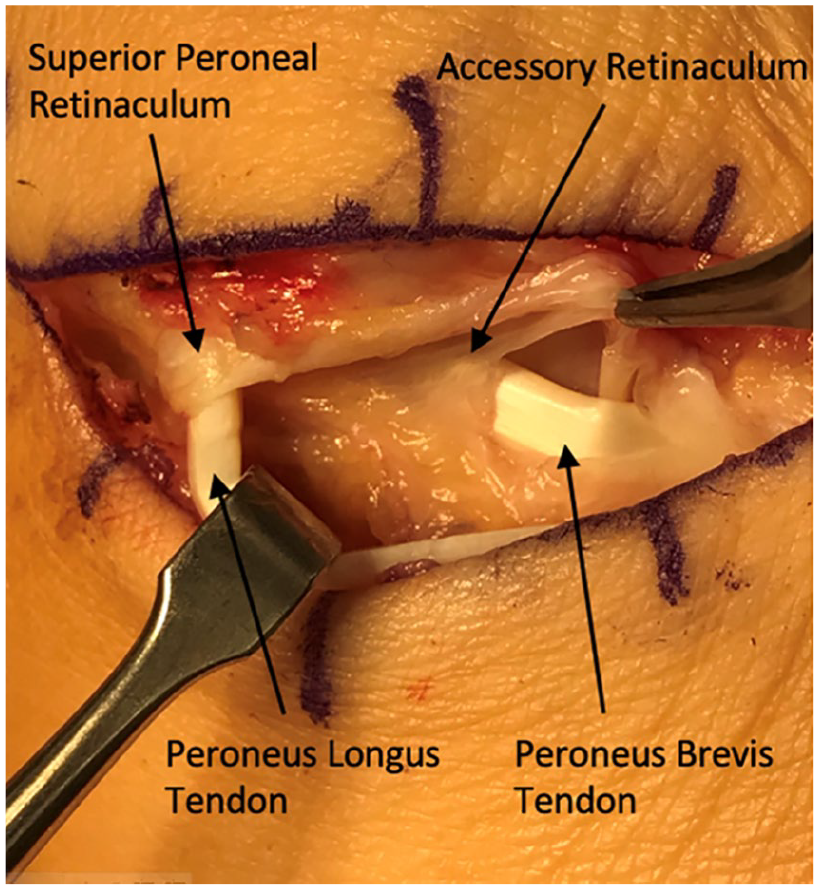
The patient continued to have right lateral ankle pain. On physical examination, she had tenderness along the peroneal tendons, ankle range of motion of 10 degrees dorsiflexion to 40 degrees of plantarflexion, subtalar motion of 5 degrees eversion to 25 degrees inversion, 4+/5 eversion with pain, and 4/5 plantarflexion. Anteroposterior, lateral, and oblique weightbearing radiographs of the right foot and ankle (Figure 2) revealed no significant osseous abnormality. A 3-T MRI of the right ankle revealed no significant abnormalities, as the radiologist was not specifically evaluating for an accessory peroneal compartment. Because non-operative management was ineffective and the patient had responded so well to surgery on the contralateral ankle, the patient elected to proceed with surgical management. The SPR was identified and split longitudinally exposing the peroneus longus tendon (Figure 3). The peroneus brevis tendon was again found to be within an accessory compartment deep to the longus, identical to the contralateral ankle (Figure 4). This accessory sheath was released to decompress the tendon and proliferative synovitis was excised.

Preoperative lateral, anterior-posterior, and oblique weightbearing radiographs of the right foot.

Peroneus longus is shown following release from its compartment and peroneus brevis is shown within its intact accessory compartment. The retinacula of the separate compartments are also demonstrated.
Peroneus longus and now peroneus brevis are visible after opening the accessory compartment that contained peroneus brevis.
Two weeks postoperatively the patient had excellent ankle range of motion with no pain and subsequently began weightbearing as tolerated. She was again started on physical therapy and by 8 weeks was asymptomatic.
Discussion
Lateral ankle pain may sometimes be associated with several anatomic variations. Anatomic variants predisposing or associated with lateral ankle disease include a flat or convex retro malleolar fibular groove, hypertrophy of the peroneal tubercle, accessory peroneus quartus muscle, low-lying peroneus brevis muscle belly, and os peroneum. According to a review by Davda et al, 2 the retromalleolar groove was found to be concave in 82%, flat in 11%, and convex in 7% of cadaveric subjects. A prominent peroneal tubercle was found in 29.1% of cadaveric subjects. The frequency of the peroneus quartus has been reported to be 6.6% to 21.7% according to cadaveric studies. 2 A low-lying peroneus brevis has been appreciated in approximately 33% of individuals. 2 Finally, the os peroneum is predominantly fibrocartilaginous, but is ossified in 20% of individuals. 2
In addition to the separate compartment for the peroneus brevis bilaterally, our patient also had a peroneus quartus and low-lying peroneus brevis muscle belly on the left, and peroneal synovitis on the right, which may have also been a contributor to the patient’s pain.
Interestingly, MRI of the left ankle did not differentiate between a split tear of the peroneus brevis, a peroneus quartus, a separately enclosed peroneus brevis with a low-lying muscle belly and previous surgery of the calcaneonavicular joint. MRI of the right ankle also did not demonstrate the separate peroneal compartments, proliferative synovitis, and previous surgery of the calcaneonavicular joint. A low-lying peroneus brevis muscle belly can be difficult to diagnose on MRI, as distal extension of the peroneus brevis muscle belly changes with foot position. 6 According to Mirmiran et al, 5 the sensitivity of MRI in detecting a low-lying muscle belly is considerably low at 3.23% but has a high specificity of 94.74%. This may be attributed to the radiologist not specifically evaluating for a low-lying peroneus brevis and therefore not positioning the ankle for this indication. When assessing for peroneal tendon pathology, better differentiation of the tendons and synovial sheath content can be appreciated at 20 degrees of plantarflexion. 6 Alternatively, ultrasonography can be used to assess the synovial sheath and peroneal tendons.1,4
Another reason for the patient’s foot and ankle pain is her bilateral pes planus. In a systematic review, Kumar et al 3 found a significant improvement in the American Orthopaedic Foot & Ankle Society ankle-hindfoot score following operative intervention with lateral column lengthening when prolonged nonsurgical management failed to relieve pain and symptoms. However, in this case, the patient’s pain was not resolved following this procedure and was therefore likely attributed to another pathology such as her low-lying muscle belly of the peroneus brevis, peroneus quartus, proliferative synovitis, or accessory peroneus brevis compartment.
Strengths of this case include its uniqueness of the separate compartment for the peroneus brevis, straightforward treatment, and good outcome. A limitation of this case report is that the patient’s pain may have been due to the low-lying muscle belly, the peroneus quartus, or proliferative synovitis rather than from the accessory compartment. However, the anomaly of an additional compartment of the peroneus brevis may have contributed to her lateral ankle pain.
Conclusion
To the authors’ knowledge, this is the first reported case of separate compartments of the peroneus brevis and peroneus longus tendons. This case suggests that in the setting of chronic lateral ankle pain refractory to nonoperative management that includes physical therapy and immobilization, one might consider separate compartments of the peroneus brevis and longus tendons as potential cause of the pain. Furthermore, these sheaths may hide additional pathology responsible for chronic pain. MRI of the ankle may not demonstrate the presence of separate peroneal compartments unless specifically evaluating for the condition. Therefore, persistent symptoms may suggest consideration for surgery.
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because this manuscript is based on a single case. Written informed consent for patient information and images to be published was provided by the patient and her parent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.