
Abstract
Background:
The prevalence, indications, and preferred methods for gastrocnemius recession and tendo-Achilles lengthening—grouped as triceps surae lengthening (TSL) procedures—in foot and ankle trauma are supported by a scarcity of clinical evidence. We hypothesize that injury, practice environment, and training heritage are significantly associated with probability of performing adjunctive TSL in the operative management of foot and ankle trauma.
Methods:
A survey was distributed to members of the American Orthopaedic Foot & Ankle Society and the Orthopaedic Trauma Association. Participants rated how likely they would be to perform TSL at initial management, definitive fixation, and after weightbearing in the presence and absence of a positive Silfverskiöld test in 10 clinical scenarios of closed foot and ankle trauma.
Results:
A total of 258 surgeons with median 14 years’ experience responded. Eighty-five percent reported foot and ankle fellowship training, 24% reported traumatology fellowship training, 13% both, and 4% no fellowship. Ninety-nine percent reported performing TSL with a median 25 TSL procedures per year, 72% open gastrocnemius recession, and 17% percutaneous tendo-Achilles lengthening). Across all scenarios, we observed low overall 8% probability with fair agreement (κ = 0.246) of performing TSL (range, 1% at initial management of an unstable Weber B bimalleolar ankle fracture with negative contralateral Silfverskiöld test to 29% at definitive fixation of tongue-type calcaneus fracture with positive contralateral Silfverskiöld test). Silfverskiöld testing significantly influenced TSL probability at all time points. University of Washington training (β = 1.5, P = .007) but not trauma vs foot fellowship training, years in practice, academic practice, urban setting, or facility trauma designation were significantly associated with likelihood of performing TSL.
Conclusion:
Orthopaedic traumatology and foot and ankle surgeons report similar indications, methods, and low perceived propensity to use TSL in the management of foot and ankle trauma. We found that graduates of 1 fellowship training site were more likely to perform TSL in the setting of acute trauma potentially indicating the need for better scientific data to support this practice.
Level of Evidence:
Level V, therapeutic.
Introduction
Gastrocnemius recession and tendo-Achilles lengthening—herein grouped as triceps surae lengthening (TSL) procedures—are surgical techniques described to improve restricted ankle dorsiflexion.21,23 Limited clinical evidence supports the use of TSL for the treatment of midfoot and forefoot overload syndromes, forefoot ulcers, and Achilles tendinopathy. 9
TSL procedures, and particularly variations of the gastrocnemius recession, are also advocated by some surgeons as adjunctive interventions in the treatment of foot and ankle trauma.4 -6,16,19 Proponents argue that these procedures aid in the restoration of hindfoot and midfoot alignment,16,19 facilitate fracture reduction,4 –6 and improve final range of motion.14,20 However, adjunctive TSL procedures—whether performed at the time of initial fracture temporization, definitive internal fixation, or after return to weightbearing—have not been shown to improve fracture reduction, union rate, reduce pain, reduce the risk of fixation failure, or alter the risk of post-traumatic arthritis after surgical management of ankle, hindfoot, or midfoot trauma. TSL procedures incur additional risks of sural nerve injury, 19 loss of strength and fatigue resistance, 8 and altered gait mechanics.7,14
Neither the prevalence of use of adjunctive TSL procedures in foot and ankle fracture surgery nor the optimal timing of TSL with regard to injury and weightbearing status has been characterized among the orthopaedic trauma and foot and ankle surgical communities. The purpose of this survey is to characterize TSL practice patterns in the management of foot and ankle fractures. We hypothesize that injury features, timing, physical examination information, practice characteristics, and training heritage are meaningfully associated with likelihood of performing adjunctive TSL procedures in the operative management of closed foot and ankle trauma.
Materials and Methods
A survey was developed using published guidance 22 to assess the propensity of practicing surgeons for performing adjuvant TSL procedures in prototypical examples of acute foot and ankle trauma (see online Supplementary Material).The primary survey outcome was, “How likely are you to perform a gastrocnemius recession or tendo-Achilles lengthening?” (collectively, a TSL procedure) for a given clinical scenario. The primary outcome was self-reported on an ordinal Likert scale of 1 for “never” to 5 for “always.” Independent variables included one of 10 specific fracture and/or dislocation patterns across a spectrum of injury energy and severity, with description and representative radiographs, the timing of the surgical intervention (at the time of initial temporizing management such as closed reduction with external fixation or pinning; at the time of definitive internal fixation; or after initiation of weightbearing), and the result a Silfverskiöld test for gastrocnemius tightness of contralateral limb at the time of injury or definitive management or ipsilateral limb at the time of initiation of weightbearing. Covariables putatively considered to influence the primary outcome (TSL procedure) included location and type of fellowship training (foot and ankle, orthopaedic traumatology, both, or neither); years in practice; practice setting; geographic location; American College of Surgeons or equivalent trauma level designation of primary practice facility; and preferences about method of TSL, including preferred procedure and, if open, preferred approach, management of the plantaris tendon, and fascial closure.
Ten clinical case vignettes representative of distinct, archetypal pathologies in foot and ankle trauma for which TSL could reasonably be considered as an adjunctive treatment during initial temporizing management, definitive treatment, or after the patient resumes weightbearing were developed. The cases described closed fractures including 2 levels of severity of ankle fracture (unstable Weber B bimalleolar fracture and Weber C trimalleolar fracture dislocation), tibial plafond fracture (B-type anterior tibial plafond fracture with intact fibula and C-type tibial plafond fracture with fibular fracture), talus fracture (minimally displaced talar neck fracture and displaced talar body fracture dislocation), and calcaneus fracture (displaced split depression-type calcaneus fracture and displaced tongue-type calcaneus fracture) as well as 1 Chopart fracture dislocation and 1 Lisfranc fracture dislocation. Participants were provided a descriptive classification with salient features of the closed injuries as well as 2 to 3 radiographic views of the injury as appropriate for the pathology (Supplement S1).
The survey was distributed to approximately 2519 members of the American Orthopaedic Foot & Ankle Society (AOFAS) and 2400 members of the Orthopaedic Trauma Association by e-mail and made available on the respective websites of these societies. Responses were accepted from December 1, 2021, through February 28, 2022, using Google Forms (Google, Menlo Park, CA).
Statistical Analysis
Frequency distributions between categorical variables were compared by Fisher exact χ2 test. Likert scale responses were treated as ordinal interval data with evaluation of parametric vs nonparametric distribution by skewness testing. 17 The probability of performing a TSL procedure for each permutation of each scenario was approximating by scaling discrete Likert responses (range, 1-5) to a probability score from 0 to 1. This probability score was analyzed as continuous data, reporting mean and 95% CI. Comparisons between grouping by Silfverskiöld test and timing of treatment were made using 2-tailed Student t test of independent means. Interrater agreement was calculated using Conger’s extension of Cohen κ without weights for multiple raters. A multivariable ordered linear regression model was developed to assess for associations of survey respondent practice and training of with overall probability of performing TSL. Analyses were performed using Stata, 15 MP (StataCorp, College Station, TX).
Results
Training and Practice
A total of 258 unique responses were recorded, a crude response rate of approximately 5.2%. The median duration of practice after training was 14 (interquartile range, 7-23) years. Locationwise, 64.7% of respondents practiced in North America, 7.8% Europe, 3.4% South America, 1.9% Oceania, 1.5% Middle East, 0.7% Asia, and 0.4% Africa. Notably, 3 Texans distinguished their location as a distinct region and/or country. Overall, 84.5% of respondents reported fellowship or advanced specialty training in foot and ankle surgery, 24.4% of respondents reported fellowship or advanced specialty training in orthopaedic traumatology, 13.2% reported dual fellowships or advanced training in both orthopaedic traumatology and foot and ankle surgery, and 4.3% of respondents reported advanced training in neither subspecialty. University of Washington/Harborview Medical Center was the most frequently reported (19.6%) trauma fellowship. Baylor (9.8%), University of Washington/Harborview Medical Center (7.4%), Union Memorial (5.4%), and OrthoCarolina (4.4%) were the most frequently reported foot and ankle fellowships. Practice environments were described by 51.9% as private, 3.6% academic, 8.5% hospital employed, 8.1% combination of private and academic practice, and 0.8% military. The trauma designation of respondents’ primary facility was 29.1% level I, 3.2% level II, 17.4% level III, and 23.3% no trauma designation.
TSL Method
Overall, 98.5% of respondents reported performing TSL procedures in their practice, with median self-reported estimate of 25 (interquartile range, 12-50) procedures per year. The preferred method of TSL for 72.1% of respondents was an open transverse gastrocnemius recession (Strayer, modified Vulpius, or Baumann type procedure), 16.9% percutaneous tendo-Achilles lengthening, 3.5% endoscopic gastrocnemius recession, 2.0% open tendo-Achilles lengthening, 2.0% open tongue-in-groove gastrocnemius recession (Baker or modified Fulp and McGlamry), 2.0% open proximal medial gastrocnemius recession, 1.2% variable preference, and 0.4% open pie crusting of the gastrocnemius fascia. Preferred TSL method was not associated with fellowship subspecialty training (P = .630). Of the respondents who preferred an open TSL procedure, 74.1% preferred a medial incision, 25.1% preferred a posterior incision, and 0.8% choose either based on positioning. In addition, 39.8% routinely locate and resect the plantaris tendon. Finally, 57.9% reported they do not routinely repair the fascial incision.
Likelihood of TSL
Survey respondents reported a low overall 7.6% probability (95% CI 6.5%-8.7%) with fair agreement (κ = 0.246) of performing TSL across all scenarios at all time points in treatment, ranging from 0.8% at the initial management of an unstable Weber B bimalleolar ankle fracture in the presence of negative contralateral Silfverskiöld test to 29.3% at the time of definitive fixation of a tongue type calcaneus fracture in the presence of positive contralateral Silfverskiöld test (Table 1). The contralateral Silfverskiöld test was significantly associated with a greater probability of performing TSL for all scenarios at both initial management and definitive fixation at P <.001. The ipsilateral Silfverskiöld test was significantly associated with a greater probability of performing TSL for all scenarios at the initiation of weightbearing at P <.001. By scenario, tongue-type calcaneus fracture was most likely to be treated with adjunctive TSL (19.5%, 95% CI 6.5%-8.7%), followed by closed Chopart fracture dislocation (8.8%, 95% CI 7.0%-10.6%), closed Lisfranc fracture dislocation (8.2%, 95% CI 6.5%-10.0%), closed displaced talar body fracture dislocation (7.2%, 95% CI 5.9%-8.6%), closed displaced intra-articular split-depression calcaneus fracture (7.2%, 95% CI 5.8%-8.5%), closed C-type tibial plafond fracture with fibular fracture (6.2%, 95% CI 5.1%-7.4%), closed minimally displaced talar neck fracture (4.9%, 95% CI 3.9%-6.0%), closed Weber C trimalleolar ankle fracture dislocation (5.3%, 95% CI 4.2%-6.4%), closed B-type anterior tibial plafond fracture with intact fibula (4.3%, 95% CI 3.3%-5.4%), and unstable Weber B bimalleolar ankle fracture (4.2%, 95% CI 3.3%-5.1%).
Probability of Performing Adjunctive TSL for Closed Foot and Ankle Trauma. a
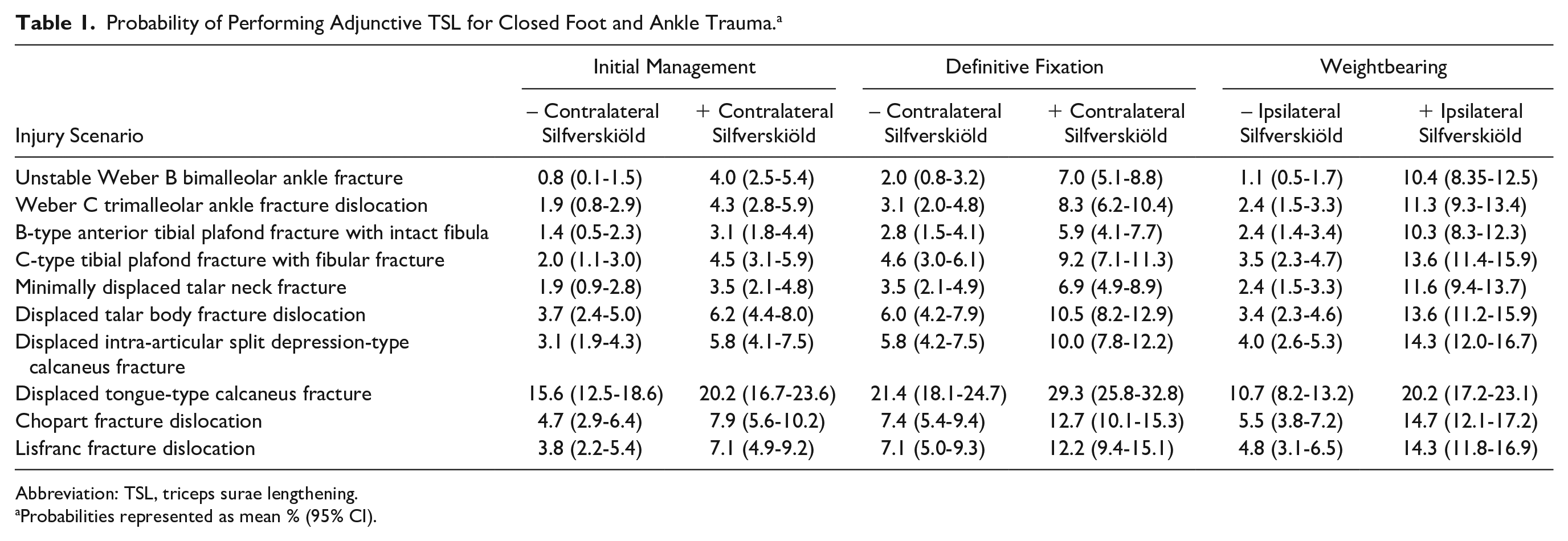
Abbreviation: TSL, triceps surae lengthening.
Probabilities represented as mean % (95% CI).
Multivariable analysis identified a significant association between fellowship training at the University of Washington/Harborview Medical Center in either foot and ankle surgery or orthopaedic traumatology odds ratio of performing TSL (β = 1.5, 95% CI 0.4-2.6, P = .007), but not with years in practice, private vs academic practice; practice in a rural, suburban, or urban environment; facility trauma level designation; or other foot, ankle, or no fellowship training excluding fellowship training at the University of Washington (Supplement S2).
Discussion
In this survey of practicing orthopaedic traumatology and foot and ankle surgeons, we observed fair agreement (κ = 0.25) on and low overall 8% (range, 1%-29%) self-reported probability of performing TSL including gastrocnemius recession or tendo-Achilles lengthening as an adjunctive procedure in the management of closed foot and ankle fractures. The probability of TSL was significantly associated with specific injury pattern. A positive contralateral Silfverskiöld test early in treatment significantly influenced probability of TSL, reflecting proactive management of anticipated tightness in all injury patterns. A positive ipsilateral Silfverskiöld test early in treatment at weightbearing significantly influenced probability of TSL, reflecting reactive management of late gastrocnemius tightness in all injury patterns. Graduates of foot ankle or traumatology fellowship from a single institution demonstrated independently 49% greater odds of recommending TSL after considering other practice characteristics, perhaps reflecting a cultural influence on the TSL practice. The probability of TSL was not significantly associated with type of fellowship training, experience in practice, academic practice, urban or rural setting, or facility trauma designation. To our knowledge, this is the first cross-sectional assessment of TSL practices in the operative management of foot of ankle fractures.
Gastrocnemius recession and tendo-Achilles lengthening procedures were initially described to treat spasticity of the calf muscles limiting ankle motion. By elongating the triceps surae, the ankle may dorsiflex to a greater degree—typically 18 degrees. 18 Silfverskiöld’s description of “reduction of the uncrossed two-joints muscles of the leg to 1-joint muscles in spastic conditions” 21 has been interpreted with various modifications. Baumann’s intramuscular recession of the aponeurosis over the proximal gastrocnemii muscle bellies does not involve the conjoint tendon or the soleus. 3 Strayer’s procedure involves dividing the conjoint medial and lateral gastrocnemii tendon distal to the termination of the muscle bellies, preserving the soleus. 23 Vulpius’s inverted V recession, 25 Baker’s, 2 Cozen’s, 8 as well as Fulp and McGlamry’s tongue in groove techniques 13 all represent more distal variations of the Strayer procedure, which also affect the soleus muscle. The selectivity of these procedures decreases while the length achievable increases with more distal location along the triceps surae. 12
Hatt and Lamphier 15 were the first in 1947 to describe a TSL technique applied to fracture care. The authors used Hoke’s triple hemisection, a multilevel tendo-Achilles lengthening tenoplasty, to improve ankle motion after cast management of comminuted lower limb fractures in US Army patients—“a condition opposed to the usual civilian type of post-poliomyelitis in which muscle imbalance results in shortening of the Achilles tendon.” 15 Of note, anatomic internal fixation was not performed, early motion was not permitted, and TSL was performed in a reactive manner for restricted ankle motion. Benirschke and Kramer suggested assessing for gastrocnemius equinus as a possible “predisposing condition” in Lisfranc injury, and were the first to advocate for acute, adjuvant gastrocnemius recession at the time of definitive fracture fixation, “because a tight gastrocnemius can cause the Lisfranc surgical repair to fail.” 4 These authors and their colleagues have advocated for the acute use of gastrocnemius recession in tibial plafond, calcaneus, talus, and midfoot injuries to facilitate fracture reduction, protect fracture repairs, and improve range of motion.5,16 Surgeons who completed fellowships at these authors’ institution reported a higher probability of performing TSL procedures in the operative management of closed foot and ankle fractures.
We have identified a practice endorsed by 99% of survey respondents that lacks clinical data demonstrating a treatment effect. At the time of writing, there are no published clinical data to support the claim that acute, adjunctive gastrocnemius recession, tendo-Achilles lengthening, or other TSL procedure positively affects outcomes following foot and ankle fracture surgery. On the other hand, TSL procedures may have adverse consequences. Gianakos et al in a systematic review of 23 level III and level IV studies found that gastrocnemius recession for nontraumatic conditions improved dorsiflexion range of motion, AOFAS scores, and visual analog scale scores, yet most patients demonstrated loss of plantarflexion power, impaired fatigue resistance, and alterations to gait kinematics with compensatory activity at the knee and subtalar joints, with an overall complication rate of 14%. 14 The extrapolation of an association between gastrocnemius tightness and degenerative midfoot/forefoot pathology10,11,18,19 and objective benefits of treatment1,14 to acute fracture care is mechanistically logical. However, an association between gastrocnemius tightness and risk of foot or ankle trauma as a predisposing condition has not been described. Nor is a preventative treatment effect of TSL for reducing the risk of post-traumatic arthritis after fracture surgery are presently supported by clinical evidence. The risks of TSL in patients with traumatic injuries may be different from described risks of TSL in nontraumatic conditions; patients with nontraumatic gastrocnemius tightness may be more likely to have preexisting spasticity, cognitive impairment, malnutrition, and other medical conditions associated with adverse surgical outcomes.
There are limitations to this work, chiefly related to bias inherent to survey research. We canvassed the membership of 2 major orthopaedic specialty societies with international membership whose constituents typically have specialty training and routinely manage closed foot and ankle fractures. Our sampling method may have introduced bias by selecting only society members, only 2 societies with primarily North American constituency, and provision of the survey in English language, which limits external validity to the global orthopaedic community as well as to the general orthopaedic profession beyond surgeons who care for complex foot and ankle fractures. Our findings are sensitive to response bias, particularly if proponents of TSL in fracture care were more likely to complete the survey. Our response rate of 5% is low even among surveys of orthopaedic surgeons, 22 but considerably higher than typical response rates of 1% to 2% distributed by AOFAS and OTA via this modality (personal communication with Association staff). Ten arbitrarily selected cases with minimal clinical information (information on soft tissue conditions, preinjury ambulatory status, functional demands, and health history were not provided) cannot approximate the variety of situations or factors, which could elucidate respondents’ propensity to perform TSL in actual practice. Respondents were not presented scenarios of intraarticular block to motion, for which TSL would be insufficient, or combined gastrocnemius and soleus tightness, for which gastrocnemius recession would be insufficient and tendo-Achilles lengthening would be required. We have analyzed discrete ordinal responses with parametric frequency distributions as continuous interval data with parametric tests, a practice with supporting evidence.17,24
In conclusion, orthopaedic trauma and foot and ankle surgeons report similar indications, similar methods, and similarly self-reported propensity to use TSL in the management of foot and ankle trauma. The practice of TSL in acute foot and ankle fracture surgery appears to be modestly prevalent, although certainly not routine nor currently evidence-based. Prospective evaluation of gastrocnemius recession and tendo-Achilles lengthening in fracture surgery is necessary to demonstrate a treatment benefit as well as to quantify the risks in this context.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221126719 – Supplemental material for Triceps Surae Lengthening in Foot and Ankle Trauma: A Survey of OTA and AOFAS Members
Supplemental material, sj-pdf-1-fao-10.1177_24730114221126719 for Triceps Surae Lengthening in Foot and Ankle Trauma: A Survey of OTA and AOFAS Members by Joseph T. Patterson, Sean T. Campbell, Stephen J. Wallace, Erik A. Magnusson, Iain S. Elliott, Kevin Mertz and Stephen K. Benirschke in Foot & Ankle Orthopaedics
Footnotes
Supplement 1
Supplement 2
Acknowledgements
The authors would like to acknowledge the support of the Research Committees of the American Orthopaedic Foot & Ankle Society and the Orthopaedic Trauma Association for the support of this work.
Ethical Approval
Ethical approval for this study was obtained from University of Southern California Institutional Review Board (UP-21-00935).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Joseph T. Patterson, MD, received support for the present manuscript (eg, funding, provision of study materials, medical writing, article processing charges, etc) from AO North America, Young Investigator Research Development Award—unrestricted funds used to pay submission fee and AOFAS survey distribution fee.
Supplemental Material
Supplemental material is available online (SURVEY PDF is available online).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.