
Abstract

Introduction
Talar fractures can be divided into central (body and neck) and peripheral. 11 The peripheral fractures commonly affect the head, the lateral, posteromedial, and posterolateral processes of the talus. 2 An uncommon type of peripheral fracture is at the middle facet, in which there is a depression of the subtalar middle facet through the talar body. The injury was initially characterized by Storm et al 9 in 1996, followed by descriptions by Vlahovich et al 10 in 2005 and Clanton et al 5 in 2013, with a total of 4 cases reported in these 3 studies. Recognition of this lesion and proper treatment could be challenging, directly affecting patients and leading to poor short- and long-term results as a consequence of its intraarticular nature.9,10 This report describes the diagnosis, treatment, and outcomes of 2 patients with this fracture pattern.
Case Reports
Case 1
A 28-year-old male patient was admitted to Jose de Carvalho Florence Municipal Hospital (Sao Jose dos Campos, SP, Brazil) 3 hours after a fall from approximately 2 m, complaining of pain in the lateral and medial aspect of the left ankle. The patient was not able to weightbear. Physical examination showed swelling with mild ecchymosis over the mentioned areas and pain when palpating the sinus tarsi and sustentacular regions. The initial investigation was carried out with conventional radiographs. Only the ankle lateral view portrayed a fracture line with a displacement of the talar lateral process and an increase in the middle subtalar joint space (Figure 1). A computed tomographic (CT) scan was performed to further portray the lesions. The images demonstrated a fracture with impaction of the talar middle facet articular surface associated with a nondisplaced talar head fracture, starting in the impaction zone and extending to the head. In addition, there was a displaced lateral process fracture on the lateral aspect with subtalar articular surface involvement (Figure 1). Surgical treatment was chosen for the 2 fractures because of articular surface displacement.

(A) Lateral ankle radiograph showing a lateral process fracture of the talus (arrowhead). The depressed talar middle facet (arrow), the calcaneal middle facet (plus) counterpart and the increased joint space are also visible. (B) Computed tomographic imaging exhibiting the depressed middle facet (arrow), the displaced fracture line toward the talar head (arrowhead) and the talar lateral process displaced fracture (star).
Surgery was carried out with the patient in dorsal decubitus and spinal block anesthesia. Two approaches were used, one for each topography. The medial incision was straight and horizontal, centered on the sustentaculum tali, approximately 4 cm in length. After sectioning the skin and subcutaneous tissue, the superficial portion of the deltoid ligament was identified and divided in the same direction. At that moment, the tendons of the flexor digitorum longus and hallux muscles had the sheath opened and were recognized and retracted, exposing the joint capsule between the sustentaculum tali and the talar middle facet. After opening of the capsule and debris cleaning, it was possible to identify the depressed facet joint and the fracture line in direction to the head (Figure 2). The impacted and depressed fracture was reduced using a small osteotome. The resulting bone failure zone was filled with a cancellous bone graft taken from the ipsilateral calcaneal tuberosity through a 1-cm lateral incision. After provisional fixation with Kirschner wires and radioscopic control, both facet and neck fractures were fixed with three 2.0-mm cortical screws. A 3-cm lateral approach, 5 mm distal to the tip of the lateral malleolus, horizontal and centered on the lateral process of the talus, was performed. The lateral capsule of the subtalar joint was identified and sectioned, allowing access to the lateral process fracture, consisting of a 15-mm fragment displaced anteriorly (Figure 2). After direct reduction, provisional fixation with Kirschner wires, and fluoroscopic control, the fracture was fixed with two 2.0-mm cortical screws. The wounds were irrigated with saline, sutured in layers, and the patient was placed in a splint.
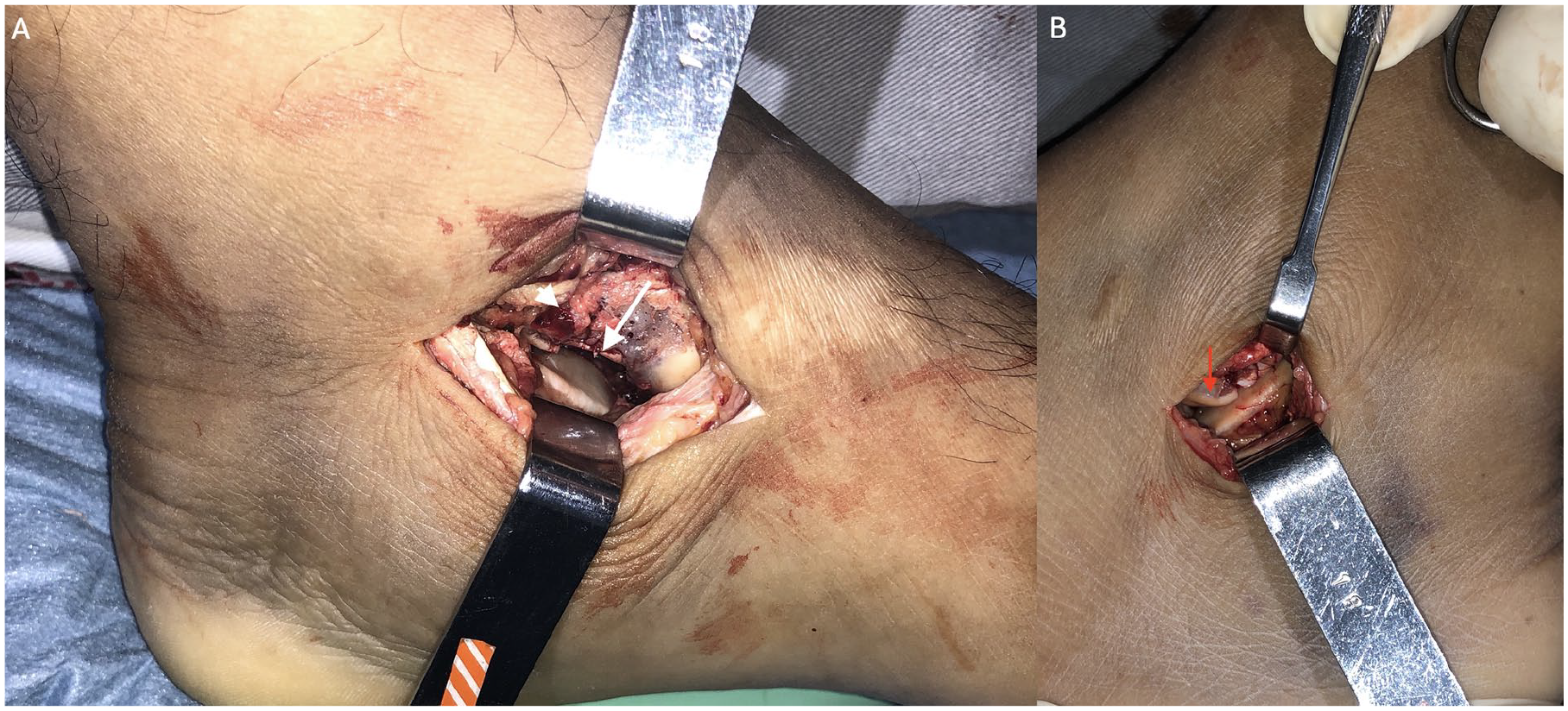
(A) Medial approach picture demonstrating the identification of the depressed middle facet (arrowhead) and the fracture line directed to the talar head (arrow). (B) Lateral incision picture showing the displacement of the talar lateral process (arrow).
The splint was replaced by a removable boot 1 week after the surgery, and guided mobility exercises were initiated. Partial weightbearing started after the fourth week, progressing to full weightbearing after the eighth postoperative week. The last follow-up was performed 21 months after surgery. During this clinical visit, the patient presented with no pain for the usual activities—when assessed by one fellowship-trained orthopaedic foot and ankle surgeon—and with 80% normal subtalar mobility as opposed to the contralateral noninjured side (Figure 3). Functional assessment using the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scale was 97 points. Radiographic imaging showed congruent joint surfaces and no signs of early arthritis (Figure 3).

(A) Inversion and (B) eversion range of motion at the last follow-up assessment (21 months). (C) Lateral radiograph performed at the occasion shows a reduced middle and lateral facets along with a preserved joint space.
Case 2
The second patient, a 24-year-old man, was involved in a car accident, presenting to the same hospital with a left foot trauma. Clinical evaluation showed changes similar to the first case, swelling with mild ecchymosis over the medial and lateral hindfoot. Radiographic investigation displayed a fracture of the talar lateral process and a middle subtalar articular contours absence (Figure 4). Images from the CT showed a fracture with talar middle facet articular surface depression and a nondisplaced fracture that extended to the talar head, extending to the talonavicular articular surface (Figure 4). A lateral process fracture with minimal displacement was also present (Figure 4). Based on these findings, surgical treatment of the middle facet and nonsurgical treatment of the lateral process were selected. A medial approach was accomplished (Figure 5), through which the joint surface was reduced, the defect was filled with a cancellous bone graft (taken from the calcaneal tuberosity), and the fracture was fixed with one 2.0-mm screw. The talar head extension was not fixed because it was found incomplete and stable.
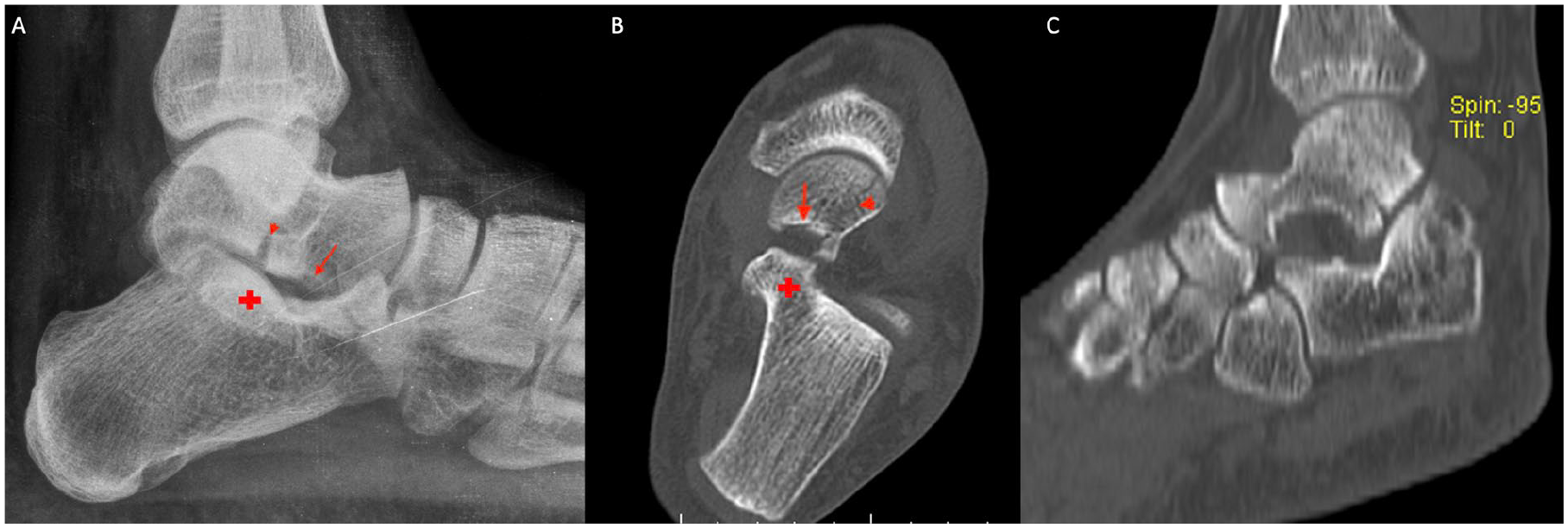
(A) Lateral ankle radiograph showing the talar lateral process fracture (arrowhead), the depressed talar middle facet (arrow), the calcaneal middle facet (plus), and the expansion of joint space. (B) Computed tomographic (CT) imaging showing the depressed middle facet (arrow) on the axial view and the nondisplaced fracture line to the talar head (arrowhead). Calcaneal middle facet (plus) is also evident in panel A. (C) Sagittal CT view displaying the talar lateral process fracture with a minor displacement.

Medial approach picture (A) revealing the depressed middle facet (arrowhead) and the fracture line for the talar head (arrow). Inversion (B) and eversion (C) movements at the last follow-up visit (21 months). Lateral radiograph (D) performed at the moment displaying the reduced middle facet and a preserved joint space.
The postoperative regimen was executed in the same way as described for the first case, and the last follow-up occurred 21 months after the surgery. The patient had an AOFAS score of 82 points because of occasional mild pain, limitation for sports activities, 70% normal subtalar mobility (same assessor), and some difficulty walking on uneven terrain (Figure 5). Radiographs showed preserved joint spaces with no osteoarthritis signs (Figure 5).
Discussion
Vlahovich et al 10 reported a talar middle facet fracture case with a pattern identical to what was described in this study, presenting joint surface depression associated with a sagittal fracture line extending to the talar head. The authors emphasized that this was an infrequent fracture type, which had been previously reported only once by Storm et al. 9 However, the talar middle facet fracture characteristics cited by Storm et al 9 were different from the present report and the case described by Vlahovich et al. 10 Storm et al 9 reported an intra-articular middle facet fracture, with CT imaging showing a loose bony body interposed at the subtalar joint, with no areas of articular depression. Clanton et al 5 described 2 talar middle facet fractures, only discernable by magnetic resonance imaging. The mechanism was characterized based on chondral lesion type, regarding anatomical defect areas, and the presence of a free chondral fragment associated with edema of the underlying subchondral bone. 5 No fracture line toward the talar head or middle facet subchondral depression was reported. 5
The trauma mechanisms of this report’s patients were a fall from an elevated level and a car accident, unlike what happened in the 3 cases described by Vlahovich et al 10 and Clanton et al, 5 all caused by snowboard accidents. Regarding the type of associated fracture, in both of our 2 cases and in 2 patients described by Clanton et al, 5 there was a talar lateral process fracture, which was not found by Vlahovich et al. 10 An association of eversion, axial compression, and dorsiflexion is the described mechanism for producing a talar lateral process fracture. 3 However, a possible mechanism for the impacted fracture of the middle facet of the talus was not discussed by the previous authors. In this case report, the lateral process had a fracture pattern that suggests a possible compression by the posterior facet of the calcaneus, from posterior to anterior (Figures 1 and 4). Considering that the medial side had a depression generated by compressive forces, a possible mechanism could be axial compression with varus and internal rotation of the calcaneus in relation to the talus. This movement would increase contact between medial joints, allowing a vertical force to produce the collapse. 8
Peripheral talar fractures usually produce a subtle clinical picture that is often interpreted as an ankle sprain, and the fracture might not be noticed in the initial evaluation. 7 In the cases described by this report, the most evident fracture on radiographs was the talar lateral process. A joint space widening of the subtalar middle facet on the lateral ankle radiography was found in both cases and was identified by surgeons habituated to analyzing images of this region, by using the facets’ parallelism and orientation (Figures 1 and 4). However, if the radiograph is not performed with the correct technique and foot properly positioned, the diagnosis could be easily missed.4,6 Another fact contributing to the lesion’s nonrecognition is that a detailed analysis of this region of the talus is rarely performed in emergency care by a specialized physician. A CT study could represent fracture details with precision. Still, because this structure has a small area with a horizontal orientation, in acquisitions with thicker slices, the fracture may not be detected. 10 Magnetic resonance imaging could identify these injuries. Nevertheless, as these techniques are not the standard in foot trauma, this fracture might be more frequent than what is described. 5 A high degree of suspicion is necessary to diagnose peripheral talar fractures, especially the middle facet joint impaction fracture. 12
Clanton et al 5 treated their 2 cases nonoperatively. However, no subchondral bone fracture and displacement were noticed. The treatment described in this report was surgical with joint fracture direct reduction, bone grafting, and stabilization with screws, similar to what was accomplished by Vlahovich et al. 10 The criteria used to make this decision were that were joint fractures with load surface displacements. The middle facets have an important role in load and force transmission through the acetabulum pedis.1,8 The triplanar and pivotal subtalar motion also requires middle facets for proper rotation and shear around joint axis. 1
Conclusion
Impaction fracture of the middle facet articular surface is a peripheral talar fracture with very few cases described in the medical literature. Its diagnosis requires a meticulous physical examination, radiographic analysis (particularly a good lateral view), and CT evaluation. Surgical treatment should be considered due to the fact this is a displaced intraarticular fracture in a weight-bearing area.
Footnotes
Ethics and Means of Dissemination
Ethical approval for this study was waived by Hospital Municipal José de Carvalho Florence Review Board because this is a case report and patients consented for the publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.