
Abstract
Background:
Different fixation techniques are established for first metatarsophalangeal joint (MTPJ) arthrodesis, including compression screws, plates, Kirschner wires, metal- and bioabsorbable screws as well as staples. The purpose of this study was to investigate and present first clinical and radiologic results using a novel human, allogeneic cortical bone screw for arthrodesis of the first MTPJ.
Methods:
Arthrodesis of the first MTPJ was performed in 31 patients with hallux rigidus. Percentage union and time to union were the first outcomes; visual analog scale for pain, hallux valgus angle (HVA), intermetatarsal angle, and American Orthopaedic Foot & Ankle Society (AOFAS) hallux score were secondary outcomes.
Results:
Median time to union was 89 days, and union was observed in all patients. There were 4 complications (2 osteolysis margin, 1 cystic brightening, and 1 severe swelling at the first follow-up) all of that resolved at last follow-up. Pain significantly decreased from visual analog scale 8.0 to 0.2 points (P < .0001). The HVA decreased from 30.4 to 10.2 degrees in the patient group with deformities. The total AOFAS score increased significantly from 48 to 87 (P < .0001).
Conclusion:
Primary and revision arthrodesis of hallux rigidus with the human, allogeneic cortical bone screw reveals satisfying results similar to clinical and radiologic outcomes of other surgical techniques. Within 1 year, the human, allogeneic cortical bone screw is fully remodeled to host bone.
Level of Evidence:
Level IV, retrospective case series without control group.
Keywords
Introduction
Different fixation techniques are established for hallux rigidus arthrodesis of the first metatarsophalangeal joint (MTPJ) using compression screws, dorsal plating, Kirschner wires, pins, and staples.15,22 These are currently considered the gold standard in the treatment of hallux rigidus. High fusion rates ranging between 90% and 100% were achieved with arthrodesis.4,14,37 However, Massimi et al 22 reported union rates as low as 53%. Prat et al 28 reported a correlation between nonunion after first MTPJ arthrodesis and diabetes mellitus.
Early clinical trials using the human, allogeneic cortical bone screws for arthrodesis of the first MTPJ showed promising results with complete incorporation and full remodeling within the host bone.2,16,27 Biological augmentation of arthrodesis in foot and ankle surgery using allogenic bone shows satisfying results and high fusion rates without experiencing adverse events because of its osteoconductive potential.24,33 Other bone augmentation materials such as demineralized bone matrix (DBM) consisting of a collagen scaffold and several growth factors, most importantly bone morphogenetic proteins, result in a high positive turnover. 35 Thus, DBM can actively induce bone formation by its osteoinductive potential following endochondral ossification because of the recruitment of mesenchymal stem cells from bone.3,30 The safety of human allogeneic, sterilized bone transplants regarding disease transmission, biological tolerance, potential graft rejection, and allosensitization is well known because allogeneic bone transplants (eg. bone chips, bone blocks) are widely used in regenerative, maxillofacial, and orthopaedic surgery.7,9,29 In the case of the human, allogeneic cortical bone screw, hardware removal is not necessary and biofilm development was not reported as described for titanium and stainless steel screws and plates.1,13,17,32 Because of similar stiffness 26 of the human, allogeneic bone screw and the host bone, stress shielding and disuse atrophy can be avoided. 27 The human, allogeneic cortical bone screw is remodeled to host bone, 2 and because of its architecture, the presence of Haversian canals, transcortical vessels, and the lacunocanalicular system, it allows fluid and cell movement that is initiated by bone strain, guiding the bone remodeling process. 10
The aim of this study was to present results of the human, allogeneic cortical bone screw used for primary and revision arthrodesis of the first MTPJ. Bone union with remodeling into the host bone was set as primary outcome. Secondary outcomes were the longitudinal investigation of the visual analog scale (VAS) pain score as well as the hallux valgus angle (HVA), the intermetatarsal angle (IMA), and the American Orthopaedic Foot & Ankle Society (AOFAS) hallux score.
Patients and Methods
A total of 31 patients were retrospectively evaluated following first MTPJ arthrodesis between 2016 and 2021 using the novel human, allogeneic cortical bone screw (Shark Screw®, Surgebright GmbH, Lichtenberg, Austria). The study was conducted in line with the Helsinki Declaration and was approved and supervised by the local ethics committee of the City of Vienna, Austria (EK 21-175-VK).
Inclusion criteria were age between 18 and 85 years with radiologically certified hallux rigidus. Exclusion criteria were oncologic treatment in the past and chronic alcohol and drug abuse. In Austria, patients generally remain 3 days in total in the hospital, with 1 day each for admission, surgery, and discharge. Clinical follow-up included functional outcomes as well as the evaluation of pain using the VAS (0-10; 0 = no pain, 10 = highest pain) and the AOFAS hallux score (0-100; 0 = worst outcome, 100 = best outcome). Because of the arthrodesis, first MTPJ motion was not detected after surgery and AOFAS score could reach maximally 90 points. Radiologic outcomes included the longitudinal evaluation of the HVA and IMA. Furthermore, the optical density (measured in counts) of the human, allogeneic cortical bone screw in the host bone and of the surrounding host bone was measured on standard radiographs and evaluated in 4 time points: immediately after surgery and at time intervals of 3-6 months, 6-12 months, and after 12 months.
Surgical Procedure
In case of strong deformities, poor bone quality, big bone defect after slipping off using the cup and cone technique, or a primary Brandes surgery revealing a short stump of the proximal phalanx, 1 intramedullary Shark Screw® was used. In any other case, 2 crossed Shark Screws® were used (Figure 1).

Surgical procedure (2 crossed Shark Screws®): (A) Lateral view; starting from an imaginary center line, the Kirschner wires were placed once dorsally and once plantarly so that they did not touch each other. This leaves enough space for drilling, tapping, and placing the Shark Screws®. (B) Anteroposterior view: a 1.6-mm Kirschner wire was placed from proximal medial to distal lateral, dorsal, and a second Kirschner wire from distal medial to proximal lateral, plantar. (C) Lateral and (D) anteroposterior views: these correspond to the later desired position of the Shark Screw®. The Shark Screws® were screwed in without much resistance. (E) Lateral view: protruding material was sawn off at the bone level. The transplant was smoothened and functions as a bone bridge and guiding substance for host cell migration. (F) Postsurgical plaster.
A medio-dorsal skin incision was made and the first metatarsal head was exposed. Cartilage removal of the first MTPJ was performed with the appropriate cup and cone reamer. After removal of the reamers, the bone surfaces were freshened with a thin drill bit to enhance bone union. The metatarsal head and the proximal phalanx were pressed firmly against each other, and the joint was temporarily fixed with a 1.6-mm Kirschner wire to keep it stable. The correct position of the arthrodesis was checked using a stable sterile board. Coming from an imaginary midline, a 1.6-mm Kirschner wire (more torsion stability) was placed from proximal medial to distal lateral, dorsal, and a second 1.6-mm Kirschner wire from medial distal to proximal lateral plantar. One of the 1.6-mm Kirschner wires was exchanged for a 1.2-mm Kirschner wire because of the internal size of the reamer. The core hole was gradually reamed over the 1.2-mm Kirschner wire. Depending on the size of the bone, either two 4.0-mm or two 4.5-mm Shark Screws® were used. After cutting the threads and thoroughly rinsing the drill holes, the Shark Screws® were inserted without much resistance. After a fluoroscopy check, the protruding material was sawn off at bone level. Last, stepwise wound closure was performed (Figure 1).
Postoperative Protocol
After the foot was swollen down (3-5 days postoperatively), patients were fixed with a forefoot soft cast with inclusion of the big toe for a minimum of 6 weeks (Figure 1). No weightbearing on the foot was allowed for the first 4 weeks; in the remaining 2 weeks, increasing weightbearing on the foot was permitted in the cast.
Statistical Analysis
Descriptive statistics were used to present the demographic data. For the secondary outcome measures, paired Student t tests were performed. A P value <.05 was considered to be significant with a power >0.8. All statistical analyses were performed using Origin Pro statistical software (OriginPro, version 2021b; OriginLab Corporation, Northampton, MA).
Results
Demographic data are presented in Table 1. In 10 cases, previously failed surgeries were documented (Austin osteotomy n=4, pseudarthrosis after metal plate arthrodesis n=2; basic resection Brandes n=2; Scarf osteotomy n=1; pseudarthrosis after metal screw fixation n=1). Eleven patients presented with deformities (HVA >20 degrees). In 26 cases, an osteosynthesis was performed with 2 crossed human, allogeneic cortical bone screw; in 5 patients, osteosynthesis was performed using 1 intramedullary human, allogeneic cortical bone screw (Table 2). One human, allogneiec cortical bone screw fractured during surgery because the surgeon tried to introduce the screw lower than the thread was prepared for; nevertheless, the screw was left in place because the arthrodesis was stable. Mean duration of surgery was 63±10 minutes and the median hospital stay of the patients was 3 days (3-28 days). Hospital days include 1 presurgery day with all the preparation for the surgery, the surgery day, and discharge 1 day after surgery. One patient had a hospital stay of 28 days because of an additional treatment of a diabetic ulceration on the first metatarsal bone with intravenous antibiotic therapy (Table 2). Mean follow-up was 11 ± 4 months. One patient requested a reoperation because the correction was too much (3 degrees valgus after surgery, patient requested 5-8 degrees valgus for cosmetic reasons). Bone union (Table 2) was observed as early as 40 days after surgery but was achieved in all patients at a median time of 89 days. At the first follow-up, 1 patient showed severe swelling. Lightening margins were recorded in 2 patients at first and second follow-up, which disappeared at later follow-up. Temporal dynamics and cystic brightening were observed in 1 patient. There were no pathologic signs at the last follow-up radiographs. Because of the COVID-19 pandemic situation, some patients omitted follow-up visits at scheduled times; thus, the range of bony union is very large (40-500 days) because bone union could only be detected with actual radiographs when patients were present for the visit. VAS pain score significantly improved after surgery (P < .001; Table 2). The total AOFAS score significantly improved after surgery (black line, P < .001; Table 3, Figure 2).
Patient Data and Clinical Data (N = 31).
Abbreviation: BMI, body mass index.
Data of Surgery and Rehabilitation.

Abbreviations: MTPJ, metatarsophalangeal joint; VAS, visual analog scale.
1 patient received additional antibiotic therapy to treat diabetic ulceration (hospital stay 28 days).
Overcorrection; 3 degrees was corrected to 8 degrees.
Some patients omitted follow-up visits because of the COVID-19 pandemic situation.
P < .0001 vs presurgery.
AOFAS Hallux Score Details. a

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society hallux score; IP, interphalangeal; MTP, metatarsophalangeal.
Values are mean ± SD (range). MTP joint motion is not possible anymore because of arthrodesis. AFOAS total score of 90 is the maximal achieved score postsurgery because of arthrodesis of the first MTP.
P < .05, **P < .01, ***P < .001, ****P < .0001 vs presurgery.
P < .05 and ‡P < .01 vs 3 months after surgery.

AOFAS hallux score subgroups: pain, function, axial position, and AOFAS total. The maximal achieved scores after surgery are 35 for function and 90 for AOFAS total, because of arthrodesis of the first metatarsophalangeal joint. AOFAS, American Orthopaedic Foot & Ankle Society.
Average presurgical HVA (Table 4) in patients with deformity was 30 degrees, which improved significantly to 10 degrees (P = .001) after surgery. For the hallux rigidus patients without deformity, the HVA improved from 12 to 7 degrees (P < .001; Table 4), and IMA also improved significantly in both groups. At last follow-up, there was no change in the HVA and IMA in comparison to just after surgery (Table 4).
Hallux Valgus Angle and Intermetatarsal Angle. a
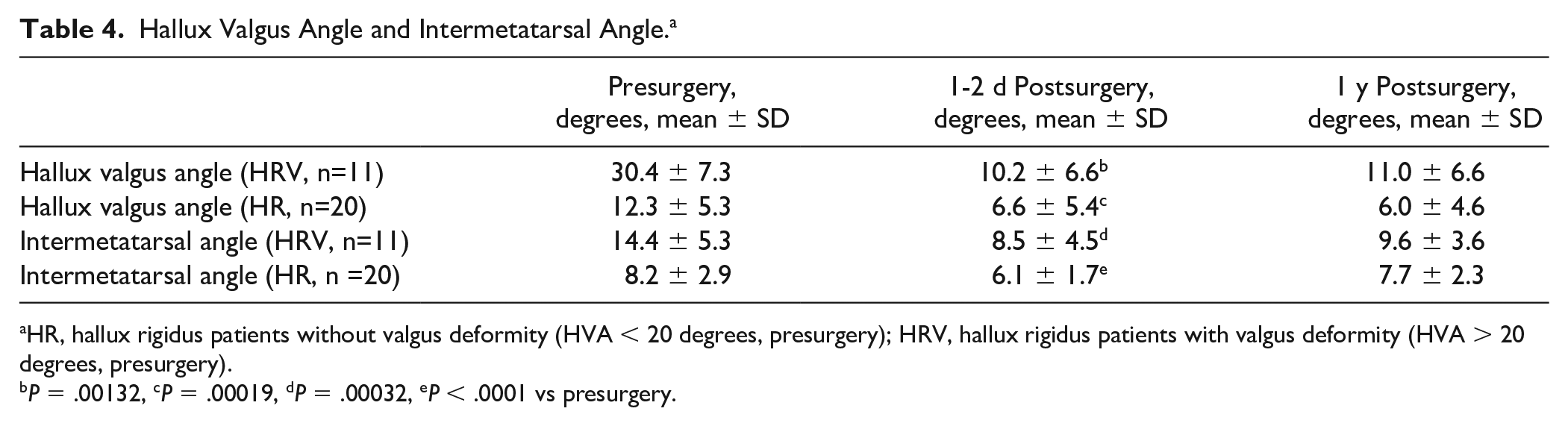
HR, hallux rigidus patients without valgus deformity (HVA < 20 degrees, presurgery); HRV, hallux rigidus patients with valgus deformity (HVA > 20 degrees, presurgery).
P = .00132, cP = .00019, dP = .00032, eP < .0001 vs presurgery.
A hallux rigidus patient without deformities treated with 2 crossed Shark Screws® using the cup and cone technique is presented in Figure 3A-E. The integration of the crossed human, allogeneic cortical bone screws is well visible, after 12 months (Figure 3E); only a faint line of the human, allogeneic cortical bone screw is visible.

A hallux rigidus patient without deformities treated with 2 crossed Shark Screws® using the cup and cone technique: (A) presurgery and (B) 6 weeks, (C) 4 months, (D) 7 months, and (E) 12 months postsurgery. The integration of the crossed human. allogeneic cortical bone screws is well visible; after 12 months, only a faint line of the human, allogeneic cortical bone screw is visible.
A Weil osteotomy on second-fourth metatarsal and a proximal interphalangeal arthrodesis on the second toe, additionally to the hallux rigidus arthrodesis treated with 1 intramedullary screw using the cup and cone technique, is shown in Figure 4A-D. The human, allogeneic cortical bone screw was placed intramedullary. Six months after surgery, all screws are already well integrated into the bone (Figure 4D).

Hallux rigidus patient treated with 1 intramedullary Shark Screw® (5 × 35 mm) using the cup and cone technique for first metatarsophalangeal arthrodesis additional to second-fourth Weil osteotomies and second proximal interphalangeal arthrodesis with Shark Screw® at 3.5 mm: (A) presurgery, (B) just after surgery, and (C) 3 months and (D) 6 months postsurgery; the screws are already well integrated into the bone.
A diabetic patient with a severe ulceration and hallux rigidus on the first MTPJ is presented in Figures 5A-D and 6A-E. The treatment of the ulceration as well as of the severe hallux rigidus (after refreshing the surfaces of the joint) was performed simultaneously. The healing of the ulceration was obtained within 10 weeks (Figure 5D). The bony healing was obvious 12 months after surgery (Figure 6D), and the bone screws were nearly invisible after 20 months (Figure 6E).

Clinical results of the diabetic patient treated with antibiotic therapy and arthrodesis after refreshing the surfaces of the joint of the hallux rigidus at the same time: (A) 1 week after surgery, (B) 2 weeks after surgery, (C) 6 weeks after surgery, and (D) 10 weeks after surgery; the ulceration was completely healed.

Radiologic results of the diabetic patient in whom union was observed 160 days after surgery: (A) presurgery, (B) postsurgery, (C) 6 weeks postsurgery, (D) 12 months postsurgery, and (E) 20 months postsurgery; the human, allogeneic cortical bone screws are nearly invisible.
Bone density was evaluated radiographically (Figure 7). Four months after surgery, the density of the human, allogeneic cortical bone screw was not significantly different from the host bone, and after 17 months the optical density was similar to the host bone, with 2732±435 and 2594±366 for the human, allogeneic cortical bone screw and the host bone, respectively.
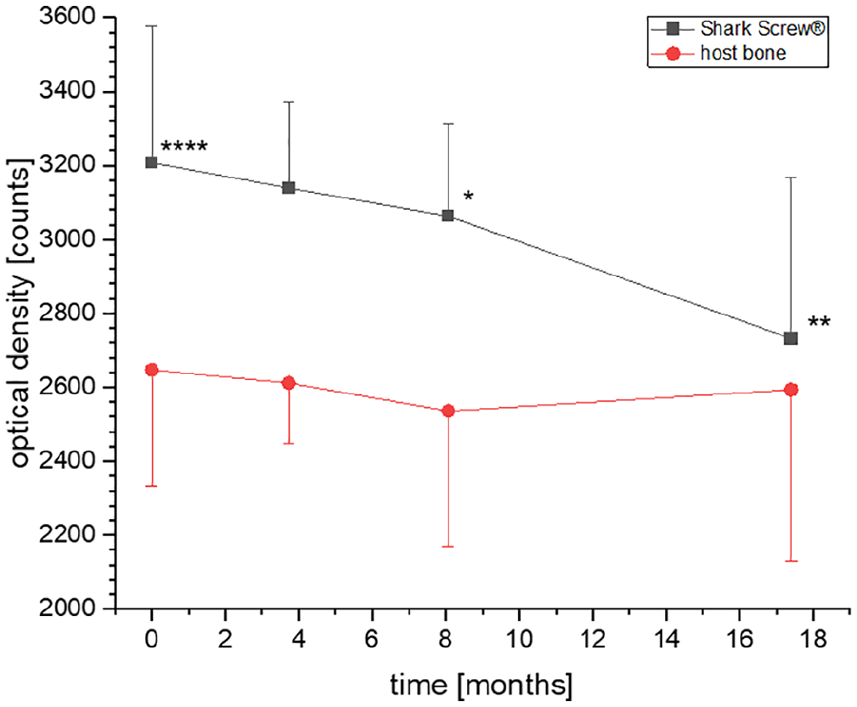
Bone density (optical density [counts]) was evaluated radiographically for the human, allogeneic cortical bone screw in the host bone and of the host bone around the screw. Average time points of evaluation was just after surgery and at 4, 8, and 17 months after surgery. *P < .05 and **P < .01 vs postsurgical values; ****P < .0001 vs the density of the host bone just after surgery.
Discussion
The novel human, allogeneic cortical bone screw (Shark Screw®) shows promising results for arthrodesis of the first MTPJ in patients with hallux rigidus and ensures a stable osteointegration, regardless of previously performed surgeries, with a low rate of complication and without the need of hardware removal or donor site morbidity. The remodeling of the human, allogeneic cortical bone crew into the host bone is nearly completed after 1 year. Additionally, the HMA and IMA were significantly reduced in all patients and did not change over time.
Demineralized allografts such as DBM are discussed to have a high osteoinductive potential because of the better accessibility of bone morphogenetic proteins resulting from the demineralization. 36 On the other hand, the osteoinductive capacity of bone grafts is not only dependent on bone morphogenetic proteins but also related to the presence of soluble minerals such as calcium and phosphate. 12 Therefore, bone allografts, such as the human, allogeneic cortical bone screw, do actually have an even higher osteoinductive potential compared with DBM. 20 Because of its physiological bony architecture, the human, allogeneic cortical bone screw allows bone regeneration, vascularization, and migration of cells of the immune system into the human, allogeneic cortical bone screw in a short time. 2 The measurement of the optical density confirmed the subjective impression on the radiographs that the human, allogeneic cortical bone screw is remodeled to host bone over time. Others have shown that the human, allogeneic cortical bone screw has haversian canals that allow fluid movement and ingrowth of blood vessels into the human, allogeneic cortical bone screw as early as 10 weeks postsurgery. 2 This triggers the bone remodeling process. 10 Blocking the osteoclast function, for example, by using metal screws thereby limits transcortical vessel formation and remodeling. 10 Histologic analysis of an explanted part of a human, allogeneic cortical bone screw with surrounding host bone revealed vascularization of the graft, with newly formed compact lamellar bone exactly fitting to the implant, plump osteoblasts with osteoid production, and osteocytes within the lacunae of the graft. 2 The human, allogeneic cortical bone screw is a safe alternative to other implants. The provider of the human cortical allograft (DIZG gGmbH) did not record any transmission of diseases over all the years of its activity. The allograft avoids the building of biofilm, as observed when using stainless steel or titanium screws and plates.1,13,17,32
The complication rate is high after hallux rigidus correction and is reported as high as 28%, depending on the technique and the material used.15,34 In our case series, complications were recorded in 4 patients during early follow-up, which all resolved at last follow-up. None of our patients presented numbness, elevation of the hallux off the ground, or metatarsalgia as reported elsewhere. 25 Stress fractures were not observed in our cohort. Possible complications of first MTPJ arthrodesis include, in addition to general surgical complications, above all insufficient or missing osseous development (pseudarthrosis), as well as pain and irritation caused by the implant. Nevertheless, revision surgery is necessary in 4% to 15% of the patients.5,14,15,34,37 In our cohort, 1 patient requested revision because of an overcorrection.
The union rate obtained (100%) is similar to other studies,18,21,25 but lower fusion rates are reported too, for the arthrodesis of the first MTPJ (81%-99%4,8,14,15,22,28,31). Tobacco use increased the time to union by 10 days in our study, but because there were only 4 smokers in the patient cohort, it did not reach statistical significance.
Median time to union was 89 days (13 weeks) in our patient cohort, which is lower than that reported by Kaufmann 18 (8 months) or Massimi et al 22 (21 weeks). Latif et al 21 described a time to union of 6-8 weeks for 75% of the patients and bony union in all patients after 12-16 weeks, which is similar to our results. Roukis 31 described 64 days as mean time to union. Hodel et al 15 described in their review article time to fusion after arthrodesis of between 4 and 31 weeks. Because of COVID-19, some of our patients omitted scheduled follow-up visits and bone union could only be recorded at the next follow-up. We could not observe any difference between the primary and revision surgery group in respect to time to union.
HVA and IMA were significantly reduced after surgery (from 30 to 10 degrees and from 14 to 8.5 degrees for HVA and IMA pre- and postsurgery, respectively) and did not change over time. These results are similar to other studies 4 for HVA. IMA was reported as 11 to 12 degrees by other authors. 4 Hodel et al 15 described an HVA of 11 to 15 degrees postsurgery and that positioning of the arthrodesis angle is crucial for optimal bone-to-bone contact, allowing bony healing. 15
VAS pain score decreased significantly after surgery (P < .0001). This is in agreement with the literature. 28 Pain during physical activity can be significantly reduced by arthrodesis of the first MTPJ.4,14,23
The AOFAS hallux score 19 showed significantly higher values postoperatively throughout the follow-up, accompanied by satisfying clinical results. The AOFAS score in our older patient cohort was 48 presurgery, which is similar to other studies.4,15,18 Mean postsurgical AOFAS score at last follow-up was 86 (median 90), similar to other studies (range 83-92),15,18 and was found to be 79 by another study for an older patient group. 4 Very good results were also reported in younger, sportive patients with a relatively higher level of physical activity. 6 The trend to higher AOFAS with younger age was also detected in our patient cohort. In our revision group, the median AOFAS score was 86 in comparison to 90 for the primary surgery group. We could not detect a lower AOFAS score in the revision group.
An interesting observation was one patient with preoperative diabetic ulceration on the affected foot. Infections are reported to be an exclusion criterion for the arthrodesis and can only be managed after screw removal. 11 However, the first MTPJ arthrodesis using the human, allogeneic cortical bone screw with concomitant debridement of the ulcerative tissue was performed in the same session. The ulceration completely healed with an additional antibiotic treatment.
The main limitation of the study is the retrospective design of the study with no control group.
In conclusion, primary arthrodesis of hallux rigidus with the human, allogeneic cortical bone screw reveals results similar to reports in the literature for other techniques and for metal or bioabsorbable screws with a low complication rate. Especially for revision surgery and in older and/or diabetic patients, this is the surgical procedure of choice, because it gives similar results as studies that used other techniques for younger patients and primary surgeries. The main advantage of the technique reported here is that no second operation is needed to remove hardware; in addition, the bone screw replaces missing or eroded bone and revisions are possible without any limitations.
Footnotes
Ethical Approval
The study was conducted in line with the Helsinki Declaration and was approved and supervised by the local ethics committee of the City of Vienna, Austria (EK 21-175-VK, on September 10, 2021).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.