
Abstract
Background:
Management of displaced intraarticular calcaneus fractures can be operative or nonoperative. Several randomized and case-controlled trials have been recently conducted in order to reach a consensus. The purpose of this analysis is to provide recommendations for the management of these injuries based on the best available clinical evidence.
Methods:
An up-to-date search was conducted using predefined eligibility criteria. The Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA) was followed. Randomized and prospective clinical trials were only included after agreement among all authors. Relevant literature was appraised for methodologic quality using the Cochrane collaboration tool for the randomized controlled trials (RCTs) and Newcastle Ottawa Score for the prospective trials. Outcome measures included American Orthopaedic Foot & Ankle Society ankle-hindfoot score, visual analog scale score, return to activity, complications, residual pain, and development of arthritis. RevMan, version 5.3.5 software, was used for data analysis. A P value of <.05 was considered statistically significant, and CIs were set at 95%.
Results:
A total of 13 studies and 1251 patients were included in our analysis. This involved 10 RCTs and 3 prospective clinical trials. Shoe fitting problems and failure to return to activity favored the operative group. No other studied variables showed clear superiority of a specific treatment approach.
Conclusion:
The best evidence available at this time favors an advantage to operative treatment. Patients should be informed that the clear differences are centered on comfort of shoe wear and return to desired activity level.
Introduction
Calcaneal fractures are one of the challenging injuries in orthopaedic practice, which usually result from an axial compressive force, such as fall from height or road traffic accident. 5 Calcaneal fractures represent 1% to 2% of all human body fractures, and the calcaneus is the most commonly fractured tarsal bone. 5 They could be intra- or extraarticular in the form of avulsion fracture of the sustentaculum tali, calcaneal tuberosity, or anterior process. 5 Sanders classification is the most widely used system for intraarticular calcaneal fractures. It depends on the number of intraarticular fracture lines in the coronal computed tomography (CT) scan. 21 Sanders types II, III, and IV are collectively categorized as displaced intraarticular calcaneal fractures (DIACFs). 21
Recently, the management of DIACF has been controversial, with several studies favoring the operative treatment,18,24 whereas others found no difference between the operative and nonoperative management.10,19 Randomized controlled trials (RCTs) were accordingly conducted, aiming to establish a consensus in the treatment of these injuries.1,3,4,6,7,9,17,19,23,24
Conservative treatment involves limb elevation, splinting, nonweightbearing for an average of 6 weeks, and physiotherapy for rehabilitation, which may take up to 2 years. 19 However, the bone deformity caused by the initial injury is left unmanaged, potentially leading to heel deformity, arthritis, or chronic pain. These are the reasons behind literature advocating for the operative treatment of these fractures. 14
Conversely, any operative management of these injuries aims at correcting the bone deformity, providing stable fixation, and allowing expeditious return to physical activity. 16
There has been a wide variation in the operative techniques used to manage these injuries, starting from the extensile lateral approach with or without bone grafting to the recent minimally invasive techniques. 22 Further, there has been a massive advancement in the implants used for calcaneal fractures, from the traditional Kirschner wires (K-wires) 27 to screws and the new low-profile plates. 25
However, a large cohort of patients still experience significant symptoms after undergoing the operative treatment.4,6 Shoe fitting problems and chronic foot pain or discomfort have been frequent challenges following these injuries regardless of the treatment type because of change in the heel width and calcaneal length. 26 Moreover, life quality scores have been frequently low in patients with calcaneal fractures. 2
This meta-analysis aims to provide level I and II recommendations for DIACF management based on the best available evidence.
Materials and Methods
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 15 and Cochrane Handbook 8 for Systematic Reviews of Interventions 5.1.0, using a predefined search strategy agreed among all authors.
Search Strategy
Medline and Embase databases, alongside the Cochrane library, were searched from inception to December 2021. The search was performed with the following MeSH terms: intraarticular fractures AND Calcaneus AND displaced AND Conservative OR Surgical management. An additional search was also performed looking for clinical trials in the ClinicalTrials.gov database (http://clinicaltrials.gov) and the World Health Organization (WHO) International Clinical Trials Registry Platform search portal (http://apps.who.int/trialsearch/).
Study Selection
Two authors independently reviewed all search terms, titles, abstracts, and full-text articles for relevance. Any disagreement between the 2 authors regarding the inclusion or exclusion of the studies was resolved in a meeting with a third senior author. The following are our inclusion and exclusion criteria for this study.
Eligibility Criteria
Inclusion criteria:
Studies directly comparing nonoperative and operative DIACF management
Levels I and II (RCTs and prospective comparative) studies
Studies in the English language only
Human studies only
Exclusion criteria:
Studies involving cadavers
Biomechanical studies of treatment options
Abstracts, case reports, systematic reviews, and retrospective studies
Data Extraction
Data from eligible studies were independently retrieved by 2 authors and added to an Excel sheet presented in Table 1. The tabulated data includes author, year, study type, country of origin, sample size, mean age in years, sex ratio, follow-up in years, fracture classification system, and measured outcomes.
Characteristics of All Included Studies.
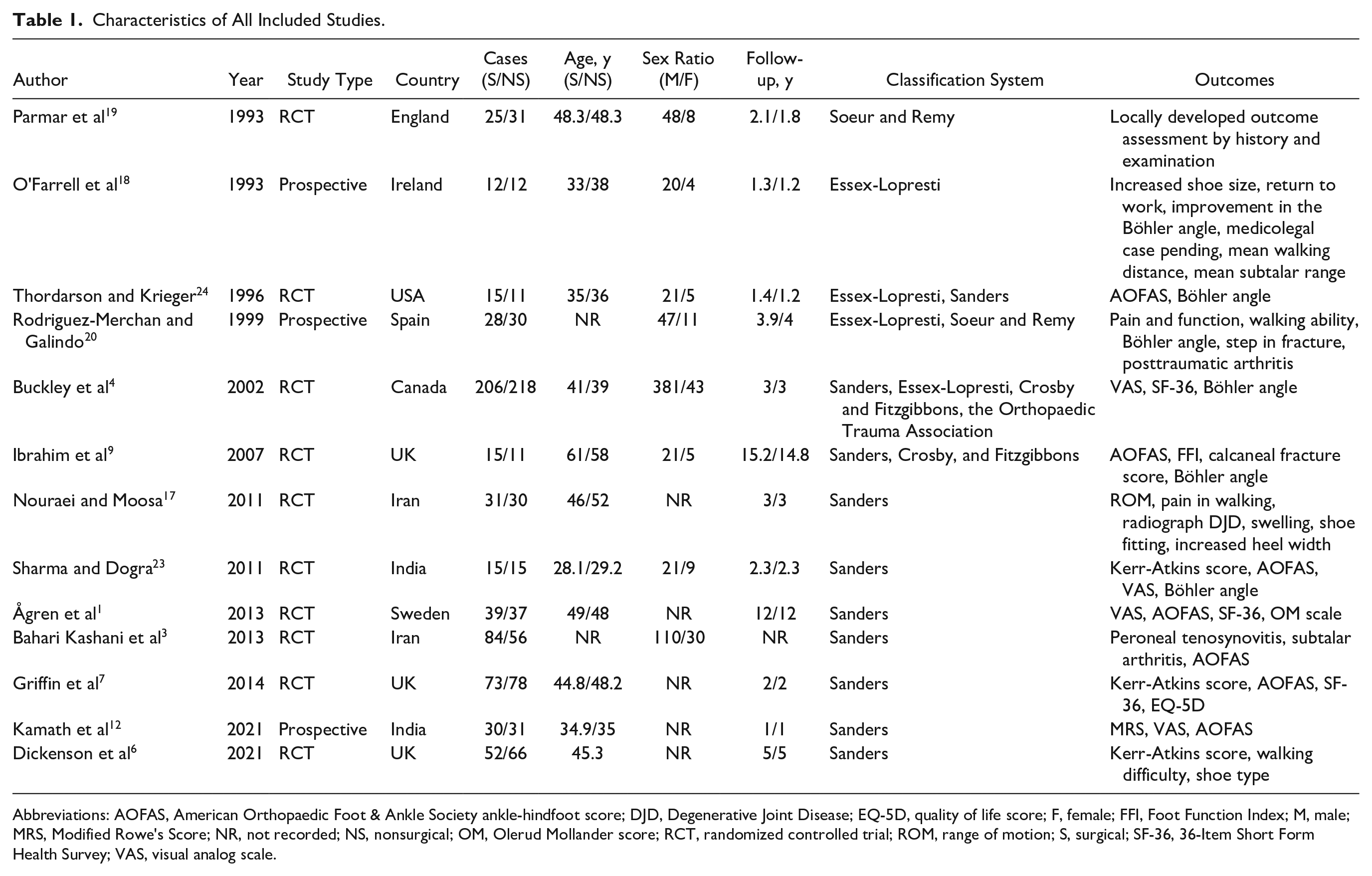
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot score; DJD, Degenerative Joint Disease; EQ-5D, quality of life score; F, female; FFI, Foot Function Index; M, male; MRS, Modified Rowe's Score; NR, not recorded; NS, nonsurgical; OM, Olerud Mollander score; RCT, randomized controlled trial; ROM, range of motion; S, surgical; SF-36, 36-Item Short Form Health Survey; VAS, visual analog scale.
Data Synthesis and Statistical Methods
In this analysis, continuous and dichotomous variables were assessed using mean and risk difference, respectively. Data extracted from the included studies were pooled for meta-analysis using RevMan, version 5.3.5, software (Nordic Cochrane Centre, Copenhagen, Denmark), and forest plots were extracted. A P value of <.05 was considered statistically significant, and CIs were set at 95%. χ2 test was used to identify heterogeneity. Heterogeneity size was formally determined with I2, wherein I2 of 0% to 25%, 25% to 75%, and greater than 75% were considered as low, moderate, and high heterogeneities, respectively. A random effects model was applied in studies with high heterogeneity (I2 >75%), whereas a fixed effects model was used when there was low or moderate heterogeneity.
Outcome Measures
The outcome measures, which were consistently reported for analysis, were shoe fitting problems, residual pain, failure to return to activity (RTA), American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, complications, and development of arthritis. Other outcome parameters, such as visual analog scale, quality of life EQ5D, change in calcaneal height, change in the Böhler angle, and Kerr-Atkins score, reported sporadically in various studies were noted; however, we were unable to include these in our meta-analysis owing to inconsistent reporting.
Results
Literature Search Results
Our initial search, which included Medline, Embase, and Cochrane databases, retrieved 491 articles. After the removal of duplicates, 295 articles remained. Subsequently, all noncomparative studies were excluded, leaving 31 articles that were screened against the eligibility criteria. Finally, 13 studies were deemed suitable after excluding 18 studies that failed to meet the inclusion criteria. We have demonstrated this process in a PRISMA flow diagram (Figure 1).
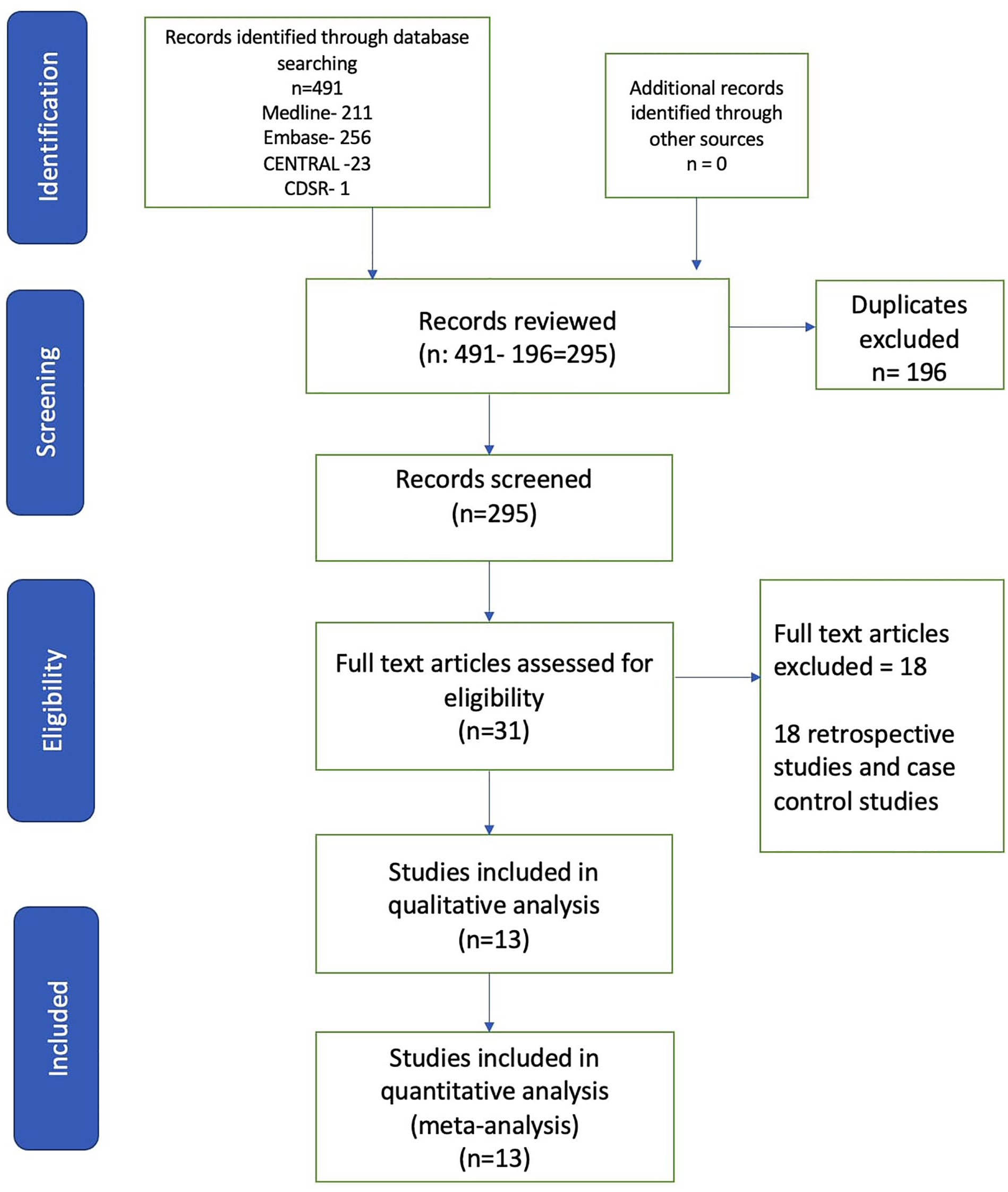
PRISMA flowchart for the meta-analysis.
Study Characteristics and Patient Population
The 13 studies (Table 1) included 1251 patients, of which 626 patients were nonoperatively treated and 625 underwent operative treatment. Ten studies were RCTs,1,3,4,6,7,9,17,19,23,24 and 3 were prospective studies.10,18,20 Sanders classification was the most commonly agreed method to classify intraarticular calcaneal fractures in the included studies. Most of these injuries occurred in the middle age group (28-58 years)1,3,4,6,7,9,10,17-20,23,24 and showed a male preponderance. Complications were reported in in 8 studies, development of arthritis in 7 studies, residual pain in 5 studies, failure to RTA in 5 studies, AOFAS score in 5 studies, and shoe fitting problems in 5 studies. The mean follow-up period in the included studies was 4.1 years.
Quality Assessment
RCTs included in the study were assessed for quality by 2 authors (using the Cochrane Handbook for Systematic Reviews and Interventions tool). The RCTs were assessed on parameters, including randomization, allocation concealment, blinding of participants and outcome assessment, incomplete outcome data, selective outcome reporting, and other biases. Most of the RCTs in the meta-analysis had a low risk of bias for all the parameters except for blinding of participants and personal bias. The risk of bias graph and risk of bias summary are presented in Figures 2 and 3, respectively. The included prospective comparative studies were assessed for quality using the Newcastle-Ottawa Scale with a subjective score out of 9. Selection criteria, comparability, and outcomes were the parameters assessed. All the included prospective studies scored above 6 and were of good quality (Table 2).

A figure displaying the risk of bias for the randomized controlled trials included in the meta-analysis. Each color represents the risk of bias in each of the domains (red = high risk, yellow = unclear, and green = low risk).

A figure displaying the risk of bias for each of the included randomized controlled trials. The color represents the quality in the each of the domains (red = high risk, yellow = uncertain, and green = low risk).
Newcastle Ottawa Score for the Included Prospective Studies.

Outcomes
Shoe fitting problems
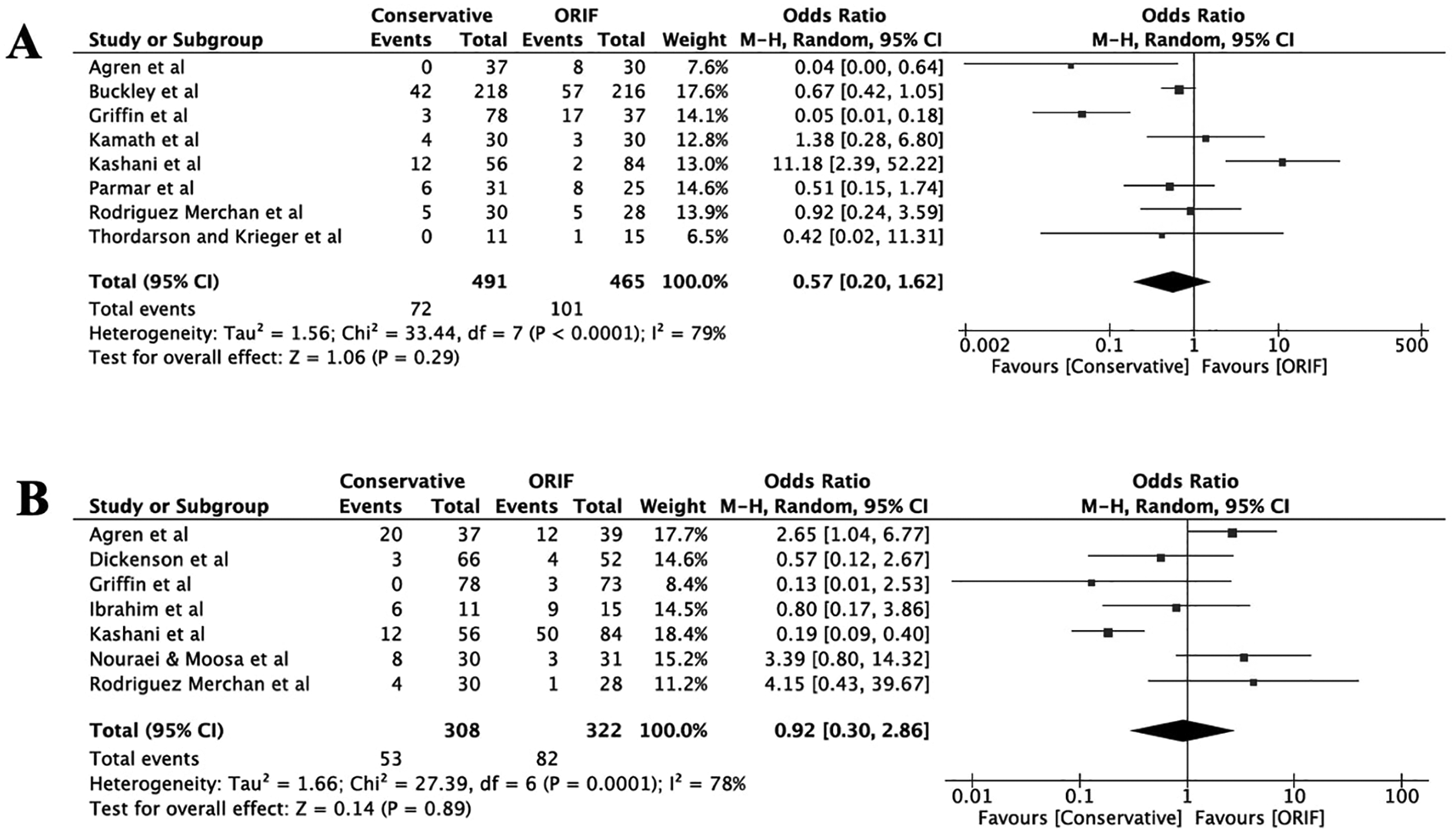
Shoe fitting problems were reported in 5 studies, which included 285 patients, and the results favored the operative treatment for DIACF. There was moderate heterogeneity (I2 = 67%); therefore, a fixed effects model was used (Figure 4A).

Forest plots showing the comparison of (A) shoe fitting problems and (B) failure to return to activity between the 2 groups. (IV, independent variable; M-H, Mantel-Haenszel.)
Failure to RTA
Failure to RTA was reported in 5 studies, which included 245 patients, and the results favored the operative group (Figure 4B).
AOFAS score
The AOFAS score was reported in 5 studies, which included 340 patients. No statistically significant difference between the groups was noted (Figure 5A).

Forest plots showing the comparison of (A) AOFAS score and (B) residual pain between the 2 groups. (AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot score; IV, independent variable; M-H, Mantel-Haenszel.)
Residual pain
Residual pain was reported in 5 studies, which included 263 patients. The results were not in favor of any of the treatment options (Figure 5B).
Complications
Complications were reported in 8 studies, which included 956 patients, with no statistically significant difference between the 2 groups (Figure 6A).
Forest plots showing the comparison of (A) complications and (B) development of arthritis between the 2 groups. (IV, independent variable; M-H, Mantel-Haenszel.)
Arthritis
Development of arthritis was reported in 7 studies, which included 630 patients. The results did not favor any of the treatment options (Figure 6B).
Sensitivity Analysis
A sensitivity analysis was performed on all the comparison results. No change was observed in the results of residual pain and development of arthritis when individual studies were removed. The AOFAS score favored the ORIF group when Ibrahim et al’s study 9 was removed; however, the study was well conducted and demonstrated a low risk of bias in the quality assessment. Therefore, no good reason was noted to exclude it from the results. Complications demonstrated a statistically significant result, favoring the conservative treatment when Bahari Kashani et al’s study 3 was removed. A meticulous assessment was conducted on the methodology of the aforementioned study, and a consensus was made to retain it. When Griffin et al’s study 7 was removed, failure to return to preinjury work displayed no difference in either treatment option. A careful analysis was performed, and the study showed a very low risk of bias; therefore, the study remained included in the statistical analysis. The results of shoe fitting problems become insignificant for any of the treatment options when Nouraei and Moosa’s, 17 O’farrell et al’s, 18 and Thordarsen et al’s 24 studies were individually removed. A thorough evaluation was performed, and all the aforementioned studies displayed good quality criteria.
Discussion
In the present analysis, operative treatment may be superior to conservative management of DIACF on certain occasions. Shoe fitting problems were overall lower in the operatively treated patients, and most of the patients returned to their preinjury work or activity. The AOFAS score, despite slightly favoring operative management, did not show a statistically significant difference. Residual pain, development of arthritis, and complications in the form of skin problems or nerve palsy did not specifically favor any of the treatment options.
The mainstay of the operative management of DIACF is to achieve anatomical reduction, correct varus malalignment, and provide stable fixation. Despite best efforts, there is still little understanding of other factors that could influence the outcomes.4,14 Patient demographics, soft tissue handling, fixation method, bone graft use, immobilization duration, and rehabilitation protocol could have underestimated influential roles on the final outcome.4,14
Shoe fitting problems appeared to be less in the operatively treated patients, perhaps because varus malalignment correction is an integral step of any operative technique for treating these injuries. 24 O’Farrell et al 18 suggested that better outcomes in operatively treated patients are due to anatomical reduction and early mobilization. This was reinforced by Thordarson and Krieger 24 who demonstrated better functional and radiologic outcomes for the operative cohort.
Buckley et al 4 emphasized the significance of treatment individualization based on patient demographics and fracture patterns. They concluded similar clinical outcomes in both groups as a whole; however, they found variations in the clinical outcomes in certain subgroups. Their results displayed better outcomes for the operative group in certain fracture patterns, such as fractures with large Böhler angles. Moreover, they established particular patient factors that made a statistically significant preponderance toward the operative management, such as fractures in females, young age, and patients not receiving worker’s compensation. In addition, further studies have reported better functional outcomes for the operative treatment of fracture patterns causing fibular impingement.6,7
Conversely, the factors that displayed a statistically significant association with poor outcomes when operatively treated were those resulting from high-energy mechanisms, those associated with comminution or small Böhler angle, severe associated injuries, fracture blisters, delayed presentation, patients with preinjury heavy workload, in receipt of worker’s compensation, smoking, alcoholism, diabetes mellitus, peripheral vascular disease, and high body mass index.4,14
Bahari Kashani et al 3 examined peroneal tenosynovitis as a primary outcome parameter between operative and nonoperative management. They found a statistically significant difference, favoring the operative management. Peroneal tenosynovitis has been observed by other studies to occur more in fractures with fibular impingement and significant lateral comminution, highlighting the significance of subdividing these fractures and not taking them collectively.
Advocates of the conservative management of DIACF postulate that the pain associated with these injures arises not only from the bone displacement but also from the soft tissue injury occurring at the time of the initial trauma.1,9,10,19 Furthermore, the late development of arthritis is believed to be due to cartilage necrosis at the time of injury, which may affect the outcomes despite the best operative anatomical reduction. 13 The extensile lateral approach to the calcaneus has also been traditionally known for its wound breakdown and/or infection. 22 However, the incidence of complications, such as skin problems or nerve palsy, was not significantly higher in the operative group in this analysis. Dickenson et al 6 reported the long-term outcomes of the UK Heel Fracture (HeFT) trial for DIACF management. They reported an increase in the reoperation rate in the operative group. However, the particular outcome was not consistently reported in other studies; therefore, no robust conclusions could be drawn.
This study is partially in agreement with the most recent meta-analysis conducted by Wei et al 26 who concluded better functional and radiologic outcomes for the operatively treated group. However, the strength of this study lies in the involvement of only RCTs and prospective trials that provide level I and II evidence for DIACF management.
Meena et al 14 conducted a meta-analysis comparing operative and nonoperative management of intraarticular calcaneal fractures. They reported a higher rate of return to work in the operatively treated group, but on the expense of increased complications rate. Although, they included RCTs only in their analysis, this study could be criticized for the small sample size and certain outcomes were concluded from as low as 2 studies. The result of Jiang et al 11 meta-analysis is quite similar to Meena et al 14 findings; however, the former involved RCTs in addition to case-controlled trials.
The current study has, nonetheless, some limitations. First, various patterns of intraarticular calcaneal fractures, degree of varus malalignment, and fibular impingement were not specifically compared across the various studies. Second, the follow-up periods were as low as 1 year in some studies and up to 15 years in others, making the comparison between functional outcomes challenging. Third, certain outcomes were not consistently compared across all studies. Fourth, radiologic outcomes were not used in our analysis owing to inconsistent reporting. The change in the Böhler angle was, for example, reported only in 2 of the involved studies with 56 patients. This was insufficient to draw robust conclusions on this perspective.
Conclusion
DIACF management should be individualized, and operative treatment has to be reserved for selected cases with certain patient factors and fracture patterns. Poor outcomes have been associated with the operative treatment in patients with diabetes mellitus, peripheral vascular disease, high body mass index, smoking habit, alcoholism, delayed presentation, fracture blisters, and severe associated injuries. Fracture patterns with fibular impingement, significant lateral comminution, and large Böhler angle show better outcomes with the operative treatment. Further high-quality RCTs comparing specific calcaneal fracture subgroups and highlighting the role of various surgical techniques and rehabilitation protocols are required.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221101609 – Supplemental material for Systematic Review of Operative vs Nonoperative Treatment of Displaced Intraarticular Calcaneal Fractures
Supplemental material, sj-pdf-1-fao-10.1177_24730114221101609 for Systematic Review of Operative vs Nonoperative Treatment of Displaced Intraarticular Calcaneal Fractures by Amr Selim, Nikhil Ponugoti and Suresh Chandrashekar in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because all the data were available and previously published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.