
Abstract

Introduction
Infection of the tuber calcanei1,5,7,9 is a debilitating problem, with below-knee amputation or subtotal or complete calcanectomy being widely accepted treatment options. Several bone-sparing treatment options exist. However, they offer limited infection control. Moreover, the psychological burden of long-term hospitalizations and intravenous antibiotic treatment make such treatments unsuitable for many patients. Four main surgical approaches are described for treating tuber calcanei infection1 -3,5,7: anterior, lateral, medial, and posterior. In the anterior approach, the posterior facet of the subtalar joint is elevated, effectively gaining access through the sinus tarsi; such an approach would require heavy fixation, making it less favorable in the presence of infection. In the lateral approach, protection of the sural nerve and peroneal tendons is critical. The medial approach goes through the tarsal tunnel; hence, protection of the posterior tibialis nerve and its branches is needed along with the tibialis posterior, flexor digitorum longus, and flexor hallucis longus tendons. A posterior approach using heel soft tissue splitting originally described by Gaenslen 2 effectively protects the anatomical structures discussed above, allowing the needed exposure for complete debridement of the infected tissue. In recent years there have been several reports on this approach to treat calcaneal ulcers,1,4 with good results. However, to our knowledge, to date, there are no reports of Gaenslen’s approach combined with a wedge calcaneal osteotomy to salvage infected heels in patients with diabetes.
Technique
Indications
We report the successful treatment of 6 patients with tuber-calcanei pathology using a thin wedge- or “saber”-shaped cut modification of Gaenslen’s 2 approach. Patients were between 45 and 70 years old, with a relevant medical history of type 2 diabetes mellites with a hemoglobin A1c range of 8% to 10%. The patients all failed a minimum of 3 months of nonoperative treatment, including surgical ulcer debridement, antibiotic treatment (intravenous/oral), and hyperbaric chamber oxygenation. The patients were sent for a vascular surgeon consultation to determine if vascular intervention is needed before the surgery and confirm sufficient perfusion (ankle-brachial index > 0.75) for wound healing before surgery.
Operative Technique
Patients are positioned prone on the surgical table with a pneumatic tourniquet around the thigh and ankle support. As per Gaenslen, 2 the posterior approach begins with a midcalcaneal incision with a mid-Achilles extension, as shown in Figure 1A. After sufficient calcaneal exposure, we perform a wedge osteotomy of the tuber calcanei, as shown in Figure 1B. Two osteotomes protect the surrounding structures and soft tissue during the osteotomy. The first is inserted into the lateral half of the tuber immediately posterior to the posterior facet. The second osteotome is placed beneath the posterior subtalar facet to protect the upper limit of the osteotomy. We remove the infected bone segment and debride the soft tissue, and all specimens are cultured and sent for pathologic examination, as shown in Figure 2. The histology report demonstrated infection involving all layers of soft tissue and underlying bone in all cases. After removing the infected slice and reaching what appear to be clean margins, the bone fragments are fixed and compressed using nonradiopaque magnesium-based screws (Figure 3). The putative advantage of these screws is that part of the degradation process releases hydrogen gas (H2), forming magnesium hydroxide (Mg(OH)2) when reacting with magnesium, allowing for reduction of the inflammatory process, much like other biodegradable polymers.6,8 Before wound closure, bioactive glass “Bonalive" is inserted into the surgical wound, reducing the microbial load by 2 mechanisms. The first is through the release of sodium (Na+) from the surface of the bioactive glass, which induces an increase in pH, effectively creating an alkaline environment. 3 The second is through the rise in osmotic pressure due to elevation in salt concentration (Na+, Ca+2, and Si+ ion release). The incision is closed using 0/3 nylon sutures or staples and dressed in Inadine and gauze pads.
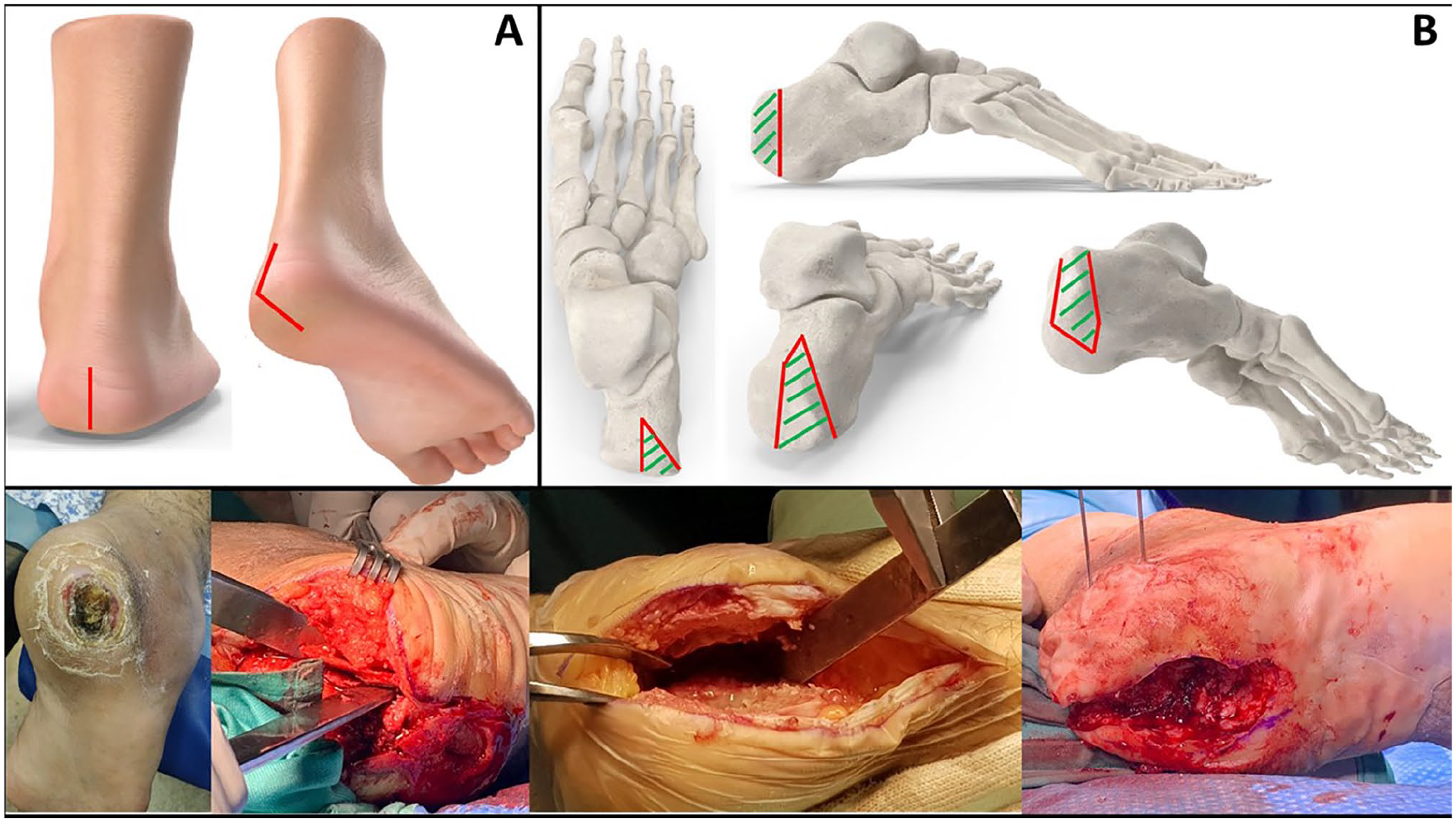
(A) A posterior and plantar oblique view of a foot diagram with a red line marking the incision. (B) Four views of the calcaneus with red lines marking our osteotomy and green lines representing the infected wedge removed. Bottom: intraoperative clinical pictures showing an infected wound before removal, and 3 different surgical cases.

(A) Infected specimen removed from the calcaneus. (B) A slide demonstrating chronic inflammation in all layers of soft tissue and bone. (C) A slice demonstrating chronic osteomyelitis affecting bone fragments.

Radiographs of 2 patients A and B showing lateral and Harris calcaneal views postoperation and 18 months postoperation showing good healing of the osteotomy site with no evidence of infection in both patients.
Postoperative Follow-up
Following surgery, patients remain hospitalized for several days with intravenous antibiotic treatment through a peripherally inserted central catheter line, after which they are discharged for outpatient follow-up with no weight-bearing allowed. The first follow-up visit is scheduled 3 weeks following surgery, at which time we inspect the surgical wound and remove the sutures. Blood work was reviewed (specifically white blood cell count and C-reactive protein) and demonstrated a decrease in infection and inflammation markers in all cases. The patient is discharged with a total contact cast until the next follow-up visit, at which time they complete a 6-week course of intravenous antibiotics on a home therapy basis. At the 3- and 6-month follow-ups, all patients demonstrated clinical and radiologic eradication of the infection and good surgical site healing with no weightbearing restrictions, as shown in Figures 3 and 4B.

Two different patients following the saber cut modification of Gaenslen’s approach procedure: (A) one case 6 weeks postoperation with partially open wound without signs of infection; (B) surgical scar 6 months postoperation demonstrating good wound healing and full weightbearing.
Discussion
Infection of the tuber calcanei is a debilitating disease needing thorough surgical treatment and often leading to limb amputation.1,4,5,7 We present the advantages and pitfalls of different surgical approaches and describe a novel saber cut approach as a modification to Gaenslen’s approach, which to our knowledge has not been reported to treat tuber calcanei infection in patients with diabetes. Of the 6 patients treated thus far, all have successfully eradicated the infection without sacrificing foot stability. All patients have shown good surgical site healing, returning to full weightbearing within 1-2 months after the operation (Figure 4B). We encountered 1 delayed wound closure without active infection at 6 weeks postoperation (Figure 4A), and we decided to maintain the patient as nonweightbearing until secondary wound closure at 3 months postoperation. With all the above in mind, we believe that this novel saber cut modification of Gaenslen’s approach may allow the successful treatment of patients who would otherwise have lost the infected limb.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221099023 – Supplemental material for Tuber Calcanei Osteomyelitis Eradication via Modified Gaenslen’s Approach
Supplemental material, sj-pdf-1-fao-10.1177_24730114221099023 for Tuber Calcanei Osteomyelitis Eradication via Modified Gaenslen’s Approach by Ariel D. Levine, Claude Picard, Michael Alperson, Majd F. Sirhan, Oren Ben Lulu and Aharon Liberson in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.