
Abstract
Background:
Magnetic resonance imaging (MRI) is commonly used for evaluation of ankle cartilage repair, yet its association with clinical outcome is controversial. This study analyzes the correlation between MRI and clinical outcome after cartilage repair of the talus including bone marrow stimulation, cell-based techniques, as well as restoration with allo- or autografting.
Methods:
A systematic search was performed in MEDLINE, Embase, and Cochrane Collaboration. Articles were screened for correlation of MRI and clinical outcome. Guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) were used. Chi-square test and regression analysis were performed to identify variables that determine correlation between clinical and radiologic outcome.
Results:
Of 2687 articles, a total of 43 studies (total 1212 cases) were included with a mean Coleman score of 57 (range, 33-70). Overall, 93% were case series, and 5% were retrospective and 2% prospective cohort studies. Associations between clinical outcome and ≥1 imaging variable were found in 21 studies (49%). Of 24 studies (56%) using the composite magnetic resonance observation of cartilage repair tissue (MOCART) score, 7 (29%) reported a correlation of the composite score with clinical outcome. Defect fill was associated with clinical outcome in 5 studies (12%), and 5 studies (50%) reported a correlation of T2 mapping and clinical outcome. Advanced age, shorter follow-up, and larger study size were associated with established correlation between clinical and radiographic outcome (P = .021, P = .028, and P = .033).
Conclusion:
Interpreting MRI in prediction of clinical outcome in ankle cartilage repair remains challenging; however, it seems to hold some value in reflecting clinical outcome in patients with advanced age and/or at a shorter follow-up. Yet, further research is warranted to optimize postoperative MRI protocols and assessments allowing for a more comprehensive repair tissue evaluation, which eventually reflect clinical outcome in patients after cartilage repair of the ankle.
Keywords
Introduction
The necessity of treating symptomatic articular cartilage defects in orthopaedic surgery has been increasingly recognized worldwide, with the development of several cartilage repair techniques in recent years. To assess postoperative repair tissue formation, magnetic resonance imaging (MRI) is frequently used to assess the structural integrity of both cartilage defects and repair tissue.24,45,51,57,60,65,68,73,88
As described by Hayashi et al, 39 the commonly used 2-dimensional and the more advanced isotropic 3-dimensional MRI sequences can be used to evaluate the morphology of cartilage repair. Other MRI sequences like Spoiled Gradient Recoiled Echo are excellent for cartilage segmentation and quantification of cartilage volume but are often of limited utility in the postoperative setting. In many cases, appropriate metal artifact reduction sequences are necessary (eg, after medial malleolar osteotomy), which further reduce the quality of imaging. 38 Compositional MRI acquisitions like T1rho, T2 mapping, and delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) provide a way to detect biochemical and microstructural changes within the cartilage layer. Quantitative MRI sequences have the potential for tissue characterization after reparative and regenerative surgical treatment of osteochondral lesions of the talus (OLTs). 69 Nevertheless, the correlation between radiologic and clinical outcome is still an ongoing debate among the orthopaedic community.24,40,41,57,67,78
In 2017, leading experts in cartilage repair of the ankle gathered in Pittsburgh for the 1st International Consensus Meeting on Cartilage Repair of the Ankle. Among the published manuscripts from this meeting, van Dijk et al 85 reported that routine MRI is not indicated in the follow-up after cartilage repair because evidence of correlation between clinical outcome and posttreatment imaging is lacking. Thus, the consensus recommended that postoperative imaging should be considered in patients with a mechanical cause for symptoms (eg, loose body or chondral flap). Although information about postoperative imaging in the setting of cartilage repair in the knee has been studied in a systematic review, there is a paucity of comprehensive data in cartilage repair of the ankle. 28 Hence, the purpose of this work is to evaluate the correlation between MRI and clinical outcome after articular cartilage repair of the talus and to identify parameters that associate imaging and clinical outcome.
Methods
A systematic literature review was performed on MRI after articular cartilage repair of the talus. Included cartilage repair techniques ranged from bone marrow stimulation procedures (MS) over cell-based cartilage transplantation (CB) to cartilage restoration techniques. Data from individual articles were analyzed to determine the correlation between MRI parameters and clinical outcome. The search was conducted on October 12, 2020, in the electronic databases of MEDLINE, Embase, and the Cochrane Collaboration using the following parameters: (cartilage repair OR cartilage restoration OR autologous chondrocyte implantation OR autologous chondrocyte transplantation OR matrix-assisted autologous chondrocyte transplantation OR matrix-induced autologous chondrocyte implantation OR MACT OR MACI OR characterized chondrocyte implantation OR autologous osteochondral transplantation OR osteochondral autologous transplantation OR OATS OR osteochondral autograft transplantation OR OCT OR mosaicplasty OR osteochondral allograft transplantation OR OCA OR microfracture OR microfracturing OR autologous matrix-induced chondrogenesis OR AMIC OR Chondro-Gide OR Chondrogide OR particulated juvenile cartilage allograft transplantation OR PJCAT) AND (magnetic resonance imaging OR MRI OR delayed gadolinium enhanced OR dGEMRIC OR T2 mapping OR T2 index OR radiologic OR radiological OR radiographic) AND (talus OR ankle OR talar). Two independent reviewers screened all articles by title and abstract and applied the following inclusion criteria: therapeutic or diagnostic studies of cartilage repair, minimal follow-up of 12 months, clinical assessment, postoperative imaging evaluation with MRI, full text available in English or German. Exclusion criteria were case reports, animal and cadaver studies, etiologic studies, osteoarthritis, and unavailable full texts in English or German. All references of systematic reviews were evaluated for inclusion. All included articles were assessed for established correlation analysis between clinical and imaging outcome.
The guidelines for Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) were used, 61 and the protocol was registered on PROSPERO database (reg. no. CRD42021232791). 16 The quality of each study was assessed regarding selection bias (patient selection and homogeneity), attrition bias (analysis based on the availability of MRI parameters), detection bias (blinding and independence of MRI observer(s)), and reporting bias (selective reporting of correlation results). The Coleman Methodology score 25 modified by Ramponi et al 66 was used to assess the quality of the methodology. Extracted data from the selected studies included patient demographics, sample sizes, surgical procedure(s), MRI techniques and scores, defect sizes, and clinical outcome scores along with correlation statistics. The primary outcome of this study was to assess established correlations between postoperative MRI and clinical outcome in patients after cartilage repair of the ankle with the secondary aim to identify parameters that associate imaging and clinical outcome.
Statistical Analysis
All statistical analyses were performed in SPSS for Mac (version 23.0, SPSS Inc, Chicago, IL). For meta-analysis, all studies were stratified into 2 groups based on either presence or absence of correlation between postoperative imaging parameters and clinical outcome. The chi-square test and point-biserial analysis were applied to identify variables that determine established associations between imaging and clinical outcome. Following variables were included in the analysis: level of evidence, Coleman score, use of the composite magnetic resonance observation of cartilage repair tissue (MOCART) score, use of T2 mapping, subchondral assessment, cartilage repair technique (MS, CB, cartilage restoration), study size, patient age, defect size, and follow-up time. Correlation analyses that were not performed or Pearson coefficients that could not be obtained were classified as not applicable (NA). Significance was set at P < .05.
Results
A literature search in MEDLINE resulted in 2103 articles, in Embase in 554 articles and in Cochrane in 30 articles. After removal of 318 duplicates, 2369 articles remained for screening. Following the application of the inclusion and exclusion criteria, 43 articles were finally included in the review and meta-analysis (Figure 1).
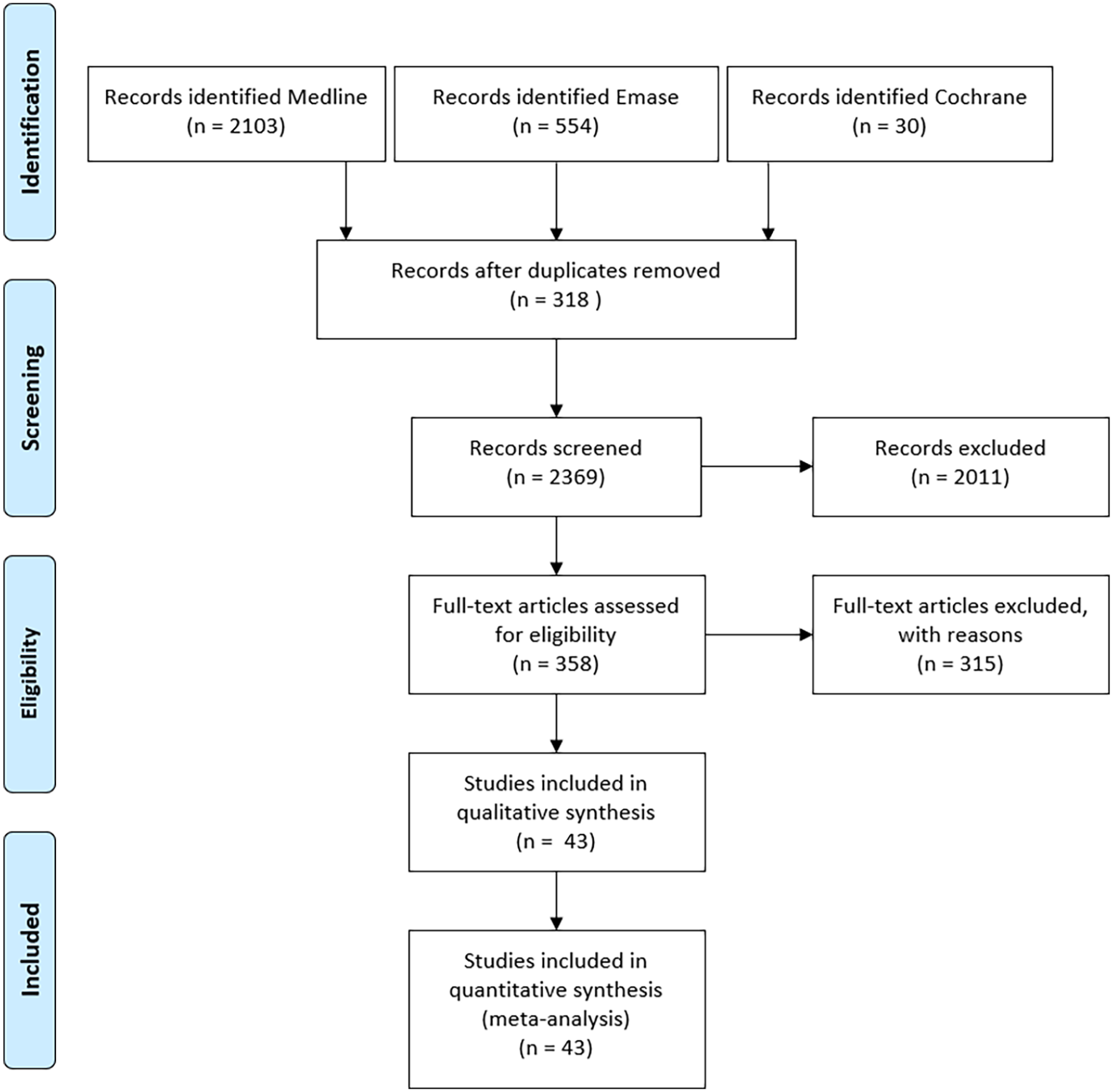
Flowchart of the literature search. 61
Of these, the majority (93%) were case series, 5% retrospective and 2% prospective cohort studies. Besides standardized MRI techniques, T2 mapping was used in 23% and diffusion weight imaging (DWI) in 7% of studies. Procedures were classified in bone marrow stimulation (MS) including microfracture (MF) or autologous matrix induced chondrogenesis (AMIC), cell-based techniques (CB), namely, autologous chondrocyte implantation, and cartilage restoration comprising osteochondral auto- and allograft transplantation. MS was performed in 58% (n = 25), CB in 21% (n = 9), cartilage restoration in 19% (n = 8), and a combination (cohort studies) in 2% (n = 1) of the studies (Table 1).
Study and Patient Characteristics.
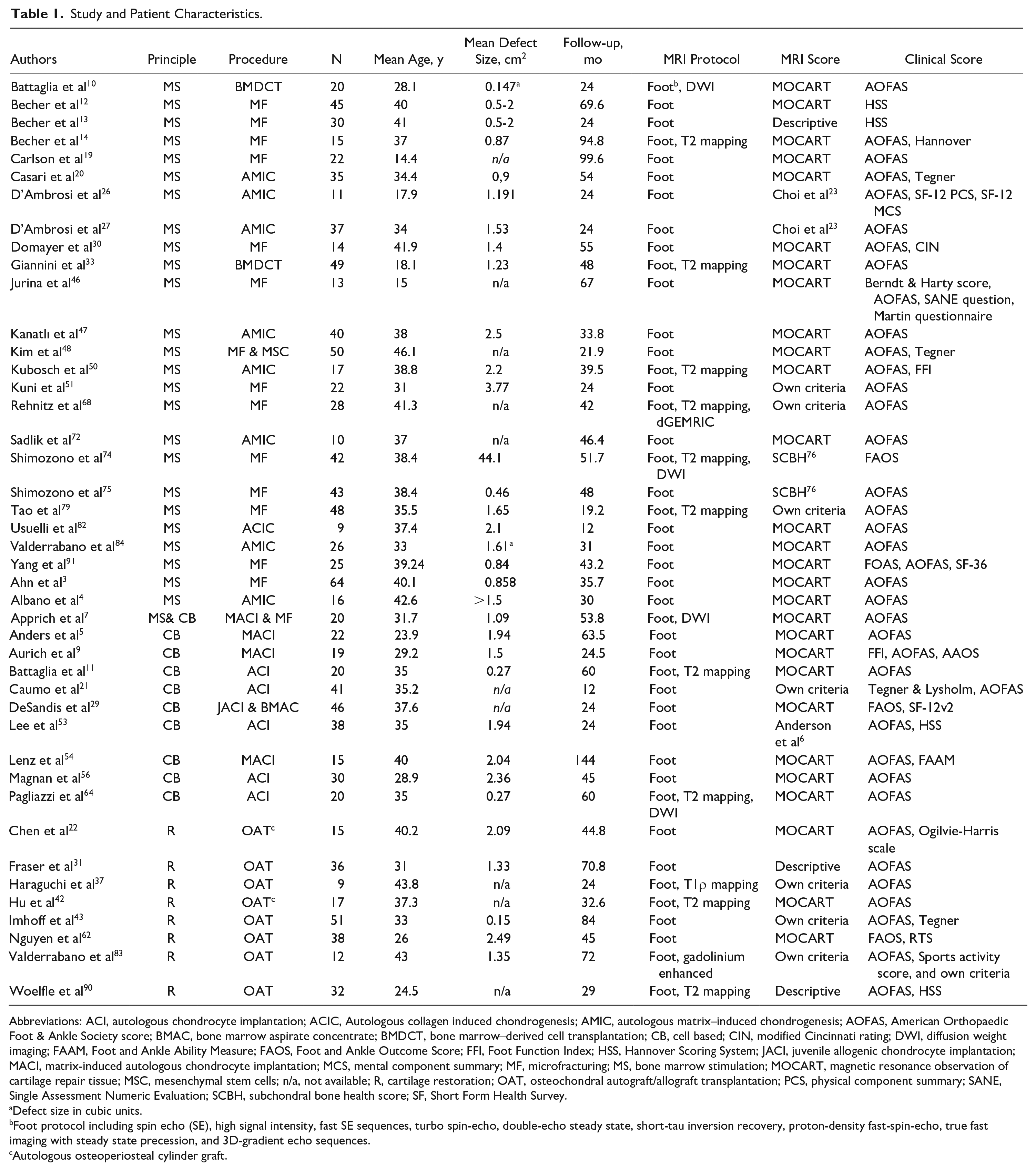
Abbreviations: ACI, autologous chondrocyte implantation; ACIC, Autologous collagen induced chondrogenesis; AMIC, autologous matrix–induced chondrogenesis; AOFAS, American Orthopaedic Foot & Ankle Society score; BMAC, bone marrow aspirate concentrate; BMDCT, bone marrow–derived cell transplantation; CB, cell based; CIN, modified Cincinnati rating; DWI, diffusion weight imaging; FAAM, Foot and Ankle Ability Measure; FAOS, Foot and Ankle Outcome Score; FFI, Foot Function Index; HSS, Hannover Scoring System; JACI, juvenile allogenic chondrocyte implantation; MACI, matrix-induced autologous chondrocyte implantation; MCS, mental component summary; MF, microfracturing; MS, bone marrow stimulation; MOCART, magnetic resonance observation of cartilage repair tissue; MSC, mesenchymal stem cells; n/a, not available; R, cartilage restoration; OAT, osteochondral autograft/allograft transplantation; PCS, physical component summary; SANE, Single Assessment Numeric Evaluation; SCBH, subchondral bone health score; SF, Short Form Health Survey.
Defect size in cubic units.
Foot protocol including spin echo (SE), high signal intensity, fast SE sequences, turbo spin-echo, double-echo steady state, short-tau inversion recovery, proton-density fast-spin-echo, true fast imaging with steady state precession, and 3D-gradient echo sequences.
Autologous osteoperiosteal cylinder graft.
The MOCART score 57 was utilized in 28 studies (65%), 10 (23%) used their own defined criteria or only descriptive measures, 2 (5%) the Subchondral Bone Health (SCHB) Score, 74 2 (5%) the Choi classification, 23 and the Anderson’s modified MRI-based classification system 6 was applied once (2%), which also evaluated the Mintz cartilage grading system. 60 Further, 9 studies (21%) assessed postoperative imaging with T2 mapping, 1 (2%) T1ρ mapping, and 1 (2%) dGMERIC.
Regarding clinical outcome, the American Orthopaedic Foot & Ankle Society (AOFAS) score 49 was the most commonly evaluated functional clinical score, with its application in 88% of studies, whereas other scores like the Foot and Ankle Outcome Score (FAOS), 70 Tegner activity scale, 80 Short Form Health Survey (SF-24, SF-36),17,87 Foot Function Index (FFI), 18 and Hannover Scoring System (HSS) 81 were used in a minority of studies.
Methodologic assessment resulted in moderate overall risk of bias with a mean modified Coleman score of 57 (range, 33-70). Although selection bias could not be ruled out in 64% of the included studies, potential detection and attrition bias were found in 22% and 44%, respectively. Risk for reporting bias was low, with only 7% of all studies. Three Level IIb to IIb (Coleman score range, 61-66) and 40 Level IV (Coleman score range, 33-70) studies were included. Detailed study quality assessment can be found in Table 2.
Study Quality.
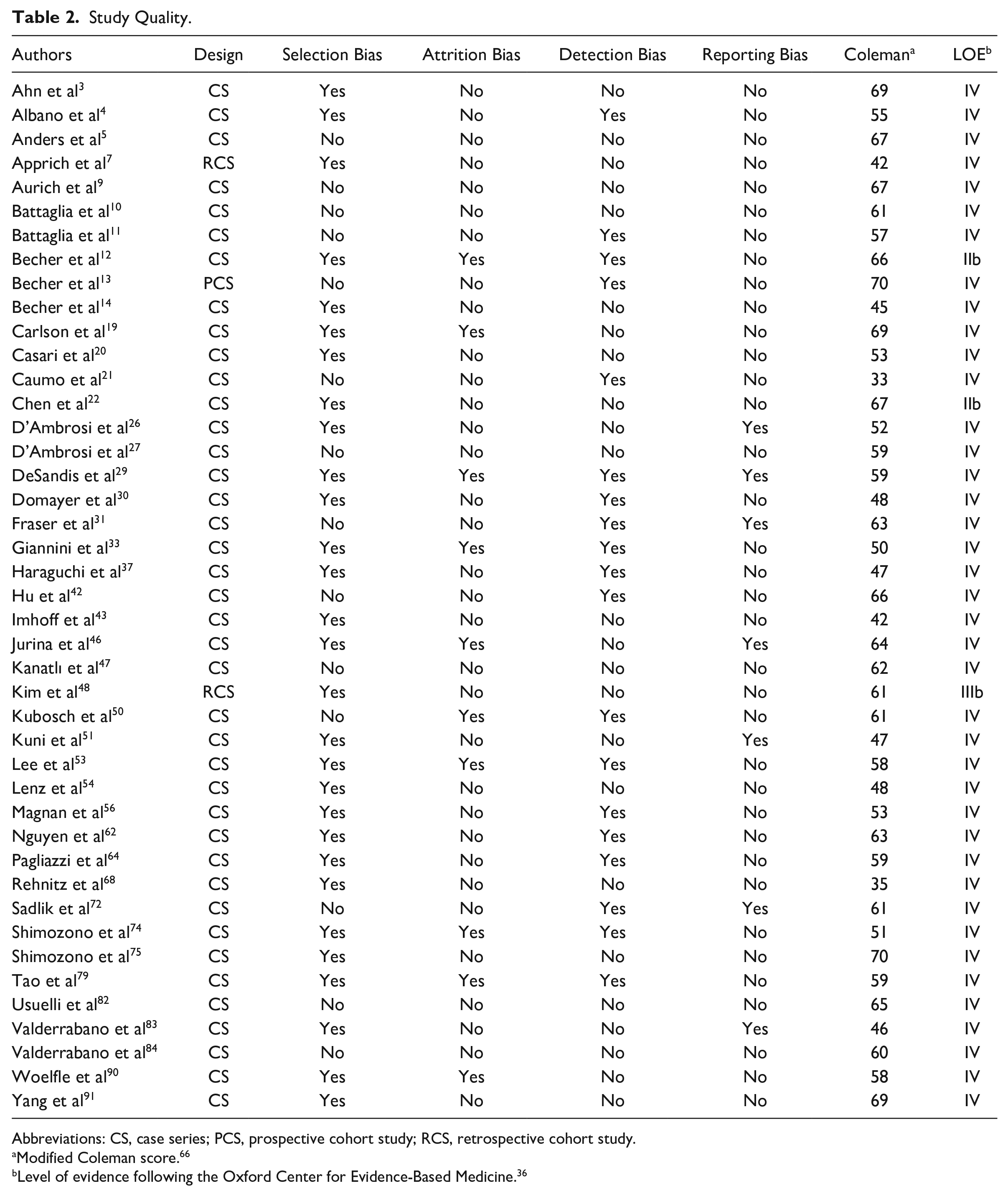
Abbreviations: CS, case series; PCS, prospective cohort study; RCS, retrospective cohort study.
Modified Coleman score. 66
Level of evidence following the Oxford Center for Evidence-Based Medicine. 36
To evaluate the correlation between clinical and radiological outcome, the majority (n = 28; 65%) used the Spearman rank coefficient or the Pearson correlation coefficient. Magnan et al, 56 Woelfle et al, 90 and Imhoff et al 43 performed parametric or nonparametric statistical hypothesis tests, and D’Ambrosi et al 26 used a multivariant correlation analysis. Rhenitz et al 68 and Nguyen et al 62 both utilized a receiver operating characteristic analysis. There was no clear specification of the statistical analysis in 12% of the included studies. Correlation coefficients could be calculated in n = 5 studies (12%), because detailed case descriptions were available of all included patients.
Of the included 43 studies, a correlation between 1 or more imaging variables and clinical outcome was found in 21 (49%) articles (Table 3). Of the 24 studies (56%) utilizing the composite MOCART score, 7 (29%) reported a correlation with clinical outcome. Five of 13 studies (39%) evaluating the correlation of defect fill and clinical outcome showed an association.9,21,47,64,79 Of all 10 studies evaluating the correlation between T mapping and clinical outcome, 5 (50%, 4 × T2, 1 × T1ρ) showed a correlation.8,11,26,37.51,55,64,68,79 The correlation of diffusion-weighted imaging (DWI) and clinical outcome was shown in none of the 3 (0%) included studies.
Correlations Between the MRI and Clinical Outcome Scores. a

Abbreviations: LOE, level of evidence; MOCART, magnetic resonance observation of cartilage repair tissue; SCBH, subchondral bone health score.
Numbers provided represent exact correlation coefficients; if no coefficients were given, “yes” or “no” was used to indicate that articles found or did not find a correlation between radiologic and clinical outcome, respectively. –, not applicable.
P value unavailable.
P < .05.
P < .01.
Analyzing the metadata, advanced age, shorter follow-up, and study sample size were associated with established correlation between clinical and radiographic outcome (r = 0.367, P = .021; r = −0.335, P = .028; and r = 0.326, P = .033, respectively). None of the other assessed variables showed significant influence on the relationship of MRI and clinical outcome.
Bone Marrow Stimulation
Most studies assessing MS (n=26) evaluated correlation of imaging and clinical outcome after MF (54%; n=14) or a combination of MF with spongiosa, cell-free scaffold, or mesenchymal stem cells (15%; n=4). Other techniques used were AMIC (19%; n=5), bone marrow–derived cell transplantation (BMDCT) (8%; n=2) or autologous collagen-induced chondrogenesis (ACIC) (4%; n=1). Patients were treated at a mean age of 34 (range 14-46) years of age for cartilage defect and evaluated after a follow-up of 43 (range 12-100) months after the cartilage repair. Fifteen of 26 studies (58%) reported 1 or more significant correlations between clinical outcome and imaging parameters. Three studies found a correlation of the composite MOCART score and clinical outcome.48,50,91 Four studies reported a correlation of the subgroups of the MOCART score. Kanatli et al 47 noted that filling of the defect is significantly correlated with outcome, Battaglia et al 10 reported a correlation of the signal of the repair and Ahn et al 3 of the subchondral bone marrow edema (BME) volume with clinical outcomes. Apart from the studies evaluating the MOCART score, BME was associated with inferior outcome in 3 studies,51,75,79 and Shimozono et al 74 reported a correlation of the subchondral bone health score (SCBH) and clinical outcome. Although Becher et al 12 found a correlation between clinical outcome and effusion, D’Ambrosi et al 26 stated that the Choi score on CT was correlated with clinical outcome, yet reported nonsignificance for MRI scores. A positive correlation of clinical outcome and T2 mapping was found in 3 studies.10,68,79
Cell-Based Techniques
Of the 10 studies evaluating CB, 9 studies (90%) investigated the correlation of ACI and 1 (10%) of juvenile articular cartilage allograft with clinical outcome. Patients were treated at a mean age of 33 years (range 24-40) for OLT and evaluated after a follow-up of 51 months (range 12-144). Four of 10 studies (40%) reported 1 or more significant correlations. DeSandis et al 29 reported a correlation of the composite MOCART score and clinical outcome and Aurich et al 9 as well as Pagliazzi et al 64 found a correlation with the subscore defect filling. Caumo et al 21 reported in a descriptive classification that filling, integration, and subchondral signals were correlated with clinical outcome. Additionally, Pagliazzi et al 64 noted a significant association between T2 mapping and clinical outcome.
Cartilage Restoration Techniques
Eight studies evaluated the correlation after cartilage restoration, of which 6 (75%) used OAT and 2 (25%) osteoperiosteal cylinder. Patients were treated at a mean age of 35 years (range 25-44) and evaluated after a follow-up of 50 months (range 24-84). Six of 8 studies (75%) reported 1 or more significant correlations. All 3 studies assessing postoperative imaging using the MOCART score found a significant correlation of the composite score with the clinical outcome.22,42,62 Although Valderrabano et al 83 reported a correlation but did not use a scoring system, Imhoff et al 43 found a correlation of the repair surface with clinical outcome. Haraguchi et al 37 reported a negative correlation of T1ρ mapping and clinical outcome.
Discussion
The main finding of this study is that MRI parameters do not correlate well with the clinical outcome at a minimum follow-up of 12 months after cartilage repair of the talus. However, there is some evidence that postoperative MRI mirrors clinical outcome in patients with advanced age at a short- to midterm follow-up. Nevertheless, there is a paucity of high-quality research regarding the clinical value of postoperative imaging, especially its predictive value for long-term clinical outcome remains uncertain.
Of the included studies, most (n=26) analyzed the correlation of imaging and outcome after MS procedures, and the results were controversial with a small majority of 15 studies finding a correlation (58%). The current study did not identify a radiologic parameter that was predominantly correlated with clinical outcome in these studies. The most consistent reported parameter after MF was the composite MOCART score, which was associated with better clinical outcome in 5 studies,48,50,74,75,91 as well as changes in the subchondral bone like the presence or changes of BME.3,51,74,75,79 In fact, the role of the subchondral bone in cartilage repair has received increasing interest over recent years.35,59,77 Large BME has been shown to negatively affect cartilage repair outcome in the knee, especially in patients undergoing cell-based procedures. 59 Recently, Jung et al emphasized the importance of subchondral parameters in the evaluation of cartilage repair in the knee. 44 They found that subchondral bone defects and bone marrow edema were correlated with cartilage repair tissue quality and clinical symptoms after matrix-associated ACI with concomitant autologous bone grafting. However, the current meta-analysis could not translate these finding to cartilage repair in the ankle with only 6 of 15 studies (40%), which have investigated this association, finding a significant association with clinical outcome. Of these, 5 studies reported a significant correlation of BME with clinical outcome after MS, and only 1 study identified BME as a correlating parameter after CB.3,21,51,74,75,79 Interestingly, Caumo et al 21 reported that the absence of edema was found to correlate with worse clinical outcomes after ACI. The authors described this finding as a sign of insufficient subchondral remodeling after ACI leading to a deficiency in the maturation process, which ultimately results in poor clinical outcome. Conversely, all studies reporting a relationship between BME and clinical outcome after MS stated that the absence or reduction of subchondral BME correlated with superior clinical outcome.3,21,51,74,75,79
Regarding the correlation of MRI and clinical outcome after CB for OLT, evidence is scarce in the current literature, with only 4 of 10 studies (40%) reporting a statistically significant association.9,21,29,64 The most consistent parameter reported was “defect filling” with 3 studies stating statistical significance,29,64 whereas 1 study each identified T2 mapping signal and the composite MOCART as being related to clinical outcome.9,21 Because these studies were heterogenous in follow-up time and assessment of radiologic parameters, the interpretation of its clinical value is challenging. In fact, potential correlations of imaging and clinical outcome after CB have been more intensively studied in the knee joint. In a meta-analysis in 2013, 10 of 19 studies reported a significant correlation between graft hypertrophy and repair tissue signal (as defined by the Henderson score), 40 with a moderate to good correlation of the overall Henderson score with clinical outcomes. 15 Similar to McCarthy et al, 58 who reported a significant association of defect fill, overall signal intensity, and surface of repair tissue with clinical outcome at 12 months after ACI, the mentioned meta-analysis from 2013 had a shorter follow-up period, with studies demonstrating a correlation at 6 months postoperatively and a maximal follow-up of 60 months when compared to the current study. As seen in the results of this study, shorter follow-up was significantly associated with the finding of correlation between clinical and radiographic outcome. Prior studies have shown that complete graft maturation is found 13.5 months after MS and 12-24 months after CB treatment,34,63 yet graft deterioration might start as early as 30 months after cartilage repair with declining imaging scores over time.20,71 Consequently, although optimal timing for MRI evaluation after cartilage repair still remains controversial, some authors suggest a time period between 12 and 30 months as potentially ideal for postoperative imaging in asymptomatic patients to mirror clinical outcome, which is supported by the current findings. 1
Interestingly, the greatest percentage of correlation was found after cartilage restoration techniques. Six of 8 studies (75%) evaluating restoration techniques found a positive correlation to clinical outcome.22,37,42,43,62,83 Similar to the included MS studies, most studies evaluated the composite morphologic appearance on MRI with only limited information about specific subscale parameters. The largest cohort in the current review with 38 patients after OAT, Nguyen et al 62 found a significant correlation between the MOCART score and the ability to return to one’s previous level of activity. In contrast to the ankle joint, studies investigating OAT in the knee were able to identify specific MRI parameters like cystic subchondral change, missing of trabeculae crossing the defect site, abnormal articular cartilage signal and signs of decreased osteointegration that were associated with worse clinical outcome.86,89 Hence, it would be interesting to see if similar findings can be reported after cartilage restoration in the ankle.
Generally, the lack of association between conventional MRI and clinical outcome in cartilage repair of the knee 28 and ankle, as seen in the current study, may stem also from the still rather unspecific nature of current MRI scores such as the MOCART, Osteochondral Allograft MRI Scoring System (OCAMRISS). As Ackermann et al 2 pointed out in a study investigating the effect of the augmentation of bone marrow aspirate on clinical and imaging outcomes after OCA to the knee, the majority of OCAMRISS subscales (same applies to the MOCART) are dichotomous and score solely the absence or presence of the respective MRI feature. Thus, this may result in missing small but potentially clinically relevant differences in graft maturation and integration. This may have also led to the current finding that the correlation of postoperative MRI and clinical outcome is more pronounced in patients with advanced age as increased interindividual differences in cartilage regeneration potentially exist in these patients, thus generating a large enough effect size to be detected by current MRI scores.
In contrast to morphologic MRI techniques, compositional MRI sequences like T2 mapping are able to provide compositional information about tissue formation after cartilage repair. 76
However, this technique is largely used for research settings and is generally not clinically employed. Compared with morphologic MRI sequences, T2 mapping has been able to demonstrate changes in water content and collagen orientation, which is known to play an important role in degeneration of cartilage.8,55 Water content increases in pathologic cartilage and destruction of collagen fiber network increases T2 relaxation, which is an early sign of cartilage degeneration. T2 relaxation in repair tissue differs for each repair technique, which might be helpful in identifying hyaline-like tissue as found in cell transplantation repair techniques compared to fibrocartilage that can be found after MS. 52 Although T2 mapping has been more profoundly studied after cartilage repair of the knee with inconsistent correlation to clinical outcome, 69 there is still insufficient evidence for any association with clinical outcome in cartilage repair of the ankle. The current systematic review identified 5 studies across all groups of cartilage repair (MS, CB, and cartilage restoration) that reported significant correlations with clinical outcome.10,50,64,68,79 Further improvement of current qualitative MRI and more advanced MRI techniques may provide more insight into detailed cartilage repair tissue morphology and maturation, thus generating qualitative data ultimately helping to predict outcome after cartilage repair. 32
This systematic review and meta-analysis has inherit limitations, which have to be acknowledged. First, the included studies show variation in methodology, cartilage repair techniques, and MRI sequences. Whereas cartilage repair with MS is the most investigated technique, studies assessing postoperative imaging in CB and cartilage restoration techniques are scarce making it challenging to draw meaningful conclusions. Because of heterogenous MRI sequences used it is difficult to draw comprehensive conclusions about a specific MRI technique in the evaluation of cartilage restorative procedures. Second, the small sample sizes and different follow-up times of the included studies increase the risk of bias, especially as the quality of cartilage repair tissue varies over time, resulting in the comparison of groups with variable tissue maturation stages. Notably, small sample sizes allow only for the detection of large effect sizes, thus introducing the risk of type II error. Consequently, larger study sizes are needed to identify smaller but potentially clinically relevant effects after cartilage repair. This is highlighted by the findings in the current meta-analysis, where studies with larger sample sizes were more likely to detect a correlation of MRI and clinical outcome.
Conclusion
Interpreting MRI in prediction of clinical outcome in ankle cartilage repair remains challenging; however, it seems to hold some value in reflecting clinical outcome in patients with advanced age and/or at a shorter follow-up. Yet, further research is warranted to optimize postoperative MRI protocols and assessments allowing for a more comprehensive repair tissue evaluation, which eventually reflect clinical outcome in patients after cartilage repair of the ankle.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221092021 – Supplemental material for Correlation of Postoperative Imaging With MRI and Clinical Outcome After Cartilage Repair of the Ankle: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114221092021 for Correlation of Postoperative Imaging With MRI and Clinical Outcome After Cartilage Repair of the Ankle: A Systematic Review and Meta-analysis by Manuel Waltenspül, Christoph Zindel, Franziska C. S. Altorfer, Stephan Wirth and Jakob Ackermann in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because the current study is a systematic review and synthesis of published data. The study uses data from previous published studies which are available in the public domain. No new (personal) data was collected for current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.