
Abstract
Background:
A bunionette is a painful prominence of the fifth metatarsal head. This study aimed to compare the clinical outcome of 2 corrective osteotomies, namely, the Mau-type and Ludloff-type osteotomies. We report results with regard to correction, healing, complications, and patient-reported outcomes.
Methods:
Thirty-two patients who underwent bunionette corrective surgery from March 2011 to May 2017 were included in the study. All patients had pre- and postoperative radiographs. The pre- and postoperative fourth-fifth intermetatarsal angles (IMAs) and postoperative fifth metatarsal bowing angle were measured. Radiographic union was assessed at 12 weeks. All patients completed the Self-Reported Foot and Ankle Score (SEFAS) questionnaire to assess clinical outcome. Thirty-two patients (43 feet) were available for follow-up and completed the SEFAS score. Twenty-two Mau-type and 21 Ludloff-type osteotomies were performed.
Results:
The mean pre- and postoperative IMA for Mau was 10.5 and 4.3 degrees, respectively, and for the Ludloff was 10.2 and 4 degrees, respectively, with no statistically significant difference between the 2 groups. The Mau caused more bowing with a mean of 9.8 degrees as compared to a mean of 3.5 degrees with the Ludloff. No patients in the Mau group reported clinical problems related to the increased bowing. All osteotomies united. The Mau cohort had a mean SEFAS score of 45 and the Ludloff cohort a mean of 46. No feet had fair or poor outcome scores.
Conclusion:
Patient satisfaction after bunionette correction with an oblique shaft rotational osteotomy was good. Orientation of the osteotomy did not affect outcomes. Postoperative bowing of the fifth metatarsal was greater with the Mau-type osteotomy. Postoperative fifth metatarsal bowing had no negative clinical effects. The trend in our unit has been a preference toward the Mau-type osteotomy as it is perceived to be more stable.
Level of Evidence:
Level III, retrospective comparative series.
Introduction
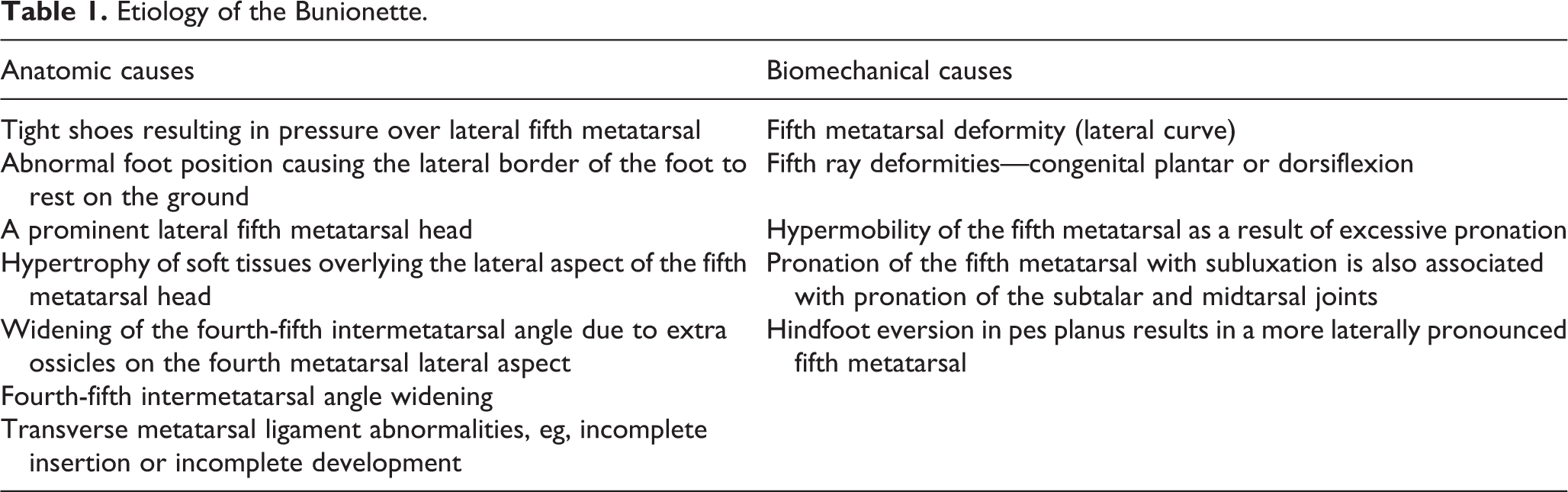
A bunionette, or Tailor bunion, consists of bony and soft tissue elements and is characterized by a painful prominence of the lateral aspect of the fifth metatarsal head. The cause of the fifth metatarsal head’s excessive prominence may be a rotational component of the ray that results in pronation. 22 In the case of a cavovarus foot, plantarflexion as well as abduction of the fifth ray causes a bunionette with an associated plantar keratosis. 22 The underlying bony prominence leads to chronic irritation of the overlying bursa. 9 The condition often presents together with hallux valgus, both of which are often noted with a flexible flatfoot. 22 The etiology of the bunionette can be divided into anatomic and biomechanical causes 4 (Table 1).
Etiology of the Bunionette.
The incidence of bunionette is more common in women (3-10 times more) than men and most often occurs during the fourth and fifth decades of life. 21 Patients often complain of pain, swelling, erythema, and keratosis over the lateral and/or plantar aspect of the fifth metatarsal head. 20 The symptoms are aggravated by closed shoe wear and impact activities.
A radiographic classification system for the bunionette was described by Coughlin, consisting of 3 types. Incidence of type 1 is 16% to 33%, type 2 is 10%, and type 3 is 57% to 74% (Figure 1). 8 A fourth type was described by Fallat et al, 11 which is a combination of types 1 to 3 and normally occurs in patients with rheumatoid arthritis. 2,5,10,17

Coughlin radiographic classification for bunionettes. (A) Type 1: Enlarged fifth metatarsal head. (B) Type 2: Lateral bowing of fifth metatarsal. (C) Type 3: Increased fourth-fifth intermetatarsal angle.
Radiographic evaluation of a patient with a bunionette is necessary to define the type of deformity and quantify the severity, which will then guide management. The following measurements need to be recorded 2,20 : metatarsal head diameter (normal is less than 13 mm2), fourth-fifth intermetatarsal angle (IMA) (normal is less than 8 degrees [average 4.5 degrees]). 22
More than 30 different osteotomies, both open and minimally invasive, have been described for the operative treatment of bunionettes, when conservative treatment fails. 4,8,9,16,18 -20 The goal of surgery is to remove the painful lateral prominence of the fifth metatarsal head and decrease the fourth/ fifth intermetatarsal angle and thereby decrease the width of the foot. 13 Two of the described osteotomies are the Ludloff type and Mau type, which are oblique rotational shaft osteotomies. Both techniques have already been described for correction of a moderate to severe type 2 and 3 bunionette in the literature, but never compared. 2,4,20 The Ludloff osteotomy has the drawback of being unstable to ground reaction forces whereas the Mau osteotomy results in bowing of the metatarsal, which could result in a new pressure point. 1
The aim of this retrospective study was to evaluate whether there is a difference in clinical and radiologic outcome between the Mau- (Figure 2) and the Ludloff-type (Figure 3) osteotomies for the correction of a bunionette. Our hypothesis was that the Mau type would be more stable but that the Ludloff type would result in less bowing of the lateral border of the fifth metatarsal.

Mau-type osteotomy: results in bowing due to midosteotomy fixation point.
Ludloff-type osteotomy: No bowing caused as fixation is at proximal end of osteotomy.
Methods
All patients who underwent bunionette corrective surgery using a Mau-type or Ludloff-type osteotomy from March 2011 to May 2017 were included in the study. Ethical approval was obtained from the local ethics committee. The exclusion criteria included age ≤16 years, treated with any technique other than the osteotomies described above, any other concomitant surgery to the ipsilateral foot and if patients were not available for follow-up.
Operative treatment was considered in a symptomatic bunionette once conservative management failed. Both procedures and subsequent follow-up were done by the 2 senior authors working in the unit. The surgeons in each case performed their preferred osteotomy. Forty-three feet in 32 patients were included in the study. There were 27 female and 5 male patients. The average age was 42 (range, 17-66) years for the Ludloff group and 50 (range, 17-69) years for the Mau group. Sixteen patients (22 feet) had the Mau-type osteotomy and 16 patients (21 feet) had the Ludloff-type osteotomy. Six patients had bilateral Mau-type osteotomies, and 5 patients had bilateral Ludloff-type osteotomies. The average length of follow-up was 35.5 (range, 7-56) months for the Mau group and 30 (range, 8-81) months for the Ludloff group.
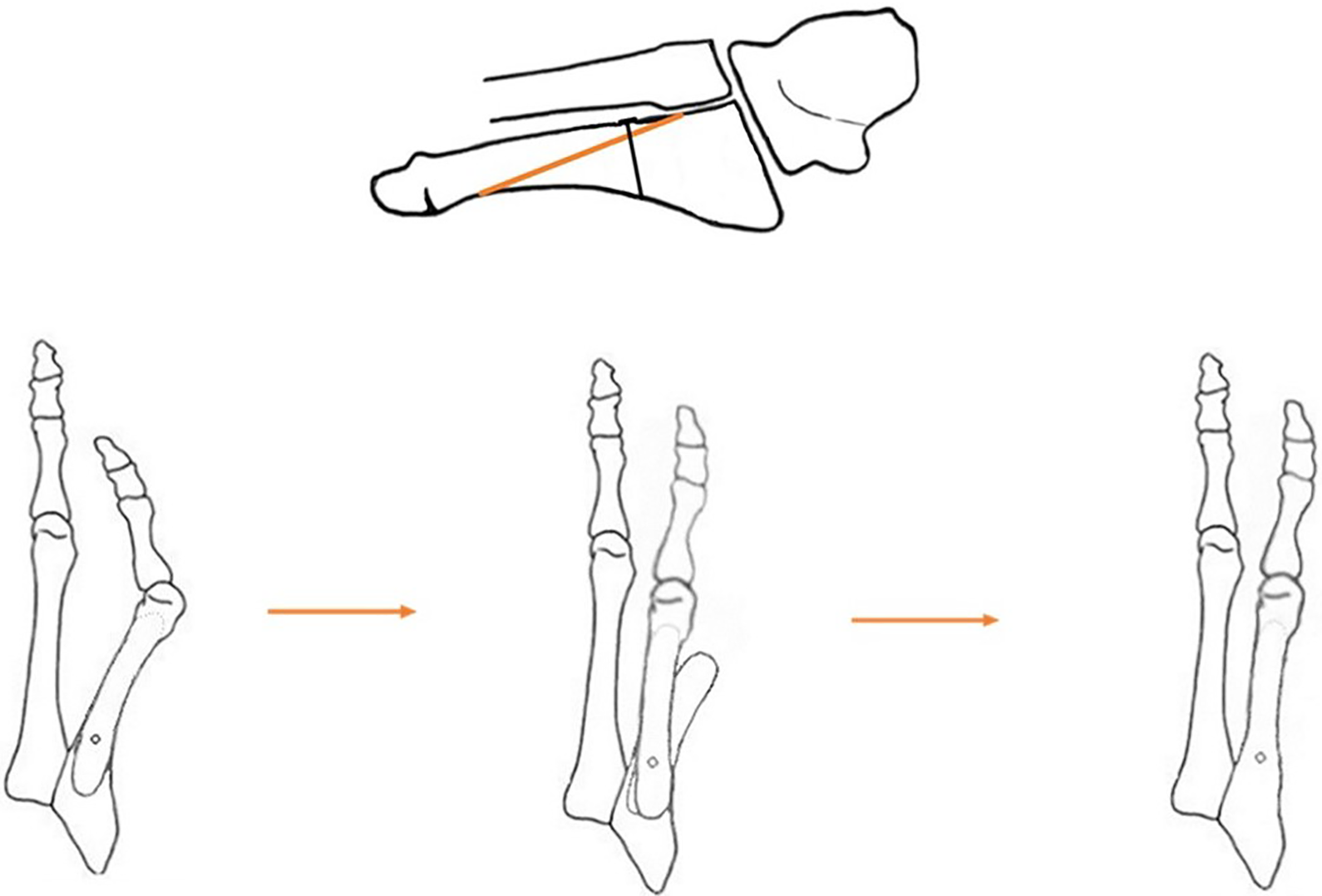
All patients had preoperative standard weightbearing foot radiographs. The preoperative radiographs were used to measure the fourth-fifth intermetatarsal angle (IMA), which is the angle between a line drawn down the long axis of the fourth and fifth metatarsal shafts, respectively. This angle was then used to aid in classifying and quantifying the deformities (Table 2). Postoperative weightbearing radiographs were performed at 12 weeks for measurement of the fourth-fifth IMA and bowing of the fifth metatarsal and to confirm union of the osteotomy. 17 Union was defined as the presence of cross trabeculation across the osteotomy on 2 views. Bowing was quantified by measuring the angle formed by the longitudinal axis of the proximal and distal shafts of the fifth metatarsal (Figure 4).
Patient Bunionette Classified According to Coughlin’s Radiographic Classification.


Angle of bowing: measured between the longitudinal axis of the proximal and distal fragments.
Clinical outcome was assessed with the Self-Reported Foot and Ankle Score (SEFAS) questionnaire (which is a validated patient-reported outcome measure [PROM]) at the most recent follow-up. 7 A total SEFAS score of 0 represents the most severe disability whereas a score of 48 represents normal function. The score is then subclassified as excellent (SEFAS >41), good (SEFAS 34-41), fair (SEFAS 27-33), and poor (SEFAS <27).
Complications were recorded from the clinical records. All information was documented on an Excel spreadsheet. Anonymity of the patients was maintained using a coded system. Statistical analysis of the data was done using a paired t test to assess for a difference within a specific cohort and an unpaired t test to determine whether there was a significant difference between the 2 cohorts. Statistical difference was defined as P <.05.
Operative Technique
The patient was positioned supine with a tourniquet applied to the thigh. The patient was given an ankle block for postoperative pain control. A longitudinal incision was made from the proximal phalanx of the fifth toe to the base of the fifth metatarsal. The capsule of the fifth MP joint was opened using a longitudinal incision. The bunionette was resected using an oscillating saw. Caution was taken to only resect the exostosis and not violate the metatarsal head.
Mau-Type Osteotomy
The Mau osteotomy was marked starting distal dorsal just proximal to the head of the fifth metatarsal, exiting plantar proximal just distal to the fourth-fifth intermetatarsal joint (Figure 2). The distal two-thirds of the osteotomy was cut using the oscillating saw. The cut was made perpendicular to the long axis of the metatarsal to avoid elevating or depressing the metatarsal. In cases with plantar keratoses, the metatarsal was elevated to offload the callus, by aiming the saw cephalad. 17 A cannulated 2 mm screw was placed proximally, perpendicular to the partial osteotomy. With the K-wire in place, the screw is inserted only 75% of the way (Figure 5A). By keeping the wire in place and only partially inserting the screw gave control over the osteotomy and allowed for rotation of the distal fragment around the wire. The proximal third of the osteotomy was them completed (Figure 5B). The distal fragment of the metatarsal was then rotated medially to correct the fourth-fifth IMA (Figure 5C). The proximal screw was then fully tightened to secure the osteotomy in a reduced position. The screw was tightened while visualizing the osteotomy being compressed to avoid overtightening and risk fracturing the cortex. The foot was screened under image intensifier to confirm adequate reduction of the fourth-fifth IMA. The osteotomy was then fixed with 1 or 2 additional 2-mm screws, depending on the size of the metatarsal preferably with a low-profile head which did not require countersinking and thus minimizing the risk for fracturing the cortex. It was important to check that the fixation screws were not too long on the plantar aspect, as they can cause pain with weightbearing. The overhanging lateral bone shelf was resected using an oscillating saw (Figure 5D).

(A) Distal half of osteotomy is performed first and secured with a cannulated screw inserted 75% of the way in. (B) The proximal half of the osteotomy is completed. (C) The distal half is rotated medially and secured. (D) A second cannulated screw is used for final fixation and the overhanging bony shelves are resected.
Ludloff-Type Osteotomy
The Ludloff osteotomy was marked starting proximal dorsal just distal to the fourth-fifth intermetatarsal articulation, exiting plantar distal proximal to the metatarsal head (Figure 3). The proximal half of the osteotomy was cut using an oscillating saw. The cut was made perpendicular to the long axis of the metatarsal to avoid elevating or depressing the metatarsal. A cannulated 2-mm screw was placed as proximal as possible and perpendicular to the partial osteotomy. With the K-wire in situ, the screw was inserted only 75% of the way. By keeping the wire in place and only partially inserting the screw control over the osteotomy allowed for rotation of the distal fragment around the wire. The distal half of the osteotomy was then completed. The distal fragment of the metatarsal was then rotated medially to correct the fourth-fifth IMA. The proximal screw was then fully tightened to secure the osteotomy in a reduced position. The foot was screened under image intensifier to confirm adequate reduction of the fourth-fifth IMA. The osteotomy was then fixed with one or 2 additional 2-mm screws, depending on the size of the metatarsal. The overhanging lateral bone shelf was resected using an oscillating saw. Since this osteotomy was less stable, a lateral 2 mm plate was sometimes used for extra stability if required (Figure 6). The addition of a plate allowed for early weightbearing with decreased risk of osteotomy displacement. Thirteen patients in this cohort had additional plate fixation as 3 fixation screws could not be used. This additional fixation could be bulky and was an extra expense.

Supplemental fixation with a plate for the Ludloff-type osteotomy.
Closure
A capsulorrhaphy of the lateral capsule was performed using Vicryl 2-0 with the fifth toe held in a neutral position (Figure 7A). The wound was closed in layers. A well-padded dressing was applied (Figure 7B).

(A) A capsulorrhaphy of the lateral capsule is performed using the “shoe lace” technique. (B) A thin piece of sponge is used as a spacer in the fourth web to protect the capsulorrhaphy while it heals.
Postoperative Care
The foot was placed in a heel wedge shoe and the patient was allowed to heel weightbear as tolerated from day 1. The patient was instructed to elevate the foot for the first 2 weeks. The bandages were changed at week 1,2, and 4.
The patient was transitioned into supportive shoes at 6 weeks. Physiotherapy was started at this time.
Radiographs were taken at 12 weeks to assess for bony union. The patient could return to normal activities after 3 months once radiographic union was confirmed.
Results
The Mau cohort had a mean preoperative IMA of 10.5 (range, 5 - 18) degrees and mean postoperative IMA of 4.3 (range, 0 -11) degrees(P< 0.05). The Mau osteotomy had an average IMA correction of 5.9 degrees. The Ludloff cohort had a mean preoperative IMA of 10.2 (range, 6 - 16) degrees and mean postoperative IMA of 4 (range, 0 -7) degrees (P < 0.05). The Ludloff osteotomy had an average IMA correction of 6.2 degrees. There was no statistical difference between the 2 cohorts with regard to preoperative IMA (P = 0.77) and postoperative IMA (P = 0.545). Therefore, there was no difference with regard to power of correction between the 2 osteotomies. Pre- and postoperative IMA for both cohorts is documented in Table 3. The Mau osteotomy had a mean bowing angle of 9.8 (range, 0-18) degrees while the Ludloff osteotomy had a mean bowing angle of 3.5 (range, 0-7) degrees (P < .05). No patient reported symptoms related to the bowing. All osteotomies progressed to union at 3 months on radiograph.
Radiographic Measurements.

Abbreviation: IMA, intermetatarsal angles.
The Mau group had a mean SEFAS score of 45 (range, 34-48) of which 20 (90.9%) feet had excellent outcomes and 2 (10%) feet had good outcomes. The Ludloff group had a mean SEFAS score of 46 (range, 40-48), of which 19 (90.47%) feet had excellent outcomes and 2 (9.5%) feet had good outcomes. No feet in either group scored as fair or poor outcomes. There was no statistical difference (P = 0.4) in patient satisfaction between the 2 cohorts. The SEFAS score for each cohort is documented in Table 4.
SEFAS Scoring for Both Cohorts.

Abbreviation: SEFAS, Self-Reported Foot and Ankle Score.
The following complications were noted. In the Mau-type osteotomy group, 1 patient had a stress fracture through the osteotomy site at 2 months postoperatively that healed after a month in a boot, 1 patient had slight dorsal angulation of the fifth toe but did not require additional surgery, and 1 patient experienced mild discomfort with shoe wear over the scar. Three patients in the Mau group required removal of hardware, because of the screws being too long and causing pain with weightbearing. In the Ludloff-type osteotomy group, 1 patient reported subjectively that the foot width looked unchanged pre- and postsurgery, but clinically his symptoms had resolved. One patient had removal of hardware 8 months after the index procedure due to plantar irritation from the fixation screws being too long. None of the patients complained from irritation due to the plate fixation.
Discussion
When nonoperative treatment of a bunionette fails in relieving symptoms, operative treatment is indicated. 19 There are multiple operative options for the management of bunionettes. Cooper et al 6 reported that recurrence occurs when the chosen procedure fails to address the severity of the deformity. It is therefore important to take into consideration the magnitude of the IMA when choosing the appropriate corrective procedure. Distal osteotomies such as a distal chevron and lateral eminence resection of the head are normally reserved for type 1 and mild (IMA < 12 degrees) type 2 and 3 deformities. Distal osteotomies are limited in that the distal fragment can only be translated 50% of the metatarsal width before becoming unstable and risking dorsal malunion. 3 Kitaoka et al 15 only got a mean IMA correction of 2.6 degrees with a distal chevron osteotomy and reported that distal osteotomies would be inadequate for IMA greater than 13 degrees. Bewick et al 3 and Waizy et al 20 reported similar findings regarding distal osteotomies. Diaphyseal osteotomies such as the scarfette, Ludloff type, and Mau type are preferred in moderate to severe (IMA >12 degrees) type 2, 3, and 4 deformities. 21 Proximally based osteotomies have fallen out of favor because of risk of damage to the fifth metatarsal blood supply. 17,18,20 Authors prefer the oblique-type osteotomy, especially for severe type 3 deformities, because of the ability to control length and rotation as well as elevation and depression of the metatarsal head while concurrently preserving the proximally based metatarsal blood supply. 18 This retrospective study compared the clinical outcomes using the SEFAS score and radiographic correction using radiograph measurements of 2 commonly used metatarsal realignment osteotomies, namely, the Mau type and Ludloff type. 4,20 The 2 cohorts were matched according to the Coughlin classification and preoperative IMA (10.5 vs 10.2 degrees) so as to allow for comparative analysis.
A longitudinal diaphyseal osteotomy extending proximal dorsal to distal plantar (Ludloff type) was described by Coughlin, with 93% of patients reporting good or excellent results using a subjective satisfaction assessment. 8 In our study, 90.5% of the patients in the Ludloff group reported excellent results using the validated SEFAS scoring system. The benefit of this osteotomy is that it can be rotated at its base, around the proximal fixation point making it powerful with minimal bowing of the metatarsal. The concern with the Ludloff-type osteotomy is that the orientation of the bony cut results in distractive forces across the osteotomy site when weightbearing due to the ground reaction force. This could result in failure of fixation and loss of correction or elevation of the metatarsal. Elevation of the metatarsal results in transfer metatarsalgia, which is one of the commonly reported complications after bunionette correction. In previous studies, patients were kept nonweightbearing for 6 weeks in a short cast to minimize the risk of malunion. 8,17 The author (P.N.F.) added plate fixation in 13 cases to allow for early weightbearing. In our study cohort, all patients united at 12 weeks with no loss of correction.
The reverse Ludloff-type osteotomy is not a new concept and has been used in the form of the Mau osteotomy to correct hallux valgus. Studies have shown that the Mau- and scarf-type osteotomy have similar outcomes and success rates to the Ludloff-type osteotomy when treating hallux valgus. 16,18,21 The orientation of the Mau osteotomy results in compressive rather than distractive forces acting across the osteotomy site with weightbearing. This compressive force would be in addition to the compressive screws placed across the osteotomy site, which provide the initial stability. The downside is that the center of rotation around the proximal fixation is not as proximal as with the Ludloff type (Figure 3). The metatarsal will therefore bow around the more distal (midshaft) fixation point giving a “banana” like shape to the metatarsal (Figure 2). This bowing is of concern as it could cause a new area of abnormal pressure with shoe wear. Although the amount of bowing was found to be statistically greater with the Mau osteotomy in this study, no patient reported clinical symptoms from the bowing. We postulate that the abductor digiti minimi, which overlies the lateral border of the metatarsal, acts as padding to pressure over the area of bowing.
The average fourth-fifth IMA for normal feet ranges from 3 to 11 degrees with an average fourth-fifth IMA of 6.2 degrees, whereas symptomatic bunionettes have an average fourth-fifth IMA angle of 9.6 degrees. 10,12,21 The average fourth-fifth IMA after correction of deformity using the scarfette osteotomy has been reported to be 1.8 degrees ± 2.21 degrees in one study and 5.7 degrees in another. 16,21 In our study, the average postoperative fourth-fifth IMA after the Mau-type osteotomy was 4.3 degrees and 4 degrees after the Ludloff-type osteotomy. Both osteotomies achieved correction within the normal range, with neither showing superior corrective ability. Another benefit of these oblique osteotomies is the relatively large surface area that results from the osteotomy, which decreases the risk for nonunions. 20 There was no nonunion in both cohorts of this study. Thus, despite being a diaphyseal osteotomy, there does not seem to be an increased risk for nonunion.
Complications associated with operative bunionette correction include painful hardware and transfer metatarsalgia. Coughlin et al 9 reported that 87% of his patients required hardware removal. He used a combination of small fragment screws and K-wires for fixation. Small fragment screws have a prominent screw head that can cause subcutaneous irritation. 8 Vienne et al 19 reported removal of screws in 18% of cases because of prominence on the lateral aspect of the metatarsal. They used 2.7-mm compression screws for fixation. We removed hardware in 4 (9%) feet. All cases of removal were due to the fixation screws being too long, causing plantar irritation with weightbearing. It is important to confirm appropriate screw length intraoperatively to avoid reoperation. Because we used a 2-mm screw with a low-profile head, we had no irritation from the screw heads.
Transfer metatarsalgia occurs when the fifth metatarsal is shortened, elevated, or resected. 18 Transfer metatarsalgia was fairly common in the early literature when fixation of osteotomies was not performed. Keating et al 14 reported on a distal osteotomy that was not internally fixed and had a 76% incidence of transfer metatarsalgia. The incidence is far less in the current literature because of the use of fixation but still occurs with proximal and distal osteotomies. Translating the chevron osteotomy more than 50% may result in instability and elevation of the metatarsal. 6 The rotational diaphyseal osteotomy has the benefit of maintaining length and controlling elevation, thereby minimizing transfer metatarsalgia. We had no cases of transfer metatarsalgia in our cohorts. The metatarsal can be elevated by aiming the osteotomy cephalad or depressed by aiming caudad. Patients with associated painful plantar keratosis, commonly seen in cavovarus feet, have been reported to have poorer outcomes after bunionette correction. Maher et al 16 reported on the scarf osteotomy for bunionette correction and found the least satisfaction in patients with cavovarus feet because of a 10.8% recurrence of plantar keratoses. These oblique osteotomies (Mau and Ludloff) can be used to elevate the metatarsal. By elevating the metatarsal, pressure is alleviated off the plantar keratoses. We had no cases with a cavovarus deformity requiring this modification.
This study has found that the direction of the osteotomy did not affect the measured outcome as both cohorts had similar results, with both techniques scoring in the excellent to good range on the SEFAS score. Technically, one osteotomy is no more difficult to perform than the other, and as the study shows, either one should lead to good outcomes; thus, surgeon preference should be the determining factor as to which technique is performed. Over time, however, the Mau-type osteotomy has become the preferred method for both senior authors. Intuitively, it seems to provide better mechanical stability across the osteotomy site, because of the orientation of the osteotomy resulting in compressive rather than distractive forces acting across the osteotomy site with weightbearing. There is also a cost saving as additional plate fixation is not required for early mobilization.
Conclusion
Type 2 to 4 bunionettes were successfully managed with either a Mau- or Ludloff-type rotational osteotomy, with excellent or good outcomes and good radiologic correction. Despite the Ludloff-type osteotomy being less stable, there were no cases of nonunion or displacement in our series. The Mau-type osteotomy did result in significantly more bowing of the metatarsal but with no clinical sequelae. Thus, the decision as to which osteotomy to perform should be up to surgeon preference.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011421993793 - Comparison of 2 Oblique Fifth Metatarsal Osteotomies for the Management of a Bunionette
Supplemental Material, sj-pdf-1-fao-10.1177_2473011421993793 for Comparison of 2 Oblique Fifth Metatarsal Osteotomies for the Management of a Bunionette by Richard Paterson, Nikiforos Pandelis Saragas and Paulo Norberto Faria Ferrao in Foot & Ankle Orthopaedics
Footnotes
Ethics approval
University of the Witwatersrand, Human research ethics committee (Medical) Protocol No: M171175.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.