
Abstract
Background:
Distal tibia fractures are common in the pediatric patient population. Recent reports suggest that patients with closed low-energy distal tibial fractures treated with short leg casts (SLCs) have similar radiographic outcomes with improved functional outcomes compared to those treated with long leg casts (LLCs). However, to date there has not been a study comparing these treatment modalities for Salter-Harris (SH) II distal tibia fractures. The purpose of this study was to compare the radiographic and time to weightbearing outcomes between patients with SH-II tibial ankle fractures treated with an SLC vs an LLC.
Methods:
A retrospective review on SH-II distal tibia fractures was performed at a Level I pediatric trauma center from 2013 to 2020. Primary outcomes included final coronal angulation, sagittal angulation, and time to weightbearing.
Results:
A total of 59 patients with SH-II distal tibia fractures were treated with an SLC (22 patients, median age 11.79 years) or an LLC (37 patients, median age 12.17 years). There was no statistically significant difference between the 2 treatment groups for coronal angulation at final follow-up, sagittal angulation at final follow-up, or percentage of patients fully weightbearing at 6 weeks (P > .05). No patients required subsequent remanipulation or operative treatment in either treatment group.
Conclusion:
In this retrospective review with relatively short-term follow-up, SLCs were found to be noninferior to LLCs for treatment of reduced SH-II distal tibia fractures. This casting option may still be considered by surgeons who are nonoperatively managing pediatric distal tibia fractures.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Pediatric ankle fractures are the third most common fracture involving the growth plate and account for 11% to 38% of physeal injuries.3,9 When describing pediatric ankle fractures, the Salter-Harris (SH) classification system is most commonly used. SH-II injuries are fractures that extend through the physis and include a proximal metaphyseal segment often referred to as a Thurston-Holland fragment.4,9 Various studies examining distal tibial fractures have reported that SH-II fractures occur in roughly 40% of all distal tibia fractures in the pediatric population.4,5,7 This is particularly alarming as the distal tibial physis contributes to approximately 3-4 mm/y and 40% of the final tibial length. 3
Closed low-energy distal tibial ankle fractures have historically been treated with an above-the-knee long leg cast (LLC). However, recent studies have shown that treatment with a below-the-knee short leg cast (SLC) leads to similar radiographic outcomes with faster time to weightbearing, shorter time to union, and improved range of motion (ROM) and stiffness when compared to treatment with LLCs for midshaft and distal shaft pediatric tibia fractures.1,8 Despite showing the efficacy of SLCs for distal tibial injuries, these studies were restricted to tibial shaft fractures without physeal or metaphyseal involvement. Since 2020, 2 noncomparative studies have described the efficacy of SLCs in the management of distal tibial fractures involving the physis.11,12 Both concluded that SLCs were an effective treatment option for minimally displaced SH-II fractures. Although promising, the noncomparative nature of these studies limited the generalizability of any conclusions that could be drawn relative to the standard LLC. Therefore, the purpose of this study was to directly compare the final radiographic outcomes, need for subsequent fracture manipulation or conversion to operative treatment, and the percentage of patients fully weightbearing at 6 weeks between SLCs and LLCs for nonoperatively managed distal tibial SH-II fractures.
Materials and Methods
This retrospective study was performed with IRB approval (1654383-3). All electronic medical records were identified for patients who were treated for a tibial fracture (CPT codes 27750-27848) at our Level I pediatric trauma center from January 1, 2013, to September 24, 2020. A total of 1220 patient charts was identified. Patient charts were reviewed to determine eligibility within the study. Included patients were ambulatory school-aged children between the ages of 6 and 18 years at the time of initial service, were diagnosed with closed SH-II fractures of the distal tibia, and were treated with closed reduction and casting using either an LLC (Figure 1) or SLC (Figure 2). Additionally, patients were required to have a minimal displacement of at least 3 degrees in both the coronal and sagittal plane in order to be included in the study. Excluded patients were those who required immediate open treatment, those with open fractures, those with distal tibial fractures that were not SH-II patterns, and those who underwent conservative treatment that was not an LLC or SLC. Fifty-nine patients met these criteria and were included in the study.

A Salter-Harris II distal tibia fracture that was managed with a long leg cast. Coronal (left) and sagittal (right) radiographs are presented prior to reduction (top) and at final follow-up (bottom).

A Salter-Harris II distal tibia fracture that was managed with a short leg cast. Coronal (left) and sagittal (right) radiographs are presented prior to reduction (top) and at final follow-up (bottom).
All included patients were initially treated in the Emergency Department after anteroposterior (AP) and lateral radiographs of the injured tibia were obtained. Patients then underwent closed reduction under conscious sedation. The patient was placed in either an SLC or an LLC, with the knee at 20 degrees of flexion. Cast length was selected at the discretion of the surgeon and was independent of fracture morphology for the included patients. All patients were initially nonweightbearing after cast application and were closely followed in clinic with AP and lateral radiographs over a standard, institution-specific period of ≥3 months. Full weightbearing was permitted at 6 weeks if at least 50% cortical bridging on AP and lateral radiographs was noted.
Using medical records, demographic and clinical information was acquired for each patient case. This included age at the time of injury, gender, laterality of the fracture, fibular involvement, cast type, prereduction coronal angulation, prereduction sagittal angulation, coronal angulation at final follow-up, sagittal angulation at final follow-up, weightbearing status at 6 weeks, need for subsequent cast wedging, need for subsequent remanipulation, and need for subsequent surgical intervention.
Radiographic evaluation was performed by 2 authors, S.P.D. and V.V.K., who performed 3 measurements in the coronal plane and 3 measurements in the sagittal plane using radiographs at final follow-up. This technique is outlined in Figure 3. The mean coronal and sagittal angulation value was recorded for each case. Measurements were taken using the Picture Archiving and Communication System (PACS). Malunion was defined as angulation greater than 5 degrees in the coronal or sagittal plane at final follow-up. 2

Measurement technique is demonstrated. Coronal (left) and sagittal (right) radiographs are presented prior to reduction (top) and at final follow-up (bottom). For both coronal and sagittal orientations, measurement begins at the midline axis of the tibia. Measurement stays in the midline axis of the tibia until discontinuity due to fracture is reached (midline discontinuity point). An angle is formed between midline discontinuity point and tibiotalar interaction midpoint.
Data analysis was performed using IBM SPSS Statistics for Macintosh (version 28.0; IBM Corp). For categorical variables, a Fisher exact test was performed. 6 Results were reported as a count and frequency. For continuous numerical variables, a Shapiro-Wilk test was performed, and it was determined that all continuous numerical variables were not normally distributed, so an exact version of the Mann-Whitney U test was performed. Results were described as a median with an interquartile range (IQR). For this study, α was defined as <0.05. There was no prior power analysis, and sample size may increase the chance of a type II error. Exact versions of each test were performed to reduce the impact of small sample size.
Results
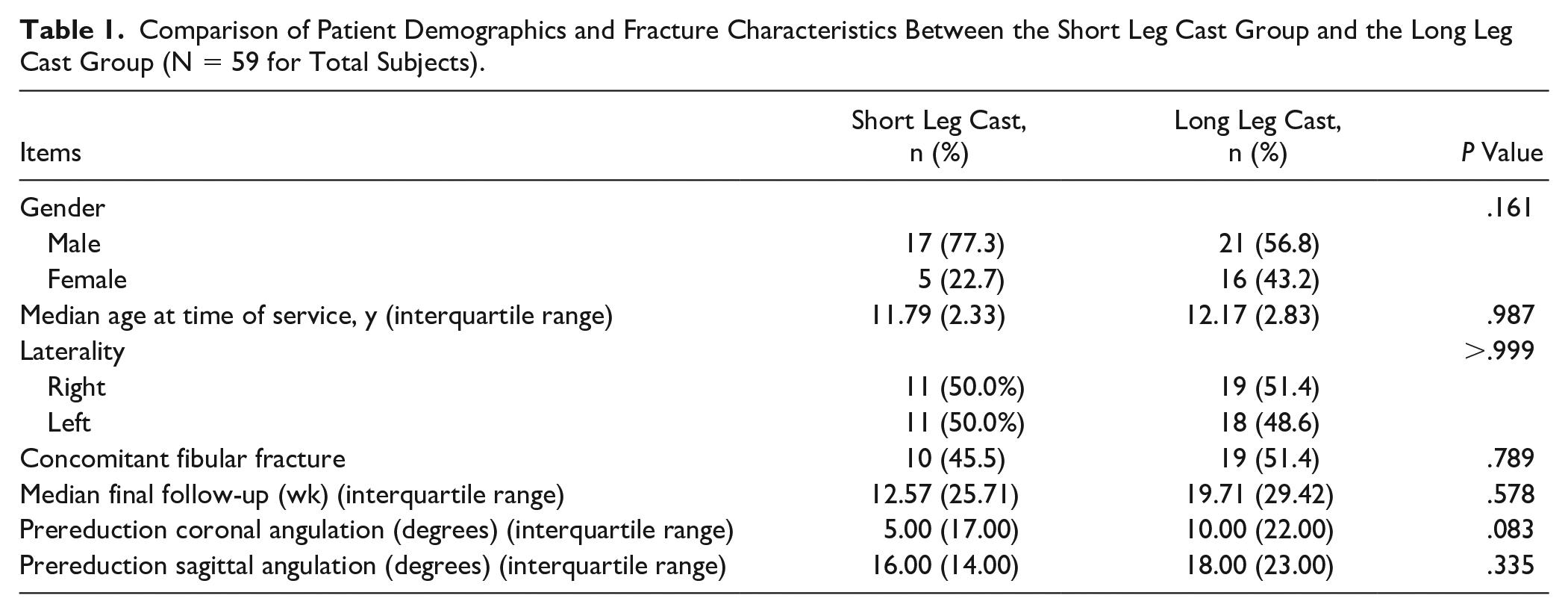
Among the 59 patients who were treated nonoperatively with casting for SH-II fractures, 22 patients were treated with an SLC (median age 11.79 years, IQR 2.33 years), and 37 patients were treated with an LLC (median age 12.17 years, IQR 2.83 years). The patient demographics and fracture characteristics are presented in Table 1. There was no significant difference between the groups regarding gender, median age at time of service, laterality of the fracture, concomitant fibular fractures, median final follow-up, baseline prereduction coronal angulation, or baseline prereduction sagittal angulation (P > .05).
Comparison of Patient Demographics and Fracture Characteristics Between the Short Leg Cast Group and the Long Leg Cast Group (N = 59 for Total Subjects).
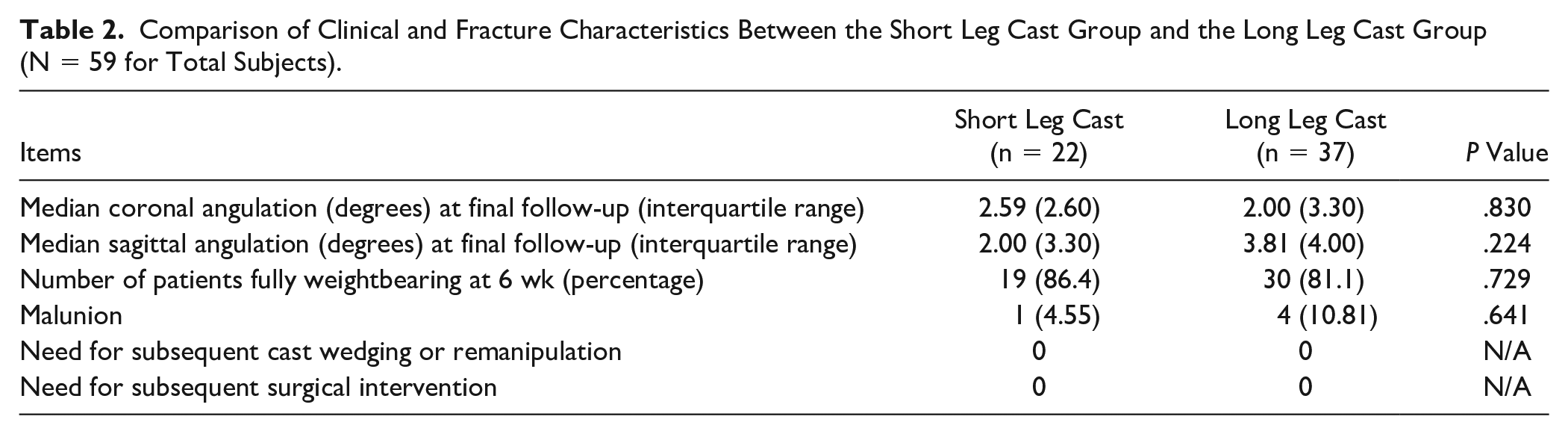
Coronal angulation at the time of final follow-up, sagittal angulation at the time of final follow-up, and percentage of patients fully weightbearing at 6 weeks were the 3 major clinical/radiographic outcomes of this study (Table 2). There was no significant difference in coronal or sagittal angulation between the 2 groups (P > .05). Additionally, there was no difference between the groups for the percentage of patients fully weightbearing at 6 weeks (P = .729). Moreover, for each casting group, there were no instances where subsequent cast wedging, subsequent remanipulation, or subsequent surgical intervention were needed (Table 2). There was no significant difference in the rate of malunion between the groups (P = .641).
Comparison of Clinical and Fracture Characteristics Between the Short Leg Cast Group and the Long Leg Cast Group (N = 59 for Total Subjects).
Discussion
The goals of treatment for pediatric ankle fractures include restoring joint congruency, the ankle mortise, lower extremity alignment, and physeal anatomy to preserve pain-free ankle function and normal growth as the patient matures into adulthood. To meet this expectation, many authors have favored restrictive and conservative protocols using long leg casts and nonweightbearing for distal tibial shaft or SH-II fractures.1,8,9 Although nonweightbearing protocols with LLCs have proven effective, authors had postulated on the benefits of treating low-energy closed distal tibial fractures with an SLC and weightbearing as tolerated to provide a greater degree of freedom to the patient and family during treatment. 10
In 2018, Limbu et al presented the first published data that directly compared SLCs against LLCs for middle and distal third tibial shaft fractures. 8 The authors designed a randomized prospective study with 60 patients and found no difference between the groups in mean union time (P = .379), mobility at the ankle (P = .702), or weightbearing status at 6 weeks (P = .766). Of note, the authors reported a significantly increased range of motion at the knee in the SLC group compared with the LLC group (P < .001). Moreover, residual knee and ankle stiffness was lower in the SLC group. Though this prospective study is promising, the authors did not compare their coronal or sagittal angulation outcomes between the groups and chose to compare their values to those reported in the literature. Additionally, the study was restrictive in its generalizability to distal tibial fractures as the authors did not report the number of midshaft vs distal shaft fractures included in the study and pooled both groups together.
More recently, Barnett et al 1 published a retrospective study comparing SLC outcomes against LLC outcomes for patients with fractures of the distal third of the tibial shaft. They presented a study on 85 children and reported that SLC groups achieved radiographic union at an earlier time (P = .026), there was no significant difference in final coronal angulation between the groups (P = .677), and there was a faster time to weightbearing in the SLC group (P = .0001). Although this study was well designed, the authors did not include distal tibial fractures associated with the metaphysis or physis or report final sagittal angulation outcomes, which is a critical component for evaluating alignment outcomes for weightbearing structures like the tibia.
An additional study by Thomas and Hennrikus in 2020 reported good efficacy for the management of SH-II distal tibial fractures with SLCs. 12 The authors concluded that many of these fractures can be treated solely with SLCs and without reduction, provided the maximum displacement is less than 3 mm. Although the authors noted no difference between the radiographic outcomes for the 2 groups, they did not report outcome values for either group, did not report their methodology for statistical analysis, and did not report values denoting statistical significance. Thus, it would appear their study was noncomparative in nature. Additionally, a subsequent 2021 study by Souder and Vaughan evaluated the outcomes of pediatric distal tibial physeal fractures treated with SLCs or patellar tendon bearing casts. 11 Like the study by Thomas and Hennrikus, the authors also reported good efficacy of SLCs for the management of distal tibial physeal injuries.
In an effort to better understand the role of SLC treatment for pediatric distal tibia fracture, this retrospective study was designed to directly compare outcomes between SLC- and LLC-treated patients with SH-II distal tibia fractures.1,8,11,12 The results from this study suggest that there is no significant difference in radiographic outcomes between patients treated with an SLC and patients treated with an LLC for the management of SH-II distal tibial fractures. For both casting groups, there was an equally low rate of malunion with no reported instances of remanipulation, cast wedging, or subsequent surgical intervention. These findings support the growing trend in the literature suggesting that SLCs are not an inferior treatment option to LLCs for distal tibial and ankle injuries. Proponents of the LLC cite better theoretical rotational control of the fracture leading to improved fracture outcomes, but the results presented in this study would suggest that the SLC provides an equivalent level of control and healing of the fracture site. 9 Although the SLC proved to be a viable therapeutic intervention for the management of SH-II tibial ankle fractures, there was no evidence in this study to suggest an increased percentage of patients fully weightbearing at 6 weeks relative to the LLC group. When combined with the results reported in prior studies, the data would suggest that SLCs have radiographically equivalent outcomes compared with LLCs for the nonoperative management of closed low-energy distal tibial fractures involving the diaphysis, metaphysis, or physis.
This study was limited in its retrospective nature. As a result, patients were not randomized, and the data were restricted to chart review, which is intrinsically limited by variability in clinical documentation between providers. Moreover, although our institution provides structured guidelines for follow-up for these injuries, there was some degree of variability in the follow-up timing for many cases. Radiographic outcomes have an intrinsic limitation based on the software and measurement tools. Additionally, the radiographic measurements were measured in a non-anonymized manner. Moreover, all outcomes were also limited by the number of patients involved in this study. Because of the lack of power analysis, there is an increased possibility for type II error. In the future, a well-designed, multicenter, randomized controlled study is necessary to determine if SLCs are viable treatment options for these fractures and to determine if there is a functional benefit to using an SLC over an LLC for SH-II distal tibial fractures. This study was also limited as it did not evaluate intraarticular SH fractures amenable to closed treatment methods. Well-designed future comparative studies are needed to address the efficacy of SLCs relative to LLCs for these challenging injury patterns as well.
This retrospective cohort study suggests that an SLC is a viable treatment option for the management of pediatric distal tibial SH-II fractures. Compared with LLCs, there was no significant difference in coronal or sagittal angulation at final follow-up. These results also suggested there was no statistically significant benefit regarding the percentage of patients fully weightbearing at 6 weeks when using an SLC for this injury pattern. Because of the limited number of SLC patients involved in this study, these results must be interpreted with caution.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114211069063 – Supplemental material for A Retrospective Comparison of Above- vs Below-the-Knee Cast Treatment for Salter Harris-II Distal Tibia Fractures
Supplemental material, sj-pdf-1-fao-10.1177_24730114211069063 for A Retrospective Comparison of Above- vs Below-the-Knee Cast Treatment for Salter Harris-II Distal Tibia Fractures by Suhas P. Dasari, Vasil V. Kukushliev, Alexander R. Graf, Xue-Cheng Liu and Scott E. Van Valin in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
Sergey Tarima, PhD, a member of the biostatistics department at the Medical College of Wisconsin, provided statistical consultation and outlined the plan for statistical analysis that was used for this study.
Authors’ Note
This work has been submitted as an abstract to the annual 2022 Orthopaedic Research Society meeting.
Ethical Approval
Ethical approval for this study was obtained from the IRB (1654383-3).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.