Introduction/Purpose: Deltoid ligament injuries are controversial in many aspects: the best method to assess the stability of a Weber B fibular fracture, the indications of deltoid repair after lateral side surgical fixation, the best technique of deltoid repair and the efficacy of superficial deltoid repair alone, compared to repair of both deep and superficial deltoid ligaments, to restore medial ankle stability. The last point is specifically important because of the technical difficulty of repairing the deep deltoid ligament, specially if performed after fixation of the fibular fracture and the syndesmosis, which is the common scenario. The aim of the study was to evaluate the ability of superficial deltoid repair without deep deltoid repair to restore medial ankle stability in cases of deltoid ligament injuries.
Methods: Ten fresh frozen ankle cadaveric specimens were used. Anteromedial dissection was performed to expose the ankle joint and to visualize the deltoid ligament. After good exposure, stress valgus and stress external rotation tests were performed with observation of the medial gutter and the medial part of the ankle joint for any widening. In all specimens, the ankle was stable at this point. Then, the superficial deltoid ligament was detached by sharp dissection from the medial malleolus followed by transection of the deep deltoid ligament completely at its midportion. Stress valgus and stress external rotation tests were repeated to demonstrate the gross instability of the ankle joint. Then, the superficial deltoid ligament was repaired using a suture anchor to the medial malleolus without any repair of the deep deltoid ligament. Then, stress valgus and stress external rotation tests were performed again to assess the medial ankle stability.
Results: All ankles were stable initially as confirmed by stress valgus and stress external rotation tests. After cutting both components of the deltoid ligament, the ankles were found to be grossly unstable using the same tests. After repair of the superficial deltoid, all ankles were stable again with a medial space equal to the initial status and with negative stress valgus and stress external rotation tests.
Conclusion: Surgical repair of the superficial deltoid ligament without repair of the deep deltoid ligament in cases of deltoid ligament injury may be sufficient to restore medial ankle stability. Limitations of the study include that all potential secondary restraints are intact in the cadaveric study compared to the actual situation where other structures like the capsular attachments may be injured especially if a fracture dislocation is encountered. Clinical trials are needed to confirm this finding.
DOI: 10.1177/2473011421S00001
Risk Factors for Nonunion Following Tibiotalocalcaneal Arthrodesis: A Systematic Review and Meta- Analysis
Amiethab A. Aiyer, MD; Sumit S. Patel, MS; Jose Perez, MD; Ettore Vulcano, MD; Jonathan R. Kaplan, MD
Introduction/Purpose: Tibiotalocalcaneal (TTC) arthrodesis is a routinely utilized salvage procedure that treats patients with severe talar and subtalar joint disease. Unfortunately, nonunion is a relatively common complication postoperatively which can increase risks and costs for patients. The goal of this study is to review the literature to identify risk factors for nonunion post TTC arthrodesis and stratify them based on strength of evidence. A meta-analysis will be performed on risk factors when appropriate to establish values based on pre-existing studies.
Methods: Five databases (CINAHL, Cochrane Library, EMBASE, MEDLINE, and Web of Science) were searched from inception to May 17th, 2020. Two independent reviewers screened abstracts and full-text articles for those that included risk factors predictive of nonunion for TTC arthrodesis. Any disagreements were discussed between the two reviewers and a third reviewer served as the ultimate decision maker if a consensus could not be reached. Relevant data regarding participants’ characteristics, study design, follow-up time, statistical tests and identified risk factors were extracted from the included studies. The two reviewers independently appraised the methodological quality of the studies using the Quality In Prognosis Studies tool. Those risk factors described in multiple studies were included in the meta-analysis. Random effects meta-analyses were summarized as forest plots of individual study and pooled random effect results. Results were reported as odds ratios (OR) with 95% confidence intervals (CI).
Results: Database search identified 428 articles, of which 113 were screened for full text. Eight studies involving 607 patients were included and 33 potential risk factors for nonunion were identified. Risk factors were stratified into demographic, preoperative, intraoperative and postoperative. Results of the meta-analysis established two significant risk factors for nonunion following TTC arthrodesis. Strong evidence supports that prior neurological deficits, such as Charcot neuroarthropathy and diabetes neuropathy, are associated with nonunion following surgery (OR: 2.86, 95% CI: 1.56 - 5.23). There was moderate evidence to suggest that preoperative infection was predictive for nonunion (OR: 3.99, 95% CI: 1.26 - 12.68). Although our meta- analysis did not find smoking (OR: 1.75, 95% CI: 0.90 - 3.38) or diabetes (OR: 2.28, 95% CI: 0.98 - 5.34) to be significant risk factors, multiple high quality studies support these as comorbidities that increase the likelihood of nonunion.
Conclusion: TTC arthrodesis can be an effective salvage procedure but is associated with high nonunion rates. The results of our meta-analysis suggest that prior neurological deficits, such as Charcot neuroarthropathy or diabetes neuropathy, have strong evidence for failure to achieve union. Although our meta-analysis did not find other statistically significant risk factors, the findings of individual studies in our review suggest that diabetes mellitus and smoking are both factors which can lead to failure of fusion. Surgeons should be cognizant of these risks when performing TTC arthrodesis and carefully monitor patients with the aforementioned comorbidities to achieve successful results.
DOI: 10.1177/2473011421S00002
Cavovarus with A Twist: Coronal and Axial Plane Rotational Deformity in the Midfoot of Charcot- Marie-Tooth Patients
Tonya W. An, MD; Edward T. Haupt, MD; Max Michalski, MD; Jari Salo; Glenn B. Pfeffer, MD
Category: Hindfoot; Midfoot/Forefoot
Keywords: Charcot Marie Tooth; Cavovarus Foot Deformity; Weight Bearing CT
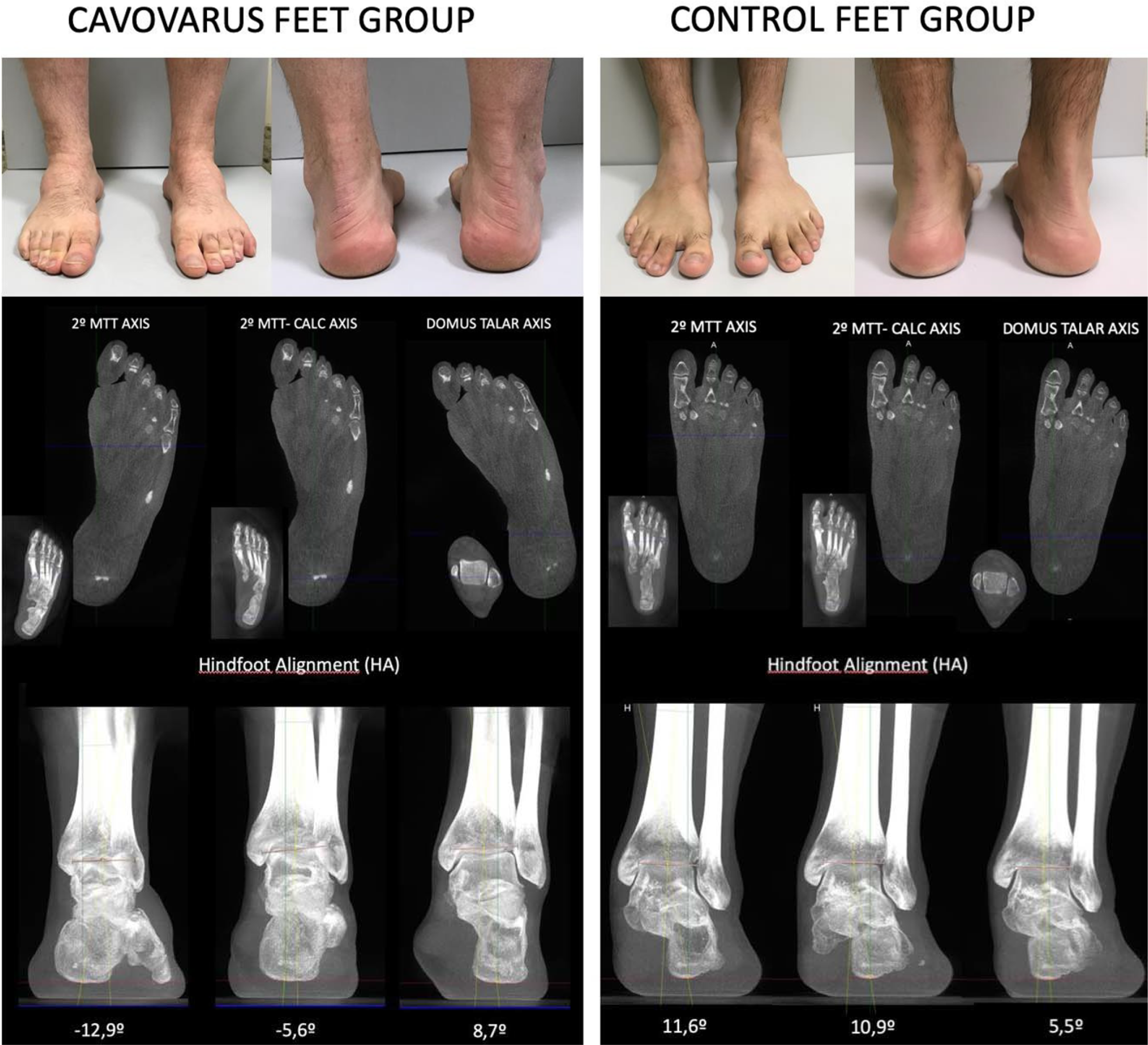
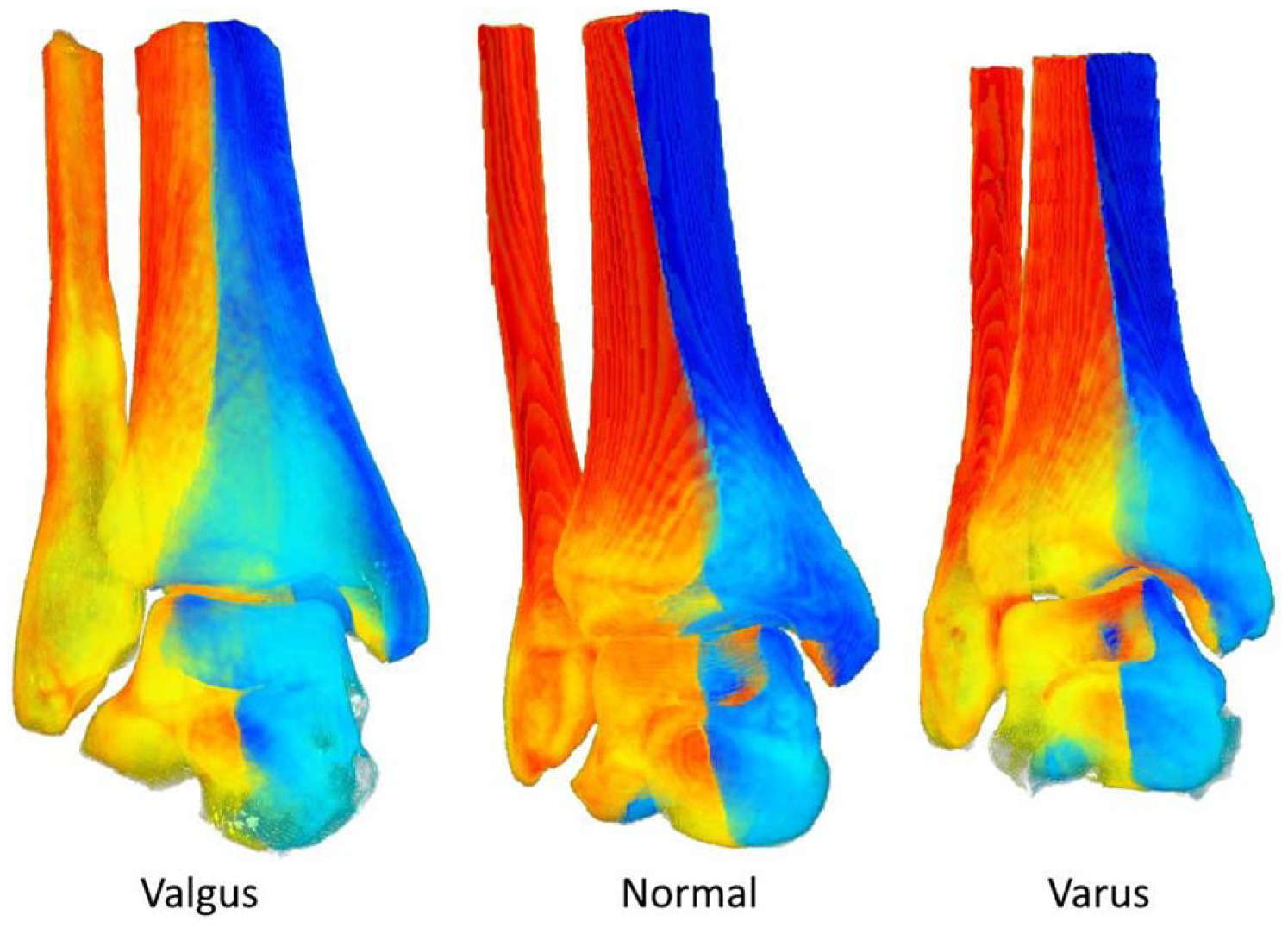
Introduction/Purpose: The cavovarus deformity of Charcot-Marie-Tooth (CMT) disease typically presents with hindfoot varus and forefoot valgus. This seemingly paradoxical relationship is poorly understood. Better insight into this complex three- dimensional alignment under physiologic load-bearing conditions is possible using weight-bearing computed tomography (WBCT). This is the first study to examine the extreme rotational deformity in the midfoot of CMT patients, and thereby provides a key to the successful operative correction of the CMT cavovarus foot.
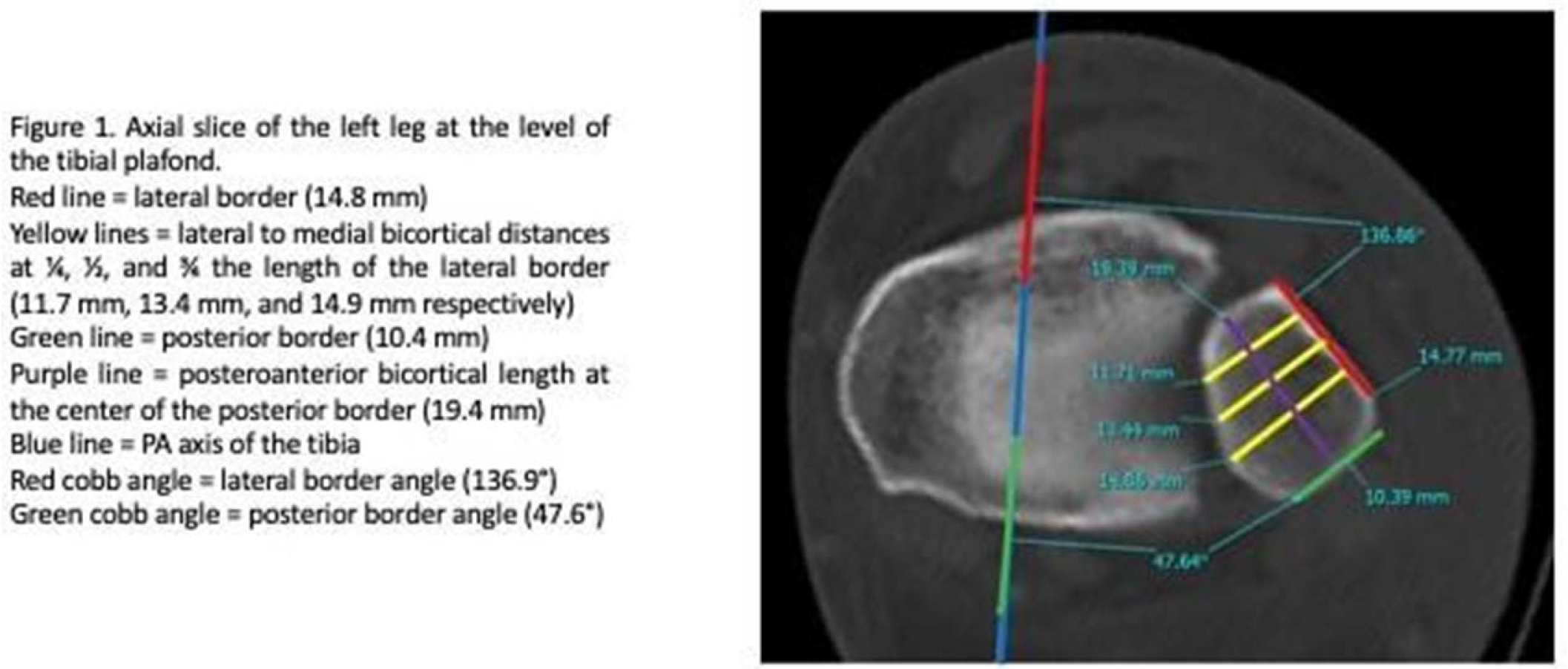
Methods: We retrospectively reviewed the WBCTs of patients with CMT who presented to a single surgeon. Those with history of bony surgical correction, severe degenerative joint disease, or open physes in the foot, were excluded. Scans were analyzed using three-dimensional analysis software (Disior Bonelogic) to generate axes of select bones and their relationship relative to the tibial plafond anterior-posterior axis in the axial plane. The coronal alignment of the foot involved angular measurements of the calcaneus, talar dome, midfoot and forefoot relative to the ground. We reported quantitative alignment parameters and compared the measurements to WBCT of 20 controls.
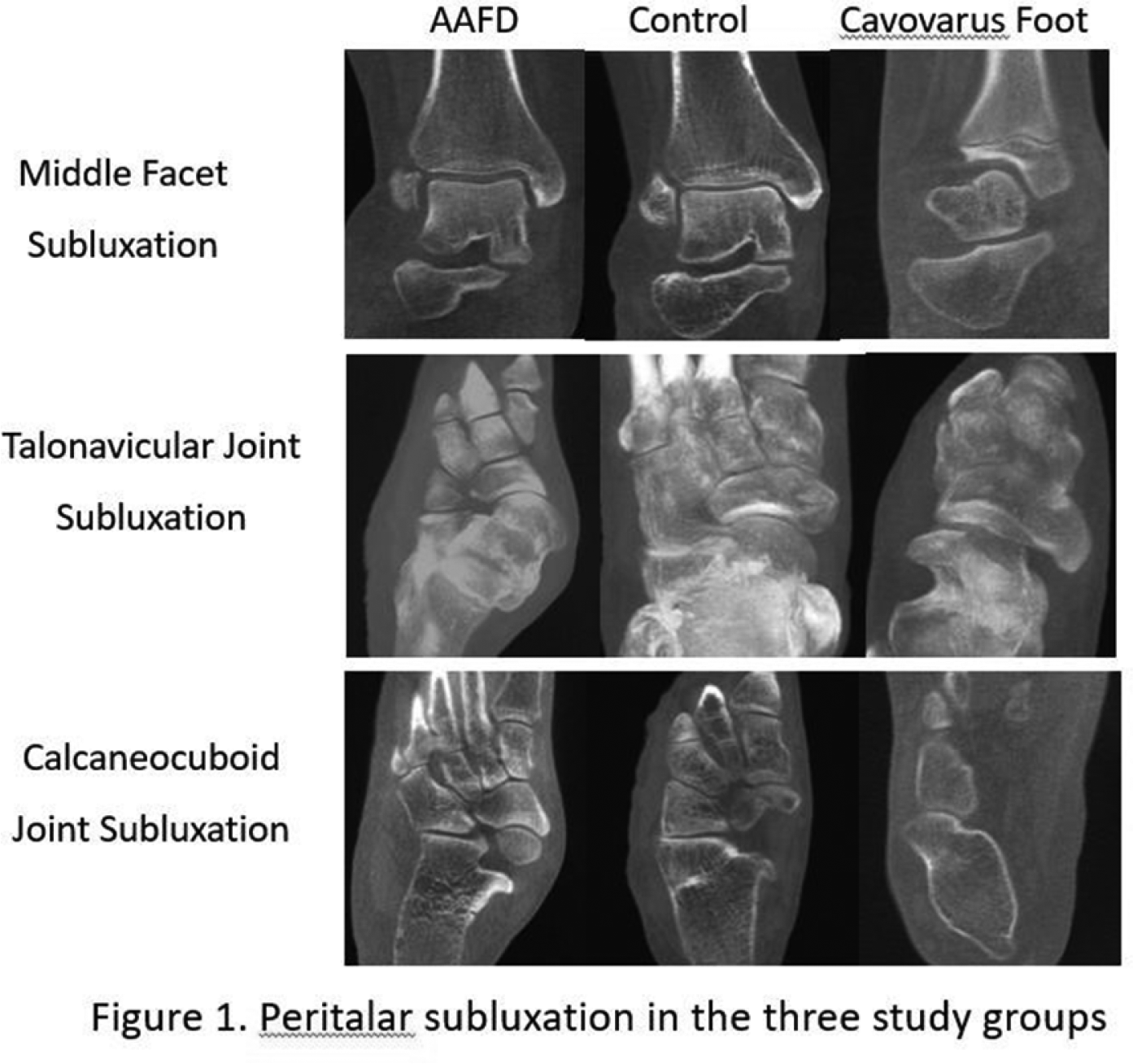
Results: 17 WBCT scans from 15 CMT patients (average age 24 years) met criteria for inclusion. In the axial plane, external rotation of the distal tibia accounted for the varus heel position rather than subtalar malalignment. The greatest change in axial alignment occurred between the talar neck and navicular (26 degrees). The average talonavicular (TN) medial uncoverage angle was -15 degrees for CMT patients, indicating medial overcoverage, compared to +11 degrees for controls, (p<0.01). Coronal plane analysis revealed varus rotational deformity at the calcaneus (23 degrees), a peak of 61 degrees varus across the navicular and cuboid, then compensatory rotation of the cuneiforms and metatarsals to achieve a plantigrade forefoot (11 degrees varus). In comparison, controls averaged 9 degrees coronal valgus at the calcaneus and 34 degrees varus at the naviculo-cuboid level, (p<0.01). Figure 1 shows the WBCT scans of a representative CMT patient and control case.
Conclusion: This three-dimensional WBCT analysis is the first to characterize and quantify the axial and coronal rotational deformity in CMT. Axial plane deformity had a center of rotational angulation at the talonavicular joint, associated with medial ’overcoverage’ of the talar head, likely from chronic tibialis posterior over-pull. The peak coronal deformity was localized at the navicular and cuboid, which measured nearly twice as much as controls. These observations suggest dorsiflexion osteotomy of the 1st metatarsal would fail to address the coronal rotation; releases through the talonavicular joint may be necessary to abduct and de-rotate the midfoot to achieve a plantigrade foot.
DOI: 10.1177/2473011421S00003
Strength and Compressive Ability of Midfoot Fusion Nail vs Midfoot Fusion Bolt and Role of Subtalar Fusion
Victor Anciano, MD; D. Barcel, MD; Phillip Kaiser, MD; Nahir Habet, PhD; Co-Author -Todd A. Irwin, MD; Carroll P. Jones, III, MD
Introduction/Purpose: Surgical management of midfoot Charcot arthropathy typically includes fusion through the midfoot to obtain a stable plantigrade foot. Multiple surgical strategies exist, including variable combinations of internal fixation with plates, or thin wire external fixator frames, or both. More recently, intramedullary beams and bolts have been used as an alternative means of fixation. The current understanding of midfoot fusion lacks knowledge of how much stiffness, strength and compression is provided using two different intramedullary midfoot fusion devices. The purpose of this study is to assess 3 point bending strength of midfoot fusion nails versus bolts as well as to test their compressive abilities. Additionally, we looked to assess how the addition of a subtalar fusion affects midfoot stiffness and rotational control in a cadaver model.
Methods: Bone blocks and cadaver feet were used for compression and biomechanical testing, respectively. Bone blocks were pre-drilled with an undersized pilot bit and then cut in two. A washer-type load cell measured the compressive force produced by the implants. Sixteen (8 nails and 8 bolts) compressive tests were performed. Ten matched cadaver foot specimens were prepared, and medial column fusions were performed with midfoot fusion nails or bolts (10 each). Another ten matched specimens were prepared evaluating midfoot fusion nails with or without subtalar fusions. Specimens were placed on a custom platform at 20 degrees of dorsiflexion. A linear variable differential transformer (LVDT) was used to record local displacement at the midfoot (Figure 1). Each specimen underwent 3000 cycles of compressive loading (200N - 1000N) followed by displacement- controlled loading to 9mm of total axial displacement via servo-hydraulic test frame. The Wilcoxon signed rank test (paired analysis) was used for analysis.
Results: The overall performance between nail vs bolt matched specimens or between nail only vs nail with subtalar fusion showed no statistical difference with regards to stiffness. The compressive force tests show the nail to be significantly stronger in all aspects of the analysis. When comparing nail vs bolt matched specimens, only the accumulated height drop at the end of cycling was significantly different (p=0.008). For the nail only VS nail with subtalar fusion, only the displacement before fatigue was significantly different (p=0.035). There was no difference among the matched pairs with regards to stiffness, displacement after fatigue or maximum force during load to failure.
Conclusion: This study highlights important biomechanical and compressive data comparing midfoot fusions using nails vs bolts. The compressive force test of nails was superior to bolts. This could provide valuable insight when considering implants for arthrodesis. The overall comparison between matched pairs of nails vs bolts did not provide significant differences among those groups. Similarly, adding a subtalar fusion did not provide significant mechanical improvement based on this model. The clinical utility of these findings is limited by the difficulty in recreating a Charcot like scenario using cadavers.
DOI: 10.1177/2473011421S00004
Risk Factors for Postoperative Falls in Foot and Ankle Surgery
Nicholas A. Andrews; Jared R. Halstrom, BS; Kenneth J. Fellows; Austin Hughes; David A. Patch, MD; Whitt Harrelson; Tanvee Sinha; Ashish Shah, MD
Introduction/Purpose: Falls following orthopaedic surgery are a known entity in the healthcare field possessing significant patient morbidity and driving increased healthcare cost. The vast majority of studies have focused on the incidence and risk factors for postoperative falls in the inpatient setting, however, this is in direct contrast to shifts seen toward same-day outpatient orthopaedic surgery over the past decade. It is crucial to better understand the incidence and risk factors for falls in a mixed inpatient and outpatient model. Additionally, no study to date has examined the risk factors for falls after foot and ankle surgery.
Methods: A total of 168 patients were administered a questionnaire and interviewed to investigate the incidence of postoperative falls. Patients completed surveys pertaining to fall history pre- and post-operatively, fall risks, current medical status, and use of an ambulatory assist device. Medical records were reviewed. Questionnaires and interviews were completed at 2 week and 6-week post-operative follow up visits. Factors found to be associated with postoperative falls in univariate analysis (p<.05) were included in a binary logistic regression model.
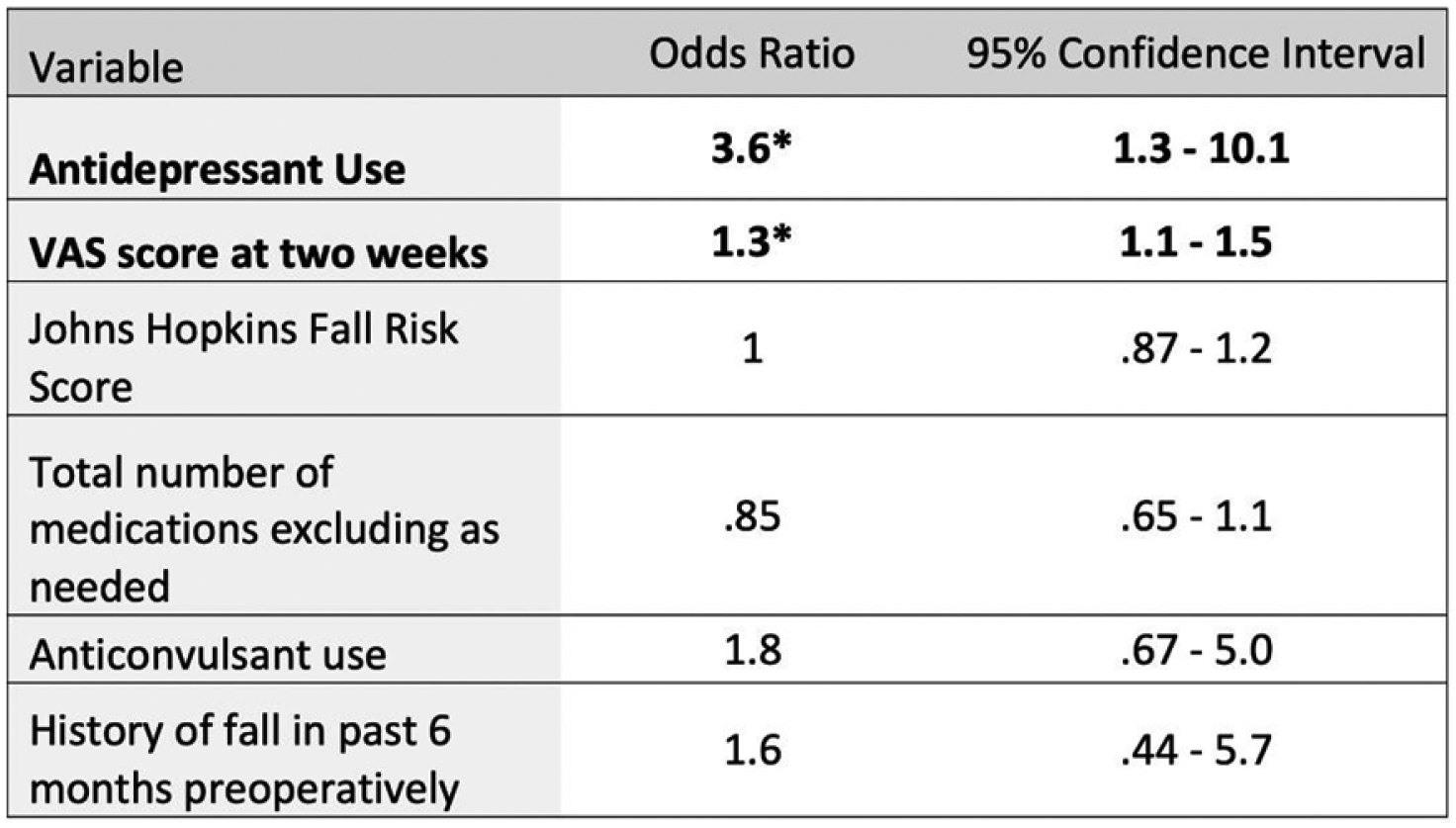
Results: Full six-week follow-up was present in 138 patients. A total of 87 (63.0%) females and 51 (37.0%) males with a median age of 52 (21 IQR) and BMI of 32.4 (11 IQR) were included. The total fall incidence in the first six postoperative weeks was 29.7% (41 patients). In multivariate analysis, antidepressant use and VAS score at two weeks postoperatively were independently associated with falls OR 3.6 (95% CI 1.3 - 10.1) and OR 1.3 (95% CI 1.1 -1.5), respectively. The results of other variables included in the model were as follows: The Johns Hopkins Fall Risk Score OR 1.0 (95% CI.87-1.2), total number of medications excluding as needed OR.85 (95% CI.65-1.1), anticonvulsant use OR 1.8 (95% CI.67 - 5.0), and history of falls in the past six months preoperatively 1.6 (.95% CI.44 - 5.7).
Conclusion: The high outpatient fall rate in foot and ankle surgery warrants awareness of risk factors. Antidepressant use has been associated with falls, but has not been established as a risk factor for postoperative falls. Surgeons should be aware of the risk of postoperative falls in this patient population. The postoperative VAS score at two weeks was also shown to be independently associated with falls. Adequate postoperative pain control is vital to minimize such falls. This study has identified antidepressant use and postoperative VAS score at two weeks as two independent risk factors for postoperative falls in foot and ankle surgery.
DOI: 10.1177/2473011421S00005
Functional Outcomes and Deformity Correction of Double vs Triple Arthrodesis in Stage III Posterior Tibial Tendon Insufficiency. A Prospective Cohort Study
Ahmed K. Attia, MD; Amr A. Mohammed; Wael El-Adly, MD; Mo’men M. Mohamed, MSc; Aly Mohamadean, MD; Ahmed E. Osman, MD
Introduction/Purpose: Posterior tibial tendon insufficiency (PTTI) remains the most important contributor to AAFD. When the deformity becomes rigid, management options are limited to arthrodesis. Triple arthrodesis is considered the gold standard for treating painful, rigid flatfoot deformities with proven long-term reliability of correction and favorable functional outcomes. However, the necessity of fusing an unaffected calcaneocuboid joint has been questioned, and double arthrodesis has been suggested as an alternative to triple arthrodesis. The double arthrodesis has been proven to restore function, provide a plantigrade foot, and protect against postoperative ankle valgus. This study aims to prospectively compare double and triple arthrodesis in terms of functional outcomes and deformity correction. To the best of our knowledge, this is the first prospective comparative study in the literature to date.
Methods: This is a prospective comparative cohort study carried out between May 2017 and May 2019. The study was approved by the IRB at Assiut University and done according to the Helsinki declaration. Patients with AAFD stage III aged between 15 and 40 years old were assigned to double arthrodesis or triple arthrodesis. The groups were prospectively followed for one year. Primary outcomes were union rates, AOFAS scores, and radiological parameters of deformity correction plain radiographs. Secondary outcomes were operative time, time to union, and complications. Twenty-three patients matched the inclusion criteria. Thirteen (all males) patients underwent double arthrodesis, while ten (nine males and one female) patients underwent triple arthrodesis. The mean age for double and triple arthrodesis was 20.15+-5.63 and 25.10+-8.36 years, respectively, and the mean follow-up lengths were 12.46 and 12.9 months, respectively, with no statistically significant differences in age, follow-up or gender between both groups.
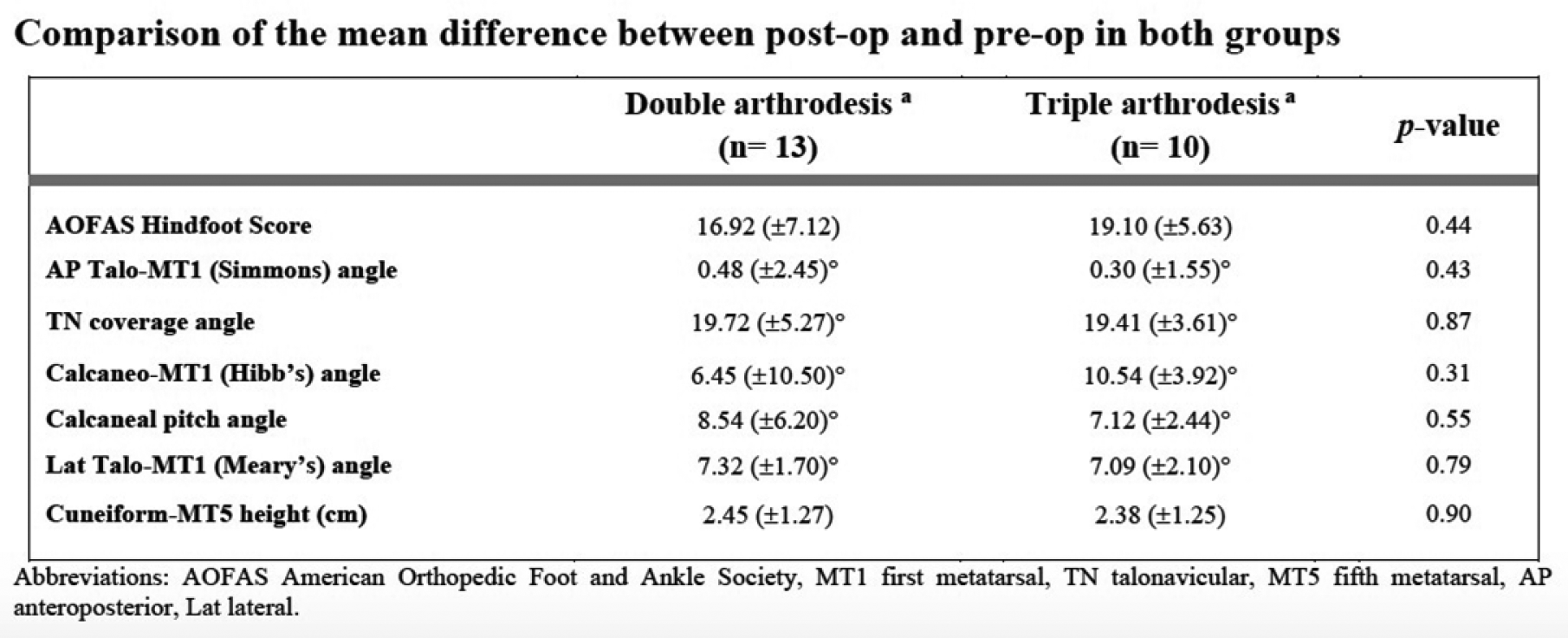
Results: All patients in both groups achieved union by four months. The mean time to union in the double and triple arthrodesis groups was 3.39+-0.65 vs. 3.31 +-0.6 months, respectively, with no statistically significant differences (P=0.77). The mean operative time in the double arthrodesis group than the triple arthrodesis group, 55.77+-15.18 vs. 91.6+-24.14 minutes (P<0.001), respectively. Both double and triple arthrodesis groups had a statistically significant improvement of the mean AOFAS hindfoot score postoperatively (71.46 +-7.77 vs. 88.38 +-3.66, P<0.001) and (66.9 +-7.69 vs. 85 +-5.83, P<0.001), respectively. Both double and triple arthrodesis groups had statistically significant improvement of preoperative Meary’s angle, calcaneal pitch, Cal-MT5 height, calc-MT1 angle, and TN coverage angle postoperatively. There were no statistically significant differences between double vs. triple arthrodesis groups in AOFAS score improvement or the magnitude of deformity correction.
Conclusion: Double arthrodesis is an equally reliable surgical option for AAFD stage III for achieving union, improving the functional outcomes, and deformity correction as triple arthrodesis with a significantly shorter operative time in the former. The authors recommend double arthrodesis if the calcaneocuboid joint is unaffected.
DOI: 10.1177/2473011421S00006
Alignment of the Hindfoot Following Total Knee Arthroplasty: A Systematic Review
Mohammad Azam; James J. Butler; Nathaniel P. Mercer; Eoghan T. Hurley, MB BCh BAO; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle; Hindfoot
Keywords: Hindfoot; Valgus; Ankle
Introduction/Purpose: The purpose of this systematic review was to evaluate changes in the alignment of the hindfoot following total knee arthroplasty (TKA), subjective clinical outcomes following surgical intervention and to analyze the level of evidence (LOE) and quality of evidence (QoE) of the included studies.
Methods: MEDLINE, EMBASE, and Cochrane Library databases were systematically reviewed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies reporting changes in the postoperative alignment of the hindfoot following TKA were included. The level and quality of evidence were recorded and assessed.
Results: Eleven studies with a total of 1142 patients (1358 knees) met the inclusion/exclusion criteria. Six studies were of level of evidence II and 5 studies were of level of evidence III. Patients with preoperative varus knee deformity and valgus hindfoot deformity demonstrated improvement in hindfoot alignment post-TKA. Patients with preoperative varus knee deformity and varus hindfoot deformity demonstrated no improvement in hindfoot alignment following TKA. Twelve different radiographic parameters were used to measure the alignment of the hindfoot across the included studies, with the tibio-calcaneal angle (TCA) most frequently utilized (27.3%).
Conclusion: This systematic review demonstrated that the hindfoot may display compensatory changes in alignment following total knee arthroplasty in patients with knee osteoarthritis. However, the marked heterogeneity between the included studies and poor quality of evidence limits any meaningful cross-sectional comparisons between studies. Further, well-designed studies are necessary to determine the changes and outcomes of hindfoot alignment following total knee arthroplasty.
DOI: 10.1177/2473011421S00007
WBCT Can Effectively Diagnose Syndesmotic Instability Among Patients with Weber B Ankle Fractures
Rohan Bhimani, MD, MBA; Soheil Ashkani-Esfahani, MD; Bart Lubberts, MD, PhD; Philip Kaiser, MD; Lorena Bejarano-Pineda,
MD; Gino Kerkhoffs, MD; Gregory R. Waryasz, MD; Christopher W. DiGiovanni, MD; Daniel Guss, MD, MBA
Introduction/Purpose: Diagnosing and treating syndesmotic instability that occurs in some Weber B ankle fractures is essential to restore normal ankle joint kinematics and optimize clinical outcomes however subtle instability can be difficult to identify. WBCT evaluates the syndesmotic joint under physiologic load. We compared the diagnostic sensitivities of one-dimensional (1D) distance, two-dimensional (2D) area, and three-dimensional (3D) volumetric measurement of the injured syndesmotic joint on WBCT, in patients with unilateral Weber B ankle fractures with surgically-confirmed syndesmotic instability, to the contralateral uninjured side.
Methods: Patients with unilateral surgically confirmed syndesmotic instability accompanying a Weber B type lateral malleolar ankle fracture (n = 23) who underwent preoperative bilateral foot and ankle WBCT were included. A separate group of patients with unilateral Weber B ankle fractures without syndesmotic instability and who underwent bilateral WBCT were included as a control group (n = 18). With the uninjured side serving as an internal control, measurements on bilateral WBCT images included: 1) syndesmotic area, 2) tibiofibular distance measured at the anterior, middle, and posterior aspect of the distal tibiofibular articulation, 3) fibular rotation, 4) distance from fibular tip to plafond, 4) fibular fracture displacement and 5) medial clear space distance. In addition, 3D volumetric measurements: 1) syndesmotic joint volume from the tibial plafond extending to 3cm and 5cm proximally, respectively 2) medial clear space volume, and 3) lateral clear space volume were calculated, and their sensitivities were compared to the aforementioned measurements.
Results: Among patients with unilateral syndesmotic instability with Weber B ankle fractures, all WBCT measurements except medial clear space distance, syndesmotic area, and anterior and posterior tibiofibular distance were significantly greater on the injured compared to the uninjured side (p-values ranging from <0.001 to 0.004). Of these measurements, 3D syndesmosis volumetric measurements spanning from the tibial plafond to a level 3cm and 5cm proximally had the highest relative volumetric ratio between the injured and uninjured side, suggesting high sensitivity to distinguish between stable and unstable syndesmotic injuries (p -values ranging from 0.001 to 0.036). In the control group without syndesmotic instability, all evaluated WBCT parameters except for MCS volume, and distal fibular tip to tibial plafond showed no significant side-to-side difference.
Conclusion: Bilateral WBCT can effectively diagnose syndesmotic instability among patients with Weber B ankle fractures. While middle incisura distance, fibular rotation, and 3D volumetric measurements can all be used to identify such instability, 3D syndesmotic volume measurements are the most sensitive and thus strongly recommended for future application in scenarios of clinical dilemma of syndesmotic injury-particularly when injuries are subtle. When performing these 3D volume measurements, it appears that syndesmosis volume extending from the tibial plafond to a height of 5cm proximally is best suited to evaluate such instability given the larger absolute side to side difference of 3.5 cm3.
DOI: 10.1177/2473011421S00008
Correction of the Hindfoot Alignment after Supramalleolar Osteomy in Ankle Varus Deformity - A Three-Dimensional Analysis Using Weightbearing CT
Arne Burssens; Peter Kvarda; Caspar S. Steiner, MD; Roman Susdorf, PhD; Ursina Peterhans; Nicola Krahenbuhl, MD; Alexej Barg, MD; Roxa Ruiz, MD; Beat Hintermann, MD
Introduction/Purpose: While correction of varus alignment at the level of the ankle joint has been investigated extensively after supramalleolar osteotomy (SMOT), the effect on the hindfoot alignment remains unclear. This can be attributed to the limitations of former 2-dimensional radiographic measurements used to quantify the complex 3-dimensional subtalar joint alignment. Therefore, we aimed to determine both the ankle and subtalar joint alignment before and after SMOT using a weightbearing CT and autogenerated 3-dimensional measurements.
Methods: Twenty-seven patients with a mean age of 53 years (SD=10.1; range=25-73) were retrospectively analyzed in a pre- post study design using weightbearing CT images. Inclusion criteria were correction of ankle varus deformity by either an opening wedge (N=19) or dome osteotomy (N=8). Exclusion criteria consisted of an additional inframalleolar bony correction, i.e. calcaneal osteotomy or subtalar arthrodesis. Corresponding three-dimensional bone models were reconstructed to compute the autogenerated measurements: tibial anterior surface (TAS) -, tibiotalar surface (TTS)-, talar tilt (TT) - and talocalcaneal (TC) angle.
Results: The pre-operative (TAS=86.9°, SD=4.9; TTS=79.8°, SD=5.6; TT=8.8°, SD=4.3) radiographic parameters of the ankle joint alignment improved significantly compared to the post-operative parameters (TAS=92.4°, SD=4.9; TTS=87.1°, SD=6.3; TT=5.1°, SD=2.7; P<0.05). (Fig. 1A) Radiographic parameters to assess the subtalar joint alignment improved significantly from preoperatively (TCax =42.8°, SD=9.3; TCsag=42.3°,SD=10.9; TCcor =29.5°,SD=11.8) to post-operatively (TCax =37.8°, SD=8.8; TCsag=39.1°, SD=10.6; TCcor=24.6°,SD=9.1; P<0.05). (Fig. 1B)
Conclusion: A supramalleolar osteotomy is able to correct both the ankle and subtalar joint alignment. However, correction at the level of the subtalar joint accounted for only 3 to 4 degrees, which was less than found for the ankle joint alignment. For cases where a higher correction at the subtalar joint is necessary, we thus suggest adding a calcaneal osteotomy or subtalar arthrodesis to the SMOT.
DOI: 10.1177/2473011421S00009
Treatment and Outcomes of Atraumatic Subtalar Dislocations in Adult Acquired Flatfoot Deformity
Shaun Chang; Joan R. Williams, MD; Bruce J. Sangeorzan, MD
Category: Ankle; Hindfoot
Keywords: AAFD; Hindfoot Deformity; Fusion
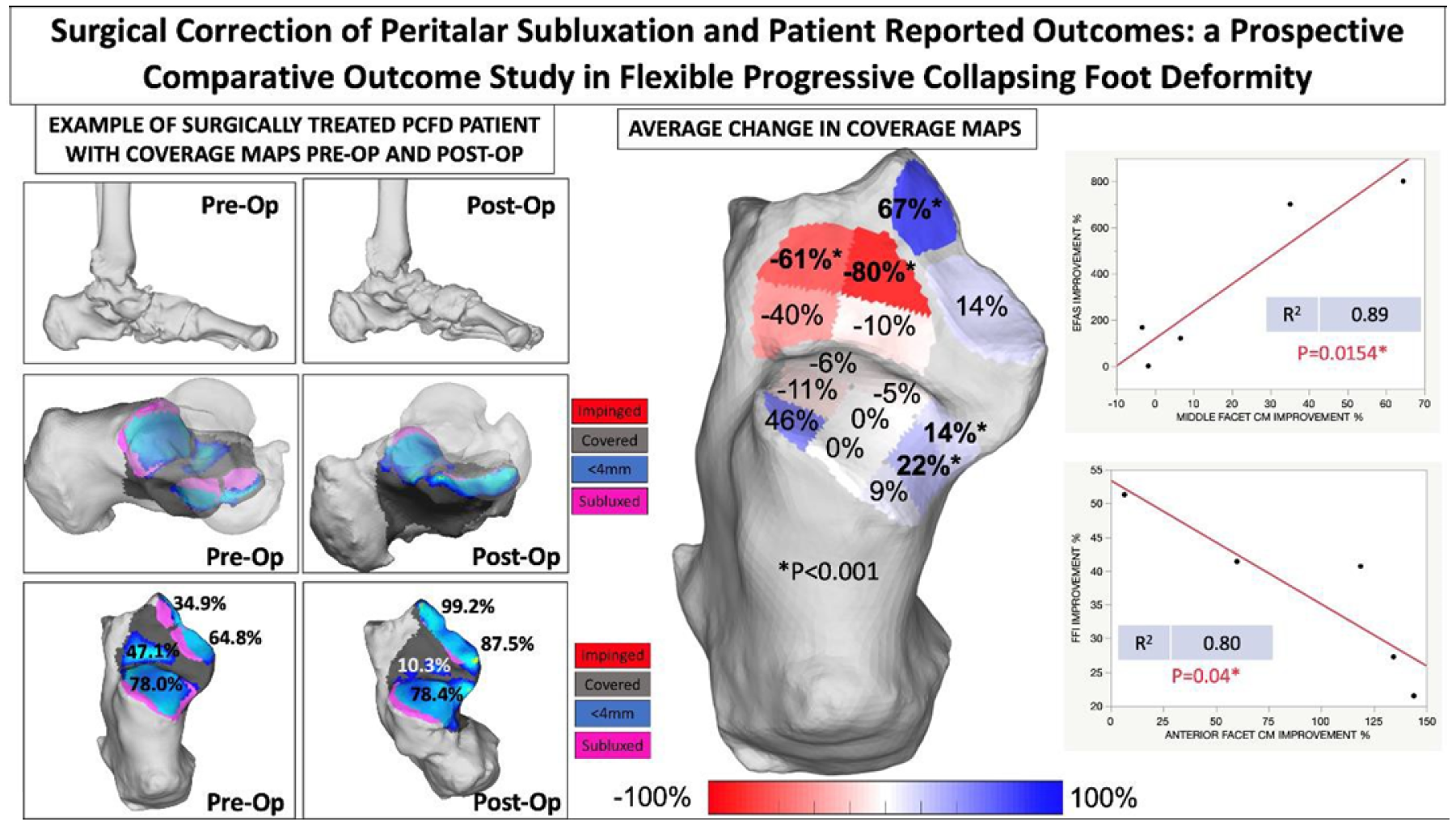
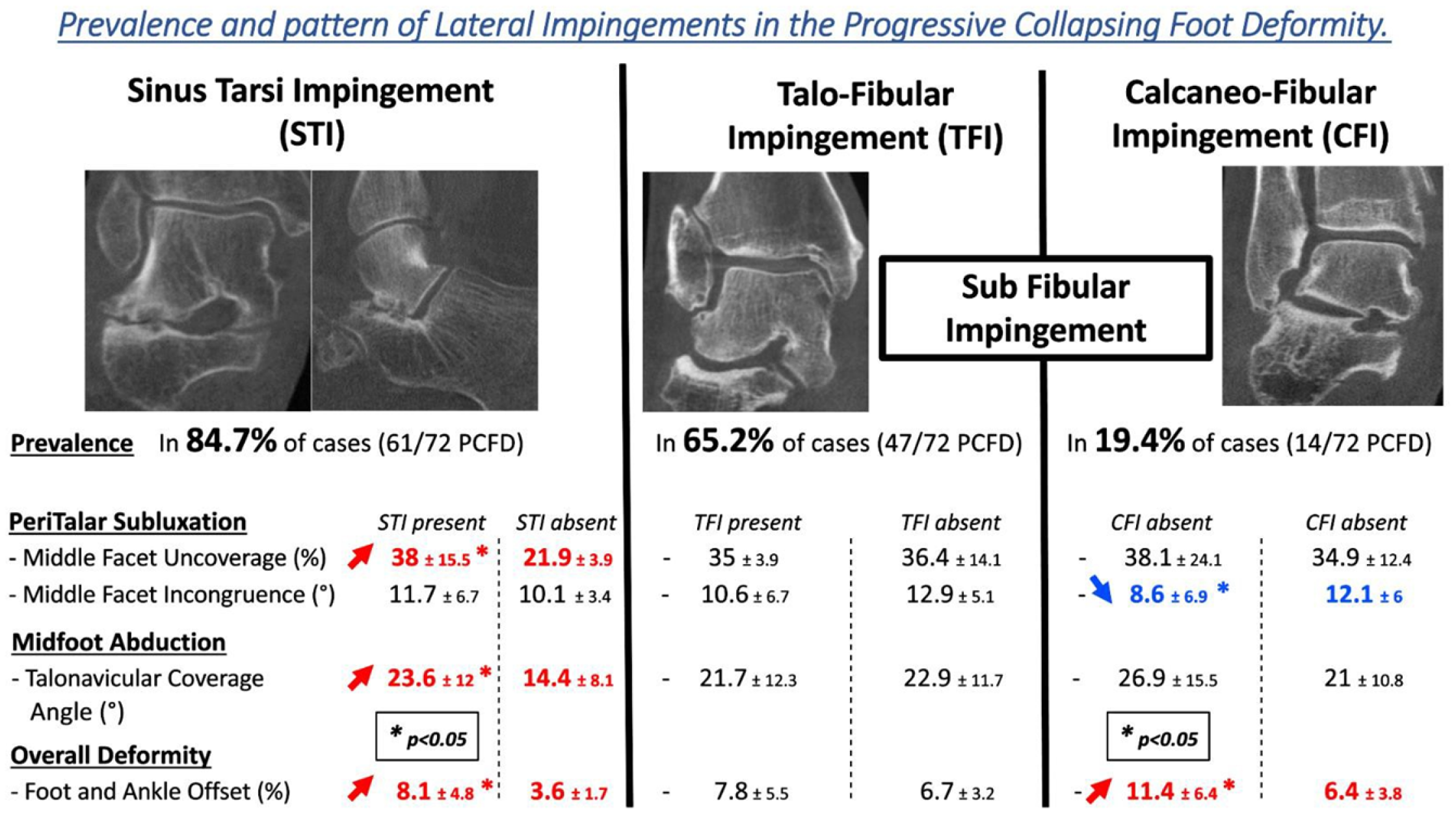
Introduction/Purpose: Painful adult acquired flatfoot is classified into multiple types, with a one category reserved for those that have rigid deformity. However, there is a subset of patients with rigid progressive collapsed foot deformity (PCFD) in which navicular and calcaneus are subluxed from the talus causing sub-fibular impingement and erosion and fixed abduction of the forefoot. This condition is not well described in the literature. The treatment of these patients can be technically difficult given the attenuation and erosion of soft tissue and articular constraints. In this study we sought to identify reduction technique, shared characteristics, treatments, and outcomes in patients with severe hindfoot valgus deformity with subluxation and subfibular impingement who were treated by subtalar reduction and arthrodesis, and talonavicular arthrodesis at a single institution.
Methods: A retrospective chart review was done of all patients who underwent flat foot reconstruction by a single surgeon. Patient were included in the study if on preoperative weight-bearing (WB) CT they met the following radiographic criteria: 3 sequential sagittal cuts of the calcaneus without the talus present, 3 sequential sagittal cuts of the talus without the calcaneus present, and the presence of a calcaneofibular articulation on coronal cuts. Patients with neuromuscular disorders or peripheral neuropathy were excluded. This review evaluated demographic data, comorbidities, complications, and the need for reoperation. Plane radiographs and CT findings were compared to identify subluxation on plane images. Patients were treated with a double, triple, or pantalar arthrodesis based on the treating surgeon’s discretion. A cohort of 23 patients has already been identified, but additional data review is currently underway.
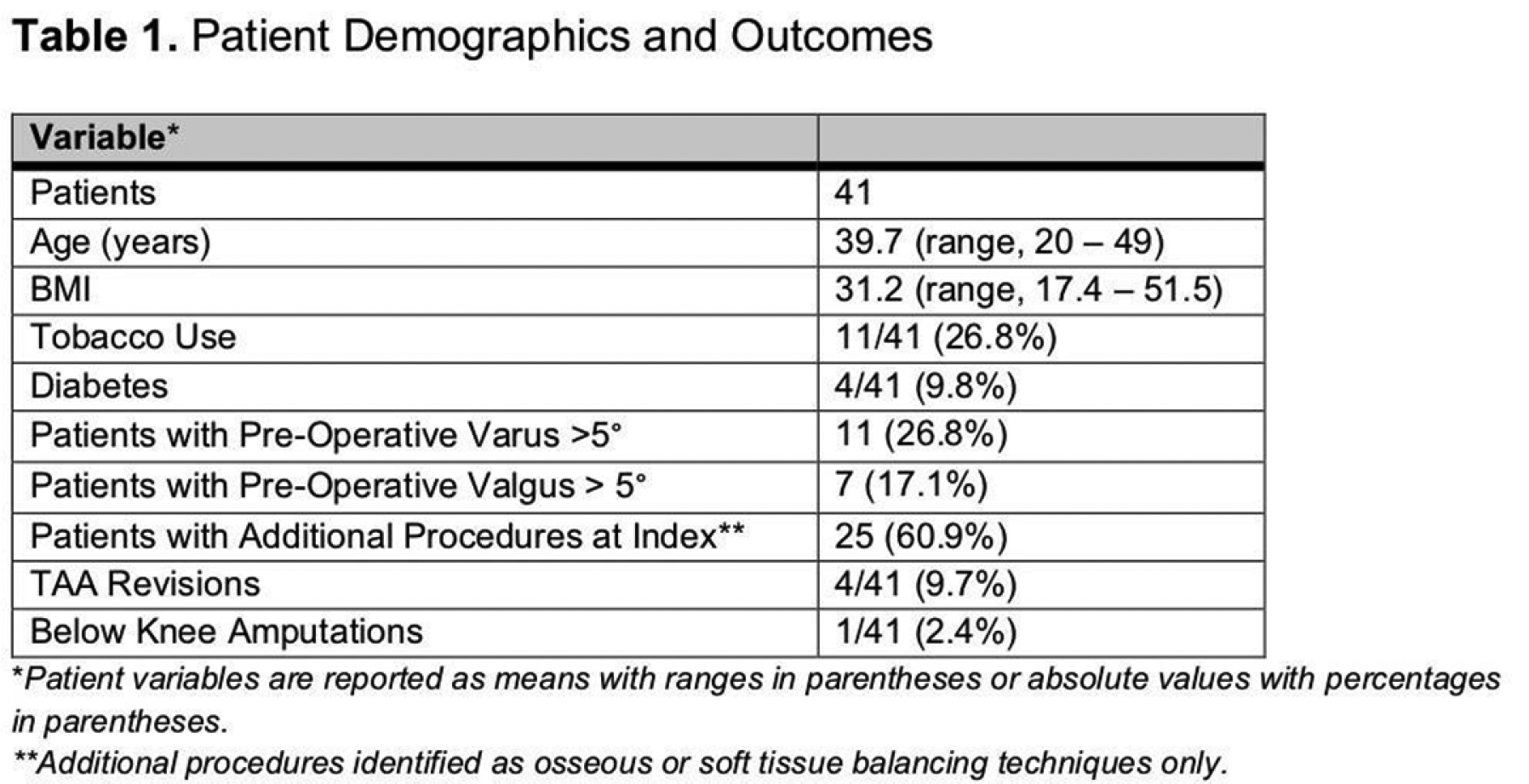
Results: The initial patient cohort consisted of twenty-three patients who met the inclusion criteria with an average age of 64.5 (range, 48-79) years. The initial cohort consisted of patients who were treated from 2009-2014. Seven of the twenty-three patients (30.4%) required reoperation for various reasons ranging from late infection to nonunion and symptomatic hardware (Table 1). We found that the average BMI for patients with this disorder was 34kg/m2. Four patients have fibular stress fractures on presentation, these patients had an average BMI of 41.6kg/m2. Specific techniques for reduction included use of distractors at subtalar and TN joints. Radiographic findings on plane films are linked to findings on CT scan. Recurrence of deformity occurred with tilt of the talus requiring bracing in 2 patients. Incomplete correction was common, particularly early in the study period.
Conclusion: PCFD is a very problem seen by foot and ankle surgeons. Physicians should be aware of the challenges presented in treating the subset of patients who have atraumatic dislocation of the subtalar joint. Diagnosis can be made on plane radiographs, though WB CT is useful for treatment planning. Treatment of these patients requires careful physical and radiographic examination. Reduction and arthrodesis is the treatment of choice. Patients should also be counseled about the possible need for reoperation given the high rate of reoperation in this population.
DOI: 10.1177/2473011421S00010
Long Term Outcome Measures Following Arthroscopically Assisted Particulated Juvenile Allograft Cartilage Implantation for Treatment of Difficult to Treat Osteochondral Lesions of the Talus
Cary B. Chapman, MD; Joseph E. Manzi; Kshitij Manchanda, MD
Introduction/Purpose: Conventional methods are not suitable for difficult to treat osteochondral lesions of the talus (OCLT) such as those defects that are large, shoulder lesions, failed previous surgery, or certain patient factors. Osteochondral autograft transfer system (OATS) has been accepted as the primary method of treatment for these more difficult defects, however, complications such as residual knee pain from the graft site, a multiday procedure, and the necessity for a malleolar osteotomy have made this technique not devoid of complications. Particulated juvenile articular cartilage transplantation for these lesions has theoretical advantage of performing the procedure arthroscopically, without need for an osteotomy or autograft. The purpose of this study is to determine long term patient reported outcomes for this procedure.
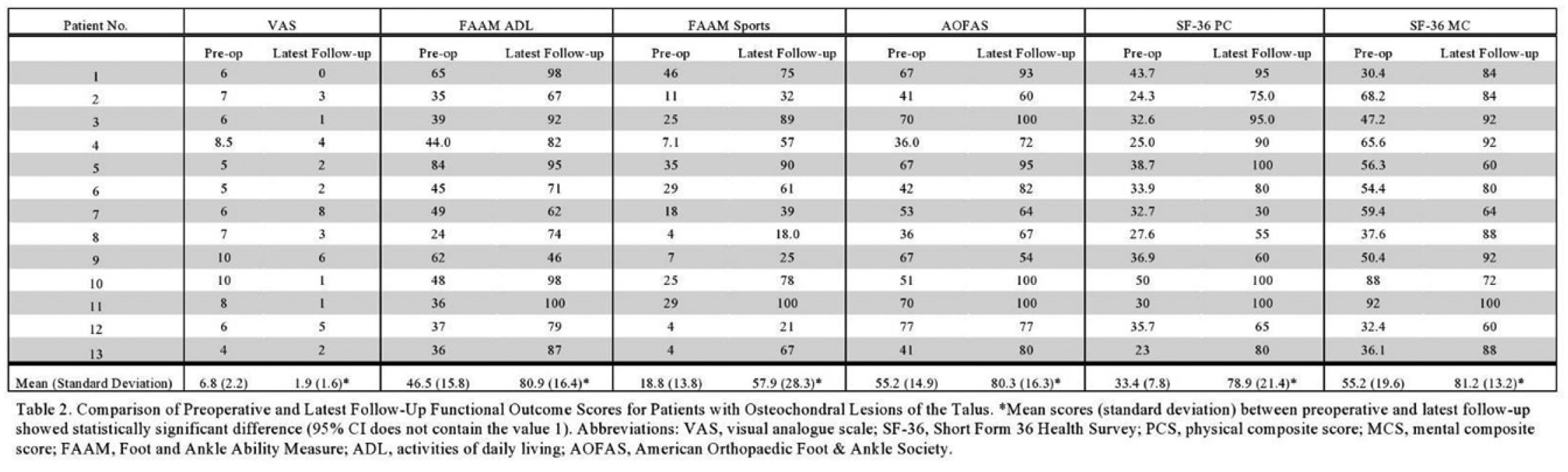
Methods: Thirteen patients with difficult to treat OCLT underwent arthroscopic assisted implantation of DeNovo NT graft into defects from 2010-2012 by the same surgeon. ‘Difficult to treat’ was defined as having at least three of the following features or two if both variables described lesion characteristics: 1) lesions size of 107mm2 or greater, 2) shoulder lesions, 3) patients who failed microfracture, 4) patient age over 40, or 5) patient BMI>25kg/m2. Patients were evaluated using physical examination, patient interviews, and pre and postoperative outcome score measures utilizing Visual Analogue Scale, Short Form 36 and Foot and Ankle Ability Measurement questionnaires, and the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scale. Patients had follow-up at 2 years, 4 years, and between 6-9 years at their most recent follow-up. Differences in functional outcome scores were compared before and after surgery.
Results: Patients (Age: 46.5+-11.8years, Body Mass Index: 28.5 +-6.1kg/m2) had on average, most recent follow-up of 8.0 years (range 72-113 months). Average VAS pain score decreased for patients by 3.9 points, 95% CI [2.18, 5.60], when compared to preoperative assessment. FAAM ADL and Sports scores also showed improvement from 46.5 to 80.9, 95% CI [21.35, 47.43] and from 18.8 to 57.9, 95% CI [21.05, 57.10], respectively. SF-36 physical component scores showed significant improvement by an average of 45.5 points, 95% CI [32.42, 58.50]. AOFAS scores improved from 55.2 to 80.3, 95% CI [12.459, 37.741]. Patient demographics and results are seen in Tables 1 and 2 respectively.
Conclusion: These results demonstrate clinically positive long-term outcomes for a cohort of patients with difficult OCLT, followed over the course of 6-8 years after treatment with arthroscopic assisted DeNovo NT implantation. Understanding the longevity of this intervention can better aid clinicians in deciding if this treatment option is appropriate for patients and should ultimately be included as part of the orthopedics’ armamentarium.
DOI: 10.1177/2473011421S00011
Clinical and Radiographic Outcomes of Minimally Invasive Chevron Bunionectomy Compared to the Modified Lapidus Procedure
Elizabeth Cody, MD; Kristin C. Caolo, BA; Scott J. Ellis, MD; A. Johnson, MD
Category: Bunion; Midfoot/Forefoot
Keywords: Bunion; Minimally Invasive; Hallux Valgus
Introduction/Purpose: Minimally invasive bunion surgery is relatively new in the United States, with the requisite burrs only approved for use by the FDA in 2017. Early reports on outcomes have been encouraging. However, no study to date has compared outcomes from the minimally invasive chevron and Akin procedures (MICA) to the modified Lapidus procedure. Our goal was to compare clinical and radiographic outcomes of MICA to those of the modified Lapidus procedure in patients with comparable deformities. We hypothesized that radiographic parameters of hallux valgus would be superior in the Lapidus group, but that there would be no significant difference in clinical outcomes or satisfaction between the two groups.
Methods: Patients were retrospectively reviewed for inclusion from a prospectively-collected foot and ankle registry at our institution. Patients were eligible if they underwent either the MICA or modified Lapidus procedure, were 18 years or older, and had preoperative and minimum 5 month postoperative weightbearing radiographs. Exclusion criteria included prior forefoot surgery, additional surgeries (such as metatarsal shortening), and concomitant foot conditions (such as flatfoot deformity). Each surgery was performed by one of six fellowship-trained orthopedic foot and ankle surgeons. Demographics, PROMIS scores, and satisfaction data were collected from the registry. Complications and reoperations were collected from chart review. The hallux valgus angle (HVA), intermetatarsal angle (IMA), and tibial sesamoid position (SP) were measured pre- and postoperatively. Patients in the MICA group were matched to patients who underwent Lapidus bunionectomy based on radiographic parameters. Differences between the groups were assessed with paired t-tests for continuous variables and chi-square tests for categorical variables.
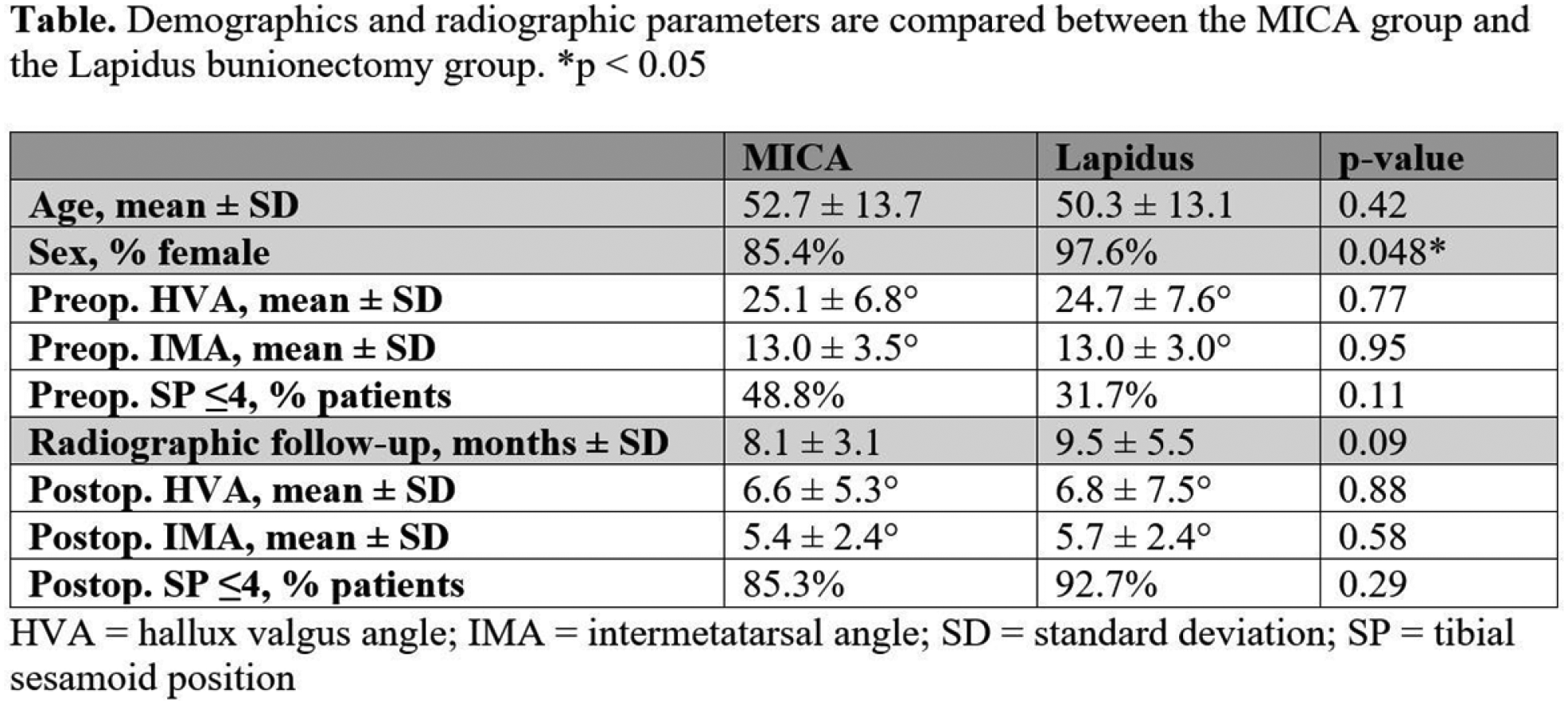
Results: 41 patients who underwent MICA and 81 patients who underwent Lapidus bunionectomy met the inclusion criteria. Of the Lapidus patients, 41 were included, matched to the MICA patients. There were no significant differences in demographics or preoperative parameters between groups aside from sex (Table). Both groups achieved similar radiographic correction (Table). Bunion recurrence (HVA >=20°) occurred in one MICA patient and two Lapidus patients, with all patients asymptomatic. The most common reason for reoperation was removal of hardware (4 patients in the MICA group, 2 patients in the Lapidus group). One additional patient in the MICA group required reoperation for wound closure, and one additional patient in the Lapidus group required a derotational proximal phalanx osteotomy.
Conclusion: This is the first study to our knowledge to compare outcomes between MICA and the modified Lapidus procedure in patients matched for bunion severity. We found that patients with similar preoperative deformities experience similar radiographic outcomes following MICA versus modified Lapidus bunionectomy. Our analysis of PROMIS scores and satisfaction data is currently underway. Although this is short-term data, it provides additional support for minimally invasive techniques which allow for faster, less painful recoveries. Further research is needed to investigate longer term outcomes and to establish which deformities are best suited to each procedure.
DOI: 10.1177/2473011421S00012
Does Time to Intervention Affect Patient Reported Outcomes after Ankle Fracture?
Yvonne Conway; Jacob Hawkins, MD; Brad Alexander, BS; Nicholas A. Andrews; Abhinav Agarwal, MBBS; Whitt Harrelson; Tanvee Sinha; Gerald McGwin; Ashish Shah, MD
Introduction/Purpose: Advances in surgical technique and technology have allowed orthopedic surgeons to attempt early operative fixation of closed ankle fractures. Little is known about the modifiable factors impacting the recovery of these patients and how early operative intervention affects patient reported outcomes. This study aims to determine if early surgical treatment can be performed safely without increasing a patient’s risk for postoperative wound complications and how time to surgery affects both clinical and patient reported outcomes.
Methods: A review of 311 patients records who underwent open reduction and internal fixation (ORIF) for an ankle fracture between July 1st, 2011 and July 1st, 2018 at a single academic center was conducted. Medical records were reviewed. Patients were contacted for collection of PROMIS Physical function, PROMIS Pain Interference, and the Foot Function Index. Patients with open fractures, high energy fractures with ipsilateral lower extremity injuries, pilon fractures, revision cases, non-respondents to the patient reported outcomes survey, and those lost to follow-up prior to radiographic evidence of union or non-union were excluded. After exclusions, 86 patients were then stratified by time to surgery after injury and injury classification. A linear regression model was constructed for each outcome instrument with the covariates of age, BMI, diabetes, smoking status, union, wound complication, time from surgery, and severe injuries by the Lauge-Hansen classification.
Results: The delayed union, nonunion, and wound complication rate was similar regardless of timing of operative intervention (p=.470, p=.149, & p=.578, respectively). At a median of 4.5 (2.0 IQR) years postoperatively, outcomes scores were as follows (median (IQR)): PROMIS Physical Function 47.9 (11.2), PROMIS Pain Interference 50.1 (17.4), FFI Pain 26.0 (52.0), FFI Disability 17.0 (49), FFI Activity Limitation 3.0 (22.0), and FFI Total 20.0 (41.5). Time to intervention was not found to have an independent effect on any outcome score. Severe injuries by the Lauge-Hasen classification were found to be independent predictors of PROMIS physical function -6.3 (Unstandardized beta, 95% CI -11.5 to -1.1). Diabetes had a significant independent effect on PROMIS pain interference 52.4 (Unstandardized beta, 95% CI 24.3 to 80.5).
Conclusion: Early surgical intervention did not significantly delayed union rate, nonunion rate, wound complications, or patient reported outcomes instruments. Severity of injury classification has a significant independent effect on patient’s physical function. Notably, this effect is above the minimal clinically important difference for PROMIS physical function. Overall, the intermediate term outcomes of ankle fracture fixation indicate patients are within one standard deviation of the population mean in terms of pain and physical function. Surgeons should be aware timing of intervention did not have an effect on outcomes scores at intermediate term follow-up.
DOI: 10.1177/2473011421S00013
Predictors of Outcomes of Microfracture for Osteochondral Lesions of the Talus
John Dankert, MD, PhD; John G. Kennedy, MD, FRCS(Orth); Yoshiharu Shimozono, MD; Timothy Deyer; Nathaniel P. Mercer
Category: Ankle
Keywords: Ankle Pain; Lesions of Talus; Osteochondral Lesions of the Talus
Introduction/Purpose: Microfracture has been widely published as a treatment modality for osteochondral lesions of the talus (OLT). However, little is known about the outcome predictors following microfracture for smaller-sized OLT (<100mm2). This study sought to define the predictors of both clinical and magnetic resonance imaging (MRI) outcomes for small OLT treated with microfracture.
Methods: A retrospective cohort study investigating patients who received arthroscopic microfracture for OLT (<10mm or 100mm2) between 2008 and 2017 were evaluated. Multivariate regression models were used to evaluate factors affecting post- operative Foot and Ankle Outcome Scores (FAOS) and Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scores. Kaplan-Meier survival curves with log-rank test were constructed and endpoint was defined as the requirement of revision surgery.
Results: Eighty-seven patients were included in the study. The mean follow-up time was 41.4+-28.7 months. The mean FAOS pain score significantly improved from 60.4+-14.8 preoperatively to 79.3+-12.8 at final follow-up (p<0.001). Patients with uncontained- type OLT had an approximately 9-point worse FAOS pain score compared to contained-type OLT (p=0.036). Patients with cystic OLT also had an approximately 9-point worse pain FAOS compared to non-cystic OLT (p=0.026). Patients with larger lesion sizes had worse postoperative MOCART scores (p=0.012). Both Uncontained-Cyst and Uncontained-Noncyst groups had significantly worse FAOS pain than the Contained-Noncyst group (p<0.001, p=0.026). Survival rates in uncontained and contained lesions were 51.5% and 84.4%, respectively (p=0.616).
Conclusion: Lesion uncontainment and the existence of cysts are independent predictors of poor clinical outcome following arthroscopic microfracture for smaller-sized OLT (<100mm2).
DOI: 10.1177/2473011421S00014
Diagnostic Accuracy of Weightbearing CT in Detecting Subtle Chronic Syndesmotic Instability: A Prospective Comparative Study
Cesar de Cesar Netto, MD, PhD; Matthieu Lalevee, MD; Alan G. Shamrock, MD; Samuel J. Ahrenholz; Francois Lintz, MD MSc FEBOT; Alexej Barg, MD; John E. Femino, MD; Donald D. Anderson; Kevin N. Dibbern, PhD; Nacime S. Mansur, MD
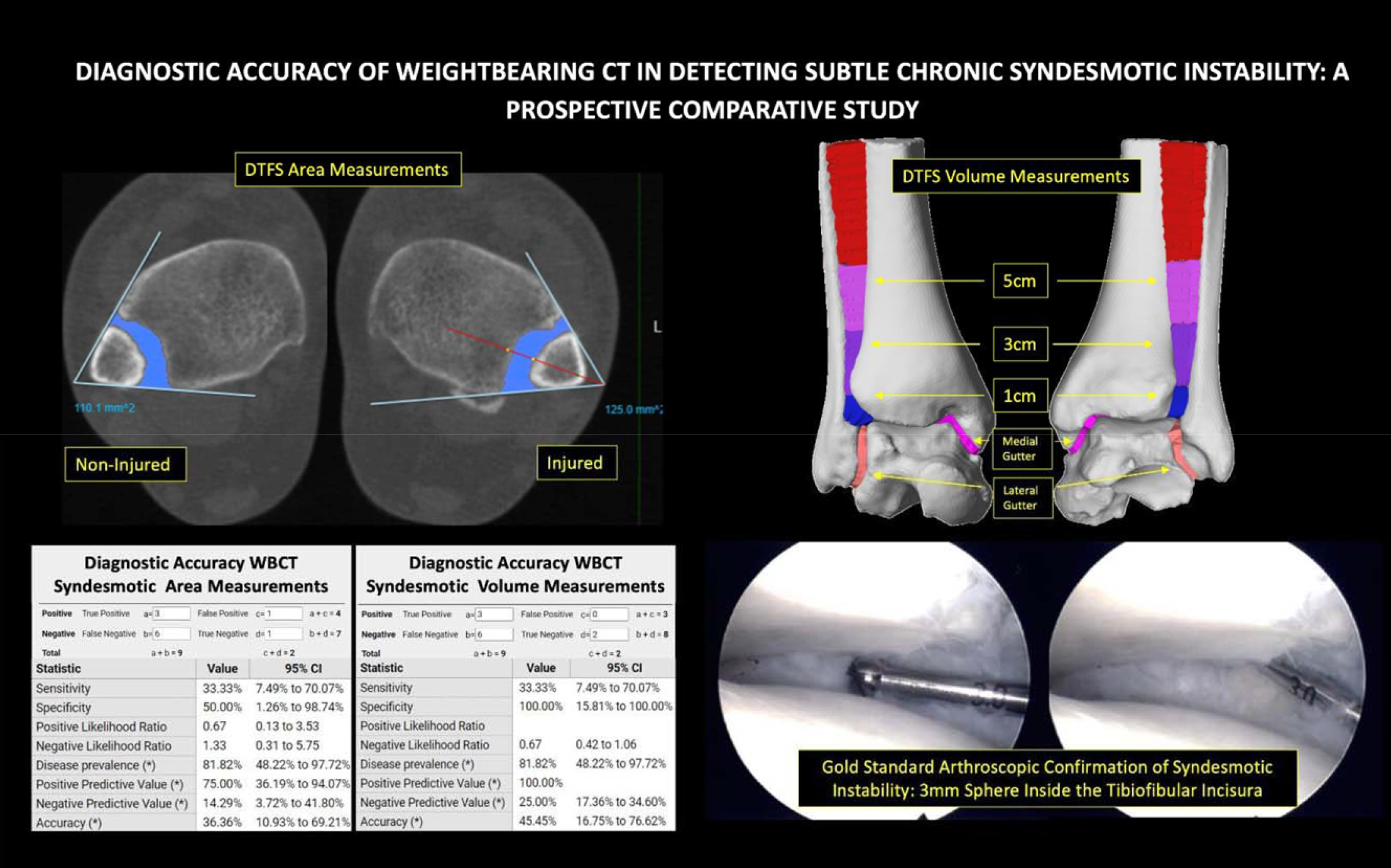
Introduction/Purpose: Improving the diagnosis of subtle syndesmotic instability (SSI) represents one of the most challenging missions in orthopedic surgery, since undiagnosed instability frequently leads to posttraumatic ankle arthritis. Stressed conventional radiographs, ultrasonography, bilateral comparative conventional CT and MRI serve as important diagnostic tools, however, the current diagnostic gold-standard is arthroscopic assessment, an invasive surgical method. The advent of weight- bearing computed tomography (WBCT) brought hope for improved non-invasive SSI diagnosis, particularly by utilizing distal tibiofibular syndesmotic (DTFS) area and volume measurements. However, to date, no studies assessed WBCT diagnostic accuracy for chronic SSI. The purpose of this study was to prospectively evaluate the diagnostic accuracy of WBCT area and volumetric measurements in patients with suspected chronic SSI, when compared to the gold-standard arthroscopic assessment.
Methods: In this IRB-approved prospective comparative study, 11 patients with suspected SSI were enrolled from July 2019 to December 2020. Patients were assessed preoperatively by bilateral standing WBCT. Raw 3D WBCT was automatically segmented by dedicated software. WBCT measurements performed: semi-automatic DTFS area (1cm proximally to tibial dome apex); DTFS volumes (1, 3 and 5cm proximally to tibial dome apex). Threshold values for WBCT abnormality were defined based on currently available data (area>105mm2 and volumes>796mm3, >3062 mm3, and >6733 mm3 for 1, 3 and 5cm, respectively). Subjects underwent surgical treatment including DTFS instability arthroscopic assessment, defined as positive when a 3mm diameter sphere could enter the syndesmotic incisura. Confirmed unstable cases were treated with open reduction/internal fixation. WBCT measurements sensitivity, specificity, positive and negative predictive values (PPV/NPV) and accuracy were calculated using confirmed arthroscopic instability as diagnostic gold standard. Paired t-tests/Wilcoxon analysis was used to compare measurements. P-values<0.05 were considered significant.
Results: When compared to non-injured sides, DTFS area and volumes were significantly higher in injured ankles at 1cm (667 vs 554mm3) and 3cm (2331 vs 2038mm3). Medial gutter volumes were also increased in injured sides (398 vs 370 mm3). DTFS volumes at 5cm and lateral gutter volumes were not different. Nine of eleven patients had confirmed arthroscopic DTFS instability. Considering WBCT area measurements, 4/11 patients were found to be positive (>105mm2), including 3 true positives (+WBCT/+Arthroscopy), 1 false positive (+WBCT/-Arthroscopy), 6 false negatives (-WBCT/+Arthroscopy), and 1 true negative (-WBCT/-Arthroscopy), leading to a 33.3% sensitivity, 50%, specificity, 75% PPV 75%, 14.3% NPV and 36% accuracy. When analysing WBCT DTFS volumes (1cm), 3/11 patients were found positive (>796mm3), depicting 3 true positives, 0 false positives, 2 true negatives and 6 false negatives, with resultant diagnostic accuracy of: 33.3% sensitivity, 100% specificity, 100% PPV, 25% NPV 25%, and 45% accuracy.
Conclusion: This is the first study to prospectively assess WBCT diagnostic accuracy of area and volume measurements in detecting chronic SSI, comparing it to arthroscopic diagnostic standard. When compared to uninjured side, DTFS area and volumetric measurements were significantly increased in injured sides of patients with suspected SSI, including medial gutter volumes, consistent with associated deltoid ligament instability. However, interestingly, we observed a diagnostic accuracy for WBCT area and volumetric measurements to be lower than initially expected. Further incorporation of additional patients, as well as introduction of an external rotational stress can potentially optimize the WBCT diagnostic accuracy for chronic SSI.
DOI: 10.1177/2473011421S00015
Three-Dimensional Distance Maps of Ankle and Syndesmotic Joints from Weightbearing CT in Progressive Collapsing Foot Deformity: A Retrospective Case-Control Study
Cesar de Cesar Netto, MD, PhD; Victoria Vivtcharenko, BS; Andrew Behrens; Matthieu Lalevee, MD; Nacime S. Mansur, MD; Donald D. Anderson; Andrew J. Goldberg, OBE MD FRCS (Tr&Orth); Alexej Barg, MD; Scott J. Ellis, MD
Introduction/Purpose: Recently, weightbearing computed tomography (WBCT) has been utilized to provide more comprehensive and accurate assessment of complex foot and ankle deformities, notably to diagnose and stage Progressive Collapsing Foot Deformity (PCFD). The 3D data provided by WBCT has enabled the developed of novel tools like distance mapping (DM), coverage mapping (CM), and volume measurements. Over the past year, novel DM and CM have shown promise in providing sensitive automated measures of peritalar subluxation, a major component of PCFD. However, the early effects of PCFD on the tibiotalar joint have not yet been quantified. This study sought to use DM and CM to objectively characterize the effects of PCFD on the tibiotalar and tibiofibular joints. We hypothesized that changes seen in early PCFD will be identified.
Methods: IRB approval for retrospective review of patient data from 2014-2020 was obtained to identify patients with clinical and radiographic diagnoses of PCFD. The first consecutive 20 patients with symptomatic flexible PCFD and high-resolution weightbearing CT examination without arthritis that had not undergone prior surgery were selected and compared with 20 controls. Fully automated volume measurements of the syndesmosis at 1cm, 3cm, and 5cm from the tibiotalar joint were performed as well as of the medial and lateral tibiotalar gutters based on models created in Disior Bonelogic. Distance Maps (DMs) were obtained for the tibiofibular incisura, tibiotalar joint, and gutters. Coverage maps (CMs) were created using the measured 3DDMs to identify joint interaction, subluxation, and impingement. Data were checked for normality using the Shapiro- Wilk W test. Two-tailed independent samples student t-tests or Wilcoxon Tests were used to assess differences between groups.
Results: There were significant decreases in coverage of all 3 anterior regions of the tibiotalar joint in PCFD patients when compared to controls along with corresponding significant increases in coverage of all 3 posterior regions (Figure). There were no significant differences in mean or minimum distances in any region of the tibiotalar joint surface. Significant increases in average and minimum DMs of the anterior medial (36%, p<0.01, 19%, p<0.03) gutter were observed with significant decreases in coverage of both anterior medial and anterior lateral regions. Significant decreases in the average and minimum distances of the tibiofibular joint were found anteriorly in PCFD patients compared to controls (-26%, p<0.006). There were no significant differences in overall syndesmotic distance or volume at any level.
Conclusion: The results of our study were able to identify that, compared to controls, patients with early stage PCFD demonstrated significant tibiotalar and tibiofibular joint changes ahead of developing the tibiotalar narrowing associated with arthritis and syndesmotic widening associated with instability. Decreases in anterior coverage with increases posteriorly support early plantarflexion of the talus in PCFD. When combined with plantarflexion of the talus and unchanged syndesmotic volume, decreases in anterior tibiofibular distances support the absence of syndesmotic joint instability in early PCFD. Novel tools may assist with clinical decision-making regarding restoration of normal tibiotalar and tibiofibular alignment during PCFD correction.
DOI: 10.1177/2473011421S00016
Fusion Rate of Subtalar Arthrodesis in Pre-Existing Ankle Arthrodesis: Is There Enough Evidence
Introduction/Purpose: Isolated subtalar arthrodesis is a commonly performed procedure, which produces high union rates. It was suggested that the fusion rate of subtalar arthrodesis is negatively affected by the presence of pre-existing ipsilateral ankle (tibiotalar) arthrodesis, though the mechanism by which this occurs remains unclear. The aim of this study is to assess the fusion rate of subtalar arthrodesis in the presence of pre-existing ipsilateral ankle arthrodesis and to suggest alternative techniques to improve fusion rate.
Methods: Electronic patient records and images of all consecutive isolated primary subtalar arthrodesis that were performed in our institution over ten years between (2009-2019) were retrospectively reviewed. Data that was collected included patients’ demographics, body mass index (BMI), smoking status, diabetes, and rheumatoid arthritis, fusion rate; other factors like the method used of the pre-existing ankle arthrodesis were also studied. Subtalar arthrodesis was performed using a lateral approach and compressed by two screws. Two groups were compared, included all isolated primary subtalar arthrodesis with or without previous ipsilateral ankle arthrodesis. Logistic regression was performed to check for the correlation between fusion rate and all factors.
Results: A total of one hundred and thirty-three (n=133) primary isolated subtalar arthrodesis were identified between (2009- 2019), amongst which twenty-one (n=21) had pre-existing ipsilateral ankle arthrodesis. Ten (n=10) recorded subtalar non-unions occurred in the pre-existing ankle arthrodesis group representing a fusion rate of only 52.4 %, as opposed to sixteen (n=16) in the isolated subtalar fusion without pre-existing ipsilateral ankle arthrodesis group representing a fusion rate of 86.9 %. A significant statistical difference between the two groups, those with ipsilateral ankle arthrodesis had a higher non-rate (P =.001). Age, gender, Body mass index (BMI), smoking status, diabetes, rheumatoid arthritis, and the method used of the pre-existing ankle arthrodesis were found not to have any significant effect on these results.
Conclusion: Our results show a significantly higher non-union rate of isolated subtalar arthrodesis in the presence of pre-existing ipsilateral ankle arthrodesis. Further research is required to help in clarifying the mechanism by which this effect occurs and to study alternative surgical techniques that might be required.
DOI: 10.1177/2473011421S00017
The Outcome of Extended Tarso-Metatarsal and Mid-Tarsal Midfoot Arthrodesis
Yahya Elhassan, MCh, FRCS (Tr & Orth); Ray Monkhouse
Introduction/Purpose: Arthrodesis of extended midfoot arthritis (more than four joints) remains surgically challenging and technically demanding due to bone loss and deformity with a goal to achieve fusion between multiple joints. Yet the outcome and fusion rate of this particular group was sparsely reported and with a lot of heterogeneity. The aim of this study is to assess the outcome of extended midfoot arthrodesis, which included a combined fusion of Tarsometatarsals, Naviculocuneiform, and/or the Talonavicular joints.
Methods: Patients who underwent extended midfoot fusion (> four joints) over ten year period (2009-2019) were identified. Only non-neuropathic patients where multiple joints midfoot fusion were performed were included, more specifically the group of patients who required combined fusion of the second and third Tarsometatarsal joints with extension to the Naviculocuneiform, the Talonavicular, and/or the first Tarsometatarsal joints. All operations were performed by the senior author through a single incision using non-locking compression lag screws and 2.7mm locking plates. Institutional review board approval was obtained to review electronic patient records and imaging. Etiology of midfoot arthritis, fusion rate, reoperation, postoperative complications, and patient satisfaction were independently evaluated. Pre-paid addressed envelopes were posted and Patient Report Outcome Measures (PROMs), including patient satisfaction, MOxFQ (Manchester Oxford Foot ) were collected, and statistical analysis was performed.
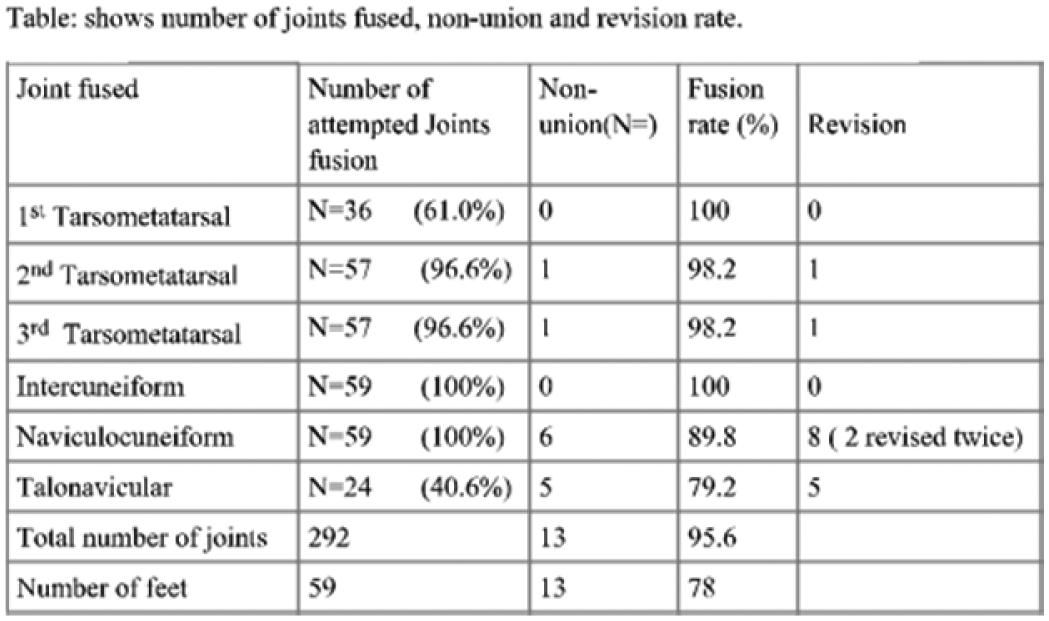
Results: Fifty-one patients (59 feet) out of 162 patients were included. The questionnaire response rate was 82.3%. Female: male ratio was 2.9:1 with a mean age 56.9. The most prevalent diagnosis was primary osteoarthritis in 54.2%, rheumatoid arthritis in 10.2 %, post-traumatic arthritis 17%. AVN of the navicular was the indication for surgery in 18.6%. Extension to naviculocuneiform and talonavicular joint was performed in 100% and 40.6% respectively. 73.8 % were satisfied, with a higher satisfaction rate in older age (P < 0.005) and talonavicular group (P <0.05).Total number of joints fused was 292, with a fusion rate of 95.6%. A lower fusion of the talonavicular and naviculocuneiform joints was observed at 89.8% and 79.2% respectively (Table).Other minor complications included removal of metal, metatarsals stress fracture, metatarsalgia, talonavicular arthrosis, delayed wound healing, SPN neuroma, and CRPS. Deep infection was not reported.
Conclusion: In this series, we highlighted that extended multiple joint midfoot arthrodesis which included fusion of the naviculocuneiform or/and the talonavicular joints produced a high fusion rate when compared to the total number of joints fused, although a lower fusion rate was observed across the naviculocuneiform and talonavicular joints. Extended midfoot arthrodesis is complex; patients should be well informed and counseled about the outcome and the consequences, with a careful approach when quoting satisfaction.
DOI: 10.1177/2473011421S00018
Results of Hallux Metatarsophalangeal Joint Arthrodesis with and without Calcaneus Autograft
Fred T. Finney, MD; D. Barcel, MD; Bruce E. Cohen, MD; W. Hodges Davis, MD; J. Kent Ellington, MD, MS; Todd A. Irwin,
MD; Carroll P. Jones, III, MD
Category: Bunion; Midfoot/Forefoot; Other
Keywords: Hallux Rigidus; Fusion; 1st MTP Joint
Introduction/Purpose: Hallux rigidus is the most common degenerative arthropathy of the foot. Primary hallux metatarsophalangeal (MTP) joint arthrodesis is the most common surgical treatment for end-stage hallux rigidus and can also be utilized for correction of hallux valgus. Though satisfaction rates following hallux MTP joint arthrodesis are very favorable, nonunion rates have been reported as high as 12%. Many surgeons use orthobiologics and/or autograft to augment arthrodeses about the foot and ankle in an effort to increase union rates. The purpose of this study is to retrospectively compare union rates of hallux MTP joint arthrodesis with and without calcaneus autograft.
Methods: A query of our institution’s administrative database was performed to identify patients who underwent a primary hallux MTP joint arthrodesis between February 2016 and February 2019. We compared patients who underwent arthrodesis with and without calcaneus autograft. Surgeon preference dictated use of autograft, as some in our group routinely use graft while others do not. Patients 18 years and older who underwent a primary hallux MTP arthrodesis were included. Patients were excluded if they had radiographic evidence of significant bone loss or if allograft or biologic therapies were used. Patient charts and final radiographs were reviewed. The primary outcome was successful union of the hallux MTP joint arthrodesis. Secondary outcomes included preoperative diagnosis, type of surgical fixation and surgical complications. Data was compared using a student T-test.
Results: There were 336 feet included in the final analysis, and 140 underwent hallux MTP arthrodesis with calcaneus autograft. Mean follow-up time was 14.8 weeks. Among all patients, 89.9% had a successful union. There was no difference in union rates between those who underwent arthrodesis with calcaneus autograft (87.9%) compared to without autograft (91.4%; p = 0.302). Hallux valgus was the preoperative diagnosis in 52.7% of cases followed by hallux rigidus (39.9%). The most common fixation method was a lag screw with a dorsal plate (80.5%). Painful hardware was the next most common complication (8.6%), and smoking and diagnosis of diabetes demonstrated no effect on union rates. In the autograft group, there were no complications related to the calcaneus autograft donor site.
Conclusion: As orthobiologics and local bone autograft gain popularity in foot and ankle surgery, it is important to report clinical outcomes and establish evidence-based guidelines for use. In this relatively large retrospective comparison, the use of calcaneal graft was noted to be safe (no complications from graft site). However, there was no difference in union rate when comparing hallux MTP arthrodesis with and without calcaneus autograft.
DOI: 10.1177/2473011421S00019
Mid-Term Prospective Evaluation of Structural Allograft Transplantation for Osteochondral Lesions of the Talar Shoulder
Amanda N. Fletcher, MD, MS; Samuel B. Adams, Jr., MD; James A. Nunley, II, MD; Mark E. Easley, MD
Category: Ankle
Keywords: Allograft; Ankle; Cartilage Defect
Introduction/Purpose: The management of large osteochondral lesions of the talar shoulder remains a clinical challenge. Their size, three-dimensional geometry, and subchondral cystic degeneration often preclude treatment with traditional measures such as microfracture and osteochondral autograft transplantation. Structural or bulk osteochondral allograft transplantation has demonstrated efficacy in several retrospective reviews. The purpose of this study was to prospectively evaluate patients who received fresh structural allograft transplantation to the talus.
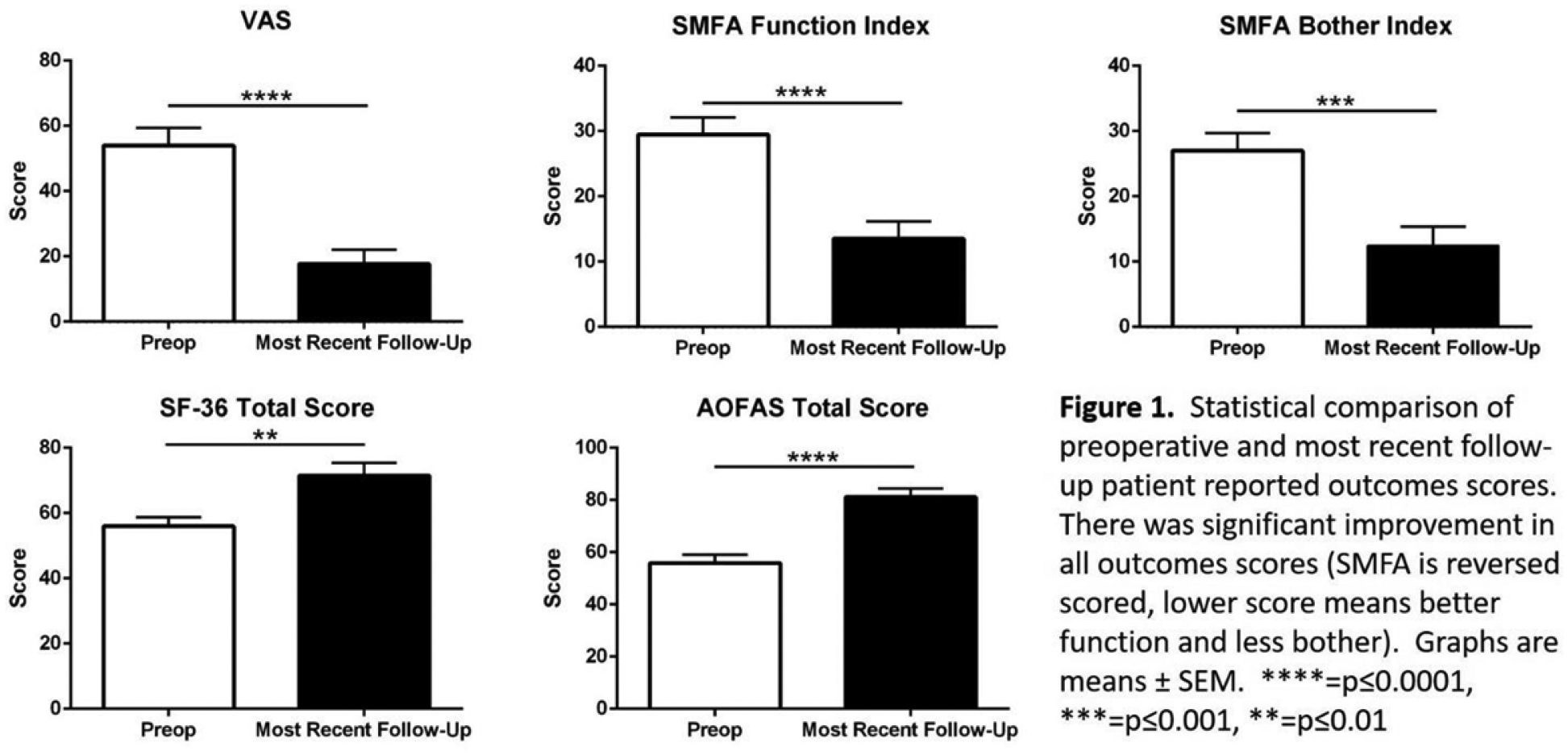
Methods: A prospective evaluation of consecutive patients who underwent fresh structural allograft transplantation for an OLT form 2010 to 2019 was performed under Institutional Review Board approval. All patients failed a minimum of 6 months of conservative management. Preoperative MRI and/or CT, as well as plain radiographs were obtained on all patients. The following patient reported outcomes questionnaires were administered preoperatively and yearly after surgery: 100mm VAS pain scale, AOFAS Ankle-Hindfoot Scale, SF-36, and the Short Musculoskeletal Functional Assessment (SMFA). Pre- and postoperative radiographs were assessed for allograft incorporation and the development of arthritis.
Results: 27 patients underwent fresh osteochondral allograft transplantation and were followed for a minimum of 2 years. The mean follow-up was 5 years (range 2-11). The average size of the OLT was 2,269 mm3 (range 813-8,366) based on CT imaging and 5,797 mm3 (range 1,136-12,489) based on MRI imaging. There was significant improvement in the VAS pain score, AOFAS Ankle- Hindfoot Scale score, the SF-36 total score, and the SMFA functional and bother indices (Figure 1). Thirteen (48%) of the patients required subsequent surgery. Twelve underwent removal of hardware and joint debridement and one patient underwent isolated joint debridement. At the time of these surgeries, two grafts demonstrated cartilage delamination. One of these patients had continued pain and progression of arthritis without additional surgery and one was converted to an ankle replacement. Therefore, the failure rate was 7%.
Conclusion: Significant improvement in pain and function can be achieved with structural allograft transplantation for large OLTs. However, it is important to council patients that painful hardware and stiffness can occur in approximately one-half of patients. An unstable graft and cartilage delamination are indicators of subsequent failure. The use of a structural allograft does not preclude subsequent ankle arthrodesis or arthroplasty.
DOI: 10.1177/2473011421S00020
Short Term Complications Following Total Ankle Arthroplasty and Associated Risk Factors: A NSQIP Database Analysis
Amanda N. Fletcher, MD, MS; Nicholas Kwon; Richard Danilkowicz; Jaewhan Kim; Nathan L. Grimm; Samuel B. Adams, Jr.,
MD
Category: Ankle; Ankle Arthritis; Diabetes
Keywords: Total Ankle Arthroplasty; Complications; Diabetes
Introduction/Purpose: Total ankle arthroplasty (TAA) has become increasingly utilized over the past 20 years to treat osteoarthritis of the ankle. The efficacy and safety of this procedure has been previously reported, but relatively few studies have documented the risk of post-operative complications associated with TAA over the past 10 years. Thus, the aim of this study is to provide a current report on the safety of TAA, particularly in association with a number of preoperative risk factors.
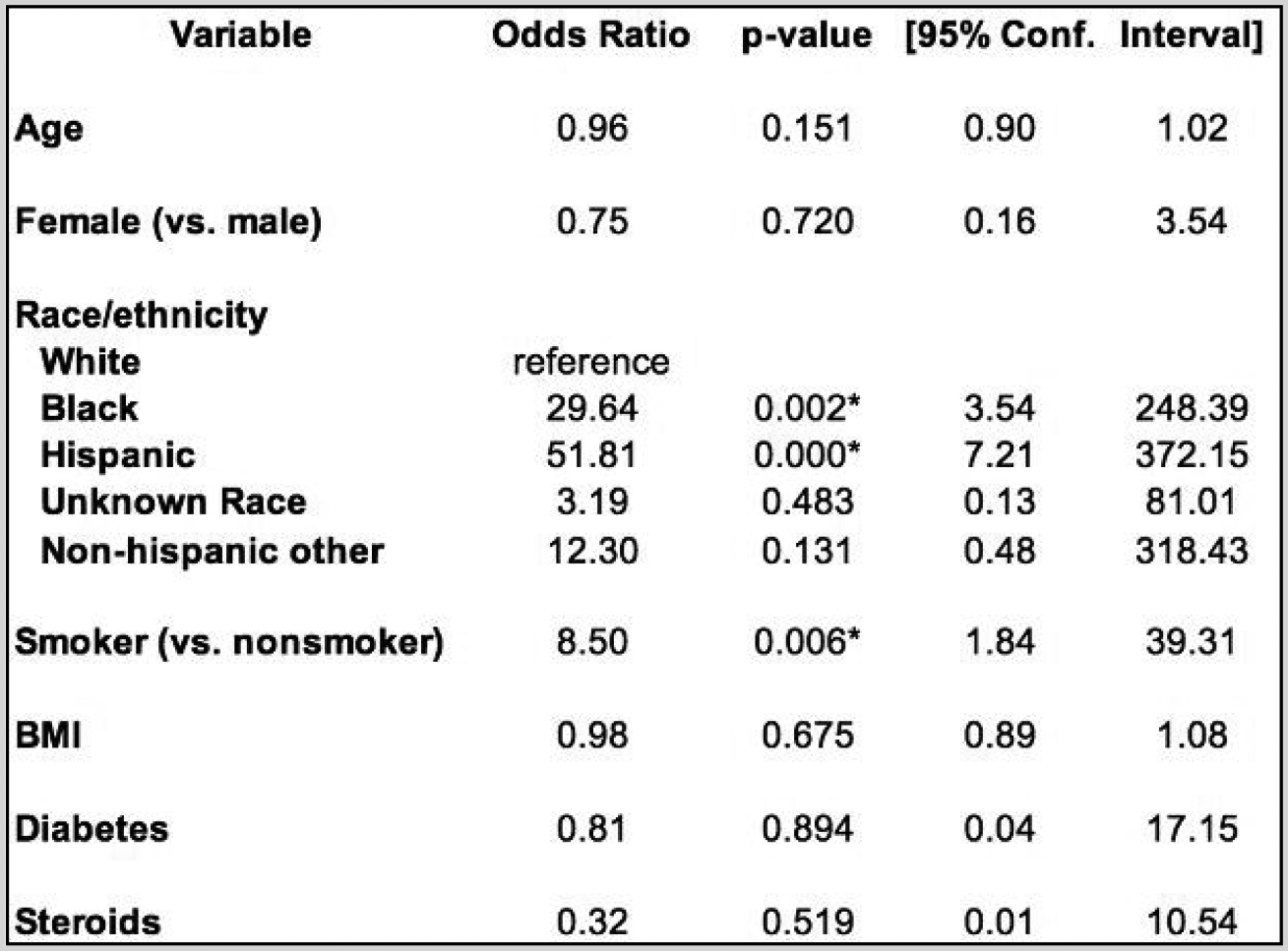
Methods: A retrospective review of all patients in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database who underwent TAA between 2012-2018 was performed. A total of 1333 patients were included in this analysis. Penalized logistic regression to consider small numbers of the postoperative complications was used to identify factors associated with incidence of the complications.
Results: The rate of readmission and superficial wound infection were found to be 1.4% and 0.6%, respectively. Risk factors associated with a prolonged hospital stay were Black race, Hispanic race, and smoking (Fig. 1). Diabetes was associated with a significantly increased risk of readmission. Age, sex, BMI, and steroid use were not associated with increased risk of postoperative complications.
Conclusion: In this study, the rate of surgical site infection and readmission in TAA was found to be relatively low, compared to published data on TKA and THA. Both race and smoking increase the risk of prolonged hospital stay, while diabetes increases the risk of readmission.
DOI: 10.1177/2473011421S00021
Short-Term Efficacy and Safety of Combined Total Talus and Total Ankle Replacement
Amanda N. Fletcher, MD, MS; Abhinav Balu; Gregory F. Pereira, MD; James K. DeOrio, MD; Mark E. Easley, MD; James A.
Nunley, II, MD; Selene G. Parekh, MD, MBA
Category: Ankle; Ankle Arthritis
Keywords: Total Ankle Arthroplasty; Talus; Aspetic Necrosis
Introduction/Purpose: The indications for both total talus replacement (TTR) and total ankle replacement (TAR) are expanding. Combined total ankle-total talus (combined TAR) is a novel treatment option for patients with end-stage ankle arthritis and talar avascular necrosis (AVN) and patients with a prior TAR and talar component collapse. End-stage talar AVN with subchondral collapse is a challenging entity to treat. Historically, an alternative treatment option was tibiotalocalcaneal arthrodesis with structural allograft which results in fair outcomes including nonunion rates up to 40%. Combined TAR is a treatment option that theoretically maintains joint range of motion and restores anatomic alignment. The purpose of this study is to evaluate the short-term outcomes for combined TAR including pain, functional outcomes, radiographic outcomes, and complications.
Methods: Consecutive patients who underwent combined TAR from 2016-2020 were retrospectively reviewed. All surgeries were performed by one of four fellowship-trained foot and ankle orthopaedic surgeons at a single academic institution. All talus implants were custom 3D printed total tali (Additive Orthopaedics, Little Silver, NJ), composed of an alloy primarily made of cobalt chrome. The implants were sized based on computed tomography scans of the contralateral talus and created to articulate with multiple TAR systems. Patient demographics, comorbidities, and surgical data were collected. Outcomes included the Visual Analog Scale (VAS) scores, radiographic alignment, range of motion, and complications. Data analysis was performed with paired t- tests and a significance level of p<0.05.
Results: A total of 66 patients (67 ankles) were included with an average 12-month follow-up. There were 35 (52.2%) men, and the average age was 56.4 years old. The majority of patients (n=42, 62.7%) underwent combined TAR for talar AVN and tibiotalar arthritis while 21 (31.3%) patients were converted from an isolated TAR and 4 patients (6.0%) from an isolated TTR to combined TAR. A total of 23 (34.3%) patients had a previous talus fracture. Significant postoperative improvements compared to preoperative included: VAS (2.8 vs. 8.2; p<0.0001), ankle dorsiflexion (11.0° vs. 4.7°; p=0.0007), ankle plantarflexion (31.9° vs. 23.7°; p<0.0001), talar declination angle (20.7° vs. 11.6°; p=0.0007), Meary’s angle (2.2° vs. 10.4°; p=0.0043), and talocalcaneal height (79.6mm vs. 74.2mm; p <0.0001). There was a total of 10 (14.9%) complications, 7 (10.4%) of which required repeat surgery. There were 3 (4.5%) failures requiring explant, revision, or amputation (Table 1).
Conclusion: Combined TAR is an efficacious and safe procedure. Patients experienced improvement in pain, ankle range of motion, and radiographic parameters postoperatively. This technique provides an anatomic treatment with preservation of ankle motion for patients with severely deficient bone stock due to talar AVN with ankle arthritis or failed TAR. To confirm these preliminary positive results, further studies are required including continued longer-term follow-up, prospective cohorts, and comparative analyses to other treatment options.
DOI: 10.1177/2473011421S00022
Ankle Arthritis Etiology Predicts Patterns of Gait Dysfunction: A Prospective Multivariate Gait Analysis
Samuel E. Ford, MD; Daniel J. Scott, MD, MBA; David Vier, MD; Scott Coleman; Shannon F. Alejandro, MD; James W. Brodsky, MD
Keywords: Ankle Arthritis; Gait Study Range of Motion; Segmental Gait
Introduction/Purpose: Preoperative factors influencing functional disability imparted on the patient by ankle arthritis have not previously been assessed with gait analysis. The purpose of this study was to assess the influence of ankle arthritis etiology and deformity, measured radiographically, on gait performance in a dedicated gait lab utilizing a multisegment foot model. With three calcaneal and four metatarsal markers in addition to standard lower extremity markers, the modified Helen Haynes model allows for the evaluation of range of motion (ROM) within the ‘ankle-hindfoot segment.’ The primary hypothesis was that three- dimensional ankle-hindfoot segment ROM would be more restricted in patients with post-traumatic ankle arthritis than other etiologies. The secondary hypothesis was that temporospatial and kinetic measures would not vary by etiology.
Methods: A longitudinal cohort of 183 patients with end-stage ankle arthritis were prospectively enrolled from 2008-2018. Mean age was 61, BMI 29, and 56% were male. Four etiologic groups were defined: Post-fracture (100), arthritis caused by planovalgus foot deformity (23), chronic instability associated with cavovarus (32), and miscellaneous (28), comprised of inflammatory (7), idiopathic (6), instability without deformity (5), septic (2), and avascular necrosis (3) as causes. The four-segment Milwaukee foot model was used in a dedicated gait lab with a 12-camera motion capture system. Gait data was collected over a minimum 20 gait cycles across a 10-meter walkway. Kinetic data was simultaneously collected with two force plates embedded in the walkway operating at 1 MHz. AP and lateral tibiotalar angles, lateral talus-first metatarsal angles, calcaneal pitch, and tibiotalar ratio were measured. Multivariate regression analyzed the effect of etiology and radiographic measures on gait function, controlling for age, gender, and BMI.
Results: The primary hypothesis was confirmed. Sagittal plane ankle-hindfoot segment ROM was lower in post-traumatic and higher in valgus patients compared to other etiological groups (P<0.0001) (Figure 1). Sagittal plane ankle-hindfoot segment ROM restriction relative to the contralateral limb was also more severe in the post-traumatic group than others (P=0.0005). Valgus AP tibiotalar angles were associated with greater sagittal plane ankle-hindfoot ROM (P=0.0016). The secondary hypothesis was disproven. Post-traumatic patients ambulate with greater maximum ankle moment than other groups (P=0.0043). Valgus patients ambulate with a comparatively longer step length (P<0.0001). Significant reductions in affected limb walking speed (P<0.0001), step length (P<0.0001), and maximum ankle moment (P=0.036), as well as increases in double limb (P=0.0007) and total support percentage (P<0.0001) were found among the miscellaneous etiology group.
Conclusion: Of the four groups, patients with post-traumatic ankle arthritis ambulated with the greatest ankle and hindfoot stiffness, but also the greatest ankle moment. Patients with valgus ankle arthritis had the greatest ROM through the ankle and hindfoot and the longest step length. In addition to diminished ROM, patients in the miscellaneous group had the lowest cadence, symmetry, and torque of gait. The etiology of severe ankle arthritis can predict the pattern of gait dysfunction, which, in turn, may inform choices of surgical reconstruction.
DOI: 10.1177/2473011421S00023
Compression of A Midfoot Osteotomy Using A Circular External Fixator: What is the Ideal Pin Configuration?
Tyler R. Freeman, MD; Henry Yu; Todd Baldini; Keanu Chee; Jason L. Koerner; Kenneth J. Hunt, MD
Introduction/Purpose: Foot and ankle deformity correction through midfoot osteotomy can be implemented in a wide variety of clinical situations. Use of a circular ring fixator for osteotomy fixation is particularly useful for patients with poor soft tissue envelopes and/or active infection as can occur in diabetes and Charcot arthropathy. The foot pins in a ring fixator can be configured to apply compression at the osteotomy site. However, the optimal pin configuration and force has yet to be determined. The purpose of this study was to quantify compressive forces achieved across midfoot osteotomies with various wire configurations in a circular ring fixator construct.
Methods: Nine through-knee amputation cadavers were stabilized with a standard circular external fixation carbon frame. A midfoot osteotomy through the transverse tarsal joint was performed using an oscillating saw. A 4mm bone wedge was removed from the osteotomy site for placement of a Tekscan pressure sensor. A two-ring frame was applied in the standard fashion and three parallel 1.8mm smooth wires were placed parallel to each other through the foot distal to the osteotomy: wire #1 proximally through the cuneiforms, wire #2 through the base of the metatarsals, wire #3 through the metatarsal shafts. After baseline pressure readings, wires were sequentially attached (wire #1 alone, wire #1-2, wire #1-3) to the ring fixator and tensioned to 90kg. Pressure readings were recorded at the osteotomy site for each sequential wire tensioning both at the hole location where the wire naturally crossed, ‘neutral’, and again at one hole ‘proximal’ (e.g., toward the osteotomy).
Results: Average compressive load at neutral hole positioning for wire #1 was 382 N. The addition of wire #2 increased the compressive load to 439 N on average. The addition of wire #3 decreased compressive force to 372 N. Similar trends were seen in proximal hole positioning where average compressive force increased following tensioning of wire #2 from 580 N to 600 N but compressive force decreased on wire #3 addition to 425 N. Therefore, tensioning forefoot thin wires in the proximal hole position increases compressive forces by 50% compared to neutral position, and adding a second wire increased compressive force by up to 15% compared to a single forefoot wire.
Conclusion: In a circular frame midfoot fusion model, the greatest compressive force was achieved with two wires tensioned in the proximal hole position. The addition of a third wire led to force decrease likely due to off-axis forces that may distract the osteotomy site given the difficulty of passing all wires perfectly parallel in all planes. Ideal positioning and tensioning of forefoot pins may optimize construct stability and compression and improve healing of the midfoot osteotomy.
DOI: 10.1177/2473011421S00024
Arthroscopic vs Open Ankle Arthrodesis: A 5-Year Comparison
Oliver Gagné, MD; Monther Abuhantash; Andrea N. Veljkovic, MD, MPH, FRCSC; Kevin J. Wing, MD, FRCSC; Murray J. Penner, MD, FRCSC; Alastair S. Younger, MB ChB, ChM, FRCSC
Category: Ankle; Ankle Arthritis; Arthroscopy
Keywords: Open Ankle Arthrodesis; Ankle Fusion; Arthroscopic Ankle Arthrodesis
Introduction/Purpose: End-stage ankle arthritis has long been managed surgically with open ankle arthrodesis (OAA). More recently, arthroscopic ankle arthrodesis (AAA) is thought to be associated with improved patient-reported outcome measures (PROMs) and fewer complications. The objective of this study was to systematically compare these two approaches in long-term PROMs, major complication rates and survivorship of the ankle fusion.
Methods: In this retrospective longitudinal cohort study, all patients with an ankle fusion done at our institution and a minimum two-year follow-up were screened for inclusion. Patients demographics at baseline were collected including: age, gender, BMI, smoking status, diabetes status as well as preoperative ankle arthritis COFAS (Canadian Orthopedic Foot and Ankle Society) type. The following PROMs were completed preoperatively, at 6-months and annually thereafter to five years: AAS, AOS, SF-36, expectation, satisfaction and swelling scores. PROMs were compared at all timepoints using a mixed-effects regression model adjusted for baseline patients’ demographics, COFAS type and PROMs. Major postoperative complications and survival analysis/rate of revision of the ankle fusions were also compared.
Results: Of 874 patients screened for inclusion, 351 ankle fusions done between 2003 and 2019 were eligible for the study, 223 AAA and 128 OAA. The two groups were similar at baseline with respect to demographics, but COFAS type was higher in the OAA group and AAS and AOS scores were better in the AAA group. At one-year post-operatively, there was a higher mean AAS score in the AAA group, but there were no other differences in outcomes at any other timepoint. Survivorship of the ankle fusion in the arthroscopic group was lower (ie higher rate of revision) due to a higher rate of amputation or fusion. Deep infection and wound complications were more common with OAA and accounted for most ankle fusion revisions in this group.
Conclusion: There were no consistent differences in PROMs of patients who underwent AAA versus OAA patients up to five- years postoperatively. Ankle fusions done arthroscopically had a lower survivorship rate compared to those done with the open approach due to a higher rate of major complications. Previously proposed advantages of AAA over OAA may therefore need to re-assessed and weighed against the technical challenges and associated complications of the arthroscopic technique.
DOI: 10.1177/2473011421S00025
Minimum 5-Year Outcomes of the Lateral Trabecular Metal Ankle Arthroplasty
Oliver Gagné, MD; Jaeyoung Kim, MD; Kristin C. Caolo, BA; Scott J. Ellis, MD; Constantine A. Demetracopoulos, MD; Jonathan T. Deland, MD
Introduction/Purpose: The treatment of ankle arthritis has changed significantly with the recent advances in total ankle arthroplasty (TAR). Many different designs of TAR have been used around the world as the biomechanical technology advances and our understanding increases. Most implant system are anterior-based and have a flat cut on the tibial prosthesis. Only one implant, the Trabecular Metal (Zimmer-Biomet, Warsaw, IN), utilizes a lateral approach with a fibular osteotomy to gain access to the tibiotalar joint and a sagittally curved tibial component. Recent publications have described a higher reoperation rate with this implant system. This study aimed to report the 5-year clinical and radiographic outcome as well as the survivorship of the implant.
Methods: Over a three-year period, two fellowship-trained foot and ankle surgeons used this implant system for patients indicated for TAR. A total of 38 patients were reviewed with an average age of 63.4+-8.6 years-old, BMI of 28.9+-4.6 and the majority (78%) had post-traumatic arthritis. Reoperations and revisions were collected prospectively as part of the local database. Patients participated in surveys preoperatively and at every annual follow-up which included the Foot and Ankle Outcome Score (FAOS). Patients were also evaluated with weightbearing radiographs preoperatively, at the 3 months postoperative and at the 5 year-mark. Those were analyzed by looking at the implant position with validated angles and comparing those over time. Further statistical analysis used paired t-test and Mann-Whitney U test.
Results: The survivorship for our cohort was 92% at the 5-year mark. Three patients had the implant extracted at 12 and 15 months postoperative. Two of those patients had revisions to stemmed TARs and one had a below-knee amputation. Reoperations otherwise included 4 fibular hardware removal and 5 medial gutter debridement. As seen in Table 1, the FAOS improved significantly for all domains at 5-year compared to preoperative status. The Pain and Symptoms domains improved above than the MCID. The implant positioning both tibial coronal and sagittal as well as talar sagittal did not significantly change between 3 months and 5 years postoperative.
Conclusion: This study describes the use of a laterally based Trabecular Metal TAR with great survivorship (92%) and clinically significant improvement in patient-reported outcomes. The rate of reoperation is higher due to prominent lateral hardware or poorly visualized medial gutters and revisions had to be performed through an anterior approach. Few other studies report 5-year outcomes from this prosthesis. There is a growing need to present more data from different centers to guide its ongoing clinical use.
DOI: 10.1177/2473011421S00026
Total Ankle Replacement vs Ankle Arthrodesis (TARVA): A Randomised, Multi-Centre Trial in Patients Over 50 with End Stage Ankle OA, Comparing Clinical and Cost-Effectiveness
Andrew J. Goldberg, OBE MD FRCS (Tr&Orth); Andrew P. Molloy, MB ChB, FRCS(Tr&Orth); Mark Bowen Davies, MD, FRACS(Orth); Steve Hepple, MB ChB; Rhys H. Thomas, MBBS, FRCS(Tr&Orth); Malik S. Siddique, FRCS (T&O); David T. Loveday, MBBS, FRCS(Tr&Orth); Sunil Dhar, MBBS,MS,MCh; Andrew J. Bing; Michael Karski; Stephen P. Bendall, MBBS, FRCS(Orth); Mark Rogers; Paul Halliwell; Stephen Milner; Viren Mishra; Michael Butler; Kashfia Chowdhury; Ekaterina Bordea; Caroline J. Dore; Dominic Hague; David N. Townshend, MBBS, FRCS(Tr&Orth); Paul Cooke
Introduction/Purpose: Both ankle replacement and ankle arthrodesis are offered as treatments to patients with end stage ankle osteoarthritis. Systematic reviews have confirmed that both procedures are effective but there has never been a robust randomised multicentre level I study comparing the two treatments. Our objective was to investigate and compare the clinical and cost effectiveness and complication rates of ankle replacement against ankle arthrodesis in the treatment of end-stage ankle osteoarthritis in patients aged 50-85 years.
Methods: 17 NHS centres and 35 surgeons across the United Kingdom participated. Formal Ethics committee approvals were obtained. A Trial Management Group was overseen by a Trial Steering Committee, and an Independent Data Monitoring Committee. Randomisation was carried out using a secure on-line service and was stratified by surgeon and the presence or absence of adjacent joint OA (based on an independently reviewed preoperative MRI scan). Participants were randomised 1:1 to either TAR or ankle fusion. The primary outcome was the change in the Manchester Oxford Foot & Ankle Questionnaire (MOXFQ) walking/standing domain scores between pre-operation and 52 weeks post-operation. Secondary outcomes measures included FAAM; FAAM (ADL); and Sport subscale scores. Quality of life was measured using the EQ-5D-5L. Total range of motion was measured using a validated method. Radiological parameters and adverse events were captured. Health economic analysis used mean incremental cost per quality-adjusted life years (QALY) gained.
Results: 1600 patients were screened for eligibility. 330 participants were consented and 303 were randomised; 282 underwent surgery and attended follow-up visits. Mean age was 68 years (71% male). The aetiology of OA was post-trauma in 60%, with 6% patients having inflammatory OA. 42% had MRI evidence of OA in the adjacent joints. The groups were well balanced at baseline on all other parameters including deformity, range of motion and baseline clinical and quality of life scores.42% had MRI evidence of OA in the adjacent joints. 54% TARs used were fixed bearing; 46% were mobile bearing. 61% of fusions were performed arthroscopically. We present all outcomes including adverse effects (death; thromboembolic events; reoperation and revision); radiological findings; and range of motion. We also present subgroup analyses looking at the performance of fixed versus mobile bearing implants; differences by age; and by the presence or absence of adjacent joint OA.
Conclusion: This is the first publicly funded, multicentre, prospective, randomised clinical trial comparing the clinical and cost effectiveness of ankle replacement against ankle fusion. It is also the first study in surgery to have detailed prospectively captured health economic data to be able to feed into the reimbursement discussions on these life transforming treatments. Due to contractual requirements of the funders the formal results cannot be released until the final report has been submitted for peer review which will not happen until the end of April 2021. The paper is submitted on behalf of the TARVA Study Group.
DOI: 10.1177/2473011421S00027
Minimally Invasive Surgery for Severe Hallux Valgus with 2 Year Minimum Follow Up in 106 Feet
David Gordon, MD, MB BCh, FRCS(Orth), MRCSEd; Thomas L. Lewis, MB ChB; Robbie Ray
Introduction/Purpose: There is widespread variation in the optimal procedure for correction of severe hallux valgus deformity. Severe hallux valgus (defined as hallux valgus angle (HVA) (>=40°) and/or 1-2 intermetatarsal angle (IMA) (>=20°)) is associated with increased complication rates including recurrence, delayed or non-union and metatarsal shortening with transfer metatarsalgia. There is limited evidence investigating the clinical or radiological outcomes following treatment of severe hallux valgus deformity with third-generation minimally invasive chevron and akin osteotomies (MICA). Objective: The primary aim was to investigate clinical patient reported outcome measures (PROMs) two years following surgery and the radiographic deformity correction for patients undergoing third-generation MICA for severe hallux valgus deformity.
Methods: Prospective observational single surgeon series of consecutive patients who underwent primary third-generation MICA with screw fixation for severe hallux valgus. The primary outcome was a validated patient reported outcome measure, the Manchester-Oxford Foot Questionnaire (MOXFQ), assessed minimum 2 years following MICA. Secondary outcomes were radiographic deformity correction, complication rates and other quality of life PROMs (EQ-5D and Visual Analogue Pain Scale).
Results: Between September 2014 and May 2018, 106 consecutive feet (n=78 patients; 73 female, 5 male) met the inclusion criteria. Prospectively collected pre-operative and 2 year PROM MOXFQ data was available for 86 feet (81.1%). At two years following surgery, the MOXFQ score significantly improved for the Pain, Walking and Standing and Social Interaction domains from 39.2 to 7.5, 38.2 to 5.9 and 48.6 to 5.5, respectively (p<0.001). Pre- and post-operative radiographic data was available for all 106 feet. Mean IMA following surgery improved from 18.2° to 6.3° (p<0.001) whilst mean HVA improved from 45.3° to 10.9° (p<0.001).
Conclusion: This study has demonstrated third-generation MICA for the treatment of severe hallux valgus deformity can achieve significant improvements in clinical PROMs and radiographic deformity correction.
DOI: 10.1177/2473011421S00028
2021 IFFAS Award for Excellence Winner: Weightbearing Radiographs Reliably Predict Normal Ankle Congruence in Weber B/SER2 and 4a Fractures: A Prospective Case-Control Study
Martin G. Gregersen, PT, MSc; Marius Molund, MD, PhD
Category: Ankle; Trauma
Keywords: Ankle Fracture Evaluation; Ankle Instability; Weber B Ankle Fractures
Introduction/Purpose: In Weber B/SER2-4 ankle fractures assessment with weightbearing radiographs to ascertain stability of the ankle mortise has been advised. However, no previous studies report whether this method leads to preservation of normal ankle congruence in ankles deemed stable. The purpose is to evaluate equivalence of ankle congruence of injured ankles after fracture union versus the uninjured side for stable Weber B/SER2 and partially unstable Weber B/SER4a fracture types.
Methods: We conducted a prospective, case-control study of 149 patients with an isolated Weber B fracture demonstrating stability on weightbearing radiographs. All participants were treated nonoperatively with a functional orthosis and full weightbearing allowed. Results from gravity stress radiographs classified ankles as SER2 or SER4a fracture types. We defined an equivalence margin in medial clear space difference of 1.0 millimeters. We also evaluated the reliability of obtaining measurements from weightbearing radiographs.
Results: No difference in medial clear space between the injured and uninjured ankle could be observed after fracture union for stable Weber B/SER2 (mean difference 0.1 millimeters, 95% confidence interval -0.3 to 0.0, P =.056) or partially unstable Weber B/SER4a fracture types (mean difference 0.0 millimeter, (95% confidence interval -0.1 to 0.1, P =.797). No between group differences could be observed (mean difference 0.0 millimeter, 95% confidence interval -0.2 to 0.2, P=.842). These findings were consistent with equivalence as the higher limit of the confidence intervals for the differences were less than the predefined equivalence margin. Estimated 95% confidence intervals for the intraclass correlation coefficients indicated excellent inter- and intraobserver reliability.
Conclusion: We demonstrated that weightbearing radiographs successfully predict preservation of normal ankle congruence when the weightbearing radiograph is deemed stable. Ankle congruence was equivalent comparing stable Weber B/SER2 and partially unstable Weber B/SER4a fracture types. Excellent reproducibility of the method of obtaining medial clear space measurements was demonstrated.
DOI: 10.1177/2473011421S00029
Return to Physical Activity after Isolated Subtalar Arthrodesis
Patrick D. Grimm, MD; Todd A. Irwin, MD; Carroll P. Jones, III, MD
Introduction/Purpose: Subtalar arthrodesis has been shown to provide reliable pain relief and deformity correction for a variety diagnoses including include primary arthritis, posttraumatic arthritis, inflammatory arthritis, talocalcaneal coalitions, and hindfoot deformity. However, the level of functional activity achievable following this procedure is unknown. The aim of this study was to assess physical activity and functional outcomes in patients following isolated, primary subtalar arthrodesis.
Methods: A retrospective review of isolated primary subtalar fusions was performed. Inclusion criteria were: age between 18 and 65, isolated primary subtalar fusion that achieved bony union, minimum 4 month radiographic follow up (XR or CT), and 1 year minimum questionnaire follow up. Patients who had neuromuscular diagnoses, adjacent joint arthritis, inflammatory arthritis, contralateral ankle or hindfoot pathology, significant medical comorbidities, or were treated under worker’s compensation were excluded. The primary outcome measure was the Foot and Ankle Ability Measure. Additional patient reported outcomes included a novel functional assessment questionnaire, Coughlin Satisfaction Score, and a contralateral hindfoot comparison score.
Results: Patient reported outcome measures were collected from 15 (10 F, 5 M) patients at a median of 78 (49, 106) months following surgery. The median FAAM ADL subscore was 83.3 (71.4, 98.8) and the sports subscore was 59.4 (40.6, 87.5). The majority (58%) of patients maintained the same level of physical activity before and after surgery. Fewer patients were able to golf, rollerskate/ice skate, run, weightlift, or take aerobics/yoga after surgery. More patients were able to dance, hike, play tennis/pickleball, or walk for exercise. More patients were able to wear shoes without limitations and fewer patients required a brace or orthotics. Good and excellent outcomes were reported by 73% of the cohort. The median contralateral comparison score for the cohort was 90 (50, 100).
Conclusion: Isolated subtalar arthrodesis can provide reliable pain relief and allow reasonable functional outcomes as demonstrated in this patient cohort. In general, most patients maintain their level of function and have fewer limitations with shoe wear. Select, higher impact activities may be more challenging for patients with a fused subtalar joint. These findings may be used to help surgeons appropriately counsel patients about expected postoperative physical activity following an isolated subtalar arthrodesis.
DOI: 10.1177/2473011421S00030
Automated Volume Measurement of the Syndesmosis Using 3D Weightbearing CT
Daniel Guss, MD, MBA; Olivia Lucchese, MSc; Soheil Ashkani-Esfahani, MD; Rohan Bhimani, MD, MBA; Gregory R. Waryasz, MD; Gino Kerkhoffs, MD; Bart Lubberts, MD, PhD; Christopher W. DiGiovanni, MD
Introduction/Purpose: Recent studies have shown that weight-bearing computed tomography (WBCT) that allows 3D volume measurement of the distal syndesmosis while under physiologic load brings about a higher accuracy in detection of syndesmotic instability, especially if subtle. Since the volume measurement method is complex, time-consuming, and has a noticeable interobserver bias, most clinicians might not still be interested in utilizing it in practice. Automatization of this measurement using computer-assisted methods will not only reduce the interobserver bias but also will be faster and more applicable in practice. This study aimed to develop an automated 3D syndesmosis volume measurement tool using image processing methods and compare the speed and the interobserver bias with human interpreters.
Methods: We included 30 patients with subtle syndesmotic instability who had undergone WBCT and were diagnosed intraoperatively. Thirty individuals with otherwise healthy ankles who had WBCT images were allocated to the control group. The volume measurement up to 5cm proximal to the tibial plafond was considered as the most sensitive and specific method to assess syndesmotic stability based on the literature. An algorithm was developed using MATLAB software that could recognize and calculate the syndesmotic volume using WBCT images. The volume measurement method was used by two orthopaedic surgeons for the same population. The time spent by each surgeon and the algorithm was measured. Finally, the values were compared using the t-test; the interobserver correlation coefficient (ICC) was also calculated. P<0.05 was considered statistically significant.
Results: The percentage of changes in 3D volume showed a significant difference at 5cm (25.4%; p<0.001), proximal to the tibial plafond. Based on our clinical study, the volume measurement up to 5cm showed a sensitivity of 95.8%, 95%CI:87.8-100, and specificity of 83.3%, 95% CI:68.4-98.2 for detection of syndesmotic instability. The ICC between the clinicians was 75% while using the automated measurement algorithm showed an ICC of 97%. The mean time spent by the clinicians was 268.4+-56.4 and by the algorithm was 2.9+-0.3 seconds (p<0.001, Figure 1).
Conclusion: Given the fact that 3D volume measurement of the syndesmosis using WBCT is still a complex technique for most clinicians while it is one of the most accurate diagnostic methods based on recent literature, developing a faster and more accurate method for 3D volume measurement of the syndesmosis leads to a more reliable and easier to use the technique to be used in practice.
DOI: 10.1177/2473011421S00031
Effect of Blood Flow Restriction Therapy Following Achilles Rupture and Repair: A Randomized Controlled Trial
Oliver B. Hansen; Andrea Papson; Stephanie K. Eble; Mark C. Drakos, MD
Category: Sports; Other
Keywords: Achilles Tendon Rupture; Return to Play; Functional Rehabilitation
Introduction/Purpose: Blood flow restriction (BFR) therapy involves the use of a tourniquet to partially occlude blood flow to the affected limb, creating an anaerobic environment during exercise. This is thought to stimulate growth and recovery by increasing the body’s anabolic response. BFR therapy can be initiated shortly after surgery since it allows for significant muscle activation with limited load bearing. To date, no existing study has evaluated the effect of using BFR therapy for recovery following Achilles tendon rupture and repair, after which patients often experience significant losses in calf strength and girth. This is a randomized controlled trial designed to study whether BFR can minimize loss of calf strength and muscle volume after Achilles rupture compared to a conventional physical therapy protocol.
Methods: Patients presenting with an acute Achilles tendon rupture were randomized into the BFR or control group. Patients in the control group performed at-home exercises and began in-person physical therapy at 6 weeks postoperatively, as is the standard of care in our practice. The exercises were standardized across groups with BFR the isolated variable. The primary outcome studied was ankle plantarflexion strength as measured during isokinetic strength testing 3 months after surgical repair. We also tested knee strength during flexion and extension. All strength tests were performed at two rotational speeds. Calf atrophy was assessed by measuring the circumference of both calves 15 cm below the joint line at the time of operation and at 2 weeks, 6 weeks, 3 months, and 6 months postoperatively. Finally, Patient-Reported Outcome Measurement Information System (PROMIS) scores were collected pre- and postoperatively.
Results: The study enrolled 43 patients, 24 of whom were assigned to the BFR group. 30 patients completed strength testing at 3 months and 26 at 6 months. Calf measurements through 3 months were completed for 39 patients and 6 month measurements were completed for 32 patients. Results for ankle plantarflexion strength at 3 months are displayed in Table 1, showing that patients in the BFR group demonstrated greater absolute strength in the operative calf compared to the control group, but no significant advantage in strength relative to the uninvolved calf. We failed to detect a significant difference in strength between groups for ankle dorsiflexion, knee extension, or knee flexion. Our model of calf circumference over time showed that BFR had a positive but insignificant correlation to calf circumference (p = 0.59). The only factors that demonstrated a significant (p<0.05) positive relationship to calf circumference were male sex and BMI.
Conclusion: We have observed significant advantages in the BFR group when analyzing absolute calf strength metrics when compared to a randomized control group. This indicates that, when used during rehabilitation following Achilles rupture, BFR therapy may increase the strength of the operative leg and may facilitate recovery and outcome.
DOI: 10.1177/2473011421S00032
Is There a Difference in PROMIS Outcomes Between Patients Who Received K-Wire or Intramedullary Implant PIP Joint Arthrodesis for Hammertoe Deformity?
Amanda M. Holleran, MD; Daniel Homeier; Judith F. Baumhauer, MD, MS, MPH; Adolph S. Flemister, MD; Irvin Oh, MD; Benedict F. DiGiovanni, MD; Gabriel A. Ramirez; Caroline Thirukumaran, MBBS, PhD, MHA; John P. Ketz, MD
Introduction/Purpose: Hammertoe corrective procedures are common foot and ankle procedures. Traditionally Kirshner wire (K-wire) fixation has been the gold standard in terms of fixation. Due issues such as pin loosening, failure, tract infection, fibrous pseudoarthrosis, and recurrent deformity with K-wire fixation, newer intramedullary implants have become widely used in the foot and ankle community. These implants have increased cost compared to K-wire fixation. The primary purpose of this study is to evaluate PROMIS T-scores for physical function (PF), pain interference (PI), and depression domains in patients who have undergone PIP arthrodesis by either K-wire or intramedullary fixation. The secondary goal is to determine if there are any differences in these two fixation groups in regard to complication or recurrence rates.
Methods: From January 2010 to November 2019, prospective Patient Reported Outcome Measure Information System (PROMIS) score data was retrospectively reviewed for patients who had undergone a hammertoe deformity correction at a multi- surgeon tertiary foot and ankle clinic. Inclusion criteria was patient’s older than 18 years, failed conservative management, undergone correction of lesser toe deformity with either K wire fixation or intramedullary fixation. Exclusion criteria was inadequate PROMIS data, previous fracture in same toe, revision surgery, both K wire and intramedullary fixation in the same toe. Preoperative scores were evaluated compared to postoperative scores at multiple time points. Chart review was also performed for patient demographics, complications, and revision surgery. PROMIS physical function (PF), depression, and pain interference (PI) scores were evaluated. Patients with incomplete data sets were excluded from the study. Complications and number of reoperations were noted for each group.
Results: 252 patients met inclusion criteria, 111 and 138 patient in the intramedullary (IM) and K-wire groups (KW) respectively. Univarate analysis demonstrated significant improvement in PROMIS PF and PI in IM group compared to KW group. Multivariate analysis demonstrated the following: KW group demonstrates a 2.9 point decrease in PROMIS PF post-operative scores relative to the IM group (95% CI -4.75 to -0.99; p = 0.003). The IM implants had significantly higher PF scores than the K-wire group at final follow up (p<0.05). BMI, smoking, and Medicare/Medicaid insurance demonstrated worse PF scores (p<0.05). PROMIS PI did not demonstrate a difference between groups (95% CI -0.377 to 3.724; p = 0.110). The KW group did not demonstrate increase recurrance rate (OR 0.348 95% CI 0.118-1.027; p = 0.056), but did trend towards a higher complication rate compared to the IM group (OR 2.049, 95% CI 0.92 to -4.54; p = 0.078).
Conclusion: There is evidence that use of intramedullary implants for operative correction of hammertoe deformity is superior to K-wire fixation in regard to post-operative patient reported measures, specifically the PROMIS domains of physical function. Intramedullary implant use does not increase complication or recurrence rates. Additionally, advanced age, increased BMI, positive smoking status, and Medicare or Medicaid payor status negatively affect patient reported outcomes, which can be used to council patients appropriately. The limitations are that cost of intramedullary implants, are more expensive when compared to conventional K-wires.
DOI: 10.1177/2473011421S00033
Early Outcomes, Revisions, and Patient Satisfaction Following Synthetic Cartilage Implant for Hallux Rigidus
Kenneth J. Hunt, MD; Mark W. Bowers, MD; Mary C. Hamati, MD; Jonathan Bartolomei, MS; Daniel K. Moon, MD, MS, MBA; Joshua A. Metzl, MD
Introduction/Purpose: Hallux rigidus is a common condition estimated to affect 1 in 40 adults older than 60 years old. Patients experience functional limitations secondary to progressive pain and stiffness of the 1st metatarsophalangeal (MTP) joint. Historically, 1st MTP arthrodesis has been considered the gold-standard treatment for end-stage hallux rigidus. In 2016, the US Food and Drug Administration (FDA) approved the use of a synthetic cartilage implant (SCI) for the treatment of hallux rigidus grades 2-4 with an aim to improve pain and preserve range of motion at the 1st MTP joint. Studies evaluating patient satisfaction and need for reoperation have varied considerably (4-20%). We aim to evaluate outcomes, complication rate, revision rate, and overall satisfaction for patients undergoing primary SCI for hallux rigidus.
Methods: In a single-institution retrospective study, we evaluated patients undergoing primary SCI for hallux rigidus between August 2016 to May 2020 by three fellowship-trained foot and ankle surgeons. Preoperatively, patient demographics, age at the time of surgery, laterality, body mass index (BMI), hallux rigidus grade, hallux valgus angle, and first-second intermetatarsal angle were collected. Operative reports were reviewed for concomitant procedures and implant size. Postoperatively, we recorded all additional treatments for continued pain or stiffness and need for revision surgery or conversion to arthrodesis. Patients were surveyed via email or telephone by an author not previously involved in their care administering patient reported outcomes (PROs): PROMIS physical function (PF), and pain interference (PI) surveys, foot and ankle SANE score, and a satisfaction survey.
Results: A total of 59 feet in 56 patients underwent a primary SCI procedure for hallux rigidus. Patients were classified as grade 2 (32%), 3 (59%), or 4 (2%). Nineteen (34%) patients underwent additional procedures, and 8 (14%) had a history of prior surgery to the MTP joint. Forty-five patients (80%) completed surveys at an average of 19.5-month follow-up. The majority (58%) considered surgery a success and 42% reported being unsatisfied or very unsatisfied. Mean (+-SD) post-operative foot and ankle SANE, PROMIS PF and PI scores were 57 (+-27), 48 (+-7) and 54 (+-9), respectively. The overall revision rate was 11% (6/56) with 3 patients undergoing conversion to arthrodesis. The majority of patients (61%) stated they would undergo the procedure again.
Conclusion: Consistent with existing literature, we found that the majority of patients undergoing the procedure were satisfied and would undergo the procedure again. Further, post-operative PRO scores were favorable, even when factoring in patients who were less satisfied. While our revision rate (11%) is consistent with early studies of the implant, 42% reported being unsatisfied or very unsatisfied with their procedure. These findings emphasize the importance of preoperative patient counseling regarding post- operative limitations, risks, satisfaction, and revisions rates. Further investigation into factors that may predict successful outcomes is needed to inform surgical decision-making and appropriate patient selection for this procedure.
DOI: 10.1177/2473011421S00034
Factors Influencing the Nonunion Rate Following First Metatarsophalangeal Joint Arthrodesis
Amir R. Kachooei, MD; Steven M. Raikin, MD; Joseph N. Daniel, DO
Introduction/Purpose: The choice of fixation, biomechanical stability, and hardware density might influence the union after the first metatarsophalangeal (MTP) arthrodesis. This study aimed to assess the influencing factors on the union rate and fixation failure after MTP-1 arthrodesis.
Methods: In this retrospective cohort study, we included 359 patients with 378 feet from the practice of two foot and ankle surgeons. The surgical technique was identical. The providers randomized patients to receive either the locking plate or cross screws, which comprised 187 (50%) plate fixation and 191 (50%) cross screw fixation. Radiographic union was assessed at three months and the final follow-up and was further categorized as symptomatic versus asymptomatic nonunion.
Results: Accounting for potential interaction between variables using multivariable logistic analysis, plate fixation (P=0.018), and diabetes (P=0.044) were significantly associated with a higher nonunion rate. At three month follow-up, 15 (8.3%) patients in the locking plate group and 5 (2.5%) patients in the cross screws group showed nonunion. Of 15 nonunion with plate fixation, 6 (40%) underwent a second surgery because of device failure, while none of the screw fixations required a second surgery (P<0.001). In comparison to asymptomatic nonunion, remaining symptomatic at three months follow-up was a significant risk factor for developing a nonunion with possible device failure at the final follow-up requiring intervention.
Conclusion: Cross screw fixation is significantly associated with a lower nonunion, device failure, and secondary surgery rate than plate fixation, which might be related to contact surfaces and biomechanical stability. Besides, the cost saving is more with the cross screws than plate and screws. Diabetic patients should be counseled about the higher nonunion rate.
DOI: 10.1177/2473011421S00035
Total Ankle Arthroplasty Outcome in Patients with Inflammatory vs Non-Inflammatory Arthritis: Systematic Review and Meta-Analysis
Amir R. Kachooei, MD; Alireza Mousavian, MD; Lew C. Schon, MD; Joseph N. Daniel, DO; David I. Pedowitz, MD, MS
Introduction/Purpose: The decision regarding total ankle replacement is challenging in inflammatory arthritis patients regarding more inferior bone quality, large bone cysts, and increased risk for infections. This systematic review aimed to compare the short and long-term results of total ankle replacement, including the revision rate and the patient-reported outcomes between inflammatory rheumatoid arthritis (RA) versus non-inflammatory ankle osteoarthritis (OA).
Methods: All published clinical studies on total ankle arthroplasty were searched in the databases. We extracted the data, specifically the American Orthopaedic Foot & Ankle Society (AOFAS) improvement, complication rate, and the reoperation rate. The results were also analyzed based on the prosthesis type.
Results: In total, 34 trials were included in our study. Out of 5,078 patients, the underlying condition was rheumatoid arthritis in 1,327 patients and was non-inflammatory osteoarthritis in 2,849 patients. There was statistically significant higher AOFAS improvement in the patients with RA vs. OA with a mean follow-up of 63 months (P=0.009). The rates of TAA removal or revision were estimated at 16% (95% CI, 10%-23%) in the OA and 13% (95% CI, 9%-18%) in the RA group. Overlapping confidence intervals showed no significant difference in the rate of failure between RA and OA. The survival rate was 66% in the OA group and 88% in the RA group during a 63-month follow-up.
Conclusion: Total ankle replacement is a safe procedure in RA patients with fewer minor and major complications relative to other reasons for ankle osteoarthritis.
DOI: 10.1177/2473011421S00036
Subtalar Arthrodesis and Dynamic Medial Column Stabilization in the Surgical Treatment of Rigid Progressive Collapsing Foot Deformity: A Comparative Analysis with Triple Arthrodesis
Jaeyoung Kim, MD; Kim Ji-Beom, MD; Woo-Chun Lee, MD
Category: Hindfoot; Midfoot/Forefoot
Keywords: Subtalar Arthrodesis; FHL; Flatfoot
Introduction/Purpose: In the surgical treatment of rigid progressive collapsing foot deformity (PCFD), triple arthrodesis has been commonly used for its ability to correct multiplanar deformities. However, complications associated with postoperative stiffness resulting from the added number of arthrodesis have led to an interest in more joint sparing options. A recent study has shown that dynamic medial column stabilization (DMCS), which transfers flexor hallucis longus tendon to the first metatarsal base, successfully restores medial longitudinal arch without the need for arthrodesis. This study aimed to evaluate the results of subtalar arthrodesis with dynamic medial column stabilization (DMCS) in treating rigid PCFD compared to the triple arthrodesis.
Methods: Sixteen patients (18 feet) who underwent triple arthrodesis (TA group) and 24 patients (24 feet) who underwent subtalar arthrodesis and DMCS (SA+DMCS group) for surgical correction of rigid PCFD were reviewed. Five radiographic parameters were measured preoperatively, 3 months, 6 months postoperatively, and at the last follow-up (minimum 2 years) to compare the amount of correction and its maintenance. Clinical outcomes were assessed using a visual analogue scale (VAS) and foot function index (FFI). Complications such as non-union, development of adjacent joint arthritis were recorded.
Results: TA group demonstrated a greater amount of correction in the Meary angle than the SA+DMCS group at 3 months postoperatively. However, the TA group showed a significant decrease in the medial cuneiform height, navicular-1st metatarsal angle, and Meary angle at 6 months compared to the initial reduction at 3 months. In contrast, the SA+DMCS group maintained initial correction throughout the follow-up (Figure 1). Clinical scores improved in all patients. Degenerative arthritis in the NC and TMT joints newly developed in nine and one foot, respectively, in the TA group. In contrast, there were no patients with newly developed arthritis in the SA+DMCS group. Postoperative valgus talar tilt occurred with nine ankles in the TA group, whereas only one ankle in the SA+DMCS group. One non-union of the subtalar arthrodesis occurred in the SA+DMCS group.
Conclusion: SA+DMCS group demonstrated a comparable amount of correction as the TA group and maintained initial correction throughout the follow-up period. Additionally, the SA+DMCS group developed fewer complications than the TA group. The current findings suggest that SA+DMCS may be a viable option in treating rigid PCFD deformity with less concern for the complications related to the stiffness.
DOI: 10.1177/2473011421S00037
Does Distal Metatarsal Articular Angle Reflect A Real Joint Deformity in Hallux Valgus?
Matthieu Lalevée; Nacime S. Mansur, MD; Eli Schmidt; Kevin N. Dibbern, PhD; Emilio Wagner, MD; Pablo Wagner, MD; Caio A. Nery; Francois Lintz, MD MSc FEBOT; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: The Distal Metatarsal Articular Angle (DMAA) has long been described as a valgus increase of the distal articular surface of the first metatarsal in Hallux Valgus (HV) deformity. Since then, several studies have reported a poor reliability of this measurement and some authors currently claim that DMAA is misinterpreted as just the rounded shape of the lateral part of the first metatarsal head reflecting pronation of the first ray and could also be biased by the first metatarsal plantarflexion angle. Our study aimed to compare the DMAA in HV and control populations after correcting, with a dedicated software, pronation and plantarflexion of the first metatarsal. We hypothesized that after correction, DMAA will be higher in the HV population, especially in juvenile cases.
Methods: We performed a retrospective case-control study including 36 HV and 20 control feet. Patients under 15 or with surgery antecedent were excluded. DMAA1 was measured as initially described on X-rays by the angle between the distal articular surface and the longitudinal axis of the first metatarsal. DMAA2 was measured on Weight Bearing Computed Tomography (WBCT) without any corrections. DMAA3 was measured after correction of the first metatarsal plantarflexion in the sagittal plane. DMAA4 was measured after correction of the pronation of the first ray relative to the ground in the coronal plane using the alpha-angle. And DMAA5 after both corrections. Corrections in the coronal and sagittal planes were performed along the axis of the first metatarsal. Normality was assessed using Shapiro-Wilk tests. Comparisons were made using Student tests for normal variables and Mann-Whitney for non-normals. Correlations between age and angles were assessed by the Pearson correlation coefficient.
Results: HV and Control groups were comparable on BMI (p=0.69), Age (p=0.58) and Gender (p=0.27). DMAA1 (25.9°+/-7.3 vs 7.6°+/-4.2; p<0.01), DMAA2 (19.1°+/-7.1 vs 3.3°+/-2.4; p<0.01), DMAA3 (16.1°+/-6.2 vs 2.9°+/-2.4; p<0.01), DMAA4 (14.4°+/-5.7 vs 2.6°+/-2.5; p<0.01) and DMAA5 (11.9°+/-4.9 vs 3.3°+/-2.9; p<0.01) were significantly higher in the HV group than in the Control group. Significant decreases in angles were present between DMAA1 and DMAA2 (Δ=-6.9; CI95[-8.6;-5.1]; p<0.01), DMAA2 and DMAA3 (Δ=-3; CI95[-4.1;-1.9]; p<0.01), DMAA2 and DMAA4 (Δ=-4.7; CI95%[-6.3;-3.1]; p<0.01), DMAA2 and DMAA5 (Δ=-7.2 ;CI95%[-8.8;-5.6]; p<0.01) and between DMAA3 and DMAA4 (Δ=-1.7 ;CI95%[-2.9;-0.5]; p<0.01) in the HV group. No significant correlation was found between the 5 different DMAA values and the age in the HV group (respectively ρ=0.1,p=0.55 ; ρ=0.31,p=0.07 ; ρ=0.19,p=0.28 ; ρ=0.1,p=0.56 ; ρ=0.04,p=0.83).
Conclusion: Although overestimated with the 2-dimensional DMAA assessment, the valgus increase of the distal articular surface of the first metatarsal was present in the HV deformity, even after correction of pronation and plantarflexion of the first ray. DMAA overestimation was close to 14 degrees on X-rays and 7 degrees on WBCT without any correction and pronation of the first metatarsal seemed to play a more important role on this overestimation than plantarflexion. Age did not seem to influence this deformity. Increase of valgus of the distal articular surface of the first metatarsal should be considered in HV correction surgical planning.
DOI: 10.1177/2473011421S00038
Impact of Resilience on Long Term Outcomes of Open Brostrom-Gould Repair
Megan Lameka; Aseel G. Dib, BS; Nicholas A. Andrews; Timothy Torrez; Vyshnavi Rallapalle; Tanvee Sinha; Ashish Shah, MD
Introduction/Purpose: The Brostrom-Gould procedure has become known as the gold standard operative procedure for lateral ankle ligament repair. However, little is known about the factors effecting the intermediate outcomes of the Brostrom- Gould repair as measured by new patient reported outcomes instruments and the impact of resilience on post-operative outcomes. This is the first study investigate the impact of resilience on the outcomes of lateral ligament repair.
Methods: A retrospective chart review was performed on 173 patients identified using CPT code 27698 who underwent open modified Brostrom Gould lateral ligament repair from Jan 2013 to June 2020. Patient demographics, comorbidities, athletic activities, post op complications as well as co-pathologies commonly seen in CAI were collected. PROMIS Pain Interference v1.1, Physical Function v1.2, and FAAM were collected. Brief Resilience Scale was used to quantify resilience. A linear regression model was constructed to evaluate the independent effect of resilience on each PROMIS and FAAM outcome instrument. Variables were included in the regression model based on an a-priori significance threshold of p<.05 in bivariate analysis.
Results: Resilience was found to have an independent effect on all PROMIS and FAAM measures when controlling for the effect of confounding variables. Resilience’s effect on outcome measures was as follows: PROMIS physical function (Unstandardized β 8.2, 95% CI 3.9 to 12.6), PROMIS Pain Interference (Unstandardized β -4.8, 95% CI -7.9 to -1.7), FAAM Activity of Daily Living Subscale (Unstandardized β 16.6, 95% CI 8.7 to 24.6), and FAAM Sports Subscale (Unstandardized β 28.4, 95% CI 15.9 to 40.9). Preoperative participation in athletic activities also had a positive independent effect on multiple outcomes metrics including: PROMIS Physical Function (Unstandardized β 9.4, 95% CI 2.8 to 16.0), PROMIS Pain Interference (Unstandardized β -5.3, 95% CI - 10.0 to -.582), and FAAM Sports Subscale scores Interference (Unstandardized β 34.4, 95% CI 15.4 to 53.4).
Conclusion: Resilience and patient participation in athletic activities are independent predictors of improved postoperative functional outcomes as measured by PROMIS and FAAM instruments at intermediate term follow-up. Resilient patients and athletes reported significantly higher physical function and less pain burden postoperatively. Furthermore, preoperative quantification of resilience could enable improved prognostication of patients undergoing lateral ligament repair of the ankle.
DOI: 10.1177/2473011421S00039
2021 J. Leonard Goldner Award Winner: Vancomycin Topically Applied at the Surgical Site Does Not Impair Diabetic Fracture Healing and Dose-Dependently Inhibits Calcified Tissue Formation by Osteoblast Precursors Cells
Alexis Hernandez, MS; Ohidur Rahman, BS; Yazan Kadkoy, MS; Katherine L. Lauritsen, BS; Alexandra Sanchez, BA; Kevin Innella, DO; Anthony Lin, BA; J. Patrick O’Connor, PhD; Joseph Benevenia, MD; David Paglia, PhD; Sheldon S. Lin, MD; Jessica A. Cottrell, PhD
Introduction/Purpose: Prophylactic vancomycin treatment decreases the rates of surgical site and deep infections by >70% for diabetic patients undergoing reconstructive foot and ankle surgery. We aimed to identify whether local vancomycin at a clinically relevant dose impaired fracture healing in diabetic rats. Our hypothesis was that local vancomycin powder to the fracture site would not affect long term healing outcomes, but continuous exposure of vancomycin would inhibit differentiation of osteoblast precursor cells and their osteogenic activity in vitro. The 25 mg/kg vancomycin was a modest increase to routine surgical site vancomycin application of 1-2 grams for a 70 kg. adult (21.42 mg/kg). Determining how vancomycin affects diabetic fracture healing is of clinical interest, particularly considering its prophylactic use in foot and ankle patients.
Methods: Following induction of a femur fracture in male BB Wistar type 1 diabetic rats, a longitudinal incision was made in the lateral aspect of the femur. Powdered vancomycin (25mg/kg) was administered to fracture site of treated (n=5), and Sham surgery (n=6) control rats. Femurs harvested at 6 weeks after fracture, were X-ray scored, µCT scanned and tested to failure in torsion. Bone marrow and periosteal cells isolated from diabetic bones and MC3T3 cells were plated for MTT survival and osteogenic assays. After 4 days, beta glycerol phosphate, ascorbic acid and either 0, 50, 500, or 5,000 µg/mL vancomycin were added to the media (n=3 per group). Cells were fixed at 7 and 14 days for alkaline phosphatase (ALP) staining and at 28 days for Alizarin Red S staining. Parametric data were analyzed using student t-tests. Non-parametric data were analyzed using a Kruskal-Wallis ANOVA on RANKs and Tukey post-hoc tests.
Results: Radiographic scoring did not show differences between the control (2.28+-1.57) and treatment (3.67+-0.75) groups (p=0.093). BV/TV was similar between the control (61.2+-8.4 %) and treatment (56.5+-5.2 %) groups (p=0.081). Mechanical testing found similar values in normalized torque to failure (69.56+-36.80 vs 50.05+-28.82 %N*mm, p=0.356), and torsional rigidity (105.97+-103.62 vs 48.68+-32.95 %Nmm2, p=0.291), for control and treatment groups, respectively. ALP staining was comparable between groups at either 7 (p=0.809) or 14 days (p=0.343) in bone marrow or MC3T3 cells. Alizarin Red S staining found dose- dependent decreases in mineralized nodule formation between the untreated (10.16+-5.01 nodules per 3.8cm2), and 500µg/mL vancomycin (3.16+-2.26 nodules per 3.8cm2) bone marrow groups at 28 days (p=0.026). Periosteal and MC3T3 cell viability were only impaired at the 5000µg/mL vancomycin dose (p=0.001).
Conclusion: Our study argues that local application of vancomycin does not affect diabetic fracture healing at clinically relevant doses. We studied a nearly 2-fold higher vancomycin dose than the ‘standard’ dose of 14.3mg/kg and less than the 143.5mg/kg dose that did not impair rat spine fusion. Although in vitro vancomycin did not affect cell viability and osteogenic staining in periosteal and MC3T3 cells, mineralized nodule formation was dose-dependently inhibited at day 28 in bone marrow cells. Our results bring novel insight into the effects of vancomycin in diabetic fracture healing and the how long-term dosing impacts cell viability and osteoblastogenesis.
DOI: 10.1177/2473011421S00040
Comparison of Suture-Button Fixation with Suture-Tape Augmentation and Trans-Syndesmotic Screw Fixation for Syndemosis Injury: A Biomechanical Study
Hong Seop Lee; Hong S. Lee, MD; Ki Won Young; Young Koo Lee, MD, PhD; Woo Jong Kim
Category: Ankle; Basic Sciences/Biologics
Keywords: Ankle; Biomechanics of the Foot and Ankle; Syndesmosis
Introduction/Purpose: The treatment of syndesmotic injuries with ankle fractures is controversial. The purpose of this study was to compare the biomechanical properties of suture-button fixation with suture-tape augmentation with those of screw fixation.
Methods: Ten matched pairs of human cadaver specimens were subjected to suture-button fixation with suture-tape augmentation or screw fixation. Each specimen underwent initial intact physiologic loading, consisting of 10 cycles of axial loading with peak of 750N, 10 cycles of external torsional loading with peak of 7.5Nm, and 10 cycles of combined axial and external torsional loading with peak of 750N and 7.5Nm at 0.05 Hz. Injuries of the anterior inferior tibiofibular ligament, tibiofibular interosseous membrane, posterior tibiofibular ligament and medial malleolar fracture were applied to each specimen. Postfixation cyclic loading consisted of 50 cycles of combinedaxial and external rotation loading with peak torques of 750 N and 7.5 Nm at a rate of 0.05 Hz. After postfixation loading, each specimen underwent failure loading by external rotation at 0.25 degrees/second. Failure torque and failure angle were measured.
Results: Mean failure torques were 15.99 +- 8.88 Nm in the suture-button fixation with suture-tape augmentation and 17.10 +- 10.38 Nm in the screw group. There was no significant difference in average failure torque between two groups (p-value = 0.669)Average failure angle in screw-fixation group (39.37 +- 10.19 deg) was significantly lower than average failure angle suture- button fixation with suture-tape augmentation (56.64 +- 9.64 deg) (p-value = 0.001).Average rotational stiffness in screw-fixation group (0.53 +- 0.24 Nm/deg) was significantly higher than average rotational stiffness in suture-button fixation with suture-tape augmentation group (0.35 +- 0.19 Nm/deg) (p-value = 0.033).
Conclusion: Suture-button fixation with suture-tape augmentation for ankle syndesmotic injury provides similar torsional strength to that of screw fixation and has lower stiffness than screw fixation. Therefore, Suture-button fixation with suture-tape augmentation can be considered as an alternative treatment option for syndesmosis injury.
DOI: 10.1177/2473011421S00041
Dynamic Syndesmotic Stabilisation and Reinforcement of the Antero-Inferior Tibiofibular Ligament with Internal Brace: Early Results and Clinical Outcome
Introduction/Purpose: Syndesmotic injuries are associated with long recovery times and high morbidity. Systematic reviews show a trend toward better outcomes of dynamic suture buttons compared to screw fixation. Higher rates of malreduction have been reported with screw fixation. The anteroinferior tibiofibular ligament (AITFL) confers the most significant component of translational and rotatory stability. Techniques have developed which reinforce the AITFL. This study aimed to assess results of syndesmotic stabilisation with dynamic stabilisation and reinforcement of the AITFL, with an early mobilisation program.
Methods: Retrospective case series of 30 patients (mean age 31 years). Syndesmotic instability was confirmed with clinical examination, MRI and weightbearing-CT. In all cases arthroscopic assessment confirmed the instability intraoperatively and anatomic reduction with an AO clamp was achieved under direct vision. Dynamic syndesmotic stabilisation with a single suture button was performed followed by the placement of an Internal Brace over the AITFL. A standardized postoperative rehabilitation protocol was established. Patients were asked to immediately weight bear in a CAM boot for 6 weeks, commence sagittal Range of Motion (ROM) at 2 weeks, cycling at 4 weeks. At 6 weeks patients continued with full ROM and strengthening, running and cutting at 8 weeks and return to sports at 10 weeks. Foot and Ankle Ability Measure (FAAM) scores were collected postoperatively and outcome of acute and chronic injuries were compared.
Results: The average follow-up was 13 months. The total FAAM score for ADL was 95+-4.9% (range, 83 - 100%) and for sport activities 87+-13.6% (range, 50 - 100%). The rating of mean postoperative function for ADL was 94+-5.5% (range, 80 - 100%) and 90+-13% (range, 35 - 100%) for sportv. The difference between acute and chronic injuries was statistically higher (p<0.05) for daily activities and sport, but the rating of current level of sport activites as well as for daily activites did not show a significant difference (p=0.9296 and p=0.1615, respectively). Twenty-seven patients (90%) rated their overall current level of function as normal or nearly normal.
Conclusion: This technique aims to directly stabilise the AITFL and the interosseous components of the syndesmosis, and allow early mobilisation and return to sport as early as 10 weeks. Early results show the procedure is safe, with comparable results to the literature. Acute injuries showed better results of the FAAM score than chronic injuries. Long term follow up will address long term outcomes, requirement for removal of devices and how well the Internal brace is tolerated.
DOI: 10.1177/2473011421S00042
Hindfoot Varus Deformity: An Essential but Easily Neglected Pathological Change in Müller-Weiss Disease
Shuyuan Li, MD, PhD; Mark S. Myerson, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: The key pathology of Müller-Weiss Disease (MWD) is fragmentation of the lateral pole of the navicular which leads to lateral rotation of the talar head, inversion of the subtalar joint, and eventually collapse of the medial arch with a paradoxical flatfoot deformity since the varus heel persists. Treatment for MWD should be based on an understanding of this unusual hind and midfoot deformity in order to achieve ideal outcomes. For years however, some authors have treated MWD as a flatfoot deformity instead of correction of the varus heel. This study used weightbearing CT (WBCT) images to demonstrate the structural and alignment changes of the hindfoot and medial arch in patients with MWD compared to those of controls and patients with adult acquired flatfoot deformity (AAFD).
Methods: Twelve patients with 17 feet from two medical centers with a clinical diagnosis of MWD were retrospectively reviewed. Ten feet with flexible AAFD were chosen as the flatfoot control group. Ten feet without deformity, arthritis, a history of trauma, or prior surgical history in the foot and ankle were chosen as normal controls. The hindfoot moment arm (HMA), foot and ankle offset (FAO), middle facet subluxation (MFS), talonavicular joint coverage angle (TNCA), and the percentage of calcaneocuboid joint subluxation (CCS) measured on WBCT were used to assess the alignment of the hindfoot and peritalar joints. The arch height index was used to assess the height of the medial arch. Positive was used to reflect lateral subluxations and negative was for the medial ones. ANOVA test were used to compare data among the three groups with a normal distribution, while Wilcoxon test were used for non normal distribution.
Results: According to WBCT analysis, patients with MWD showed totally different hindfoot alignment and peritalar subluxation characteristics compared to the AAFD and the normal control groups. In the order of MWD, AAFD and control, the mean HMA values were -3.44 mm, 15.75 mm, and 3.19 mm, FAO values were -0.72%, 7.42%, and 2.63%. TNCA values were -7.18, 22.11, and 11.37; MFS values were 14%, 45%, and 23%; CCS values were -0.19, 0 and -0.04. The arch height index values were 0.46, 0.45, and 0.58. There was statistically significant difference among the three groups in all the above parameters except the middle facet subluxation and fifth metatarsal medial cuneiform height ratios between the MWD group and the normal controls.
Conclusion: This study confirmed that hindfoot varus is a typical feature of MWD. And this is the first study to demonstrate that peritalar subluxation is an important marker. With lateral rotation of the talar head, the subtalar joint is driven into varus, with medial subluxation of both the middle facet and the calcaneocuboid joint, resulting in peritalar subluxation opposite to that of AAFD. No significant difference between the medial arch of the MWD group and the controls was present. In conclusion, structural changes of the midfoot and hindfoot totally different from the characteristics of AAFD are present in MWD.
DOI: 10.1177/2473011421S00043
2021 Roger A. Mann Award Winner: Long-Term Revision Rates and Functional Outcomes of Total Ankle Arthroplasty and Ankle Arthrodesis
Evan M. Loewy, MD; Kevin M. Goodson, MD; Kevin Huang, MS; Alexandrea Perkins, BS; Arthur K. Walling, MD
Introduction/Purpose: Recent studies have shown acceptable long-term survival rates with TAA however there remains a general paucity of information directly comparing ankle arthroplasty to arthrodesis over long-term follow-up. This study compares revision rates and functional outcomes for a large cohort of patients undergoing ankle arthrodesis or arthroplasty. All surgeries were performed by a single surgeon from 1999 to 2013. Ankle arthrodesis was performed using a standardized 3-screw technique with anterior plate supplementation. Arthroplasty was performed utilizing the Scandinavian Total Ankle Replacement (STAR) prosthesis.
Methods: A retrospective chart review was performed for 335 consecutive cases in 326 patients (198 ankles in the arthrodesis group and 137 in the arthroplasty group). Patient demographics including age, sex, body mass index (BMI), and preoperative diagnoses were collected. Foot Function Index (FFI) scores were obtained and recorded at final outpatient follow-up. Primary outcomes included the rate of revision surgery and functional outcome scores. Secondary outcomes included perioperative complications such as polyethylene fracture and patients who went on to undergo postoperative subtalar fusion for symptomatic adjacent joint arthritis.
Results: Ten (6%) ankles in the arthrodesis group and twenty-one (15%) in the arthroplasty group required revision surgery at a mean of 8.9 +- 6.5 and 61.1 +- 52.9 months, respectively [P=.039]. One hundred four of the 335 cases were available to complete functional outcome surveys at final follow-up at a mean of 11.2 +- 4.1 years from time of surgery (minimum 6-year follow-up). Mean FFI scores were significantly better in the arthroplasty group (40.3 +- 36.9) than in the arthrodesis group (61.5 +- 45.1) [P=.011]. Thirteen polyethylene components in 12 TAAs (8.7%) required replacement for fracture at an average of 9.6 +- 4.2 years postoperatively. Seven (3.5%) cases in the arthrodesis group and three (2.2%) in the arthroplasty group went on to undergo subtalar fusion at an average of 4.9 +- 3.9 years post-operation [P=.536].
Conclusion: Long-term functional outcome scores were better in TAA patients; however, the revision rate for major complications was found to be greater over time. While the ankle arthroplasty group did show a slightly lower frequency of adjacent joint arthritis progression leading to subsequent subtalar fusion, this difference was not statistically significant. To our knowledge, this is the largest and longest-term follow-up comparing the STAR prosthesis to ankle arthrodesis published in the United States to date.
DOI: 10.1177/2473011421S00044
Radiographic Indirect Parameters for First Metatarsal Rotation do not Correspond to Real Measurements in Hallux Valgus
Nacime S. Mansur, MD; Matthieu Lalevee, MD; Eli Schmidt; Tutku Tazegul; Kevin N. Dibbern, PhD; Emilio Wagner, MD; Pablo Wagner, MD; John E. Femino, MD; Caio A. Nery; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Subjective radiographic findings are commonly used in Hallux Valgus (HV) to dictate deformity aspects and surgical treatment. Head roundness, distal metatarsal metaphyseal angle (DMMA) and sesamoid positioning are being employed as predictors of ray pronation, intrinsic deformities, and soft tissue imbalance despite the lack of these observations’ reliability. Estimation of first metatarsal rotation based on different head shapes has been proposed, including classifications for its severity. The objective of this study was to demonstrate if first metatarsal rotation measured by the alpha angle in weight-bearing computerized tomography (WBCT) images correlates with its head shape. We hypothesized that alpha angle values would not reliably reflect an indirect classification for rotation, and other variables would contribute to miscalculation.
Methods: In this IRB-approved, case-control retrospective study, we analyzed 26 hallux valgus feet (19 patients) and 20 control feet (16 patients) through conventional radiographs (XR) and WBCT images. Two blinded fellowship-trained orthopedic foot and ankle surgeon performed the measurements. Head format, roundness classifications (0, 1, 2 or 3), head plantar surface diameter, hallux valgus angle (HVA), intermetatarsal angle (IMA), DDMA, sesamoid station, sesamoid rotation, sesamoid arthritis, and metatarsal rotation (alpha angle) were evaluated. Interclass Correlations Coefficients (ICC) were performed for interrater reliability. Normative data were analyzed by ANOVA and comparison among groups and methods by Student’s T-test. A multivariate regression analysis was executed to evaluate which of the measurements influenced the rotation classification and a partition prediction model constructed to find how the variables contributed to the grading system. Statistical significancy was considered for p-values of less than 0.05.
Results: All ICCs were found above 0.80 within both XR and WBCT readings. HV patients and controls were analogous regarding age and body mass index. Similarity was also found in WBCT and XR for traditional HV angles, considering both groups. Mean values were higher in HV patients than controls when evaluating alpha angle (11.51 [9.42-13.60] to 4.23 [1.84-6.62], 95%CI), head diameter (22.35 [21.52-23.18] to 21.01 [20.07-21.96]) and sesamoid rotation angle (26.72 [24.09-29.34] to 4.56 [1.63-7.50]). HVA and IMA were poorly correlated to alpha angles (values below 0.11). WBCT assessment downgraded the head roundness classification in comparison to XR. Changes in this classification were explained chiefly by the sesamoid station in the axial plane (R2: 0.37), where stations 4 to 7 were found to be strong predictors of roundness classification 2 and 3. The alpha angle had a low influence in head roundness classification (R2: 0.15).
Conclusion: Metatarsal rotation cannot be reliably predicted through head roundness. Glenosesamoid arthritis and sesamoid subluxation alter the first metatarsal head format and diameter, blurring roundness evaluation. Sesamoid stations from 4 to 7 were strong predictors of higher roundness classifications. Measurements using different readers and methods (XR and WBCT) were reliable. First ray rotation (alpha angle) values did not influence head roundness classification strongly nor were correlated to HV severity.
DOI: 10.1177/2473011421S00045
Inter-Rater Reliability of Classifications for Fifth Metatarsal Base Fractures
Max Michalski, MD; John Y. Kwon, MD; Eitan M. Ingall; Christopher P. Chiodo, MD
Category: Trauma; Midfoot/Forefoot; Sports
Keywords: 5th Metatarsal Fractures; Metatarsals; Jones Fracture
Introduction/Purpose: Fractures of the fifth metatarsal base have been a source of confusion since their original description by Jones in 1902. The term Jones’ fracture has been used indiscriminately leading to further confusion. Zone classifications have been described but never evaluated for their reliability. The most recent classification, metaphyseal versus metaphyseal-diaphyseal is unknown to most surgeons. The purpose of this study was to evaluate the inter-rater reliability of American Orthopaedic Foot & Ankle Society (AOFAS) members classifying fractures of the base of the fifth metatarsal.
Methods: A survey was emailed to members of the AOFAS including radiographs of 18 fifth metatarsal base fractures. Demographic information was collected in addition to evaluation of the 18 sets of radiographs using three classification systems. Surgeons were asked if the fracture is a Jones’ fracture, zone of the fracture and if the fracture was metaphyseal or metaphyseal- diaphyseal. A total of 223 surgeons with an average experience of 14 years in practice (range: fellow - 50 years) completed the initial survey for inter-rater reliability. Additionally, each surgeon was asked which zones or zone junctions they consider a Jones’ fracture. Reliability was tested using Fleiss’ Kappa scores.
Results: Inter-rater agreement for use of the term Jones’ fracture was moderate (kappa 0.533, 95% confidence interval (CI) [0.530, 0.535]). The zone classification had an inter-rater agreement was moderate (kappa 0.537, 95% CI [0.535, 0.539]). Inter- rater agreement for metaphyseal versus metaphyseal-diaphyseal was substantial (kappa 0.705, 95% CI [0.702, 0.708]). Results of surgeon definition of a Jones’ fracture is seen in Figure 1.
Conclusion: This is the largest study of its kind looking at inter-rater reliability of an orthopaedic classification with 223 raters. The terminology regarding the classification of fifth metatarsal base fractures remains confusing and inconsistent. The term Jones’ fracture has little meaning in terms of communicating these injuries as there is only moderate agreement when surveying surgeons and it is defined differently by most. The zone classification has similar reliability as the Jones’ fracture. The terms metaphyseal and metaphyseal-diaphyseal was the most reliable means to describe these fractures.
DOI: 10.1177/2473011421S00046
Use of Weight-Bearing Computed Tomography in the Evaluation of Abnormal Hindfoot Morphology in Charcot-Marie-Tooth Patients
Max Michalski, MD; Tonya W. An, MD; Edward T. Haupt, MD; Brandon Yeshoua; Jari Salo; Glenn B. Pfeffer, MD
Category: Hindfoot; Other
Keywords: Charcot Marie Tooth; Weight Bearing CT; Cavovarus Foot Deformity
Introduction/Purpose: The hindfoot deformity seen in Charcot-Marie-Tooth disease (CMT) is poorly understood, and the contribution of abnormal bone morphology has never been conclusively demonstrated. The purpose of this study was to compare the three-dimensional (3D) bone morphology of the talus, calcaneus and navicular in a cohort of CMT patients versus a control population. We used the data obtained from weight-bearing computed tomography (WBCT) to reconstruct the geometric shape of each bone using 3D surface meshing techniques. Surface mesh analysis of this type is commonly used in engineering to evaluate and optimize 3D geometries and structures.
Methods: A total of 17 WBCTs from 15 patients (average age 24) with CMT who underwent WBCT without previous surgeries, degenerative changes or open physes were included. These were compared to 20 healthy control WBCTs. Calcaneal measurements included the radius of curvature and the angle between the posterior tuberosity and posterior facet in the sagittal plane. Talar measurements include axial and sagittal declination between the body and neck as well as coronal rotation of the talar head relative to the body. Surface-mesh model analysis was performed comparing the average of the CMT cohort to the controls using CT analysis software (Disior Bonelogic). Means were compared with a t test (p<0.05).
Results: CMT patients had significantly less sagittal declination (plantarflexion) versus controls (14.9 versus 25.1 degrees respectively) (p<0.01). Similarly, CMT patients had less talar head coronal rotation versus controls (30.2 versus 42.5 degrees respectively) (p<0.001). There was no difference in axial rotation of the talar neck versus body between the groups (p=0.88). The calcaneal radius of curvature in CMT patients was significantly smaller than the control population (716.6 versus 2143.5 mm respectively) (p<0.05). Angular differences were also significant between the posterior tuberosity and posterior facet of the subtalar joint in the sagittal plane (CMT 57.7 degrees, control 67.9 degrees) (p<0.001). Additionally, surface-mesh model analysis demonstrated the largest differences in morphology at the navicular tuberosity, medial talar head, sustentaculum tali and anterior process of the calcaneus (Figure 1).
Conclusion: This is the first study to quantify the morphologic differences in osteology seen in CMT patients. The decreased sagittal declination of the talar neck is seen with a reciprocal decreased slope of the posterior facet of the calcaneus. The coronal rotation of the talar head and abnormal navicular tuberosity morphology shows changes seen in patients with CMT and may be attributed to unbalanced pull of the posterior tibial tendon during development. These findings will help refine, and potentially revolutionize the surgical reconstruction of cavovarus deformity in CMT patients.
DOI: 10.1177/2473011421S00047
Declining Trends in Medicare Reimbursement in Orthopaedic Foot and Ankle Surgery
Sandra Miskiel, MD; Matthew Bye, BS; Erik C. Freeland, DO; Andre J. Pagliaro, MD
Introduction/Purpose: With the increasing complexity of physician reimbursement models, understanding reimbursement trends is crucial to the financial sustainability of orthopaedic practices nationwide. Inflation-adjusted Medicare physician reimbursement for total joint arthroplasty has decreased by approximately 33% from 2000 to 2019. Recent trends in orthopaedic foot and ankle reimbursement are unknown. Thus, our study sought to analyze trends in Medicare reimbursement rates from 2000 to 2020 for common orthopaedic foot and ankle surgical procedures.
Methods: The financial database of a single academic tertiary care center was queried to identify the CPT codes most frequently utilized in orthopaedic foot and ankle care. Next, the Physician Fee Schedule Look-Up Tool from the Centers for Medicare & Medicaid Services was queried for the top 30 CPT codes utilized, and physician reimbursement data extracted. Monetary data was subsequently adjusted for inflation utilizing the consumer price index and reported in 2020 US dollars (USD). Average annual and the total percent change in reimbursement were calculated for included procedures.
Results: After adjusting for inflation, the average physician reimbursement decreased by 31.6% for all included foot and ankle procedures from 2000 to 2020, with 23/30 codes decreasing by more than 30%. The greatest decrease in reimbursement observed from 2000 to 2020 was for open treatment of calcaneal fracture at 48.3% ($2,254.17 to $1,164.97), followed by flexor tendon repair at 48.2% ($741.02 to $357.39), and open treatment of pilon fracture at 43.9% ($2,451.37 to $1,076.36).
Conclusion: Over the past two decades, physician reimbursement for foot and ankle procedures has dramatically decreased by up to 48.3%. Continued downward trends in orthopaedic foot and ankle physician reimbursement may lead to decreased access to quality foot and ankle care.
DOI: 10.1177/2473011421S00048
Hardware Choice and Risk Factors of Talonavicular Arthrodesis Non-Union
Tara Moncman, DO; Daniel O. Corr, BS; Parth Kothari, MD; Joseph T. O’Neil, MD; David I. Pedowitz, MD, MS
Introduction/Purpose: Talonavicular arthrodesis is a commonly performed procedure in orthopedic foot and ankle surgery, for conditions including osteoarthritis, instability, and others. The surgery is frequently performed as part of a double or triple arthrodesis. Multiple surgical constructs have been described, including screws, plate/screw constructs, and staple/screw constructs. Few studies exist that specifically focus on the talonavicular joint, and those that do are often limited by low patient volumes. Studies that do examine non-union of the talonavicular joint do not offer comparative data on non-union rates between the different methods of fixation. The purpose of this study was to determine the rate of arthrodesis in talonavicular fusion surgery among different fixation techniques and determine if hardware has a significant effect on union rate among patient factors.
Methods: This is a retrospective single institution, multi-surgeon study evaluating arthrodesis rates in the talonavicular joint. Adult patients undergoing primary talonavicular fusion (isolated or as part of double/triple arthrodesis) from 2015-2018 with a minimum of 3-month radiographic follow-up were studied. Patients undergoing revision talonavicular fusion or fusion as part of Charcot reconstruction were excluded. Patient radiographic and chart notes were reviewed to assess fixation type (single screw, 2-hole compression plate, or screw + staple), the status of the arthrodesis at >=3 months and any hardware complications or reoperations following the index procedure. Descriptive statistics were generated for standard patient demographics and co- morbidities. Non-union rates were calculated for the cohort as a whole and for each fixation technique utilized along with the frequency of hardware complications/removal. Univariate analysis was performed to determine risk factors for increased non- union rate, including patient demographics, co-morbidities, and fixation technique.
Results: A total of 198 patients were included. Hardware included 131 double straight screws, 42 two-hole compression plates, and 25 screw + staple constructs. Seventeen patients (8.59%) had a nonunion of the talonavicular joint at >3 months, while 18 patients (9.09%) had hardware complications of breakage or prominence and 11 (5.56%) required eventual removal. Hardware type was not a significant predictor of nonunion, as 11 patients had straight screw hardware (8.40%), while 3 had a two-hole plate (7.14%) and 3 had screw + staple (12%) (p=0.801). Hardware breakage or backing out occurred in 6/131 patients with straight screws (4.58%), 5/42 with 2-hole plates (11.90%), and 7/25 with staple + screw (28%) (p=0.001). Hardware removal was necessary in 5 (3.82%) straight screw patients, 3 (7.14%) two-hole plate patients, and 3 (12%) screw + staple patients (p=0.186). Patient age, sex, diabetic and smoking status were not significant for nonunion or hardware complication.
Conclusion: The type of hardware used in talonavicular arthrodesis is not a significant factor in achieving union. Staple + screw constructs may be more susceptible to hardware breakage or migration, but was not significant for the necessity of hardware removal, as a number of patients remain painless and achieve the intended union. The authors recommend that physicians can make decisions of which to utilize based on familiarity and preference. Further study is indicated on even larger patient cohorts with increased population of nonunion cases so that further significant patient risk factors for nonunion of the joint can be identified.
DOI: 10.1177/2473011421S00049
TranexAMIC Acid Associated with Less Wound Complications in Hindfoot Surgery
Andrew Moore; Benjamin R. Smith; Ryan J. O’Leary; Caroline P. Hoch; Christopher E. Gross, MD; Daniel J. Scott, MD, MBA
Category: Hindfoot; Ankle
Keywords: Wound Complications; Hindfoot Fusion; Total Ankle Arthroplasty
Introduction/Purpose: Tranexamic acid (TXA) is an increasingly popular antifibrinolytic therapy used to decrease bleeding during surgery and postoperative swelling. TXA has been shown to decrease bleeding in total knee arthroplasty and total hip arthroplasty, and is now routinely administered in many centers performing these operations. To date, there is very limited data on its use in foot and ankle surgery. We sought to review of the effect of TXA on outcomes of total ankle arthroplasty (TAA), hindfoot fusions, and other related hindfoot surgeries, with the hypothesis that patients receiving TXA would exhibit fewer wound complications.
Methods: We conducted a retrospective review of 252 patients (258 operations) undergoing hindfoot fusions and/or TAA between 2015 and 2020 by a single fellowship trained foot and ankle surgeon at an academic medical center. Twenty-seven patients (28 operations) were excluded for less than 90-day follow-up, leaving 230 eligible procedures (TAA=72, subtalar fusion=47, ankle fusion=37, double arthrodesis=33, tibiotalocalcaneal fusion=20, triple arthrodesis=8, total talus=4, and hardware removal=8). Patient demographics, ASA scores, comorbidities, pre-operative diagnoses, smoking status, wound complications, union status (for fusions), readmissions and reoperations were recorded and compared between TXA (n=104) and non-TXA (n=126) cohorts. Subgroup analysis was performed for TAAs and hindfoot fusions. Mean follow-up was 453 days. Continuous variables were compared using independent sample t-test, and categorical variables with chi-square test, unless more than 20% of expected values were less than 5, in which case Fisher’s exact tests were utilized.
Results: There were no significant differences in demographics, comorbidities, preoperative diagnoses or smoking status between cohorts. The TXA group exhibited significantly less postoperative infections requiring oral antibiotics (5.8% vs. 15.1%, p=.024). These included superficial (p=.174) and deep infections requiring reoperation (p=.095). Subgroup analysis of hindfoot fusions (n=146) revealed significantly shorter time to fusion between TXA and non-TXA groups (146 vs. 202 days, p=.049) and fewer reoperations (8.6% vs. 21.6%, p=.042). TXA fusion patients had significantly shorter follow-up (349 vs. 479 days, p=.020), fewer active smokers (5.2% vs. 15.9%, p=.048), but more patients with Charcot neuroarthropathy (20.7% vs. 5.7%, p=.006). Subgroup analysis of TAAs showed fewer infections requiring oral antibiotics (4.7% vs. 31%, p=.005) and less delayed wound healing (25.6% vs. 48.3%, p=.047) in the TXA cohort.
Conclusion: We found TXA use in hindfoot surgery to correlate with a reduction in wound infections requiring antibiotics and quicker time to union in hindfoot fusions. Further, the use of TXA in TAA specifically was correlated with fewer infections requiring antibiotics and lower rates of delayed wound healing. These reductions were both statistically and clinically significant. TXA has already been shown to be beneficial in other areas of orthopaedic surgery and appears to also be quite beneficial in foot and ankle surgery, though further research is needed to confirm these findings.
DOI: 10.1177/2473011421S00050
Comparing Rates of Fusion and Time to Fusion in A Viable Cellular Allograft vs Autograft in Forefoot, Midfoot, and Hindfoot Fusions
G. Andrew Murphy, MD; Shumaila Sarfani, MD; David R. Richardson, MD; Clayton C. Bettin, MD; Benjamin J. Grear, MD
Introduction/Purpose: Allograft is routinely used to enhance bone healing in foot and ankle surgery. One allograft in particular employs viable cells and bone scaffolding in a gel base. There is little evidence that compares how this material effects rate of fusion (ROF) and time to fusion (TTF) when compared to autograft in routine forefoot, midfoot, and hindfoot fusions. Our study investigates the use of a viable cellular allograft and its effect on these two variables in a population of patients undergoing fusions in the foot and ankle.
Methods: A retrospective review was conducted over a five-year span of patients undergoing fusions in the foot and ankle where the cellular allograft was used. We compared the ROF and TTF between the following three graft groups: cellular allograft alone, autograft alone, and combined allograft + autograft. Data was retrieved from the patients’ electronic medical record and TTF was recorded as the time, in days, it took for a solid radiographic fusion to form. Secondary variables collected included etiology of disease (post-traumatic, inflammatory, or diabetic arthropathy) and also analyzed for effect on ROF and TTF.
Results: Two hundred and twenty-five patients underwent a fusion in the foot or ankle over a five-year period. Autograft alone was used in 101 patients, the cellular allograft alone was used in 88 patients, and a combination of autograft and the cellular allograft was used in 36 patients. Each group were similar in their comorbid conditions and demographics. The ROF of the autograft only group was 88% (89/101), compared to the cellular allograft group’s ROF of 89% (78/88), and the combination graft group’s ROF of 75% (27/36). The average TTF between each group varied slightly, with the cellular allograft group fusing the fastest at 86, followed by the autograft alone group at 97 days, and the combined group at 112 days.
Conclusion: Our study investigated the use of a viable cellular allograft and its effect on ROF and TTF compared to autograft alone and autograft combined with said cellular allograft. We found no significant difference in ROF between autograft alone and the cellular allograft alone but did find a significant difference in ROF for the combined group resulting in lower rate of fusion. Additionally, use of the cellular allograft resulted in fastest time to fusion compared to autograft alone or a combination of the graft types.
DOI: 10.1177/2473011421S00051
Risks of Preoperative Opioid Therapy on Forefoot and Hindfoot Surgery Success
William Newton; Kevin D. Shrake; Caroline P. Hoch; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD; William Newton
Introduction/Purpose: Past studies in total joint arthroplasty and orthopaedic trauma have found that preoperative opioid therapy correlates with increased postoperative opioid use and lesser surgical outcomes. To date, these trends have not been studied in cases of forefoot or hindfoot foot and ankle surgery. We hypothesized that patients with preoperative chronic opioid use would have increased likelihood of postoperative opioid use, complications, and re-operation.
Methods: A retrospective review was conducted of forefoot, midfoot and hindfoot surgeries performed from January 2015- September 2020 by a fellowship trained foot and ankle surgeon at an academic medical center. Pre- and postoperative opioid and other analgesic use, medical history, demographic data, operative treatment, and surgical outcomes were reviewed. Records of preoperative opioid use were limited to 50 patients, 90-day postoperative opioid use to 60 patients, and 180-day postoperative opioid use to 69 patients. A total of 149 patients (female=102, male=47) with a mean BMI of 30.87 and mean follow-up up of 1.2 years were included. Of the patients undergoing hindfoot, midfoot, or forefoot arthrodesis, 71/79 joints went on to union, while there were 8 non-unions (3 sub-talar, 2 metatarsophalangeal, 1 tibiotalar, 1 talo-navicular, and 1 calcaneocuboid). The most common procedures were hammertoe correction and Achilles tendon repair. Statistical analysis was performed using correlation, linear multivariate regression, and one-way ANOVA.
Results: Preoperative opioid use was statistically significantly associated with loss to follow-up (users=10.0%, non-users=0.0%; p=.044) and continued postoperative opioid use at 90 (92%; p<.001) and 180 days (94%; p<.001). Preoperative benzodiazepine use was significantly associated with continued postoperative benzodiazepine use at 90 (20%; p<.001) and 180 days (26%; p<.001). Of comorbidities, diabetes (p=.007) and psychiatric disease (p=.025) were significant predictors of postoperative opioid use. Psychiatric disease was also a significant predictor of postoperative benzodiazepine use (p=.026). Postoperative opioid use significantly differed by surgical indication (post-traumatic=20.52 MME, prior procedure(s)=232.51 MME, instability=7.64 MME, osteomyelitis=4.67 MME; p<.001), but postoperative benzodiazepine use did not. Additionally, follow-up duration significantly differed by operated area (hindfoot=1.48 years, forefoot=0.92 years, both=3.02 years; p<.001).
Conclusion: We found that patients with preoperative opioid use have statistically significantly higher rates of loss to follow-up and continued postoperative opioid use. We also found that on average, patients with a history of prior procedures on the forefoot and/or hindfoot require statistically significantly more narcotics than those with a history of post-traumatic injuries, instability, or osteomyelitis. Patients and surgeons should be aware of this data to help appropriately council patients on post- operative expectations.
DOI: 10.1177/2473011421S00052
Hallux Valgus Multiplanar Correction Surgery Through a Minimally Invasive Technique. Our Initial Experience.
Florencia Pacheco, MD; Pablo E. Mocoçain Mac-iver, MD; Stephane Elgueta, MD; Andres Keller Díaz, MD; Ruben D. Radkievich, MD; Diego A. Villagran; David A. Salinas; Marisol Marti
Introduction/Purpose: Recently, minimally invasive surgery for hallux valgus correction has regained popularity. The minimally invasive Chevron and Akin (MICA), has been proved to be as satisfactory for patients as conventional open techniques. However, due to its design, it is difficult to correct the coronal plane malalignment, which could lead to the recurrence of the deformity. Instead, a Bösch-type osteotomy allows multiplanar correction, and with an upgrade in its fixation we can create a stable third- generation percutaneous osteotomy. We report our early results using the minimally invasive Bösch and Akin osteotomy (MIBA).
Methods: This was a prospective case series of our first 40 patients (41 feet) undergoing MIBA procedure. Outcome measures included the Manchester-Oxford Foot Questionnaire (MOXFQ), the AOFAS Forefoot Score, and the visual analog scale (VAS) for pain assessment. Radiographic measures included the hallux valgus angle (HVA), intermetatarsal angle (IMA), distal metatarsal articular angle (DMAA) and the pronation of the metatarsal. All complications and emitted radiation dosage were reported as well.
Results: At 12 months MOXFQ and AOFAS improved from 54.8 to 0.66 (p=0) and 39.1 to 99.2 (p=0), respectively. The mean preoperative VAS was 5.8, and improved during the first week to 1.3 (p<0.05). There was also a significant improvement in all radiographic parameters. We had two significant and five minor complications.
Conclusion: The MIBA procedure is a safe and effective option to achieve a multiplanar hallux valgus correction.
DOI: 10.1177/2473011421S00053
Total Talus Replacement with Subtalar Arthrodesis for End-Stage Talar Osteonecrosis and Adjacent Joint Arthritis
Gregory F. Pereira, MD; Amanda N. Fletcher, MD, MS; Abhinav Balu; James K. DeOrio, MD; Selene G. Parekh, MD, MBA
Introduction/Purpose: Late stage talar avascular necrosis (AVN) results in devascularization of the talus with osteonecrosis, subchondral collapse, talus fracturing, loss of talar height and declination, and adjacent joint arthritis. This results in significant disability for patients with limited treatment options. Tibiotalocalcaneal arthrodesis with structural allograft has been the historic treatment option for this challenging clinical scenario, however, the outcomes are fair with reported nonunion rate up to 40%. Total talus replacement (TTR) is an emerging treatment option for patients with talar AVN. TTR with subtalar arthrodesis may be utilized for end-stage talar AVN with adjacent joint arthritis. The purpose of this study is to evaluate the short-term outcomes for TTR with subtalar arthrodesis including pain, ankle range of motion, union rates, and complications.
Methods: Consecutive patients who underwent TTR with a subtalar arthrodesis from 2016-2020 were retrospectively reviewed. All surgeries were performed by one of two fellowship-trained foot and ankle orthopaedic surgeons at a single academic institution. All talus implants were custom 3D printed total tali (Additive Orthopaedics, Little Silver, NJ), composed of a cobalt chrome alloy. The implants were sized based on computed tomography scans of the contralateral talus. The plantar surface of the tali were prepared with an ingrowth surface and drill holes to accept screws and facilitate subtalar arthrodesis. Patient demographics, comorbidities, and surgical data were collected. Outcomes included the Visual Analog Scale (VAS) scores, range of motion, union rates, and complications. Data analysis was performed with paired t-tests and a significance level of p<0.05.
Results: A total of 19 patients were included with an average of 11.4 months follow-up. There were 11 (57.9%) men, and the average age was 52.3 (range, 18-75) years-old. About half (n=9, 47.4%) of the cohort had a previous talus fracture, and 17 (89.5%) patients had previous ipsilateral ankle surgery. There were 5 (26.3%) patients who underwent concomitant talonavicular arthrodesis at the time of TTR and subtalar arthrodesis. Significant postoperative improvements were observed in VAS scores (2.4 vs. 8.6; p<0.0001), ankle dorsiflexion (10.7° vs. 1.8°; p=0.0131), and ankle plantarflexion (32.9° vs. 21.3°; p<0.0068). All patients achieved a successful union of their subtalar arthrodesis (n=19/19, 100%) and talonavicular arthrodesis (n=5/5, 100%). There were 2 (10.5%) complications including 1 (5.3%) delayed wound healing successfully treated nonoperatively and 1 (5.3%) reoperation in a patient with persistent varus ankle deformity requiring distal tibia and fibula osteotomies. There were no postoperative infections, explants, or amputations required.
Conclusion: TTR with subtalar arthrodesis should be considered as a treatment option for patients with end-stage talar AVN and adjacent joint arthritis. Patients experienced significant improvement in pain and ankle range of motion. The complication rate was 10.5% with only 1 patient requiring a reoperation. A union rate of 100% was observed with no postoperative infections, explants, or amputations. This technique perves ankle motion while eliminating hindfoot pain in patients with loss of talar bony integrity and adjacent joint arthritis. Further studies are required including longer-term follow-up and prospective cohorts to ensure continued safety and efficacy.
DOI: 10.1177/2473011421S00054
Achilles Pathology and Surgical Approach Determine Post-Operative Infection Rate
Carson M. Rider, MD; Oliver B. Hansen; Mark C. Drakos, MD
Introduction/Purpose: Post-operative infections can be a devastating complication after Achilles tendon surgery. While Achilles infection rates have decreased with the development of less invasive surgical techniques, these infections remain a challenging complication for patients and clinicians due to the relative lack of vasculature in the Achilles tendon region. This study aimed to analyze rates of postoperative Achilles tendon infection based on the type of Achilles pathology and surgical approach. We hypothesized that procedures with smaller incisions that avoided the critical zone would be associated with lower infection rates than those that require larger incisions, such as reconstructions.
Methods: All patients undergoing Achilles tendon surgery at a single, multi-surgeon center between 2011 and 2020 were identified. Charts were reviewed for infection, pathology, surgical approach, incision size, and risk factors such as body mass index (BMI), smoking status, and diabetes. Rates of infection were compared between groups based on pathology and operative technique. These groups included acute rupture treated immediately, chronic pathology treated with debridement and repair, and chronic pathology treated with graft reconstruction. For patients treated for an acute rupture, minimally invasive and open approach sub-groups were compared. Further, prevalence of risk factors was compared between patients with and without post- operative infections. Statistical comparisons were performed between groups using a student’s t-test or Fisher’s exact test.
Results: A total of 1,148 cases were identified, 23 of which involved a post-operative infection requiring a return to the operating room for irrigation and debridement. The overall infection rate was 2.00%. Cases involving chronic pathology treated with graft reconstruction were associated with an infection rate of 8.96%. Acute repairs had an infection rate of 1.32% and other chronic pathologies treated without graft reconstruction had an infection rate of 0.73%. Statistical comparisons of infection rates for these sub-groups are displayed in Table 1 alongside comparisons of risk factor prevalence between the infection and non-infection groups. The comparison of risk factors between groups did not identify any significant differences. No infections were observed following the use of a distal lateral incision to treat chronic tendon pathology (179 cases) or the use of a windows incision technique for reconstructions (8 cases).
Conclusion: Analysis of infection rates indicated that treatment options requiring large incisions, such as reconstruction with a graft, pose a significantly greater risk of post-operative Achilles infection. Both minimally invasive treatments and measured open incisions were associated with similarly low infection rates for primary repair of acute ruptures. Comparison of risk factors between patients with and without infection did not reveal any significant differences. Given low infection rates for chronic pathology treated with distal lateral incisions and windows-type incisions, we recommend these whenever possible.
DOI: 10.1177/2473011421S00055
Lateral Instability in Total Ankle Arthroplasty: A Comparison Between the Brostrom-Gould and Anatomic Lateral Ankle Stabilization (ATLAS)
Calvin J. Rushing, DPM; Bryon J. McKenna, DPM; Gregory C. Berlet, MD; Antonio M. Malloy McCoy
Category: Ankle; Sports; Other
Keywords: Ankle Instability; Ankle Sprain; Total Ankle Arthritis
Introduction/Purpose: Lateral ankle instability is not uncommon after osseous cuts and soft tissue releases are performed during Total Ankle Arthroplasty (TAA), particularly with varus malalignment. The purpose of the present study was to compare the outcomes of ankles that underwent TAA with concurrent Brostrom-Gould (BG) or Anatomic Lateral Ankle Stabilization (ATLAS) at a minimum of 1-year follow-up.
Methods: Thirty-eight TAA’s underwent BG (21 INFINITY, 4 CADENCE) or ATLAS (13 INBONE-2) between August 2015 and February 2019 at a single institution and were at least 1 year postoperative (mean 18.3 months, range 12-40). Baseline patient demographics, characteristics, and operative factors were assessed via medical record and chart reviews. Radiographs parameters were measured preoperatively, at 6 weeks postoperative, and during the latest follow-up. Revisions, reoperations, and complications were classified according to the criteria established by Vander Griend et al. and Glazebrook et el., respectively. Univariate and multivariate analyses were performed.
Results: Survivorship for TAA with concurrent BG/ATLAS was 97%. Overall, TAA with concurrent BG had higher incidences of early TAA revision (4%), recurrent instability (4%), reoperation (16%), and complications (29%) compared to ATLAS. Postoperative coronal and sagittal tibiotalar alignment changes were significant for both groups (p< 0.001, p=0.014); however, the differences were greater for ATLAS (p= 0.045, p<0.001).
Conclusion: The present study is the first to compare outcomes between techniques for addressing ankle instability in the TAA population. At short-term follow-up, anatomic reconstruction produced better outcomes than the traditional BG procedure. Additional comparative studies between techniques to address instability in the TAA population are warranted.
DOI: 10.1177/2473011421S00056
High Rate of Talar Collapse in STAR Total Ankle
Daniel J. Scott, MD, MBA; David Vier, MD; Samuel E. Ford, MD; Shannon F. Alejandro, MD; James W. Brodsky, MD
Category: Ankle; Ankle Arthritis; Hindfoot
Keywords: Ankle Arthroplasty; Total Ankle Replacement; Total Ankle Arthroplasty
Introduction/Purpose: Despite substantial advancements in Total Ankle Arthroplasty (TAA), catastrophic failure due to implant subsidence remains a common and serious problem. While there are many studies of short and some of intermediate term follow- up of TAA, the number of long-term studies, especially with prospectively collected data, is much fewer, and the data on the incidence and impact of talar subsidence on those results is even more limited. Talar subsidence can be especially challenging to manage, given the limited talar bone stock and revision options as compared to the larger tibial bone stock. The purpose of this study was to evaluate the long-term incidence and characteristics of TAA implant failure.
Methods: A prospectively collected database of TAAs performed in a tertiary referral center began enrolling in 1999. Medical records/radiographs were reviewed to evaluate outcomes of TAA and final radiographs were reviewed to identify implant failure from 1999-2016. Minimum radiographic follow-up was two years. Pre-operative and post-operative radiographs were measured for ankle, foot, and implant coronal and sagittal alignment Failure and reoperation rates of two different implants, the mobile bearing Scandinavian Total Ankle Replacement (STAR) and the fixed bearing Salto Talaris (Salto) were analyzed. Paired Student t- tests were performed between groups. TAA revision surgeries were excluded if the primary TAA was performed at another institution. Reoperations were recorded according to the Reoperations Coding System (CROCS) classification of the Canadian Orthopaedic Foot and Ankle Society (COFAS). There were 149 TAAs reviewed in 146 patients (136 STARs and 13 Saltos), with an average follow-up of 7.03 years (range 2-20 years).
Results: Implant survival was 85.8% at mean 7 years. 25 TAAs demonstrated radiographic catastrophic failures, 21 underwent re- operation, and 4 declined revision surgery (Table 1). One failure was due to infection (CROCS 10), others were aseptic (CROCS 9). 13/25 failures were related to talar subsidence, all STARs (9.6% of all STARs in the series). Nine STARs (6.4%) had less severe talar subsidence but were asymptomatic, The STAR talar component, in total, subsided in 17.6% (24/136) of STARs, requiring revision in 13 (9.6%) of cases at mean 3.8 years post-op. There was no difference in pre-operative/post-operative radiographic alignment between the TAAs that did and did not fail. Twenty-six ankles (17.4%) underwent additional surgery with retention of metal components, bringing the total reoperation rate to 47/149 (31.5%).
Conclusion: At long-term follow-up, TAA demonstrates reasonable implant survival rates, especially given the learning curve that includes STARs implanted prior to the Food and Drug approval study. We describe a unique mode of failure in STARs that highlights one of the risk factors for failure in total ankle arthroplasty. This represents the highest reported rate of talar subsidence in the literature with almost 10% of STARs demonstrating talar-sided failure at mean 7-year follow-up. Surgeons who utilize the STAR total ankle should be vigilant for talar subsidence given the high rates reported in this series.
DOI: 10.1177/2473011421S00057
Association Between Hindfoot Alignment and First Metatarsal Rotation
Jesse Steadman; Neil K. Bakshi, MD; Christopher B. Arena, MD; Matthew T. Philippi; Alexej Barg, MD; Charles L. Saltzman, MD
Introduction/Purpose: The interplay between forefoot and hindfoot alignment has been well established in the literature for pathologies such as the flexible cavovarus foot. However, no study has evaluated the relationship between hindfoot alignment and first metatarsal axial rotation. Therefore, the purpose of this study is to determine the relationship, if any, between hindfoot alignment and first metatarsal axial rotation in patients with mild, moderate, and severe hindfoot varus/valgus deformity using weight bearing computed tomography (WBCT). We hypothesize that patients with hindfoot valgus alignment will be associated with a first metatarsal pronation/eversion deformity. Conversely, we hypothesize that patients with hindfoot varus alignment will be associated with a first metatarsal supination/inverted deformity.
Methods: Patients who underwent weight bearing radiographs (WBR) and WBCT between 2015 and 2018 were evaluated with inclusion/exclusion criteria. Patients with prior foot surgery/trauma were excluded. Hindfoot alignment was evaluated using the calcaneal moment arm (Figure 1; horizontal distance between the most inferior aspect of the calcaneus and an extended line approximating the longitudinal axis of the tibia). Six subgroups were created based on the severity of hindfoot malalignment 1) Moderate valgus, 2) moderate varus, 3) substantial valgus, 4) substantial varus, 5) severe valgus, and 6) severe varus. Moderate was 1/2-1 standard deviations (SD) from the mean. Substantial was 1-2 SDs from the mean. Severe was >2 SDs from the mean. Patients with CMA values within ½ SD of the mean were excluded to focus on patients with significant hindfoot malalignment. First metatarsal axial rotation was measured using the Kim and Saltzman angles (Figure 1). Meary’s angle was obtained using WBR.
Results: 196 patients were included (average age - 52.6 years). The average CMA was +6.0+-16.2mm (valgus). The average Kim and Saltzman angles were 7.7+-12.9 and 2.8+-13.1 degrees (pronated). The average Meary’s angle was 182.0+-11.9 degrees (>180 degrees-apex dorsal measurement). There was a significant association between hindfoot alignment and the Saltzman (r=0.641, p<.001) and Kim angles (0.615, p<.001). Hindfoot valgus was associated with 1st metatarsal pronation and hindfoot varus was associated with 1st metatarsal supination. There was a significant inverse relationship between Meary’s angle and the Saltzman (r=-.600, p<.001) and Kim Angles (r=-.529, p<.001). This suggests that as Meary’s angle decreases, as seen in a pes planovalgus deformity, 1st metatarsal pronation increases.
Conclusion: There is significant correlation between hindfoot alignment and 1st metatarsal rotation. We demonstrated an association between hindfoot valgus and 1st metatarsal pronation, as well as between decreased Meary’s angle and 1st metatarsal pronation. This suggests that 1st metatarsal pronation is associated with pes planovalgus deformity. We also report an association between hindfoot varus and 1st metatarsal supination, as well as between increased Meary’s angle and 1st metatarsal supination. This suggests that 1st metatarsal supination is associated with cavovarus deformity. A derotational osteotomy/fusion may be required for first metatarsal rotational correction, in addition to hindfoot correction, for patients with cavovarus/planovalgus deformities.
DOI: 10.1177/2473011421S00058
Peripheral Nerve Block Compared to Intra-Articular Injection for Post-Operative Pain Control in Total Ankle Arthroplasty: A Randomized, Controlled, and Non-Inferiority Trial
Nicholas L. Strasser, MD; Michelle Bremer; Erin C. Owen, PhD, MPH
Category: Ankle Arthritis; Ankle; Other
Keywords: Pain; Ankle Arthritis; Total Ankle Arthroplasty
Introduction/Purpose: Ankle arthritis is associated with debilitating pain and chronic disability. Total ankle arthroplasty (TAA) is increasingly performed to treat end-stage arthritis resulting in favorable clinical outcomes. Peripheral nerve blocks (PNB) are widely used for post-operative pain management; however, PNB can lead to post-operative neuropathic complications. Intra- articular injections (IAI) have been widely reported as an alternative to PNB in total knee arthroplasty, resulting in lower post- operative narcotic consumption and accelerated functional recovery. Little information exists on patient outcomes following IAI in TAA. The purpose of this study was to assess the effectiveness and tolerability of IAI compared to PNB for pain control, measured by oral morphine milligram equivalents (MME) and a Visual Analogue Pain Scale (VAS), following TAA.
Methods: We conducted a prospective, randomized, non-inferiority study involving 51 opioid naïve adults undergoing primary, unilateral TAA. Participants were randomized to IAI joint cocktail containing anesthetic and steroid at the completion of the TAA (n=26), injected in four joint capsule locations, or PNB (n=25). PNB included a single popliteal fossa block of the sciatic nerve and adductor canal block of the distal femoral nerve. Primary outcomes were mean difference in oral post-operative MME, via inpatient record and patient daily narcotic diaries, and post-operative pain measured by the VAS (0-100mm) at 24 hours and 2 weeks post-TAA. IAI was considered non-inferior to PNB if mean difference in consumption of narcotics was less than 30 MME (24 hour) and 75 MME (2 weeks), and the mean difference in pain was less than 15mm on the VAS using the upper limit of one- sided 95% confidence intervals (UCI) for increase in MME and VAS scores.
Results: There were 39 patients with complete data. Mean oral MME in 24 hours was 50.4 (sd = 38.1) in the IAI group (n=22) versus 52.9 (sd = 48.1) in PNB (n=17) with -2.4 MME mean difference (UCI 20.8). Mean VAS at 24 hours was 25.6 (sd = 25.1) in IAI compared to 25.4 (sd = 29.2) in PNB. Mean difference in VAS at 24 hours was 0.22 (UCI 14.9). Mean two week post- VAS was 13.3 (sd = 17.2) in IAI compared to 15.1 (sd = 21.2) for PNB with mean difference of -1.8 (UCI 8.5). All demonstrate non- inferiority. At two week post- IAI reported 384.6 MME (sd = 491.0) and PNB 319.2 (sd = 323.7) with 65.5 MME difference (UCI 303.6), not supporting non-inferiority.
Conclusion: IAI is non-inferior to PNB in the first 24 hours after TAA as measured by oral narcotic consumption and patient-self reported pain. At two week post-TAA, IAI resulted in non-inferior pain scores; however, non-inferiority was not confirmed for oral narcotic consumption due to the high variability in documented use. This study suggests IAI is effective for controlling immediate post-operative pain without introducing the neuropathic complications associated with PNB.
DOI: 10.1177/2473011421S00059
The Weil Osteotomy for Angular Correction of Axial Plane Deformities of the Lesser MTP Joints: A Radiographic Analysis
Carson D. Strickland, MD; Joseph T. Cline, MD; Eric D. Villarreal, MD; G. Andrew Murphy, MD
Introduction/Purpose: The oblique shortening (Weil) osteotomy of the distal metatarsal neck has been described as an effective means of correcting lesser toe metatarsophalangeal joint deformity. Previous studies have focused on clinical outcomes, complications, and the magnitude of plantar displacement and shortening. The aim of this study was to quantify the magnitude of axial plane correction obtainable when a medial or lateral displacing Weil osteotomy was used in conjunction with other procedures in forefoot reconstruction surgery.
Methods: Consecutive patients with a minimum 12-month follow-up who were treated by the senior surgeon from January 1, 2008, to September 1, 2018, were included. Review of the medical records identified 234 toes in 190 patients that had medial or lateral displacement Weil osteotomies as a part of their treatment for metatarsalgia and lesser toe deformity. Concomitant procedures were recorded. Pre- and post-operative weightbearing radiographs were analyzed to determine the amount of transverse plane change and residual varus/valgus alignment. Radiographs were then classified as good (<10 degrees of angulation), intermediate (10-15 degrees), or bad (>15 degrees). Any worsening of the post-operative alignment compared to the pre- operative alignment was noted. Follow-up notes were reviewed for clinical observations of floating toe, resting alignment, persistent pain and swelling at 3 months, complications, and need for revision surgery.
Results: The average transverse plane correction was 12.5 degrees (range 0-45 degrees). Most toes remained in some degree of radiographic varus or valgus alignment as a true neutral toe was rare. Over a third, (35%, n=81) had increased postoperative angulation; 42% of radiographs were graded as good alignment (n=99), 20% as intermediate (n=46), and 38% as bad (n=90). The most common concomitant procedures were PIP joint resection arthroplasty and distal chevron bunionectomy. Review of clinic notes revealed low incidences of floating toe (7%, n=16), clinical malalignment (8%, n=18), and need for revision surgery (3%, n=8). Persistent swelling was the most common complication, present in 44% of patients at the 3-month follow-up.
Conclusion: The medial and lateral displacing Weil osteotomy can be a powerful tool to correct lesser toe MTP joint transverse plane deviation. It was typically used with PIP joint resection and hallux valgus procedures to improve the lesser toes and overall forefoot alignment. Interestingly, most toes had a neutral or good clinical alignment regardless of the radiographic alignment. Further studies to correlate radiographic and clinical outcome measures may help define its role in correcting lesser toe deformity.
DOI: 10.1177/2473011421S00060
Surgical Imbrication of Plantar Plate to Metatarsal Neck in the Setting of Lesser Toe Metatarsophalangeal Joint Instability
Paul G. Talusan, MD; Eric Colomb; Robert N. Kent; Vandan D. Patel; James R. Holmes, MD; David M. Walton, MD
Introduction/Purpose: Persistent metatarsalgia refractory to non-operative therapy with accompanying plantar plate injury represents a common and challenging treatment problem. In previous studies, radiofrequency shrinkage has been used for the treatment of MTP joint instability secondary to low-grade plantar plate lesions.1 In the shoulder, this technique shows histological evidence of modest regenerative capacity but is also associated with several chronic sequelae including capsular stretching, nerve damage, recurrent instability, adhesive capsulitis, and thermally-induced chondrolysis.2-6 The purpose of this observational study was to examine the efficacy of surgical imbrication of the plantar plate to the metatarsal neck as a novel, cost-effective approach to repair Grade 0-1 plantar plate injuries. We sought to characterize patient-reported and radiographic outcomes in patients undergoing this procedure.
Methods: Patients from a single fellowship-trained orthopaedic surgeon (1/2017 - 12/2020) were screened by electronic medical record review. Inclusion criteria were age >18 years, a pre-operatively measured Patient-Reported Outcomes Measurement Information System (PROMIS) score, a Grade 0 or 1 plantar plate tear discovered at time of surgery, and repair via surgical imbrication to the metatarsal neck. PROMIS Physical Function and Pain Interference scores were obtained from 14 enrolled patients (median age was 55 years; range: 40-69; 12 female) post-operatively at 6-9 weeks, 3 months, 6 months, and 1-2 years. Basic demographic information and pertinent medical information were also obtained. Three fellowship-trained orthopaedic surgeons independently reviewed radiographs to assess reduction of the metatarsophalangeal joint, and joints were graded as reduced, subluxated, or dislocated. Wilcoxon signed-rank tests compared pre- and post-operative PROMIS scores. Changes in PROMIS scores were compared to numerical and categorical patient characteristics via univariate linear regressions and Mann- Whitney U-tests, respectively.
Results: Median postoperative times to most recent PROMIS score and radiographs were respectively 13.0 months (95% confidence interval: 10.0-21.4) and 7.6 months (2.9-10.0). Median preoperative and most recent Physical Function scores were 39.5 (35-50) and 52.5 (41-62), respectively (p=0.003), and median Pain Interference scores changed from 61.0 (56-68) to 53.5 (39- 58) (p=0.002) (Fig. 1). Changes in PROMIS scores showed no association with BMI, age, preoperative opioid use, wound complications, concomitant dislocation, fibromyalgia, or mood disorder (p>0.10). Preoperatively, 9 second MTP joints were concentrically reduced, and 5 were subluxated (n=14). At 6 weeks post-operation, 13 joints remained reduced (n=14). At most recent measurement, all (n=10) joints were reduced (4 patients missing data). 9 of 14 patients underwent concomitant correction of hallux valgus at time of surgery.
Conclusion: Patients with Grade 0-1 plantar plate injuries improved significantly in radiographic parameters and patient reported outcome scores following surgical imbrication of the plantar plate to the metatarsal neck. This procedure represents a novel, alternative approach that is both efficacious and cost-effective. Our work contributes valuable surgical outcomes data to a limited knowledgebase regarding pathophysiology and management for low-grade plantar plate lesions in MTP joint instability. Future work will involve larger, prospective studies to better understand outcomes of and indications for this approach.
DOI: 10.1177/2473011421S00061
The Intercalary Fragment in Posterior Malleolus Fractures: Characterization and Significance
Benjamin D. Umbel, DO; Devon Myers, DO; Benjamin C. Taylor, MD; John A. Buchan; Anthony J. Melaragno
Introduction/Purpose: Methods of fixation in ankle fractures involving the posterior malleolus have become increasingly scrutinized. With the increase in computed tomography (CT), an intercalary fracture fragment (ICF) adjacent to the posterior malleolus has often been described. Treatment of this intercalary comminution remains controversial. The primary goal of this study was to compare clinical and radiographic outcomes in patients who had direct reduction and fixation of this fragment compared to those where the ICF was removed or not reduced prior to posterior malleolus fixation.
Methods: This retrospective study included 249 trimalleolar and posterior pilon ankle fractures grouped into those who had the ICF reduced and fixed (n=74) and those where the ICF was not directly addressed or excised (n=175). CT scans were evaluated for size and location of the ICF. Demographic, radiographic and intraoperative variables were collected and analyzed. The Kellgren and Lawrence classification system was utilized to grade severity of post-traumatic arthritis during the follow up period. Chart review was performed assessing time to weightbearing, repeat surgeries and post-operative complications.
Results: For the group which had the ICF reduced and fixed, follow up radiographs demonstrated significantly worse Kellgren- Lawrence scores compared to the group that did not specifically reduce the ICF (p< 0.05). There was also a higher rate of repeat surgery in the group which had the ICF fixed, although not meeting statistical significance. There were no differences in size or location of the ICF fragment between groups. The average overall time to weightbearing amongst all patients was 9.7 +- 3.8 weeks. There was no significant difference between time to weightbearing between groups (p = 0.6). There was no significant difference in need for secondary surgeries or post-operative deep and superfical infections.
Conclusion: With the widespread utilization of CT-scans for preoperative planning of ankle fractures involving the posterior malleolus, there has been greater discussion surrounding the optimal management of the ICF when present. In our study, the primary aim was to explore radiographic changes in patients after direct reduction and fixation of this ICF compared to those without ICF fixation. We demonstrated significantly worse radiographic outcomes following attempted direct reduction and fixation of the ICF. Our results suggest that while concentric joint reduction and syndesmosis stabilization are of utmost importance, attempting to reduce and fix the ICF may lead to worse radiographic outcomes.
DOI: 10.1177/2473011421S00062
Autologous Matrix-Induced Chondrogenesis (AMIC) with Lateral Ligament Stabilization for Osteochondral Lesions of the Talus in Patients with Ankle Instability
Arnd F. Viehöfer; Jakob Ackermann; Stephan H. Wirth, MD; Fabio A. Casari; Lizzy Weigelt; Christoph Germann
Introduction/Purpose: Autologous matrix-induced chondrogenesis (AMIC) has shown to result in favorable clinical outcome in patients with osteochondral lesions of the talus (OLT). Yet, the influence of ankle instability on cartilage repair of the ankle has still to be determined. This study sought to compare the clinical and radiographic outcome in patients with and without concomitant lateral ligament stabilization (LLS) undergoing AMIC for the treatment of OLT.
Methods: This study evaluated AMIC that were implanted in patients for the treatment of symptomatic OLT with and without concomitant ankle instability. Postoperative MRI, Tegner, AOFAS and Cumberland Ankle Instability Tool (CAIT) were obtained at a minimum follow-up of 2 years. A musculoskeletal radiologist scored all grafts according to the MOCART 1 and 2.0 scores. Patients were stratified into two groups based on whether they underwent concomitant LLS for ankle instability. Patients without LLS served as controls. Patients were matched 1:1 for BMI, lesion size, follow-up and age.
Results: Twenty-six patients that underwent AMIC with a mean follow-up of 4.2 +- 1.5 years were enrolled in this study (13 with and 13 without concomitant ankle instability). Patients’ mean age was 33.4 +- 12.7 years with a BMI averaging 26.2 +- 3.7. Patients with concomitant LLS showed worse clinical outcome measured by AOFAS (85.1 +- 14.4 vs. 96.3 +- 5.8, p=0.034) and Tegner (3.8 +- 1.1 vs. 4.4 +- 2.3, p=0.012). No difference was seen between both groups regarding MOCART 1 and 2.0 scores (p=0.714 and p=0.371, respectively). Additionally, postoperative CAIT and AOFAS significantly correlated in patients that underwent concomitant LLS (r=0.766, p=0.002) with a CAIT score of > 24 (stable ankle joint) resulting in AOFAS scores comparable to scores in patients with isolated AMIC (90.1 +- 11.6 vs. 95.3 +- 6.6; p=0.442).
Conclusion: The results of this study suggest a negative influence of ankle instability on the clinical outcome of cartilage repair with AMIC for the treatment of OLT. If postoperative ankle stability is achieved in patients with LLS, however, comparable outcome as seen after isolated AMIC can be expected.
DOI: 10.1177/2473011421S00063
Does Preoperative Valgus Deformity Severity Predict Outcomes in Total Ankle Arthroplasty vs Ankle Arthrodesis?
David Vier, MD; Rasikh N. Hamid; Susan M. Odum, PhD; Carroll P. Jones, III, MD; Bruce E. Cohen, MD; Todd A. Irwin, MD; W. Hodges Davis, MD
Introduction/Purpose: Coronal plane deformity is an important consideration in the treatment of ankle arthritis, and valgus alignment presents its own unique challenges. Ankle fusions were previously considered the gold standard, but advancements in total ankle arthroplasty (TAA) implant design and surgical technique have increased its popularity in the treatment of even large coronal plane deformities. Although many studies have compared fusion to arthroplasty, no studies have directly compared these two treatments in the treatment of valgus ankle arthritis. The purpose of this study was to evaluate and compare clinical and radiographic outcomes of TAA to ankle fusion in the treatment of valgus ankle arthritis.
Methods: 137 patients with valgus ankle arthritis who underwent either TAA or ankle fusion were identified through a prospectively collected database. Minimum clinic follow-up was two years. Preoperative radiographs were measured for tibiotalar angle to include patients with valgus ankle arthritis five degrees or greater. Axial alignment views were also analyzed for preoperative hindfoot alignment. Patients who underwent tibiotalocalcaneal fusion or had previous ankle corrective osteotomy were excluded. Complications, failures, revisions, and reoperations were recorded. Failures were defined by explant of a metal component. Reoperations included any additional related ankle/hindfoot surgery including subtalar fusion. Patients were categorized by severity of preoperative valgus deformity into 4 groups: 5-10 degrees, 11-15 degrees, 16-20 degrees, and greater than 20 degrees. Outcomes were compared across these groups between TAA and ankle fusion. There were 98 patients who underwent TAA and 39 patients who underwent ankle fusion. Median follow-up was 50.4 months (inner quartile 37.4-74.1).
Results: Patients who underwent TAA with greater than 15 degrees of preoperative valgus deformity had higher rates of failures, revisions, and reoperations compared to those who underwent fusion with the same deformity severity. Overall, 44% of patients (60/137) had major or minor complications. There were 6 failures (6%) in the TAA cohort and 5 failures (13%) in the fusion cohort. 36% of fusions (14/39) underwent reoperation which was a higher rate compared to 18% of TAAs (18/98) (p=0.03). Combined fusion and TAR cohorts had less complications, failures/revisions, and reoperation rates as the severity of deformity increased (p<0.01).
Conclusion: Severity of preoperative valgus deformity is an important consideration in the surgical treatment of ankle arthritis. Patients with greater than 15 degrees of preoperative valgus had lower rates of failures, revisions, and reoperations when treated with fusion. Patients with less than 15 degrees of preoperative valgus had lower rates of failures, revisions, and reoperations when treated with TAA. Overall, patients with greater preoperative valgus deformity had less complications. Patients with valgus ankle arthritis remain a challenging problem with high complication rates regardless of surgical procedure and additional procedures should be considered to treat any coronal plane instability and foot deformity.
DOI: 10.1177/2473011421S00064
Suture Tape Reinforcement Device as an Independent Fixation Solution for Partial Syndesmosis Injuries
Gregory R. Waryasz, MD; Takahisa Ogawa, MD, MPH; Bart Lubberts, MD, PhD; Christopher W. DiGiovanni, MD; Daniel Guss, MD, MBA
Introduction/Purpose: A suture tape reinforcement device is designed for repair of syndesmotic injury. Its insertion in the fibular and tibial footprints of the anterior inferior tibiofibular ligament (AITFL) promises a dynamic constraint to external rotation, antero-posterior translation of fibula and diastasis of the syndesmosis in the coronal plane.We hypothesized that following fixation of transected syndesmosis with suture tape reinforcement, syndesmotic stability becomes similar to that of an intact syndesmosis.
Methods: Fifteen non-paired fresh frozen cadaveric specimens amputated above the knee were included in this study. Assessment of the ankle syndesmosis was performed in six stages; 1) with all syndesmosis ligaments intact; 2) after transection of the AITFL, 3) the interosseous ligament, 4) subsequent fixation with suture tape reinforcement device, 5) transection of the posterior inferior syndesmotic ligament, and 6) after removal of the suture tape reinforcement device (complete ligament transection stage). Instability measurements included anterior and posterior tibiofibular spaces measured arthroscopically under 100N lateral stress using a bone hook, tibiofibular anteroposterior and posteroanterior translation in sagittal plane measured arthroscopically under sagittal stress of 100N, and anterior tibiofibular space measured directly with a caliper under external rotation torque of 7.5 Nm. Instability measurements taken after each fixation method were compared with the intact stage and to the complete ligament transection stage using the Wilcoxon signed-rank test.
Results: The suture tape reinforcement device was able to stabilize an AITFL- and the interosseous ligament-transected stage, similar to the intact stage, with respect to all measures of instability. As for the complete ligament transection stage, after suture tape reinforcement it remained unstable in the coronal plane, compared to the intact stage: there was an increase in anterior tibiofibular space without stress (1.7 mm vs 1.1 mm, p=0.005) and with stress (1.8 mm vs 1.1 mm, p=0.007), as well as in posterior tibiofibular space with stress (2.8 mm vs 1.6 mm, p=0.002).
Conclusion: Our findings suggest that suture tape reinforcement device might be effective for fixation of partial syndesmotic injury, but not for complete syndesmotic injury. Future clinical research is needed to confirm this.
DOI: 10.1177/2473011421S00065
Evaluation of Lisfranc Injuries: How Involved is the First Tarsometatarsal Joint?
Liam H. Wong; Bopha Chrea, MD; Lara C. Atwater, MD; James E. Meeker, MD
Introduction/Purpose: Lisfranc injuries are among the most debilitating injuries to the midfoot. Various classification systems have characterized the injury patterns with specific focus on the interval between the base of the second metatarsal and the medial cuneiform as well as the importance of the ligamentous structures of the midfoot. The medial ligamentous restraints of the first tarsometatarsal (TMT) joint and the bony involvement of these injuries remains unclear. Improved knowledge on how the first TMT joint is affected in Lisfranc injuries will provide information on how best to manage these injuries.
Methods: We conducted a single institution review of all Lisfranc fractures from 2010 through 2020. Patients were identified by CPT codes. Hardcastle and Myerson Lisfranc injury classifications and computed tomography and radiograph characterizations of the first TMT joint were identified by three foot and ankle trained orthopaedic surgeons. Light’s kappa statistics (mean weighted Cohen’s kappa) evaluated inter-rater reliability of Lisfranc classifications. The effects injury mechanism and Lisfranc classification on the first TMT joint were further assessed using t-test, Mann-Whitney U, Fisher’s exact test, and analysis of variance.
Results: Of 71 patients with a Lisfranc injury, 62 (87%) had a sign of injury to the first TMT joint, which significantly varied by Lisfranc classification (P<0.001; Table). Light’s kappa coefficient for inter-rater reliability was 0.46. A fragment of the first TMT articular surface was present in 39 patients (55%; median size=10mm) and a medial capsular avulsion fragment was seen in 28 patients (39%). A fracture was present in the medial cuneiform in 25 patients (35%) and in the first metatarsal in 18 patients (25%). Forty-nine patients (69%) had medial/lateral TMT joint incongruence (median overhang=4mm); 21 (30%) had dorsal/plantar incongruence (median overhang=6mm), which significantly differed by Lisfranc classification (P<0.02) and gender (Female=3.5mm; Male=7mm; P<0.03). Angulation of articular surfaces in the first TMT joint over 5 degrees on the transverse/antero-posterior plane occurred in 32 patients (45%) and in 12 patients (17%) on the sagittal/lateral plane, which significantly differed between Lisfranc classifications (P<0.03).
Conclusion: Lisfranc injuries have great potential for long-term disability requiring careful screening and diagnosis. The overwhelming majority of Lisfranc injuries include damage to the first tarsometatarsal joint. This is the first study to our knowledge that characterizes this in detail. This study found that the most common patterns involving the first TMT joint included joint incongruity, capsular avulsion and articular surface fracture. A better understanding of injuries to the first TMT can help orthopaedic surgeons with diagnosis and management.
DOI: 10.1177/2473011421S00066
Adolescents with Lisfranc Injury Frequently Have Different Pathology with Higher Incidence of Proximal Extension of the Ligamentous Disruption
Amr Abdelgawad; Ahmed Thabet, MD
Category: Midfoot/Forefoot; Trauma
Keywords: Lisfranc Injuries; 1st MTP Joint; TMT
Introduction/Purpose: Lisfranc injuries are rare injuries in the adolescent age group and can be easily missed. Ligamentous Lisfranc injuries have been classically descried as disruption of the Lisfranc ligament (between medial cuneiform and second metatarsus) and ligamentous disruption of the first metatarso-phalangeal joint. The study aimed to report pathological pattern of Lisfranc injury in adolescent patient and if it was different from the common adult forms.
Methods: This is a retrospective study of patients with Lisfranc injury treated at a Level 1 trauma center between 2012 and 2019. This study has been IRB approved. The inclusion criteria were of adolescents with isolated Lisfranc injuries and treated via surgical intervention. The surgical intervention helped to identify the exact pathology. The study excluded patients over the age of 18, patient with high energy injuries and patients treated non-operatively. Patients’ demographics including age and gender, were recorded. Other variables included the mechanism of injury, side of injury, fracture type, the intraoperative findings of the ligamentous injury and follow-up data. Follow up radiographs were reviewed for time to bony union and any post-traumatic complications. Outcomes include wound healing status, the union status of the fracture, and complications that may arise along with treatment and follow-up.
Results: A total of 9 patients met the study inclusion criteria. Mean age was 15.4 years old, male to female ratio of 5:4, mean follow-up time was 9.5 months. All patients achieved full union at the final follow-up. The postoperative course went without complications except one for patient. The patient had prominent screw under the skin. The screw removed in the office under local anesthesia. Intraoperative findings in 6/9 (66.6 %) cases demonstrated a Lisfranc injury pattern with proximal extension through the inter-cuneiform ligament. Operative treatment in cases of proximal extension included added fixation between the middle cuneiform and middle cuneiform (screws or plates). Also noted in 2 cases, that the 1st tarso-metatrsal joint was not affected (in contrast to classic Lisfranc injury in adults). In these cases, no fixation was need for the 1st TMT joint.
Conclusion: Lisfranc injury in adolescent has frequently different pathology compared to adults’ counterparts. It commonly involves proximal extension with the ligament disruption. It also sometimes spares the ligaments of the 1st TMT joint. Orthopedic surgeons should be aware of these changes as it implies changes in the treatment strategy and fixation construct.
DOI: 10.1177/2473011421S00067
10 Year Outcomes of Unilateral vs Bilateral (Staged) Total Ankle Replacement
Nicole G. Abdul, MBChB, BMedSci, MClin Res, MRCS; Jayasree Ramas Ramaskandhan, MPT, MSc; Karen Smith, MSc, BSc;
Mohammad A. Alkhreisat, MD, FRCS T&O; Adam P. Bennett, MRCS; Malik S. Siddique, FRCS (T&O)
Introduction/Purpose: Comprehensive long-term outcomes of total ankle replacement (TAR) help guide clinicians when they are deciding on the management of patients with more than single joint arthritis. Some patients will only require unilateral TARs, while others will need bilateral TARs. When deciding on treatment plans for patients, it is important to know the long-term surgical outcomes of both of these groups before treatment can be recommended. Currently there is a paucity of literature on long-term outcomes of unilateral versus bilateral TARs. The aim of the study is to assess long-term outcomes in patients who underwent unilateral vs. staged bilateral TARs.
Methods: We performed a retrospective review of a prospectively completed hospital registry database for TAR. This consisted of a consecutive series of TARs performed by one senior surgeon from 2006 to December 2010 with 10-years of follow up. Clinical complications, radiological complications (lucency, cysts, and osteolysis), and patient reported outcome measures (WOMAC score, SF-36, general health survey, and patient satisfaction survey) were included for all patients. Outcomes were evaluated pre-operatively and at 1, 3, 5, and 10 years post-operatively. Three component mobile bearing implants were used in all patients.
Results: There were 132 unilateral TARs (Group A) vs. 24 staged bilateral TARs (Group B). WOMAC scores significantly improved from pre-op to 1 year for pain (45.3 to 77.8; 52 to 76) function (49.1 to 77.8; 53.6 to 76) and stiffness (39.8 to 67.9; 55 to 65) in both groups respectively (p<0.05). At 5 years, Group B reported higher function scores than Group A (79.1 vs. 65.7; p=0.05). At 10 years Group B reported significantly better stiffness scores than Group A (78.5 vs. 59.5; p=0.034). There was no significant difference in SF-36 scores between groups at 5 and 10 years. Group A was 40% dissatisfied with return to recreational activities compared to 30% in Group B (p>0.05). Group A reported 16% dissatisfaction with surgery compared to 10% in Group B (p>0.05). At 5 years there were a higher number of radiological and clinical complications in Group A compared to Group B.
Conclusion: For patient reported outcomes, staged bilateral TAR patients had more improvement in function at 5 years, and stiffness at 10 years, when compared to unilateral TAR patients. Unilateral TAR patients had higher rates of complications compared to staged bilateral TAR patients at 5 years.A limitation of this study was the smaller size of Group B patients compared to Group A. We will be able to present a detailed breakdown of outcomes at each time point if the abstract is selected for presentation.
DOI: 10.1177/2473011421S00068
A Bioengineered Organized Collagen-Based Microfibrous Implant Designed for Tendon Regeneration
Samuel B. Adams, Jr., MD; Michael P. Francis; Yas Maghdouri-White; Nardos Sori; Nathan Kemper
Introduction/Purpose: Tendon healing is a slow and complicated process that results in inferior structural and functional properties compared to healthy tissue. It may be possible to improve outcomes of tendon healing with enhancement of biological repair through the development of tissue engineered medical products (TEMPs). Although many tendons heal with satisfactory outcomes, others do not, leading to pain and additional cost. Current augments for repair lack either native tissue structure or composition, limiting their potential effectiveness. For example, in tendon healing, restoring native organized and dense collagen composition is a primary goal; however, most TEMPs, such as lyophilized collagen or electrospun pure collagen fibers, are mechanically weak and unstable. For optimizing stability and biocompatibility, collagen can be combined with a high-performance co-biopolymer, such as poly(D,L-lactide) (PDLLA).
Methods: The purpose of this study was to demonstrate the efficacy of a novel biointegrative construct, composed of type I collagen and PDLLA for Achilles tendon repair. PDLLA is biocompatible, has shown to support cell growth, and degrades to CO2 and H2O in vivo. The electrospun copolymer constructs were post-processed with low-temperature annealing to enhance their porosity and mechanical stability. The constructs were first tested for their ability to absorb blood and platelet-rich-plasma (PRP). Additionally, the constructs were tested in vivo by implantation in a rabbit Achilles tendon injury model by creating a 7 mm midsubstance Achilles defect. For each tendon defect, a copolymer construct was circumferentially wrapped around the defect and sutured into place. Finally, human cadaver testing was performed to assess implant handling and fixation characteristics.
Results: Collagen-PDLLA constructs absorbed more than ten times their weight in blood and PRP. Histologically, rabbit tendons showed rapid implant cellularization by 2-8 weeks, along with de novo collagen deposition. By 16 weeks, dense collagenous connective tissue was seen integrating at the tendon-implant interface and throughout the implant. Movin-Bonar scores for the collagen-PDLLA-implanted and sham-operated tendons were identical from 16-72 weeks post-operatively, indicating a return to normal tendon morphology. Overall, surgical application of the collagen-PDLLA constructs demonstrated dense collagenous fibrous connective tissue ingrowth into and around the implant. Moreover, cadaver surgical implantation of the implant in a minimally invasive Achilles tendon repair and arthroscopic rotator cuff repair, allowed easy graft orientation and delivery as well as excellent handleability and suture fixation to the native tendon.
Conclusion: Electrospun biointegrative implants were tissue-engineered to enhance cell infiltration for promoting tissue integration and functional remodeling. When implanted in the rabbit Achilles tendon, the implants demonstrated new in situ tissue generation and remodeled into dense, regularly oriented connective tissue at the tendon-implant interface. Collagenous ingrowth may be crucial in tendon protection and significantly progresses towards improving clinical outcomes following tendon injury. Moreover, the implants demonstrated additional clinical utility by absorbing greater than ten times their weight in biologic fluids which demonstrates the potential to combine this novel biointegrative implant with additional fluid based biologic therapies.
DOI: 10.1177/2473011421S00069
Increasing Age and Modifiable Comorbidities are Associated with Short Term Complications after ORIF of Ankle Fractures
Samuel B. Adams, Jr., MD; Richard Danilkowicz; Nathan L. Grimm; Jaewhan Kim; Jeffrey O’Donnell; Nicholas B. Allen
Category: Trauma; Ankle
Keywords: Ankle Fracture; Ankle; Ankle Pain
Introduction/Purpose: Ankle fractures are common orthopedic injuries with complication rates fixation of up to 40%. Limited evidence exists in the literature regarding complications in the elderly population, and moreover, these studies frequently define elderly arbitrarily at 60-65 years old. The purpose of the present study was to utilize a large, validated database to evaluate whether there is an inflection point of age when postoperative complications after an ankle fracture significantly increase.
Methods: A retrospective review of all patients in the American College of Surgeons National Surgical Quality Improvement Program database who underwent fixation of an ankle fracture between 2012-2018 was performed. Patients were identified within the database using the Current Procedural Terminology codes. Appropriate statistical analysis was performed with p-value less than 0.05 considered statistically significant.
Results: A total of 27,633 fractures were including and comprised of 221 posterior malleolar, 1,567 medial malleolar, 8,495 lateral malleolar, 10,175 bimalleolar, and 7,175 trimalleolar. A total of 1,545 complications were encountered (5.6%). There was a statistically significant association between increasing age and complications (OR=1.03; p<0.001). Further analysis shows the largest spike in complications within the age 78+ bracket. There were no overall interaction effects between age and fracture subtype (p=0.223).
Conclusion: ORIF of ankle fractures is a common orthopedic procedure performed on patients of all ages, with complications ranging in severity. In order to best counsel patients on their individual post-operative risks, large data sets are often necessary to prognosticate. This study found that postoperative complications increase with advanced age. The incidence of complications did not spike for patients around the age of 65, but rather followed an incremental linear pattern with the largest increase in odds ratio occurring at age 78 and above. Complication rate was not associated with specific fracture type based off of ICD codes.
DOI: 10.1177/2473011421S00070
Racial Disparities in Total Ankle Arthroplasty: An Analysis of a Large National Dataset
Samuel B. Adams, Jr., MD; Jason Long; Richard Danilkowicz; Nathan L. Grimm; Jeffrey O’Donnell; Jaewhan Kim
Introduction/Purpose: A significant body of literature exists that documents the racial/ethnic disparities in orthopedics. Previous studies have looked at racial disparities in total ankle arthroplasty and have shown concerning TAA utilization rates. One such study detailed a two fold difference in rate per 100,000 of 0.14 in Whites vs. 0.07 in Blacks in 1998, which continued to worsen and by 2011 the utilization rate was 1.17 in Whites vs. 0.33 in Blacks, a 4-fold difference. The purpose of this study was to update the literature and analyze the utilization rates of TAA by race as well as to detect any differences in outcomes between the groups through the most updated data available in the National Surgical Quality Improvement Program (NSQIP) database.
Methods: A retrospective cohort study was performed utilizing the National Surgical Quality Improvement Program (NSQIP) database. Patients were identified for inclusion using the Current Procedural Terminology (CPT) codes 27700 and 27702, corresponding to arthroplasty ankle and arthroplasty ankle with implant, respectively. All patient’s with known race were included, non-Hispanic White, non-Hispanic Black, Asian, Native American, and Hispanic. A total of 1164 patients met inclusion criteria for this study.
Results: A total of 1164 patients with known race undergoing TAA from 2012-2018 were included in this analysis. Of these patients 1051 (90.3%) were non-Hispanic white (White), and 113 (9.7%) were non-Hispanic Black, Asian, Native American, and Hispanic (Non-White). The mean patient age for White patients was 63.7 years, compared to 55.3 years for Non-White patients which was statistically significant. (p-value <0.01). There was a similar distribution of males and females in each group, and smoking status and presence of diabetes mellitus was similar in both groups. In the listed postoperative complications, non-white patients were at no increased risk of developing superficial wound infection, deep wound infection, PE, DVT, requiring a blood transfusion, requiring another operation, or requiring readmission to the hospital within 30 days.
Conclusion: Based on this large national data set, between the years 2012 and 2018 there was nearly 10-fold more non-Hispanic white patient’s undergoing TAA when compared to other racial/ethnic groups. This unfortunately highlights the continued, if not worsening racial disparities present in TAA. Additionally, no differences were found in post-operative outcomes based on racial or ethnic group. This indicates that different racial or ethnic groups are doing no worse post-operatively from TAA when compared to Whites.
DOI: 10.1177/2473011421S00071
Pain Mapping as a Predictive Model for Diagnosis and Treatment in Foot and Ankle Conditions
Vidhi Adukia; Martin Hughes; Alistair J. Best; Patricia Allen, MB ChB; Jitendra Mangwani, MBBS,MS(Orth),FRCS(Tr&Orth)
Introduction/Purpose: With the COVID19 pandemic, virtual consultations are becoming a necessity. Clinicians are having to adapt consultations to determine where patients’ symptoms are, and what the appropriate next line of investigation or treatment should be, without the benefit of traditional face-to-face contact. The aim of this project was therefore to use pain mapping in foot and ankle conditions, in order to see if there was a predictive correlation between certain symptomatic areas and the ultimate surgical treatment required by patients.
Methods: Data was collected prospectively from patients attending foot and ankle clinics from 2014 to 2019, and this was cross- matched with operative data subsequently. Data included patient demographics, co-morbidities, smoking status and previous injuries or surgeries. In a structured questionnaire, patients also marked the regions of the foot and ankle that they thought were the most symptomatic. The foot and ankle was divided into 12 segments for the purpose of analysis.
Results: A total of 2007 patients completed these questionnaires, from which operative data was available for 407 patients. In the first instance, data was analysed for 122 patients who underwent one of five specific procedures. Pain mapping was found to have a good predictive value for first MTP fusion and bunion surgery (n=20, 46), 1st metatarsal cheilectomy (n=10) and arthroscopic ankle arthrodesis (n=23). The least predictive pain mapping was seen for patients who had a triple arthrodesis (n=23), with those patients presenting with pain more globally in the foot and ankle.
Conclusion: The results suggest that pain mapping can be used effectively as postal questionnaires, prior to a virtual consultation, as an aid to predict diagnosis and the ultimate treatment required in some specific foot and ankle conditions.
DOI: 10.1177/2473011421S00072
The Generation Game: Has Modern Contemporary Total Ankle Replacement (TAR) Improved Survivorship?
Raju S. Ahluwalia, MBBS, MFSEM(UK), BSc, FRCS(Tr&Orth); Jean Pierre; En Lin Goh; Daniel Hay; Isobel Pilkington; Nadja Bednarczuk
Category: Ankle
Keywords: Ankle
Introduction/Purpose: Total ankle replacements (TARs) provide pain relief with preservation of movement and function. The most successful TARs are either 2nd or current 3rd generation in design, whilst 4th generation implants are steadily being introduced. This meta-analysis evaluates the survivorship of 2nd, 3rd and 4th generation ankle replacements used today to determine whether any difference between generations and bearing types exist.
Methods: A systematic review and meta-analysis of published data from January 2000 to January 2020 was conducted following PRISMA guidelines. Inclusion criteria: English language papers, adult population, >= 20 ankles with a minimum follow up >= 24 months, pre- and post-operative functional scores available. Clinical outcomes of primary TARs were evaluated as well as their associated survivorship. Statistical analyses were undertaken to determine survivorship and complications associated with the second, third and fourth generation implants and the bearing design. Ankle generations were determined from the original studies and confirmed based on literature set definitions. The modified Coleman Methodology Score was used to evaluate the quality of studies.
Results: A total of 4642 TARs in 4487patients from 51-studies were included. The mean age was 61.9years and mean follow up of 57.8months. The most common indications were post-traumatic-OA (54.5%), primary-OA (25.5%) and inflammatory-arthropathy (15.2%). Relative-risk calculations showed significant reductions in nerve-injury (p < 0.01), post-operative fracture ( p < 0.01), wound complications (p < 0.01), radiolucencies ( p < 0.01), or heterotopic bone formation (p < 0.01), aseptic loosening (p < 0.01) for later generations. Sensitivity analysis performed for the withdrawal of 2 prostheses showed 2yr survivorship for 2nd, 3rd and 4th generation TARs was 95.3%, 97.9% and 98.9% (p < 0.05). Third-generation TARs had better 10-yr survivorship compared to 2nd generation (83.50% vs. 70.76%) (p < 0.01). Bearing design had little influence on survivorship.
Conclusion: In the real world subsequent generations of modern contemporary TAR demonstrate lower rates of complications and improved survivorship independent of bearing design, without reaching designer series levels. Population changes have meant a reduction in mean age at implementation and the commonest pathology for a TAR has become post traumatic OA without a observed detrimental affect in outcomes. Even so, superior short-term survivorship of fourth generation implants is promising for the future of modern TAR surgery.
DOI: 10.1177/2473011421S00073
Performance Outcomes after Surgical Repair of Achilles Tendon Rupture in the Women’s National Basketball Association
Amiethab A. Aiyer, MD; Blake H. Hodgens; Joseph S. Geller; Michael G. Rizzo; Julianne Munoz; Jonathan R. Kaplan, MD
Category: Sports; Ankle
Keywords: Achilles Tendon Rupture; Basketball; Return to Play
Introduction/Purpose: Achilles tendon ruptures are devastating injuries in elite athletes. Current literature shows poor prognosis following Achilles tendon rupture in professional male basketball players, however there are currently no studies examining the effects of Achilles tendon rupture on performance outcomes in the Women’s National Basketball Association (WNBA). Understanding the impact Achilles tendon rupture has on return to play and performance metrics in the WNBA will provide valuable information to players, team personnel, and medical professionals on post-injury expectations.
Methods: 17 WNBA players who sustained an Achilles tendon rupture from 2000-2019 were identified from publicly available injury reports and player profiles. Demographic information collected included age, body mass index (BMI), position, and service in the WNBA when the tear occurred. Statistics were collected for the season before the injury, and two seasons after the injury, and the Player Efficiency Rating (PER) was calculated. PER is defined as ([points + rebounds + assists + steals + blocks] - [(field goals attempted - field goals made) + (free throws attempted - free throws made) + turnovers]) / games. Controls were matched by service in the WNBA, position, and PER.
Results: Following Achilles tendon rupture, four players never returned to play in the WNBA, while seven players failed to play >1 season. Players who returned saw a significant decrease in the number of minutes played per game in both their first and second seasons post-injury (mean differences -6.11 and -6.54, respectively, p<0.01). Players also suffered a significant decrease in PER during their second season after injury compared with their pre-injury PER (mean difference -2.53, p=0.024). Compared to healthy controls, players who returned to play were significantly more likely to experience a decrease in minutes played per game at both one and two seasons postoperatively (-6.11 mpg vs +1.05 mpg, p<0.01 and -6.54 mpg vs +0.53 mpg, p= 0.018, respectively), while also experiencing significant per-game decreases in field goals (-0.85 vs + 0.20, p=0.47), free throws (-1.04 vs +0.12, p<0.01), steals (-0.48 vs +0.24, p=0.018), and points scored (-2.89 vs +0.58, p=0.014).
Conclusion: Achilles tendon rupture and subsequent surgical repair in the Women’s National Basketball Association (WNBA) accounted for significantly decreased minutes played and performance outcomes in athletes at one and two years post-operatively compared to both their pre-injury year and healthy matched controls. 23.5% of players failed to return to the WNBA, while 41.2% failed to play >1 season after returning from injury.
DOI: 10.1177/2473011421S00074
Cost Analysis and Utilization of Weight Bearing CT
Nathaniel B. Alexander; Clayton C. Bettin, MD; Shumaila Sarfani, MD; Carson D. Strickland, MD; David R. Richardson, MD; G. Andrew Murphy, MD; Benjamin J. Grear, MD
Introduction/Purpose: Weightbearing Computed Tomography (WB CT) is becoming a valuable tool in the evaluation and understanding of foot and ankle pathology. With this, more practices may be interested in acquiring WB CT scanners and understanding cost effectiveness of acquisition. To date there are currently no US based reports of cost analysis of WB CT scanners. Our study is a cost analysis of WB CT at tertiary referral physician owned practice.
Methods: Data was collected for all patients who underwent imaging utilizing a weight bearing CT scanner at our institution from the date of acquisition in 2016. For ease of analysis and applicability of information across orthopedic practices, Medicare reimbursement was used as a uniform estimation of reimbursement across all insurances at a rate of $163.50 per scan. We then compared the number of scans obtained per month to total costs related to acquiring and maintaining the WB CT machine. Secondary variables collected included patient demographic information, pathology location (forefoot, midfoot, hindfoot), and utilization of the device by subspecialty.
Results: A WB CT scanner was acquired by a private group in 2016. A proforma analysis demonstrated $179,000 to acquire the machine, $30,000 for extended warranty, $995 for additional licenses. Between August 2016 and February 2021, 1702 unilateral studies and 100 bilateral studies were performed. Patients ranged in age from 6 to 92. Average age was 45 years with 45.9% male and 54.1% female. Forty-one staff utilized the CT scanner from various subspecialties with 5 Foot and Ankle (F&A) surgeons ordering 80% of scans. When dividing total costs by number of months since acquisition the monthly cost of the device is $3,318 which requires 20 scans per month when using Medicare reimbursement rates. Over a 55 month the average number of scans per month is 34. When dividing the cost of acquisition by reimbursement per scan, the breakeven point was 1,284 scans which occurred at approximately 3 years.
Conclusion: As WB CT scans become a valuable tool for the analysis of foot and ankle pathology, groups may be interested in understanding the financial implications of such an investment. Our study is the only cost analysis based in the United States of WB CT. We found that WB CT is a cost-effective tool that can be used to evaluate a number or pathologies in the foot and ankle.
DOI: 10.1177/2473011421S00075
Ten-Year Outcomes of MobilityTM Total Ankle Replacement Confirms Radiological Loosening is Not Conclusive or Reliable for Long Term Survival Analysis
Mohammad A. Alkhreisat, MD, FRCS T&O; Jayasree Ramas Ramaskandhan, MPT, MSc; Adam P. Bennett, MRCS; Karen Smith, MSc, BSc; Malik S. Siddique, FRCS (T&O)
Introduction/Purpose: Different designs of Ankle replacement are being performed nowadays, long-term outcome data is the better way to understand these implants behaviour and survival. We compared the differences in demographic data, clinical, Radiological, and patient-reported outcomes among patients who underwent total ankle replacement performed with use of the uncemented stemmed mobile bearing (MOBILITY) Total Ankle System with 10 year follow up.
Methods: We analysed 156 (15 bilateral ankles (3 non-mobility) Mobility TAR (of which 41, 45, 22 for OA, PTOA, Inflammatory arthritis respectively). Mean age 61.7 (SD 11.4) (Range 33-90). 70 Ankles had 10 years of follow up, 115 had 5 years follow up,. 96 were males, with 30 patients deceased before 10 years follow up covering 33 ankles. All from our local registry looking at the patient’s demographic data, and patient-reported outcomes as measured with use of WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index), the Foot and Ankle Outcome Score (FAOS), the 36-item Short-Form (SF-36) Health Survey, clinical and radiological outcomes and patient-satisfaction scores, collected preoperatively and at 1,3,5 and 10 years postoperatively.
Results: Of the 156 ankle1060251 had wound complications after surgery two only needed surgical debridement. 5 CRPS,16 stress fractures 2 only requiring surgical fixation,11 had subsequent STJ fusion.77 had no signs of radiolucency. The rest had some degree of radiolucency on x-ray (55% on the tibia side) only 11 where symptomatic to require further surgery (6 revised to another TAR, 2 fused, and3 required bone grafting). 11 needed osteotomies after surgery. Aseptic loosening and infection are the least common complications requiring revision. There was significant improvement in WOMAC for pain (35.9 to 67.9), function (40.6 to 66.9) and stiffness (39.4 to 62.5) from pre-op to 1 year (p<0.05), this was maintained for 10 years. Although improvement noted in the composite physical component of SF=36 (28.3 to 34.5) there was no significant increase for composite mental component score. 77.5% reported satisfaction from pain relief,72.4% with return to ADL, 40% were dissatisfied with return to recreational activities and15.5% reported dissatisfaction with overall results of surgery. Mobility TAR shown about 86% survival in our 10 years cohort.
Conclusion: With improved PROMS at 1,3,5,10 years showing Patient satisfaction score at 10 years indicates that uncemented mobile bearing implants have good long-term results, osteolysis and aseptic loosening as the least common cause of revision. It is pertinent that reporting of radiological loosening in an uncemented ankle is not conclusive or reliable for long term survival analysis.
DOI: 10.1177/2473011421S00076
Clinical and Radiological Results after Use of A Human Bone Graft (Shark Screw®) in TMT II/+II Arthrodesis
Introduction/Purpose: The tarsometatarsal joints, also called Lisfranc-joints, are the joints between the midfoot bones and the tarsal bones. The continuous arthrotic destruction of the tarsometatarsal joints leads to pain and foot deformities. The therapy of choice after failure of conservative therapy is arthrodesis. For this operation there is the possibility of using a transplant screw made of allogenic human bone material (Shark Screw), instead of conventional metal implants. This study investigates the clinical significance and radiological integration of the allogenic bone screw for arthrodesis of the tarsometatarsal joints II/+III.
Methods: This is a retrospective study involving 20 feet of 17 patients who received TMT II/+III arthrodesis with an allogenic bone screw (Shark Screw) at Speising Orthopedic Hospital in Vienna, Austria. VAS, FFI, FAOS, and AOFAS were used as measures to compare preoperative and postoperative results. Radiologic integration in the recipient bone was also evaluated.
Results: Comparing preoperative with the postoperative score of 20 feet from 17 patients, a significant reduction of the VAS (pain) from 7,6 points to 1,4 points (p=<0,001)), as well as a decrease of the VAS (function) from 7,25 points to 1,8 points has been observed. Further, a significant reduction of the FFI from 62,3% to 16,7% (p=<0,001), and a significant increase from 29,7 points to 79,9 points of the AOFAS (p=<0,001) was detected. Analyzing the FAOS score, there was a significant (p=<0,001) increase of all subscales (Symptoms, Pain, Function and Quality of life). Moreover, in all cases a good radiological integration into the recieverbone was noticed. As a result the screw was, after a follow-up time from 12 months, no longer distinguishable from the original bone.
Conclusion: These results demonstrated that the human bone screw used for TMT II/+III arthrodesis has a good outcome and reliable clinical significance. This study may be used for further investigations that should be performed to ensure this result.
DOI: 10.1177/2473011421S00077
The Incidence of Surgical Cancellations: Lessons Learned from the Resumption of Elective Orthopaedic Operating after the First Wave of COVID-19
Emlyn Amutharasan; Karan Malhotra, MRCS; Amit Zaveri, MBBS; Matthew J. Welck, MD, FRCS(Orth)
Category: Ankle; Other
Keywords: Economic Analysis; Cost Effectiveness; Elective Surgery
Introduction/Purpose: In the aftermath of the first wave of COVID-19, there was a significant backlog of elective orthopaedic cases. To address this problem, efficient running of theatres with optimal theatre utilisation was paramount. However, as new processes were introduced to reduce transmission risk, ‘last-minute’ cancellations of patients were inevitable. We report our experience of resuming elective work, with particular focus on surgical cancellations, and lessons learned.
Methods: This was a retrospective, single centre audit at a specialist elective orthopaedic hospital. We identified and examined all cancellations in foot and ankle cases between June and October 2020. Data was analysed and cancellations were categorised into groups by reason of cancellation.
Results: There were 36 cancellations out of 193 patients listed (19%). Twenty-one cancellations (57%) were directly related to COVID-19 and its processes. These comprised six patients (17%) with COVID-19 swab related issues including: booking errors, transport problems, non-attendance, and invalid swabs. Three patients (8%) contracted COVID-19 preoperatively. Nine patients (25%) cancelled their procedure at short notice amidst fears of contracting COVID-19 perioperatively. Three (8%) cancellations were due to the patient being unfit on the day of surgery - these issues were not routinely identified at pre-assessment appointments as face-to-face pre-assessment clinics had been suspended. A further 15 cancellations (42%) were due to non- COVID-19 reasons including lack of beds, unwell patients, and patients cancelling for other personal reasons.
Conclusion: Mitigation of cancellations is a key factor in maintaining theatre utilisation. Based on our experience we recommend thorough counselling of patients regarding the importance of self-isolation prior to surgery and of the pre-operative swab. Having a designated team to manage COVID-19 swabs is also critical. Reinstatement of face-to-face pre-operative assessments may help identify evolving issues and prevent last-minute cancellations. These lessons are pertinent to trusts, particularly as we emerge from subsequent waves of COVID-19.
DOI: 10.1177/2473011421S00078
Popliteal Nerve Catheters for Perioperative Pain Control in Charcot-Marie-Tooth Patients
Tonya W. An, MD; Elliot S. Schwartz; Michael S. Kissen; Gabriel A. Pollock; Glenn B. Pfeffer, MD
Category: Hindfoot; Other
Keywords: Cavovarus Foot Deformity; Charcot Marie Tooth; Pain
Introduction/Purpose: The underlying neuropathy of Charcot-Marie-Tooth (CMT) disease often makes postoperative pain control difficult. Previous institutional regimens for outpatient foot and ankle surgery in this population included preoperative single-shot regional nerve blocks and oral narcotic analgesics, but still resulted in unplanned visits for uncontrolled pain, especially after block effects abated. Longer duration of regional anesthesia effects were desired to manage pain and reduce opioid intake. We aimed to investigate the safety and efficacy of ultrasound-guided placement of popliteal nerve catheters in CMT patients undergoing foot deformity correction surgery.
Methods: Twelve CMT patients, average 28 (range 13-53) years old, undergoing reconstructive surgery by a single foot and ankle attending surgeon were consented for preoperative ultrasound-guided popliteal catheters and single-shot adductor canal blocks. Patients were separately consented for enrollment in this study and follow-up questionnaires as per Institutional Review Board protocol. Seven patients underwent joint sparing reconstruction and 5 patients had subtalar fusion. Patients were discharged on postoperative day (POD) 0. Popliteal catheters were maintained, providing continuous infusion and patient-controlled bolus doses until POD3, and then self-discontinued. Oral oxycodone 5 mg (#60-80 pills) was prescribed as needed for breakthrough pain. Daily visual analog scale (VAS) pain scores were collected by phone. Patient satisfaction (0-10) was surveyed on POD5. A pill count for opioid consumption occurred at the surgeon’s office on POD14. Five-point sensory testing using a 10g Semmes- Weinstein monofilament was performed preoperatively and on POD14.
Results: All patients tolerated the catheters well. There were no complications related to infection or catheter malfunction requiring replacement. Four of the twelve patients had pre-existing sensory deficits involving at least two areas on the five-point monofilament test (Table 1). Postoperative testing showed these deficits were unchanged and there were no instances of new sensory deficits. Postoperative VAS pain scores were typically low with the median value (interquartile range IQR) 3.7 (1.5 - 5.75) on POD1, 3.2 (1.75 - 4.25) on POD2, and 2.5 (1 - 3.5) on POD3 (Figure 1). At POD14, VAS pain was 1 (0.75-1). Patients consumed an average total of 25 oxycodone pills (IQR 9-42) over 2 weeks, less than half the prescribed number. Patient satisfaction was high with the mean (standard deviation) score of 9.1 (1.6). All patients reported they would choose to have a nerve catheter again for a similar surgery.
Conclusion: Regional anesthesia using ultrasound-guided popliteal catheters was effective for pain control in this series of CMT patients undergoing deformity correction. Opioid consumption was reduced from historical levels and no patients required emergency treatment for uncontrolled pain. These catheters provided three days of local anesthetic infusion. No new sensory deficits were detected and patients with underlying preoperative sensory deficits remained unchanged. Patients were highly satisfied. This small study group provides preliminary evidence supporting nerve catheter usage in CMT patients. Utilizing ultrasound guidance to minimize nerve injury, nerve catheters may allow safe and successful outpatient correction of CMT foot deformity.
DOI: 10.1177/2473011421S00079
Preliminary Results of an Institutional Charcot Database: Risk Factors of Conversion to Operative Treatment in Charcot Arthropathy Patients
Victor Anciano, MD; Samuel E. Ford, MD; Todd A. Irwin, MD
Category: Diabetes; Midfoot/Forefoot; Other
Keywords: Charcot Arthropathy; Charcot; Diabetes
Introduction/Purpose: Operative correction of Charcot is generally accepted for nonplantigrade deformity that cannot be accommodated with commercially available therapeutic footwear, painful ‘nonunion’ type pain, in addition to the accepted indications of osteomyelitis, persistent wounds, and non-braceability. Classification schemes associated with Charcot foot are primarily descriptive in nature. Scant literature has attempted to correlate characteristics of the deformity with a specific operative strategy to enable correction of the acquired deformity. Hence, the purpose of this study is to create a database that will shed light on much needed guidelines in the management of Charcot arthropathy. Among those guidelines, identifying risk factors for conversion to operative treatment of non-operative Charcot feet is essential.
Methods: A query of our institution administrative database was performed based on the Charcot ICD-10 codes for reconstruction procedures between 2015 - 2018. Clinic and hospital medical records were reviewed to determine if Charcot neuropathy was diagnosed and identify treatment plan. Minimal follow up was established at 2 years. Patient must have completed all surveys in the outcomes portion during their follow up period. If bilateral patients are identified, all records will be retained, and patients will be addressed as separate sides. The primary outcome was conversion to surgery. Independent risk factors analyzed were demographics, history of diabetes, peripheral vascular disease, use of anticoagulants, tobacco use, shoe wear, bracing, plantigrade foot, neuropathy, presence of ulcer, infection, and Brodsky classification. The data was both stored and analyzed in the REDCap electronic data capture tools hosted at our institution.
Results: A total of one hundred and eighty (180) records were initially queried for. Thirty-four (34) patients met the inclusion criteria. Of the 34 patients, fourteen (41%) patients had conversion to surgery. Average age of patients who converted to surgery was 53.1 compared to patients who remained in the non-operative treatment arm (age = 66.1) (p=0.05) (Table 1). Diabetes, peripheral vascular disease, anticoagulant, and tobacco use were not found to be significant risk factors. 11 (78.6%) patients who underwent surgery had diabetes compared to 8 (40%) patients in the nonoperative arm (p=0.160). 12 (85.7%) patients in the conversion arm were diagnosed with peripheral vascular disease (p=0.184). Type of shoe wear, bracing, plantigrade foot, neuropathy, presence of ulcer, and Brodsky classification were not found to be significant risk factor.
Conclusion: Identification of risk factors that lead to conversion to surgical treatment of Charcot is important. There are no well-established guidelines with regards to management or indications for surgery. This database aims to provide valuable insight into guidelines and recommendations for Charcot treatment. Preliminary results did not find independent risk factors for conversion to surgical treatment other than age. Presumably, younger patients with higher functional demands, or patients with high disease burden at younger ages are at higher risk of requiring surgical intervention. As our database expands, we will better identify risk factors and include treatment outcomes Charcot patients.
DOI: 10.1177/2473011421S00080
Clinical and PROMIS Outcomes of Maisonneuve Fractures
Nicholas A. Andrews; Abhinav Agarwal, MBBS; Megan Coffin; Kenneth J. Fellows; James Pate, BS; Vyshnavi Rallapalle; Whitt Harrelson; Ashish Shah, MD
Introduction/Purpose: Torsional injury to the foot and ankle may result in high fibular fracture with disruption of the syndesmotic ligaments, interosseous membrane, and other associated injuries to medial, posterior structures of the ankle. High Fibular Fracture at the fibular neck is referred as Maisonneuve Fracture of Fibula (MFF). These injuries are often missed or misdiagnosed as ankle sprains. Most of the current classification consider MFF a variant of ankle fracture with disruption of syndesmosis and high fibular fracture {Lauge Hansen PER, AO C3, Weber type C}. Only a few articles have described associated injuries and surgical treatment outcomes. The study’s primary aim is to evaluate the associated injuries of MFF and the outcomes of our treatment approach.
Methods: All patients undergoing syndesmotic fixation (CPT 27829) at a large tertiary academic center from 2012-2020 were identified. In these 748 patients, patient radiographs were reviewed to identify patients with Maisonneuve fractures (AO-44C3). Medical records were reviewed for patient characteristics, energy information of original injury, operative variables, and complications. Radiographic reduction was assessed on standard radiograph with assessment of the tibiofibular clear space and tibiofibular overlap on AP and mortise views, talocrural angle, the medial clear space, shenton line, and fibular station. An abnormality in one of these parameters was considered an abnormal reduction. Patients were contact to complete PROMIS Physical function and Pain Interference postoperatively. A total of 24 patients with Maisonneuve fractures were identified and included in analysis. Eleven patients completed PROMIS outcomes measures for a response rate of 55%, as four patients were deceased or incarcerated at the time of survey.
Results: The average age was 45.3 (16 SD) with a mean BMI of 31.3 (10.4 SD). Nineteen patients were male (79.2%) with only 5 females (20.8). The mechanism of injury was low energy in 16/24 patients (66.7%) leaving 8 (33.3%) patients with high energy mechanisms. In addition to the high fibular fracture, a total of 13 patients (54.2%) had a posterior malleolar fracture, 11 (45.8%) had a medial malleolar fracture, and 8 (33.3%) had a deltoid ligament injury. Seven patients (29.2%) received screw fixation compared to 14 patients (58.3%) with tightrope fixation. Three patients (12.5%) received both tightropes and screws. No patient developed wound complications, and two patients underwent reoperation. Abnormal reduction occurred in 5/24 patients (20.8%) at final clinical follow up. At a median of 20 months (25 IQR) postoperatively, the median PROMIS physical function and pain interference scores were 41.2 (13.0 IQR) and 52.8 (4.8 IQR), respectively.
Conclusion: Maisonneuve fractures are an extremely rare ankle fracture variant with a diverse subset of injury patterns. Our results show the clinical outcomes of Maisonneuve fractures are largely satisfactory in terms of wound complications and intermediate term outcomes. While 21% of patients were determined to have abnormal reduction postoperatively, we are limited by the inherent difficulties of assessing syndesmosis on plain radiographs rather than advanced imaging. PROMIS outcome scores demonstrate Maisonneuve fractures patients are more impacted by loss of function than pain, but both are within a standard deviation of the population mean.
DOI: 10.1177/2473011421S00081
Impact of Resilience on Patient Reported Outcomes of First Metatarsophalangeal Arthrodesis
Nicholas A. Andrews; Sterling Tran; Jared R. Halstrom, BS; Jessyca Ray; Whitt Harrelson; Aseel G. Dib, BS; Abhinav Agarwal, MBBS; Ashish Shah, MD
Category: Other; Ankle; Midfoot/Forefoot
Keywords: 1st MTP Joint; Arthrodesis; PROMIS
Introduction/Purpose: Resilience is an interactive dynamic construct most simply defined as the ability to recover from stress. To date, there is no literature examining the impact of resilience on the outcomes following foot and ankle surgery.
Methods: We retrospectively reviewed patients who underwent first MTP arthrodesis from September 2011 to May 2020, 98 met inclusion criteria. Medical records were reviewed for patient characteristics and union status. PROMIS Physical Function (PF), Pain Interference (PI), Depression (D), and the Foot Function Index (FFI) were collected. Resilience was measured using the Brief Resilience Scale. A multivariable linear regression analysis examining the impact of resilience on patient reported outcomes while adjusting for potential confounding covariates was conducted.
Results: At an average of 3.4+-2.6 (SD) years postoperatively, resilience was found to have an independent effect on patient reported outcomes across all instruments, except the FFI pain subscale. Resilience’s effect on the instruments was as follows: PROMIS physical function (Unstandardized β 5.0, 95% CI 2.6 to 7.4), PROMIS pain interference (Unstandardized β -4.8, 95% CI - 7.8 to -1.8), PROMIS Depression (Unstandardized β -9.4, (95% CI -12.8 to -6.1), FFI disability subscale (Unstandardized beta -13.3, 95% CI -20.3 to -6.3 ), FFI activity limitation subscale (Unstandardized beta -15.7, 95% CI -23.0 to -8.5), FFI total (Unstandardized beta -11.7, 95% CI -18.1 to -5.4), and FFI pain subscale (Unstandardized beta -6.5, 95% CI -13.1 to.01).
Conclusion: In this first study examining the impact of resilience following foot and ankle surgery, we found that resilience has an independent positive effect on overall physical function, disability, pain, and mental health following MTP arthrodesis. Preoperative resilience scores could be used to predict postoperative functional outcomes following MTP arthrodesis and guide postoperative rehabilitation. These findings help establish the role of early positive psychosocial characteristics within orthopaedic foot and ankle population.
DOI: 10.1177/2473011421S00082
Long Term Patient Reported Outcomes of Tarsal Coalition Resection in Pediatric Patients
Nicholas A. Andrews; Timothy Torrez; Jared R. Halstrom, BS; Tanvee Sinha; James Pate, BS; Abhinav Agarwal, MBBS; Michael J. Conklin; Ashish Shah, MD
Introduction/Purpose: Tarsal Coalition has been known to be associated with pes planovalgus, unrelenting pain, recurrent sprains, and arthrosis due to an abnormal connection between two or more bones of the feet following failure of segmentation during development. Three entities of coalition exist fibrous, cartilaginous and osseous. Most commonly patients present with pain during activity. On exam range of motion is usually limited and there may be valgus or varus malalignment of the hindfoot. Patients are often offered surgical resection following failure of conservative management. Few large cohort studies exist analyzing complications and patient reported outcomes of pediatric patients undergoing operative treatment.
Methods: After IRB approval, patients under the age of 18 undergoing excision of tarsal coalition at a single academic center from 2010-2019 were identified. Medical records were reviewed for variables such as demographics, surgical technique, coalition characteristics, postoperative complications, and coalition recurrence. Patients were contacted via telephone to complete a PROMIS Physical Function and Pain Interference in addition to the Foot Function Index. Contact was attempted at least 3 times before a patient was considered non-respondent. A total of 44 patients and 54 feet were included in the analysis with 17 patients (22 feet) completing patients reported outcomes.
Results: The median age at the time of surgery was 12 (IQR 3). Thirty-five feet (64.8%) were from male patients, while 19 feet (35.2%) were from female patients. Pain was the presenting symptom in 49 (90.7%) of feet. Pes planovalgus was present in 25 feet (46.3%). Forty feet (74.1%) had calcaneonavicular coalition compared to 12 feet (22.2%) with talocalcaneal coalition and 2 feet (3.7%) with both. Fibrous coalition was found in 19 feet (35.2%) and the most common. Interposition material was used in 49/54 (90.7%) feet. Wound complications or temporary neuropraxias were seen in 7/54 feet (13.0%), and coalition recurrence occurred in 3/54 feet (5.6%). At a median of 6 years (6.0 IQR) postoperatively, the median postoperative outcomes scores were as follows: PROMIS Physical Function 54.7 (17.9 (IQR)), PROMIS Pain Interference 38.7 (10.0), FFI Pain 14.0 (30.0), FFI Disability 1.0 (9.0), FFI Activity Limitation 3.0 (8.0), and FFI Total 6.0 (12.0).
Conclusion: Our study investigated complications and long-term patient outcomes following coalition resection. At follow-up, pediatric patients who underwent excision of tarsal coalition had higher physical function and less pain than the average U.S. population (PROMIS population mean is score of 50). Our recurrence rate of 5.6% is lower than reported in literature. Infection rate was similar to reports in literature at 3.1%. Overall, Coalition resection in pediatrics is a well-tolerated procedure that improves both physical and emotional health.
DOI: 10.1177/2473011421S00083
MTP Arthrodesis: Outcomes of Crossroads Dynaforce and Stryker Locking Plate
Nicholas A. Andrews; Jared R. Halstrom, BS; Jessyca Ray; Kenneth J. Fellows; Whitt Harrelson; Aseel G. Dib, BS; Abhinav Agarwal, MBBS; Osama M. Elattar, MD, MB BCh, MSc; Ashish Shah, MD
Introduction/Purpose: Metatarsophalangeal (MTP) joint arthrodesis is commonly performed for end-stage hallux rigidus with largely satisfactory results. While current literature demonstrates union rates in the low 90’s, there is still room for evolution of techniques and fixation constructs. The new Crossroads Dynaforce plate provides area for direct integration of a compression staple into the dorsal locking plate construct. The purpose of this present study was to compare outcomes of this new plating system to a standard dorsal locking plate from Stryker.
Methods: Patients undergoing primary MTP arthrodesis from 2010-2020 were identified. Patients receiving Crossroads Dynaforce plates (23 patients) and Stryker Dorsal locking plates (21) for Hallux Rigidus were selected. Radiographic follow-up of >12 weeks and no ongoing ipsilateral infection were required for inclusion. Medical records were examined for patient characteristics, operative variables, and complications. PROMIS physical function, pain interference, and depression domains were collected postoperatively in addition to Foot Function Index (FFI).
Results: The median age was 57.0 (IQR 16.0) with the average BMI of 30.4 (SD 11.2). No patient comorbidities or demographics were significantly different between Stryker and Crossroads groups. Importantly, the preoperative hallux valgus and intermetatarsal angles did not vary between groups. The use of an interfragmentary screw was significantly higher in the Stryker cohort 20/21 (95%) compared to 16/23 (70%) The rate of wound dehiscence, deep infection, and reoperation did not vary between groups. The nonunion rate did not differ between groups and was 3/21 (14.3%) in the stryker cohort compared to 1/23 (4.3%) in the Crossroads group. Patient reported outcomes measures did not differ between groups and were completed at an average of 2.2 years postoperatively (SD 1.9).
Conclusion: The Crossroads Dynaforce plate provides comparable outcomes to a legacy dorsal locking plate from Stryker in hallux rigidus. In addition to clinical outcomes, patients report similar levels of function at intermediate term follow up.
DOI: 10.1177/2473011421S00084
MTP Arthrodesis: Percutaneous Interfragmentary Screw Placement and Nerve Injury
Nicholas A. Andrews; David A. Patch, MD; Roshan Jacob; Charles R. Sutherland; Whitt Harrelson; Abhinav Agarwal, MBBS; Ashish Shah, MD
Introduction/Purpose: Iatrogenic cutaneous nerve injury is the most common complication encountered in foot and ankle surgery with limited evidence to inform surgeons on neuroprotective techniques. The purpose of this study was to assess risk for injury to the dorsomedial cutaneous nerve (DCN) during insertion of percutaneous interfragmentary screws used in metatarsophalangeal (MTP) arthrodesis.
Methods: Ten mid-tibia fresh frozen cadaver specimens were obtained for execution of this study. All cadavers were grossly and radiographically inspected for any evidence of existing pathology or prior operative intervention. Percutaneous placement of interfragmentary screw in both distal to proximal and proximal to distal fashion was performed. Only the skin was incised before reaming and screw placement. After screw placement, dissection of the great toe was conducted. The distance between the screws and the DCN was obtained. The DCN was also inspected for injury.
Results: A total of 10 cadavers were included. The average age of our population was 64 (+- 12.6). Males represented 80% of our included specimens. Injury to the DCN was not reported using the proximal to distal screw fixation. The mean distance from the dorsal cutaneous nerve using proximal to distal interfragmentary screw fixation was 7.45+- 3.85 mm compared to 4.30+-2.71 mm in the distal to proximal screw. Distal to proximal screw fixation was associated with 10% risk of nerve injury with no nerve injuries occurring at the site of proximal to distal screws.
Conclusion: In our cadaver study, proximal to distal screw fixation seems to offer neuroprotection in the setting of MTP arthrodesis. The DCN is known to have many anatomic variants, and DCN injuries can be a pretext for painful neuroma formation. Surgeons should consider careful dissection to the joint capsule in effort to decrease the risk of neurogenic injury when placing interfragmentary screws in MTP arthrodesis.
DOI: 10.1177/2473011421S00085
To Be(Ar) Or Not to Be(Ar) – Jones Dilemma?
Nicholas A. Andrews; Neha Singh; Abhinav Agarwal, MBBS; Austin Hughes; Roshan Jacob; Whitt Harrelson; Vyshnavi Rallapalle; Ashish Shah, MD
Category: Midfoot/Forefoot
Keywords: 5th Metatarsal Fractures; Jones Fracture; Fractures
Introduction/Purpose: Jones fracture is the fracture of the base of 5th metatarsal and is a commonly encountered in the clinical setting. Its management has always been a subject of great debate with paucity of consensus on post- operative weight bearing protocols. We aim to evaluate the efficacy of early weight bearing in the post-operative management of Jones fracture and assess its association with radiological union and patient reported outcomes.
Methods: Retrospectively, patients undergoing fixation of Jones fracture from January 2011 to December 2020 were identified. Radiographic follow-up of at least 8 weeks was required for inclusion yielding 40 patients. Patients were grouped by early weight bearing (EWB) as tolerated (26 patients) and non-weight bearing (NWB) for 2 weeks followed by partial weight bearing (14 patients). Medical records were reviewed for demographic variables, associated comorbidities, type of surgical construct used, fracture type, mode of injury and union. Delayed union was defined as patients without radiographic evidence of union at 12.5 weeks. Patients completed PROMIS physical function, PROMIS pain interference, and FFI scoring postoperatively.
Results: The mean age was 42.83+- 17.03 years with a female gender predominance (n=23; 57.5%) and an average BMI of 32.2 +- 8.7. Thirteen (50%) in the EWB and 5 (43%) in NWB groups experienced delayed radiological union (>12 weeks) and this did not differ by group. There was one nonunion in the NWB group and none in the EWB group. The number of wound complications did not vary by group. Seventeen patients completed postoperative FFI and PROMIS scores at a median of 40 months (41.5 IQR). The FFI and PROMIS scores did not differ by group. In the EWB group, the median PROMIS scores were physical function 43.7 (6.7 (IQR)) and pain interference 52.8 (10.1) compared to physical function 44.0 (11.6) and pain interference 55.2 (11.8) in the NWB group. The median total FFI score in the EWB group was 20.0 (27) compared to 32 (32) in the NWB group.
Conclusion: The EWB group exhibited comparable results to the NWB group after surgical fixation of Jones fracture. Importantly, PROMIS scores indicate both groups had comparable functional outcomes at long term follow up and were within a standard deviation of the general population of the United States (Score of 50 with SD of 10) for both pain and function. While further investigation is required, EWB may have equivocal results in terms of union, wound complications, and functional outcomes while allowing for early mobilization after Jones fracture fixation.
DOI: 10.1177/2473011421S00086
The Effectiveness of Perioperative Parecoxib Intravenous Administration in Foot and Ankle Surgery: A Prospective, Double-Blinded, Randomized, Placebo-Controlled Trial
Chayanin Angthong, MD, PhD
Category: Trauma; Ankle
Keywords: Ankle Fracture; IFFAS Award; Pain
Introduction/Purpose: Parecoxib is indicated for the short-term treatment of postoperative pain in adults. A systematic review assessed the analgesic efficacy of single dose intravenous (IV) or intramuscular (IM) parecoxib in acute postoperative pain and concluded that parecoxib is an effective analgesic in the postoperative setting in adults. However, little is known about its effectiveness in the perioperative intravenous administration in foot and ankle surgery. The present study conducts a double- blinded prospective randomized controlled trial via an ‘intention-to-treat analysis’ principle to compare the effectiveness of perioperative parecoxib versus placebo in patients with unstable ankle fractures who have surgical indications.
Methods: A total of 40 patients undergoing open reduction and internal fixation of the unstable ankle fractures were randomly allocated either to Group A (parecoxib 40 mg IV 30 min before surgery and then an additional 40 mg every 12 hours for 48 hours after surgery [n=20]) or Group B (placebo (saline) [n=20]). The baseline data were recorded in each patient. The efficacy of pain control was assessed by total morphine used, pain intensity (at rest/ambulation) and pain relief (at rest/ambulation) using the verbal numerical rating score (VNRS) from 0 (no pain) to 10 (worst imaginable pain) and the verbal numerical rating percentage (VNRP) from 0 (no relief) to 100 (best relief) respectively, as well as each patient’s subjective rating of the medication. The patients’ subjective rating of the medication used the classifications of ‘excellent’, ‘good’, ‘fair’, or ‘poor’. When the patients were moved to the post-anesthesia care unit (PACU) after surgery, the study procedure was to record the time as 0. The data were then recorded at 0, 4, 12, 24, and 48 hours after surgery by trained personnel. The overall adverse effects experienced by patients were reported in both groups. All outcomes were recorded by trained personnel who were blind to the patient group allocation. All surgeons, anesthesiologists, and patients involved in the process were also blind to the group allocations. The outcomes including efficacy, patients’ subjective ratings of the medication, and overall adverse effects were statistically compared between the two groups.
Results: From a total of 40 patients in the study, four patients were excluded by the study criteria. The remaining 36 patients continued in the study. The mean age of patients was 49.3 +/- 18.0 years. No significant difference was found regarding the mean age of patients between the two groups (p-value > 0.05). Male patients appeared more frequently in the saline group than the parecoxib group (p-value = 0.018). For the main outcomes, there were no significant differences between the two groups in terms of the pain intensity, pain relief, patients’ subjective ratings of the medication at both preoperative and postoperative periods, total quantity of morphine used, and side effects and acute complications of surgery (p-values > 0.05).
Conclusion: Based on the results of the present study, the perioperative administration of parecoxib could not significantly improve postoperative pain control as defined by the reduction in opioid requirements, lower pain scores, higher pain relief, and higher patients’ subjective ratings of the medication when compared to the placebo. Male predominance was significantly found in the placebo group. This may have influenced the level of pain tolerance between the two groups. This may also affect the results as no significant differences of pain parameters between the two groups in the study. Further study with larger numbers of patients is still necessary to clarify the role of preemptive parecoxib on ankle fracture surgery.
DOI: 10.1177/2473011421S00087
Correlation Between X-Ray and Weight-Bearing Computed Tomography for Imaging Evaluation of Hallux Valgus Deformity
Raul M. Espinoza Aravena, MD; Felipe R. Chaparro, MD; Cristian A. Ortiz, MD; Giovanni M. Carcuro, MD; Manuel J. Pellegrini, MD
Introduction/Purpose: Weight-bearing computed tomography (WBCT) has emerged as a valuable diagnostic tool for foot and ankle pathologies. Hallux valgus deformity values are well described in the literature, but there is a lack of correlation studies between x-rays and WBCT for the most widely used imaging parameters. The role of coronal plane deformity has gained importance in the last few years as a recurrence predictor factor. Most radiological descriptions in this topic are indirect measures of this rotational deformity. WBCT seems more precise to evaluate hallux valgus 3D deformity. Purpose: Correlate Hallux Valgus deformity parameters, metatarsal head morphology, and sesamoids position on x-rays compared to WBCT.
Methods: Hallux valgus (HVA), intermetatarsal (IMA), interphalangeal (IFA), and the distal metatarsal articular angle of the first metatarsal (DMAA) was measured on standing AP load-bearing radiographs (WBXR) and WBCT by 2 observers in hallux valgus patients. Deformity parameters obtained by both imaging methods were correlated with the Spearman Correlation (SCC) and the Intraclass Correlation Coefficient (ICC). Also, WBXR was analyzed to estimate the first metatarsal head rotation (pronation) by the round sign and sesamoids position. Then, direct pronation measurement was measured on WBCT by obtaining the Alpha Angle (AA) and sesamoids position in relation to the metatarsal head was defined. The Kappa concordance index (KCI) was determined.
Results: 40 feet with Hallux Valgus were evaluated. In WBXR the medians of HVA, IMA, IFA, and DMAA were 24.5, 12, 8.98, and 13.08 degrees respectively. In WBCT the medians were 24.75, 12.93, 6.05, and 13.03 respectively. The SCC was 0.934 for HVA, 0.956 for IMA, 0.713 for IFA, and 0.487 for DMAA, and the ICC was excellent for HVA, IMA, and IFA for both methods, excellent for DMAA in WBXR, but poor for WBCT. For rotation deformity, the correlation between metatarsal head morphology and AA was poor with a KCI of -0.073, and also for the position of the sesamoids between both methods and the KCI was 0.061.
Conclusion: Evaluated deformity parameters had an excellent correlation between WBXR and WBCT. Both methods are useful for determining HVA, IMA, and IFA in Hallux Valgus patients, but it was poor for DMAA. Also the correlation between first metatarsal head morphology on WBXR (Round sign) with metatarsal head pronation (Alpha Angle) on WBCT was poor, as well as sesamoids position. Given greater WBCT precision to evaluate rotational deformity, we believe it should be considered in the diagnostic process to most accurately understand this complex deformity.
DOI: 10.1177/2473011421S00088
A Systematic Review of the Management of Multiple Adjacent Morton’s Neuromas in the Same Foot
Introduction/Purpose: The most common presentation of Morton’s neuroma is that of a single neuroma in a single interdigital space. However, the occurrence of multiple neuromas in adjacent interdigital spaces of the same foot is not uncommon, with this scenario reported in 3-4% of all cases. Treatment of Morton’s neuroma has been studied extensively, with most authors recommending surgical intervention only after failure of non-operative approaches such as steroid injection orthoses or shockwave therapy. Whilst systematic reviews on the management of Morton’s neuroma have been performed previously, these focus on the treatment of a single neuroma in a single foot. This review aims to address this gap in the literature by systematically reviewing studies reporting treatment of multiple neuromas in adjacent intermetatarsal spaces of the same foot.
Methods: A systematic review was performed according to PRISMA guidelines. A thorough computer-based search was performed by two reviewers independently in Pubmed, Embase, Cinahl, Emcare, Web of Science and Scopus databases using relevant terms such as ‘interdigital’, ‘Morton’s’, ‘intermetatarsal’, ‘neuroma’, ‘neuralgia’, ‘adjacent’ and ‘multiple’. Title/abstract and full text screening was performed independently by the same two reviewers, using a-priori selection criteria. All original research articles (randomised control trails, cohort studies and observational studies) reporting any management strategy for multiple adjacent Morton’s neuromas in the same foot were included. Studies describing treatment of both single and multiple adjacent neuromas in the same article were included if results were clearly separated according to these distinct presentations. The methodological index for non-randomized studies (MINORS) was used to assess risk of bias and methodological quality of included studies.
Results: A total of 253 unique articles were identified, with seven studies, including 383 patients included in the final review. Of these seven studies, four describe treatment of both single and multiple neuromas in the same article, whilst three include only patients with multiple adjacent neuromas in the same foot. Simultaneous excision using a single incision was the most common strategy, reported in three studies. Whilst two studies each reported use of simultaneous excision with two distinct incisions and delayed excision respectively. Of the four studies reporting treatment of both single and multiple neuromas, the pooled proportion of patients with the later presentation was 51/354 (14.4%). Only two studies, both describing simultaneous excision with a single incision, used scoring scales to assess treatment outcomes. These articles find significant increases in Manchester Oxford Foot questionnaire (MOXFQ), 12 item short form health survey (SF-12) and American Orthopaedic Foot & Ankle Society (AOFAS) scores.
Conclusion: There is currently no evidence favouring use of a delayed excision or multiple incision approach in the treatment of multiple adjacent neuromas. However, there is a paucity of literature describing this presentation, with a number of studies failing to separate outcomes of single and multiple neuroma treatment. Given that the presentation of multiple adjacent neuromas may not be as rare as previously thought, it is important that further high-quality comparative research is performed to enable clinicians to draw firm, evidence-based conclusions to guide clinical practice. Future research should also investigate the role of alternative strategies such as non-operative treatment.
DOI: 10.1177/2473011421S00089
Non-Operative Management of Chronic Achilles Tendon Ruptures: Short Term Outcomes
Introduction/Purpose: The incidence of Achilles tendon rupture in the United States is approximately 2.6 per 100,000 person years, with a significant increase in incidence over recent years reported. Should the acute rupture not be diagnosed promptly, as is the case in up to 20% of patients, the injury may be termed chronic. A number of operative treatment strategies for chronic Achilles ruptures have been described, including v-y tendinous flap, flexor hallucis longus tendon transfer, peroneus brevis graft and free gracilis transfer. Despite the extensive investigation of non-operative treatment in acute ruptures, there is a lack of similar research into chronic injuries. This article aims to address this gap in the literature, reporting treatment results of patients treated conservatively after being deemed unfit for operative intervention.
Methods: A retrospective review of all patients receiving non-operative treatment for chronic Achilles ruptures, in the senior author’s clinic between December 2014 and May 2019 was performed. A chronic injury was defined as occurring when there was a delay of at least 28 days between initial injury and start of treatment. Patients with a minimum final follow up of less than 6 months were excluded. All patients were managed according to the previously described Leicester Achilles Management Protocol (LAMP), an eight-week functional dynamic regime with use of a VACOped boot (OPED, Valley, Germany). Formal physiotherapy treatment was also provided following completion of the LAMP. Hospital records were searched for relevant data including patient age and sex, side of injury, time between injury and start of treatment and post-treatment Achilles tendon total rupture score (ATRS).
Results: A total of 17 consecutive patients with a minimum follow up of 6 months were managed non-operatively during the stated time period. The cohort included eight males and nine females with a mean age of 63.4 14.3 years. The right side was injured in five cases, with the left side affected in 12. The mean time from initial injury to start of treatment was 43.9 days (range 30 - 102 days). The mean ATRS at 6 months post treatment was 53+-17.8. A total of 10 patients were also available for follow up at 12 months. The mean ATRS in these patients at 12 months was 73 +-15.2.
Conclusion: The mean 12-month ATRS of 73 achieved is lower than figures of 89-92.5 reported in previous studies describing operative treatment. However, our results indicate that good outcomes may be achieved using a non-operative protocol in patients who decline or are unfit for surgery. Recent research reports that the mean age of Achilles rupture has increased by 0.721 years every five years, since 1953. It could therefore be likely that an increasing number of patients suffering chronic Achilles ruptures may be unfit for surgical treatment. It is important that further research into the non-operative treatment of these patients is conducted.
DOI: 10.1177/2473011421S00090
Assessment of Ankle Fractures using Deep Learning Algorithms and Convolutional Neural Network
Soheil Ashkani-Esfahani, MD; Reza Mojahed-Yazdi; Rohan Bhimani, MD, MBA; Gino Kerkhoffs, MD; Daniel Guss, MD, MBA; Christopher W. DiGiovanni, MD; Bart Lubberts, MD, PhD
Category: Ankle; Trauma
Keywords: Ankle Fracture; Fractures; Ankle
Introduction/Purpose: Early and accurate detection of ankle fractures is crucial for reducing future complications. Radiographs are the most abundant imaging techniques for assessing fractures. We believe deep learning (DL) methods, through adequately trained deep convolutional neural networks (DCNNs), can assess radiographic images fast and accurate without human intervention. In this study, we aimed to assess the performance of two different DCNNs in detecting ankle fractures using radiographs compared to the ground truth.
Methods: In this retrospective study, our DCNNs were trained using radiographs obtained from 1050 patients with ankle fracture and the same number of individuals with otherwise healthy ankles. Inception V3 and Renet50 pre-trained models were used in our algorithms. Danis-Weber classification method was used. Out of 1050, 72 individuals were labeled as occult fractures as they were not detected in the primary radiographic assessment. Using single-view radiographs was compared with 3-views (anteroposterior, mortise, lateral) for training the DCNNs.
Results: Our DCNNs showed a better performance using 3-views images versus single-view based on greater values for accuracy, F-score, and area under the curve (AUC). The sensitivity and specificity in detection of ankle fractures using 3-views were 97.5% and 93.9% using Resnet50 compared to 98.7% and 98.6 using inception V3, respectively. Resnet50 missed 3 occult fractures while Inception V3 missed only one case. In cases that detected the fracture, the saliency map showed the location of the fracture (Figure 1).
Conclusion: The performance of our DCNNs showed a promising potential that can be considered in developing the currently used image interpretation programs or as a separate assistant to the clinicians to detect ankle fractures faster and more precisely.
DOI: 10.1177/2473011421S00091
The Use of Deep Machine Learning in Detecting Subtle Lisfranc Joint Instability on Weightbearing Radiographs and Non-Weightbearing CT Scans
Soheil Ashkani-Esfahani, MD; Reza Mojahed-Yazdi; Rohan Bhimani, MD, MBA; Gino Kerkhoffs, MD; Gregory R. Waryasz, MD; Christopher W. DiGiovanni, MD; Bart Lubberts, MD, PhD; Daniel Guss, MD, MBA
Introduction/Purpose: Diagnosis of subtle Lisfranc joint instability, as a commonly missed foot injury, has remained a concern since it can result in future disabilities if inadequately treated. Weightbearing radiographs (WBR) and conventional CT scans are the most frequent methods in healthcare centers all around the world that are used to assess tarsometatarsal injuries, specifically the Lisfranc joint. However, their accuracy in detecting subtle cases varies depending on the experience and expertise of the interpreter as well as the quality of the images. We aimed to evaluate the use of deep learning and deep convolutional neural network (DCNN) in the detection of subtle Lisfranc instability using WBR and CT scans. Our hypothesis was that this method can increase the accuracy and hasten the interpretation using these modalities.
Methods: We gathered 200 WBR and 200 CT scans of cases with subtle Lisfranc instability who were diagnosed intraoperatively; 200 WBR and 200 CT scans of patients with otherwise healthy feet were added as the control group. To increase the confidence in the results we implemented saliency maps to visualize the location of the injury as a heat map and exhibit the process of decision-making by the algorithm. The data of the study was expressed as sensitivity, specificity, accuracy, and the area under the curve (AUC). We used Inception DCNN model as the pre-trained DCNN model in this study.
Results: The performance of the DCNN using WBR resulted in sensitivity=93.6%, specificity=91.1%, Accuracy= 94.7, AUC=98.2%. DCNN applied on CT scan resulted in sensitivity=95.8%, specificity=96.9%, accuracy= 93.2, and AUC=98.4%. In cases that the injury was detected correctly by the DCNN, the saliency map had shown the location of the injury correctly as well (100%, Figure 1).
Conclusion: Here we showed that using DCNN on the currently used interpretation method can significantly improve the accuracy of interpretation using WBR and CT scans in the detection of subtle Lisfranc instability. WBR has lower costs and a lower rate of radiation, thus, improving its performance using deep learning methods can lead to a significant improvement in healthcare quality for the patient and reduced costs for the system.
DOI: 10.1177/2473011421S00092
Volume Measurements on Weightbearing Computed Tomography Can Detect Subtle Syndesmotic Instability
Soheil Ashkani-Esfahani, MD; Rohan Bhimani, MD, MBA; Bart Lubberts, MD, PhD; Gino Kerkhoffs, MD; Gregory R. Waryasz, MD; Christopher W. DiGiovanni, MD; Daniel Guss, MD, MBA
Introduction/Purpose: The ability to compare the ankle joints bilaterally in a 3D manner under physiologic weight provided by weight-bearing CT has led to a more accurate diagnostic method. While weight-bearing computed tomography (WBCT) allows 3D visualization of the distal syndesmosis, image interpretation has largely relied on 1D distance and, more recently, 2D area measurements. This study aimed to: 1) determine the sensitivity and specificity of 2D area and 3D volume WBCT measurements towards detecting subtle syndesmotic instability, 2) evaluate whether the patterns of changes in the 3D shape of the syndesmosis can be attributed to the type of ligament injury.
Methods: A total of 24 patients with unilateral subtle syndesmotic instability and 24 individuals with uninjured ankles (controls) with bilateral ankle WBCT were assessed retrospectively. First, 2D areas at 0, 1, 3, 5,10 cm, and 3D volumes at 1, 3, 5, and 10cm above the tibial plafond were measured bilaterally. Secondly, given the volume measurement at the level of 5 cm proximal to the platform as the most sensitive and specific method introduced in this study, the 3D model of the distal tibiofibular space was created based on WBCT in a subset of 8 patients out of 24 in whom the type of ligament injury was recognized via MRI. The 3D model of the injured side was superimposed on the uninjured contralateral side to visualize the pattern of changes in different planes. P<0.05 was considered statistically significant.
Results: No specific pattern was observed in 2D and 3D models of the syndesmotic space which can be attributed to a specific ligamentous tear. However, in patients with IOL rupture, the volume increased by >=39% at 5 cm height while without IOL injury the volume increased up to 26% (figure 1). The percentage of changes in 2D areas and 3D volumes showed significant differences in areas at 0cm (19.2%; p=0.004), 1cm (24.1%; p=0.002), 3cm (27.3%; p=0.003), 5cm (28%; p=0.002), and 10cm (29.3%; p=0.003) as well as volumes at 1cm (31.2%; p=0.003), 3cm (26.5%; p=0.001), 5cm (25.4%; p<0.001), and 10cm (24.7%; p=0.004) proximal to tibial plafond. Volume up to 5cm showed the lowest p-value, higher sensitivity (95.8%, 95%CI:87.8-100), and specificity (83.3%, 95% CI:68.4-98.2) for detection of syndesmotic instability.
Conclusion: We suggest 3D volume measurements, best measured up to 5cm proximal to the plafond, as a promising means of diagnosing syndesmotic instability, particularly for subtle cases that are hard to detect.
DOI: 10.1177/2473011421S00093
Donor Site Morbidity of Calcaneal, Distal and Proximal Tibial Cancellous Autografts in Foot and Ankle Surgery: A Systematic Review and Meta-Analysis of 2296 Grafts
Ahmed K. Attia, MD; Karim Mahmoud Khamis, MB BCh; Kareem Ahmed H.M.A. Elsweify; Jason T. Bariteau, MD; Sameh A. Labib, MD
Category: Other
Keywords: Bone Block Graft; Complications; Arthrodesis
Introduction/Purpose: Non-union of foot and ankle arthrodesis sites has been associated with revision surgery, morbidity and increased healthcare costs, so many surgeons elect to augment the fusion site with autologous bone grafts to improve union. While iliac crest autografts are considered the historical gold standard, other donor sites distal in the lower extremity such as calcaneus, proximal and distal tibia have been successfully used in foot and ankle surgery. This study aims to report on the safety and donor site morbidity of distal lower extremity (calcaneal, proximal and distal tibial) bone autografts. We summarized the findings in a comprehensive infographic illustration. We are unaware of any similar meta-analyses to date.
Methods: Following the PRISMA guidelines, 2 independent investigators searched several databases in December 2020 using the following keywords and their synonyms: (‘Bone graft’, ‘donor site morbidity’, ‘calcaneal graft’, ‘Proximal tibia graft’, and ‘distal tibia graft’). Besides, the reference lists from previous review articles were searched manually for eligible studies. The primary outcomes of interest were (1) Chronic pain, (2) Fracture and (3) infection whereas the secondary outcomes were (1) neurological complications, (2) sensory disturbance and hypertrophic scars, (3) other complications such as shoe-wear difficulties and gait disturbance. Inclusion criteria were: studies on complications and adverse events of lower extremity bone autografts (calcaneal, proximal tibial, and distal tibial bone autografts) reporting at least one desired outcome. Studies not reporting any of the outcomes of interest or if the full text is not available in English were excluded. Studies reporting on bone marrow aspirate or autografts for non-orthopedic indications were also excluded.
Results: After removal of duplicates, 5981 studies were identified. After screening, 85 studies remained for full-text assessment, and 15 studies qualified for the meta-analysis with a total of 2296 bone grafts.1557(67.8%) were calcaneal grafts, 625 (27.2%) were proximal tibial grafts, and 114 (5%) were distal tibial grafts. The mean age of all patients was 52.43+-16 [CI=51.77-53.08] years. The mean follow-up duration was 1.86+-1.70[CI=1.79-1.93] years. The primary surgery was reported for 2129 grafts(92.7%).Out of those, foot and ankle procedure represented 97.4% of the procedures. In calcaneal bone grafts, there were 28 cases of chronic pain [1.97%,CI:1.10-2.50%, I2=66%], 5 fractures [0.32%,CI:0.10-0.60%, I2=0%], 20 sural neuritis [1.28%,CI:0.70-1.80%, I2=0%), and no wound infections. In proximal tibial grafts there were 13 cases of chronic pain [2.08%,CI:1.01-3.2%, I2=34.5%], 1 fracture [0.16%,CI:0.10-0.50%, I2= 0%], and 3 superficial wound infections [0.48%,CI:0.10-1.01, I2=0%]. In the distal tibial grafts there were no cases of chronic pain or wound infections, 1 fracture [0.90%,CI:0.80-2.6%,I2=0%], and 5 saphenous neuritis [4.5%,CI: 0.70- 8.40%,I2=65%].
Conclusion: Calcaneal, distal tibial, and proximal tibial bone autografts are safe with a low rate of overall and major complications. We report an overall complication rate of 6.8%, which is less than half of that previously reported for iliac crest grafts. The authors recommend using distal lower extremity grafts for foot and ankle primary surgeries instead of iliac crest grafts when indicated. Clinical trials with large sample sizes are required.
DOI: 10.1177/2473011421S00094
Outcomes and Complications of Open vs Minimally Invasive Surgical Repair of Acute Achilles Tendon Rupture: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Ahmed K. Attia, MD; Karim Mahmoud Khamis, MB BCh; Pieter Dhooghe, MD, MBA, PhD; Jason T. Bariteau, MD; Sameh A. Labib, MD; Mark S. Myerson, MD
Category: Ankle; Sports; Trauma
Keywords: Achilles Tendon Repair; Open Repair; Minimally Invasive
Introduction/Purpose: Traditionally, open surgical repair has provided improved functional outcomes, reduced re-rupture rates, and quicker recovery and return to activities at the expense of increased wound complications of infection and skin necrosis compared to nonoperative management. Ma and Griffith in 1977 introduced the percutaneous approach, and over the following decades, multiple improved techniques, and modifications thereof, have been described with comparable outcomes to the open repair. The current study aims to provide updated level I evidence comparing the open and minimally invasive (MIS) through a comprehensive search of literature published in English, Spanish, Portuguese, and German while avoiding limitations of previous studies such as heterogeneous study designs and a small number of included studies.
Methods: Following the PRISMA guidelines, two independent team members searched several databases to identify randomized controlled trials (RCTs) comparing open and MIS Achilles tendon repairs. The primary outcomes were (1) Sural nerve injury, (2) Skin complications, (3) Infection (deep/superficial), whereas the secondary outcomes were (1) AOFAS/ATRS score, (2) surgical time, (3) re-rupture (4) adhesions (5) ankle range of motion. Population: Achilles tendon rupture Intervention: MIS repair Control: Open repair Outcomes: Primary: (1) Sural nerve injury, (2) Skin complications, (3) Infection (deep/superficial) Secondary: (1) AOFAS/ATRS score, (2) surgical time, (3) re-rupture, (4) adhesions, (5) ankle range of motion (6) other complications.
Results: Ten RCTs qualified for the meta-analysis with a total of 522 patients. 260(49.8%) patients had open repair while 262(50.2%) had MIS repair. The mean total complication rate was 15.5% (0-36.4%) in open repair vs. 10.4% (0-45.5%) in MIS repair, with non-significant statistical difference (RR= 1.50,CI=0.87-2.57,p= 0.14;I2=40%). The mean re-rupture rate was 2.5% (0-6.8%) in open repair vs. 1.53% (0-4.6%) with MIS repair, with non-significant statistical difference (RR=1.56,CI=0.42-5.70,p= 0.50;I2=0%). No cases of sural nerve injury were reported in the open repair group. The mean sural nerve injury was 3.4%(0-7.3%) in the MIS group, that was statistically significant (RR= 0.16,CI=0.03-0.46,p=0.02;I2=0%). The mean deep infection rate in the open group was 1.4% (0-5%) while no deep infection was reported in MIS, with no statistically significant difference (RR= 3.24,CI=0.48-20.54,p= 0.23;I2=0%). The mean superficial infection rate was 6.04% (0-18.2%) and 0.40% (0-4.5%) for open and MIS repairs, respectively, with statistically significant difference (RR= 5.70,CI=1.80-18.02,p< 0.001;I2=0%).
Conclusion: Open Achilles tendon repair is associated with longer surgical time, higher risk of superficial infection, and ankle stiffness, while MIS repair is associated with a greater risk of temporary sural nerve palsy. Re-rupture rate and functional outcomes are mostly equivalent. We found MIS to be a safe and reliable technique. However, high-quality standardized RCTs are still needed before recommending MIS as the gold standard for the management of Achilles tendon rupture.
DOI: 10.1177/2473011421S00095
Outcomes of Arthroscopic vs Open Broström Surgery for Chronic Lateral Ankle Instability: A Systematic Review and Meta-Analysis of Comparative Studies
Ahmed K. Attia, MD; Tarek A. Taha, MD; Karim Mahmoud Khamis, MB BCh; Kenneth J. Hunt, MD; Sameh A. Labib, MD; Pieter Dhooghe, MD, MBA, PhD
Introduction/Purpose: Ankle sprains are the most common ankle injury accounting for up to 85% of all ankle injuries, and nearly 20% of acute ankle sprains progress to chronic lateral ankle instability that requires surgical intervention. In recent years, there has been a growing interest in arthroscopic Broström techniques as an alternative to open surgery. In the past two years alone, four comparative studies have been published. Recent case series and cohort studies showed reliable improvement in clinical and radiographic outcomes with arthroscopic surgeryAIM. The current study aims at providing the foot and ankle surgery community with the most updated evidence comparing outcomes of open to arthroscopic Broström procedure for chronic lateral ankle instability.
Methods: This article was performed following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. Two independent authors searched several databases for relevant comparative studies in English literature were identified between database inceptions to May 2020. The primary outcomes were (1) Functional scores (KAFS, AOFAS) and (2) Pain score on VAS, whereas the secondary outcomes were differences in (1) anterior drawer and talar tilt, (2) surgical time and complications rate, (3) time to return to sports and weight-bearing. Population: Chronic lateral ankle instability (LAI)Intervention: Arthroscopic Broström procedure Control: Open Broström procedure Outcomes: Primary: Functional scores, pain Secondary: Anterior drawer and talar tilt, complications, time to return to sport and weight-bearing
Results: A total of 408 patients in eight studies met the inclusion criteria were subjected to analysis. 193 (47.3%) patients underwent open surgery, while 215 (52.7%) patients underwent arthroscopic surgery. The one year-AOFAS was 80.05 vs. 88.6 in open and arthroscopic surgery, respectively (MD= -11.96, CI= -21.26, -2.76, I2= 82%, p= 0.01). The mean one year VAS was 2.05 and 1.45 in open and arthroscopic repair, respectively (MD= 0.31, CI= 0.09 to 0.54, I2=0%, p<0.001).The mean time to weight- bearing was 14.25 weeks and 9.0 weeks in open and arthroscopic repair, respectively (MD=1.89, CI= 1.24 to 2.54, I2=99%, p<0.001).There were no statistically significant differences in the time to RTP, postoperative anterior drawer, postoperative talar tilt, and operative time. The total complications rate in open and arthroscopic repair was 21.3% vs. 10%, with statistical insignificance (OR= 0.73, 95%CI= 0.39 to 1.38, I2=0%, p= 0.34).
Conclusion: While technically more demanding, arthroscopic Broström is superior to open Broström-Gould surgery in AOFAS functional scores at six and twelve months, time to return to weight-bearing, and VAS pain scores. Operative time, complications rate, talar tilt, and anterior drawer tests are excellent and statistically comparable. Long-term clinical trials are required before recommending arthroscopic Broström as the new gold standard.
DOI: 10.1177/2473011421S00096
Return to Play after Low-Energy Lisfranc Injuries in High Demand Individuals: A Systematic Review and Meta-Analysis of Athletes and Active Military Personnel
Ahmed K. Attia, MD; Karim Mahmoud Khamis, MB BCh; Abduljabbar Alhammoud, MD; Pieter Dhooghe, MD, MBA, PhD; Daniel C. Farber, MD
Category: Sports; Midfoot/Forefoot
Keywords: Lisfranc Injuries; Athlete; Return to Play
Introduction/Purpose: Low-energy Lisfranc injury is increasingly reported in the literature. While there is a relatively large body of studies discussing the high energy Lisfranc injuries, the evidence available on this low-energy injury in active individuals with high demand remains scarce and mostly retrospective. The injury can range from a non-displaced ligamentous sprain to fracture-dislocations, and management varies from non-operative management to primary arthrodesis with a multitude of variables potentially affecting the return to play (RTP) and return to duty (RTD). This study aims to report on return to play (RTP) rate and time with regard to the type of the injury, whether bony or ligamentous, management whether non-operative, open reduction and internal fixation (ORIF) or the increasingly debated primary arthrodesis (PA).
Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, relevant studies in English literature were identified between database inceptions to June 2019. Electronic based search on MEDLINE (PubMed), EMBASE, Google Scholar, and Cochrane databases using the following keywords with their synonyms: (‘Lisfranc’ AND ‘athlete’ AND ‘midfoot sprain’). In addition, the reference lists from previous review articles were searched manually to check for eligible studies. Two investigators (AA, KM) independently reviewed all titles, abstracts, and the full text of articles that were potentially eligible based on the abstract review. The eligible studies were selected according to the inclusion and exclusion criteria. Any disagreement was resolved by the senior author (DF). The primary outcomes were (1) return to play rate and (2) time to return to play, whereas the secondary outcomes were (1) games missed, (2) time out of practice, (3) midfoot arthritis, and reoperation.
Results: 15 studies were eligible for meta-analysis with a total of 441 subjects. Out of 441 subjects, a total of 380 (86.16%) were able to return to play and duty. There were no statistically significant difference in RTP comparing op vs. non-op [OR=0.714, CI: 0.17-2.88,I2=0%] nor ORIF vs. PA [OR=0.780, CI: 0.310-1.963, I2=0%]. The overall RTP in bony and ligamentous injuries were 82.1% [CI:70.9-93.4%, I2=0%] and 95.8% [CI:92.6-99.1%, I2=0%], respectively with no statistically significant differences [OR=1.909, CI=0.64- 5.64, I2=37%]. The mean time out in non-op and op. groups were 58.01 [CI:13.6-102.4, I2=98.03%] and 116.4 [CI:62.4-170.4; I2=99.45%] days, respectively. The mean time out in bony and ligamentous injury groups were 98.8 [CI:6.1- 191.6, I2=99.82%] and 76.4 [CI:37.9-115.02; I2=99.83%] days, respectively with statistically significant differences [SMD:3.621, CI:- 5.7-13, I2=83.17%].
Conclusion: Our meta-analysis on low-energy Lisfranc injuries in high demand individuals found an overall excellent RTP/RTD rate. The time out was not affected by the management, bony or ligamentous nature of the injury nor players’ position. However, the low level of evidence and significant heterogeneity of the included studies precludes making conclusions regarding the exact time out or optimal management. Superior quality studies on low energy Lisfranc are needed.
DOI: 10.1177/2473011421S00097
Return to Play and Fracture Union after Surgical Management of Jones Fracture in Athletes: A Systematic Review and Meta-Analysis
Ahmed K. Attia, MD; Tarek A. Taha, MD; Geraldine W. Kong; Abduljabbar Alhammoud, MD; Karim Mahmoud Khamis, MB BCh; Mark S. Myerson, MD
Introduction/Purpose: Proximal fifth metatarsal fractures are among the most common forefoot injuries in athletes. Management of this injury can be challenging due to delayed union and refracture. Intramedullary screw fixation rather than conservative management has been recommended in the athletic population. This meta-analysis aims to provide an updated summary of return to play (RTP) rate and time with regard to the management, whether operative or non-operative, after Jones fractures in athletes only. We also explore the characteristics of the union such as time and rate, and complications such as refracture.
Methods: Following PRISMA guidelines, relevant studies in English literature were identified between databases inceptions to November 2019. Electronic based search on MEDLINE (PubMed), EMBASE, Google Scholar, and Cochrane databases using the following keywords with their synonyms: (‘fifth metatarsal fracture’ AND ‘athlete’ AND ‘return to play’). In addition, the reference lists from previous review articles were searched manually to check for eligible studies. Two investigators independently reviewed all titles, abstracts, and the full text of articles that were potentially eligible based on the abstract review. Any disagreement was resolved by the senior author. The primary outcomes were (1) return to play rate and (2) time to return to play, whereas the secondary outcomes were (1) games missed, (2) time to union and union rate (3) non-union, delayed union and refracture. The current study accepted the definitions of included studies for non-union, delayed union, and refracture for practicality purposes.
Results: Out of 168 studies identified, 22 studies were eligible for meta-analysis with a total of 646 Jones fractures. The overall RTP rate was 98.4% (97.3%- 99.4%) in 626 out of 646. The RTP rate in IM screw only was 98.8% (97.8%-99.7%), in other surgical fixations methods (plate, mini fix) was 98.4% (95.8%-100%) whereas in conservative management was 71.6% (45.6%-97.6%). There were three studies directly comparing the RTP in surgical versus conservative management, which showed significant superiority in favor of the surgical group OR: 0.033 CI:( 0.005-0.215) P-value <0.001. The overall time to RTP was 9.6 (8.5-10.7) weeks. The time to RTP in the surgical group (IM screw) was 9.6 (8.3-10.9) weeks, significantly less than the conservative group, which was 13.05 (8.15-17.95) weeks. The pooled union rate in the operative group (excluding refracture) was 97.3% (95.1%-99.4%), whereas the pooled union rate in the conservative group was 71.4% (49.1%- 93.7%).
Conclusion: Return to play following surgical management of Jones fractures in athletes is excellent regardless of the implant used and sport. Intramedullary screw fixation is superior to conservative management as it leads to a higher rate of return to play, shorter time to return, higher union rate, shorter time to union, and improved functional outcomes. The authors recommend surgical fixation for all Jones fractures in athletes.
DOI: 10.1177/2473011421S00098
Bulk Osteochondral Allograft for Osteochondral Lesions of the Talus: A Systematic Review
Mohammad Azam; Martin S. Davey; Christopher Colasanti; Nathaniel P. Mercer; Eoghan T. Hurley, MB BCh BAO; Yoshiharu Shimozono, MD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle
Keywords: Osteochondral Lesions of the Talus; Lesions of Talus; Ostoechondral lesion
Introduction/Purpose: The use of bulk osteochondral allograft (OCA) is often warranted in patients with a large osteochondral lesion of the talus (OLT). Previous literature reported that bulk OCA has high failure and revision rates, suggesting these procedures should be thought of as an intermediate step, buying time before arthrodesis or arthroplasty is required. However, recent studies suggest that the long-term survival of bulk OCA has improved and that these procedures may provide a definitive solution for large OLT. The purpose of this study was to systematically review the literature to ascertain the outcomes of bulk OCA for OLT.
Methods: Two independent reviewers performed the literature search based on PRISMA guidelines, utilizing the EMBASE, MEDLINE, and The Cochrane Library Databases. Studies were included if they reported outcomes of OLTs which were managed by bulk OCA.
Results: Overall, 9 studies with 112 patients (55.4% males) including 115 ankles with a mean follow-up of 72.7 (8 - 240) months were included in this review. Pre-operative OLT characteristics showed that 68.4% were medial lesions, with a mean lesion size of 3.04cm2 (0.7 - 6.1 cm2). Overall, 23.5% of patients required revision surgery following bulk OCA; 10.4% (12/115) underwent subsequent arthrodesis, 1.7% (2/115) underwent revision osteochondral grafting and 9.6% (11/115) underwent arthroscopic debridement. Radiological outcomes reporting graft failure was 21.3% (13/61), joint space narrowing was 25.2% (29/115) and cysts were present in 19.5% (15/77) of cases.
Conclusion: Patients experience satisfactory patient-reported clinical outcomes in the medium term following bulk OCA in the management of OLT. Despite recent advances in graft procurement and storage radiological graft failure and the requirement for additional surgeries still remain. At this time can only be recommended in cases that are refractory to other treatments and where the patient is aware that this may be a temporizing procedure before arthroplasty or arthrodesis.
DOI: 10.1177/2473011421S00099
Chronic Achilles Tendon Ruptures: A Systematic Review
Mohammad Azam; James J. Butler; Nathaniel P. Mercer; Eoghan Hurley; Yoshiharu Shimozono, MD; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: Chronic Achilles tendon ruptures (CATR) are an uncommon injury compared to acute ruptures. Currently, no evidence-based guidelines exist for treating CATR. The purpose of this systematic review was to present the outcomes of the current treatment options for CATR and to analyze the level of evidence (LOE) and quality of evidence (QoE) of the included studies.
Methods: In July 2020, MEDLINE, EMBASE and Cochrane Library databases were systematically reviewed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The LOE and QOE of the included studies was evaluated using the Modified Coleman Methodology Score. Studies reporting outcomes following repair of CATR were included.
Results: Thirty-one studies with 653 CATRs were included. Three studies were LOE III and 28 studies were LOE IV. Six studies reported dual technique procedures and 23 studies reported single technique procedures. Semitendinosus graft was the most frequently utilized single technique procedure amongst the included studies. Most studies reported good postoperative subjective outcomes, strength outcomes, and return to sports data at mid-term follow-up. In total, 14.6% of patients experienced postoperative complications. The most common complication was surgical wound complications (10.8%).
Conclusion: This systematic review found that no evidence-based treatment guidelines exists for CATR. Surgical management of CATR produces good clinical outcomes at mid-term follow up, but a high complication rate (14.6%) was noted. Future studies of higher QOE and LOE with improved data reporting are warranted to determine the optimal treatment strategy for CATR.
DOI: 10.1177/2473011421S00100
Cylindrical Osteochondral Allograft for Osteochondral Lesions of the Talus: A Systematic Review
Mohammad Azam; Martin S. Davey; Christopher Colasanti; Nathaniel P. Mercer; Eoghan T. Hurley, MB BCh BAO; Yoshiharu Shimozono, MD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle
Keywords: Ankle; Osteochondral Lesions of the Talus; Lesions of Talus
Introduction/Purpose: Ankle injuries commonly result in damage to the articular cartilage of the talus. The use of cylindrical osteochondral allografts (OCA) for osteochondral lesions of the talus (OLT) smaller than 1.5cm is increasingly common, particularly in cases whereby autologous osteochondral transplantation (AOT) is contraindicated. The primary aim of this study is to systematically review the outcomes of cylindrical OCA for OLT. The secondary aim of this study is to compare the outcomes of cylindrical OCA and AOT in the management of similar cases of OLT.
Methods: Two independent reviewers searched the literature based on PRISMA guidelines, utilizing the EMBASE, MEDLINE, and The Cochrane Library Databases. Only studies that reported outcomes of cylindrical OCA in the management of OLT were included.
Results: Overall, 4 studies with 100 patients including 101 ankles were included in this review. Pre-operative OLT characteristics showed 69.3% of OLT lesions were located medially, with a mean lesion size of 1.47cm2 (0.46 - 4.2 cm2). Overall, 16.8% of ankles required surgical revision following cylindrical OCA; 1.0% (1/101) underwent subsequent arthrodesis, 6.9% (7/101) underwent revision osteochondral grafting and 7.9% (8/101) underwent subsequent arthroscopic debridement. Radiological outcomes between the graft failure were reported as 10.0% (3/30), joint space narrowing as 30.4% (14/46), and cysts as 42.9% (27/63). Significantly higher revision rates were reported following cylindrical OCA when compared to AOT at over two years follow up (28.1% versus 6.7%, p = 0.02).
Conclusion: Our systematic review established that although there are high rates of patient satisfaction following cylindrical OCA for OLT, these are less than those reported with AOT for the same condition. Concerns regarding the rates of radiological deterioration as well as the need for surgical revision may represent harbingers for poorer long-term outcomes.
DOI: 10.1177/2473011421S00101
Use of Extracellular Matrix Cartilage Allograft May Improve Infill of the Defects in Bone Marrow Stimulation for Osteochondral Lesions of the Talus
Mohammad Azam; Yoshiharu Shimozono, MD; Emilie Williamson, MD; Nathaniel P. Mercer; Eoghan T. Hurley, MB BCh BAO; Hao Huang; Timothy Deyer
John G. Kennedy, MD, FRCS(Orth)
Category: Ankle
Keywords: Ankle; Osteochondral Lesions of the Talus; Lesions of Talus
Introduction/Purpose: The purpose of this study is to evaluate the effectiveness of Extracellular Matrix Cartilage Allograft (EMCA) as an adjuvant to bone marrow stimulation (BMS) compared to BMS alone in the treatment of osteochondral lesions of the talus (OLT).
Methods: A retrospective cohort study comparing patients treated with BMS with EMCA (BMS-EMCA group) and BMS alone (BMS group) between 2013 and 2019 was undertaken. Clinical outcome was evaluated with the Foot and Ankle Outcome Score (FAOS) pre-and postoperatively. Postoperative MRIs were evaluated using a modified Magnetic Resonance Observation of Cartilage Tissue (MOCART) score. Comparisons between groups were made with the Man-Whitney U test for continuous variables and the χ2 or Fisher exact test for categorical variables.
Results: Twenty-four patients underwent BMS with EMCA (BMS-EMCA group) and 24 patients underwent BMS alone (BMS group). The mean age was 40.8 years (range, 19 to 60 years) in BMS-EMCA group and 47.8 years (range, 24 to 60 years) in BMS group (p=0.060). The mean follow-up time was 20.0 months (range, 12-36 months) in BMS-EMCA group and 26.9 months (range, 12 to 55 months) in BMS group (p=0.031). Both groups showed significant improvements in all FAOS subscales. No significant differences between groups were found in all postoperative FAOS. The mean MOCART score in BMS-EMCA group was higher (76.3 vs 66.3), but not statistically significant (p=0.176). The MRI analysis showed that 87.5% of BMS-EMCA group had complete infill of the defect with repair tissue, however less than half (46.5%) of BMS group had complete infill (p=0.015).
Conclusion: BMS with EMCA is an effective treatment strategy for the treatment of OLT and provides better cartilage infill in the defect on MRI. However, this did not translate to improved functional outcomes compared with BMS alone in the short-term.
DOI: 10.1177/2473011421S00102
Influence of Local Chemokine Delivery and Postoperative Peripheral Blood Mobilization on Achilles Tendon Repair
Kevin C. Baker, PhD; Erin A. Baker, PhD; Paul T. Fortin, MD; Zachary M. Vaupel, MD; Bo N. Loy, MD
Introduction/Purpose: Mesenchymal stem cells (MSCs) have demonstrated promise in augmenting the surgical repair of full thickness tendon tears. Despite this promise, obtaining a therapeutic concentration of MSCs is time-, labor- and resource intensive, and is subject to ever-tightening governmental regulations. Our group recently demonstrated that postoperative mobilization of MSCs from the marrow compartment and into peripheral blood via subcutaneous granulocyte- colony stimulating factor administration enhanced tendon-bone healing in a rat model of surgical repair of a full-thickness supraspinatus tendon tear. We hypothesized that combining postoperative stem cell mobilization with local delivery of a chemokine that stimulates MSC chemotaxis would enhance the surgical repair of a mid-substance Achilles tendon transection.
Methods: Following IACUC approval, Achilles tendons were unilaterally frayed via multiple longitudinal scalpel blade nicks in 24 Lewis rats. Tendons were then surgically transected, followed by repair with braided non-absorbable suture in a modified-Kessler pattern. Based on randomization (n=6/group), the tendon anastomosis was coated with a resorbable chitosan hydrogel containing 100 ng of the chemokine, CCL5 (RANTES), or hydrogel without RANTES. Skin closure and anesthesia recovery were then performed; rats were allowed ad libitum activity. Beginning 24 hours postoperatively, rats received a daily subcutaneous injection of either a peripheral blood mobilizing agent, AMD3100 (5 mg/kg), or saline; dosing was repeated at 48 and 72 hours. At the 4- week endpoint, Achilles tendons harvested en bloc. Decalcified histologic sections were stained with H&E and Alcian Blue as well as immunostained for Collagen III, CD163, and CD68. Slides were digitized (40x magnification) and graded by blinded reviewers via modified-Bonar score to assess tendon integrity.
Results: Rats that received local application of RANTES-loaded chitosan hydrogel had worse (higher) modified-Bonar subscores with respect to tenocyte morphology, collagen orientation, and ground substance staining, though none of these comparisons were statistically significant (p=0.068, p=0.672, and p=0.407, respectively). Animals that received subcutaneous AMD3100 alone, or in conjunction with RANTES-loaded chitosan hydrogel displayed the best (lowest) total modified Bonar scores, though these comparisons were also not statistically significant (p = 0.498). No significant differences were found with respect to CD163 (p=0.132) and CD68 (p=0.104) staining. Despite a lack of statistical significance, animals that received AMD3100 displayed a higher number of both macrophage subtypes. No differences were found with respect to Collagen III immunostaining (p=0.808).
Conclusion: Tendon repair and regeneration remains a significant clinical challenge, which may be aided by MSC transplantation. The mobilization of endogenous marrow-derived MSCs into peripheral blood and subsequent recruitment via local chemokine delivery may be an efficacious way to enhance tendon repair without the need for ex vivo processing. We failed to demonstrate significant effects of stem cell mobilization via AMD3100 injections, and chemokine-directed recruitment, though trends were present indicating that AMD3100 alone may be beneficial. Additional work is required to draw any translatable conclusions from this research.
DOI: 10.1177/2473011421S00103
Analysis of Complications Following Distal Ankle Nerve Blocks for Foot and Ankle Procedures
Ania Bartholomew; Tyler Slone; Michael Ciesa; Nicholas A. Cheney, DO; Brian C. Clark
Category: Ankle; Arthroscopy; Bunion; Hindfoot; Midfoot/Forefoot; Other
Keywords: Ankle Block; Complications; Foot and Ankle Instability (Ligament Injuries)
Introduction/Purpose: Popliteal nerve blocks are a common procedure employed by anesthesiologists to augment intraoperative anesthesia and provide postoperative pain control. Unfortunately, these can be associated with unintended complications including pain, numbness, and foot drop, sometimes without clear resolution. Studies from Kahn (2017), Anderson (2015), Park (2018), Lauf (2020) suggest complications higher than previously reported with Lauf (2020) finding short-term complication rates of 10.1% and 4.1% long-term as confirmed by EMG. Our study looked to address the complication rates from an alternative anesthetic procedure, a distal ankle nerve block involving anesthesia to the five nerve(s) more intimately involved in the surgical procedure. This alternative technique may provide equivalent anesthetic properties and pain relief as popliteal blocks, with fewer complications for many patients across various demographics.
Methods: We retrospectively reviewed patient charts and messaging from 2019 to 2021 that received a distal ankle field block for various surgical procedures including ankle arthroscopy, ankle fractures, and lateral ankle stabilizations. The five nerves anesthetized in the distal ankle nerve block included the tibial, superficial and deep peroneal, sural, and saphenous. Thus far, 61 surgeries have been reviewed and analyzed for neuropathic complications and confirmed via EMG.
Results: Of the 61 patients analyzed, 3 patients were found to have a superficial peroneal neuropathy that included dorsal numbness as a result of the distal ankle block, resulting in a 4.92% complication rate. 1 patient required a rescue block to be performed postoperatively for pain. The remaining 57 patients recovered appropriately and without complications. No motor complications have been found from patients receiving distal ankle nerve blocks, as performed by the senior author.
Conclusion: With the absence of motor complications and markedly reduced incidence of sensory complications, distal ankle nerve blocks may be a beneficial alternative to popliteal nerve blocks for various foot and ankle orthopedic surgeries. As motor complications can result in life-altering disability, an anesthetic procedure with reduced negative motor outcomes can improve surgery and recovery prognosis. Future directions for this study include adding more patients to increase the sample size, as well as continuing to follow current patients, monitoring symptoms or complications.
DOI: 10.1177/2473011421S00104
Intramedullary Nailing vs Plating of the Fibula for Ankle Fractures in the Young Active Patient
Gonzalo F. Bastias, MD; Natalio R. Cuchacovich Mikenberg, MD; Felipe G. Diaz; Paulina Gutierrez, MD; Gerardo Munoz, CAE; Rodrigo Melo, MD; Magdalena I. Jofre; Jorge Filippi, MD, MBA
Category: Ankle; Trauma
Keywords: Ankle Fracture; Clinical Outcomes; Intramedular Fibular Nail
Introduction/Purpose: The use of fibular nailing (FN) for fixation of lateral malleolar fractures has been rising in recent years. Currently, it has been validated as an effective minimally invasive approach to ankle fractures specially in patients with high risk of wound dehiscence, diabetics and elderly low-demand patients. While most of the studies comparing the use of a fibula nail versus plating (PL) are carried out in this population at risk, the use of FN in younger patients with higher functional demands has been hardly studied. The aim of this study is to compare the functional and quality of life outcomes of patients treated with FN and PL in an active population.
Methods: We performed an IRB-approved retrospective study including ankle fractures treated in our hospital from January 2017 to February 2020, with a minimum followup of one year. We included only patients between 18 and 55 years old treated by five fellowship-trained foot and ankle surgeons and divided into two groups according to the method of fixation of the fibula: intramedullary nailing (FN) or plating (PL). Demographics, medical comorbidities, type of fracture, reoperations and complications were collected. Functional and clinical evaluation included the Lower Extremity Functional Score (LEFS) and Short form 12 (SF 12) were obtained at an average of 28 months follow-up (range 14-50).
Results: Eighty-five patients were included in this study with a mean age of 36.9 years old (range 16-55). The FN group was conformed by 31 patients (18 men) while the PL group consisted of 54 patients (32 men). Both groups were comparable in terms of age, sex, type of fracture, open fractures, number of malleoli compromised (P>0.05). Union was achieved in all patients. The complication rate was 3.2% (1 patient) in the FN group versus 5,5% (3 patients) in the PL group (p=0.66). Two patients (6.5%) in the FN group and 7 patients (13%) in the PL group required hardware removal (p=0.36). There were no significant differences in SF-12 physical component (p=0.30), SF-12 Mental component (p=0.52) and LEFS Score (p=0.88).
Conclusion: In this comparative study, there were no differences between the FN and PL groups for fixation of the fibula in terms of functional results and quality of life at an average of 28 months follow-up. Complications and hardware removal rates had no statistical differences between both groups. This is the first report on the literature comparing both fixation strategies on an active high-demand population.
DOI: 10.1177/2473011421S00105
Learning Curve for Fixation of the Posterior Malleolus in Trimalleolar Ankle Fractures Through A Posterolateral Approach
Gonzalo F. Bastias, MD; Juan P. Bergeret, MD; Jose M. Rojas Fuentes, MD; Victor M. Barrientos; Rodrigo Jose Gutierrez Boris; Bastian A. Leonart Correa, MD; Patricio A. Fuentes
Introduction/Purpose: Fractures of the posterior malleolus (PM) are present in 7-44% of all ankle fractures. Controversy exists referring to the optimal strategy for the fixation of these fractures. The anatomical reduction of the PM has been related to better functional outcomes and lower rates of posttraumatic osteoarthritis. The posterolateral (PL) approach has proven useful for obtaining an accurate reduction of the articular step-off and remotion of intraarticular fragments that may interfere with the reduction. Common reported complications are wound dehiscence, sural nerve injuries and persistent intraarticular step-off of the PM. There have been no previous reports on the literature regarding the learning curve (LC) of this approach. The aim of this study was to assess the LC of performing a PLA by orthopedic surgeons.
Methods: A retrospective study was performed including patients with posterior malleolar fractures treated by eight orthopedic foot and ankle surgeons between 2012 and 2018 in a Level-I trauma center. Open reduction and internal fixation using a PL approach was used in all patients. Demographic data, fracture pattern and approach-related complications were noted. Anatomical reduction or persistent step-off and of the PM was assessed with postoperative CT-Scan. The LC-CUSUM (Learning Curve - Cumulative Sum) quantitative assessment was used to evaluate the learning curve in terms of approach-related complications and quality of reduction. Based on the acceptable failure rate was defined by less than 10% of approach-related complications and less than 15% of patients with postoperative step-off greater than 1 mm.
Results: We included 167 patients with a mean age of 47 years old (R22 - 75). PM morphology was classified according to Haraguchi being I:52.1%, II:46.1% and III:1.8%. Mean size of the PM was 29.8% (R13 - 58). The overall approach-related complications incidence was 10.2 % being the most frequent: wound complications and sural nerve paresthesias. Persistent step-off >1 mm was present in 23 patients (13.8%) on CT-Scan. LC-CUSUM score peaked at the 31st case for significant reduction of approach-related complications. There was a decrease in the incidence of approach-related complications from 19.4% in the first 31 cases and 8,1% in cases 32nd-167th. There was a significant reduction of persistent step-off >1 mm with the LC-CUSUM score peaking after the 28th case. This manifests in a decrease from 21.4% incidence in the first 28 cases versus 12.2% in cases 28th- 167th.
Conclusion: The learning curve for fixation of PM fractures using a PL approach, as indicated by a cumulative sum quantitative assessment, corresponds to 31 cases for achieving success in terms of approach-related complications and 28 cases for an acceptable quality of reduction. These results are useful for novice trainees in this approach for defining a point of competence and assess the feasibility to achieve expertise in centers with lower caseloads of PM fractures.
DOI: 10.1177/2473011421S00106
Percutaneous Modified Lapidus Procedure with Early Weightbearing: Technique and Early Outcomes of the First 30 Cases
Bryan Bean, MD; Devin R. Mangold, MD; Mostafa Abousayed, MD, MSc; Michelle M. Coleman, MD, PhD; John Thompson, MD; Gregory P. Guyton, MD
Introduction/Purpose: Minimally invasive techniques (MIS) have focused on first metatarsal osteotomies in hallux valgus correction. Concurrently, new fixation methods allow early weightbearing protocols with the open Lapidus procedure, with nonunion rates comparable to those of more traditional protocols requiring nonweightbearing. We aimed to assess clinical and radiographic results of an MIS-modified Lapidus technique with axial nail fixation (Phantom Lapidus Intramedullary Nail: Paragon28, Englewood, CO USA) and early weightbearing.
Methods: After institutional review board approval, the first 30 consecutive percutaneous MIS-modified Lapidus procedures by a single surgeon were retrospectively reviewed. Indications for surgery included moderate to severe hallux valgus deformity with or without first tarsometatarsal joint (TMT) instability, first TMT arthritis, adolescent bunion, and failed prior surgery. All patients initiated weightbearing within 12 days and returned to regular footwear by 6 weeks postoperatively. Patients had a minimum follow-up period of 3 months (average 8.3 months). The pre- and postoperative visual analog scale (VAS) pain scores, intra- and postoperative complications, and need for revision surgery were recorded. Pre- and postoperative radiographs were used to evaluate the hallux valgus angle (HVA), 1-2 intermetatarsal angle (IMA), and sesamoid station. Postoperative radiographs were evaluated for signs of hardware loosening and union of the first TMT arthrodesis site. A postoperative CT scan was obtained if nonunion was suspected.
Results: Thirty consecutive percutaneous modified Lapidus procedures were performed in 28 patients. VAS scores improved from 4.1 preoperatively to 1.8 at final follow-up. The IMA decreased 8.3 degrees to an average of 5.9 degrees. The HVA decreased 19.2 degrees to 11.7 degrees. The medial column was shortened by 0.6%. There were no intraoperative complications. There were two reoperations, including one nonunion requiring revision first TMT fusion with autograft and one hallux valgus recurrence requiring a distal chevron osteotomy. There were no wound complications, surgical site infections, hardware complications, postoperative transfer metatarsalgia, or nerve-related problems.
Conclusion: The current study provides clinical evidence that the intramedullary nail is a biomechanically stable construct evidenced by the high union rate, lack of hardware failure, and tolerance for early weightbearing. This percutaneous modified Lapidus technique may allow for a low rate of wound complications, accelerated rehabilitaion, and improved cosmesis.
DOI: 10.1177/2473011421S00107
Modified Brostrom with and without Suture Tape Augmentation: A Systematic Review
Michael D. Bedrin; Andres S. Piscoya; Alexander Lundy; Tobin T. Eckel, MD
Introduction/Purpose: The Modified Brostrom (MB) has become the gold standard for operative management of chronic lateral ankle instability. Despite overall good clinical outcomes with this procedure, recent biomechanical data has called into question the strength and durability of this technique. Accordingly, the addition of suture tape to the MB construct has been described in an attempt to more closely recreate the natural biomechanical properties of the ankle lateral ligament complex. Despite its increasing popularity, the Modified Brostrom with suture tape augmentation (MBA) remains controversial due to a lack of clinical data. The purpose of this study is to determine the differences in clinical outcomes of MB compared to MBA.
Methods: A systematic review of the literature was performed using PubMed, Embase, and CINAHL to identify English-language articles from 2009 - present discussing outcomes with the MBA technique. Total number of patients, patient demographics, follow-up time, subjective and objective outcome measures, return to sport, recurrent instability, and complications were evaluated.
Results: A total of 4 studies (2 retrospective cohort studies, 2 case series) involving 156 patients with MBA met inclusion criteria. Average follow-up time was 13.8 months. Of the 3 studies reporting patient-reported outcome measures both pre-and post- operatively, there was a significant improvement in all measures (p<0.05). Two studies compared MB directly to MBA, one of which found a statistically significant difference in the Foot and Ankle Ability Measure (FAAM) in favor of the MBA (93.1 vs 90.5, p=0.027), while American Orthopaedic Foot & Ankle Society (AOFAS) score was not significantly different (p>0.05) between MB and MBA across studies. One study reported a significantly greater rate of return to sport at 12 weeks in the MBA group versus the MB (82% vs 27%, p<.001). There were no significant differences in complications between MB and MBA.
Conclusion: MBA for chronic lateral ankle instability can produce good short-term clinical outcomes with few complications, comparable to MB. The overall quality of evidence is low, and long-term, prospective, head-to-head comparison data will be needed to determine the clinical efficacy, complication profile, and cost-benefit relationship of the MBA technique as it compares to the MB.
DOI: 10.1177/2473011421S00108
Accuracy of Weightbearing CT vs Non-Weightbearing CT Scans for Patient-Specific Instrumentation in Total Ankle Arthroplasty
Gregory C. Berlet, MD; Antonio M. Malloy McCoy; Devon Consul, DPM; Benjamin D. Umbel, DO; Mitchell Thompson
Category: Ankle
Keywords: Weight Bearing CT; Total Ankle Arthroplasty; Ankle
Introduction/Purpose: Total ankle arthroplasty (TAA) is a popular and viable option for end stage ankle arthritis. Accuracy and reproducibility in placing the implant on the mechanical axis has been shown to be paramount in total ankle replacement. Patient specific pre-operative navigation up until this past year has been based off of non-weightbearing computerized tomography (CT). Our institution has created a protocol to use weightbearing CT in the pre-operative patient specific navigation for TAA using the ProphecyTM system. The purpose of our study was to compare the accuracy and reproducibility of implant alignment and size using WBCT versus prior studies using NWBCT for the Prophecy reports.
Methods: Patients who underwent TAA using our WBCT protocol for their Prophecy scans had their charts reviewed to see if they met the proper inclusion criteria. Inclusion criteria was a primary TAA with proper follow-up to have first post-operative weightbearing radiographs. The first post-operative weightbearing radiographs were used to measure alignment of the axis of the implant in frontal and sagittal planes comparative to the tibial axis. These results were then compared to the pre-operative prophecy scans to determine reproducibility. The size of the implants components were also recorded for each patient and compared to the pre-operative predicted implant sizes from the patient specific reports. Our results were also compared to previous studies on reproducibility of patient specific navigation when using non-weightbearing CT.
Results: Ten patients met our inclusion criteria of WBCT ProphecyTM preoperative planning. 100% of the TAA were within the intended target of less than 50 varus or valgus. The average post-operative coronal alignment was an average of 0.844 degrees. Average sagittal plane deformity was 1.88 degrees post-operative. Tibial component size was properly predicted 100% of the time and talar component in all but one patient.
Conclusion: This data supports superior accuracy and reproducibility in pre-operative patient specific navigation when utilizing WBCT for TAA vs published controls with non-weightbearing CT.
Gregory C. Berlet, MD; Mark A. Prissel, DPM; Emily E. Zulauf; Antonio M. Malloy McCoy
Category: Ankle; Ankle
Keywords: Ankle Arthrodesis; Ankle; Fusion
Introduction/Purpose: Ankle arthrodesis is a time-tested surgical treatment for end-stage ankle arthritis. Fixation constructs continue to evolve with recent advancements in anterior ankle plating. A systematic review of anterior approach ankle arthrodesis using anterior plating was performed to analyze outcomes such as time to weight bearing, union rate, and complications.
Methods: A systematic literature search was performed following Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) guidelines was performed. Inclusion criteria were as follows: 1) prospective or retrospective comparative study or consecutive case series reporting clinical outcomes following ankle arthrodesis; 2) surgeon technique includes anterior incisional approach with anterior plating construct; 3) minimum 3 months follow-up; and 4) reported outcomes including time to weight bearing, union or nonunion rate, complications, and patient population characteristics including age and comorbidities. Thirteen citations met inclusion criteria. Studies were organized into three groups based on similar time to weightbearing protocols.
Results: Mean time to weightbearing was as follows: Group A. 0.6 weeks, Group B. 6 weeks, and Group C. 9 weeks with fusion rates of 95.2%, 95.4%, and 96.6%, respectively. The average time to weightbearing post-operation across all groups was 4.6 weeks with a mean union rate of 95.3% (82 to 100%).
Conclusion: Wound healing complications and infection rates did not increase with earlier weight bearing guidelines. This systemic review revealed comparable fusion rates across different weight bearing regimens following anterior plate fixation for ankle arthrodesis, supporting re-evaluation of historically accepted weightbearing protocols.
DOI: 10.1177/2473011421S00110
Maintenance of First Ray Length after First Metatarsophalangeal Joint Distraction Arthrodesis Using Allograft Discs: A Statistical Analysis
Gregory C. Berlet, MD; Antonio M. Malloy McCoy; Mitchell Thompson; Devon Consul, DPM; Mark A. Prissel, DPM
Category: Midfoot/Forefoot
Keywords: 1st MTP Joint; Arthrodesis; First Metatarsophalangeal Joint Arthrodesis
Introduction/Purpose: The first metatarsophalangeal joint (MTPJ) is one of the most common locations for arthritis in the foot. When conservative methods fail, two main surgical treatment options exist, fusion or joint implant. For various reasons these surgeries can fail leaving relatively few salvage options. A common salvage option is the first MTPJ distraction arthrodesis. Use of allograft discs to decrease surgical time and donor site morbidity has become an increasingly popular option for MTP distraction arthrodesis. The purpose of this study was to look at the maintenance of the first ray length in first MTPJ distraction arthrodesis using allograft discs.
Methods: We reviewed 14 patients who underwent first MTPJ distraction arthrodesis, measuring first ray length at the first post- operative weightbearing radiograph and most recent weightbearing radiograph. Average follow up was 12.75 months between radiographs.
Results: Average shortening was 3 mm on the lateral measurements and 2.3 mm on the AP measurements. CT verified overall nonunion rate was 43% whereas, symptomatic nonunion rate was 21%.
Conclusion: Amount of shortening and graft size did appear to have a positive correlation. Union rate did not affect shortening of first ray, but revision for a failed implant arthroplasty did correlate with increased shortening compared to revision for a failed first MTPJ fusion. Our data suggests a 2-3 mm shortening of the first ray can be predicted over the first 12 months after a first MTPJ distraction arthrodesis using allograft discs. Longer term studies with larger patient populations, and a comparative study to cortical autograft would provide more accurate insight to outcomes of first MTPJ distraction arthrodesis.
DOI: 10.1177/2473011421S00111
Bosch Osteotomy for Hallux Valgus Correction: Results at a Mean 10-Year Follow-Up
Alessio Bernasconi, MD PhD FEBOT; Maria Rizzo; Anna Paola Russo; Salvatore Vallefuoco, MD; Amedeo Guarino; Massimo Mariconda
Category: Bunion; Midfoot/Forefoot
Keywords: Bunion; Hallux Valgus; Bunionectomy
Introduction/Purpose: Boesh osteotomy (BO) is a surgical option for the correction of hallux valgus (HV). The aim of this study was to assess the long-term clinical and radiographic results in a cohort of patients treated at our institution.
Methods: In this retrospective cohort study, we included 58 HVs (28 right, 30 left) in 46 patients (42 females, 4 males; mean age and BMI at surgery 44 +- 15 (range, 15-64) years and 26 +- 4 (range, 22-38) points, respectively) who underwent HV correction by BO and were followed at a minimum of 7 years. The range of motion (ROM), the American Orthopaedic Foot & Ankle Society’s Forefoot scale (AOFAS-FS) and the Visual Analogic Scale (VAS) for pain were recorded. On weightbearing radiographs, the Hallux Valgus Angle (HVA), Intermetatarsal Angle (IMA), the Distal Metatarsal Articular Angle (DMAA) and the Sesamoid position were measured and compared with pre-operative values. The complication rate and first metatarsophalangeal joint stiffness were also assessed.
Results: At a mean follow-up of 10+-2 (range, 7-17) years, mean+-standard deviation AOFAS-FS and VAS were 89+-11 (range, 67-93) and 2.1+-2.8 (range, 0-7) points, respectively. In 62% of patients there was no pain while in 38% an occasional pain was referred. In 42 (72%) cases there was no limitation in the choice of footwears. Radiographically, we found a significant improvement in the HVA (from 33.9°+-6.7 to 18.8°+-5.6, p<0.001), in the IMA (14.2°+-3.1 to 9.4°+-2.7, p<0.001), in the DMAA (from 30.3°+-6.8 to 11.5°+-5.1, p<0.001) and in the sesamoid position (median value from 3 to 1, p<0.001). In 36 (62%) cases the ROM was greater than 75° while in 22 (38%) it ranged between 30° and 75°. Complications occurred in 6 (10%) cases (3 superficial infections, 1 accidental removal of the K-wire, 1 metatarsal head necrosis and 1 development of osteoarthritis), which did not require any surgery at the longest follow-up.
Conclusion: Boesh technique provided satisfactory clinical and radiographic outcomes in the correction of Hallux Valgus which persisted at a mean 10-year follow-up. The complication rate was not different from more recent techniques described in literature.
DOI: 10.1177/2473011421S00112
Static vs Dynamic Fixation of Distal Tibiofibular Syndesmosis: A Review of Overlapping Meta-Analyses
Alessio Bernasconi, MD, PhD, FEBOT; Domenico Marasco, MD; Jacopo Russo, MD; Antonio Izzo, MD; Salvatore Vallefuoco, MD; Francesco Coppola, MD; Giovanni Balato, MD, PhD; Francesco Smeraglia, MD, PhD; Francois Lintz, MD MSc FEBOT; Shelain Patel, FRCS
Introduction/Purpose: Multiple Level I meta-analyses have been led comparing traditional static vs. more recently-introduced dynamic strategies of fixation for injuries of the distal tibiofibular syndesmosis (TFS). The aim of this review was to assess their robustness and methodological quality, providing support in the choice of a treatment strategy in case of TFS injury using the highest level of evidence.
Methods: In this systematic review, conducted in accordance with the PRISMA guidelines, we identified meta-analyses/systematic reviews comparing static and dynamic fixation methods after acute TFS injury. Robustness of studies was evaluated using the Fragility Index (FI) for meta-analysis and the Fragility Quotient (FQ). The risk of bias was evaluated using the Assessment of Multiple Systematic Reviews(AMSTAR) instrument. Finally, the Jadad Decision Algorithm was applied to select the study which provided the highest quality of evidence to develop recommendations for the fixation strategy of these lesions.
Results: Out of 1302 records, 4 Level I meta-analyses were included in this study. Analyzing the statistically significant dichotomous outcomes, the median FI was 3.5 (IQR, 2 to 5.5; range, 1 to 9) while the median FQ was 1.9% (IQR, 1 to 3.5; range 0.35 to 4.4). In total, 37% had a FI of 2 or less and 75% of outcomes had a FI of 4 or less. According to the AMSTAR score and Jadad algorithm, the largest meta-analysis was selected as the highest evidence provided so far.
Conclusion: We selected the meta-analysis by Grassi et al. as the highest quality provided so far, which found that dynamic fixation reduced complication rates and improved clinical outcomes compared to static methods of fixation. We demonstrated that meta-analyses with statistically significant dichotomous outcomes comparing dynamic and static fixation for treating injuries of the distal tibiofibular syndesmosis are fragile, with a change in less than 4 patients or less than 2% of the study population sufficient to reverse a significant outcome to nonsignificant. Based on these findings, we recommend caution when interpreting the results of these studies.
DOI: 10.1177/2473011421S00113
Weightbearing CT Assessment of Foot and Ankle Joints in Pes Planovalgus Using Distance Mapping
Alessio Bernasconi, MD PhD FEBOT; Cesar de Cesar Netto, MD, PhD; Sorin Siegler, PhD; Maui Jepsen, BSc; Francois Lintz, MD MSc FEBOT
Introduction/Purpose: The goal of this study was to describe the abnormal joint surface interaction at the ankle, hindfoot and midfoot joints in patients presenting with Pes Planovalgus (PP) using three-dimensional (3D) distance mapping on weightbearing computed tomography (WBCT) images by comparing a series of PPs to a series of normally-aligned feet. We hypothesized that in PPs joint interactions would reveal significantly increased spaces in the medial side of the ankle, hindfoot and midfoot joints.
Methods: In this case-control study, ten feet (10 patients) with asymptomatic PP (cases; N=10) were compared to 10 matched- paired (by age, gender and body mass index) normally-aligned feet (10 patients) (controls; N=10). Three-dimensional models were produced from the images and distance maps representing joint surface configuration were generated for the ankle, hindfoot and midfoot joints. The distance maps for each joint were then compared between the two groups and between regions in the same group.
Results: In PP patients there was a significantly increased surface-to-surface distance anteromedially at the ankle joint (+46.3%, p<0.001) along with an increased distance on the anterior halves of both the medial (+21.3%, p=0.098) and lateral malleoli (+22.7%, p=0.038). At the posterolateral corner of the posterior facet of the subtalar joint we found an increased surface-to- surface distance (by 57.1%, p< 0.001), while at the talonavicular joint there was a reduction of the distance at the superomedial corner (-20%, p=0.097) along with a significant increase in the upper central (+20%, p=0.039) and lateral (+30.7%, p=0.015) zones. A reduction of the surface-to-surface distance was also observed in three of the four zones of the calcaneocuboid joint. Finally, a statistically significant increase in the mean distance was observed at the naviculocuneiform and tarsometatarsal joints in a range between 38% and 93.4% (p<0.001 in all cases).
Conclusion: We found significant differences in surface-to-surface interaction at the foot and ankle joints between Pes Planovalgus and normally-aligned controls. Distance mapping on WBCT images could be used in clinical practice as a diagnostic support to gauge the morphological changes of articular spaces occurring in Pes Planovalgus.
DOI: 10.1177/2473011421S00114
Cost-Effectiveness of Weight-Bearing Computed Tomography in Diagnosing Syndesmotic Instability
Rohan Bhimani, MD, MBA; Owen F. Searle; Soheil Ashkani-Esfahani, MD; Gregory R. Waryasz, MD; Gino Kerkhoffs, MD; Christopher W. DiGiovanni, MD; Daniel Guss, MD, MBA; Bart Lubberts, MD, PhD
Introduction/Purpose: To optimize clinical outcomes, accurate diagnosis and treatment of syndesmotic instability is critical, but subtle instability can be challenging to identify. Weightbearing computed tomography (WBCT) has proved to be a reliable tool for diagnosing syndesmotic instability under physiologic load. We aimed to examine the cost-effectiveness of WBCT with radiographs and/or conventional CT for the diagnosis of syndesmotic instability from a patient perspective.
Methods: A decision tree model was constructed to examine the cost-effectiveness of WBCT versus conventional CT (NWB CT) versus weightbearing (WB) radiographs versus non-weightbearing (NWB) radiographs (base case) as initial imaging with additional possible imaging for1268 patients with suspected syndesmotic instability. Patient’s clinical and radiological notes were evaluated until the diagnosis of syndesmotic instability was established. The decision tree’s probabilities, durations, and image counts were based on patient data. The main outcomes were 1) total imaging costs needed before syndesmotic instability was diagnosed, 2) quality-adjusted life-years (QALYs), 3) incremental cost-effectiveness ratios (ICERs), and 4) overall radiation dose prior to diagnosis. Imaging costs and radiation dose were derived from National Medicare reimbursement rates and the American College of Radiology, respectively. An incremental cost-effectiveness ratio threshold of $50,000 per quality-adjusted life years was used to evaluate cost-effectiveness. In addition, one-way and two-way sensitivity analyses were performed to determine the robustness of our findings.
Results: WBCT resulted in 0.057 additional QALY gained per week compared with NWB radiographs, indicating WBCT to be more effective than NWB radiographs. Costs for WBCT imaging were $38.71 higher than NWB radiographs for an ICER of $38,563.96/QALY. Applying a commonly used threshold of $50,000 per QALY, the patient’s willingness-to-pay for the amount of quality-adjusted life-year gained from using WBCT as an initial imaging modality was $54.41, suggesting WBCT first imaging strategy was a cost-effective intervention. In our study, the cost of WBCT imaging was $157.35. Sensitivity analyses demonstrated that WBCT was more cost effective than NWB radiographs up to a cost of $173.05. Additionally, initial WBCT resulted in lower overall radiation dosage (6.4 uSv) compared to the use of the other three imaging modalities as initial imaging strategy (initial NWB radiographs - 12.41 uSv; initial WB radiographs - 8.30 uSv, NWB CT first - 25 uSv).
Conclusion: WBCT leads to higher QALYs compared to other diagnostic imaging modalities, resulting in improved outcomes for patients by eliminating redundant imaging.
DOI: 10.1177/2473011421S00115
Defining Reference Values for the Anatomical Axis of Syndesmosis and Landmark for the Clamp Placement to Minimize Malreduction
Rohan Bhimani, MD, MBA; Soheil Ashkani-Esfahani, MD; Bart Lubberts, MD, PhD; Daniel Guss, MD, MBA; Gino Kerkhoffs, MD; Christopher W. DiGiovanni, MD; Gregory R. Waryasz, MD
Introduction/Purpose: Malreduction of the fibula within the incisura is often caused by an eccentric clamp or screw placement and short fibular length. Weightbearing computed tomography (WBCT) has proven to be a reliable method to diagnose syndesmotic instability and can be used as a template to determine the syndesmotic axis and optimal position to place the clamp. We aimed to determine the anatomic axis of the syndesmosis, or the trans-syndesmotic angle (TSA) in healthy individuals on WBCT, and to see if side-to-side and gender based variations exist. We also aimed to determine the clamp’s medial tine placement along the trans-syndesmotic axis.
Methods: The study group was made up of patient population without ankle injury who underwent bilateral foot and ankle WBCT imaging (n = 100; 200 ankles). Measurements on bilateral WBCT images included: 1) TSA at 1cm, 2cm, and 3cm proximal to tibial plafond, respectively; 2) Medial tine of the clamp positioning at 1cm and 2 cm along the syndesmotic axis. The medial tine clamp position was described in terms of the percentage of anterior to posterior tibial diameter from the anterior cortical boundary. In addition, the aforementioned TSA measurements were compared to historically defined 30 degrees of syndesmotic axis. Paired t-test was used to compare side to side and gender based differences. A p-value < 0.05 was considered statistically significant.
Results: In the uninjured healthy population, the mean trans-syndesmotic angles were 17.60, 21.60, and 24.10 at 1cm, 2cm, and 3cm proximal to the tibial plafond respectively. The clamp’s medial tine should be positioned 24.7% and 21.3% of the AP tibial cortical distance, posterior to the anterior tibial cortex at 1cm and 2 cm proximal to the tibial plafond. There was no significant side to side or gender based differences for any of the measurements. Additionally, all three weightbearing TSA measurements were significantly larger than the historically defined syndesmotic angle of 30 degrees (p<0.001).
Conclusion: Preoperative WBCT imaging provides a reliable template to determine TSA and to plan optimal clamp tine positioning along the syndesmotic axis. Our study has established normal ranges for cross-sectional syndesmotic axis measurements during weight-bearing and established that no differences exist between laterality and gender in patients without syndesmotic injury.
DOI: 10.1177/2473011421S00116
The Lateral Hook Test: What is the Amount of Force that Should Be Applied to Evaluate Syndesmotic Instability Using Arthroscopy?
Rohan Bhimani, MD, MBA; Bart Lubberts, MD, PhD; Noortje Hagemeijer, MD; John Z. Zhao, MD; Jirawat Saengsin, MD; Go Sato, MD; Gregory R. Waryasz, MD; Christopher W. DiGiovanni, MD; Daniel Guss, MD, MBA
Introduction/Purpose: The lateral hook test is considered the gold standard for the diagnosis of coronal plane syndesmotic instability during arthroscopy. The amount of distal tibiofibular space is directly related to the amount of lateral directed applied force. This study aims to determine the optimal amount of forced needed during a lateral hook test to evaluate syndesmotic instability in the coronal plane. The secondary aim was to determine the amount of displacement variation that occurs when the lateral force is angled anteriorly or posteriorly.
Methods: Ten fresh-frozen above-knee amputated cadaveric specimens underwent arthroscopic evaluation of the distal tibiofibular joint. The assessment was done first with all syndesmotic and ankle ligaments intact and subsequently with transection of the anterior inferior tibiofibular ligament (AITFL) and the interosseous ligament (IOL). In all scenarios, a lateral hook test was performed under increasing force from 0N to 120N of direct force, with increments of 20N. The lateral hook test was performed in: 1) the neutral position (no angulation), 2) anterior inclination of 15 degrees, and 3) posterior inclination of 15 degrees under the aforementioned force. Anterior and posterior coronal plane distal tibiofibular space were arthroscopically measured. Descriptive statistics were employed to determine the force and the most sensitive method to pull during arthroscopic evaluation to detect syndesmotic instability.
Results: Among the specimens, after transection of AITFL and IOL, the anterior and posterior coronal plane space increased with increment in force until 60N and then displayed no change in these measurements despite the increase in force. In the intact state, there was an increase in syndesmosis coronal space with increase in force. Of the three methods of force application, the posteriorly directed force has the largest absolute value for the anterior and posterior coronal space, suggesting it is the most sensitive in distinguishing between stable and unstable syndesmotic injury.
Conclusion: Arthroscopic coronal plane evaluation under 60N of direct force is best suited to distinguish stable from an unstable syndesmosis. Syndesmosis anterior and posterior coronal plane space measurement demonstrate the largest absolute difference when subjected to posteriorly directed force, suggesting that this new method of assessment has the highest potential for diagnosing even subtle syndesmotic instability, along with a lower propensity for error.
DOI: 10.1177/2473011421S00117
Allograft Reconstruction for Unsalvageable and Recurrent Tears of Both Peroneal Tendons
Daniel D. Bohl; James W. Brodsky, MD; Lincoln Dutcher
Introduction/Purpose: Surgical reconstruction for the complete loss of both peroneal tendons is challenging, with no established standard. This is true both for concomitant tears that extend superior to the superior peroneal retinaculum, and for nonfunctioning, unsalvageable peroneal tendons after prior repair or reconstruction, which have recurrent tears, tendon degeneration, scarring, and stretching. These cases have in common that there is no option for retention of the native tendons. Allograft reconstruction can bridge long defects, reestablishing the insertion of the proximal musculo-tendinous unit to the lateral foot. However, there are limited published data on allograft reconstruction, and series are small and heterogenous. This study reports the results of allograft reconstruction at a mean of 4.1 years follow-up (range 1.5-7.3 years).
Methods: A retrospective study reviewed patients who had allograft reconstruction for unsalvageable or recurrent tears of both the peroneus brevis and peroneus longus tendons. In all cases, the unsalvageable segments of both peroneal tendons were excised. A hamstring allograft tendon with width of >6mm was pre-stretched, then anchored to the proximal 5thmetatarsal, and also sutured to itself and the adjacent brevis stump, if viable. The peroneal retinaculae were reconstructed over the allograft tendon. The peroneal muscle-proximal tendon units were extensively stretched inferiorly using suture loops in the tendons. They were maximally tensioned and anastomosed to the maximally tensioned allograft while holding the hindfoot in maximum eversion. Of the 14 eligible patients, 13 had minimum one-year follow-up and constituted the study population. Mean age was 50.7 years (range 26.3-68.6 years). Ten patients had at least one prior peroneal tendon surgery; four patients had at least two.
Results: At mean follow-up of 4.1-years, seven patients were ‘very satisfied,’ one ‘satisfied,’ one ‘neutral,’ and two ‘dissatisfied.’ Ten stated they would have the procedure again, one would not. Two could not be reached to answer these questions. Visual analogue scale pain score decreased from 4.6 to 3.4 (p=0.150), ankle osteoarthritis scale (AOS) pain subscale decreased from 36.2 to 13.8 (p=0.013), AOS disability subscale decreased from 42.8 to 21.9 (p=0.032), and AOS total score decreased from 39.5 to 17.8 (p=0.014). No statistical change in SF-36 physical function score (p=0.547) or PROMIS physical function score (p=0.580) was detected. At last examination, 12 of 13 patients had active eversion and a palpable, tensioned graft. The patient without active eversion underwent triple arthrodesis; no other patient had additional peroneal or hindfoot surgery.
Conclusion: Allograft interposition is effective to reconstruct unsalvageable concomitant tears of both peroneal tendons as well as the most difficult revision cases of nonfunctioning, unsalvageable peroneal tendons after prior repair or reconstruction, which have recurrent tears, tendon degeneration, scarring, and stretching. There is a high rate of restoration of peroneal function, a reasonable rate of patient satisfaction, and statistically significant improvements in ankle-specific patient-reported outcomes.
DOI: 10.1177/2473011421S00118
Anatomy of the Naviculocuneiform Joint
George J. Borrelli, MD; Mossub Qatu, MD; Christopher J. Traynor; Joseph Weistroffer; James R. Jastifer, MD
Introduction/Purpose: The naviculocuneiform (NC) joint has a role in numerous pathologies of the foot and ankle. There is little in the published literature quantifying the cartilage of the articulating surface and its unique anatomical features. The purpose of this study was to quantify and describe the articular surface of the NC joint. Our hypothesis was that the cartilage surface would have anatomic features that would guide surgeons when performing procedures such as joint preparation and screw placement.
Methods: Twenty cadaver NC joints were dissected, and the articular cartilage quantified by calibrated digital imaging software.
Results: The mean dorsal to plantar height of the navicular facets was 18mm, with a maximum height not exceeding 21mm. The mean height of the medial, middle, and lateral cuneiform facets was 15mm, 17mm, and 15mm, respectively. The mean length from the medial to middle navicular facet was 14mm, approximately 41.3% the mean length across all three navicular facets (34mm). For the distal navicular articulation, 75.4% of the mean surface area was articular cartilage. For the proximal medial, middle, and lateral cuneiform articulations, 69.6%, 75.7%, and 75.8% of the mean surface areas were articular cartilage, respectively.
Conclusion: This study provides an anatomic description of the NC joint to guide surgeons when operating on the NC joint. Two clinical observations can be made from this data. First, when preparing the NC joint for arthrodesis from a dorsal approach, the surgeon should be aware that the cartilage of the NC joint can extend up to 21mm from dorsal to plantar. This is also a useful estimate of screw length in the subchondral bone. Second, the central third of the navicular, where the majority of navicular stress fractures occur, lies in the inter-facet ridge between the medial and middle facets.
DOI: 10.1177/2473011421S00119
3-D Generated Anatomic Custom Talar Cement Spacers: A Technical Tip and Literature Review
Kimberly K. Broughton, MD; Bonnie Y. Chien, MD; Derek S. Stenquist; Caroline Williams, BA; Christopher P. Miller, MD; John Y. Kwon, MD
Keywords: Trauma; Foot and Ankle Infection; Ankle Arthroplasty
Introduction/Purpose: Three dimensional printing is an actively emerging field within the realm of medical devices. This technology expands therapeutic options and customization of implants to individual patients. The ability to create products that replicate normal bony anatomy has been a significant advancement in the setting of difficult clinical scenarios. 3-D generated, custom implants increase the potential for joint and limb salvage with the goal of improving functional outcomes. We present a technical tip for utilizing 3-D printing technology to create custom, anatomically-matched antibiotic cement spacers for limb- salvage applications. We present two illustrative cases and share our experiences, lessons learned, and a succinct review of the pertinent literature merging 3-D printing and the use of antibiotic cement as temporary and permanent reconstructive solutions.
Methods: While the majority of 3-D printing is done for the purpose of generating devices for implantation, we present a technical tip for designing a 3-D printed mold from which to create an antibiotic cement spacer for implantation. Two case illustrations demonstrate comorbid patients presenting with infected implants, osteomyelitis, bone loss, deformity and wound dehiscense. We describe the process of patient selection, implant design, fabrication, and implantation of a custom molded antibiotic cement talus for the purpose of limb salvage.
Results: Case illustrations present two successful limb salvage patients while giving a thorough explanation of our technique, learned tips and tricks. This applied technology builds on prior use of antibiotic cement in limb salvage of the lower extremity, most of which is joint sacrificing. 3-D printing the mold for an anatomic talus cement spacer results in a joint sparing limb salvage solution.
Conclusion: Utilization of currently available 3-D printing technology as applied to production of anatomic cement spacers should be considered to enhance limb salvage. This innovative application of printing technology is merged with current, pertinent literature regarding antibiotic cement to offer surgeons expanded options for temporary or definitive reconstructive techniques in some of the most challenging patients.
DOI: 10.1177/2473011421S00120
Outcomes of Posterior Malleolar Fixation in Ankle Fractures in A Major Trauma Centre
Nelson Bua; Luckshmana A. Jeyaseelan; Lee Parker, FRCS(Tr&Orth); Amaury Trockels; Catrin Sohrabi; Alexandros Vris; Nima Heidari; Francesc Malagelada Romans
Introduction/Purpose: Ongoing controversy exists over the indications and benefits of posterior malleolar fixation in ankle fractures. These injuries require careful evaluation of the bony and ligamentous structures with theoretical benefits of posterior malleolar fixation now widely accepted as restoration of articular congruity, restoration of fibular length and stabilisation of the syndesmosis. Surgical and patient report outcomes are varied in the literature with analysis limited by the lack of standardisation in functional outcomes and small patient populations. Posterior malleolar fixation does extend operative time and potentially increases complication rate. The aim of this pragmatic study was to evaluate the outcomes of posterior malleolar fracture fixation in the setting of a major trauma centre. Our hypothesis is that posterior malleolus fixation leads to improved clinical outcomes.
Methods: A total of 320 patients were identified with operatively treated ankle fractures involving a posterior malleolus component, between January 2012 and January 2018, with minimum 2 year follow-up. Patient electronic records were assessed for demographic data including age, gender, mechanism of injury, co-morbidities and smoking status. Pre-operative imaging, including CT was used to evaluate the nature of the injury and classify the posterior malleolar fracture according to the Mason classification. One hundred and sixty patients underwent posterior malleolus fixation as part of their surgery and 160 patients did not. The Manchester-Oxford Foot Questionnaire (MOXFQ) at final follow-up, was the primary patient outcome measure.Complications were noted to be minor (superficial infection or delayed wound healing) or major (DVT/PE, deep infection, chronic regional pain syndrome (CRPS), arthrofibrosis, further intervention for post-traumatic arthritis, hardware failure or irritation). All cause reoperation rates were also noted.
Results: Fixation of the posterior malleolus was associated with a statistically significant improvement in patient outcomes. Mean MOXFQ score in the unfixed posterior malleolus group was 24.03 (0 - 62), compared to 20.10 (0 - 67) in the fixed posterior malleolus group (p =0.04). Outcomes were worse with increasing size of posterior malleolar fragment. When compared with either posterior malleolus fixation alone or syndesmotic stabilisation alone, poorer outcomes were seen when the posterior malleolus fixed with additional syndesmotic stabilisation, with mean MOXFQ scores of 21.73 (0-60), p =0.057. Metalwork-related issues were higher in the posterior malleolus fixed group (24/160 (15%) versus 10/160 (6.2%), p=0.03). Re-operation rate was double (34/160 (21.2%) vs 16/160 (10%), p = 0.03). The main cause of this was hardware related issues.
Conclusion: This pragmatic study is one of the largest published series that assesses patient reported outcomes in posterior malleolar fixation. The key finding is that posterior malleolar fixation is associated with a statistically significant improvement in patient reported outcome scores. However, the overall complication rate was 10.7% higher in the fixation group and the risk of reoperation was over double. Further research should focus on high quality randomised controlled trials with long term follow-up to assess long term impacts of this complex ankle injury pattern.
DOI: 10.1177/2473011421S00121
Development of a Machine Learning Algorithm for Prediction of Complications after Ankle Arthrodesis
Amador Bugarin; Akash A. Shah; Sai Devana, MD; Changhee Lee; Nelson F. SooHoo, MD
Introduction/Purpose: Ankle arthrodesis and total ankle replacement are the most commonly performed procedures for surgical management of ankle arthritis. Arthrodesis provides effective pain relief but the rate of complications after arthrodesis is higher as it is more commonly performed in patients with comorbidities that preclude ankle replacement. Accurately risk- stratifying patients who undergo ankle arthrodesis would be of great utility, given the significant cost and morbidity associated with developing major perioperative complications. There is a paucity of accurate prediction models that can be used to pre- operatively risk-stratify patients for ankle arthrodesis. We aim to develop a machine learning (ML) algorithm for prediction of major perioperative complication after ankle arthrodesis as well as compare its performance against traditional predictive models based on logistic regression.
Methods: This is a retrospective cohort study of adult patients who underwent ankle arthrodesis at any non-federal California hospital between 2015 and 2017. The primary outcome was readmission within 30 days or major perioperative complication - venous thromboembolism within 30 days, myocardial infarction within 7 days, pneumonia within 7 days, systemic infection within 7 days, surgical site bleeding within 90 days, and wound complications within 90 days. We build ML and logistic regression models that span different classes of modeling approaches: XGBoost, AdaBoost, Gradient Boosting, and Random Forest. Discrimination and calibration were assessed using area under the receiver operating characteristic curve (AUROC) and Brier score, respectively. We utilize a partial dependence function to measure the importance of an individual feature by assessing the average effect in predicted risks when its value is altered. We rank the contribution of the included variables to the prediction of adverse outcomes.
Results: A total of 1,084 patients met inclusion criteria for this study. There were 131 major complications or readmission (12.1%). The optimized XGBoost algorithm demonstrates higher discrimination (AUROC: 0.707 + 0.052) compared to LR (0.691 + 0.055). The receiver operating characteristic curves for the XGBoost and logistic regression models are visualized in Figure 1. XGBoost also outperforms the three other ML models. This model was well calibrated (Brier score: 0.103 + 0.001). The variables most important for the XGBoost model include diabetes, chronic kidney disease, implant complication, and major fracture. Five of the ten most important features for XGBoost were markedly less important for the traditional logistic regression model: male sex, prior hip fracture, cardiorespiratory failure, acute renal failure, and dialysis status.
Conclusion: We report a ML algorithm for prediction of major perioperative complications after ankle arthrodesis. The optimized XGBoost model is well-calibrated and demonstrates superior risk prediction to logistic regression. This tool may identify and address potentially modifiable risk factors, helping to accurately risk-stratify patients and decrease likelihood of major complications. Notably, the predictors most important for XGBoost are different from those for logistic regression. This suggests that the superior discriminative capability of ML methods stems from their ability to capture complex non-linear relationships between variables that logistic regression is unable to detect.
DOI: 10.1177/2473011421S00122
The Medial Gastrocnemius Release: A Safe and Effective Alternative for Treatment of Isolated Gastrocnemius Contracture
Patrick E. Bull, DO; Antonio M. Malloy, McCoy; Mitchell Thompson; Maria R. McGann, DO; Gregory C. Berlet, MD
Introduction/Purpose: Gastrocnemius recession is a popular procedure utilized to treat a myriad of lower extremitychronic conditions related to isolated gastrocnemius contracture (IGC). Recent anatomical research detailing the variable relationship between the distal gastrocnemius and soleus tendons has raised important questions regarding the safety of some traditional recession procedures. Alternative gastrocnemius recession strategies may offer comparable clinical results while avoiding the surgical risk related to conjoint tendon anatomical variability.
Methods: Ten matched pairs of above-knee fresh frozen cadavers were randomized to receive either a medial gastrocnemius recession (MGR) procedure or a gastrocnemius intramuscular recession ‘Baumann’ procedure. Postoperative dorsiflexion improvement was measured and then compared between groups. Detailed post-operative surgical dissections were performed on all specimens to assess structures at risk, conjoint tendon morphology, and anatomical symmetry.
Results: MGR and GIAR procedures were equally effective at producing significant increases in passive ankle dorsiflexion. No sural nerve injuries were observed. 35% of specimens showed direct muscular fusion of at least a portion of the distal gastrocnemius muscular tissue to the adjacent soleus, with sections of no distal transactable gastrocnemius tendon present.
Conclusion: The MGR produced comparable results to the Baumann/GIAR in a cadaver model. We feel that the MGR is an attractive alternative to traditional gastrocnemius recession techniques due to the simple approach, the region’s predictable anatomy, its low risk to surrounding vital structures, and its early evidence of effectiveness. We also concluded that the conjoint tendon anatomy is highly variable and that surgeons must account for this unpredictability when surgically treating IGC. We predict that the biggest risk associated with conjoint tendon region recession procedures is inadvertent soleus transection and subsequent over lengthening related plantar flexion weakness.
DOI: 10.1177/2473011421S00123
Infrequent Adventitious Bursitis Associated with A Palpable Metatarsal Mass: Series of Cases
Virginia M. Cafruni, MD; Ana C. Parise, MD; Jonathan M. Verbner, MD; Daniel S. Villena, MD; Leonardo A. Conti, MBA,PhD; Pablo Sotelano, MD; Nelly M. Carrasco, MD; Maria Gala Santini Araujo, MD
Category: Midfoot/Forefoot
Keywords: Metatarsalgia; Pain; Forefoot
Introduction/Purpose: Adventitious bursae are structures that appear in adulthood, as a mechanism for protection. It may develop at sites where subcutaneous tissue (ST) is exposed to friction and high pressure. In the forefoot, adventitious bursitis is usually adjacent to bony prominences of the metatarsal heads and is one of the causes of forefoot pain. There are different stages of the pathology, at the beginning there is a small bursa without cavity, subsequently this cavity will gradually acquire a larger size, until becoming independent. The degeneration of the connective tissue which is the characteristic of the adventitious bursa. Figure 1.We present four cases of adventitious bursitis in patients who complained of a fluctuating mass on the forefoot associated with localized pain on palpation and pressure.
Methods: We reviewed the cases of 4 patients treated by one of us (MGSA) for forefoot pain associated with a palpable mass. We obtained the information from the medical records: clinical presentation, radiographs, ultrasound, magnetic resonance imaging (MRI), treatment, histological diagnosis (if it was available) and outcomes. Pain was assessed with visual analog scale (VAS).
Results: The four patients complained of a mass on the forefoot associated with pain. The skin was normal with no signs of infection. Ultrasound and MRI showed heterogeneous images in the ST in high pressure areas. Patients were diagnosed according to the previous studies and treated conservatively. The treatment consisted of cryotherapy and walker boot until they had shoe insoles with metatarsal olive in order to unload the metatarsus. Forefoot pain improved markedly from an initial VAS of 8.5 to 3.5 in the first month and the palpable mass decreased. Except in one patient whose studies were not conclusive and mass does not decrease in size and she required an excisional biopsy. The anatomopathological diagnosis was consistent with adventitial bursitis.
Conclusion: Adventitious bursitis of the plantar forefoot is not a frequent pathology and it can be confused with a foreign body granuloma, localized infection or a tumoral mass among other possible diagnoses due to the clinical and imaging presentations. It is important to take this diagnosis into account when dealing with metatarsalgia and have fluent communication with the radiologist in order to avoid an unnecessary surgery and to establish the appropriate treatment to improve the symptoms.
DOI: 10.1177/2473011421S00124
Tarsal Tunnel Syndrome Following Medializing Calcaneal Osteotomy
Virginia M. Cafruni, MD; Facundo Bilbao, MD; Facundo Galich, MD; Guillermo Cardone, MD; Nelly M. Carrasco, MD
Introduction/Purpose: The tarsal tunnel syndrome is a compressive neuropathy that affects either the posterior tibial nerve, within the tarsal tunnel, or one of its terminal branches. It can be caused by extrinsic or intrinsic factors. Even though the tarsal tunnel syndrome has been reported as a complication of lateralizing calcaneal osteotomy, we have not identified in the literature reports of this syndrome associated to medializing calcaneal osteotomy. We report the case of a 60-year-old female who developed a tarsal tunnel syndrome, on the third postoperative week, following a medializing calcaneal osteotomy for flatfoot correction with stage IIB posterior tibial tendon dysfunction.
Methods: We reviewed and obtained the information from the medical records of this patient: clinical examination, radiographs, computed tomography, magnetic resonance imaging, and outcome. Pain was assessed with visual analog scale (VAS).
Results: The patient is a 60-year-old female with left stage II posterior tibial tendon dysfunction who failed to respond to conservative treatment. Medializing and lengthening (Evans) osteotomies of the calcaneus were performed, together with posterior tibial tendon repair and spring ligament reconstruction. In the postoperative, after a cast replacement into a more plantigrade position, the patient developed symptoms that suggested a compressive neuropathy of posterior tibial nerve within the tarsal tunnel associated to calcaneal medializing osteotomy. Initial conservative treatment failed and the posterior tibial nerve was explored under loupe magnification and the tarsal tunnel was released. Figure 1. An immediate improvement in pain was observed postoperatively and almost full recovery occurred within 6 months.
Conclusion: In our case report, the tarsal tunnel syndrome was a consequence of the osteotomy fragment displacement that generated a reduction of the tarsal tunnel volume. It has been described that the tarsal tunnel syndrome symptoms become more evident with ankle dorsiflexion and eversion, in our patient this can be associated with the symptom exacerbation presented when the cast was placed into plantigrade position. We conclude that even though in the literature the tarsal tunnel syndrome has been mainly associated to lateralizing osteotomies, it is important to take this complication into account when performing a medializing osteotomy.
DOI: 10.1177/2473011421S00125
Medium to Long-Term Results of Combined Deltoid and Foot Reconstruction for PCFD (Stage IV) Valgus Ankle
Kristin C. Caolo, BA; Cesar de Cesar Netto, MD, PhD; Jonathan Garfinkel, MS; Andrew R. Roney, BA; Jiaqi Zhu; Jonathan T. Deland, MD
Category: Ankle; Hindfoot; Other
Keywords: Adult Acquired Flatfoot Deformity; Deltoid; Joint Preserving Surgery
Introduction/Purpose: There is limited documentation of the results of the treatment of advanced progressive collapsing deformity with talar tilt. No article to our knowledge with pre-and post-operative ankle x-rays has more than eight patients and average follow up more than three years.
Methods: This article presents the results of twenty consecutive patients with medium to long term follow up. All patients had deltoid reconstruction with tendon graft from the talus to the tibia and foot reconstruction to achieve a heel centered under the lower leg, a stable midfoot and a mild to moderately plantarflexed first metatarsal. Patients were followed an average 10.8 years (SD = 4.6, Range 4.6-17) and had standing pre-and post-operative radiographs along with FAOS and PROMIS scores. Radiographs were assessed for talar tilt preoperatively, early postoperatively and at final follow up. Data was analyzed with paired t-tests, Mann Whitney U test, fisher’s exact test and univariable linear regression. All p-values are two-sided and statistical significance was evaluated at the 0.05 alpha level.
Results: Two patients failed the procedure; one had an ankle fusion and the second infection eventually required a BKA. The remaining 18 patients were satisfied with their procedure, maintained significant improvement in outcome scores and talar tilt and required no other procedure on their ankle. The mean talar tilt preoperatively was 10.9 degrees (SD = 3.9) and at final follow up 4.2 degrees (SD = 2.8) (P<0.0001). Initial correction of the talar tilt as documented by early post-operative (mean early follow-up years = 2.2, SD = 1.9) with standing radiograph was maintained within 3 degrees in comparison to final radiographic follow up (Mean=0.56, 95%CI (-0.40, 1.51) P<0.0001).
Conclusion: Combined deltoid and foot reconstruction, as described, has acceptable results in majority of patients at medium to long term follow up.
DOI: 10.1177/2473011421S00126
Prescribing Fewer Opioid Pills to Hallux Valgus Patients Undergoing Minimally Invasive Bunion Correction: A Prospective Comparative Study
Kristin C. Caolo, BA; Celia Marion; Rebecca Paugh; A. Johnson, MD
Category: Bunion; Midfoot/Forefoot
Keywords: Hallux Valgus; Minimally Invasive; Pain
Introduction/Purpose: This study aims to compare opioid usage and patient satisfaction with postoperative pain management in similar hallux valgus (HV) patients who underwent minimally invasive distal chevron akin (MIS) correction with patients who underwent modified Lapidus and scarf corrections. We hypothesized that patients who underwent minimally invasive bunionectomy would consume fewer opioids and report similar satisfaction with pain management compared with modified lapidus and scarf patients.
Methods: This study is a single center prospective study of 33 patients diagnosed with hallux valgus undergoing MIS bunion correction who received a novel opioid prescribing protocol used by the senior author. Preoperatively, patients undergoing MIS corrections were counseled on the expectations of pain after surgery, received a take home pamphlet, and were prescribed opioids for moderate surgery (5-15 pills). These patients were then compared to a cohort of 25 hallux valgus patients status post Lapidus or scarf bunionectomy who were prescribed 40-60 opioid pills without preoperative coaching or handouts. Patients were excluded if they used opioids or muscle relaxants preoperatively or had a known history of a substance use disorder. Patients completed surveys postoperatively for eight weeks reporting pain level, number of opioid pills consumed, refill requests, and satisfaction with their pain management plan.
Results: There was a significant difference (p< 0.001) in mean pills consumed between MIS patients who averaged 2.5 opioid pills (5mg Oxycodone/pill) and modified Lapidus and scarf patients who averaged 25.2 opioid pills (5mg Oxycodone/pill) at all time points (Table 1). There was no significant difference between the ratio of pills taken to pills prescribed between both groups (p>0.05). Patients had comparable levels of pain at all time points (p>0.05). MIS patients did not request any refills, whereas Lapidus and scarf patients requested a total of 5 refills over the course of the study.
Conclusion: HV patients who underwent MIS correction achieved equivalent analgesic effect when compared to similar HV patients who underwent Lapidus or scarf procedures. The Lapidus and scarf group received approximately four times the amount of opioids and consumed 11 times the amount of pills. This study demonstrates that HV patients undergoing MIS bunion correction require far fewer opioid pills to achieve the same level of postoperative pain control compared with Lapidus and scarf patients. This study also suggests that a novel postoperative prescribing protocol utilized by the senior surgeon may decrease the number of pills both prescribed and consumed by patients.
DOI: 10.1177/2473011421S00127
Effect of Postoperative Immobilization Time on PROMIS Scores and Clinical Outcomes in Ankle Fracture Patients
Dwayne D. Carney; Parth S. Vyas, DO; Justin Hicks, BS; Jeffrey E. Johnson, MD; Jeremy J. McCormick, MD; Sandra E. Klein, MD; Jonathon D. Backus, MD
Introduction/Purpose: Ankle fractures are among the most common injuries that Orthopaedic Surgeons treat; yet, little guidance exists in postoperative protocols for ankle fractures concerning time of immobilization and weightbearing. Results from previous studies have been mixed; demonstrating improved outcomes, no difference in outcome, or poorer outcomes including increased wound complications in patients who are mobilized early. Here, we aim to investigate the association between early immobilization and patient reported outcomes. Our null hypothesis was that no difference in PROMIS scores would be identified in patients when comparing the effect of time of immobilization and time of weightbearing.
Methods: A chart review identified ankle fractures that underwent surgical fixation between 2015 and 2020 at a level 1 trauma center and its associated facilities. One-hundred nineteen patients from 8 providers met inclusion criteria for our final analysis. Fifty patients were immobilized for <6 weeks and 69 patients were immobilized for at least 6 weeks. Our primary outcome measures included the PROMIS questionnaire, time of immobilization, and time to full weightbearing. Our secondary outcome measures included time to return to work, wound complications (infection, delayed healing), and complications associated with fracture fixation (loss of reduction, delayed union, reoperation, hardware failure). Repeated-measures ANOVAs were used to predict each of the PROMIS outcomes of anxiety, depression, physical function, and pain interference. Each model included the predictors of age, sex, race, BMI, payor, provider, time to radiographic union, time to return to work, time to full weightbearing, and early vs late immobilized groups.
Results: There were no differences in PROMIS scores between mobilization groups and time to full weightbearing (p>0.05). Furthermore, there were no differences in wound complications nor complications associated with fracture fixation (p>0.05). Across our cohort, physical function scores were negatively impacted by higher BMI, increasing age and longer time to return to work/play (p<0.05). Our analysis further showed that depression, anxiety, pain interference and physical function levels improve as a function of time (p<0.05). African Americans showed more pain interference than other groups of patients (p<0.05). No difference in PROMIS scores were identified between treating providers (p>0.05).
Conclusion: In this study, the null hypothesis was accepted. Data from our analysis shows no significant differences between the early and late mobilization and weightbearing groups in terms of PROMIS outcomes nor with wound complications and complications associated with fracture fixation. Our study does suggest that early mobilization after operative treatment of ankle fractures is safe and results in similar patient reported outcomes with no increased risk of complication. We did find that African American patients experienced more pain that other groups and we aim to further explore this topic to find potential modalities to address this disparity.
DOI: 10.1177/2473011421S00128
Benefits of Ankle Arthroscopic Debridement in Acute and Subacute in Ankle Fractures
Paolo Ceccarini, MD; Fabrizio Marzano; Lorenzo di Giacomo; Giuseppe Rinonapoli, MD; Auro Caraffa
Introduction/Purpose: The purpose of this study was to evaluate the benefits of ankle arthroscopy at the time of ORIF or after six months in patients with residual symptoms. The hypothesis was that in patients treated arthroscopically at the time of ORIF, there were faster and better clinical results than those treated after or untreated with arthroscopy.
Methods: In this retrospective study, we compared three homogeneous groups of selected patients with specific inclusion criteria (144in total, mean age 38.2 years). They have been surgically treated for an ankle fracture (bimalleolar or trimalleolar without frank syndesmotic injuries) with open technique (ORIF) or arthroscopic ORIF (AORIF), between 2016 and 2019. The AO classification system was used for each patient. The clinical assessment was based on the Foot and Ankle Outcome Score (FAOS).
Results: At the final follow-up (mean 36 months), both patients treated with ankle arthroscopic debridement at the time of ORIF and patients treated with arthroscopic debridement after ORIF showed a significant improvement of the FAOS, which reported84 and 85 respectively at final follow-up.
Conclusion: Through direct visualization of intra-articular structures, ankle arthroscopy can offer an essential option for patients both in acute and in sequelae after an ankle fracture. More studies are needed to understand the real effectiveness of the procedure, especially in acute at the same time of osteosynthesis.
DOI: 10.1177/2473011421S00129
Effectiveness of Endoscopic Assisted Repair in Achilles Tendon Ruptures Compared to Percutaneous and Open Repair
Paolo Ceccarini, MD; Fabrizio Marzano; Lorenzo di Giacomo; Giuseppe Rinonapoli, MD; Auro Caraffa
Introduction/Purpose: The Achilles tendon rupture is the third most common tendon’s injury, with an incidence of 16- 18/100000. Various repair’s techniques are described, however the best surgical treatment remains controversial. Our purpose was to evaluate the effectiveness of endoscopic assisted repair compared to traditional open repair and percutaneous technique.
Methods: We carried out a prospective observational study in patient operated in our Orthopedic Department between 2017 and 2019. We enrolled 47 patients (40 M; 7F), with a mean age 42,5 y.o with a mean follow up 32 months (12-60). The patients were divided in 3 groups according to the surgical procedures. Group A included 15 patients underwent to endoscopic assisted repair, Group B: 11 patients with percutaneous repair and group C 21 patients open repair. Demographic data, injury mechanisms, operation’s time and technique were recorded. At final f-u complications, functional score (VAS, AOFAS AH, ATRS) were requested. The statistical analysis was performed with the t-student test. IRB approved.
Results: The 78% of injuries occurred during recreational sport activities, with a majority during football amatorial matches. Operation’s time was 42,5 minutes for group A, 33,3 for group B, 33,5 for group C. Among group A, 1 patient developed a DVT. In group B no major complications were reported. In group C a patient suffered from infection with suture insufficiency. Ankle stiffness was reported in 25% of patients in group C. No axonotmesis or neurotmesis of suralis was observed; 16 of patients complained transitory paresthesia in the postoperative. The mean time to return to work’s activity was 44,2 days for group A, 35,6 days for group B, and group C 91,1 days, while the mean time to return to drive was in average 72,1 days for group A, 66 days for group B, 92,3 days for group C. ATRS was 79,3 for group A, 87,6 group B and 72,75 group C.
Conclusion: This technique is safe and achievable with low postoperative pain and complications, early return to activities, and satisfactory functional outcomes. Compared to standard percutane-ous repair, endoscopy-assisted repair of Achilles tendon ruptures may be useful because it ensures precise placement of sutures through the ten-don and real-time visualization of the gap. Further large-scale, randomized and prospective clinical trials must be the subject of future prospective study.
DOI: 10.1177/2473011421S00130
Hallux Valgus Pronation Correction by Scarf Osteotomy: Prospective Case Series with WB-CT Scan
Felipe R. Chaparro, MD; Cristian A. Ortiz, MD; Raul M. Espinoza Aravena, MD; Manuel J. Pellegrini, MD; Giovanni M. Carcuro, MD
Introduction/Purpose: Hallux valgus is one of the most prevalent foot deformities. Coronal metatarsal rotation (pronation) has been recognized as a key element in hallux valgus deformity and an important prognostic factor for recurrence. New surgical techniques have been developed in order to specifically address pronation deformity but tend to be technically demanding. With the advent of weight bearing CT (WBCT), accurate pronation measurement has improved. Deformity correction by means of metatarsal osteotomies has been an effective way to correct transverse plane deformity but its capacity for pronation correction is not well established. Purpose: Assess transverse and coronal plane rotation deformity correction by WBCT in hallux valgus patients after scarf osteotomy.
Methods: We prospectively analyzed hallux valgus deformity in patients who underwent Scarf osteotomy for symptomatic hallux valgus with preoperative and at least 3 month postoperative WBCT for comparison. Intermetatarsal angle (IMA), hallux valgus angle (HVA) and alpha angle (AA) for first metatarsal rotation (pronation) was measured by 3 different observers. The intraclass correlation was determined. Pre and postoperative measurement change was established by T-test and Wilcoxon for related samples.
Results: 40 feet in 25 patients were included. The interclass correlation between observers was 0.9 for AA (pronation), 0.92 for IMA and 0.95 for HVA in preoperative evaluation and 0.94 for AA, 0.65 for IMA and 0.82 for HVA in postoperative evaluation. The mean preoperative and postoperative AA of the first metatarsal was 8.9 degrees (range -8.83-24,40, SD 6.8) and 6.3 degrees (range -10.7-28.4, SD 8.3) respectively, resulting in a significant first ray pronation change of -2.5 degrees (P =.006). The media preoperative and postoperative IMA was 13.1 degrees (SD 2.9) and 4.9 degrees (SD 2.0) respectively, demonstrating a significant change (P <.001). The media preoperative and postoperative HVA was 25 degrees (SD 6.7) and 5.9 degrees (SD 4.2) respectively, demonstrating a significant change (P <.001)
Conclusion: The Scarf osteotomy for hallux valgus deformity has a significant power to correct both transverse and coronal plane (pronation) deformity.
DOI: 10.1177/2473011421S00131
Factors Associated with Surgical Success of End Stage Ankle Arthritis with Minimum 4-Year Follow-Up
Sagar Chawla, MD, MPH; Jane Shofer, MS; Daniel Norvell; William R. Ledoux; Bruce J. Sangeorzan, MD
Introduction/Purpose: Both total ankle arthroplasty (TAA) and ankle arthrodesis (AA) are effective treatments for ankle arthritis. This study sought to use a statistical modeling approach to determine factors associated with success following either surgery. While a number of studies have explored risk factors associated with complications, our aim was to guide management based on factors which may be predictive of success.
Methods: We retrospectively analyzed data from a prospective multicenter cohort study conducted between May 2012 and May 2015. We compared outcomes in 448 patients who had follow-up of at least 4 years and were treated for ankle arthritis with either TAA or AA. We collected baseline factors including demographics, pre- and post-operative outcome scores including the Foot and Ankle Ability Measure (FAAM), Short Form-36 (SF-36) Physical and Mental Component Summary scores, pain, ankle related adverse events, and radiographs (coronal tilt and sagittal subluxation). We defined fully Successful as an increase in the FAAM ADL score by the minimum clinically important difference (MCID) and the absence of post-operative complications. We performed a multivariate logistic regression model adjusted for age, sex, BMI, and surgery type to identify associations with success.
Results: Of the 517 patients who consented, had surgery and completed post-operative surveys, 414 (80.0%) underwent TAA and 103 (19.9%) underwent AA. Of the 517 patients, 448 patients (86.7%) had a minimum of 4-year follow-up. Of the 448 patients, 331 (73.9%) were successful) outcome and 117 (26.1%) were not fully successful. Out multivariable logistic model found female sex (0.83 +- 0.03, p=0.002), treatment with TAA (0.80 +- 0.020, p=0.001), and no previous surgery (0.82 +- 0.03, p=0.030) as variable significantly associated with success. Notably, mental health factors and pre-operative radiographic measurements, including coronal tilt and sagittal subluxation, were not significantly associated with success.
Conclusion: Surgeons treating patients with ankle arthritis have two viable surgical alternatives. Recognizing the factors associated with mid-term success may be as valuable as knowing risk factors associated with failure. In addition, we also find variables thought to affect outcomes, mental health and pre-operative radiographic measurements such as coronal plane misalignment, were not found to significantly affect outcomes.
DOI: 10.1177/2473011421S00132
Comparison of Outcomes of Arthroscopic Modified Broström Procedure for CLAI in Patients with Solitary ATFL Injury and in Patients with ATFL and CFL Complex Injury
Introduction/Purpose: ATFL (Anterior talofibular ligament) and CFL (Calcaneofibular ligament) are most commonly injured structures when ankle sprained. There has been debate about whether CFL should be recovered by surgery. Recently, several studies have verified that MBP (Modified Broström procedure) with IER (Inferior extensor retinaculum) augmentation demonstrated good outcomes even in patients with ATFL and CFL complex injury. However, some studies presented that IER augmentation cannot cover CFL injuries because of a different vector. If so, we hypothesized that the patients with solitary ATFL injury would show better outcomes comparing with patients with ATFL and CFL complex injury when same arthroscopic MBP was performed for each group.
Methods: 208 ankles were included between September 2015 and October 2019. All the patients were underwent arthroscopic MBP with IER augmentation using knotless suture anchor technique. Complete ATFL injuries were determined by arthroscopy and CFL injuries were examined by magnetic resonance image. 26 ankles of which talar tilt angle was less than 9 degrees in ATFL and CFL complex injury group were excluded. Finally, 38 ankles with solitary ATFL injury and 31 ankles with ATFL and CFL complex injury were enrolled. Clinical and radiological outcome were measured and compared between two groups. Clinical outcome was divided into objective and subjective outcome. Objective outcomes were composed of VAS, AOFAS score and FAOS. Subjective outcome was presented as subjective satisfaction score (1: Excellent, 2: Good, 3: Fair, 4: Poor). Improvement of degree of anterior talar translation and talar tilt angle between preoperative and 12 months after surgery was measured as a radiological outcome.
Results: P-values of VAS score at preoperative, 3 months, 6 months and 12 months after surgery were 0.3761, 0.2609, 0.3893 and 0.2547 respectively (95% confidence interval[CI]). P-values of AOFAS score at preoperative, 3 months, 6 months and 12 months after surgery were 0.2079, 0.64, 0.6339 and 0.2683 respectively (95% CI). P-values of FAOS and subjective satisfaction score at 12 months after surgery was 0.1379 and 0.6338 respectively (95% CI). P-values of anterior talar translation and talar tilt angle were 0.4371 and 0.0002 respectively (95% CI). The degree of talar tilt angle improvement was -1.91 in solitary ATFL injury group and -5.48 in ATFL and CFL complex injury group.
Conclusion: The outcomes of arthroscopic MBP with IER augmentation for chronic lateral ankle instability in patients with Solitary ATFL injury and in patients with ATFL and CFL complex injury showed no differences except talar tilt angle improvement. Though talar tilt angle improvement showed difference between two groups, the degree of improvement was even better in ATFL and CFL complex injury group. It means arthroscopic MBP could be a good treatment options for chronic lateral ankle instability patients regardless of CFL injury.
DOI: 10.1177/2473011421S00133
Feasibility of Arthroscopic Anterior Talofibular Ligament Repair and Comparison Between Arthroscopic and MR Findings for Anterior Talofibular Ligament Injuries
Introduction/Purpose: The Modified Broström Operation (MBO) has been frequently used to treat chronic lateral ankle instability. Recent studies of arthroscopic anterior talofibular ligament (ATFL) repair found that if the ligament is detached at the fibular attachment or there is sufficient remnant tissue, it can be directly repaired using suture anchors. In this study, ATFL injuries were classified and the feasibility of arthroscopic ATFL repair according to injury type was determined. The diagnostic validity of magnetic resonance imaging (MRI) of ATFL injuries was investigated by comparing MRI and arthroscopic findings.
Methods: The 197 ankles (93 right, 104 left; 12 bilateral) of 185 patients (90 men and 107 women; mean age, 33.5 years, range: 15-68 years) were treated between September 2015 and October 2019. All patients underwent arthroscopic MBO after a diagnosis of chronic lateral ankle instability. ATFL injuries were classified according to their grade and arthroscopically determined location (type 2: partial rupture, type 3A: fibular detachment, type 3B: talar detachment, type 3C: midsubstance rupture, type 3D: absence of ATFL, type 3E: os subfibulare). Two musculoskeletal radiologists blinded to the surgical findings evaluated all of the ankle injuries and classified them as described above. An oblique-coronal MRI sequence was used to improve diagnostic accuracy.
Results: The kappa value for interobserver reliability was 0.82 (95% confidence interval [CI], 0.76-0.88), indicating excellent interobserver reliability. The kappa value for the agreement between the arthroscopic findings and MRI findings was also high (0.85; 95% CI, 0.79-0.91). Among the 197 injured ankles, according to ankle arthroscopy, 67 were type 2 (34%), 28 were type 3A (14%), 13 were type 3B (7%), 29 were type 3C (15%), 26 were type 3D (13%), and 34 were type 3E (17%).
Conclusion: In this study, arthroscopic ATFL repair was feasible in ~14% of ATFL injuries related to chronic lateral ankle instability. The ATFL classification system proposed herein could help surgeons to determine treatment options before surgery in patients with ATFL injuries, and even evaluate acute injury. Our results also supported the use of MRI for diagnosing ATFL injuries and showed that it is an informative tool during the preoperative period.
DOI: 10.1177/2473011421S00134
Corticosteroid Injection for Morton’s Interdigital Neuroma: A Systematic Review
Jun Young Choi, MD; Min Jin Kim, MD; Jin Soo Suh, MD, PhD
Introduction/Purpose: This review aimed to evaluate the effects of corticosteroid injections for Morton’s neuroma using an algorithmic approach to assess the methodological quality of reported studies using a structured critical framework.
Methods: Several electronic databases were searched for articles published until April 2020 that evaluated the outcomes of corticosteroid injections in patients diagnosed with Morton’s neuroma. Data searches, extraction, analysis, and quality assessments were performed according to the PRISMA guideline, and the clinical outcomes were evaluated using various outcome measures.
Results: With 3-12 months of follow-up, corticosteroid injections provided a satisfactory outcome according to Johnson satisfaction scores without two studies. Visual analogue scale scores showed maximal pain reduction between 1 week and 3 months post-injection. We found that 140 subjects out of 469 (29.85%) eventually underwent surgery after receiving corticosteroid injections due to persistent pain.
Conclusion: Corticosteroid injections showed a satisfactory clinical outcome in patients with Morton’s interdigital neuroma in spite of almost 30% of included subjects eventually underwent operative treatment. Our recommendation for the future study includes using more objective outcome parameters, such as foot and ankle outcome scores or foot and ankle ability measures. Moreover, studies about the safety and effectiveness of multiple injections at the same site are highly necessary.
DOI: 10.1177/2473011421S00135
Low Tibial Valgization Osteotomy for More Severe Varus Ankle Arthritis
Introduction/Purpose: Low tibial valgization osteotomy with medial opening wedge (LTO) is generally indicated for ankle arthritis with a small talar tilt (TT). We addressed the following research questions: the efficacy of LTO for more significant varus ankle arthritis, the effect of additional inframalleolar correction followed by LTO, and the preoperative or operation related factors influencing postoperative TT decrease.
Methods: We retrospectively reviewed the radiographic and clinical findings of 31 patients with more significant varus ankle arthritis (>=8 degrees) who underwent LTO or LTO plus inframalleolar correction. We grouped the included patients according to combination with inframalleolar correction and postoperative decreased TT. Furthermore, a binary logistic regression analysis was performed to determine the factors influencing postoperative TT decrease.
Results: Even though the mean TT was unchanged postoperatively (from 12.1 to 9.9 degrees, P =.052), clinical parameters were significantly increased. In the group with concomitant inframalleolar correction, we found that TT was more corrected (3.9 vs 1.8 degrees, P =.023) with a greater lateralization of the talar center and a greater correction of the hindfoot alignment to valgus. The results of the binary logistic regression analysis showed a significant relationship between postoperative decreased TT and preoperative talar center migration (P =.016), hindfoot alignment angle (P =.033), hindfoot moment arm (P =.041), and hindfoot alignment ratio (P =.016).
Conclusion: LTO in more significant varus ankle arthritis could result in clinical improvement, although TT was not significantly changed. We recommend adding inframalleolar correction after LTO for the patients with more significant varus ankle arthritis.
DOI: 10.1177/2473011421S00136
Outcomes of Minimally Invasive Proximal Chevron Metatarsal Osteotomy for Moderate to Severe Hallux Valgus Deformity
Introduction/Purpose: The effectiveness of minimally invasive surgery (MIS)-distal chevron metatarsal osteotomy (DCMO) for the correction of moderate to severe hallux valgus deformity is unclear. Traditionally, proximal chevron metatarsal osteotomy (PCMO) has been considered a reliable procedure for correcting severe hallux valgus deformity. This study aimed to clarify the clinicoradiographic outcomes of our novel MIS-PCMO technique and compared its outcomes to those of MIS-DCMO performed during the same timeframe. We addressed the following research questions: (1) can the MIS-PCMO technique be an effective option for correcting moderate to severe hallux valgus deformity?; (2) are there differences in the extent of deformity correction possible with MIS-PCMO and MIS-DCMO?; and (3) what points should be considered before performing the MIS-PCMO technique?
Methods: We prospectively compared the outcomes of patients who underwent MIS-PCMO (n=20 patients; 22 surgeries) and those of patients who underwent MIS-DCMO (n=23 patients; 26 surgeries) for moderate to severe hallux valgus deformity (hallux valgus angle [HVA] >=30o) between January 2017 and December 2018. The minimum follow-up duration for inclusion in this study was 18 months. The HVA, first-to-second intermetatarsal angle (IMA), distal metatarsal articular angle (DMAA), relative length of the second metatarsal, medial sesamoid position, and Meary angle were measured preoperatively and at the final follow- up.
Results: Compared to MIS-DCMO, MIS-PCMO resulted in significantly greater correction of the HVA (P<0.001) and IMA (P=0.01), along with Meary angle improvement (P<0.001); however, the DMAA worsened (P=0.01). Furthermore, there was a significantly greater change in the relative second metatarsal length in the MIS-DCMO group (P=0.01). There were no significant between-group differences in the correction of the medial sesamoid position (P=0.445).
Conclusion: MIS-PCMO can be a better option for correcting moderate to severe hallux valgus deformities than MIS-DCMO. However, this technique should be applied carefully when the preoperative DMAA is already large because the DMAA can become worse postoperatively.
DOI: 10.1177/2473011421S00137
Comparison of Midterm Outcomes Between the Intramedullary Fibular Nail and the Locking Plate for the Treatment of Unstable Ankle Fractures in Active Young Patients
Introduction/Purpose: We aimed to compare the midterm radiological and clinical outcomes between closed reduction and internal fixation (CRIF) using the fibular intramedullary nail (IMN) and open reduction and internal fixation (ORIF) using plates for the treatment of unstable ankle fractures in active young patients.
Methods: In this retrospective cohort study, 204 patients treated with CRIF using the fibular IMN (94 patients) or ORIF using the locking plate (110 patients) were included after at least 3 years of follow-up. The mean patient age was 41.4 years. Radiographic evaluation included the quality of reduction assessed by plain radiography and the three-dimensional (3D) reconstruction model using the CT scan images as well as the development of posttraumatic ankle osteoarthritis (PTOA) assessed by weightbearing plain radiography. Clinical evaluation included the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score, Olerud and Molander score (OMAS), the Foot and Ankle Outcome Score (FAOS) and visual analog scale (VAS) pain score as well as complications.
Results: In an assessment by both plain radiography and the 3D reconstruction model, the fair or poor reduction was more observed in the IMN group than in the ORIF group at final follow-up (P <.001). Poor reduction in the IMN group was significantly related to Weber type C, pronation type injury, and comminuted fibular and trimalleolar fractures (P <.001). PTOA was observed in 21.3% in the IMN group compared to 9.1% in the ORIF group (P =.024). There were no significant differences in clinical outcomes between the 2 groups. There were significantly fewer postoperative complications in the IMN group than in the ORIF group (9.5% vs 39%, P <.001).
Conclusion: Surgeons should consider ORIF for unstable ankle fractures in active young patients with Weber type C, pronation type injury, and comminuted fibular and trimalleolar fractures.
DOI: 10.1177/2473011421S00138
Efficacy of Hook-Type Locking Plate and Cancellous Screw in the Treatment of Displaced Medial Malleolar Fractures in Elderly Patients
Introduction/Purpose: We aimed to compare the midterm radiologic and clinical results between hook-type LCP and conventional malleolar screws for elderly medial malleolar fractures. We hypothesized that elderly patients treated with the hook- type locking compression plate (LCP) would have better fracture healing and clinical outcomes than those treated with cancellous lag screws, with fewer postoperative complications.
Methods: In total, 258 patients treated with a hook-type locking plate (hook LCP group: 121 patients) or partially threaded cancellous lag screws (screw group: 137 patients) over 65 years of age with at least 36 months’ follow-up were included in this retrospective study. Radiographic assessments included the union rate and interval to fracture union. Clinical assessment was performed using the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score, Olerud and Molander score (OMAS), visual analog scale (VAS) pain score, and postoperative complications.
Results: The comminuted fracture rate was higher in the hook LCP group than in the screw group (p < .001). The interval to fracture union was significantly shorter in the LCP group than in the screw group (10.2 +- 7.0 vs. 12.3 +- 6.7, p =.015). There were no significant differences between the two groups regarding AOFAS, OMAS, and VAS pain scores at the final follow- up. There was a trend toward a lower rate of complications, including revision procedures, in the hook LCP group than in the screw group (19.9% vs. 28.5%, p =.107 and 6.6% vs. 13.9%, p =.074). The overall cost in the hook LCP group was 5.8% lower than that of the screw group despite the higher cost of the hook-type LCP.
Conclusion: Hook-type LCP may be an alternative option for treating medial malleolar fractures with comminution in elderly patients.
DOI: 10.1177/2473011421S00139
Retrospective Study Analyzing Trends in Antibiotic Use in Patients with Osteomyelitis of the Ankle and Foot
Shivan N. Chokshi; Tsola Efejuku; Daniel Jupiter, PhD; Jie Chen, MD, MPH; Vinod K. Panchbhavi, MD, FACS
Category: Ankle; Hindfoot; Midfoot/Forefoot
Keywords: Outcomes Measures; Ankle; Bone Orthobiologics
Introduction/Purpose: Antibiotic resistance has quickly become one of the most pressing current public health challenges. Many studies have analyzed general prescription trends, but little information exists about how antibiotic therapy is utilized in orthopedic practice- particularly in patients with Osteomyelitis of the Ankle and Foot. Thus, a retrospective analysis was performed using EMR data to understand temporal tends in antibiotic use, as well as the impact of patient-specific factors on antibiotic use.
Methods: Patients with Osteomyelitis of the Ankle and Foot who were given antibiotics within 12 weeks of their diagnosis were identified in the EMR database using ICD 10 codes (M86.17, M86.67, M86.8X7, M86.171, M86.172, M86.27, M86.679, M86.279, M86.671, M86.672, M86.07, M86.271, M86.37) for foot and ankle Osteomyelitis and the VA Drug Classification Code (AM000) for antibiotics. We then stratified these patients by age (0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69,70-79, 80-89, 90-99), gender (male, female), and year by decade (2001, 2010, 2020). In addition, pre-disposing risk factors of Osteomyelitis, such as Diabetes, Hypertension, and Chronic Ischemic Heart Disease, were analyzed for association with antibiotic use.
Results: Our search identified 85,767 patients, of whom 50,043 (58.35%) received antibiotics within 12 weeks of Osteomyelitis diagnosis. Overall, Males (60.01%) were slightly more likely than Females (54.88%) to use antibiotics. Stratification by age revealed a skewed distribution with the highest incidence of antibiotic use seen in 50-59 year-olds (61.93%). This was more than double the incidence of antibiotic use seen among 20-29 year-olds (30.63%). Additionally, we discovered notable increases in antibiotic usage over time. The most substantial increases occurred from 2001 to 2010 (14.08% to 33.71%, respectively) and 2010 to 2020 (33.71% to 60.51%, respectively). Lastly, patients with pre-existing co-morbidities were found to have a higher usage of antibiotics, when compared to patients without the co-morbidity. Specifically, prior Hypertension increased use by 11.73%, followed by Chronic Ischemic Heart Disease (10.50% increase) and Diabetes (8.40% increase). The above differences were found to be statistically significant at a p-value of <.0001.
Conclusion: This analysis provides insight into present and past antibiotic usage in patients with Foot and Ankle Osteomyelitis. Overall, patients aged 50-59, males, and with Chronic Ischemic Heart Disease are the most likely to take antibiotics within 12 weeks of their diagnosis. This is all against the background of rising antibiotic use, with notable increases since 2001. The data necessitates a deeper look into antibiotic use in patients with foot and ankle injuries as a whole.
DOI: 10.1177/2473011421S00140
Anterior Capsule Reconstruction in the Setting of PVNS
Aman Chopra; Eric Z. Lukosius; Selene G. Parekh, MD, MBA
Category: Ankle; Other
Keywords: Ankle; Outpatient; Ankle
Introduction/Purpose: Pigmented villonodular synovitis (PVNS) is a rare benign proliferative disease affecting tendon sheaths and synovial tissue. Most cases of PVNS arise in the hip and knee joints, while < 5% of total cases occur in the foot and ankle. PVNS of the ankle has a high rate of recurrence and can be destructive to the affected joints if incompletely removed. This case series analyzes functional outcomes after PVNS surgical resection and anterior ankle capsular reconstruction, using a novel technique.
Methods: This case series included three patients who underwent surgery between 2010 and 2020 for their ankle pain and swelling caused by PVNS. The surgical technique involved a posterior, midline approach for PVNS resection of the affected ankle joint, followed by a standard anterior approach for capsular excision. Subsequent anterior capsular reconstruction was performed with a regenerative tissue matrix and a bioresorbable anchoring system. Preoperative and postoperative range of motion testing for the ankle and subtalar joints were assessed along with appropriate radiographs and MRI imaging.
Results: All three surgical procedures for PVNS of the ankle resulted in successful recovery and promising clinical outcomes. The mean cohort age was 43.7 (R:36-58) years and follow-up period was 52.3 (R:4-123) months. Preoperative ankle dorsiflexion and plantarflexion along with subtalar inversion and eversion range of motion were all normal. Postoperative ankle motion and subtalar motion were recorded at final follow up and found to be unchanged. No complications or recurrence of PVNS occurred.
Conclusion: This case series demonstrates that PVNS surgical resection and anterior ankle capsular reconstruction is a safe and effective treatment modality that allows for maintenance of pre-operative motion. Further investigation is warranted to better understand the clinical outcomes of this surgical technique on PVNS recurrence.
DOI: 10.1177/2473011421S00141
Clinical and Patient Reported Outcomes Following Peroneus Brevis Reconstruction with Hamstring Tendon Autograft
Bopha Chrea, MD; Stephanie K. Eble; Jonathan Day; Oliver B. Hansen; Martin J. O’Malley, MD; Scott J. Ellis, MD; Mark C. Drakos, MD
Introduction/Purpose: Peroneal tendon injuries are a common cause of lateral ankle pain and instability. While the use of hamstring autograft has been proposed as a viable surgical option for peroneus brevis reconstruction, reported outcomes with this technique are limited in the literature. We present patient-reported and clinical outcomes for patients who underwent peroneus brevis reconstruction with hamstring autograft.
Methods: Thirty-one patients were retrospectively identified who underwent peroneus brevis reconstruction with hamstring autograft for peroneal tendinopathy between February 2016 and May 2019. All patients who had a peroneus brevis reconstruction were included and all concomitant procedures were noted. Patient-Reported Outcomes Measurement Information System (PROMIS) surveys were prospectively collected preoperatively and at a minimum of 1 year postoperatively (average 24.25, range 12-52.70) months. Retrospective chart review was performed to evaluate the incidence of postoperative complications and reoperations at an average of 30.23 (range, 14.62-53.72) months.
Results: When evaluating pre and postoperative patient-reported outcome surveys (n=26; 84%), on average patients reported improvement in every PROMIS domain evaluated, with significant improvement in Physical Function (+5.99; p=0.006), Pain Interference (-8.11; p<0.001), Pain Intensity (-9.02; p<0.001), and Global Physical Health (+7.29; p=0.001). Three patients reported persistent pain at a minimum of 1 year postoperatively of which 2 required re-operation. No patient reported persistent pain or discomfort at the harvest site of the hamstring autograft.
Conclusion: Patients undergoing peroneus brevis reconstruction with hamstring autograft experienced excellent patient- reported and clinical outcomes. Few postoperative complications were observed, and patients reported improvements across all patient-reported outcome domains, with significant improvements for pain and function domains. Reconstruction with hamstring autograft represents a viable surgical option in the setting of peroneal tendinitis or tears.
DOI: 10.1177/2473011421S00142
Comparing Open vs Minimally Invasive Techniques for the Correction of Hallux Valgus: Clinical and Patient Reported Outcomes
Bopha Chrea, MD; Jonathan Day; Daniel M. Dean, MD; Rose E. Cortina, MD; Megan Reilly, MD; Kristin C. Caolo, BA; Rebecca A. Cerrato, MD; A. Johnson, MD
Introduction/Purpose: Multiple operative techniques have been developed for hallux valgus with varying success. While correction has been traditionally achieved through open surgical approaches, there has been a growing interest in minimally invasive surgical (MIS) techniques. The purpose of this study was to compare clinical and patient-reported outcomes for patients undergoing hallux valgus correction with Lapidus, Scarf and MIS. Our hypothesis was that while a superior clinical correction would be achieved with open techniques there would be similar patient-reported outcomes among open and MIS techniques.
Methods: A total of 257 patients who underwent Lapidus (n=82), Scarf (n=82) or MIS (n=93) hallux valgus correction between January 2017- January 2020 at one of two academic institutions by 1 of 9 foot and ankle-fellowship trained orthopedic surgeons were included in this study. Only 3 of 9 performed MIS correction. The average age at the time of surgery 55.4 (range 14-79). Patients were required to have a minimum baseline and 1-year postoperative Patient-Reported Outcomes Measurement Information Scores (PROMIS) and minimum 3-month clinical follow-up. Retrospective chart review was performed to assess the incidence of postoperative complications and reoperations, with an average clinical follow-up of 8 months.
Results: All groups had statistically significant differences between pre- and post-operative measurements of HVA, IMA, DMAA, and tibial sesamoid position (<0.05). In addition, the Lapidus group demonstrated change in all parameters measured including Meary’s angle, sagittal IMA and Seiberg index. All groups had statistically significant improvement in the PROMIS physical function, pain interference, and global health physical at 1 year (p<0.05). The Lapidus group had significant improvement in all 6 PROMIS domains measured. There were no significant differences in PROMIS score changes from pre to post-op for any PROMIS domain when comparing MIS vs Scarf vs Lapidus. Complications: Minor Complications were classified as infection, symptomatic hardware, delayed union, nerve irritation, transfer metatarsalgia (Lapidus n=14 (17.1%), Scarf n=2 (2.4%), MIS n=15 (16.1%)). Major complications were classified as nonunion, recurrence, hallux varus, recurrence (HVA >20) (Lapidus n=7 (8.5%), Scarf n=9 (11.0%), MIS n=9 (9.7%)).
Conclusion: In the last decade, there has been a growing interest in the use of minimally invasive surgical MIS techniques for the treatment of hallux valgus. When compared with traditional open techniques using Lapidus and Scarf osteotomies MIS presents a safe and effective approach to treating hallux valgus.
DOI: 10.1177/2473011421S00143
Influence of Complications and Revision Surgery on Fulfilment of Expectations in Foot and Ankle Surgery
Bopha Chrea, MD; Jonathan Day; Jensen K. Henry, MD; Elizabeth Cody, MD; Scott J. Ellis, MD
Introduction/Purpose: Fulfilment of patients’ expectations following foot and ankle surgery has been previously studied, and shown to be an effective modality in assessing patient-reported outcomes (PROs). While this assessment has been shown to correlate well with patient satisfaction and other validated PROs, the impact of postoperative complications on fulfilment of expectations is unknown. The aim of this study is to therefore investigate the impact of postoperative complications on fulfilment of patients’ expectations.
Methods: Preoperatively, patients completed a validated Foot and Ankle Expectations Survey consisting of 23 questions encompassing domains including pain, ambulation, daily function, exercise, and shoe wear. At 2 years postoperatively, patients answered how much improvement they received for each item cited preoperatively. A fulfilment proportion (FP) was calculated as the amount of improvement received versus the amount of improvement expected. Chart review was performed to identify patient demographics, comorbidities, pain management, and postoperative complications, which were classified as minor (infection requiring antibiotics) or major (return to OR for revision, deep infection). FP in patients with a complication was compared to patients who did not experience a complication. In addition, the Foot and Ankle Outcomes Score (FAOS), satisfaction, and Delighted-Terrible scale (how they would feel if asked to spend the rest of their life with their current foot/ankle symptom) were collected at final follow-up.
Results: Of the 271 patients (mean age 55.4 years, 65% female), 31 (11.4%, mean age 53.6, 58% female) had a postoperative complication: 25 major (19 revisions, 6 deep infections requiring I&D), 4 minor (4 superficial infections requiring antibiotics), and 2 major and minor (revision and superficial infection). Average time from complication to completion of fulfilment survey was 15 (+- 3.6) months. The groups were similar in diagnoses. Complications were associated with significantly worse FP (0.69 +- 0.45 vs 0.86 +- 0.40, p=0.02). Having a complication significantly correlated with worse satisfaction, Delighted-Terrible scale, and FP (p<0.001). FAOS domains were similar between groups preoperatively; postoperatively, patients without complications had significantly higher ADL and QoL scores (p<0.05). Demographically, there was no difference in age, sex, BMI, Charlson Comorbidity Index, depression/anxiety, or pain management between the two groups.
Conclusion: Our data suggests that postoperative complications following foot and ankle surgery are associated with worse patient-reported fulfilment of their surgical expectations even after recovery from the initial surgery and complication. This finding is independent of preoperative expectations, and correlates with patient satisfaction with their procedure. Therefore, while patient-perceived fulfilment following foot and ankle surgery is multifactorial, the incidence of a postoperative complication negatively impacts fulfilment as well as satisfaction following surgery.
DOI: 10.1177/2473011421S00144
Do Custom Orthotics Help Improve Pain and Function in Patients with Progressive Collapsing Foot Deformity
Christy Christophersen, MD; Sean Zeller; Alicia M. Gotcsik; Gabriel A. Ramirez; Caroline Thirukumaran, MBBS, PhD, MHA; Judith F. Baumhauer, MD, MS, MPH
Introduction/Purpose: Progressive collapsing foot deformity presents with pain, deformity and functional limitations affecting quality of life. The prevalence of this condition ranges from 3-10% depending on the age and sex of the patient. Sixty percent of patients have concurrent medical problems that may delay or limit the ability to undergo surgical intervention. Non-operative treatments such as ankle bracing or custom orthotics are costly and their value to improve pain and function has not been examined with validated patient-centered instruments, specifically patient reported outcome measures. The purpose of this study was to assess if use of a modified UCBL orthosis improved PROMIS pain interference (PI) and physical function (PF) in patients with progressive collapsing foot deformity (PCFD).
Methods: Prospective PROMIS data (PF, PI) was obtained from 2015 to 2020 for all patients who obtained a modified UCBL orthosis for PCFD. Patients with PROMIS data pre- and post-obtaining an orthotic with a minimal follow up of 90 days were included. Patients who elected to pursue operative treatment after receiving the orthotic were noted using CPT codes. Patients without complete evaluations were excluded (Figure 1). The primary outcome was PROMIS Scores (PF and PI) before and after orthotic usage. Covariate analysis included patient demographics including age, gender, marital status, race and ethnicity, and orthotic laterality. We estimated separate mixed effects linear regression models with patient random effects for each PROMIS outcome.
Results: There were 282 patients included in our cohort with an average age of 57 years. 61% were female and 87.8% were White. Patients had an average follow-up of 467 days +/- 366. Multivariate analysis indicates that there was a 0.94 decrease in PROMIS PF t-score relative to orthotic usage at final follow up (p = 0.035 +/- 7.47) with an increase of 0.76 PROMIS PI t-score (p value = 0.085 +/- 7.40). Despite limited measureable impact on PROMIS outcomes using custom orthotics, only eleven patients subsequently pursued surgery and underwent operative fixation at an average of 461 days after initial evaluation. There were no differences in regard to race, ethnicity or orthotic laterality and PROMIS scores.
Conclusion: Publications have focused on outcomes of operative treatment for FCFD, with few examining orthotics. Our study demonstrates a lack of pain and functional improvement with a modified UCBL questioning the potential value of this costly item. However, despite this only 3.9% of patients subsequently underwent surgery. This work raises additional questions: ‘What does the patient hope to improve with treatment?’ ‘What is the role of risk assessment in patients considering treatment choices?’ Patient reported outcomes can be used in shared decision making, not only to align expectations, but also when allocating healthcare dollars to durable medical goods.
DOI: 10.1177/2473011421S00145
Low Tibial Valgization Osteotomy for Varus Ankle Arthritis: Does Age Effect the Outcome?
Kyung Ah Chun, MD; Jun Young Choi, MD; Jin Soo Suh, MD, PhD
Introduction/Purpose: Evidence-based literature identifying the age limit for low tibial valgization osteotomy (LTO) is lacking to date. We addressed the following research questions: (1) is LTO effective for ankle arthritis in patients over 65 years?; (2) does patients’ age alter the effectiveness of LTO?; and (3) does preoperative Takakura stage affect the degree of correction in patients over 65 years?
Methods: We retrospectively reviewed the radiographic and clinical findings of 49 cases which underwent LTO. Patients were divided into two groups according to age at operation (19 cases in group 1 aged >=65 years and 30 cases in group 2 aged <65). Patients in a single group were regrouped into two subgroups according to preoperative Takakura stage (stage II+IIIA versus IIIB) to determine if the degree of correction varied in Takakura stage IIIB.
Results: Significant changes in radiographic parameters were observed with no significant differences in the amounts of correction between groups 1 and 2. Comparison of Takakura stage II+IIIA in group 1 to that in group 2 and stage IIIB in group 1 to that in group 2 revealed no significant differences in the amounts of correction.
Conclusion: LTO could be indicated for patients over 65 years if patient selection was appropriate. LTO in patients over 65 years showed similar radiographic improvements to those in younger patients, and the correction was successfully maintained during the follow-up period. The correctional power of all radiographic parameters did not vary by preoperative Takakura stage.
DOI: 10.1177/2473011421S00146
Considering the Normal Tibial Values of Axial Rotation in Adults for Deformity Correction Osteotomies and Post-Operative Evaluation of Complex Tibial Fractures
Introduction/Purpose: Tibial torsion has been mainly analyzed in pediatric deformities of lower limbs. Nevertheless this parameter has acquired relevancy in treatment of rotational deformities in adult population, that require axial correction. There are few articles that report normal values of tibial torsion, mostly in children, parameter that must be corrected in deformities to improve long term outcomes. Normal values in our population need to be established for preoperative planning and corrections. Our objective is to establish a normality parameter of tibial torsion in adults, that helps us in surgical planning of tibial rotational mal alignment and evaluation of the postoperative axial axis in complex tibial fractures.
Methods: Descriptive study. We analyzed 18 computed tomography of 18 patients (35 tibias), through the Horos v.3.3.5 program, specifically in the 3D curved-MPR. Inclusion criteria: adult patients, without prior knee, leg or ankle deformities, without post-traumatic sequelae of the limb. Exclusion criteria: severe osteoarthritis of the knee or ankle, presence of osteosynthesis material in the limb, presence of previous osteotomies. Measurements were performed in standardized form previously defined by two foot and ankle orthopedic surgeons. We establish the comparison between both legs of each patient to determine posible variability and measurement interobserver correlations through kappa values.
Results: All continuous variables are reported as means +- standard deviations. Student t-test was performed for continuous variables depending on the normality of the data distribution. We also performed de paired t-test to identify any significant differences in left and right tibial measurements. Statistical analyses were carried out by an independent statistician using Stata 16 statistical software. Measurements were performed establishing parameters in axial cuts of the tibia and overlapping two images previously determined. 18 patients (35 tibias) were measured, one limb was deleted for severe compromise the tibial plafond by osteoarthritis. 15 male and 3 female patients with an average of 65 years old (62-76 years). Mean external rotation of the distal tibial was 33° (16.1°-49.8°), difference between left and right tibias was in mean values of 1.95°, not being considered statistically significant. Interobserver correlation was reported at 97% in left tibia and 98% in the right, by intraclass correlation.
Conclusion: Tibial torsion is an important component when correcting tibial axial deformities in adults. Our study shows higher normal values than the ones reported in current literature, but it is important to mention that the best parameter of evaluation is the comparison with the contralateral extremity of each patient.
DOI: 10.1177/2473011421S00147
Presence of Complications in the Transition of a Bone Transport to a Definite Internal Fixation System without Pin Holiday: Case Report
Introduction/Purpose: Bone transports are an alternative in the treatment of severe injuries of lower extremities. They are generally associated to axis problems, delayed bone union in the docking site and pin infection. There is no evidence in the need of having a window period between the transport system and the definite internal fixation. Objetive: Describe the complications seen in a group of 6 patients that went through a tibial bone transport with circular external fixator and posterior internal fixation without pin holiday.
Methods: Restrospective and decriptive study of 6 patient that went through tibial bone transport between 2012-2019, in a level 1 trauma center. Inclusion criteria considered patients >18 years old, with intra or extramedular internal fixation systems. We registered different parameters including patients comorbilities, transport time, transport index, type of internal fixation used and complications during the time of observation and treatment. We registered our clinical evaluation and both laboratory and imagenologic exams.
Results: 100% of patients were men, with an average of 35.8 years old (22-48 yo). 66% of injuries compromised distal tibia, 83% considered open fractures. Average transport length was 7.43 centimeters (3-11cms) in 3.5 months (1.3-6 months), with average follow up of 52 months (24-72months). Tibial transport index in our study was of 1,2month/cm. The main complication in our study was bone consolidation delay in the docking site (50%), and 33% presented deep infection, all of them in the open fracture group.
Conclusion: Pin holiday has been justified by the reduction in pin site infection. In our series there where no pin site infection cases, and only two deep infections which were associated with an important soft tissue injury that required free flap coverage.
DOI: 10.1177/2473011421S00148
Clinical Outcomes of Nano Arthroscopy in the Office Setting for the Treatment of Anterior Ankle Impingement
Christopher Colasanti; Nathaniel P. Mercer; Jeremie Garcia; Tobias Stornebrink, MD; Gino Kerkhoffs, MD; Jari Dahmen, BSc,BSc(Med); John G. Kennedy, MD, FRCS(Orth)
Category: Ankle; Arthroscopy
Keywords: Ankle Arthroscopy; Talus; Sports
Introduction/Purpose: The hypothesis was that IONA would provide the patient with a unique experience of their pathology and facilitate their rapid recovery through an awareness of their own condition, and that using IONA would accelerate recovery to sports-specific activities compared to the literature using standard arthroscopic procedures.
Methods: This was a retrospective cohort study investigating patients who underwent IONA for anterior ankle impingement between 2019 and 2020. Clinical outcomes were evaluated using the following methods preoperatively and at final follow-up: The Foot and Ankle Outcome Scores (FAOS) and Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Interference and Pain Intensity domains. A five-point Likert scale regarding patient satisfaction was evaluated at final follow-up. Wilcoxon signed-rank test was performed to compare preoperative and postoperative outcome scores.
Results: Thirty-one patients were included in this study, which included eighteen males and thirteen females with a mean age of 41.7 +- 15.5 years (range, 17-69 years) and a mean body mass index (BMI) of 27.3 +- 5.7 kg/m2 (range, 19.37-41.5). The mean follow-up time was 12. +- 1.9 months (range, 11-15 months). There were 27 patients who participated in sports activity prior to IONA-arthroscopy procedure. Of those, 26 patients (96%) returned to their sports activities. The median time to return to sports was 3.9 weeks (range, 1.5 to 12 weeks). Patients reported an overall positive experience with a mean rating scale of 9.71 +- .8 (range, 6 to 10). Twenty-seven patients (87%) reported the highest rating (10/10) for overall positive experience and felt that seeing their procedure in real-time aided in their understanding of their underlying pathology. Lastly, twenty-nine patients (94 %) expressed willingness to undergo the same procedure again.
Conclusion: The current study demonstrates that IONA treatment of anterior ankle impingement results in significant pain reduction, a low complication rate, and excellent patient-reported outcomes with high rates of return to work/sport. Additionally, IONA for anterior ankle impingement leads to high patient satisfaction with a significant willingness to undergo the same procedure again.
DOI: 10.1177/2473011421S00149
Inter-Rater and Intra-Rater Reliability of the Lawrence and Botte Classification System of Fifth Metatarsal Base Fractures
Michelle M. Coleman, MD, PhD; Naudereh B. Noori, MD; Mostafa Abousayed, MD, MSc; Neeta Shenvi; Devin R. Mangold, MD; Patrick M. Kennedy; Casey Kuripla, MD; Walter C. Hembree, MD; Niall A. Smyth, MD; John Thompson, MD; Stuart D. Miller, MD; Kirk Easley, Gr
Category: Trauma; Midfoot/Forefoot
Keywords: Fifth Metatarsal Fractures; Fractures; General Principles / Context
Introduction/Purpose: Fractures of the proximal fifth metatarsal are common injuries with a unique history. Treatment of these fractures is controversial, in part due to confusion regarding the nomenclature of the fracture subtypes. The most commonly utilized classification system is the Lawrence and Botte classification, which separates fractures into zones 1, 2, and 3 based on their relationship to the tuberosity and the 4th-5th intermetatarsal articulation. The purpose of this study was to evaluate the inter-rater and intra-rater reliability of the Lawrence and Botte classification of fifth metatarsal base fractures.
Methods: Thirty sets of x-rays representing an equal number of zone 1, zone 2 and zone 3 fractures of varying chronicity were sent to eleven fellowship trained orthopedic foot and ankle surgeons. Surgeons were asked to classify each fracture according to the Lawrence and Botte classification system (round 1). No review of the classification system or visual aids were provided. Two weeks later, the same set of x-rays were reordered and renumbered in a random fashion. The surgeons then re-classified each fracture in a blinded fashion under the same conditions (round 2). Inter-rater and intra-rater reliability was summarized using the kappa statistic. To determine the source of variability between the zones, additional analyses were performed to determine the kappa statistic for a) combined zone 1 and 2 fractures versus zone 3 fractures and b) combined zone 2 and 3 fractures versus zone 1 fractures.
Results: The Lawrence and Botte classification demonstrated substantial overall inter-rater agreement for both rounds 1 and 2 (kappa = 0.66 and 0.65, respectively). Zone 1 fractures demonstrated the highest inter-rater reliability (kappa = 0.83 and 0.83). There was moderate agreement for zone 2 fractures (kappa = 0.51 and 0.50). There was substantial agreement for zone 3 fractures (kappa = 0.64 and 0.65). Dichotomous evaluation of the zone 1 vs. combined zones 2-3 boundary yielded excellent agreement (kappa = 0.83, 0.83). The combined zones 1-2 vs. zone 3 boundary yielded a much lower agreement (kappa = 0.66, 0.65). Intra-rater reliability varied by individual, with kappa values ranging from 0.60 to 0.90, corresponding to modest to almost perfect agreement.
Conclusion: The Lawrence and Botte classification system has overall substantial inter-rater and intra-rater reliability, but assessment of the interface between zone 2 and zone 3 fractures is much less reliable than that between zone 1 and zone 2. Previous studies of isolated zone 1 fractures most likely contain a homogenous fracture cohort, while studies of zone 2 or zone 3 fractures are likely to include a mixture of fracture types. Future studies may utilize supplemental imaging or modify the classification to best determine treatment of these more distal fractures.
DOI: 10.1177/2473011421S00150
Mid-Term Results after Lateral Transfibular Approach Total Ankle Arthroplasty
Michelle M. Coleman, MD, PhD; Mostafa Abousayed, MD, MSc; Cesar de Cesar Netto, MD, PhD; Moses Lee, MD; Camilla Maccario, MD; Thomas I. Sherman, MD; Lew C. Schon, MD
Introduction/Purpose: Continued improvements in total ankle arthroplasty (TAA) implant design have led to promising clinical outcomes. The lateral transfibular approach TAA allows for excellent visualization of the center of rotation of the ankle and allows for correction of rotational and sagittal deformity by shortening or lengthening of the fibula. Furthermore, the curved implant design allows for minimal bony resection. The purpose of this study is to report the medium-term clinical and radiographic results for consecutive patients who underwent the lateral approach TAA.
Methods: IRB approval was obtained for this study. Consecutive patients who underwent lateral approach TAA for tibiotalar arthritis by a single surgeon were enrolled on a prospective basis from January 2013 to June 2015. This time period represented the initial case series of TAA performed by the surgeon. Patient reported outcomes (PROs) were collected including the Ankle Osteoarthritis Scale (AOS), 12-item short-form survey (SF-12), and Visual Analogue Pain Scale (VAS). The need for subsequent procedures was recorded. Radiographs were evaluated for preoperative and postoperative alignment using the lateral distal tibial angle (LDTA), tibiotalar surface angle (TTS), anterior distal tibia angle (ADTA), and the lateral talar station (LTS). Radiographs were also evaluated for the development of peri-implant lucency and subsidence. Data was tested for normality. T-tests were used to determine differences between preoperative data and postoperative data. A p<0.05 was considered significant.
Results: 53 patients who underwent 59 TAA procedures were included. Average follow-up was 5.7 +/- 0.9 years. Average age was 53 +/- 7.0. Comorbidities included smoking (11/53), diabetes (6/53), and prior procedures (33/53). Sixteen ankles (27%) underwent one or more subsequent procedures including gutter debridement (7/59), debridement for periprosthetic infection (3/59), and removal of hardware (7/59). All fibular osteotomies healed. Four ankles had asymptomatic peri-implant lucency or cysts (4/59). No patients had subsidence or required revision of the tibial or talar components. Coronal and sagittal alignment were significantly improved for all measures (p<0.05). VAS scores improved from a mean of 7.5 preoperatively to 1 at final follow- up (p<0.0001). SF-12 physical component scores improved from 34 to 41.5 (p=0.0227). AOS scores improved from 54.8 to 19.1 (p<0.0001).
Conclusion: At medium term follow-up, patient reported outcomes remain significantly improved in patients after lateral approach TAA. There were very few radiographic findings of lucency and cyst formation, and all of these were asymptomatic. No revision of metal implants was required. Excellent deformity correction was achieved. The rate of subsequent procedures was high, although the rate of actual component revision was 0%. Lateral approach TAA appears to have overall good outcomes at medium term follow-up.
DOI: 10.1177/2473011421S00151
Risk Factors for Complications Associated with Minimally Invasive Medial Displacement Calcaneal Osteotomy
Michelle M. Coleman, MD, PhD; Mostafa Abousayed, MD, MSc; John Thompson, MD; Bryan Bean, MD; Gregory P. Guyton, MD
Category: Hindfoot
Keywords: Medial Displacement Calcaneal Osteotomy; Minimally Invasive; Valgus
Introduction/Purpose: Several minimally invasive medial displacement calcaneal osteotomy (MIS MDCO) techniques have been described utilizing differing methods for creating the osteotomy. However, there are few clinical reports of the safety profile and outcomes after percutaneous MDCO procedures. The purpose of this study was to describe short-term outcomes and complications associated with MIS MDCO for the correction of hindfoot valgus deformities.
Methods: A retrospective study was conducted of all patients who underwent consecutive minimally invasive MDCO for the treatment of a hindfoot valgus deformity by a single fellowship-trained foot and ankle orthopaedic surgeon from September 2013 to August 2018. Demographic data, treatment data, and complications were recorded from the electronic medical record for the duration of the patient’s follow-up. Univariate statistics were used to determine the relationship between complications and demographic/treatment variables. A p<0.05 was considered significant.
Results: Patients who underwent 189 MIS MDCO procedures were included in the study. Median follow-up was 12 months (interquartile range, 7 to 25 months). Osteotomy healing complications were present in 7% of cases. A 12-month cluster of osteotomy healing complications was observed. Healing complication rates were 28% during the cluster and 0.7% outside of the cluster. Osteotomy healing complications were significantly associated with higher American Society of Anesthesiologists (ASA) classification, female sex, current tobacco use, and higher body mass index (BMI). Healing complications were not associated with osteotomy technique (saw vs. burr) or fixation type. Other complications included wound dehiscence (3%), surgical site infection (2%), transient nerve symptoms (6%), and persistent nerve symptoms (2%). Nerve symptoms were significantly associated with an increased number of concomitant procedures.
Conclusion: Patients with higher ASA classification, current tobacco use, and higher BMI were at higher risk for osteotomy healing complications after minimally invasive MDCO procedures. Patients were also more likely to develop nerve complications with more extensive surgical procedures. These findings may be useful for surgeons when counseling patients regarding their surgical risks and when optimizing their comorbidities preoperatively.
DOI: 10.1177/2473011421S00152
Risk Factors for Nonunion in Pediatric Lateral Column Lengthening (Mosca) Procedures
Michael J. Conklin; Shane F. Strom; Alexandra H. Seidenstein; Nicholas A. Andrews; Jared R. Halstrom, BS; John S. Doyle; Ashish Shah, MD
Introduction/Purpose: The Evans/Mosca procedure remains the most utilized extra-articular osteotomies for correction of pes planus. This desired lengthening is created by inserting a graft in the anterior aspect of the calcaneus through a complete transverse osteotomy. Failure of conservative methods, particularly for rigid pes planus, is a primary consideration for surgical management. Complications of the Evans procedure include delayed union, nonunion, malunion, subluxation of the calcaneocuboid joint, and persistent lateral column pain. Our study analyzes risk factors for development of non-union.
Methods: After IRB approval 120 patients charts and 157 feet were analyzed for incidence of non-union which was defined by clinical and radiographic evidence of absence of union >6 months. Delayed union was diagnosed if there was clinical evidence of healing without complete union at >6 months. Exclusion criteria included age >18 and revision lateral column lengthening. Patients’ medical records were reviewed for basic demographics, complications, and surgical technique.
Results: The cohort consisted of 75 females (47.8%) and 82 males (52.2%). The median age was 12 with an interquartile range (IQR) of 3. A total of 6 patients (3.7%) had wound complications or nerve injury. Nonunion occurred in 7 of 157 feet (4.5%) with 2 of 157 feet (1.3%) experiencing delayed union. The median age for patients with nonunion was significantly higher than those who achieved union (13.2 (IQR 2.75) vs. 11.2 (IQR 3) respectively). The fixation construct used was associated with increased risk of nonunion. Patients with screw fixation had the highest rate of nonunion at 50% (2/2) compared to pin and/or staple fixation at 6.8% (5/73), no fixation at 4% (3/75), and plate fixation at 0% (0/2). Both delayed union patients were treated with ultrasound bone stimulation, both patients were able to achieve complete union. Revision was attempted in 5/7 nonunions with all operative patients achieving union.
Conclusion: Our study analyzed risk factors for developing non-union in patients undergoing calcaneal lengthening osteotomy for pediatric pes planus. We found age at time of surgery and graft fixation method to be significant risk factors for development of non-union. Our study highlighted that those patients who had non-union was on average >2yrs older at time of surgery. Overall, lateral column lengthening is a well-tolerated procedure with a complication rate, including non-and delayed union, of 10.8%. Surgeons should be aware, in the largest cohort of pediatric Evans/Mosca procedures to date, patient age and type of fixation were associated with nonunion.
DOI: 10.1177/2473011421S00153
Association of First Metatarsal Pronation with Patient-Reported Outcomes and Recurrence Rates in Hallux Valgus
Matthew S. Conti, MD; Tamanna Patel, BA; Jiaqi Zhu; Stephen V. Costigliola; Andrew J. Elliott, MD; Stephen F. Conti, MD; Scott J. Ellis, MD
Introduction/Purpose: Hallux valgus (HV) is a triplanar deformity of the first metatarsal in which the first metatarsal adducts, dorsiflexes, and pronates with an average increase in pronation between 2° and 8° compared with normal patients (Kimura JBJS, Campbell FAI). Despite these radiographic changes of the first metatarsal in patients with HV, no correlation between postoperative two-dimensional radiographic parameters and patient-reported outcomes has been reported (Thordarson FAI). The purpose of this study was to determine if a postoperative decrease in first metatarsal pronation (1MTPronation) was associated with changes in patient-reported outcomes as measured by the PROMIS physical function, pain interference, and pain intensity domains or recurrence rates in patients with HV who undergo a first tarsometatarsal fusion (modified Lapidus procedure).
Methods: This study included thirty-nine consecutive HV patients who underwent a modified Lapidus procedure, had preoperative and >=2-year postoperative PROMIS scores, and had 1MTPronation measured using the previously described triplanar angle of pronation (FAI, in press) on preoperative and at least 5-month postoperative weightbearing CT scans. Multivariable regression analyses were used to investigate differences in the change in PROMIS domains preoperatively and 2-years postoperatively between patients with ‘no change/increased 1MTPronation’ and ‘decreased 1MTPronation.’ No differences in preoperative radiographic parameters or patient characteristics found between two groups. A secondary analysis using multivariable regression modeling was performed to determine if patients with a decrease in 1MTPronation between 2°-8° (‘moderate pronation change’) had greater improvements in PROMIS scores compared with ‘minimal pronation change’ (<2°) and ‘substantial pronation change’ (>8°) groups. A log-binomal regression analysis was performed to identify if a decrease in 1MTPronation was associated with recurrence of the HV deformity (postoperative HVA>=20°
Results: The decreased 1MTPronation group (n=26) had a statistically significant greater improvement in the PROMIS physical function scale by 7.2 points (95% confidence interval (CI) 2.1-12.3, P=0.007) compared to the no change/increased 1MTPronation group (n=13). There were no statistically significant differences in PROMIS pain interference (P=0.380) or pain intensity (P=0.443) scores between the two groups. The secondary analysis found that patients in the moderate pronation change group (n=15) had significantly better improvements in the PROMIS physical function and pain intensity domains than the minimal pronation change group (n=14) (Table 1). The moderate pronation change group also had greater improvements in the PROMIS pain interference and pain intensity domains than the substantial pronation (n=10) change group (Table 1). Recurrence rates were significantly lower in the decreased 1MTPronation pronation group when compared to the no change/increased 1MTPronation group (11.5% and 46.2%, respectively; risk ratio 0.25, 95% CI 0.07-0.84, P=0.025).
Conclusion: In patients undergoing a modified Lapidus procedure for correction of their HV deformity, a postoperative decrease in pronation of the first metatarsal, especially between 2° and 8°, was associated with improvement in PROMIS scores at two- years postoperatively and a lower recurrence rate. These results suggest that the rotational component of the hallux valgus deformity may play an important role in outcomes following surgery, and consequently, surgeons should consider addressing but not overcorrecting the first metatarsal pronation deformity when performing a surgical procedure for the treatment of hallux valgus.
DOI: 10.1177/2473011421S00154
Crista Volume Measured from 3D Reconstructions Shows a Relationship to Sesamoid Station
Stephen F. Conti, MD; Audrey Clarke; Matthew S. Conti, MD; Mark C. Miller, PhD; Scott J. Ellis, MD
Introduction/Purpose: The hallux valgus (HV) deformity results in progressive subluxation of the sesamoids from their position (station) under the plantar surface of the first metatarsal head. This subluxation may result in erosion of the crista that separates the sesamoid grooves due to contact with the tibial sesamoid during weightbearing. While previous work using weightbearing CT (WBCT) scans has suggested that tibial sesamoid position is associated with degenerative change of the sesamoid metatarsal joint (Katsui FAI), no studies have quantified the relationship between sesamoid metatarsal degenerative changes and sesamoid subluxation. The purpose of the current investigation is to examine the relationship of the volume of the crista to first metatarsal pronation and sesamoid station, using three-dimensional models of patients’ deformities created from WBCT scans.
Methods: Thirty-nine HV patients and nine normal subjects underwent weightbearing or simulated weightbearing CT (WBCT) imaging. Crista volume was determined using a line drawn to connect the nadir of each sulcus on either side of the intersesamoidal crista for the length of the crista (Figure 1). The Mann-Whitney U test was used to compare mean crista volume between HV and normal patients. WBCT scans were used to establish sesamoid position using a four-stage scale (Kim FAI 2015) and quantify first metatarsal pronation using 3D reconstructions as previously described (Campbell FAI 2018). Single-factor analysis of variance (ANOVA) tests were used to compared the crista volume and pronation angle between the four sesamoid stations. A linear regression was performed to determine whether crista volume was associated with the pronation angle. Spearman’s rank coefficient (r) was used to test the relationship of the sesamoid station against the crista volume and pronation angle.
Results: The mean crista volume in HV patients was 80.10 mm3 +- 35 mm3 and in normal subjects was 150.64 mm3 +- 24 mm3, which differed significantly between the two groups (P<0.001). Mean crista volumes were found to be statistically significantly different between the sesamoid stations (P<0.001) with decreasing crista volumes significantly and strongly correlated with increasing sesamoid station (r = -0.80, P<0.001). The mean standard deviation values of the crista volume by sesamoid station were 154.4 mm3 +- 18.7 mm3 for station zero, 98.19 mm3 +- 26.9 mm3 for station one, 78.45 mm3 +- 30.1 mm3 for station two, and 44.77 mm3 +- 13.5 mm3 for station three. There was no difference in the mean pronation angle between the four sesamoid stations (P=0.37). Additionally, no statistically significant relationship was found between sesamoid station and pronation angle. The pronation angle was not associated with crista volume (P=0.52).
Conclusion: Our study found that HV patients have significantly lower mean crista volumes compared to normal patients. Crista volume was strongly correlated with sesamoid subluxation/station, suggesting that tibial sesamoid subluxation results in erosion of the crista. In contrast, the pronation deformity was not associated with crista volume demonstrating that the degenerative changes of the sesamoid metatarsal are not related to the rotational deformity of the first metatarsal. This supports the hypothesis that tibial sesamoid subluxation may result in osteoarthritis of the sesamoid metatarsal joint and may be an overlooked source of pain in HV.
DOI: 10.1177/2473011421S00155
Functionality and Outcomes Following Utilization of an Arizona Brace for Non-Operative Foot and Ankle Care
Daniel O. Corr, BS; Francis P. Landman; Joseph T. O’Neil, MD; Steven M. Raikin, MD
Introduction/Purpose: The Arizona ankle foot orthotic (AFO) is a popular custom-molded orthotic stabilizer often used to treat posterior tibial tendon dysfunction, chronic Achilles tendonitis, ankle trauma and other pathologies. In the case of ankle injury or deformity, a resulting proprioceptive deficit may result in functional instability. There exists little evidence demonstrating the effectiveness of an Arizona brace in the course of non-operative treatment with regard to alleviation of pain and a return to standard daily activity. Previous analysis has shown Arizona bracing to be a viable treatment for posterior tibial tendon dysfunction, but is yet to incorporate a larger spectrum of pathologies. Furthermore, patient satisfaction with the brace, and continued use of the brace to aid in function in the longer-term has yet to be assessed.
Methods: Patients who were prescribed an Arizona ankle brace as a means of non-operative treatment at our institution from 2017-2018 were eligible for retrospective study for follow up of 2-4 years. Pre-bracing diagnosis was noted. Eligible patients were contacted via email to complete survey assessments. Patients were asked to use a 5-point Likert scale (0-4) to rate their overall satisfaction with the brace as a treatment device. Patients were also asked to report if they eventually proceeded to surgical intervention, how often they still wear the brace throughout the day, how long they wore the brace if they’d discontinued use, whether the brace was easy to wear, and - if no - what made the brace difficult to wear. Patients also completed two VAS pain rating scales - one when walking with the brace, one when walking without - and the FAAM-ADL subscale to evaluate their level of function.
Results: Surveys were completed by 118 patients with average age 63.2 years and average BMI 31.9 kg/m2. Patients reported an average satisfaction of 2.1/4, with 61 (51.7%) stating they were ‘satisfied’ or ‘very satisfied’ with the brace. At the time of survey, 74 patients (62.7%) reported that they no longer use the brace at all. Sixty responded that the brace was easy to wear, while 58 (49.5%) stated that the brace was difficult to wear, with the most common reason being that the brace was too bulky and difficult to wear with shoes on. Pain rating was significantly lower when walking with the brace versus without (44.6 vs. 63.6, p=0.003). Patients braced for valgus ankle deformity (n=11) had higher FAAM-ADL scores at follow-up than those with ankle arthritis (n=45) or tendonitis (n=36).
Conclusion: The Arizona ankle brace is a worthy first-line nonoperative treatment for a number of ankle pathologies, as it may help to avoid the need for surgical intervention. The brace may be more adept in correcting broad foot/ankle deformities as opposed to bony or tendinous irregularities, and patients should be counseled with regards to the varying patient satisfaction and comfort while wearing the brace. Larger cohort studies are indicated to further investigate diagnostic significance and bracing efficacy.
DOI: 10.1177/2473011421S00156
Medicare Bundled Payment Model for Total Ankle Arthroplasty
Daniel O. Corr, BS; Gandhi Riddhi; Joseph T. O’Neil, MD; Steven M. Raikin, MD; Rachel J. Shakked, MD
Category: Ankle; Other
Keywords: Total Ankle Arthroplasty; Payment Reform; Economic Analysis
Introduction/Purpose: Total ankle arthroplasty (TAA) is included in the Centers of Medicare and Medicaid Services’ (CMS) Bundled Payments for Care Improvement (BPCI) initiative for lower extremity joint replacements. This model has been demonstrated to be for total hip arthroplasty (THA) and total knee arthroplasty (TKA). However, there remains concern that the model underestimates expected costs for TAA due to the unique healthcare needs of TAA patients including higher implant costs, longer procedures, and an increased demand for postoperative acute care services due to non-weightbearing. The purpose of this study was to analyze the breakdown of costs associated with inpatient and outpatient care and assess the difference between Medicare beneficiary reimbursements and actual costs for the episode of care.
Methods: An IRB-approved retrospective review was conducted of patients with Medicare who underwent TAA between July 2014 and June 2018. The surgeries were performed at seven facilities affiliated with a singular institution hospital system. Patients undergoing TAA in this time period were identified using an institutional arthroplasty database and were eligible for study. Of 99 patients who met this criterion, financial data was available for 72. Demographics including age, gender, BMI, and comorbidities were collected via chart review. Episode start and end dates, first post-acute care discharge destination, and total episode costs were recorded. Total episode cost was subdivided into inpatient facility cost, surgeon fees, and post-acute care discharge costs (inpatient rehab facility costs, skilled nursing facility expenses, or home health aide fees). Patients were stratified into two groups based on 90-day costs of care, a ‘positive group’ not exceeding the bundled payment allocation and a ‘negative group’ which did exceed.
Results: No statistically significant difference was found among demographics between the positive and negative patient groups. Average group age was 70.5 years and 72.9 years, respectively, and both groups had average BMI of 29.3 kg/m2. Age-adjusted Charlson Comorbidity Index was 3.35 for the positive group and 3.40 for the negative group. Total episode costs were 50% higher in the negative group compared to the positive group ($31,462 vs. $15,845). The total post discharge costs for the negative group were $17,912 which is significantly higher than those of the positive group ($2,502) (P<0.001). Thirteen patients (18.1%) attended skilled nursing facilities, and 12 of these patients exceeded the allocated budget. Average SNF cost was $13,089, which nearly matched the entire inpatient cost (facility + surgeon fees) of $13,400. Home health aide requirement was significant at 39% (n=28), and 15 of these patients (54%) also came in over budget.
Conclusion: Results suggest that there is a considerable possibility for patients undergoing TAA to have post-acute care requirements that drive cost over budget, including admittance to skilled nursing facilities and home health aide, likely sue to the added necessity for extended immobilization in an older patient population. Such parameters should be factored into the BPCI reimbursement model for TAA.
DOI: 10.1177/2473011421S00157
Novel Minimally Invasive Sliding Calcaneal Osteotomy: A Case Series
Daniel O. Corr, BS; William Conaway, MD; Rabun S. Fox, MD; David I. Pedowitz, MD, MS
Introduction/Purpose: Sliding calcaneal displacement osteotomy is a mainstay in the treatment of hindfoot deformity. A lateral oblique or L shaped incision and direct visualization of the calcaneus is the traditional open approach to this osteotomy. Complications of this approach are not common and include wound dehiscence, delayed union, neurovascular damage, tarsal tunnel syndrome, symptomatic bony overhang and peroneal fibrosis. Several techniques have been developed to address the limitations of the open approach including osteotomy with a Gigli saw, percutaneous endoscopic assisted osteotomy, and most recently minimally invasive osteotomy (MICO) with a low speed, high torque burr. Each of these techniques has limitations. This report presents a simple minimally invasive technique that may help mitigate wound issues without the technical hurdles of a steep learning curve.
Methods: Patients undergoing MICO procedures with the senior author from February 2019 - June 2020 who had not undergone previous foot/ankle surgery were retrospectively enrolled. Patients underwent clinical and radiographic assessment preoperatively as well as at 2, 6, 12, and 24 weeks postoperatively. The technique utilizes a 1.5cm incision along the plane of osteotomy, centered about a K-wire placed through both cortices of the calcaneus at the midpoint of the osteotomy plane. The plane and K-wire placement are determined under radiographic guidance. A micro-sagittal saw is rested on the K-wire and used as a cutting block in the coronal plane. After the osteotomy is created and mobility of the calcaneus confirmed, the K-wire is removed. The mobile segment is adjusted as needed, held in placed by dorsiflexing the ankle, and fixed using two posterior-to-anterior 6.5 cannulated screws, one 1cm superior to the other. The wounds can then be irrigated and closed.
Results: 37 patients were treated using this technique. 24 (65%) patients were female, with average age 56.9 years. Osteotomies were performed concomitantly with procedures including flexor digitorum longus transfer, subtalar fusion, triple arthrodesis, talonavicular fusion, hallux valgus corrective osteotomy, and Strayer gastrocnemius recession. Thirty-five (95%) patients achieved radiographic fusion within 1 year postoperatively with 28 (76%) fusing by 3-month follow up. Two (5%) patients developed a radiographic non-union without instability and opted to be managed expectantly. Of note, one patient is a diabetic current smoker with Rheumatoid Arthritis, while the other is a non-diabetic former smoker. A single patient was readmitted within 90 days for incision and debridement of a dehisced wound from subtalar fusion performed concomitantly. One patient underwent eventual removal of the screw compressing the calcaneal osteotomy site due to hardware prominence. No patients reported peroneal symptoms postoperatively. No patients reported any other complications related to the osteotomy.
Conclusion: Sliding calcaneal displacement osteotomy is a well-established component in the treatment of hindfoot deformity. Although larger lateral oblique and L shaped incisions allow direct visualization of the osteotomy, more minimally invasive approaches have been used. The proposed technique in the current report offers a low non-union rate, minimal surgical footprint, easily available surgical instruments, reliable osteotomy plane, and short surgical time.
DOI: 10.1177/2473011421S00158
How Has Opioid Prescribing in Total Ankle Arthroplasty Changed with Time and State Legislation? A National and State-Level Analysis
Daniel J. Cunningham, MD; Colleen Wixted; Nicholas B. Allen; Andrew Hanselman; Samuel B. Adams, Jr., MD
Category: Ankle; Ankle Arthritis
Keywords: Pain; Outcomes Measures; Total Ankle Arthroplasty
Introduction/Purpose: Total ankle arthroplasty (TAA) is an increasingly-utilized treatment for ankle arthritis, and opioids are commonly used as part of perioperative pain control. However, many states have enacted opioid-limiting legislation to reduce perioperative opioid prescribing. The aim of this study was to evaluate the impact of time and state legislation on perioperative opioid prescribing in TAA.
Methods: This study is a retrospective, observational review of 90-day perioperative opioid prescribing in 1,829 patients undergoing TAA throughout the United States using a large insurance database. Initial and cumulative volumes and rates of opioid prescription filling were recorded along with baseline patient and operative characteristics. Dates of state legislation enactment were also recorded. Student t-tests, analysis of variance (ANOVA), and multivariable linear and logistic regression were utilized to analyze the impact of time and state legislation on opioid prescription filling.
Results: In the 90-day perioperative time period, initial and cumulative opioid prescription filling in oxycodone 5-mg equivalents has decreased significantly from 2010 (63.8 initial and 163.3 cumulative oxycodone 5-mg equivalents filled) to 2019 (41.1 initial and 67.2 cumulative oxycodone 5-mg equivalents filled). States with opioid-limiting legislation saw larger and more significant reductions in initial and cumulative opioid prescription filling pre-act to post-act (63.3 to 50.6 oxycodone 5-mg equivalents filled with legislation vs 61.4 to 51.9 oxycodone 5-mg equivalents filled without legislation initial and 146.4 to 93.3 oxycodone 5-mg equivalents filled with legislation vs 125.1 to 108.6 oxycodone 5-mg equivalents filled without legislation cumulative).
Conclusion: This study demonstrates that orthopaedic surgeons in states with opioid-limiting legislation have responded by significantly reducing 90-day perioperative opioid prescribing in TAA. These results encourage states without legislation to enact opioid-specific laws to reduce opioid prescribing.
DOI: 10.1177/2473011421S00159
Regional Anesthesia Decreases Early Perioperative Opioid Demand but Increases Late Opioid Demand in Ankle and Distal Tibia Fracture Surgery
Daniel J. Cunningham, MD; Ariana Paniagua; Isabel DeLaura; Gloria X. Zhang; Billy I. Kim; Jonathan Kim; Terry Lee; Micaela LaRose; Samuel B. Adams, Jr., MD; Mark Gage; Mark Gage
Category: Ankle; Trauma
Keywords: Pain; Outcomes Measures; Ankle Fracture
Introduction/Purpose: Regional anesthesia (RA) is commonly used in ankle and distal tibia surgery. However, the pragmatic effects of this treatment on inpatient and outpatient opioid demand are unclear. The hypothesis was that RA would decrease inpatient opioid consumption and have little effect on outpatient opioid demand in patients undergoing ankle and distal tibia fracture surgery.
Methods: All patients ages 18 and older undergoing ankle and distal tibia fracture surgery at a single institution between 7/2013 and 7/2018 were included in this study (n=1,310). Inpatient opioid consumption (0-72 hours post-operative) and outpatient opioid prescribing (1-month pre-operative to 90-days post-operative) were recorded in oxycodone 5-mg equivalents (OE’s). Adjusted models were used to evaluate the impact of RA on inpatient and outpatient opioid demand.
Results: Adjusted models demonstrated decreased inpatient opioid consumption in patients with RA (12.1 estimated OE’s without RA vs 8.8 OE’s with RA from 0-24 hours post-op, p<0.001) but no significant difference after that time (9.7 vs 10.4 from 24-48 hours post-op, and 9.5 vs 8.5 from 48-72 hours post-op). Estimated cumulative outpatient opioid demand was significantly increased in patients receiving RA at all timepoints (112.5 OE’s without RA vs 137.3 with RA from one-month pre-op to two- weeks, 125.6 vs 155.5 OE’s to 6-weeks, and 134.6 vs 163.3 OE’s to 90-days, all p-values for RA <0.001). Figure demonstrates a histogram of the inpatient opioid consumption in patients with and without RA.
Conclusion: In ankle and distal tibia fracture surgery, RA was associated with decreased early inpatient opioid demand but significantly increased outpatient opioid demand after adjusting for baseline patient and treatment characteristics. These findings provide information on the real-world impact of RA and temper enthusiasm for perioperative nerve blockade.
DOI: 10.1177/2473011421S00160
State Regulation Positively Impacts Opioid Prescribing Patterns in Ankle Fracture Surgery: A National and State-Level Analysis
Daniel J. Cunningham, MD; Michael Blatter; Samuel B. Adams, Jr., MD; Mark Gage
Category: Ankle; Trauma
Keywords: Ankle Fracture; Pain; Outcomes Measures
Introduction/Purpose: The impact of time and state regulation on opioid prescribing in orthopaedic trauma is not well known. The purpose of this study is to evaluate the impact of time and state-level opioid legislation on 90-day perioperative opioid prescribing in ankle fracture surgery from 2010 - 2019.
Methods: This is a retrospective, cohort study using a national insurance database including commercial insurance, Medicare, Medicaid, and cash pay patients to evaluate 90-day perioperative opioid prescription filling in 40,286 patients ages 18 and older undergoing Current Procedural Terminology codes 27766, 27769, 27792, 27814, 27822, and/or 27823 between 2010 and 2019 in all 50 United States. The primary study outcome was initial and cumulative 90-day perioperative opioid prescription filling and rates of filling and refills.
Results: Mean first prescription volume has not changed dramatically from 2010 (37 oxycodone 5-mg pills) to 2019 (33.3 oxycodone 5-mg pills). However, cumulative prescriptions within the 90-day perioperative timeframe have decreased considerably from 2010 (128.5 oxycodone 5-mg pills) to 2019 (70.4 oxycodone 5-mg pills, p<0.001), and cumulative prescription filling in years 2018 and 2019 was significantly less than in 2010. Legislation targeting duration or duration and volume had the largest impacts on initial and cumulative opioid prescribing (approximately 14-22 fewer oxycodone 5-mg pills filled in states with legislation compared to states without legislation, p<0.001). The figure shows state-level pre-act and post-act cumulative 90-day opioid prescribing in ankle fracture surgery.
Conclusion: In ankle fracture surgery, cumulative opioid prescribing has decreased dramatically over time. In addition, states with opioid prescribing legislation had larger reductions in perioperative opioid prescribing compared to states without opioid legislation. Legislation targeting duration or duration and volume had the largest impacts on opioid prescribing.
DOI: 10.1177/2473011421S00161
Time and State Legislation Have Decreased Opioid Prescribing in Elective Foot and Ankle Surgery in the United States
Daniel J. Cunningham, MD; Nicholas Kwon; Nicholas B. Allen; Andrew Hanselman; Samuel B. Adams, Jr., MD
Introduction/Purpose: The opioid epidemic has focused attention on opioid overprescribing. State legislation has been enacted to reduce acute opioid prescribing. However, the impact of this legislation on elective foot and ankle surgery is largely unknown. The purpose of this study was to evaluate the impact of opioid limiting legislation on opioid prescribing in elective foot and ankle surgery.
Methods: 90-day perioperative opioid prescription filling in oxycodone 5-mg equivalents was identified in all patients ages 18 and older undergoing non-trauma, non-arthroplasty foot and ankle surgery from 2010 - 2019 using a commercial database. States with and without legislation were identified and opioid prescription filling before and after legislation was tabulated. Unadjusted and adjusted analyses were performed to evaluate the impact of time and state legislation on perioperative opioid prescribing in this patient population.
Results: Initial and cumulative opioid prescribing decreased significantly from 2010 to 2019 (39 vs 35.7 initial and 98.1 vs 55.7 cumulative oxycodone 5-mg equivalents, p<0.001). States with legislation had larger and more significant reductions in initial and cumulative opioid prescribing compared to states without legislation over similar timeframes (41.6 to 35.1 with legislation vs 40.6 to 39.1 without legislation initial oxycodone 5-mg equivalents prescription filling volume and 87.7 to 62.8 vs 88.6 to 74.1 cumulative oxycodone 5-mg equivalents prescription filling volume, p<0.001). The figure shows state-level changes in opioid prescription filling from pre-act to post-act.
Conclusion: State legislation and time have been associated with large, clinically relevant reductions in 90-day perioperative cumulative opioid prescription filling although reductions in initial opioid prescription filing have remained low. These results encourage states without legislation to enact restraints to reduce the impact of the opioid epidemic.
DOI: 10.1177/2473011421S00162
Readability of Online Foot & Ankle Patient Resources
Coleman Cush; Brian Foster; Hui Zhang, MD; Gerard J. Cush, MD
Category: Other
Keywords: Patient Education; Ankle; General Principles / Context
Introduction/Purpose: The internet is a popular source of health information for patients. Professional organizations, such as the American Orthopaedic Foot & Ankle Society (AOFAS) and the American Academy of Orthopaedic Surgeons (AAOS) have created patient-directed websites containing high quality information. However, previous studies have demonstrated that these sites are often written at a level that is too complex for the average reader. We aimed to investigate the current landscape of the readability of these websites.
Methods: Online patient resources on foot and ankle topics published by the AOFAS and AAOS were reviewed. Each page was analyzed using the Flesch Kincaid Grade Level (FKGL) and Flesch Reading Ease (FRE) formulas. Sites were noted if they were written at or below an 8th grade reading level, which corresponds to the average US reading level. An independent two-sample t- test or chi-square test, where appropriate, were used to compare resource characteristics between the two professional societies.
Results: 162 total sites were reviewed, including 113 from the AOFAS and 49 from the AAOS. Overall, the mean FKGL was 9.4 (range, 6.7 - 15.3) and the mean FRE was 56.3 (range, 24.4 - 73.1). Websites written by the AAOS had significantly lower FKGL scores than sites written by the AOFAS (9.0 vs 9.5, p=0.01). 31.3% of all sites were written at or below an 8th grade reading level. Websites published by the AAOS had significantly more sites published at this level than sites published by the AOFAS (44.9% vs 25.7%, p=0.02).
Conclusion: Online patient information on foot and ankle topics published by professional organizations are often written at a level that is too complex for the average reader. There was a statistical but not clinically significant difference between sites published by the AAOS and AOFAS. Professional organizations should continue to develop their online patient resources, with emphasis on increasing their readability.
DOI: 10.1177/2473011421S00163
What are the Injures that Lead to Post-Traumatic Ankle Osteoarthritis? A Long-Term Retrospective Analysis of 533 Patients
Chris Cychosz, MD; Nacime S. Mansur, MD; Matthieu Lalevee, MD; William J. Lorentzen; Elijah Auch; Natalie Glass, PhD; Phinit Phisitkul, MD; John E. Femino, MD; Donald D. Anderson; Cesar de Cesar Netto, MD, PhD
Category: Ankle; Ankle Arthritis
Keywords: Ankle Arthritis; Ankle Fracture; Total Ankle Arthroplasty
Introduction/Purpose: Ankle osteoarthritis (AO) is an incapacitating condition for patients and an important burden for medical assistance. It is well known that the vast majority of AO occurs as a sequela of previous trauma, however, it is currently unknown what types of injuries of the foot and ankle most commonly lead end-stage arthritis. The purpose of this study was to investigate the etiology of end-stage ankle osteoarthritis in all patients who underwent ankle fusion or replacement at a tertiary care center over a 20-year period. Our hypothesis was that the most common injury patterns would correspond to low-energy lesions.
Methods: The electronic medical record was queried using current procedural terminology (CPT) codes for ankle fusion or ankle replacement to identify all patients who underwent either of these procedures at a single tertiary academic center over a 20-year period. Etiologies were broadly grouped as Pilon/Plafond fracture, ankle fracture, talus fracture, tibia fracture, single or recurrent sprains, infection/septic joint, systemic disorder (Charcot arthropathy, rheumatoid arthritis, hemophilic arthropathy) and idiopathic/primary osteoarthritis. Each fracture pattern was then subclassified using commonly accepted classification systems by two independent observers in addition to the grade of arthritis at time of fusion or replacement. Reliability among readers was assessed by Kleiss kappa. Normative data were analyzed by ANOVA and comparison among groups and methods by Student’s T- test.
Results: A total of 533 patients were included in this study. The initial injury patterns were broadly classified as: pilon/plafond (65), ankle (173), sprains (110), talus (17), tibia (22), tibio-talar dislocation without fracture (1). Other identified etiologies included rheumatoid arthritis (18), charcot arthropathy (11), progressive collapsing foot deformity (21), septic arthritis (5), and cavovarus (6). The average time interval between the initial injury and definitive treatment for end-stage arthritis was 558 days. Ankle fractures classified as 44C1 (14,1%), 44B3 (10.6%), 44B2 (9.3%) followed by pilon 43C3 (6.5%) and 43C1 (4.1%) were the most prevalent subclassification found in the fractures group.
Conclusion: The main etiology for AO is secondary, due to trauma. History of ankle sprains and instability was found in 20.6%. Fractures corresponded to 54,6% of our cohort, ankle fractures producing most of these lesions. When considering the subtype of injury, ankle fractures with a 44C1 and a 44B3 classification were the more frequent presentation. These findings could support the argument that complex low-energy rotational traumas do not carry a benign course. Comprehension of the AO etiology scenario may guide prevention policies and specific primary treatment guidelines with the objective of diminishing disease impact on population and health care system.
DOI: 10.1177/2473011421S00164
Second-Look Arthroscopy after Surgery for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Jari Dahmen, BSc,BSc(Med); Jelmer T. Vreeken; Tobias Stornebrink, MD; Kaj Emanuel; Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Introduction/Purpose: The primary aim was to assess and compare cartilage quality after different surgical interventions evaluated by second-look arthroscopy (SLA). Secondary aims were to report concomitant diagnoses found during SLA, and to correlate the cartilage quality with clinical- and radiological outcomes.
Methods: A literature search was performed through PubMed, Embase (Ovid), and Cochrane Library. The primary outcome was the difference of cartilage quality as assessed with SLA between different surgical interventions. The Moderator analysis was used to calculate differences between treatment groups. Associated 95% confidence intervals (CI) were calculated with the Clopper- Pearson interval. Additionally, correlations between the cartilage quality and clinical- or radiological outcomes were calculated and percentages of concomitant diagnoses per treatment group were reported.
Results: Nineteen studies comprising 447 ankles having undergone SLA 14 months after the initial surgery were included. The cartilage quality success rate for bone marrow stimulation (BMS) was 53% (95% CI 38-68%), for Retrograde Drilling (RD) 100% (95% CI 66-100%, for fixation (FIX) 92% (95% CI 70-89%), for Osteochondral Transplantation (OCT) 94% (95% CI 69-99%) and Chondrogenesis-Inducing Techniques (CT) this was 81% (95% CI 70-89%). The success rate of BMS was significantly lower than FIX, OCT and CIT. There were no significant differences in success rates between the other treatment options. The incidence of concomitant diagnoses found during second-look arthroscopy differed among different treatment strategies. For BMS, a positive correlation was found between the International Cartilage Repair Society score (ICRS) and AOFAS-scores (rc =.67, p <0.01). For OCT, no significant correlation was found between the MOCART score and the ICRS (rc =.36, p =.23).
Conclusion: Bone marrow stimulation yields inferior cartilage quality as assessed with SLA in comparison to fixation, osteo(chondral) transplantation and cartilage implementation. The role of the quality of the subchondral bone and its repair must be highlighted concerning correlation with clinical outcomes and long-term success as well as prevention of development of osteo- arthritis.
DOI: 10.1177/2473011421S00165
Talar Osteoperiostic Grafting from the Iliac Crest (TOPIC): 2-Year Results of a Novel Press-Fit Surgical Treatment for Large Talar Osteochondral Lesions
Jari Dahmen, BSc,BSc(Med); Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Introduction/Purpose: The purpose of this study was to present the surgical technique and to evaluate the clinical and radiological outcomes of a new press-fit OATS technique for large primary and secondary talar osteochondral defects of the talus, Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC).
Methods: Forty patients underwent a press-fit TOPIC procedure. Mean age was 38 years (SD 4.6). Pre- and postoperative clinical assessment at 12- and 24-months follow-up included the American Orthopaedic Foot & Ankle Society (AOFAS) score, the Short- Form 36 (SF-36) Mental Component Scale (MCS) and Physical Component Scale (PCS), the Numeric Rating Scales (NRS) of pain at rest, during walking and stairclimbing, and the Foot and Ankle Outcome Score (FAOS). Return to work was assessed in time and rate. Remodeling of the contour of the talus, bone ingrowth and consolidation of the implanted graft were assessed on computed tomography (CT) one year post-operatively.
Results: All patients were available for the two-year follow-up. The AOFAS improved from 48 to 90 (p<0.05). All NRS scores improved: the NRS during rest from 3 to 0 (p<0.05), the NRS during walking from 5 to 1 p<0.05), and the NRS during stairclimbing from 5 to 1 (p<0.05). Both components of the SF-36 improved. The PCS improved from 34 to 47 (p<0.05) and the MCS from 37 to 66 (p<0.05). All FAOS subscales significantly improved. 70% returned to sport at pre-injury sports level and mean time to return to sports was 9 months (SD 2.4). All patients showed remodeling of the talus and all grafts showed consolidation as well as bone ingrowth on the CT scans. All patients returned to work, at a mean time of 4 months post-operatively (SD 4.4). One patient had a temporary loss of n. saphenous sensibility.
Conclusion: The TOPIC procedure is a highly promising surgical treatment option for large primary and secondary talar OCDs. Despite these good mid-terms clinical, sports and radiological outcomes, longer follow-up is necessary to assess the clinical outcome and the progression of osteoarthritis at the long term.
DOI: 10.1177/2473011421S00166
Talar Osteoperiostic Grafting from the Iliac Crest (TOPIC): Return to Sports Outcomes of A Novel Press-Fit Surgical Treatment for Large Talar Osteochondral Lesions
Jari Dahmen, BSc,BSc(Med); Quinten Rikken; Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Category: Ankle
Keywords: Talar Osteochondral Lesions; Osteochondral Autograft; Return to Play
Introduction/Purpose: The purpose of this study was to evaluate the sports outcomes of a new press-fit OATS technique for large primary and secondary talar osteochondral lesions of the talus (OLTs), Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC).
Methods: The study population included amateur and professional athletes with a talar osteochondral lesion size of at least 10 mm in diameter as measured anteroposteriorly or mediolaterally. The surgical intervention in question was the Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC) procedure, which was performed in a press-fit way. Sports outcomes at a minimum of 24 months included return to sports rates, level (return to any level of sports, return to pre-injury levels of sports, and return to performance), including corresponding return to sports times of the aforementioned levels.
Results: A total of 30 athletes, including 1 professional athlete, were assessed. All patients were available for the follow-up at 24 months post-operatively. The mean follow-up duration was 24 months (SD 4.5). The mean lesion size was 356 mm2. Return to any level of sports rate was 90% (95% CI 83 - 95) with an associated time of 8.4 months (SD 2.3). Return to pre-injury level of sports rate was 72% (95% CI 60 - 83) with an associated time of 9.5 months (SD 3.0). Return to performance was 30% (95% CI 20 - 40) with an associated return to performance time of 12 months (SD 4.6).
Conclusion: Our study suggests that a TOPIC procedure can be considered a good option in the management of large osteochondral lesions of the talar dome in an active sports population, with adequate return to sports and work outcomes. Further research is required to optimize our surgical technique and show long-term outcomes.
DOI: 10.1177/2473011421S00167
The Incidence of Osteochondral Lesions after Isolated Syndesmotic Injury: A Systematic Review and Meta-Analysis
Jari Dahmen, BSc,BSc(Med); Sjoerd A. Stufkens, MD, PhD; John G. Kennedy, MD, FRCS(Orth); Gino Kerkhoffs, MD
Introduction/Purpose: To determine the incidence of osteochondral lesions of the ankle (as well as their location and size) incidence after isolated syndesmotic injuries.
Methods: A literature search was performed to identify studies published using PubMed (MEDLINE), EMBASE, CDSR, DARE, and CENTRAL. Two authors separately and independently screened the search results and conducted the quality assessment using the MINORS criteria. Available full-text studies published in English, Dutch and German were eligible for inclusion. OCL incidence as well as location after isolated syndesmotic injuries were extracted from the original articles and subsequently pooled. Whenever possible, OCL incidence per syndesmotic timing (Acute/subacute/chronic) was calculated, pooled and compared with a random effects model.
Results: Nine articles were included with 694 syndesmotic injuries. Overall (O)CL incidence was 21.6% (95% CI 18.7 - 24.8%). This rate was 15.9% (95% CI 12.2 - 20.4), 11.4% (95% CI 5.9 - 21.0), and 54.2% (95% CI 44.2-63.8) for the acute, sub-acute, and chronic isolated syndesmotic group, respectively, thereby showing a significant difference in incidence rate between the acute and chronic syndesmotic injuries group (p<0.05). Concerning overall (O)CL incidence, 74.6% (95% CI 65.9 - 81.2) of the lesions were located on the talar dome and 16.7% (95% CI 10.9 - 24.6%) of the lesions were located on the distal tibia (p<0.05). (O)CL size was not reported in any of the studies. Concerning location difference between the acute and chronic group, the incidence of talar (O)CLs was higher in the acute group than in the chronic group (100% 95% CI 93.9 - 100% vs. 46.8% 95% CI 33.3 - 60.8%.) (p<0.05).
Conclusion: This meta-analysis showed that (osteo)chondral lesions of the ankle are frequently associated with isolated syndesmotic injuries. (O)CL incidence was significantly higher in the chronic isolated syndesmotic injuries group compared to the acute group (54% versus 16%). The vast majority of (O)CLs were located on the talar dome.
DOI: 10.1177/2473011421S00168
Limited Evidence for Biological Adjuvants in Hindfoot Arthrodesis: A Systematic Review and Meta- Analysis of Clinical Comparative Studies
John Dankert, MD, PhD; Dexter Seow; Youichi Yasui, MD; Wataru Miyamoto; James D. Calder, MD, MBBS, FFSEM, FRCS(Tr&Orth), PhD; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: The purpose of this study was to evaluate the efficacy of biological adjuvants in hindfoot arthrodesis.
Methods: A systematic review of the PubMed and Embase databases was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines using specific search terms and eligibility criteria. Assessment of evidence was three-fold: level of evidence by criteria published by The Journal of Bone & Joint Surgery, quality of evidence by the Newcastle-Ottawa scale and conflicts of interest. Meta-analysis was performed by fixed-effects models for studies of low heterogeneity (I2 <25%) and random-effects models for studies of moderate to high heterogeneity (I2 >=25%).
Results: Hindfeet totaled 1579 patients as protocol and 1503 patients per protocol. Final reported mean follow-up ranged from 2.8 months to 43 months. Twelve of the 17 included studies were comprised of patients with comorbidities associated with reduced healing capacity. Based on the random-effects model for non-union rates for autograft versus allograft, the risk ratio was 0.82 (95% CI, 0.13 to 5.21; I2 = 56%; p = 0.83) in favour of lower non-union rates for autograft and for autograft versus rhPDGF/ß-TCP, the risk ratio was 0.90 (95% CI, 0.74 to 1.10; I2 = 59%; p = 0.30) in favour of lower non-union rates for rhPDGF/ß-TCP.
Conclusion: There is a lack of data to support the meaningful use of biological adjuvants compared to autograft/allograft for hindfoot arthrodesis. The meta-analysis favoured the use of autograft when compared to allograft, but favoured rhPDGF/ß-TCP instead when compared to autograft in the short-term follow-up.
DOI: 10.1177/2473011421S00169
The Effect of Single vs Serial Platelet-Rich Plasma Injection in Osteochondral Lesions Treated with Microfracture: An in Vivo Rabbit Model
John Dankert, MD, PhD; Youichi Yasui, MD; Ichiro Tonogai, MD, PhD; Nathaniel P. Mercer; Margaret B. Goodale, DVM; Lisa A. Fortier, PhD; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: Platelet-rich plasma (PRP) has gained increasing interest as a potential therapeutic augment for decreasing inflammation and enhancing healing after cartilage injury. However, it remains unknown whether osteochondral repair outcomes benefit from multiple PRP injections. We performed this animal study to investigate the effects of serial PRP injections on cartilage repair tissue, subchondral bone remodeling, and joint inflammation.
Methods: Forty-eight adult New Zealand White rabbits were randomly assigned to receive either one (1P), two (2P), or three (3P) PRP injections. Cylindrical full-thickness cartilage defects with subsequent microdrilling were created on the central medial femoral condyle of both knees. PRP injections were provided on the day of surgery and every 2 weeks thereafter until the assigned number of injections was achieved for each group. Rabbits in each group were euthanized at 3, 6, or 12 weeks postoperatively. Cartilage repair tissue was assessed using the International Cartilage Repair Society (ICRS) macroscopic and modified ICRS histological scoring systems. Subchondral bone remodeling was evaluated by micro-computer tomography (µCT) analysis. Joint inflammatory cytokines including IL-1, IL-1ra, IL-6, IL-8, TNFα, and TGFβ were assessed by quantitative polymerase chain reaction.
Results: Macroscopic assessment at 3 and 6 weeks demonstrated improved mean ICRS macroscopic scores in the PRP groups compared with the control group, although this difference was not significant. The mean ICRS macroscopic score at 12 weeks in Group 3P was significantly lower than the control, but there was no significant difference compared with Group 1P and Group 2P (Control: 6.1+-3.3, Group 1P: 3.4+-2.7, Group 2P: 4.2+-2.9, Group 3P: 0.7+-1.5). The mean modified ICRS histological score was significantly higher at each time point for the PRP groups compared with the control group, but there was no significant difference in the scores among PRP groups. There were no significant differences in outcomes for the characteristics evaluated by µCT nor inflammatory cytokine levels among each group at each time point.
Conclusion: Serial PRP injections, as compared to a single PRP injection, do not have a significant impact on cartilage repair tissue nor inflammatory cytokine levels at 12 weeks after surgery in an in vivo animal model. Further work is necessary to determine the effect of single versus serial PRP injections on cartilage repair tissue in humans.
DOI: 10.1177/2473011421S00170
Sural Nerve Injury in the Achilles Tendon Repair with Dresden Instruments: Anatomical Study
Anderson E. David, MD; Cesar E. Gamba; Claudia Reyes; Diego F. Feijo; Juan P. Borrero; Gustavo A. Gil
Introduction/Purpose: The surgical reconstruction of the Achilles tendon has evolved in favor of the use of percutaneous techniques over the traditional approach with wide approaches to reduce the complications inherent to this procedure. These percutaneous techniques can present lesions of the sural nerve. The objective of this study is to evaluate the distance of this structure with respect to the instruments used in the Dresden technique.
Methods: Dissections were made in 16 anatomical pieces (ankles) to which a reproduction of the complete Achilles lesion was previously made and reconstructed using the technique to be studied. After this, the distance of the instrument position with respect to the sural nerve was measured, as well as other relevant measures, and the presence or absence of nerve injury was evaluated.
Results: None of the pieces there was lesion of the sural nerve neither by direct injury nor by entrapment, in addition, an approximate distance of 10mm of the nerve was found with respect to the entry site of the percutaneous needles as described by the technique. The location of the nerve was always external to the Crural Fascia. We demonstrate a safety area in which the instruments can be used without lesions of the sural nerve.
Conclusion: The technique described by Amlang with the use of Dresden instruments has a low rate of cutaneous complications and infection compared to the traditional approach for this injury, we find that if the risk of presenting injury is performed properly of the sural nerve is low and its reproduction, for the repair of Achilles injuries, should be considered as the first option over traditional open management.
DOI: 10.1177/2473011421S00171
Incidence of Deep Vein Thrombosis (DVT) in Patients Using A Knee Scooter
Stuart Davidson; Nina Pogorzelski; Thomas C. Dowd, MD; Jeannie Huh, MD
Introduction/Purpose: Functional limitations after lower extremity injury often require the use of an assistive device such as a knee scooter. Many patients find these devices to be easier and more comfortable to use than crutches or walkers. There is concern regarding the possible correlation between scooter use and DVT. Prior literature demonstrated decreased venous flow with the knee flexed, and venous stasis is a known risk factor for DVT1-3. Further, healthy volunteers using a scooter demonstrated a significant decrease in volumetric blood flow rate at the popliteal fossa4. We report the incidence of DVTs after prescription of a scooter following lower extremity injury. We hypothesized that DVT rates would be higher in patients using a scooter compared to rates of DVT in the NSQIP database
Methods: A retrospective record review of adult patients age 18-74 within the Military Health System (MHS) database between 2010-2020 was completed to identify the total number of patients who were prescribed a knee scooter and those who subsequently developed a DVT. Additional demographic and clinical data were collected on patients who had both a scooter and a DVT. This was compared with recorded 2015 NSQIP data on DVT incidence in major orthopaedic surgery procedures.
Results: Between 2010 and 2020, 46,840 of patients within the MHS database were prescribed a rolling scooter after a lower extremity injury or surgery. Of those patients who were prescribed a scooter, 377 subsequently developed a DVT within 90 days of prescription. DVTs were diagnosed on average 26.5 days after scooter prescription. The incidence of DVT of in this population was 0.8%.
Conclusion: In the Military Health System database, the use of a knee scooter following lower extremity injury or surgery is associated with a higher incidence of DVT compared to the 2015 NSQIPS incidence of DVT following major orthopedic surgery (0.80% vs 0.55%), and is most frequently diagnosed within 30 days of scooter prescription. Higher level study is needed to confirm these findings and identify risk factors of patients who experience DVTs associated with scooter use after lower extremity injury or surgery.
DOI: 10.1177/2473011421S00172
Homolateral Lisfranc Fracture/Dislocation of 1st - 5th Metatarsals in a Collegiate Quarterback: A Case Study
Steven R. Dayton, BA; Kurt M. Krautmann, MD; Michael Boctor; Vehniah K. Tjong, MD; Anish R. Kadakia, MD
Category: Sports; Midfoot/Forefoot
Keywords: TMT; Lisfranc Injury; Return to Play
Introduction/Purpose: Lisfranc injuries encompass a spectrum of injuries to the tarsometatarsal (TMT) joint complex from ligamentous sprains to fractures with dislocation. While studies have shown it is possible to return to sport (RTS) after low- energy injuries, no literature exists demonstrating RTS after homolateral fracture/dislocation of all 5 metatarsals. We present a novel surgical technique for repair of homolateral Lisfranc fracture/dislocation of the 1st-5th metatarsals. Fusion of the 2nd and 3rd TMT joints provides stability of the middle column. Internal bracing of the 1st TMT joint gives stability while preserving greater physiologic motion in a high-level athlete.
Methods: A dorsal approach is used for fusion of the 2nd and 3rd TMT joints with medial approach for internal bracing of the 1st TMT joint. 2nd and 3rd metatarsals were denuded of cartilage, and the fusion site was fully prepared. Rigid fixation was applied to the fusion sites. Guidewire for the cannulated Internal Brace system is inserted into the base of the 1st metatarsal. Fluoroscopic imaging confirmed positioning and the 3.4mm drill is passed over the wire, followed by the cannulated tap. A 4.75mm Swivelock anchor with Fibertape suture is inserted into the metatarsal base. The guidewire is placed in a reciprocating position on the medial cuneiform. The 2.7 mm drill is passed over the wire, followed by the 3.5 mm tap. A 3.5 mm Swivelock is then loaded with the Fiberwire from the 1st metatarsal. Tensioning is performed, and the 3.5 mm Swivelock is inserted into the medial cuneiform.
Results: The athlete was cleared to return to full competition 9 months following surgery with physical exam demonstrating stability in both dorsiflexion and abduction. Weight bearing x-rays showed no evidence of hardware failure and no instability in the 1st TMT joint. CT scan demonstrated solid fusion of 2nd and 3rd TMT joints and maintained anatomic reduction of the 1st TMT joint. At 1-year post-op, patient was having pain over the 4th TMT joint. He had a second surgery to remove an exostosis at the 4th TMT joint as well as remove the screw from the 3rd metatarsal to the middle cuneiform. His pain had resolved at most recent follow up. He returned to game action in the final game of his senior season.
Conclusion: The literature demonstrates return to sport is possible for athletes with Lisfranc injuries though the data focuses on either purely ligamentous injuries or Myerson type B and C fractures. This case study demonstrates a novel surgical approach to homolateral fracture/dislocation. While return to sport in this athlete took longer than lower-energy injuries, it is possible for athletes with homolateral displacement to return to full competition.
DOI: 10.1177/2473011421S00173
Implant Related Artifact Around Metallic and Bio-Integrative Screws: A CT Scan 3D Hounsfield Unit Assessment
Cesar de Cesar Netto, MD, PhD; Nacime S. Mansur, MD; Tutku Tazegul; Matthieu Lalevee, MD; Hee Young Lee; Andrew Behrens; Francois Lintz, MD MSc FEBOT; Alexandre L. Godoy-Santos, MD; Kevin N. Dibbern, PhD; Donald D. Anderson
Category: Basic Sciences/Biologics; Hindfoot
Keywords: CT; Implant Cost; Screws
Introduction/Purpose: Implant-related artifact (IRA) represents an important limitation in Computed Tomography (CT) assessment of osteotomy and fracture healing, bone-implant integration, and success of fusion procedures. Metallic implants are the most used in foot and ankle surgery and are recognized as important IRA generators. Absorbable and bio-integrative (BI) implants are attractive options for bone fixation when postoperative CT imaging is likely, particularly in procedures with higher risk for nonunion. However, the literature comparing IRA with metallic and BI implants is scarce. The objective of this study was to assess the degree of IRA around metallic and BI cannulated screws. Our hypothesis was that BI implants would demonstrate significantly decreased IRA around the inserted screws.
Methods: In this cadaveric/CT imaging study, 2 below-knee specimens were used. Medial displacement calcaneal osteotomy was performed through a 5-cm long lateral heel approach. Calcaneal tuberosity was displaced medially by 10mm and fixed provisionally with 2 parallel K-wires under fluoroscopic guidance. Specimens were fixed with two headless 4.0 millimeters cannulated screws, either metallic or BI. Cone-beam CT imaging of both specimens was acquired following osteotomy screw fixation (120kVp, 5.5mA, 0.25mm isotropic). Using a dedicated software, the overall dispersion of Hounsfield units (HU) in a 3D cube of 30mm edge length was assessed. Four HU lines were then traced parallel to the screws, crossing the osteotomy site. Lines 1, 2, 3 and 4 were positioned respectively: In close proximity, over, inside the cannulation and away from the implant. The HU dispersion in these lines was measured and compared between metallic and BI implanted specimens, using T-tests/Wilcoxon analysis. P-values<0.05 were considered significant.
Results: When compared to the BI implant, the average HU was pronouncedly and significantly increased around metallic implants in the lines with more close proximity (Line 1), over the screw wall (Line 2) and inside the screw cannulation (Line 3), when considering both the whole line extension inside the 3D cube as well as in a selected 8mm line-segment across the calcaneal osteotomy line: Line 1 (entire, 7.26 vs -159; selected, -5 vs -249) Line 2 (entire, 4.846 vs 108; selected, 6286 vs 151.2); Line 3 (entire, 1664 vs 144; selected, -277.7 vs 198.7) selected). However, across Line 4 (away from the implant), the HU dispersion was interestingly and significantly decreased around the metallic implant (entire, -49 vs 178.5; selected, -110 vs 221), potentially as result of beam hardening artifact, concentrating HU close to the metal, and shielding the surrounding cancellous bone from being accurately reconstructed.
Conclusion: In this cadaveric imaging study, we compared Implant-related artifact (IRA) around metallic and bio-integrative (BI) implants utilized to fix medial displacement calcaneal osteotomies. We found metallic implants to demonstrate significantly and pronouncedly increased HU dispersion in in close proximity with the implants and significantly decreased dispersion more distantly from the implant, shielding the surrounding cancellous bone, and potentially hindering the assessment of bone density quality and bone/osteotomy/fusion healing in its neighborhood. BI implants represent an alternative to decrease these IRA effects. Additional clinical studies are needed to confirm and expand our findings.
DOI: 10.1177/2473011421S00174
Surgical Correction of Peritalar Subluxation and Patient Reported Outcomes: A Prospective Comparative Outcome Study in Flexible Progressive Collapsing Foot Deformity
Cesar de Cesar Netto, MD, PhD; Nacime S. Mansur, MD; Matthieu Lalevée; Francois Lintz, MD MSc FEBOT; Kristian Buedts, MD; Andrew J. Goldberg, OBE MD FRCS (Tr&Orth); Jonathan T. Deland, MD; John E. Femino, MD; Donald D. Anderson; Kevin N. Dibbern, PhD
Introduction/Purpose: Peritalar subluxation (PTS) of the hindfoot is a critical finding in Progressive Collapsing Foot Deformity (PCFD). Subluxation of the middle facet and sinus tarsi impingement have recently been shown to represent essential markers of pronounced and potentially progressive deformity. Weightbearing CT (WBCT) imaging and three-dimensional (3D) distance (DM) and coverage maps (CM) allow a complete and accurate assessment of PTS markers across the entire peritalar surface. This prospective comparative study aimed to assess the effectiveness of joint-sparing realignment surgical treatment for flexible PCFD in reducing PTS and to correlate the improvement with patient-reported outcomes (PROs). We hypothesized that surgical treatment would significantly improve PTS markers, mainly decreasing sinus tarsi coverage/impingement and middle facet subluxation, and that this improvement would correlate with increased PROs.
Methods: In this IRB-approved prospective and comparative study, we enrolled patients with flexible PCFD, no prior surgeries, and failed conservative treatment. Included patients (n=10, 7 females/3 males, mean age 57.2, range 37-74) underwent joint-sparing surgical realignment procedure by a single surgeon. Standing weightbearing CT (WBCT) was completed preoperatively and 3- months postoperatively. Following automatic bone segmentation, 3D distance maps (DMs) of the entire peritalar surface were generated, and coverage of the subtalar joint articular facets (anterior, middle, and posterior) and sinus tarsi were assessed as markers of PTS. Joint coverage was defined as the percentage of articular space where DMs were <5 mm. Coverage Maps (CM) were built highlighting areas of adequate joint interaction (blue), joint subluxation (pink), and impingement (red). PROs were evaluated preoperatively and at the latest follow-up. Differences between preop/postop measurements and PROs were assessed by independent t-tests/Wilcoxon and bivariate analysis. P-values <.05 were considered significant.
Results: The overall follow-up was 8.2 months (6-13 months). Medial displacement calcaneal osteotomies, lateral column lengthening, and first ray realignment procedures (either Cotton osteotomy or Lapidus) were performed in all patients. Foot and Ankle Offset significantly improved from 10.6% preoperatively to 3.1% postoperatively (p=0.0005), on average. Significant averaged improvement was also observed in anterior facet joint coverage (61.6%), as well as a reduction in sinus tarsi coverage/impingement (-43.2%) (both p<0.001). Middle (19.5%, p=0.08) and posterior facet joint coverage (3.5%, p=0.06) also demonstrated improvements, however not significant. PROs improved significantly on average postoperatively, with the European Foot and Ankle Surgery (EFAS) Score increasing from 3.1 to 7.3 (p=0.02) and the Foot Function Index (FFI) improving from 71.5 to 48.7 (p=0.01). Improvements in EFAS scores and FFI significantly correlated with improvements in middle facet coverage (R2 0.89, p=0.0154) and anterior facet coverage (R2 0.80, p=0.04), respectively.
Conclusion: Our study was the first to evaluate WBCT 3D distance mapping’s role in the assessment of surgical correction of PTS in patients with PCFD. We found significant improvements in subtalar joint anterior facet coverage and sinus tarsi impingement following surgical reconstruction, with a trend to significant improvements in middle and posterior facet joint coverage. More importantly, improvements in middle and anterior facet coverage correlated significantly with improved PROs (EFAS score and FFI, respectively). Based on our study results, optimization of subtalar joint coverage and reduction of PTS should be goals of surgical treatment of PCFD patients.
DOI: 10.1177/2473011421S00175
Three-Dimensional Coverage Maps in the Assessment of Chopart Subluxation in Progressive Collapsing Foot Deformity
Cesar de Cesar Netto, MD, PhD; Andrew Behrens; Matthieu Lalevee, MD; Amanda Ehret; Nacime S. Mansur, MD; Donald D. Anderson; John E. Femino, MD; Francois Lintz, MD MSc FEBOT; Alessio Bernasconi, MD PhD FEBOT
Keywords: Adult Acquired Flatfoot Deformity; Midfoot; Biomechanics of the Foot and Ankle
Introduction/Purpose: Progressive collapsing foot deformity (PCFD), formerly termed Adult-Acquired Flatfoot Deformity (AAFD), is a complex 3D deformity characterized by peritalar subluxation (PTS) of the hindfoot through the triple joint complex. In this context, adjacent structures may adopt different positions and boney relations can change, producing areas increased contact or subluxation. The objective of this study was to use 3D distance maps (DMs) and coverage maps (CMs) from weightbearing CT (WBCT) images to assess subluxation across the Chopart joint in PCFD patients. We hypothesized that CMs would show decreased coverage indicative of subluxation through certain regions of the Chopart joint in PCFD patients when compared to the controls.
Methods: In this IRB-approved, retrospective case-control study, we analyzed WBCT data of 18 consecutive patients with flexible PCFD and 10 controls. Using principle component analysis, candidate coverage area was divided into nine regions on the talar head and 4 regions on the calcaneal-cuboid (CC) articular surface. Novel 3D distance mapping (DM) technique was used to objectively characterize joint coverage across the entire Chopart joint surface on both the talus and calcaneus. Distance maps were measured in millimeters and colored to highlight covered areas. Areas with distances less than 4mm were defined to be covered, while areas with distances greater than 4mm were considered to be uncovered. Joint coverage was defined as percentage of articular area with DMs lower than 4 mm. Coverage Maps (CM) were created to highlight areas of coverage (teal) versus non- coverage (pink). Comparisons were performed with independent t-tests, assuming unequal variances. P values <.05 were considered significant.
Results: Changes in coverage percentages of PCFD cases relative to controls are indicated in attached figure 1. The middle lateral region of the talar head was found to have a 9% increase in coverage in PCFD cases relative to the controls (p = 0.011). The plantar region of the calcaneal-cuboid joint was found to have a 18% decrease in coverage compared to the controls. Except for the dorsal medial regions, the medial side of the talar head saw overall decreases in coverage. However, these values were not statistically significant.
On the calcaneus, the plantar region of the calcaneal-cuboid joint was found to have a significant coverage decrease of 18% relative to the controls (p = 0.017). There was also a decrease in coverage observed in the medial region of the calcaneal-cuboid joint and an increase in the dorsal and lateral areas.
Conclusion: Our results support the occurrence of significant Chopart joint changes in early flexible PCFD. Increased lateral and decreased medial/plantar talar head coverage point to internal rotation and plantarflexion of the talus. Associated dorsal migration of the cuboid where plantar and medial areas have decreased coverage indicate subluxation through the entirety of the Chopart joint. Novel 3D coverage mapping enabled objective quantification of subluxation though the Chopart joint in early stage PCFD. These findings may assist clinical decision making regarding the restoration of normal joint alignment during PCFD corrections. Further studies are needed to establish thresholds of change associated with degeneration.
DOI: 10.1177/2473011421S00176
Three-Dimensional Distance and Coverage Maps in the Assessment of Peritalar Subluxation in Progressive Collapsing Foot Deformity
Cesar de Cesar Netto, MD, PhD; Shuyuan Li, MD, PhD; Victoria Vivtcharenko, BS; Elijah Auch; Francois Lintz, MD MSc FEBOT; Scott J. Ellis, MD; John E. Femino, MD; Kevin N. Dibbern, PhD
Category: Ankle; Basic Sciences/Biologics; Hindfoot; Other
Introduction/Purpose: Progressive collapsing foot deformity (PCFD), formerly termed Adult-Acquired Flatfoot Deformity (AAFD), is a complex 3-dimensional (3D) deformity characterized by peritalar subluxation (PTS) of the hindfoot through the triple joint complex. PTS severity is typically measured at the posterior facet of te subtalar joint, but recent studies have called this into question and presented the middle facet as a more accurate marker of deformity. The objective of this study was to use 3D distance mapping (DM) from weightbearing computed tomography (WBCT) images to assess PTS in PCFD patients and controls across the entire peritalar suface. We hypothesized that 3D DMs would identify the middle facet as a superior marker for PTS, as well as indicate increased extra-articular sinus tarsi and subfibular inpingements in PCFD patients.
Methods: In this case control study, we analyzed WBCT data of 20 consecutive patients with flexible PCFD and 10 controls. Novel 3D distance mapping (DM) technique was used to objectively characterize joint coverage across the entire peritalar surface, including both articular (anterior, middle and posterior facets of the subtalar joint) and nonarticular regions (sisus tarsi and subfibular areas). Distance maps were measured in millimeters, and colored to highlight regions of interest. Distances from 1-4mm were shown in blue to indicate expected joint interaction/extra-articular proximity, while distances under 1mm were highlighted in yellow/red indicating close bone proximity consistent with joint space narrowing (articular) or impingement (extra-articular). Joint coverage was defined as percentage of articular area with DMs <4 mm. Coverage Maps (CM) were built highlighting areas of adequate joint interaction (blue), joint subluxation (pink), and impingement (red). Comparisons were performed with independent t-tests or Wilcoxon tests. P values <.05 were considered significant.
Results: Overall, coverage was decreased in articular regions and impingement was increased in nonarticular regions of PCFD patients. Objectively, a significant 46.6% average increase in the uncoverage of the middle facet of the subtalar joint was observed in PCFD patients (p<.001), consistent with signifcant middle facet subluxation when compared to controls. No significant similar uncoverage was identified in the anterior or posterior facets. Extra-articularly, an overall 98% increase in sinus tarsi coverage was identified in PCFD patients (p<.007) with direct sinus tarsi impingement in 6 of 20 patients with PCFD, and one of the controls. Direct subfibular impingement was noted in only 1 of 20 PCFD patients, but subfibular space narrowing greater than 2 standard deviations was noted in 17 of 20 PCFD patients. Attached figures demonstrate examples of distance and coverage maps, as well as a comparative averaged assessment of peritalar surface coverage in PCFD and controls.
Conclusion: Our study results revealed that when compared to controls PCFD patients demonstrated that a significant decrease in 3D measures of subtalar joint coverage was only identified in the middle facet, but not at the anterior or posterior facets. We also determined significantly decreased inter-bone distances in the sinus tarsi and subfibular regions of PCFD patients, confirming the occurrence of extra-articular impingement in those areas. We hope that the use of these 3D accurate and objective measures of distance (DM) and coverage maps (CM) of middle facet subluxation will support early detection of PCFD patients at high risk for progressive collapse.
DOI: 10.1177/2473011421S00177
Does BMI Effect Intermediate Outcomes of Open Brostrom-Gould Repair?
Aseel G. Dib, BS; Nicholas A. Andrews; Timothy Torrez; James Pate, BS; Kalah Ozimba; Roshan Jacob; Whitt Harrelson; Sameer Naranje; Ashish Shah, MD
Introduction/Purpose: High BMI is a known risk factor for development of CAI and intraarticular pathology, but few studies have examined BMI’s impact of the outcomes of lateral ligament reconstruction. The open Brostrom-Gould reconstruction, an anatomic repair, is the gold standard for repair of the lateral ligamentous complex. We aim to evaluation the impact of BMI on patient reported outcomes after open Brostrom-Gould repair.
Methods: A total of 201 patients who underwent open Brostrom-Gould Repair were identified using CPT code. Patients undergoing repair for acute ligamentous injury were excluded. A completed telephonic survey was required for inclusion yielding 92 patients. The telephone survey included: PROMIS Physical Function (PF), Pain Interference (PI), and Depression domains(D) and the Foot and Ankle Ability Measure (FAAM). Medical records were examined for patient characteristics, operative variables, and complications. Patients were grouped by BMI <30 and BMI >30.
Results: A total of 28 males (30%) and 61 females (69%) were including in this study. The average time at completion of survey was 4.1 years (standard deviation of 2.8). The median age was 44 with an interquartile range (IQR) of 20, while the median BMI was 31.5 with an IQR of 13.4. Obese patients had significantly worse PROMIS PF (Median 44.5 IQR 7.4 vs median 48 IQR 16.5) and FAAM Activity of Daily Living subscale scores (Median 61.6 IQR 30.0 vs. median 82.7 IQR.36). Patients’ FAAM self-reported overall level of function was significantly lower in obese patients (Median 70.0 IQR 20.0 vs median 85 IQR 29). The BMI groups did not vary by other PROMIS domains or FAAM subscales.
Conclusion: At intermediate term follow-up, Obese patients report significantly worse physical function after open Bostrom- Gould repair compared to non-obese patients. Surgeons should be aware of this when prognosticating the outcomes of anatomic ankle reconstruction.
DOI: 10.1177/2473011421S00178
Reduction Quality of Open vs Percutaneous Techniques for the Posterior Malleolus
David Distefano; Steven Karnyski, MD; Benjamin Kuhns; John P. Ketz, MD; Matthew Barra; Brittany Haws
Category: Ankle; Trauma
Keywords: Weber B Ankle Fractures; Weber C Ankle Fracture; Operative Approach
Introduction/Purpose: Ankle fractures with posterior malleolar involvement are common. Fixation of the posterior malleolus (PM) in these injuries remains controversial & currently, there is no evidence to guide operative decision making for the PM. This study compares radiographic & clinical outcomes between percutaneous & open fixation techniques of the PM.
Methods: All ankle fractures between 01/2010 & 01/2018 with surgical stabilization of the PM were reviewed from a level 1 trauma center. High-energy (i.e. pilon), open & pathologic fractures were excluded. Orthopaedic Trauma Association (AO/OTA) fracture pattern, PM articular surface comminution, incarcerated fragments & loose bodies were recorded based on pre-operative CT scans. Patients were either treated with direct reduction (DR) or percutaneous reduction (PR). Intra-operative & serial post- operative radiographs were used to measure PM articular reduction & graded as satisfactory (<2mm articular step-off) or poor (>2mm articular step-off). Medical records were reviewed for fixation technique & complications. Patient-reported outcomes measurement information system (PROMIS) scores were used to compare clinical outcomes. Univariate methods including x2, Fischer exact test, One-way ANOVA were used & a multivariate nominal logistic regression model was constructed to evaluate predictors of a satisfactory reduction.
Results: A total of 120 patients (ages 19-84) were included. DR through an open approach was performed in 91 patients & PR in 29. The DR cohort had a higher rate of satisfactory reduction (92.3% vs 75.9%, p=0.04). Articular comminution was identified in 65 (50.4%) & this morphology had a higher rate of satisfactory reduction with ORIF (94% vs 66.6%, p=0.04). There was no difference in reduction quality for non-comminuted fractures treated open or percutaneously (90.2% vs 83.3%, p=0.64). Incarcerated fragments or loose bodies were identified in 58 (48.3%) of fractures. There was a trend for improved reduction quality in the DR group for this morphology (p=0.08). Multivariate analysis identified that open approach is associated with a satisfactory reduction (p=0.02). No difference in complication rate between groups or PROMIS scores (p>0.05) for 64 patients with average final follow up of 19 months (range 6-60 months) were found.
Conclusion: This study demonstrates that DR of the PM via an open approach in low energy ankle fractures leads to improved radiographic outcomes compared to percutaneous techniques without a difference in complication rate. This study also highlights the utility of a pre-operative CT scan to better assess the morphology of the posterior malleolus as articular comminution, interposed fragments or loose bodies were common findings that are difficult to assess on plain radiographs & may alter surgical plan if present. However, no difference in PROMIS scores were seen between direct and percutaneous reduction techiniques.
DOI: 10.1177/2473011421S00179
Flexor Digitorum Longus Transfer for Posterior Tibial Tendon Dysfunction is the Standard of Care: Does the Evidence Support It?
Sean W. Dooley; Thomas Evashwick-Rogler; Christopher D. Murawski, MD; Gregory P. Guyton, MD; Niall A. Smyth, MD
Category: Basic Sciences/Biologics; Hindfoot; Other
Introduction/Purpose: Flexor digitorum longus (FDL) transfer, in conjunction with osseous procedures, is used routinely for the treatment of posterior tibial tendon dysfunction (PTTD). It is well established however that the relative power of the FDL tendon is significantly inferior than that of the native posterior tibial tendon. The purpose of this study is to systematically evaluate the evidence that supports or refutes the use of an FDL transfer in the surgical treatment of PTTD.
Methods: A systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta- Analysis. Using the terms ‘flexor digitorum longus OR FDL AND posterior tibial tendon dysfunction OR PTTD OR adult acquired flatfoot OR AAFD’ we searched the PubMed/Medline database. Both clinical and biomechanical studies were eligible for inclusion.
Results: Forty-one studies met the inclusion criteria, including 31 clinical studies and 10 biomechanical in vitro studies. All 31 clinical studies consisted of Level IV evidence, and support the use of an FDL transfer. There was significant heterogeneity of the clinical evidence due to the variety of concomitant procedures. Of the 10 biomechanical in vitro studies, 2 support the use of an FDL transfer, although these did not assess the procedure in isolation. 8 biomechanical in vitro studies specifically assessing the effect on of an FDL transfer contradict its use for PTTD.
Conclusion: There is poor quality clinical evidence to support the use of an FDL transfer for PTTD and the biomechanical literature refutes the use of the procedure. It remains unknown if the clinical improvement reported in the literature can be attributed to the FDL transfer or the concomitant osseous procedures. Additional studies are needed to assess the validity of the FDL transfer and whether alternatives are available to preserve the PTT muscle.
DOI: 10.1177/2473011421S00180
Percutaneous Fixation of Metatarsals Fractures with Kirchner’s Wire, Comparison of Antegrade and Retrograde Technique
Sebastian R. Drago, MD; Patricio Alfonso Zagal Alvarado, MD; Jaime Ugarte; Vicente Phillips; Martin Contreras, MD; Gonzalo F. Bastias, MD
Category: Trauma; Midfoot/Forefoot
Keywords: Metatarsals; Fractures; K-Wire
Introduction/Purpose: The antegrade intramedullary nailing technique with Kirchner’s wire (K-wire) (EAK) for the management of metatarsal fractures (MTT) is recent and with few reports. Our objective was to evaluate and compare the clinical results among patients operated on in our center for MTT fractures using the EAK technique versus the traditional retrograde technique (ERK).
Methods: Retrospective, analytical study. We reviewed the cases of patients with a diagnosis of MTT fracture and surgical indication operated with EAK or ERK between February 2010 and January 2016. First and fifth metatarsal fractures were excluded from the analysis, as well as patients in which a fixation method other than K-wire was used. Demographic data, clinical and radiological results were recorded. A total of 34 patients (34 feet, 70 metatarsals) were analyzed and were divided into two groups: Group 1, operated with EAK (15 feet, 22 metatarsals), and Group 2, operated with ERK (19 feet, 48 metatarsals). Statistical analysis was carried out with Fisher’s exact test and Mann-Whitney U test for non-parametric variables, with fixed statistical significance at p <0.05.
Results: The median age was 37 years [IQR = 51-25.25], p = 0.128. Both groups presented similar soft tissue involvement (p = 1,000), similar associated injury rate (20.0% vs 42.1%, p = 0.271), and similar proportions of diaphyseal and neck fractures (p = 0.659 and p = 0.733 respectively). The group operated with the EAK technique presented a lower report of metatarsalgia (6.7% (1) vs 47.3% (9), p = 0.020), shorter rest time since injury (94 days [IQR = 129-82] vs 144 days [IQR = 210-122], p = 0.002) and shorter time to full load (7 weeks [IQR = 9-6] vs 10 weeks [IQR 12.5-8.5], p = 0.002). EAK and ERK did not show differences in criteria for poor reduction (p = 1.00), number of re-interventions (p = 0.560), infections (p = 0.492), or metatarsophalangeal stiffness (p = 0.451).
Conclusion: Metatarsal fracture fixation with EAK presented a lower rate of metatarsalgia and shorter rest time compared to ERK, demonstrating similarity in terms of quality of reduction and complication rate.
DOI: 10.1177/2473011421S00181
Recovery Position vs Prone Position in the Surgical Treatment of Trimalleolar Ankle Fractures Using Posterolateral and Medial Approach
Sebastian R. Drago, MD; Patricio Alfonso Zagal Alvarado, MD; Martin Contreras, MD; Marcelo F. Concha; Juan Pedro Bergeret, MD; Gonzalo F. Bastias, MD
Introduction/Purpose: Posterolateral (PL) and medial approaches have been increasingly used for open reduction and internal fixation (ORIF) of trimalleolar ankle fractures. Traditionally this procedure is performed on the prone position. Nevertheless, this position itself has been related to general complications as brachial plexus injury and postoperative visual loss. Moreover, the prone position can provide difficult access for medial malleolar reduction. Recovery position was recently described as an alternative but its results have not been evaluated yet. This study aimed to compare the results using recovery position (RP) versus prone position in the surgical treatment of trimalleolar fractures.
Methods: A retrospective analytic study was conducted in a Level 1 trauma center, analyzing patients who underwent ORIF for trimalleolar ankle fractures using posterolateral and medial approaches over 3 years. 58 ankles were divided according to the position used in the surgical fixation: Group 1 positioned in RP (27 ankles), and group 2 positioned in prone (31 ankles). Demographics, surgical time, hospital stay, quality of reduction, surgical site complications and re- interventions were compared between both groups. Statistical analysis was performed with Shapiro-Wilks test to assess normality in distribution, Chi-square test, and t-student test for group differences in parametric variables as Fisher’s exact test and Mann-Whitney U test in non- parametric variables with a p-value set at 0.05.
Results: Median age was 47 years old (IQR 40-58). Both groups were similar regarding age (p=0.794), gender (p=0.902), and posterior malleolus Haraguchi (p=0.064) and Bartonicek-Rammelt (p=0.055) classifications. Surgical median time was 115 (IQR 100-130) and 100 (IQR 75-129) minutes for RP and prone groups respectively (p=0,085), Both groups showed similar rates of lateral, posterior and medial malleolus insufficient reduction (Table attached). Median hospital stay was 4 (IQR 2-9 and 2-7 for RP and prone respectively) days for both (p=0,86) (Table attached). Surgical site complications and re-interventions were similar between both groups (p=0.349 and p=1.0 respectively).
Conclusion: The RP showed similar results than the prone position while providing an accessible simultaneous approach to the posterolateral and medial regions of the ankle.
DOI: 10.1177/2473011421S00182
Patient Reported and Functional Outcomes for Revision Lateral Ankle Ligament Reconstruction
Theodora C. Dworak, MD; Bruce E. Cohen, MD; W. Hodges Davis, MD; J. Kent Ellington, MD, MS; Carroll P. Jones, III, MD;
Scott B. Shawen, MD; Todd A. Irwin, MD
Category: Sports; Ankle
Keywords: Ankle Instability; Broström; PRO
Introduction/Purpose: Despite multiple surgical treatment options for revision lateral ankle ligament reconstruction surgery, few studies describe the functional or patient reported outcomes. The purpose of this study is to describe the patient reported and functional outcomes for patient who required revision lateral ankle ligament reconstruction.
Methods: We present follow-up of 26 patients who underwent revision lateral ankle ligament reconstruction between January 2010 and December 2019 at a single institution. Clinical notes and operative reports were reviewed to determine surgical techniques. Patient reported outcomes were completed using the Foot and Ankle Outcome Score (FAOS), Visual Analog Scale Pain, Visual Analog Scale for Ankle Instability, and Visual Analog Scale for Satisfaction. Functional outcome was evaluated with the hop test. Ankle stability was evaluated on physical exam with anterior drawer and inversion stress test.
Results: Initial ligament reconstruction consisted of Brostrom (n=15), Brostrom Evans (n=3), Allograft (n=2) and Unknown (n=6). Revision lateral ligament reconstruction consisted of Brostrom (n=15), Brostrom Evans (n=2) and Allograft (n=9). Median follow up time after revision was 22 months. At last follow up, 20 patients (76.9%) had grade 0 inversion stress and anterior drawer test indicating stability. Median FAOS ADL sub score was 97 and median FAOS Symptom sub score was 79. Median VAS Pain was 3, median VAS Instability was 3 and median VAS satisfaction was 9.5. The single-leg hop test (Limb Symmetry Index %) was completed by 18 patients, with median score of 86.4% compared to their non-operative extremity. Six patients had persistent pain, three of which required additional surgery.
Conclusion: The high majority of patients that require revision lateral ankle ligament reconstruction maintain a stable ankle on exam and are satisfied with their surgical results. Functional outcomes are similar but not symmetrical to their non-operative extremity.
DOI: 10.1177/2473011421S00183
Patient Reported Outcome Measures (PROMIS) of Primary Total Ankle Arthroplasty in Patients Under 50 Years of Age
Pierce Ebaugh, DO; Travis H. Alford; Elizabeth Davis, MD; Kamen J. Kutzarov, MD; Michael C. Greaser, MD; William C. McGarvey, MD
Introduction/Purpose: Compared to more prevalent arthritic conditions, ankle arthritis is complicated by an earlier age of onset. With advancements in 4th generation primary and revision componentry, total ankle arthroplasty (TAA) is considered an option for end-stage ankle arthritis in younger patients aligning with paradigm shifts in knee arthroplasty. Recently published data demonstrates excellent survivorship and complication rates in short/mid-term follow-up of younger patients who received a primary TAA. Additionally, older TAA patients display comparable PROMIS relative to hip/knee arthroplasty. However, there remains a paucity of literature surrounding the PROMIS of younger patients undergoing TAA. Thus, our aim was to assess PROMIS of individuals less than 50 years of age receiving a primary total ankle arthroplasty
Methods: A retrospective cohort analysis of adult patients < 50 years who received a primary total ankle replacement at a single academic institution between 2003 and 2019 was conducted. Patient demographics, diagnosis, treatment, and outcome characteristics were recorded from a chart review of 41 patients with at least one year of post-surgical follow-up (Table 1). Post- operative PROMIS scores were obtained via telephone interviews. Primary outcomes that were measured included emotional and physical health, activity limitation, ambulation, and global health. SF-36, PROMIS Global Health, and Sickness Impact Profile Ambulation were used. Functional outcomes in our study sample were compared with age and gender-matched norms from a general US population, and 95% confidence intervals were calculated for each functional outcome mean. Student t-test was used for continuous variables, and chi-square analysis was used for categorical variables.
Results: Thirty-one of 41 eligible patients were interviewed. The average age at surgery was 40 years old. Clinical and radiographic follow-up was a mean of 59.7 months and 31.2 months following TAA, respectively. General health as measured with the SF-36 was not significantly different from age/gender-matched norms. Eighty-seven percent of patients would choose to have a TAR again. While 58% reported being limited in vigorous activities, 61% were able to ambulate frequently for long periods of time. On average the patients did not report ongoing pain, and only 16% reported fatigue that hindered activities. Eighty-one percent reported returning to full employment and performing their duties without difficulty, and 84% reported they resumed all normal social activities. Primary implant survivorship was 88%.
Conclusion: Despite a younger age and potentially increased demands, patients younger than 50 years of age undergoing primary total ankle arthroplasty are generally very satisfied with their index procedure at a mean follow-up of nearly 5 years. Our findings of positive outcomes on their health and well-being may improve surgeon insight for TAA as a preferred treatment for younger individuals with end-stage ankle arthritis.
DOI: 10.1177/2473011421S00184
Retrospective Study Analyzing Risk Factors of Foot and Ankle Amputation in Patients with Diabetes Diagnosed with Osteomyelitis
Tsola Efejuku; Shivan N. Chokshi; Daniel Jupiter, PhD; Jie Chen, MD, MPH; Vinod K. Panchbhavi, MD, FACS
Category: Ankle; Diabetes; Midfoot/Forefoot
Keywords: Ankle; Diabetes; Diabetic Foot
Introduction/Purpose: Osteomyelitis is an invasive infection of the bone that commonly afflicts patients with diabetes mellitus. This bacterial infection can lead to the need for amputation of portions of the foot or ankle. While the association between Osteomyelitis and amputation has been studied, little is known about additional underlying health conditions that can predispose diabetic patients to an increased risk of amputation. Understanding these relationships will be useful in early screening to prevent severe effects associated with the loss of the foot or ankle. Thus, a retrospective analysis was performed using EMR data to evaluate the effect of prior Peripheral Vascular Disease (PVD) or Neuropathy on amputations in Type 2 DM patients with Osteomyelitis.
Methods: Patients with Type 2 Diabetes Mellitus and Osteomyelitis who had a foot or ankle amputation within 12 weeks of diagnosis, compared to those who also had PVD or neuropathy were identified. This was done in the EMR database using ICD 10 codes for Osteomyelitis (M86), Type 2 Diabetes Mellitus diagnosis (E11), Foot or Ankle amputations (1005524, 1005529, 28810, 1005525, 28805, 1800300006, 371186005, 180040009, 726651003, 723726002, 723731000, 180038004, 78785006, 28800, 180157006, 723312009, 773821000, 773819005, 397218006), Peripheral Vascular Diseases (I73), and Neuropathy (G62). We then stratified these patients by age (18-29, 30-39, 40-49, 50-59, 60-69,70-79, 80-89), gender (male, female), and year by decade (2001, 2010, and 2020).
Results: Our search identified 125,741 patients with T2DM and Osteomyelitis, of whom 10,850 had a foot or ankle amputation within 3 months of diagnosis. 28,242 patients with T2DM, Osteomyelitis, and prior PVD were identified. These patients were found to be 2.6 times more likely to receive a foot or ankle amputation. 12,860 patients with prior Neuropathy were identified.. These patients were found to have 1.36 times more likely to receive a foot or ankle amputation. When stratified by gender, Women were found to be at greater risk of Amputation than Men, for both prior PVD and Neuropathy (2.9 vs 2.47 times greater risk, respectively). Age stratification revealed patients aged 50-59 have the highest risk for a foot or ankle amputation (10% higher risk). This was more than triple the risk seen in patients aged 18-29. The above differences were found to be statistically significant at a p-value of <.0001.
Conclusion: This analysis provides insight into the pre-disposing risk factors of Foot and Ankle amputations in patients who have Type 2 Diabetes Mellitus and Osteomyelitis. Of the two risk factors analyzed, Peripheral Vascular Disease was associated with the highest risk of amputation. Overall, females and patients aged 50-59 are at the highest risk of amputation with underlying PVD. As comorbidities become more frequent and the number of foot or ankle amputations continues to rise since 2001, more research on associated risk factors will be necessary to more effectively screen these patients.
DOI: 10.1177/2473011421S00185
Cyclic Fatigue and Creep Resistance Testing of the PUMA SystemTM
J. Kent Ellington, MD, MS; Kathy Stecco
Category: Ankle; Basic Sciences/Biologics; Trauma
Keywords: Syndesmosis; Biomechanics; Biomechanics of the Foot and Ankle
Introduction/Purpose: The PUMA System (Panther Orthopedics, Sunnyvale, CA) is an FDA cleared. superelastic, nitinol based fixation device for the ankle syndesmosis which provides stabilization without over-compression or loosening due to creep from cyclic loading. Objective The objective of this study was to test resistance to lengthening (creep) of the PUMA System in cyclic fatigue testing.
Methods: Five PUMA System devices, each having a nitinol Body consisting of six layers, were cycle-tested between 20/40 pounds per cubic foot (lb/ft3) polyurethane foam Bone Blocks (Figure 1).[1] The PUMA System devices were set up with an initial device Active Length of approximately 66 millimeters (mm) between their polyether ether ketone (PEEK) Anchor buttons. All devices were tightened to a minimum of 11.1 Newtons (2.5 pounds force) and cycled at 5 cycles per second (5 Hz) for 4500 cycles to 2.4 mm displacement. Device Active Length was recorded pre- and post-testing. Devices were visually inspected for any break in the 30 nitinol layers. [1] ASTM F1839: Standard Specification for Rigid Polyurethane Foam for Use as a Standard Material for Testing Orthopedic Devices and Instruments.
Results: None of the 30 layers incorporated in the 5 PUMA SystemTM device Bodies failed due to cyclic fatigue. Also, there was little-to-no difference between pre- and post-testing Active Length (Figure 2). More specifically an average increase of only 0.2% in length with a with a Standard Deviation of 0.16% evidences no significant creep (Table 1).
Conclusion: The PUMA SystemTM allows for ankle syndesmosis repair with an implant that experiences no significant creep as demonstrated in cyclic-fatigue testing under challenging displacement cycle testing.
gggg
DOI: 10.1177/2473011421S00186
Effectiveness of a Superelastic Nitinol Device for Fixation of Syndesmosis in Ankle Fracture
J. Kent Ellington, MD, MS; Kenneth J. Hunt, MD
Category: Ankle; Trauma
Keywords: Syndesmosis; Ankle Fracture; Trauma
Introduction/Purpose: Syndesmosis injuries are increasingly common. Available fixation options are not yet optimal. The PUMA System (Panther Orthopedics, Sunnyvale, CA) is an FDA-cleared superelastic, nitinol-based fixation device for the ankle syndesmosis which provides stabilization without over-compression or loosening during cyclical loading. The spring-like design of the PUMA System allows physiological micro-motion while maintaining continuous compression and resisting syndesmosis widening, without material creep. The objective of this prospective study is to assess the effectiveness and complication rate of the PUMA device for treatment of fracture-associated syndesmosis injuries.
Methods: We prospectively collected radiographic and clinical data on 32 consecutive patients treated for fracture-associated syndesmotic disruption with the PUMA SystemTM at 8 centers. Primary outcome measures included adverse event rates, radiographic evaluations for syndesmosis integrity and implant failure, and rates of revision surgery.
Results: All 32 patients had successful repair of their ankle syndesmosis (Figure 1). The mean age of patients at time of operation was 42 years (range 16- 68). There were 13 females (13/32, 40.6%) and 19 (19/32, 59.4%) males. Postoperative radiographic evaluations confirmed satisfactory syndesmosis healing with maintained reduction in the ankle mortise in 33/33 (100%) ankles. There was no evidence of lysis, device migration or syndesmotic or medial clear space widening. There were no infections or soft tissue complications. All fractures healed. No devices required removal and there were no revision surgeries.
Conclusion: The PUMA SystemTM provides physiologic stabilization of the syndesmosis due to the design features that allow for continuous compression without creep. We found no device-related complications nor construct failures in our series. The superelastic implant design allows physiologic motion at the syndesmosis but does not creep or stretch following displacement. This flexibility obviates the need for routine removal. The implant’s low-profile buttons without suture and knot tying requirements eliminate the concern for subcutaneous knot irritation and slippage. Additional biomechanical and clinical outcomes study of this device may further optimize rehabilitation protocols for patients treated for syndesmotic injury.
DOI: 10.1177/2473011421S00187
The Routine Use and Cost Analysis of Acid-Fast Bacilli and Fungal Cultures in Foot and Ankle Surgery: A Retrospective Study
Zein S. El-Zein, MD; Scott Diamond; Margaret Bohr; Erin A. Baker, PhD; Mackenzie M. Fleischer; Corinn Gehrke, MS; Paul T. Fortin, MD; Zachary M. Vaupel, MD
Category: Other; Diabetes
Keywords: Foot and Ankle Infection; Cost Effectiveness; Microbiology
Introduction/Purpose: Infections pertaining to orthopaedic surgery play a major role in patient morbidity and increased healthcare-associated expenses. In the setting of foot and ankle surgery for infection, it is common practice to send acid-fast bacilli (AFB) and fungal intraoperative cultures, although there is no standard protocol in place. In this study, the rate of positive AFB and fungal cultures and associated costs in a consecutive series of foot and ankle surgeries was retrospectively assessed.
Methods: Under an IRB-approved protocol, CPT codes were used to identify 447 procedures in 320 patients, who underwent foot and ankle surgery for infection by fellowship-trained foot and ankle orthopaedic surgeons at a Level 1, private, academic hospital from 2014 to 2019. A medical records review was performed to collect microbiology and patient demographic data. Materials and labor cost data, which was provided by the institution, was used to quantify a total culture cost.
Results: In this series, there were 185 male and 135 female patients with an average age of 57 years (range, 10-105) and average BMI of 31 kg/m2 (range, 13-56). No patients had positive AFB cultures and 20 patients (7.5%) had positive fungal cultures. There were 434 AFB and 525 fungal cultures performed during these procedures. Based on total cultures performed, there were 0% (0/434) AFB and 5% (26/525) fungal culture positivity rates. The total intra-institutional cost (i.e. labor and materials) for AFB cultures was $23,967. The total labor/materials cost for negative and positive fungal cultures was $12,428 and $2,371, respectively. The total labor/materials cost for all the cultures obtained over the time frame of our study was $38,767.
Conclusion: This study highlighted low rates of positive AFB and fungal cultures in the orthopaedic foot and ankle surgery service in a 6-year retrospective review, as well as substantial institutional costs of routine use of intraoperative cultures. While this series included cases from three fellowship-trained foot and ankle orthopaedic surgeons, this study will be expanded to analyze AFB and fungal culturing practices and cost in other orthopaedic subspecialties. Creating and implementing a standardized protocol may achieve cost effectiveness of cultures without diminishing patient outcomes.
DOI: 10.1177/2473011421S00188
Sesamoidectomy Utilizing a Medial Approach with a Bur: Patient Outcomes and Early Complications
William M. Engasser, MD; J. Chris Coetzee, MD; Jeffrey D. Seybold, MD; Bryan D. Den Hartog, MD; Patrick B. Ebeling, MD; Fernando C. Raduan, MD; Kayla Seiffert
Introduction/Purpose: Patients with pathology of the sesamoids can have significant pain and disability both with activities of daily living and high impact athletic movements. Sesamoidectomy is a widely used procedure for patients who fail conservative treatment measures. Traditional dorsal or plantar approaches for sesamoidectomy have shown to successfully alleviate pain but complications are noted, including hallux varus deformity, painful plantar incision, and clawing of the hallux. Additionally, the dorsal approach is technically difficult because of poor visualization, which can lead to unnecessary disruption of important plantar ligamentous structures. An alternative medial approach using a bur provides many advantages compared to traditional approaches.
Methods: This was a retrospective chart review of patients undergoing sesamoidectomy using a bur with a medial approach to the sesamoid metatarsal articulation. Data collected included patient demographics, radiographic analysis, and outcomes: Veterans Rand 12 Item Health Survey (VR-12), Foot and Ankle Ability Measure (FAAM), Visual Analog Scale (VAS), patient satisfaction, and complications.
Results: In patients (10 feet) with an average age of 36.5 (range, 13-77) years were analyzed. Six patients underwent medial sesamoidectomy, three underwent lateral sesamoidectomy, and one patient underwent excision of both medial and lateral sesamoids using a bur. The average latest follow up was 11.9 months. Scores were improved from pre-operatively to most recent follow-up for VR-12 Physical (29.43 vs 53.86), FAAM ADL (48.8 vs 94.1 points), FAAM Sports (7.8 vs 87.4 points), and VAS (57.8 vs 8.6). Patient satisfaction with the treatment was 96.4%. There were zero complications or additional procedures performed.
Conclusion: In this series, sesamoidectomy utilizing a medial approach with a bur provided excellent pain relief, zero complications, and significantly improved outcome scores at early follow up. The medial approach is familiar to orthopedic foot and ankle surgeons, provides adequate exposure, and eliminates the possibility of a painful plantar incision. Furthermore, this technique allows for maintenance of the plantar plate, flexor hallucis brevis (FHB) tendon, and all other ligamentous structures that attach to the sesamoids. Larger studies with longer term follow up are needed to further our knowledge on this surgical technique.
DOI: 10.1177/2473011421S00189
Acute Achilles Tendon Rupture, A More Cost-Effective Surgical Technique Option: Dresden-Calcaneal Tunnel
Gonzalo Enríquez, MD; Mario I. Escudero, MD; Manuel J. Pellegrini, MD; Alfredo Nuñez
Introduction/Purpose: Surgical treatment remains the standard of care for active patients with acute midsubstance Achilles tendon ruptures. Clinical decisions must be made, often under circumstances of limited resources. The objective of our study was to describe a reduced cost minimally invasive surgical technique. The use of suture anchor increases the tensile strength of the repair, allowing to prevent tendon lengthening and re-ruptures during early rehabilitation, but these present a high cost and are not exempt from complications such as pullout, local irritation and bone edema. A simple and low-cost alternative that allows us to replace the function of the anchors is to drill a bone tunnel in the calcaneus and pass a high-resistance suture through it.
Methods: After obtaining IRB approval, a retrospective review of 12 patients with acute Achilles tendon rupture treated with the modified Dresden-Calcaneal Tunnel technique, between January 2019 and August 2020 and followed up for 6 months. Clinical outcome was assessed using the AOFAS, FAOS and SF-36 scores. Complications, and time to return to work and light sport activity were assessed.
Results: The AOFAS score was 94 +/- 5, FAOS 95% +/- 2 and SF-36 92 +/- 4 at 6 months postoperatively. The recovery time of the patients was 10-18 weeks. The postoperative recovery time to exercise was 16-24 weeks. There was only 2 cases with discomfort in relation to the suture knot near to the calcaneal tunnel, but both case refers spontaneous relief at the second month postoperative.
Conclusion: This new and minimally invasive technique could be a more cost-effective option in the management of acute Achilles tendon rupture with good functional outcomes. These strategy presents a low occurrence of complications, permit a strong fixation, avoid sural nerve entrapment and respect the biologic environment.
DOI: 10.1177/2473011421S00190
Extended Chevron Osteotomy in the Management of Mild-Severe Hallux Valgus: Clinical Results in a Long-Term Follow-Up
Abraham Espinosa-Uribe, MD; Jaime I. Ortiz Garza, MD; Jorge Luis R. Terán; Fernando Alfredo F. Garza; Eduardo R. Carranza-Cantú, MD; Jorge A. Gutierrez, MD, MA
Category: Bunion
Keywords: Osteotomies; Bunion; Hallux Valgus
Introduction/Purpose: Hallux Valgus (HV) is a forefoot complex deformity. More than 200 surgical techniques for its treatment have been described, Chevron Osteotomy and its modifications represent a widely accepted highly reproducible option in the HV treatment. Since described in 1991 the Extended Chevron Osteotomy (ECO) represents a distal osteotomy with a plantar diaphyseal extension. Biomechanically the advantages it offers are even greater stability, early consolidation by increasing the contact surface and correcting the facet with a minimum shortening. It also offers lower morbidity and a lower rate of complications. However, there is controversy regarding long-term follow-up for most of these procedures. This study aims to demonstrate ECO for the correction of moderate to severe HV in a long-term follow-up.
Methods: We reviewed 25 feet (20 patients) with moderate to severe HV in which the Intermetatarsal Angle (IMA) greater than 16⁰. The mean age was 64 years and the patients were followed by a mean of 30 (14 to 59) months. Additionally, 8 patients (N=12 feet) were followed with a mean of 68 (50 to 86) months. The following scales were applied before and after surgery: the functional scale of the American Orthopaedic Foot & Ankle Society (AOFAS) for the forefoot and the Visual Analog Scale (VAS). In the same way, the radiographic measurements corresponding to HV were made pre and postoperative. This research study was approved by our institution and hospital research ethics committee. Additionally, all the patients were reviewed under the Mexican law NOM-004-SSA3-2012 regarding Clinical file and privacy rights.
Results: In the AOFAS for forefoot and VAS scales an improvement of 51.28 (CI95% 46.34 to 56.21) -6.08 (CI 95%-6.65 to -5.50) points, respectively. Regarding the angular values, the correction was -9.08⁰ (CI 95% -10.29 to -7.86) for the IMA. There was one foot with post-surgical infection (4%) and two feet (8%) with transfer metatarsalgia. Additionally, we documented a mean AOFAS forefoot score of 90.16 (+- 5.27) and a mean of 0.8 (+- 0.4) VAS scale during a second follow-up period of 68 months (range from 50 to 86 months) in 8 patients (N=12 feet). Statistically significant differences (p <0.05) were documented by the means of these long-term follow-up periods in the AOFAS score and VAS scale regarding the pre-surgical scores.
Conclusion: According to the results obtained, we consider that the ECO technique for the treatment of moderate to severe HV provides significant functional improvement and angular correction (p <0.05) and good clinical outcomes on both long-term follow-up periods. ECO technique represents a highly reproducible option when performing HV correction.
DOI: 10.1177/2473011421S00191
Correction of Ankle Varus Deformity using Patient Specific Dome Shaped Osteotomy Guides Designed on Weight Bearing CT
Sebastian Faict; Arne Burssens; Kristian Buedts, MD
Introduction/Purpose: Dome shaped supramalleolar osteotomies are a well-established treatment option for correcting ankle deformity. However, the procedure remains technically demanding and is limited by a two-dimensional (2-D) radiographic planning of a three-dimensional (3-D) deformity. Therefore, we implemented a weight-bearing CT-scan (WBCT) to plan a 3-D deformity correction using patient specific guides.
Methods: A 3-D guided dome shaped supramalleolar osteotomy was performed to correct ankle varus deformity in a cohort of 5 patients with a mean age of 53,8 years (range: 47-58). WBCT images were obtained to generate 3-D models, which enabled a deformity correction using patient specific guides. These technical steps are outlined and associated with a retrospective analysis of the clinical outcome using the EFAS score, Foot and Ankle Outcome Score (FAOS) and Visual Analog Pain scale (VAS). Radiographic assessment was performed using the tibial anterior surface angle (TAS), tibiotalar angle (TTS), talar-tilt angle (TTA), hindfoot angle (HA), tibial lateral surface angle (TLS) and tibial rotation angle (TRA).
Results: The mean follow-up was 40,8 months (range 8-65) and all patients showed improvements in the EFAS score, FAOS and VAS (p < 0.05). A 3-month postoperative WBCT confirmed healing of the osteotomy site and radiographic improvement of the TAS, TTS and HA (p<0.05), but the TTA and TRA did not change significantly (p>0.05).
Conclusion: Dome shaped supramalleolar osteotomies using 3-D printed guides designed on WBCT, are a valuable option in correcting ankle varus deformity and mitigates the technical drawbacks of free-hand osteotomies.
DOI: 10.1177/2473011421S00192
Retrospective Chart Review: Weight Bearing CT Scans and the Measurement of the Lisfranc Ligamentous Complex
Spencer Falcon, MD; Thomas J. McCormack; Matthew Mackay, MD; Armin Tarakemeh, BA; Scott Mullen, MD; Paul Schroeppel, MD; Megan R. Wolf, MD; Bryan G. Vopat, MD
Introduction/Purpose: Lisfranc Ligamentous Complex injuries are commonly misdiagnosed due to their unreliable projection on plain films. Many studies have striven to establish baseline measurements of the frequently injured articulations. While cadaver, MRI, ultrasound, and non-weight bearing computer tomography (CT) have been utilized, weight bearing CT (WBCT) scans are a relatively new imaging modality that has not yet been utilized to establish reproducible and widely-referenced baseline anatomic positions. The hyoptheses of this study are: 1. Standing, weight bearing CT scan will allow for evaluation and measurement of the Lisfranc joint complex. 2. There will be no side to side variation or sex-based differences in the Lisfranc joint complex.
Methods: A retrospective chart review was conducted using the electronic medical record. Inclusion criteria was applied as follows: patients who have undergone weight bearing CT of the bilateral lower extremities from 2018 to 2020. One hundred twelve foot CT scans were acquired for measurements. Measurements were collected by two independent reviewers twice in order to achieve inter- and intra-reliability. The measurements were then analyzed in order to establish a baseline for normal anatomy, compare injured to non-injured side, and observe any sex-based differences.
Results: Measurements of uninjured legs were utilized to define normal parameters for Lisfranc ligamentous complex (LLC) injuries. Averages were found for measurements of base 1 to 2 MT 2.7mm (SD=0.7mm), medial cuneiform to 2nd MT [M2-C1] 3.7mm (SD=0.7mm), intercuneiform distance 1.2mm (SD=0.3mm), sagittal descent 12.2mm (SD=5.4mm).Patient’s with injury to LLC had a larger base of M1-M2, distance from base of first metatarsal to base of second metatarsal (Δ=.5903, p <.0001) and M2- C1 interval (Δ=1.8008, p<0.0001). Males had significantly higher M2-C1 (p=0.0031), intercuneiform distance (p=0.0039), and sagittal descent (p=0.0008) compared to female patients.No significant differences were found with regard to left vs right side in any of the measurements. Intercuneiform distance (p=0.0039) was found to significantly decrease as age increased, while sagittal descent significantly increased with increased age (p=0.0066).
Conclusion: This study is one of the first investigations aims to assist in defining baseline anatomic measurements for Lisfranc ligamentous complex parameters on WBCT. The values and comparisons obtained were able to reinforce that weight bearing CT is valuable in identifying subtle injuries to the LLC while also demonstrating that there is male-to-female and age-related differences that should be kept in mind when radiographically evaluating imaging studies of injured patients.
DOI: 10.1177/2473011421S00193
Retrospective Chart Review: Weight Bearing CT Scans and the Measurement of the Tibiofibular Syndesmosis
Spencer Falcon, MD; Thomas J. McCormack; Matthew Mackay, MD; Armin Tarakemeh, BA; Scott Mullen, MD; Paul Schroeppel, MD; Megan R. Wolf, MD; Bryan G. Vopat, MD
Introduction/Purpose: Tibiofibular Syndesmosis injuries are commonly misdiagnosed due to their unreliable projection on plain films. Many studies have striven to establish baseline measurements of the distal tibial and fibular articulation. While cadaver, MRI, ultrasound, and non-weight bearing computer tomography (CT) have been utilized, weight bearing CT (WBCT) scans are a relatively new imaging modality that has not yet been utilized to establish reproducible and widely-referenced baseline anatomic positions. The hypotheses of this study are: 1. Standing, weight bearing CT scan will allow for evaluation and measurement of the tibio-fibular syndesmosis. 2. There will be no side to side variation or sex-based differences in syndesmosis measurements.
Methods: A retrospective chart review was conducted using the electronic medical record. Inclusion criteria was applied as follows: Patients who have undergone weight bearing CT of the bilateral lower extremities from 2018 to 2020. One hundred twenty ankle CT scans were acquired for measurements. Measurements were collected by two independent reviewers twice in order to achieve inter- and intra-reliability. The measurements were then analyzed in order to establish a baseline for normal anatomy, compare injured to non-injured side, and observe any sex-based differences.
Results: Measurements of uninjured legs were utilized to define normal parameters for tibiofibular syndesmosis on weight bearing CT. Averages were found for measurements of anterior incisura 3.2mm (SD=1.1mm), middle incisura 3.9mm (SD=1.1mm), posterior incisura 5.6mm (SD=1.7mm), alpha angle 16.3° (SD=6.3°), medial clear space 2.2mm (SD=0.6mm).Patients with syndesmotic injuries had significantly larger measurements for anterior (p<0.0001), middle (p=0.0007), and posterior incisura (p=0.002) when compared to uninjured ankles. Males had significantly higher medial clear space widening (p=0.0012) compared to female patients. Anterior incisura (p <0.0001), posterior incisura (p=0.0005) were found to significantly decrease as age increased.
Conclusion: This study aims to assist in defining baseline anatomic measurements for syndesmotic parameters. The values and comparisons obtained were able to reinforce that weight bearing CT is valuable in identifying subtle injuries to the TFS while also demonstrating that there is male-to-female and age-related differences that should be kept in mind when radiographically evaluating imaging studies of injured patients.
DOI: 10.1177/2473011421S00194
Contact Pressure Reduction in the Anterior Ankle During Placement of Short Leg Splints
Nicholas Farrar, MD; Kempland C. Walley; Kameron A. Shams, MD; Kristopher Mell; David M. Walton, MD; James R. Holmes, MD; Paul G. Talusan, MD
Category: Trauma; Ankle
Keywords: Wound Complications; Trauma; Biomechanics of the Foot and Ankle
Introduction/Purpose: Lower extremity splints are commonly used in orthopaedic care throughout emergency departments, operating rooms, and outpatient clinics. Although the mainstay of ankle immobilization, they have been associated with ulcers due to high contact pressures over bony prominences and the anterior ankle. High contact pressures may occur in the anterior ankle when splint padding is applied while the ankle is in a plantarflexed position and subsequently dorsiflexed as the plaster or fiberglass hardens. The purpose of this study is to measure contact pressures in the anterior ankle when cast padding is applied in a plantarflexed position and subsequently dorsiflexed. We hypothesized, that the removal of padding over the anterior ankle following dorsiflexion would result in reduced anterior ankle contact pressures.
Methods: Short leg posterior U-splints were applied to the right lower extremity in two healthy volunteers with an underlying pressure transducer [Tekscan I-Scan system (Tekscan Inc, South Boston, MA, USA)] on the skin surface centered over the tibialis anterior tendon. Anterior ankle surface pressures were measured when the padding was applied in maximum plantar flexion and dorsiflexed to neutral position as measured by a goniometer. This was then repeated in the same subjects but prior to dorsiflexion, a 3cm x 3cm square of padding was removed over the pressure transducer prior to dorsiflexion. Percent change from initial contact pressure centered on the tibialis anterior with either Webril (Covidien/Medtronic, Dublin, Ireland), or Specialist Cotton Blend Cast Padding (BSN Medical, Charlotte, NC, USA) was calculated.
Results: There were 2 limbs analyzed for presentation of this pilot data. The percent change in anterior ankle contact pressure when padding was applied in plantar flexion and then placed in neutral was an average increase of 264% with just padding and 238% with padding and plaster. [TP1] Subsequently, the removal of padding from the anterior ankle resulted in an average decrease of 126% of[TP2] the increased pressure relative to baseline measurements (Figure 1). The reduction in contact force with the removal of Webril was greater than Specialist.
Conclusion: In this pilot data, we report increases in anterior ankle contact pressures when splint padding is applied in plantar flexion and re-positioned into neutral. However, removal of anterior ankle padding reduces pressure over the anterior ankle and may reduce the risk of iatrogenic splint related ulcers in this area. Additionally, this technique may elicit varying reductions in anterior ankle pressure depending on the type of cast padding utilized. This data, though preliminary, underscores the importance of avoiding excess padding over the anterior ankle during splint application.
DOI: 10.1177/2473011421S00195
A Biomechanical Investigation on the Effects of Deep Deltoid Ligament Repair Combined with Flexible and Rigid Syndesmotic Fixation
John E. Femino, MD; Christina Hajewski; Jessica E. Goetz, PhD; Kyle R. Duchman, MD
Introduction/Purpose: The role of deep deltoid ligament (DDL) repair in the setting of an unstable syndesmotic injury is largely unknown, and the optimal fixation strategy for syndesmosis stabilization is controversial. The purpose of this study was to investigate the effect of an augmented, anatomic repair of the DDL combined with flexible or rigid syndesmotic stabilization using a cadaveric model.
Methods: 10 pairs of fresh-frozen through knee cadaveric specimens were used for biomechanical testing which included subjecting the specimens to 5 Nm of external rotation torque while under 750 N of axial compression. Whole-foot rotation angles were measured and rotation and translation of the fibula, tibia, and talus were tracked with optical motion capture. Specimens were tested intact and then after destabilization by sectioning the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament, interosseous ligament and membrane extending 7 cm proximal to the ankle joint, and both bands of DDL. The intact fibula was a surrogate for an anatomically fixed fibula. Each specimen underwent mechanical testing both with and without DDL reconstruction added to flexible syndesmotic stabilization using a suture button (SB) plus AITFL reconstruction. In the final test, the syndesmosis was rigidly stabilized using a 4.5 mm screw.
Results: Destabilization increased the foot rotation under the applied axial load and torque to 170% (+-49%) of that of the intact case. After flexible syndesmotic stabilization (AITFL + SB) foot rotation was 109% (+-26%) of intact condition. Addition of the deltoid ligament reconstruction (AITFL + SB + DD) reduced rotation to 87% (+-31%) of the intact condition. Fixation with a screw alone came closest to the rotation of the intact specimen (93% +- 17% of intact), and like the flexible repair, the addition of DDL reconstruction to the screw increased rotational stability (85% +- 35% of intact).
Conclusion: DDL reconstruction provides improved resistance to external rotation stress when added to both flexible and rigid syndesmotic stabilization. Although our results with both the flexible and rigid constructs demonstrated increased constraint to external rotation stress compared to the intact specimen, these results should be thought of as time zero data, and the implants likely experience some creep with early motion and graduated weight bearing. Our demonstration of increased stability with a deltoid ligament reconstruction suggests that this addition may be beneficial for unstable syndesmotic injuries.
DOI: 10.1177/2473011421S00196
Divergent vs Parallel Screw Configurations for Subtalar Arthrodesis: Comparing Clinical Outcomes
Carlton Fernandes; Eric B. Johnson; Brandon W. Moritz; Matthew R. McDonald, MD; Amgad M. Haleem Amin, MD, PhD; Paul A. Kammerlocher, MD
Introduction/Purpose: Subtalar arthrodesis is a frequently performed surgery used to treat several hindfoot pathologies. Rigid fixation is essential for successful fusion and percutaneous screws are most commonly used. Controversy still exists regarding the most optimal screw configuration. While cadaveric biomechanical studies have shown diverging screw configuration to be superior to parallel screws, this has never been proven in the clinical setting. The aim of this study was to compare fusion rates and clinical outcomes between patients treated with divergent versus parallel screw constructs for subtalar arthrodesis.
Methods: We conducted a retrospective review of 58 patients that underwent subtalar arthrodesis during a four-year period at our institutions. Patients were divided into two groups based on screw construct; diverging versus parallel. Outcomes measured were radiographic and clinical evidence of fusion at 3 months, American Orthopaedic Foot & Ankle (AOFAS) ankle-hindfoot and Visual Analog Scale (VAS) scores at final follow up and post-operative complications.
Results: Thirty patients underwent subtalar fusion with a divergent screw construct and twenty-four with parallel screws. The mean age was 58.5+-13.9 years and mean follow up period was 44.5+-20.8 months. The overall fusion rate at 3 months was 94.8%. The fusion rate for the divergent screw group was 93.3% versus 96.4% for the parallel screw group, showing no statistical significance (p=0.60). Overall, the mean AOFAS and VAS scores improved post-operatively by 28.1+-5.49 and 4.27+-1.45 points respectively (p<.0001). In the divergent group, mean improvement in AOFAS and VAS scores was 28.5+- 4.99 and 4.39+-1.42 versus 27.7+-6.05 and 4.14+-1.48 in the parallel screw group, showing no statistical significance (p=0.59 and p=0.44). The overall complication rate was 5.2% with no statistically significant difference between the two groups (6.7% versus 3.6%, p=0.60).
Conclusion: When used for fixation during subtalar arthrodesis, divergent and parallel screw constructs have similar radiological union rates and clinical outcomes when it comes to fusion rates at 3 months, post-operative improvement in AOFAS scores and complication rates. Screw configuration should be determined by surgeon experience and comfort level.
DOI: 10.1177/2473011421S00197
Prospective Radiographic Assessment of Intraoperative Range of Motion with Total Ankle Replacement
Oliver Gagné, MD; Rogerio C. Bitar; Jaeyoung Kim, MD; Kristin C. Caolo, BA; Guilherme H. Saito, MD; Elizabeth Cody, MD; Jonathan T. Deland, MD; Scott J. Ellis, MD; Constantine A. Demetracopoulos, MD
Category: Ankle Arthritis
Keywords: Ankle Arthroplasty; Ankle Arthritis; Gait Study Range of Motion
Introduction/Purpose: One of the proposed benefits of total ankle replacement, when compared to ankle fusion is the preservation of range of motion (ROM) of the ankle. Preservation of ankle motion may improve quality of life as evidenced by patient-reported outcome measures (PROMs). However, despite improving dorsiflexion intraoperatively during TAR, studies have not demonstrated large improvements in dorsiflexion (DF) at final followup after TAR. The objective of this study was to radiographically evaluate and quantify preoperative, intraoperative ankle dorsiflexion and plantarflexion (PF), compare it to post- operative ankle ROM, and determine the effect of Achilles lengthening (TAL) on preserving dorsiflexion motion that is gained during surgery.
Methods: This prospective study compared 111 patients with an average age of 62.3 years who underwent primary total ankle replacement with one of four different implants between March and December 2019. A total of 71 patients (64%) had an associated TAL based on the surgeon’s decision. Intraoperative fluoroscopy was utilized by the primary surgeon to document the maximal dorsiflexion and plantar flexion at the end of the case. This was completed after the TAL on a perfect lateral. Standardized weight bearing at maximum ROM positions lateral radiographs were obtained twelve months postoperatively. The change in range of motion was analyzed using a paired t-test with a significance level of 0.05.
Results: The cohort’s preoperative range was 22.0° (8.1°DF, 14°PF) and was increased to 38.5° intraoperatively (12.7°DF, 25.8°PF) as described in Table 1. Postoperative ROM is 24.9° (11.7°DF, 13.2°PF) which means that 65% of the intraoperative ROM is preserved. Preoperative and intraoperative range of motion was not different between the group that had a TAL compared to no TAL. At the year postoperatively, the dorsiflexion was similar between both groups. The group who did not have a TAL went from 12.8 intraoperatively to 12.2° postoperatively whereas the group who had a TAL went from 12.2° to 11.3° which was statistically equivalent.
Conclusion: This study is the first to assess how much ankle range of motion is retained after TAR. Overall, we observed that 65% of dorsiflexion was retained after TAR. TAL as a concomitant procedure did not effect the proportion of dorsiflexion motion that was retained. Additional studies are needed to determine how to best optimize and increase ROM after TAR.
DOI: 10.1177/2473011421S00198
Proximal Fifth Metatarsal Fracture Treated with Plantar Plating: Retrospective Multi-Surgeon Case Series
Stephanie S. Gardner, MD; Derek M. Klavas, MD; Pedro E. Cosculluela, MD; Travis W. Hanson, MD; Keith A. Heier, MD; Kevin E. Varner, MD
Category: Midfoot/Forefoot; Sports; Trauma
Keywords: 5th Metatarsal Fractures; ORIF; Trauma
Introduction/Purpose: Proximal fifth metatarsal fractures are a common foot injury. Previous surgical treatments have consisted of intramedullary screw fixation and a newer technique of plantar plating due to non-union and refractures seen with screw fixation. Purpose of this multi-surgeon case series study is to evaluate clinical and radiographic outcomes and complication rates after fifth metatarsal plating for proximal fifth metatarsal fractures in recreational and elite athletes.
Methods: Retrospective multiple surgeon case series involving patients who underwent fifth metatarsal plantar plating for proximal fifth metatarsal fractures with a mean follow-up of 33.1 months (range, 12-52). Elite and recreational athletes were included. Demographic data, radiographic evaluation, and clinical notes were analyzed. Patient phone conversations were made to document complications outside of our electronic medical record.
Results: Forty-four patients (45 fractures) were treated with plantar plating technique with a mean age of 37.3 years (range 14- 80). Five patients sustained refractures (11.1% of patients), 2 at previous fracture site, 1 through a screw hole, 1 proximal to plate, and 1 distal to plate. All refractures were treated non-operatively. No wound complications were seen. No secondary revision surgery was needed and union rate was 100% at final follow up.
Conclusion: With a one year minimum follow up, plantar plating of proximal fifth metatarsal fractures is a viable option for treatment of both acute and chronic fractures as well as after failed intramedullary screw fixation with low refracture rates and without non-unions. Plantar plating allows the surgeon to have direct visualization of fracture reduction and ease of access for bone grafting. Both elite and recreational athletes can benefit from the plating technique.
DOI: 10.1177/2473011421S00199
National Survey of COVID-19 Infections Among Head Surgical Specialists Regarding Orthopedic Foot and Ankle Surgeons in Mexico
Fernando Alfredo F. Garza; Jaime I. Ortiz Garza, MD; Abraham Espinosa-Uribe, MD; Eduardo R. Carranza-Cantú, MD; Jorge A. Gutierrez, MD, MA
Category: Other
Keywords: Changes; Health Care; Practice Models
Introduction/Purpose: The health contingency due to COVID19 has represented an unprecedented state of health contingency with implications for the economy and public health. There is a concern in the medical community regarding the risk of contagion of COVID19. Recently, the occupational risk of contagion by COVID19 has been described in surgical specialties that involve proximity to the face and airway of the patient Ophthalmology and Otorhinolaryngology and head and neck surgery (ENT). A possibility has been raised that Foot and Ankle joint surgeons have some occupational protection due to the distance greater than 1m with respect to the patient’s airway during surgical activities. The objective of this study is to compare COVID-19 infections referred by different surgical specialties and subspecialties.
Methods: An observational, cross-sectional, and descriptive study will be carried out in which a survey will be applied to 134 surgical specialists divided into 3 groups (ophthalmology, ENT, and orthopedic surgeons performing foot and ankle surgery) during the months of August to September 2020.Percentage prevalences of each variable to be evaluated will be obtained, likewise, a Chi- square test will be applied to determine statistical differences between the proportions of referred positivity in the 3 groups. This research study was reviewed by our institution and hospital research ethics committee. All participants gave their informed consent at the time of conducting the survey, as well as allowing the use of their responses for the purposes of this project.
Results: A total of 134 surveys pertaining to 30, 69, and 35 Mexican ophthalmology, ENT, and orthopedic surgeons who perform foot and ankle surgery respectively were evaluated. The geographical distribution of the surveys is identified in figure 1. After the statistical analysis, non-significant statistical differences (p> 0.32) were documented in the proportion of infections between ophthalmologists or ENTs, with respect to the proportion of infections referred by COVID-19 in the group of Orthopedic foot and ankle surgeons surveyed.
Conclusion: When analyzing the results of this survey-type study, it is possible to establish that the statistically non-significant differences between the proportions of infections of the groups of specialists evaluated could suggest that the working distance with respect to the patient’s airway is not a protective factor for contagion. by COVID-19. Preventive strategies, as well as the vaccination of health personnel involved in patient care, are essential.
DOI: 10.1177/2473011421S00200
The Adelaide Experience: Short Term Results with the Use of Cartiva Implant
Gil Genuth, MD; Peter Stavrou, MD, FRACS; Christopher H. Brown, FRACS, MBBS, FRCSC
Introduction/Purpose: Hallux rigidus is the most common arthritic condition of the foot. There are only few surgical options that does not require fusing the 1st MTPJ thus allowing motion in the joint. A new first metatarsophalangeal (MTP) joint hemiarthroplasty with a polyvinyl alcohol (PVA) hydrogel implant (Cartiva) has demonstrated pain relief and functional outcomes equivalent to first MTP arthrodesis at 2 and 5 years postoperation in few studies done in North America. We would like to present the Adelaide short term result with the use of this implant.
Methods: 40 Patients who underwent first PVA hydrogel MTP hemiarthroplasty in Adelaide by two senior foot and ankle surgeons (C.B and P.S) and by two international foot and ankle fellow (G.G and J.P) between 2017 and 2019 were included in this study. The follow up period was 24 months postoperation. Patients underwent physical examination and radiographic evaluation and completed a pain VAS, the Short-Form-36 (SF-36), and the Foot and Ankle Ability Measure (FAAM) sports subscale and activities of daily living (ADL) subscale. At the time of this study, 40 patients had reached 2 year follow-up.
Results: There were no lost to follow up, leaving 40 patients with mean age 63.4 (range, 40.1-79.9) years. Mean follow-up was 24 months (range, 6-30 months). Postoperative active MTP natural joint dorsiflexion and peak MTP dorsiflexion were mean 18.2 (range, 10.0- 30.0) and 29.7 (range, 10.0-45.0) degrees, respectively. Pain VAS, SF-36, FAAM ADL, and FAAM Sports scores demonstrated clinically and statistically significant improvements. Radiographically, no patient demonstrated changes in implant position, implant loosening or subsidence, or implant wear. One implant was removed because of persistent pain 7 months post surgery and was converted to fusion 3 months after the removal of the Cartiva implant.
Conclusion: Short term results for the use of Cartiva implant in Adelaide show that functional outcomes improved significantly, pain was reduced significantly, and the implant demonstrated excellent survivorship. Our results are similar for those described in the North American literature
DOI: 10.1177/2473011421S00201
An Anatomical Study of the Sural Nerve: A Review of Cadaveric Data and Comparison with 3 Tesla MRI
Claudio B. Ghetti; Brendon Mitchell; Vrajesh J. Shah; Brady K. Huang; William Kent; Ian M. Foran, MD
Introduction/Purpose: The sural nerve (SN) is a distal cutaneous nerve that provides sensation to the lateral foot and ankle, and is at risk of iatrogenic injury during surgery at the foot and ankle.1 Previous anatomic studies of the SN are limited to cadaveric studies with small sample sizes.2,3,4,5,6,7,8,9 We analyzed a large cohort of high-field 3 Tesla (3T) magnetic resonance images (MRI) of the ankle to obtain a more generalizable, in-vivo sample of the distal course of the SN. A comparison of this in- vivo method of measurement vs. cadaveric studies may provide surgeons with a more accurate representation of SN anatomy and its relation to anatomic landmarks.
Methods: We performed a retrospective review of 3T MRI studies of the ankle performed at our institution between January 2015 and December 2020. Three blinded reviewers measured the vertical distance of the SN to the distal tip of the lateral malleolus (DTLM), the horizontal distance of the SN to the DTLM, and the lateral border of the Achilles tendon (LBA) at the level of the DTLM. Also measured was the horizontal distance of the SN to the LBA at the level of superior Achilles insertion (SAI) onto the calcaneus as well, as 5 cm above the SAI. Intraclass correlation coefficient was calculated to assess reliability between reviewers. A total of 204 3T MRIs of the ankle were included.
Results: The mean vertical distance from the SN to the DTLM was 2.2 +- 0.5 cm (ICC, 0.85; range 0.9-3.6 cm). The mean horizontal distance of the SN to the DTLM at the level of DTLM was 1.7 +- 0.3 cm (ICC, 0.98; range 0.8-3.0 cm). The mean horizontal distance of the SN to the LBA at the level of DTLM was 1.9 cm +- 0.3 cm (ICC, 0.91; range 1.0-2.9 cm). The mean horizontal distance from the SN to the LBA at the level of the SAI and 5 cm above the SAI was 2.6 +- 0.4 cm (ICC, 0.85; range 1.4-3.7 cm) and 0.9 +- 0.2 cm (ICC, 0.87; range 0.4-1.8 cm), respectively. Neither height nor BMI were strongly associated with the distance of the SN to any of our anatomic landmarks (R2 < 0.08 for all measurements).
Conclusion: Several of our measurements summarized in differed from those reported in previous cadaveric studies. Although our mean horizontal distance of SN to LBA at SAI differed notably from cadaveric studies (2.6 cm vs 1.8-2.1 cm), a 2018 ultrasound study of the SN by Popieluszko et al observed a mean distance of 2.4 cm for this measurement. This concordance may indicate reliability between in-vivo methods of measurement vs. cadaveric studies. In-vivo measurements may also provide a more accurate representation of the anatomy, as these methods are not subject to the effects of embalming and dissection required of cadaveric studies.
DOI: 10.1177/2473011421S00202
The Relationship of the Sural Nerve and Anatomic Landmarks Relevant to the Extensile Lateral and Sinus Tarsi Approaches: A 3T MRI Study
Claudio B. Ghetti; Brendon Mitchell; Vrajesh J. Shah; Brady K. Huang; William Kent; Ian M. Foran, MD
Category: Hindfoot; Trauma
Keywords: Calcaneal Fractures; Sinus Tarsi Approach; Calcaneus Fractures - Treatment
Introduction/Purpose: The extensile lateral and sinus tarsi approaches are commonly used during foot and ankle surgery, and pose a risk of iatrogenic injury to the sural nerve, a cutaneous nerve that innervates the ankle and lateral foot. Our understanding of the SN’s location is based primarily on anatomic cadaver studies with small sample sizes. Our research analyzes a large cohort of high-field 3 Tesla (3T) magnetic resonance images (MRI) of the ankle to obtain a more generalizable, in-vivo sample of the distal course of the SN. A better understanding of the course and variability of the sural nerve will allow surgeons to minimize the risk of iatrogenic injury to the SN.
Methods: High-field 3T MRI studies of the ankle performed at our institution between January 2015 and December 2020 were analyzed. The vertical distance of the SN to the distal tip of the lateral malleolus (DTLM), horizontal distance of the SN to the DTLM, and the lateral border of the Achilles tendon (LBA) at the level of the DTLM were measured by 3 blinded reviewers. Also measured was the horizontal distance of the SN to the LBA at the level of superior Achilles insertion (SAI) onto the calcaneus, as well as 5 cm above the SAI. We then analyzed upper and lower quartile ranges to compare the outer anatomic distribution frequencies of the SN to the locations of common approach incision lines. This outer limit analysis may serve to quantify the variability of the SN.
Results: A total of 204 3T MRIs of the ankle were included. 1st and 4th quartile ranges for vertical distance from the SN to the DTLM were 0.9-1.9 cm and 2.5-3.6 cm respectively. 1st and 4th quartile ranges for horizontal distance of the SN to the DTLM at the level of DTLM were 0.8-1.5 cm and 2.0-3.0 cm respectively. 1st and 4th quartile ranges for horizontal distance of SN to the LBA at the level of DTLM were 1.0-1.6 cm and 2.1-2.9 cm respectively. 1st and 4th quartile ranges for horizontal distance of SN to the LBA at the level of the SAI were 1.4-2.3 cm and 2.8-3.7 cm respectively. 1st and 4th quartile ranges for horizontal distance of SN to the LBA, 5 cm above SAI were 0.4-0.8 cm and 1.0-1.8 cm, respectively.
Conclusion: The vertical distance from SN to DTLM was greater than the previously reported maximum of 2.6cm in 25% of cases. This highlights the risk of injury to the sural nerve with the extensile lateral approach. Our first quartile range for vertical distance of SN to DTLM of 0.9-1.9cm indicates that even at the lowest range of values, the SN remains clear of the incision line used in the sinus tarsi approach, which extends from the DTLM to the base of the fourth metatarsal. The sural nerve is still at risk during posterior extension or retraction of the sinus tarsi incision.
DOI: 10.1177/2473011421S00203
Autologous Osteochondral Transplantation for Osteochondral Lesions of the Talus: Does Gender Impact Outcomes?
Arianna L. Gianakos, DO; Olasumnbo Okedele; Sean Flynn; Mary K. Mulcahey, MD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle
Keywords: Autograft; Ankle; Osteochondral Lesions of the Talus
Introduction/Purpose: Autologous osteochondral transplantation (AOT) is commonly used in the treatment of osteochondral lesions (OCL) of the talus. There is limited data comparing gender differences in the incidence and presentation of talar OCLs and resultant outcomes following AOT. The purpose of this study is to compare these differences between male and female patients.
Methods: Eighty-seven consecutive patients who underwent AOT were retrospectively reviewed. Patients were divided into two groups based on gender. Demographic data and OCL defect characteristic data were recorded. Functional outcomes were assessed pre- and post-operatively using the Foot and Ankle Outcome Score (FAOS). The Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score was used to assess cartilage incorporation.
Results: Fifty-six (64%) males and 31 (36%) females with a mean clinical follow-up was 47.2 months were included in this study. OCL defect size was significantly larger in male patients (112.8mm2) when compared with female patients (88.7mm2) (p<0.0001). Male patients presented with a significantly longer duration of symptoms (p<0.001) and OCLs were more likely to be associated with a recognized trauma (p=0.0006) when compared with female patients who typically presented with associated chronic ankle instability. Mean FAOS improved pre- to postoperatively from 50 to 81(p< 0.001) with a statistically significant increase found in male patients (p<0.0001). The mean MOCART score was 82.1 in male and 86.7 female patients. (p<0.0001).No differences were found in knee donor site morbidity, complication rate, or revision surgery between male and female patients.
Conclusion: Our study demonstrates that male patients typically present with talar OCLs that are larger in size, associated with a recognized trauma, and with longer symptom duration when compared with female patients. Talar OCLs in female patients typically were smaller in size and associated with chronic ankle instability. In addition, male patients had greater improvement in FAOS scores following AOT. Therefore, understanding these differences may influence the management and treatment of talar OCLs in male and female patients.
DOI: 10.1177/2473011421S00204
Gender May Affect Mid-Term Outcomes Following Bone Marrow Stimulation for Osteochondral Lesions of the Talus
Arianna L. Gianakos, DO; Emilie Williamson, MD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle
Keywords: Osteochondral Lesions of the Talus; Lesions of Talus; Clinical Outcomes
Introduction/Purpose: Bone marrow stimulation (BMS) is typically indicated as a surgical intervention for patients who have symptomatic osteochondral lesions of the talus (OLT). Despite differences in ankle biomechanics and cartilage morphology between male and female patients, there is scant evidence examining whether these differences affect outcomes following BMS. The purpose of this study was to compare the outcomes in female and male patients following BMS in the treatment of OLTs.
Methods: A retrospective analysis comparing female and male patients treated with BMS for OLT between 2007 and 2015 was performed. Clinical outcomes were evaluated using the Foot and Ankle Outcome Scores (FAOS) and Short-Form 12 (SF-12). Magnetic resonance imaging (MRI) at final follow-up was evaluated with the modified magnetic resonance observation of cartilage repair tissue (MOCART) score.
Results: Thirty-one females and 38 males were included in this study. The mean patient age was 39.6+-16.9 for females and 36.5+-14.5 years for males. There was no significant difference in age, lesion size, follow-up time, and a number of concomitant procedures. Lateral lesions occurred more frequently in male patients (p=0.034). In female patients, the mean FAOS pain score improved from 60.2 +- 15.5 preoperatively to 84.0 +- 8.9 at 1-2 year follow-up (p<0.001), and then decreased to 80.0 +- 13.1 at final follow-up at 3-4 years, which was not statistically significant (p=0.191). In male patients, the mean FAOS pain score improved from 64.7 +- 17.0 preoperatively to 83.1 +- 9.2 at 1-2 year follow-up (p<0.001), and then decreased to 76.0 +- 14.6 at final follow- up at 3-4 years (p=0.023). The mean MOCART scores were 59.3 +- 24.0 in female patients and 67.3 +- 23.6 in male patients (p=0.278).
Conclusion: Lateral lesions were more common in male patients possibly indicating an acute traumatic etiology. Medial lesions were more common in female patients indicating potentially a chronic pathology. This may have implications in reducing the incidence of OLT in female patients. The outcomes following BMS in both female and male patients were good with no significant differences in FAOS pain score and MOCART score at short-term follow-up. FAOS scores in male patients were more likely to decrease after 1-2 years post-surgery, implying a possibly faster decline than in female patients.
DOI: 10.1177/2473011421S00205
Long-Term Outcomes of Autograft Osteochondral Transplantation for Osteochondral Lesions of the Talus: Eight to Twelve Years Follow-Up
Arianna L. Gianakos, DO; Nathaniel P. Mercer; John Dankert, MD,PhD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle
Keywords: Osteochondral Lesions of the Talus; Clinical Outcomes; Ankle
Introduction/Purpose: Autologous osteochondral transplantation (AOT) is a replacement strategy used to treat osteochondral lesions of the talus (OLT), typically reserved for the treatment of lesions of larger sizes, highly cystic lesions, or in patients who have failed previous treatment. The purpose of this study was to evaluate the long-term (>8 years) clinical and radiographic outcomes of AOT for the treatment of OLT in the form of a retrospective case series.
Methods: Patients who underwent AOT between 2006 and 2008 were evaluated. Functional outcomes were assessed pre- and post-operatively using the Foot and Ankle Outcome Score (FAOS), and Short-Form-12 (SF-12) general health questionnaire. The most recent post-operative MRI was evaluated with the modified Magnetic resonance Observation of Cartilage Repair Tissue (MOCART) score.
Results: Twenty-eight patients who underwent AOT were included and evaluated at a mean follow-up of 122.9 months. The mean FAOS pain subscale improved from 52.7 to 82.9 and the mean SF-12 improved from 30.3 to 58.3 at final follow-up (both, p < 0.01). The mean FAOS pain subscale then decreased to 77.6 at final follow-up, but this decrease was not statistically significant (p=0.293). At the final follow-up, the mean FAOS subscale scores of symptoms, pain, daily activities, sports activities, and quality of life were 66.6, 77.6, 86.0, 60.4, and 53.6, respectively. The mean VAS score was 2.2 at a final follow-up. The mean MOCART score was 83.8 with a mean MRI follow-up of 82.8 months. Ten patients (35.7%) had additional surgery, with the most common procedure being arthroscopic anterior ankle debridement. One patient failed AOT and developed osteoarthritis of the ankle requiring a total ankle replacement.
Conclusion: AOT appears to be an effective treatment for OLT with good long-term clinical and radiographic outcomes. Secondary procedures were typically minor and the overall clinical failure rate was low.
DOI: 10.1177/2473011421S00206
Outcomes Following Arthroscopy for Anterior Impingement in the Ankle Joint in the General and Athletic Populations: Does Gender Play a Role?
Arianna L. Gianakos, DO; Axel Ivander; Christopher W. DiGiovanni, MD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle; Arthroscopy; Sports
Keywords: Arthroscopy; Athlete; Clinical Outcomes
Introduction/Purpose: To provide an overview of the clinical outcomes of arthroscopic procedures used as a treatment strategy for anterior ankle impingement and to determine if gender affects outcomes.
Methods: A systematic literature search of the Medline, Embase, and Cochrane databases was performed during June of 2019. The combination of search terms utilized included the following: ‘ankle’, ‘impingement’, ‘talus’, ‘osteophyte’, ‘arthroscopy’, ‘surgery’, ‘procedures’, and ‘treatment’. Two reviewers independently performed data extraction consisting of demographic data, intraoperative arthroscopic data, functional outcome scores, patient satisfaction, complications, return to play, and gender differences.
Results: Twenty-eight articles evaluating a total of 1,506 patients were included in this systematic review. Sixty percent (17 of 28) and 14% (4 of 28) of studies assessed anterolateral and anteromedial impingement, respectively. Overall, good to excellent results were reported following arthroscopic treatment in patients with anterior ankle impingement with an average success rate of 81.04%. Eleven studies reported return to sport with an average return to sport of 8 weeks. The most common concomitant pathology found during arthroscopic evaluation included synovitis, osteophytes, meniscoid lesions, and AITFL injury. Four studies (15%) failed to report gender as a demographic variable. Only 7 (25%) studies reported gender analysis with four (57%) studies demonstrating differences when comparing gender outcomes. Female patients have higher rates of traumatic ankle sprains, chondral injury, and chronic ankle instability associated with anterior ankle impingement when compared with male patients.
Conclusion: Our systematic review demonstrates that arthroscopic treatment for anterior ankle impingement provides good to excellent functional outcomes, and good return to sports rates in the athletic population. This study underscores that lack of statistical analysis evaluating outcomes comparing male and female populations. Our study does demonstrate that female patients have higher rates of traumatic ankle sprains, chondral injury, and chronic ankle instability associated with anterior ankle impingement when compared with male patients. Therefore, women may benefit from both AMI/ALI resection as well as lateral ankle ligament repair or reconstruction in order to address both impingement and chronic lateral ankle instability.
DOI: 10.1177/2473011421S00207
Standardization of the Foot Sagittal Axis for Measurement of Hindfoot Alignment Using Weight- Bearing Computed Tomography (WBCT)
Alexandre L. Godoy-Santos, MD; Eduardo A. Pires; Carlos Lobo; Cesar de Cesar Netto, MD, PhD; Fabio C. Fonseca, MD; Rafael B. Sposeto, MD
Introduction/Purpose: The radiographic measurement of hindfoot alignment (HA) suggested by Saltzman, worldwide accepted, uses the medial aspect of the foot as the sagittal axis. When defining the medial face of the foot as its axis, the adduction and abduction deformities of the forefoot are disregarded, making it necessary to rotate the ankle internally or externally to acquire the radiographic image according to Saltzman protocol. The emergence of weight-bearing computed tomography (WBCT) allowed immeasurable advancements for a better understanding of the joints relations of the foot and ankle under stress. Previous studies using this technology adopted several sagittal axes to measure HA. Our hypothesis is that the adduction observed in the forefoot of the cavovarus feet illusively accentuates the real deformity of the hindfoot.
Methods: Two evaluators calculated the HA of twenty-eight feet - 14 cavovarus and 14 neutral or slightly valgus (control group) - in three different sagittal axes (second metatarsal axis, calcaneus - second metatarsal axis and talar dome axis). Measurements were compared by Student’s t-test after normality test by Shapiro-Wilk method. Observers’ agreement was evaluated by intraclass correlation coefficient (ICC). P-values <.05 were considered significant.
Results: We found excellent intra-observer (0.93) and inter-observer (0.9) agreements following the measuring assessment. The average Foot and Ankle Offset (FAO) of the cavovarus feet group was -3.35 (-0.64 - -7.01), while the control group was 2.01 (-1.3 - 6.4). The mean difference in HA when comparing the axis of the talar dome with the axis of the second metatarsal was 9.88 ° (3.1 ° - 17 °), while in the control group the mean difference was 3.16 (0.2 ° - 7.5 °). All of these data showed statistical significance.
Conclusion: As a great variability was observed in the measurements of hindfoot alignment in the cavovarus foot group in the sagittal axes analyzed, this article suggests standardizing the measurement of hindfoot alignment using the talar dome axis. In addition, it becomes possible to quantify adaptations of the hindfoot secondary to modifications of the forefoot in an isolated manner.
DOI: 10.1177/2473011421S00208
Epidemiology of Ankle Sprain in the Military: A Systematic Review of Literature
Ezra Goodrich; Brandon L. Morris, MD; Christina Hermanns; Ashley A. Herda; Armin Tarakemeh, BA; Bryan G. Vopat, MD
Category: Ankle; Sports
Keywords: Ankle Sprain; Ankle Instability; Sports
Introduction/Purpose: Ankle sprains occur frequently within the general population, however, the extent to which this injury impacts the military population remains unknown. The purpose of this study was to systematically review the literature describing ankle sprains in the military population.
Methods: Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, articles were retrieved from PubMed, Embase, and Cochrane Library using the search terms ‘military,’ ‘epidemiology,’ ‘incidence,’ ‘prevalence,’ ‘ankle sprain,’ and ‘ankle instability.’ Inclusion criteria consisted of active military duty status, English language, and levels of evidence I-IV.
Results: Nineteen articles were included, representing 1,671,763 study participants from six countries and four branches of the military. Among the ten studies that reported ankle sprain incidence in terms of overall injury incidence, seven studies reported ankle sprain as the most common injury, with an incidence ranging from 2.20% to nearly one third of all injuries in the paratrooper population. Ankle sprain was also reported as the most common injury among lower extremity injuries in two studies, with incidences of 35% and 38.7%, respectively. Ankle sprain incidence rate per 1,000 person-years was reported in four studies, with values ranging from 15.3 to 58.4. Incidence rate was also reported for males and females separately in three of these studies, ranging from 33.89 to 52.7 for males, and 41.17 to 96.4 for females. The number of days lost to ankle sprain ranged from one to eight days per servicemember.
Conclusion: Ankle sprains are among the most prevalent injuries within the military population, with a reported incidence that is higher for females than males. This injury results in time away from active duty, which impacts overall readiness within the military system.
DOI: 10.1177/2473011421S00209
Sex-Specific Differences Following Lateral Ankle Ligament Repair
Ezra Goodrich; Matthew Vopat, MD; Jordan Baker; Armin Tarakemeh, BA; Kim Templeton; Mary K. Mulcahey, MD; Paul Schroeppel, MD; Scott Mullen, MD; Bryan G. Vopat, MD
Introduction/Purpose: Chronic ankle instability is a common condition that can be treated with lateral ankle ligament repair. These procedures have a reported success rate greater than 85% in the literature, but little has been reported about the differences in postoperative outcomes between males and females. The purpose of this study was to evaluate sex-specific outcomes following lateral ankle ligament repair.
Methods: In this systematic review and meta-analysis, we utilized Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) criteria to search for articles on electronic databases. Inclusion criteria consisted of English-language, in-vivo clinical studies, mean follow-up of at least one year, sex-specific evaluation of outcomes, and study participants who underwent primary lateral ligament repair. Functional postoperative outcomes for males and females were recorded and statistically analyzed.
Results: Out of 2,768 studies, eight (0.29%) met inclusion criteria and were analyzed in this review. These studies included 631 patients (409 males [65%] and 222 females [35%]) who underwent primary lateral ligament repair for ankle instability. There was no statistically significant difference between males and females in terms of Karlsson scores (93.5 +- 1.6 for males, 92.7+- 2.3 for females, P =.1582) or American Orthopaedic Foot & Ankle Society (AOFAS) scores (90.44 +- 4.82 for males, 90.19 +- 3.54 for females, P =.1586). Postoperative success was defined as a ‘good’ or ‘excellent’ Karlsson score (>81), and success rate analysis revealed no statistically significant difference between males and females (86% +- 7.1% for males, 87% +- 3.5% for females, P =.9374).
Conclusion: There was no difference in postoperative mean Karlsson scores, AOFAS scores, or success rates between males and females who underwent primary lateral ankle ligament repair. This surgical procedure appears to have comparable outcomes in both sexes; however, more research is warranted to further assess the impact of patient sex on postoperative outcomes.
DOI: 10.1177/2473011421S00210
Treatment of Chronic Ankle Instability in the Military Population
Introduction/Purpose: The high incidence of ankle sprain within the military sets the stage for prevalent chronic ankle instability. The purpose of this review was to compare and evaluate chronic ankle instability treatment strategies in the military population.
Methods: Electronic databases were systematically searched for English-language, human studies with a military patient population that had been diagnosed with and treated for chronic ankle instability. Exclusion criteria were animal, cadaver, and review studies and case reports.
Results: Eight studies met inclusion criteria and represented 695 military service members-625 males (89.9%) and 70 females (10.1%). The four treatment strategies included were Broström-related procedures, modified Watson-Jones procedure, Colville’s technique, and anatomic lateral ligament reconstruction using semitendinosus tendon allograft. The percentage of subjective satisfactory outcomes ranged from 80 to 94.7%, and the percentage of objective satisfactory outcomes ranged from 72 to 100%. The range for Broström-related procedures was 73.2% (objective) to 94.7% (subjective). The modified Watson-Jones procedure had a subjective satisfactory outcome of 80% and objective satisfactory outcome of 72%. Colville’s technique had an objective satisfactory outcome of 100%. No satisfaction outcome was available for the study utilizing the anatomic lateral ligament reconstruction with semitendinosus tendon allograft. Mean American Orthopaedic Foot & Ankle Society (AOFAS) scores, anterior drawer displacement, talar tilt, and visual analogue scale (VAS) scores were also reported.
Conclusion: This review demonstrates that the Bröstrom procedure has consistently satisfactory outcomes within the military population, and Colville’s technique is another promising option for this patient population, but would require future studies to fully support this claim.
DOI: 10.1177/2473011421S00211
Analysis of Change in Patient Reported Outcome Measures Following Minimally Invasive Chevron Akin Osteotomies (MICA) in Hallux Valgus Surgery
David Gordon, MD, MB BCh, FRCS(Orth), MRCSEd; Thomas L. Lewis, MB ChB; Robbie Ray
Introduction/Purpose: There is a need to understand the rate of improvement following minimally invasive chevron akin osteotomies (MICA) for correction of hallux valgus deformity using validated patient reported outcome measures (PROMs) and whether this change is clinically meaningful in order to help counsel patients as to their progress.
Methods: Between July 2014 and November 2018, data was prospectively collected from consecutive patients pre-operatively and at 6, 12, and 24 months following MICA. The primary outcome measure was the change in Manchester Oxford Foot and Ankle Questionnaire (MOXFQ) score at each timepoint following MICA. Secondary outcomes include radiographic deformity correction, and exploration of cases where PROMs did not improve following MICA.
Results: 190 feet with complete PROM data at each time point, were identified from a cohort of 334 feet undergoing third generation MICA. There was a statistically significant improvement in MOXFQ score for each MOXFQ domain at each time point following MICA although the majority of the improvement was within the first 6 months. 17 feet had worse MOXFQ Index scores at the six month timepoint compared to pre-operatively. Of these feet, 82.4% (n=14) improved over time such that by two years their score had improved compared to their pre-operative score.
Conclusion: There is a statistically significant improvement in MOXFQ score at every time point following MICA for hallux valgus. The majority of patients who scores are worse at 6 months following will go on to have improved function compared to their pre-operative state.
DOI: 10.1177/2473011421S00212
Bilateral vs Unilateral Minimally Invasive Hallux Valgus Surgery: A Propensity Matched Case-Control Study with 2 Year Clinical Patient Reported Outcomes
David Gordon, MD, MB BCh, FRCS(Orth), MRCSEd; Sophie A. Crooks; Thomas L. Lewis, MB ChB; Robbie Ray
Introduction/Purpose: Hallux valgus deformity correction using a third-generation Minimally Invasive Chevron Akin osteotomy technique (MICA) is becoming increasingly popular. There is limited patient reported outcome measure (PROM) outcomes for patients undergoing bilateral hallux valgus corrective MICA surgery during a single operative case.
Methods: Between July 2014 and May 2018, 59 consecutive patients comprising 118 feet underwent bilateral MICA in a single operative case. 1:1 propensity score matching based on preoperative PROM assessment, age, and radiographic deformity data was carried out to match each foot in the bilateral cohort with 118 feet who had undergone unilateral MICA. The primary outcome measure was the Manchester-Oxford Foot Questionnaire (MOXFQ) which was prospectively measured pre-operatively, six months and two years post-operatively. Secondary outcomes included complication rates and radiographic deformity correction with regards to the hallux valgus angle (HVA) and inter-metatarsal angle (IMA).
Results: At minimum 2 year follow up, the MOXFQ post-operative scores had significantly improved for every domain (p <0.001) in both unilateral and bilateral cohorts compared to pre-operative assessment. For all domains of the MOXFQ, there was no statistically significant difference in 6 month or two year outcomes between patients undergoing bilateral and unilateral MICA surgery (p >0.05 for all outcome measures). There was no statistically significant difference between the two cohorts in complication rate (p=>0.05) or post-operative IMA or HVA (p >0.05).
Conclusion: This study demonstrates that there is no significant difference in patient reported outcome measured at two year follow-up between patients who underwent bilateral versus unilateral MICA. This study should reassure surgeons who perform bilateral hallux valgus surgery in a single case that, in the medium-term, there is no difference in clinical or radiographic PROMs compared to unilateral surgery. There are potentially positive health economic benefits of performing bilateral surgery in a single sitting if clinically indicated.
DOI: 10.1177/2473011421S00213
The Impact of Hallux Valgus on Function and Quality of Life in Females
David Gordon, MD, MB BCh, FRCS(Orth), MRCSEd; Thomas L. Lewis, MB ChB; Robbie Ray
Introduction/Purpose: The effect of hallux valgus (HV) on health-related quality of life (HRQOL) and the relationship between radiographic severity of deformity and patient reported outcome measures (PROMs) is poorly understood. The aim of this study was to compare the HRQOL of female patients with HV to the UK population. The secondary aim was to assess the correlation between PROMs, including HRQOL, with radiographic severity of deformity.
Methods: Weight bearing radiographic data (hallux valgus (HVA) angle; intermetatarsal (IM) angle) were measured in consecutive female patients presenting with symptomatic HV. Each patient prospectively completed the Euroqol EQ-5D-5L questionnaire (EQ- 5D), Visual Analogue Scale for Pain (VAS-Pain) and Manchester Oxford Foot Questionnaire (MOXFQ). Data were stratified into age ranges and compared with an EQ-5D United Kingdom general population reference dataset. Pearson R correlation values were calculated for the PROMs and radiographic deformity.
Results: Between July 2015 and March 2020, 425 consecutive female patients presented with symptomatic HV for consideration for surgery. EQ-5D-5L data were prospectively collected for 396 of these patients (93.2%). EQ-5D-5L Index scores were significantly worse for females with HV when compared with females in the general population. There was a moderate correlation with MOXFQ Index score and EQ-5D-5L Index (R=-0.51, p<0.001) and VAS-Pain scores (R=0.54, p<0.001). There was no correlation between radiographic HV deformity and HRQOL measures or MOXFQ scores.
Conclusion: Female patients presenting with HV deformity have a significantly reduced quality of life compared with the UK general population. The radiographic severity of deformity did not correlate with health-related quality of life measures or foot and ankle specific PROMs. Foot and ankle specific clinical PROMs do correlate with HRQOL and may be a better marker of the negative effect of symptomatic hallux valgus deformity on quality of life.
DOI: 10.1177/2473011421S00214
Two Year Patient Reported Outcomes of 334 Minimally Invasive Chevron Akin Osteotomies (MICA) in Hallux Valgus Surgery
David Gordon, MD, MB BCh, FRCS(Orth), MRCSEd; Thomas L. Lewis, MB ChB; Robbie Ray
Introduction/Purpose: There are many different procedures described for the correction of hallux valgus deformity. Minimally invasive surgery has become increasingly popular, with clinical and radiological outcomes comparable to traditional open osteotomy approaches. There is increasing interest in hallux valgus deformity correction using third-generation minimally invasive chevron akin osteotomy (MICA) technique. Objective: To assess the radiographic correction and 2-year clinical outcomes of third-generation MICA using validated outcome measures.
Methods: This is a prospective single-surgeon case series of 420 consecutive feet undergoing MICA surgery between July 2014 and Jan 2019. Primary clinical outcome measures included the Manchester-Oxford Foot Questionnaire (MOXFQ), EQ-5D, and the Visual Analogue Pain Scale. Secondary outcome measures included radiographic parameters, and complication rates.
Results: Pre-operative and 2 year post-operative patient reported outcomes were collected for 334 feet (79.5%). At minimum 2 year follow-up, the MOXFQ scores (mean +- standard deviation (SD)) had improved for each domain: pain; pre-operative 43.9+- 21.0 reduced to 9.1+-15.6 post-operatively (p<0.001), walking and standing; pre-operative 38.2+-23.6 reduced to 6.5+-14.5 post- operatively (p<0.001) and social interaction; pre-operative 47.6+-22.1, reduced to 6.5+-13.5 post-operatively (p<0.001). At 2 year follow-up, the VAS Pain score (mean +- SD) improved from a pre-operative of 31.3+-22.4 to 8.3+-16.2 post-operatively (p<0.001). 1-2 intermetatarsal angle (mean +- SD) reduced from 15.4°+-3.5° to 5.8°+-3.1° (p<0.001) and hallux valgus angle reduced from 33.1°+-10.2° to 9.0°+-5.0° post-operatively (p<0.001).
Conclusion: Third-generation MICA showed significant improvement in clinical outcomes at 2 year follow-up and can be successfully used for correction of a wide range of hallux valgus deformities.
DOI: 10.1177/2473011421S00215
Effect of Long and Short Term HgbA1c on Surgical Treatment Outcomes of Diabetic Patients with Emergent Foot and Ankle Surgery
Sunny Gotewal; Vinod K. Panchbhavi, MD, FACS; Daniel Jupiter, PhD
Category: Ankle; Diabetes; Midfoot/Forefoot
Keywords: Diabetic Foot; Complications; Surgical Site Infection
Introduction/Purpose: Elevated HgbA1c are associated with higher postoperative complications. It is not as well understood whether the HgbA1c levels measured at the time of surgery, or those measured in the months prior to surgery, are more strongly associated with complications. We carried out a study of our EMR examining whether historic HgbA1c and burden of diabetes, are more or less impactful than more proximately measured HgbA1c.
Methods: We identified patients using CPT codes for ankle, tibia, fibula, and femur fracture repair. Similarly, post-operative complications (infection, dehiscence, DVT, PE and SSI) were retrieved using ICD 9 and 10 codes. Variables recorded were comorbidities and complications, age, sex, race, ethnicity, marital status, and HgbA1c. HgbA1c was noted within a month before and a month after repair, and within 18 months and 6 months before repair. For each complication, the association with every other variable was assessed using t-test or chi-squared/Fisher’s exact tests, for continuous and categorical variables, respectively.
Results: 20 patients had the data needed to carry out the analysis. While t-test revealed no significant differences between those with and without complications, either in terms of long or short term HgbA1c, the differences between HgbA1c at a year prior to surgery appear to be larger.
Conclusion: Given that differences between historic HgbA1c in those with and without complications appear to be larger than the differences in more recent HgbA1c using our small sample size, we would like to explore whether these relationships are significant, using larger data sets.
DOI: 10.1177/2473011421S00216
Lower Extremity Injury Rates on Artificial Turf and Natural Grass Playing Surfaces: A Systematic Review
Heath P. Gould; Stephen J. Lostetter; Eric R. Samuelson; Gregory P. Guyton, MD
Category: Sports
Keywords: Athlete; Sports; National Football League
Introduction/Purpose: Artificial turf (AT) playing surfaces have emerged as a common alternative to natural grass (NG) at all levels of athletic competition from youth to professional. While several prior articles have compared the lower extremity injury rates on AT and NG, the heterogeneity of these studies in terms of design and methodology has led to widely variable results. The purpose of this systematic review was to determine whether any definitive conclusions can be drawn with regard to the risk of lower extremity injury on AT and NG playing surfaces.
Methods: A systematic review of the English-language literature was performed according to the PRISMA guidelines. All included studies presented a direct comparison of injury rates on AT versus NG playing surfaces. No restrictions were made with regard to sport, level of competition, level of evidence, or year of publication. Studies that examined only head injury rates (e.g. concussions) without any comparison of overall injury rates or lower extremity injury rates were excluded. Systematic reviews and meta-analyses were also excluded. The following data elements were extracted from each article: publication year, study design, level of evidence, industry funding, cohort selection process (ad-hoc vs. systematic), sport, level of competition, number of athletic seasons, injury setting, AT type, overall injury rate, knee rate, and foot & ankle injury rate. AT types were classified into Old Generation (1st or 2nd generation) or New Generation (3rd generation or higher).
Results: 53 articles met inclusion criteria. 31 articles compared overall injury rates on AT versus NG. Roughly one-half of these studies (51.6%) found no significant difference between NG and AT, while roughly one-third (35.5%) found a higher overall injury rate on AT and just 4 studies (12.9%) found a higher overall injury rate on NG. Similarly, of the 26 articles comparing knee injury rates, 14 studies (53.8%) reported no difference between AT and NG, 8 studies (30.8%) reported a higher injury rate on AT, and 4 studies (15.4%) reported a higher injury rate on NG. With regard to foot & ankle injuries, however, a majority of articles (14/24, 58.3%) reported a higher injury rate on AT. Comparatively few articles (3/24, 12.5%) reported a higher foot & ankle injury rate on NG, while the remaining articles (7/24, 29.2%) reported no difference in foot & ankle injury rate between AT and NG.
Conclusion: The present study is a systematic review of 53 articles in the English-language literature that compared injury rates on AT and NG. Our findings suggest that the rates of overall injury and knee injury are similar between these two playing surfaces, though AT may be associated with a higher rate of foot & ankle injuries compared to NG.
DOI: 10.1177/2473011421S00217
The Top 100 Most Impactful Articles on the Achilles Tendon: An Altmetric Analysis of Online Media
Heath P. Gould; Joseph M. Bano; William Rate; Matthew Civilette; Andrew S. Cohen; Eric R. Samuelson; Brett Haislup; Blake M. Bodendorfer
Introduction/Purpose: Achilles tendon injuries affect a wide range of individuals, including both recreational and competitive athletes. In the elite athlete population, Achilles tendon ruptures are typically season-ending injuries and can be career-threatening. Due to these impacts on individual players’ careers as well as team success, Achilles tendon injuries often generate substantial discussion in the mainstream media and among the general public. However, traditional citation-based metrics fail to capture the dissemination of Achilles research that occurs outside the realm of scientific journal publications. Thus, the purpose of this study was to use the Altmetric Attention Score (AAS) to identify the 100 most impactful articles in online media pertaining to the Achilles tendon and assess their characteristics.
Methods: The Altmetric database (Digital Science, Holtzbrinck Publishing) was queried to identify all published articles pertaining to the Achilles Tendon. The articles were stratified by highest to lowest AAS and the top 100 articles with the highest scores were included for analysis. Several data elements were extracted for each article: title, article type, article topic, year of publication, journal name, authors, institutional affiliations, and online mentions (i.e., the number of times the article was mentioned in news, blog, Twitter, Facebook and Wikipedia sources). The geographic origin of each article was also determined by the institutional affiliation of the first author, which was categorized as American (originating in the United States), European (originating in Europe), or Other. Linear regression was used to determine the relationship between online mentions and AAS.
Results: The initial search yielded 3,810 articles published between 1957 and 2021. AAS of the top 100 articles ranged from 37 to 476 with a median of 65 (interquartile range: 42-110). The selected articles were published in 39 journals. The most prevalent article type was randomized controlled trial (21.8%), followed by systematic review / meta-analysis (13.9%). The most prevalent article topics were treatment (39.6%), rehabilitation and return to play (11.9%), epidemiology (11.9%), and biomechanics (11.9%). Of the top 100 articles, 25.0% were American, 45.0% were European, and 30.0% were published outside of the United States or Europe. AAS had a strong correlation to Twitter mentions (r = 0.81), a moderate correlation to Google Scholar mentions (r = 0.52), and a weak correlation to Facebook mentions (r = 0.49).
Conclusion: This study used AAS to characterize the 100 most impactful Achilles articles in online media. As access to research continues to move away from the conventional printed format, it is critically important to understand how orthopaedic information is disseminated online. Our findings suggest that alternative metrics broaden the definition of article impact beyond what is provided by traditional citation-based metrics and should be considered as a supplemental means of assessing the overall impact of published scientific literature.
DOI: 10.1177/2473011421S00218
Transglutaminase Modification of Tendon Collagen
Christopher E. Gross, MD; James C. Rex; Daniel J. Scott, MD, MBA; Amy Bradshaw, PhD
Introduction/Purpose: Achilles tendinopathy is one of the most common overuse conditions encountered in foot and ankle surgery. Various etiological risk factors for this disease have been explored: age, body-mass index, and patient specific biomechanics. However, the pathogenesis remains poorly understood. Healthy tendon is composed primarily of type III and I collagen, which undergo post-translationally modification by lysyl oxidase and transglutaminase (TG) enzymes. The expression and activity in the latter of these two is poorly characterized in Achilles tendon. This study aims to describe the function of a specific transglutaminase, TG2, within solubilized collagen and Achilles tenocyte cultures, and to demonstrate evidence of TG2 activity within pathologic human Achilles tendon tissue.
Methods: Acellular Collagen: Type I collagen gels were aliquoted into a silicone well plate. Gels were then seeded with either 2.4 ng of TG2 or a control. Two sets of gels were prepared; one undergoing a 10% stretch at 2Hz for 24 hours and the other a static control. TG2 substrates were labelled, and the relative quantity of higher molecular weight collagens produced by TG2 activity was compared. Tenocytes: Human tenocytes were grown in 3D cultures as well as traditional cultures in a conditioned fibroblast growth media. Proteins expressed by tenocytes in both cultures were extracted and examined for TG modification. Pathologic Tendon: After receiving Institutional Review Board approval, tissue was collected from patients undergoing debridement of Achilles tendinopathy. Collagen was extracted in 0.1M acetic acid and Western blot analysis was used to identify TG2 crosslink epitopes.
Results: In each of three experimental paradigms: acellular, cellular, and human tendon extracts, evidence for transglutaminase modification of collagen I was noted. Dynamic conditions increased TG2 modification of collagen in acellular cultures, as evidenced by higher molecular weight collagen forms. Western blot analysis of protein expression demonstrated that tenocytes cultured in 3-D produced higher levels of TG-modified proteins than those in 2-D. Similarly, western blot analysis demonstrated presence of TG2 modification epitopes in the harvested human Achilles tendon tissue. However, the enzyme itself did not appear to be strongly expressed and could not be detected from the samples.
Conclusion: Transglutaminase 2 expression by tenocytes in 3D culture and evidence for transglutaminase-dependent modification of collagen I by TG2 under dynamic loading supports a key role for transglutaminase in tendon biology and in repair. Though evidence of TG2 modification was found in diseased human samples, the absence of detectable TG2 expression suggests that it may play a significant role in the healthy physiologic turnover of Achilles tendon collagen.
DOI: 10.1177/2473011421S00219
Calcitonin Gene-Related Peptide in Charcot Foot Neuroarthropathy
Yi Guo; Lew C. Schon, MD; Sharada Paudel, PhD; Tyler Feltham; Lumanti Manandhar; Zijun Zhang
Introduction/Purpose: Charcot neuroarthropathy (CNA) is a destructive joint condition secondary to neuropathic deficiency. For more than a century, the pathogenesis of CNA has been interpreted as unprotected injury and/or uncontrollable inflammation in a neuropathic joint, with little understanding its cellular and molecular pathology. Histologically, a hallmark of CNA is bone and cartilage fragments engulfed by hyperplastic synovium. Synovium is richly innervated. Neuropeptides, such as calcitonin gene- related peptide (CGRP), are secreted by neuronal and non-neuronal cells of the nervous, endocrine, and immune systems, and regulate inflammation. This study investigated the expression of CGRP in the synovial samples collected from CNA and non-CNA joint conditions, and the effects of CGRP on the proliferation and collagenolysis of fibroblast-like synoviocytes (FLS) isolated from CNA synovium in vitro.
Methods: For this study, six CNA and 14 non-CNA synovial samples were collected during foot and ankle surgery. The donors included 10 male and 10 female, age from 14 to 79 years (mean 48). The non-CNA conditions consisted of osteoarthritis, ankle instability, Os Trigonum and osteochondritis dissecans.
Western blot and immunohistochemistry of CGRP were performed to detect and localize CGRP expression in the CNA and non- CNA synovium.
FLS was isolated from CNA synovium and cultured with, or without, human CGRP (10nM) in the culture media, for comparison of cell proliferation. Additionally, FLS were seeded on the collagen-coated 24-well plate and simulated with CGRP (10nM) and recombinant human tumor necrosis factor-alpha (TNF-α). After 7 days, the residual collagen on the bottom of the culture plate were stained and imaged for area measurements.
Data were analyzed with t test or one-way Analysis of Variance, followed with post hoc Tukey’s test.
Results: By western blot, there was significant CGRP expression in the CNA synovium (5/6; Fig1). Except of an intense CGRP band in one of the osteoarthritis samples, only recognizable CGRP bands were shown in the samples of other non-CNA conditions. The average density of CGRP (in greyscale) in the CNA group was about 2-fold of that in the non-CNA group (10126 +- 5346 vs. 5377+-3734; p < 0.05). Immunohistochemistry demonstrated intense CGRP staining in the intimal layer of the CNA synovium (arrows) but not in the non-CNA synovium (Fig1). Treated with CGRP, the number of FLS in tissue culture increased. Cell number doubling time was 1.0 day (+-0.4) for the CGRP treated FLS and 2.2 days (+-0.5) for the control (p < 0.05). When the culture media were supplemented with CGRP and TNF-α, FLS eroded a larger area of collagen coating comparing with TNF-α alone in the media (p < 0.05).
Conclusion: A knowledge gap in understanding the molecular and cellular pathology of CNA hampers the development of disease-modifying therapies. This study showed an increased CGRP, with a concentration in the intimal layer, in the CNA synovium as compared with the synovium in the non-CNA foot conditions. The increased CGRP expression in CNA synovium may be part of the unbalanced neuropeptide signaling in the neuropathic pathology. Functionally, CGRP stimulated FLS proliferation and degrading collagen in vitro. These effects suggest that CGRP may play a role in bone and joint destruction in the Charcot foot.
DOI: 10.1177/2473011421S00220
Conditioned Medium of Mesenchymal Stem Cells Prevents Degenerative Changes in Ankle Osteoarthritis in Rat Models
Daniel Guss, MD, MBA; Omid Koohi-Hosseinabadi; Moein Zarei; Bart Lubberts, MD, PhD; Christopher W. DiGiovanni, MD; Nader Tanideh
Introduction/Purpose: Osteoarthritis (OA) is the most common degenerative joint disorder, characterized mainly by progressive articular cartilage degradation, subchondral bone thickening, osteophyte formation, and synovial inflammation. About 80% of ankle OA is believed to be post-traumatic and affects the younger population leading to a higher risk of disabilities during life. Mesenchymal stem cells (MSCs) have shown promising effects in preventing the degenerative process of OA via paracrine effect and great differentiation potential. Recently, using chondrocyte conditioned medium (CCM) that contains all necessary secretomes was shown to enhance MSC differentiation and regeneration of the cartilage tissue. In this study, we aimed to assess the effects of intraarticular injection of MSCs plus CCM on the degenerative process of monoiodoacetate (MIA)-induced ankle OA in rats.
Methods: Fifty male rats were randomly divided into 5 groups (n=10): Non-treated control group (C); the group treated with intra-articular Hyaluronic acid (HA). Hyaluronic acid has shown beneficial effects on the degenerative process of OA in different reports. The other treatment groups received intraarticular synovial derived MSCs (5′105), intraarticular CCM, and intraarticular MSCs combined with CCM (MSC+CCM), respectively. Induction of ankle OA was conducted via 1 mg MIA injection in the right tibiotarsal joint for two consecutive days. Three months after starting the treatments, radiological assessments of joint space width (Normal=0, reduced=1, abcent=2) and osteophytes of the tibia and talus (No osteophyte=0, small=1, moderate=2, severe=3) were performed. Ankle specimens were obtained for histopathological examination of the joint surface, matrix, cell distribution, cell viability, subchondral bone, and mineralization; lower scores indicated more severe damages. Scores for each assessment were recorded. Mann-Whitney U test was used for comparisons and p-value<0.05 was considered statistically significant.
Results: Our findings showed significant differences between the controls and the treatment groups regarding all pathological scores including joint surface, matrix, cell distribution, cell viability, subchondral bone, and mineralization, that were higher and radiological scores including joint space width and osteophytes of the tibia and talus that were lower in the controls (P<0.05; Figure 1). Among the treatment groups, HA-treated rats showed significantly lower pathological and higher radiological scores compared to CCM, MSC, and MSC+CCM (P<0.05). Among CCM, MSC, and MSC+CCM treated groups, no significant difference was found regarding the pathological and radiological scores (P>0.05). However, although not statistically noticeable, the MSC+CCM group showed slightly better outcomes, both radiologically and histopathologically, compared to the MSC and CCM groups (Figure 1).
Conclusion: Our results showed that the combination of CCM can have a similar effect on the degenerative changes in ankle OA. However, the combination of MSC+CCM showed better scores regarding pathological and radiological evaluation. Although further studies with a greater population seem to be needed to validate these outcomes, our study indicates the efficacy of CCM in reducing the degenerative rate of OA. CCM is also known as ’secret factors’ since it is still a ‘black box’ in terms of identifying its content and effects.
DOI: 10.1177/2473011421S00221
Deep Learning Improves the Accuracy of Weightbearing CT Scan in Detecting Subtle Syndesmotic Instability
Daniel Guss, MD, MBA; Reza Mojahed-Yazdi; Soheil Ashkani-Esfahani, MD; Rohan Bhimani, MD, MBA; Gregory R. Waryasz, MD; Gino Kerkhoffs, MD; Bart Lubberts, MD, PhD; Christopher W. DiGiovanni, MD
Introduction/Purpose: Weightbearing CT (WBCT) scan provides an ability to compare the ankle joints bilaterally in a 3D manner under physiologic load. According to our recent investigations, 3D volume measurement of the syndesmosis, if measured up to 5cm proximal to the tibial plafond, can detect the instability with an accuracy of 90%, sensitivity of 95.8%, and specificity of 83.3%. However, these values can differ based on the knowledge and experience of the human interpreter. Deep learning, as a subset of machine learning, has shown promising potentials in processing and analyzing images and detecting abnormalities within the images using deep convolutional neural networks (DCNN). Herein, we aimed to assess the accuracy, sensitivity, and specificity of 3D volume WBCT evaluation using DCNN algorithms in patients with subtle syndesmotic instability.
Methods: In this study 140 bilateral ankle WBCT scans of patients with subtle syndesmotic instability who were diagnosed intraoperatively were allocated to the patient group. The control group comprised 140 bilateral ankle WBCT images of healthy individuals. We utilized inception V3 model for our DCNN. Data augmentation and transfer learning were used; however, the images were not preprocessed in terms of change in size and resolution. The data were divided as 80:10:10 for training, validation, and test subsets, respectively. The outcome of the study was expressed as sensitivity, specificity, F-score, and the area under the curve (AUC).
Results: The performance of our DCNN algorithm showed a sensitivity of 99.41%, specificity of 99.34%, F-score of 99.37%, and 99.99% AUC (Figure 1). The change in loss value of the train data was plateaued after 40 iterations. Axial images were the most appropriate images that were used by the algorithm to detect the instability.
Conclusion: In this study we observed that using DCNN in the process of WBCT image interpretation for diagnosis of syndesmotic instability, particularly in subtle cases, makes this modality almost perfect with a very small chance of missing a case. Training a DCNN using a greater number of inputs is still recommended to improve the validity and reliability of this method. Providing a heat map will also help clinicians discover the process of decision-making by these algorithms as DCNNs are sometimes called 'black box'.
DOI: 10.1177/2473011421S00222
Effect of Pathology on Patient Reported Outcomes of MTP Arthrodesis
Jared R. Halstrom, BS; Nicholas A. Andrews; Sterling Tran; Jessyca Ray; Whitt Harrelson; James Pate, BS; Austin Hughes; Roshan Jacob; Ashish Shah, MD
Introduction/Purpose: Metatarsophalangeal (MTP) joint arthrodesis of the hallux is a common and reliable procedure performed on patients with various pathologies including hallux rigidus and hallux valgus. While the effect of foot pathology on MTP arthrodesis union rates has been previously explored, there is a lack of literature comparing long term patient reported outcomes between pathology types. The purpose of this present study was to compare patient reported and clinical outcomes following MTP fusion between those with hallux valgus and hallux rigidus.
Methods: Patients undergoing primary MTP arthrodesis from 2010-2020 were identified. Additionally, Radiographic follow-up of >12 weeks, no ongoing ipsilateral infection, and complete response to a postoperative patient report outcomes (PROMIS AND Foot Function Index (FFI)) survey were required. After these criteria, 112 patients remained and were grouped by hallux valgus (HV, 53) and hallux rigidus (HR, 59). Medical records were examined for patient characteristics, operative variables, and complications. Patients were grouped by indication and compared.
Results: Nonunion rates and complications including wound dehiscence, infection, and reoperation were not different between indications. Patients completed the patient reported outcomes instruments a median of 1.9 years (IQR 2.6) postoperatively. All patient reported outcomes measures were not significantly different between pathology groups with PROMIS physical function ((median, IQR) HR 44.6, 9.9 vs. HV 44.1, 12.2), pain interference (HR 52.8, 9.9 vs. HV 52.4, 12.3), FFI pain scale (HR 33.3, 40.0 vs. HV 28.3, 37.0), FFI disability scale (HR 30.0, 41.0 vs. HV 28.9, 41.0), FFI activity limitation scale (HR 10.0, 27.0 vs. HV 10.0, 23.0), and FFI total (HR 25.8, 50 vs. HV 37.4, 37).
Conclusion: Arthrodesis of the first MTP joint provides similar nonunion and complication rates between hallux valgus and rigidus groups. At intermediate follow-up, MTP arthrodesis provides comparable validated patient reported outcomes scores between these two groups. Surgeons should be aware of these results when prognosticating the effect of MTP arthrodesis.
DOI: 10.1177/2473011421S00223
Toward Preventing Arthritis: A Comparison of Synovial RNA in Osteoarthritic Ankles and Knees
Mary C. Hamati, MD; Robert Maynard; Jonathan Bartolomei, MS; Michael J. Zuscik, PhD; Cheryl L. Ackert-Bicknell, PhD; Kenneth J. Hunt, MD
Introduction/Purpose: Osteoarthritis (OA) of the lower limb is a debilitating, incurable, expensive and prevalent condition in people over 45. Although ankle posttraumatic OA (PTOA) has the highest incidence, primary OA is increasingly recognized. The difference in OA incidence between lower limb joints is partly driven by differences in cartilage architecture and chondrocyte function at each site, with ankle chondrocytes showing reduced responsiveness to inflammatory mediators and more metabolic activity than those in the knee. Synovium also contributes to the pathogenesis of OA, however its potentially differential role in knee versus ankle OA remains an unanswered question. We aim to understand the molecular contribution of synovial dysregulation in the progression of ankle and knee OA to uncover candidate pathways for the development of targeted therapeutic paradigms.
Methods: After obtaining informed consent from patients undergoing total knee or ankle replacement, basic surgical, past medical history, and imaging data was collected. Synovium samples were harvested during surgery and processed for RNA. Bulk 150 bp, paired-end RNA seq was conducted using standard protocols using the Illumina NovaSeq6000 platform. After quality control trimming, reads were aligned to human reference genome (GRCh38) using STAR (v 2.5) using the Maximum Mappable Prefix method and HTSeq (V0.6.1) was used to index mappable reads per gene. Counts were corrected for gene length using the FPKM method. Differential expression was determined using the edgeR (v 3.16.5) package for R, after adjustment using a scaling normalization factor and P-values were corrected using the Benjamini and Hochberg method. Similarities between samples were determined using Spearman Correlation and degree of similarity was visualized considering the first three Principal Components (PC).
Results: RNA was obtained from 6 end-stage ankle OA, 1 end-stage knee OA patients. Of the ankle samples, two were PTOA and the remaining four were primary OA. The PTOA and the primary OA samples showed high sample correlation regardless of class (correlation coefficients ranged from 0.844 to 0.941). In contrast, the total knee sample was less correlated with the ankle samples (correlation coefficients ranged from 0.719 to 0.878). By using the first three PC, we observed that there was no obvious differentiation among the ankle OA samples, but there was clear separation between ankle and total knee samples. We observed an enrichment of genes annotated to the Gene Ontology clusters 'Extracellular Structure Organization' and 'Inflammatory Response' when comparing the two types of OA.
Conclusion: These initial pilot results of an ongoing study support our hypothesis that synovial transcriptome differs between the knee and ankle in end-stage osteoarthritis and that anatomic site is a larger driver of synovial expression differences than OA type. This is supported by previous differences reported between ankle and knee chondrocytes in end-stage OA. These findings emphasize the importance of investigating synovial tissue to better understand the microenvironment of the ankle joint and pathogenesis of all etiologies of OA. The ultimate goal is the development of clinical tests and therapeutics aimed at slowing or discontinuing the degenerative process in ankle arthritis.
DOI: 10.1177/2473011421S00224
Tracking Patient Reported Outcomes in Orthopaedic Surgical Patients at a Single Institution
Mary C. Hamati, MD; Atlee Witt; Michaele Francesco Corbisiero; Michael Tuffiash; Kenneth J. Hunt, MD
Introduction/Purpose: As the American healthcare system evolves into a value-based reimbursement model, emphasis on tracking and reporting healthcare outcomes has expounded. Patient reported outcome Measures (PROMs) are exceedingly valuable to orthopedists as a means to measure improvement and satisfy regulatory requirements. The NIH Patient-Reported Outcomes Measurement Information System (PROMIS) surveys are favored due to their accessibility, efficiency, and minimal floor and ceiling effects. Furthermore, they have been shown to predict outcomes after orthopedic surgeries. Psychosocial factors have also become increasingly important in predicting surgical outcomes. We aim to report the development and implementation of an institutional PRO data collection platform, including PRO completion rates and improvements in PROs for patients undergoing orthopaedic surgery.
Methods: We implemented a secure, HIPAA compliant, automated and EHR integrated, institutional platform to collect PROMs using a cloud-based tool. Patients undergoing surgery by sports medicine and foot and ankle surgeons were included and organized into four surgical pathways: (1) foot and ankle, (2) sports-knee, (3) sports-hip, and (4) sports-shoulder. PROMIS Physical Function (PF), PROMIS Pain interference (PI), site-specific (foot and ankle, knee, hip, and shoulder) Single Assessment Numeric Evaluation (SANE), and the brief resiliency scale (BRS) were collected at the patient’s pre-operative visit. The PROMIS and SANE surveys were again collected at 3-, 6-, and 12-month post-operative visits. Surveys were disseminated automatically and patients were able to complete PROMs onsite on secure tablets or remotely through their personal device. Primary outcomes included compliance rates, baseline PRO scores, and change in scores at the various post-operative timepoints for patients in the four surgical pathways.
Results: More than 6,000 patients were included, with majority of patients from the sports-knee (47%), followed by sports- shoulder (27%), foot and ankle (23%), and sports-hip (4%) pathways. Average completion rate was highest at the pre-operative timepoint for all pathways (81%), with completion rates of 62% at 50% at 6 months and 45% at 12MO. Compliance rates were lowest highest in the foot and ankle pathway at 12 months (62%). Average baseline scores for all patients were 40.8 for PROMIS PF, 61.1 PROMIS PI, 41 SANE, and 3.9 for BRS. Baseline scores didn't significantly vary between the surgical pathways. Scores improved for all patient pathways at all timepoints for PROMIS PF, PI and SANE PROMs (Table 1). No workflow disruptions were noted for survey administration.
Conclusion: Tracking PROs using an automated platform is feasible in orthopaedic clinics. Compliance rates are very good and dependent on provider, staff, and patient buy-in. Patients undergoing surgery had an average baseline PROMIS PI scores >=1 standard deviation from the normal population and all scores improved after surgery. Importantly, statistical significance doesn't always reflect minimum clinically important differences (MCIDs). MCIDs for PROMIS PF and PI have been reported to fall between 5-10 points depending on range of values and methods of calculation. Further investigation into outcomes by procedure type and patient factors is warranted to identify predictive factors of surgical outcomes.
DOI: 10.1177/2473011421S00225
Prevalence of Asymptomatic Bone Marrow Edema in the Talus in Professional Ballet Dancers: Preliminary Data from 2-Year Prospective Study
Ethan R. Harlow, MD; Pranav Khambete; Jason Ina, MD; Shana N. Miskovsky, MD
Category: Ankle; Sports
Keywords: Talus; Bone Stress Injuries; Sports
Introduction/Purpose: Bone marrow edema (BME) appears as increased interstitial fluid accumulation within the bone marrow on magnetic resonance images (MRI). Asymptomatic BME has been found incidentally and described in competitive athletes, long- distance runners, and patients with altered biomechanics where the true etiology remains unclear. The natural history and clinical implications of asymptomatic BME in the elite and actively-competing athlete is not well characterized. Moreover, there is debate on how to manage and counsel patients on these findings in a high-risk bone such as the talus. This study presents early data from a prospective enrollment study of professional ballet dancers characterizing the prevalence of asymptomatic BME in the talus.
Methods: Fourteen (14) professional ballet dancers enrolled in the 2-year prospective, IRB-approved study after informed consent was obtained. Exclusion criteria included: subjects reporting foot and ankle pain or disability on initial preseason evaluation, foot and ankle surgery or injury within the last year prior to evaluation, and any contraindications for MRI. Subjects underwent a physical examination and completed Foot and Ankle Ability Measure (FAAM) and Foot and Ankle Disability Index scores (FADI). Bilateral foot and ankle MRIs without contrast were completed upon study enrollment and interpreted by a blinded, fellowship-trained musculoskeletal radiologist.
Results: Of 14 professional ballet dancers enrolled in the study, 6 were female, 8 were male, and the mean age was 24.4 years. All dancers reported no pain or disability in their feet and ankles at the time of evaluation and had physical exam findings unremarkable for performance-limiting pathology. Of the 14 dancers, 64% (9) had MRI evidence of talar BME. 6 subjects had bilateral talar BME and 3 had unilateral findings. 53% (8) had BME localized to the posterior process of the talus, 13% (2) localized in the talar body, 13% (2) localized to the talar head and neck, and 20% (3) subjects had pan-talar BME. All subjects had BME seen only on T2 sequences with one patient demonstrating bilateral pan-talar BME on both T1 and T2 sequences. There was no significant correlation using Welch’s unequal variances t-test (α = 0.05) between talar BME and either FADI or FAAM scores.
Conclusion: These findings demonstrate a high prevalence (64%) of talar bone marrow edema in asymptomatic professional ballet dancers with benign physical exams and normal functional scores. Yet, the long-term clinical significance of these findings are unknown.
DOI: 10.1177/2473011421S00226
Clinically Significant Improvement in Pre vs Post-Operative PROMIS Scores after Cavovarus Reconstruction in Patients with Charcot-Marie-Tooth Disease
Edward T. Haupt, MD; Tonya W. An, MD; Giselle M. Porter; Max Michalski, MD; Glenn B. Pfeffer, MD
Category: Ankle; Hindfoot; Midfoot/Forefoot; Other
Keywords: Charcot Marie Tooth; Outcomes Measures; Cavovarus Foot Deformity
Introduction/Purpose: Charcot-Marie-Tooth (CMT) disease is an inherited progressive neurologic disorder characterized by extremity deformities and functional deficits. Surgery is indicated for substantial functional deficits and severe deformity. Reconstructive surgery is individualized and multifaceted to correct the cavovarus deformity, and maximize function with tendon transfers and joint stabilization procedures. No previous study has reported improvement from pre-operative baseline patient reported outcome measures to post-operative outcome measures. We studied PROMIS scores and patient satisfaction surveys to report improvements in physical function, pain interference, and depression. Our hypothesis was that CMT patients' preoperative baseline would be significantly worse than the control population in all domains, and that they would experience demonstrable improvement greater than the minimally clinically important difference (MCID) for the 3 PROMIS score domains tested post- operatively.
Methods: Prospective PROMIS scores were collected on 147 feet in 89 patients who had reconstructive foot surgery for CMT during a 40-month period (June 2016-December 2020) by a single surgeon. Radiographic and clinical data were recorded prospectively to identify complications. Each patient completed a battery of physical function (PROMIS-PF), pain interference (PROMIS-PI), and mood/depression (PROMIS-M) instruments pre-operatively, every 3 months for the first post-operative year, and annually thereafter. Pre-operative PROMIS scores are reported for patients prior to any surgery on either foot to establish a functional baseline. Post-operative PROMIS values are reported only after the last planned surgery was completed in the common setting of staged bilateral surgeries. Patient satisfaction surveys were administered at last follow-up. Post-operative complications were recorded. Statistical analysis was performed with students t-test for continuous variables and chi-squared analysis for categorical variables. PROMIS scores are reported as mean (+/- standard deviation).
Results: 41 patients met inclusion criteria for reporting pre-operative baseline PROMIS scores, and 57 patient’s post-operative PROMIS data were included after the final reconstructive surgery within the study window. Mean follow-up was 26 months. Pre- operative baseline PROMIS demonstrate CMT patients have worse PROMIS-PF, PROMIS-PI, and PROMIS-M than the population which is statistically and clinically significant. All PROMIS domains were improved by clinically and statistically significant values. PROMIS-PF improved from 38 (+/-6) to 46 (+/-5), a 4-5x improvement over MCID (2). PROMIS-PI improved from 59 (+/-8) to 51 (+/-7) representing a 1-2x improvement in the MCID (4). PROMIS M improved from 53 (+/-10) to 49 (+/- 5) achieving MCID 2. >90% were highly satisfied and would undergo surgery again. There were 7 complications: 1 deep infection, 2 superficial infections, 1 superficial wound dehiscence, and 3 unplanned hardware removals. 5/7 of these patients experiencing complications remained ’satisfied' or 'very satisfied'.
Conclusion: Patients with CMT disease have baseline functional deficits in physical and mental health as judged by PROMIS measures that were worse than the population means in all 3 tested domains. Surgical reconstruction produced clinically significant improvements in PROMIS-PI, PF, and M domains at up to 4 years of follow-up. Patients were highly satisfied with the results with an acceptable rate of post-operative complications.
DOI: 10.1177/2473011421S00227
Pain Tolerance Self-Assessment vs Objective Pressure Sensitivity: Do Patients Accurately Estimate Their Own Pain Tolerance?
Edward T. Haupt, MD; Giselle M. Porter; Timothy P. Charlton, MD; David B. Thordarson, MD
Category: Basic Sciences/Biologics; Other
Keywords: Pain; PROMIS; Clinical Outcomes
Introduction/Purpose: Effective pain treatment remains elusive in the orthopedic foot and ankle practice as evidenced by the variable experience of pain, post-operative or otherwise. Intrinsic pain tolerance is likely contributing to this variability in the patient’s experience of pain. Pressure dolorimetry is a validated, objective measure to assess pressure sensitivity and is correlated with pain tolerance. No previous study in the orthopedic foot and ankle literature has attempted to correlate objective versus subjective pain tolerance. General mental health is associated with central pain sensitization and may also affect pain tolerance. Our hypothesis was that subjective self-assessment of pain tolerance would be correlated with objective dolorimetry. We hypothesized that mental patient-reported outcome scores would also be correlated to objective pain tolerance.
Methods: Prospectively-collected patient-reported outcome scores (PROMIS), dolorimetry measurements, and survey data of subjective reported pain tolerance were collected pre-operatively on 50 consecutive patients by two surgeons in an urban orthopedic foot and ankle practice. Patients were included if they had normal sensation on the plantar foot and no prior surgery or plantar heel source of pain. Each patient underwent objective measurement of their ability to withstand pressure applied to the plantar heel causing 5/10 pain using a hand-held dolorimeter with digital pressure measurement display. Each patient was administered a preoperative battery of PROMIS physical function (PF), pain interference (PI), and mood/depression (M) instruments, and a separate survey where they scaled their subjective tolerance to pain and discomfort. Statistical analysis was performed utilizing students t-test for continuous variables. Correlations were evaluated with Pearson’s R coefficient. Data are reported as means (+/- standard deviation) unless otherwise noted.
Results: 50 patients received hand-held dolorimetry measurements, completed the pain tolerance survey, and completed PROMIS measures. Dolorimetry data from the plantar heel was normally distributed with mean force 24 N/cm2 (+/-10) to reflect a 5/10 pain experienced by the patient. Patients were shown to estimate their pain threshold with mean subjective pain threshold 6.8/10 (+/-2) regardless of objective pain data or PROMIS scores. The mean PROMIS scores of the sample were PF (41+/-8), PI (60+/-7), and M (49+/-9) reflecting a sample with decreased physical function and increased pain which could be expected in an outpatient foot and ankle clinic. There was a negative correlation of R=(-0.432) regarding PROMIS-M with dolorimetry objective pain tolerance which was statistically significant (p<-0.05). Patients had more features of depression/anxiety (PROMIS-M score >60) had a statistically significant decrease in pain threshold to 18+/-8 N/cm2 compared to 30 +/- 9 N/cm2 for those who were less depressed (p<0.01)).
Conclusion: Subjective self assessment of pain tolerance is not well correlated to objective pain threshold data or other markers of mental health, and should not influence medical decision-making. Features of depression on PROMIS-M are associated with an objectively lower pain threshold which is in agreement with prior findings of central pain sensitization in patients with depression and anxiety in other studies. Future work is required to correlate dolorimetry data with post-operative medication utilization, and patient-reported outcome measures after surgery.
DOI: 10.1177/2473011421S00228
Implementation and Evaluation of a Formal Virtual Medical Student Away Rotation in Orthopaedic Surgery During the COVID-19 Pandemic
Brittany E. Haws, MD; Sandeep Mannava; Bonnie K. Schuster; Benedict F. DiGiovanni, MD
Category: Other
Keywords: General Principles / Context; Informed Decision; Health Care
Introduction/Purpose: Away rotations are a valuable experience for medical students when applying for residency. However, in light of the ongoing coronavirus disease 2019 (COVID-19) pandemic, traditional in-person away rotations were largely suspended during the 2020-2021 residency application cycle. As such, there has been significant interest in the development of virtually-based substitutes. The purpose of this study is to evaluate the utility of a formal virtual fourth year medical student away rotation in orthopaedic surgery by surveying student, resident, and faculty participants.
Methods: A two-week virtual orthopaedic elective was offered to fourth-year medical students from outside institutions in lieu of a traditional in-person away rotation. The course was conducted via online video conferencing and consisted of multiple components including nightly subspecialty case-based didactics, weekly social events with residents, assigned resident mentors, student case presentations, and the ability to attend the residency’s daily conferences. Following course completion, anonymous surveys were administered to students as well as resident and faculty participants to evaluate the rotation. 23 of 24 participating students (96%) completed the student survey and 22 of 24 participating faculty and residents (82%) completed the resident/faculty survey.
Results: Most students were very (87%) or somewhat satisfied (9%) with their experience and found the virtual rotation to be a very (35%) or somewhat useful (61%) substitute for in-person rotations. Students indicated the virtual rotation very (91%) or somewhat positively (9%) influenced their perception of the residency. All students indicated the rotation was very educational. Most students (91%) reported the rotation was very useful for learning about the program and culture, with the subspecialty didactics and happy hours being the most useful. Faculty and residents indicated the virtual rotation was useful for getting to know the students, with resident mentoring and case presentations most useful. Faculty and residents reported the rotation was useful for assessing student characteristics such as knowledge base and interpersonal communication skills. Students' qualitative responses highlighted the small group size, educational value, quality of interactions with residents/faculty, and opportunities for participation as positive features of the rotation.
Conclusion: A well organized, formal virtual orthopaedic surgery away rotation can be a valuable experience for medical students that provides educational value, insight into a program’s culture, and an opportunity to demonstrate interest in the program. Virtual rotations can also be useful tool for residencies to share information about their program and learn more about prospective applicants. Features such as dedicated subspecialty case-based didactics, resident social events and mentoring, student case presentations, and small group formats are recommended to maximize value.
DOI: 10.1177/2473011421S00229
Outcomes Following Intramedullary Nail vs Plate Fixation for Tibiotalocalcaneal Arthrodesis: A Systematic Review
Erik Hegeman; Thomas C. Dowd, MD; Jeannie Huh, MD
Category: Ankle Arthritis; Hindfoot; Trauma
Keywords: Tibiotalocalcaneal Arthrodesis; TTC; Intramedullary Nail
Introduction/Purpose: Tibiotalocalcaneal arthrodesis (TTCA) is indicated to treat pain and dysfunction that may result from a variety of ankle and hindfoot pathologies by achieving fusion of the tibiotalar and subtalar joints. Two common fixation methods exist to achieve TTCA: retrograde intramedullary nail (IMN) fixation and plate fixation using a lateral trans-fibular or posterior Achilles-tendon splinting approach. The purpose of this study is to review the literature and compare the outcomes of TTCA using IMN fixation with those of plate fixation using a lateral trans-fibular approach.
Methods: A comprehensive search of the PubMed, Cochrane, and EMBASE databases was performed on 01 February 2021 for studies of all levels of evidence pertaining to TTCA using IMN and plate fixation. Reasons for exclusion included: no formal joint preparation, non-English language, concomitant methods of fixation (e.g., IMN with additional plate fixation) and follow-up less than 12 months.
Results: Fourteen studies (11 level III and 3 level IV) met criteria and were included. A total of 386 fusions were documented in 356 patients [259 (67%) IMN and 127 (33%) plate fixation]. In the IMN group, union rates at the tibiotalar joint (TTJ) were 84% (219/259) and subtalar joint (STJ) were 90% (229/259) with an overall complication rate of 20% (53/259). Average initial AOFAS scores were 34.3+-7.9, increasing to 72.4+-9 postoperatively. In the plate fixation group, union rates at the TTJ were 82% (103/127) and STJ were 86% (108/127) with an overall complication rate of 30% (39/127). Average initial AOFAS scores were 37.0+-6.9, increasing to 74.4+-12.5 postoperatively. No statistical differences were noted between the TTCA IMN and plate cohorts when comparing rates of TTJ or STJ union (p= 0.6, and p=0.2, respectively) and postoperative AOFAS scores (p=0.59). However, the plating group had a statistically higher overall complication rate (p=0.02).
Conclusion: A systematic review of the available literature suggests that there is no statistical difference in union rates or functional outcomes between TTCA using intramedullary nail or lateral trans-fibular plate fixation. However, the lateral trans- fibular plate has a statistically higher complication rate when compared to intramedullary nails. Further comparative prospective cohort studies and randomized controlled trials are needed to further elicit differences between these groups and confirm the findings of this systematic review.
DOI: 10.1177/2473011421S00230
Case Report: Tibiotalocalcaneal Arthrodesis Utilizing a Titanium Mesh Implant for Limb Salvage after Failed Charcot Reconstruction
Introduction/Purpose: Tibiotalocalcaneal (TTC) arthrodesis has been employed as a mean to achieve hindfoot fusion and limb salvage. A particular challenge in limb salvage is achieving successful fusion in the setting of massive bone deficit. Several augmentation strategies have been trialed in this setting, such as structural allografts, 3D printed implants, fibular strut grafts, to name a few.
Methods: We present a case describing TTC fusion for limb salvage utilizing a titanium mesh implant, combined with bone graft in the setting of massive bone deficit in an individual with Charcot arthropathy from Diabetes Mellitus and HIV after Pilon fracture, performed as revision procedure after failed Charcot reconstruction with a ringed external fixator and femoral head allograft with subsequent nonunion.
Results: At last follow-up (22 months postoperative) patient is weight bearing as tolerated in Charcot Restraint Orthotic Walker boot. CT imaging at 18 months postoperative demonstrates stable implant and arthrodesis.
Conclusion: Use of a titanium mesh implant is a reasonable option combined with bone graft for augmentation of TTC fusion in the setting of massive bone deficit.
DOI: 10.1177/2473011421S00231
Efficacy of Bone Graft on Fusion Rates in Primary Open Ankle Arthrodesis: A Systematic Review
John Heifner, MD; Joseph G. Monir, MD; Christopher W. Reb, DO
Introduction/Purpose: Success in ankle arthrodesis has been reported between 74% and 100%. Despite many recent reports with success rates >95%, the modern literature details a precipitous increase in the use of biological adjuvants for primary ankle arthrodesis. These additions raise the cost of the procedure and potentially incur morbidity related to the donor site or adverse graft response. For these reasons the routine use of bone graft has come under scrutiny with no consensus regarding its use. The cost - both direct and indirect - of biological adjuvant should be weighed against its added value to clinical outcomes. This systematic review aimed to assess the efficacy of bone autograft versus no graft on achieving a clinically successful primary open ankle arthrodesis fixated using cannulated screws.
Methods: Included studies were divided into 3 groups based on the use of bone graft: no bone graft (NBG), fibular onlay with local autograft (FOBG), and the use of autograft without fibular onlay (BG). Pooled data analysis was performed, and fusion rates were frequency weighted in order to appropriately judge the impact of each study. Cohen’s d was used to evaluate effect size for the use of bone graft. Modified Coleman Methodology Score (MCMS) was calculated to analyze reporting quality.
Results: These selected studies described outcomes for a total of 884 patients with mean follow up of 46 months. The reviewed literature was of moderate quality, with an MCMS of 60.6. The weighted mean rate of fusion for the 3 groups was 96% in the NBG group (n=182), 96% in the FOBG group (n = 257), and 95% in the BG group (n = 445), with no significant difference between the groups (p=0.98). Use of bone graft resulted in a Cohen’s d effect size of 0.10 (95% confidence interval 0.07- 0.26). Time to fusion for the 3 groups was 13.60 weeks for the NBG group, 14.51 weeks for the FOBG group, and 15.10 weeks for the BG group, with no significant difference between the groups (p=0.87). Number needed to treat was 7 with the event of interest defined as a fusion rate less than 95%.
Conclusion: Bone graft use in primary open ankle arthrodesis fixated with cannulated screws did not have a significant effect (p=0.98) on union rates and yielded a small effect size. Further data demonstrated that 7 ankle arthrodesis patients need to be treated with bone graft in order to prevent 1 clinically significant nonunion. The current findings are both clinically and economically relevant, as commercial bone graft carries additional cost and autologous graft harvest is not consistently a benign endeavor. With increased cost and potential for complication, bone graft use should demonstrably improve clinical outcomes in order to validate these additional burdens.
DOI: 10.1177/2473011421S00232
Evaluation of Union Rates Between Two Fixation Constructs with Use of an Allograft Bone Wedge in the Lapidus Procedure
Introduction/Purpose: The Lapidus procedure is used to treat a painful bunion deformity by decreasing motion and aligning the first ray of the foot. Although structural allograft has been previously described as acceptable practice for reconstructive foot and ankle surgery, outcomes following the addition of an allograft bone wedge at the Lapidus arthrodesis site are unknown. The biomechanical properties of various internal fixation constructs for Lapidus have been evaluated in cadaveric models with no consensus on the superiority of a single fixation method. Our objective was to report union rates for the Lapidus procedure with and without the use of an allograft bone wedge and to determine if fixation construct influenced the rates of union.
Methods: Lapidus patients with fixation constructs of 2 crossed compression screws (CS) and a medial locking plate with single intra-articular screw (LPS), with and without use of an allograft bone wedge were retrospectively analyzed. Inclusion required a postoperative CT scan which evaluated union status, with greater than 50% bony bridging across the arthrodesis site used as determination of bony union. Exclusion criteria included age younger than 18 years, prior midfoot surgery, concomitant surgical procedures which may alter the normative healing process, neuropathy and inflammatory disease. Demographic and radiographic outcomes were analyzed between the wedge and no wedge groups. Pre and post operative radiographic measurements included intermetatarsal angle (IMA), first cuneiform-metatarsal length (CML) and relative length of the 1st metatarsal (RLM). Two sample t tests were used to evaluate the radiographic measurements and risk differences were calculated to evaluate rates of union. All analyses were executed using SAS Studio version 9.04.
Results: A total of 81 cases were included with 54 cases in the wedge group and 27 cases in the no wedge group. Preoperative IMA, CML and RLM measurements were not significantly different between the groups (p >0.05 for each). An overall union rate of 92% was found, with a significant difference (p=0.01) between the wedge group with 87.5% union and the no wedge group with 100% union (Table 1). With LPS fixation, there was no significance difference (p>0.05) in rates of union between the wedge (N=25) and no wedge (N=21) groups. With CS fixation, there was a significant difference (p=0.014) in rates of union between the wedge (N=29) and no wedge (N=6) groups. Postoperative radiographic comparisons between the wedge and no wedge groups were not significant for IMA (p=0.89), CML (p=0.16) and RLM (p=0.32) measurements.
Conclusion: With LPS fixation, rates of union were not significantly different between the wedge (96% union) and no wedge groups (100% union). This finding highlights the importance of a robust fixation construct which is an important predictor of union in Lapidus procedures. Use of an allograft wedge can facilitate intraoperative decisions on the appropriate amount of bony resection and decrease the risk of metatarsalgia due to shortening. Lapidus arthrodesis with an allograft bone wedge fixated with a medial locking plate and intra-articular compression screw provides the ability to maintain first ray length and achieve greater corrections with satisfactory union rates.
DOI: 10.1177/2473011421S00233
Syndesmosis Injury Imparts A Large Negative Effect on Patient Reported Outcomes: A Systematic Review
John Heifner, MD; Jack E. Kilgore; Jennifer A. Nichols; Christopher W. Reb, DO
Category: Trauma; Ankle; Sports
Keywords: Syndesmotic Injury; Ankle Fracture; Return to Play
Introduction/Purpose: Syndesmosis injuries are common, comprising up to 25% of all ankle sprains and being present in 35% or more of ankle fractures. Within the narrative of the syndesmosis literature, the substantial negative impact of syndesmosis injury is commonly described in intuitive yet qualitative terms. Therefore, a constructive criticism of the literature is to question how often and how well these reports have characterized the magnitude of the impact of the syndesmosis injury itself compared to confounding factors like concomitant injury. Indeed, such information particularly in aggregate, has the potential to influence clinical practice. Within this context, the objective of this systematic review was to assess how often and how well the literature has characterized the magnitude of syndesmosis injury.
Methods: Included reports were grouped based on the setting in which syndesmosis injury was studied: (1) isolated syndesmosis disruption compared to lateral ankle sprain, (2) isolated syndesmosis disruption, (3) ankle fracture with concomitant syndesmosis disruption compared to ankle fracture with no syndesmosis disruption, and (4) ankle fracture with concomitant syndesmosis disruption without a comparison group with no syndesmosis disruption. Literature quality was assessed via the Modified Coleman Methodology Score (MCMS). Patients with and without syndesmosis injury were compared by independent sample t-tests using pooled values for specific patient reported outcome measures. Additionally, for these datasets, effect sizes were computed using Cohen’s d.
Results: Mean MCMS across all four groups was 59.9, indicating a moderate level of evidence. MCMS did not differ significantly between groups (p = 0.07). Analysis of reported outcomes indicated that syndesmosis injury has a significant (p = 0.007) effect and a large negative effect (effect size = 1.77) (Figure 1) on time to return to play when comparing athletes with isolated syndesmosis sprain to those with lateral ankle sprain. Additionally, analysis of ankle fracture patients indicated that syndesmosis injury has a large negative effect on functional outcomes (effect sizes > 0.80 for Olerud Molander and AOFAS scores), but little effect on pain (effect size = 0.14 for VAS pain). Studies which reported long term outcomes (mean 87 months) showed a very large negative effect (effect size 9.24) for Olerud Molander scores across 95 patients.
Conclusion: In athletic populations, days missed due to syndesmosis disruption was statistically significant with a large effect size compared to lateral ankle sprain. Further, among ankle fracture patients, Olerud Molander and AOFAS scores indicate a large negative impact of syndesmosis disruption on functional outcomes despite a small negative impact on short term pain. These results indicate that the continued impact of this injury extends beyond the initial painful period and requires more attention. These patient-reported outcomes support the qualitative assertions that syndesmosis injury potentially imparts a large negative effect on clinical outcomes.
DOI: 10.1177/2473011421S00234
The Prognostic Value of Syndesmosis Malreduction for Revision Surgery: A Systematic Review
John Heifner, MD; Jack E. Kilgore; Jennifer A. Nichols; Christopher W. Reb, DO
Introduction/Purpose: Reported rates of syndesmosis malreduction are highly variable due to applied criteria that differ in imaging modality, threshold for malreduction and use of the contralateral ankle for comparison. Studies have emphasized the importance of anatomic reduction while providing inconclusive evidence for the need for revision surgery in malreduced ankles. With no industry standard for determining malreduction, it is unclear whether the most commonly used criteria is a valuable discriminator for clinical decision making. Our objective was to describe the rates of syndesmosis revision that are reported in the literature and to determine if malreduction diagnoses are reliable in predicting the need for syndesmosis revision surgery.
Methods: Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta Analyses) guidelines, a systematic review of the literature was performed in order to describe revision syndesmosis surgery. Included studies were grouped based on criteria for determining malreduction - group 1 (N = 954) used unilateral radiograph, group 2 (N = 41) used unilateral CT scan, group 3 (N =531) used bilateral CT scan and group 4 (N = 119) used bilateral radiograph. Evidentiary quality was graded with the Modified Coleman Methodology Score (MCMS). Student t tests were used to calculate the differences between groups for rates of malreduction and revision. For the screening criteria most commonly used to determine malreduction, the test characteristics sensitivity, specificity and positive predictive value (PPV) were calculated.
Results: Pooled rates of malreduction and revision for the groups using CT scan (groups 2 and 3, N = 572, mean follow up 16 months) were 23.5% and 0.25% respectively. Pooled rates of malreduction and revision for the groups using bilateral imaging (groups 3 and 4, N = 650, mean follow up 20 months) were 18.5% and 0.8% respectively. Significant differences were found between CT scan and radiograph for malreduction (p<0.001) and for revision (p=0.02). Significant differences were also found between bilateral and unilateral imaging for malreduction (p=0.01). The malreduction criteria of a 2mm difference in tibiofibular space on CT scan between the injured and uninjured side was used in 6 studies (N = 531, mean follow up 19 months). The sensitivity of this criteria for detecting cases which required revision was 100%, specificity 78%, and PPV 6%.
Conclusion: It is unclear whether high rates of malreduction are due to suboptimal surgical repair which lead to clinical detriment or are they solely an imaging finding which depend heavily on the criteria for diagnosis. The most commonly used criteria for malreduction - a 2mm side-to-side difference in tibiofibular space on CT scan - is highly sensitive for reoperations. The specificity and PPV indicate that a threshold of more than 2mm is needed to better evaluate those ankles which may require revision surgery. Based on the current findings, malreduction diagnoses do not adequately translate from disease-oriented information to patient-oriented information.
DOI: 10.1177/2473011421S00235
Surgical Reconstruction of Progressive Collapsing Foot Deformity Restores Kinematics during Simulated Level Walking
Jensen K. Henry, MD; Jeffrey W. Hoffman, MS; Jaeyoung Kim, MD; Brett D. Steineman; Daniel R. Sturnick, MS; Constantine A. Demetracopoulos, MD; Jonathan T. Deland, MD; Scott J. Ellis, MD
Category: Basic Sciences/Biologics; Hindfoot
Keywords: Biomechanics of the Foot and Ankle; Flatfoot; Gait Study Range of Motion
Introduction/Purpose: Progressive collapsing foot deformity (PCFD) is a complex 3-dimensional pathology with a wide variety of surgical treatments. Regardless of technique, operative management of PCFD aims to restore normal foot architecture with attention to avoid the consequences of under- or over-correction. However, current methods of evaluating PCFD correction rely on static measurements, which do not assess dynamic function of the foot. Recent advances in robotic technology allow for the dynamic assessment of surgical correction of PCFD. This study sought to assess the effects of 2 osteotomies for PCFD, the medializing calcaneal osteotomy (MCO) and lateral column lengthening (LCL), on kinematics and plantar pressure during simulated gait. We hypothesized that the combination of LCL and MCO would restore joint kinematics and plantar pressure values to normal levels.
Methods: Twelve cadaveric mid-tibia specimens (mean age 73 years, 8 female) were loaded on a 6-degree of freedom robotic gait simulator. Ground reaction forces and muscle forces were optimized utilizing an established iterative process. An 8-camera motion capture system was utilized to calculate joint kinematics using reflective markers attached by k-wires into bone. Plantar pressures were recorded using a pedography mat attached to the force platform. Testing was performed first in the native intact state, and again after creation of the flatfoot model. After flatfoot testing, surgical reconstruction and testing were performed in stages with MCO, and LCL with sequential 6mm and 8mm grafts. Bias-corrected bootstrapped 95% confidence intervals were calculated from the repeated measures difference between normal, flatfoot, post-MCO, post-MCO and post-reconstructive conditions. Center of plantar pressure excursion index (CPEI) was calculated and compared between conditions using a repeated measures ANOVA with Tukey post hoc analysis.
Results: Overall, surgical correction restored kinematics to normal levels (Figure). MCO alone resulted in statistically significant improvement in subtalar eversion in the first 20% of stance, and post-MCO subtalar kinematics were statistically similar to normal. LCL (either 6mm and 8mm) alone did not significantly correct talonavicular abduction after PCFD. However, in conjunction with MCO, LCL was able to significantly correct talonavicular kinematics throughout the majority of stance phase, with kinematics statistically similar to normal levels. Each surgical step (LCL 6mm, LCL 8mm, MCO) resulted in sequential lateralization of the center of plantar pressure. At the culmination of surgical reconstruction (MCO + LCL), plantar pressure was significantly corrected compared to PCFD (P<0.0001). After surgical reconstruction, CPEI was slightly increased (lateralized) in comparison to normal, but was not significantly different from the normal state.
Conclusion: The findings from this study support our hypothesis that surgical reconstruction of PCFD via MCO and LCL restores normal level walking kinematics. While the isolated effect of MCO and LCL resulted in significant changes in subtalar and talonavicular kinematics, the synergistic effect of combining MCO and LCL were most effective in restoring normal kinematics. However, lateralization of plantar pressure after combining MCO and LCL compared to the normal condition indicates the potential for overload of the lateral column, as described previously. Therefore, surgeons should be cautious in increasing osteotomy size at the lateral column to avoid overload.
DOI: 10.1177/2473011421S00236
The Impact of Progressive Collapsing Foot Deformity on Foot & Ankle Kinematics and Plantar Pressure During Simulated Gait
Jensen K. Henry, MD; Jeffrey W. Hoffman, MS; Jaeyoung Kim, MD; Brett D. Steineman; Daniel R. Sturnick, MS; Constantine A. Demetracopoulos, MD; Jonathan T. Deland, MD; Scott J. Ellis, MD
Category: Basic Sciences/Biologics; Hindfoot
Keywords: Biomechanics of the Foot and Ankle; Flatfoot; Gait Study Range of Motion
Introduction/Purpose: Progressive collapsing foot deformity (PCFD) is a 3-dimensional pathology associated with insufficiency of the posterior tibial tendon (PTT), ligamentous failure, joint malalignment, and aberrant plantar force distribution. Existing knowledge of PCFD consists of static measurements, which provide information about the structure of the foot but none about its function. Cadaveric gait models provide an opportunity to measure motion both at the joints primarily affected in PCFD and the adjacent joints that are at risk for progressive subluxation and arthritis. This study sought to develop a flatfoot model for a robotic gait simulator and quantify gait kinematics and plantar pressure between normal and flatfoot conditions, which we hypothesized would be altered after the creation of a flatfoot deformity model.
Methods: Cadaveric specimens were loaded on a 6-degree of freedom robotic gait simulator and the extrinsic tendons were attached to linear motors. Ground reaction forces and muscle forces were optimized utilizing an established iterative process. An 8-camera motion capture system was utilized to calculate joint kinematics using reflective markers attached by k-wires into bone. A plantar pressure mat attached to the force platform was used to calculate the center of pressure excursion index (CPEI) for each condition. The flatfoot model was created via sectioning of the spring ligament and medial talonavicular joint capsule followed by cyclic axial compression until 5-15° of talonavicular abduction was achieved in a static, loaded pose. Testing of the flatfoot state was then performed with inactivation of the PTT. Bias-corrected bootstrapped 95% confidence intervals were constructed from the repeated measures difference between flatfoot and normal conditions. Paired t-tests were used to compare the CPEI between conditions.
Results: Twelve mid-tibia cadaveric specimens (mean age 73 years, 8 female) with no prior foot/ankle surgery were used. There were significant differences in kinematics between normal and PCFD conditions at the ankle, subtalar, and talonavicular joints (Figure). There was significantly increased ankle plantar flexion in flatfoot in the first 80% of stance phase. There was significantly greater subtalar eversion in flatfoot compared to normal from 10-90% of stance phase. Talonavicular abduction and eversion were also significantly greater in flatfoot from 10-100% of stance. The CPEI was significantly decreased in the flatfoot condition (Figure), indicating a medialization in center of pressure (p<0.0001).
Conclusion: The results from this study support our hypothesis of altered kinematics and plantar pressure after flatfoot deformity creation and corroborate previous biomechanical studies of static alignment in PCFD. Increased talonavicular abduction and subtalar eversion are hallmarks of flatfoot deformity, and increased ankle plantarflexion may represent the plantarflexed position of the talus in PCFD. In addition, plantar pressure was significantly medialized with flatfoot deformity. These findings highlight the utility of the gait simulator as a tool for future study of PCFD, especially for analysis of deformity patterns and the specific effects of individual interventions.
DOI: 10.1177/2473011421S00237
Biomechanical Comparison of Cannulated Screws vs Nitinol Staple for Tarsometatarsal Fusion in A Cadaveric Model
Alexander S. Herrin; Zachary Koroneos; Sherif T. Elakkari; Gregory Lewis, PhD; Temitope Adebayo; Umur Aydogan, MD
Introduction/Purpose: Patients with hallux abducto-valgus typically require first-tarsometatarsal arthrodesis procedures for which the method of fixation is controversial. Nitinol staples have increased in popularity due to their pseudoelastic, and fatigue resistant properties that allow for shape memory. The objective of this study was to evaluate the performance of a Nitinol staple and crossed-screws through three-dimensional diastasis measurements for the first-tarsometatarsal joint in a 4-point bending isolated cadaveric joint model. We tested the hypothesis that a medially applied Nitinol staple would provide the same dynamic stability as crossed-screws while allowing for more physiologic motion.
Methods: Seven matched-pairs of lower limb cadaveric specimens were thawed and dissected to isolate the first-tarsometatarsal joint including the first-metatarsal, medial cuneiform, and joint capsule. One specimen from each donor was fixed with a Nitinol staple placed on the medial side of the joint while the other specimen was fixed with two cannulated crossed-screws. Specimens were potted and tested in an MTS test frame (MTS FlexTest 40 MTS, Eden-Prarie, MN) in a 4-point bending setup (Figure 1A) while maintaining a temperature of 37°C. The diastasis between the first-metatarsal and medial cuneiform was measured at two points on the plantar aspect of each bone near the joint (Figure 1B). Specimens were pre-loaded to 10 N, then stepwise increases in cyclic loading performed at 1 Hz and 50 cycles, at 5 N force intervals until failure (complete separation) at the joint occurred. Diastasis measurements were recorded after every 25 N (250 cycles).
Results: 3 of 7 matched pairs of specimens have been tested to date. All specimens were able to endure loading up to a peak load of 225 N (2000 cycles) (Figure 1C). At this peak-load, specimens fixed with the Nitinol staple had an average diastasis of 0.79 mm +/- 0.70 mm (average +/- std deviation) versus 0.39 mm +/- 0.16 mm in specimens fixed with screws. Specimens fixed with the staple construct failed at 277 N +/- 51 N whereas those fixed with screws failed 315 N +/- 48 N. Results for 4 additional matched pairs are pending.
Conclusion: There has been debate as to whether the rigid fixation of crossed-screws or the compressive shape memory properties of Nitinol staples are advantageous for tarsometatarsal arthrodesis. No previous study has compared the two methods of fixation in a cadaveric model. In this study no significant differences between the two methods have been detected to date. However, other benefits of the staple construct may include decreased procedural time, decreased time under anesthesia, and possible permittance of earlier post-operative weightbearing.
DOI: 10.1177/2473011421S00238
Vascular Evaluation of Diabetic Patients Presenting with Radiographic Calcified Vessels of the Foot and Ankle
Dolfi J. Herscovici, Jr., DO, FAAOS; Julia M. Scaduto, APRN
Introduction/Purpose: Calcification of the vessels is a common finding in patients with peripheral arterial disease (PAD) and can indicate a compromised extremity. The incidence of PAD disease has been reported in approximately 29% of diabetics and calcification may also indicate a foot or ankle at risk. The purpose of this study was to evaluate toe pressures (TP) in patients who presented with radiographic calcification of vessels in the foot and ankle and determine if adequate flow existed despite the calcification.
Methods: Using a Diabetic Registry from January, 2011 through February, 2021, a retrospective review was used to identify patients who presented with x-ray calcifications of the foot and ankle and was compared to patients who had undergone TP. For the purpose of this study, the findings of Vitti et al., who demonstrated that no surgical failures occurred in patients with TP >68 mm Hg, were used to stratify patients as having adequate (68 mm Hg) or a compromised (<68 mm Hg) blood flow to the foot. The patients' age, body mass index (BMI), hemoglobin A1C, smoking history, use of insulin, whether they could adequately detect a 5.07 monofilament and whether they had adequate TP were all recorded.
Results: A total of 43 patients were identified with radiographic calcification of the foot and ankle. Within this population the average age was 68.1 years (45-89), the average BMI was 30. 8 (18.4-51.1), with an average A1C of 7.7 (5.5-14.2). Three patients (7%) were smokers. Eighteen patients (42%) could adequately detect a 5.07 monofilament and only 20 patients (47%) were on insulin. A TP evaluation was performed on a total of 53 patients. A total of 13 patients who had calcification of the vessels and who had TP evaluations were identified. Within this group, 11 patients demonstrated TP values > 68 mm Hg with only 2 patients demonstrating compromised TP.
Conclusion: Calcification of vessels in the foot and ankle has been stated to suggest vascular compromise and indicate a foot and ankle at risk. These patients are obese, older individuals with poor glycemic control who, for the most part, are neuropathic. However, in this small study group, patients who had calcification of their vessels and had TP, demonstrated that despite the calcifications, adequate blood flow was achieved into the foot. This may indicate that combined with improved glycemic control, patients can undergo elective or semi-elective surgical procedures with adequate healing rates expected.
DOI: 10.1177/2473011421S00239
Comparison of Clinical Results Between Locking Plate Fixation and Screw Fixation for Intra-Articular Calcaneal Fractures
Naohiro Hio, MD, PhD; Masanori Taki, MD, PhD
Category: Trauma; Hindfoot
Keywords: Calcaneus Fractures - Treatment; Internal Fixation; Sinus Tarsi Approach
Introduction/Purpose: The purpose of this study is to compare the results of the two fixation groups for intra-articular calcaneal fractures based on the hypothesis that the locking plate group (P-group) can have a less corrective loss but smaller range of motion due to soft tissue contracture than the screw alone group (S-group).
Methods: P-group included ten feet, five feet of which were categorized as Sanders classification type 2, four as type 3, one as type 4. S-group included 11 feet, nine as type 2, two as type 3. In both groups, small incisions such as sinus tarsi approach were used, and P-group was fixed with a locking plate, and canulated cancellous screws if necessary, while S-group was fixed with canulated cancellous screws only. We assessed range of motion of the ankle joint and subtalar joint, Creighton-Nebraska scale (CN scale) and pre- and postoperative width and height of the calcaneal body and step of subtalar joint surface.
Results: The mean postoperative range of motion in the P-group / S-group was 15°/46.2° / 13.2°/45.9° for ankle dorsiflexion/plantarflexion, and 5°/13° / 5.5°/16° for subtalar joint eversion/inversion, respectively. The mean postoperative clinical score was 89.8+-9.5 points / 93.9+-8.0 points on the CN scale, and the mean pre- and postoperative imaging evaluation showed improvements in the mean width from 120.7+-8.9% to 107+-6.7% / 122.6+-13.4% to 112.9+-10.7%, in the mean height from 88.7+-4.6% to 97.8+-3.3% / 88.3+-5.8% to 99.4+-5.3%, and in the mean step of subtalar joint surface from 6.2+-5.3 mm to 0.7+-1.1 mm / 10.5+-7.6 mm to 1.5+-2.5 mm. As complications, peroneal tendinopathy and transient peroneal neuropathy were observed in one case each in the both groups.
Conclusion: There was no significant difference between the two groups in the corrective loss and postoperative range of motion.
DOI: 10.1177/2473011421S00240
A Detailed Analysis of Workplace Foot and Ankle Injuries
Caroline P. Hoch; Alexander Caughman; Adam Griffith; Caroline P. Hoch; James C. Rex; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Introduction/Purpose: In 2018 over 96,000 foot and ankle injuries resulted in lost workdays. The average 2017-2018 workers compensation claim for ankle injuries was $17,210 for medical costs with an additional $13,276 of indemnity. Workplace foot injuries were similarly expensive, averaging $15,762 in medical costs and $11,866 in indemnity. These costs highlight the burden workplace foot and ankle injuries place on both workers and employers. This study analyzes the incidence, rate, and days lost from work due to foot and ankle injuries across different industries, age groups, and genders and compares these findings to other musculoskeletal injuries. These findings will help us better understand which industries are greater impacted by foot and ankle injuries and what factors may influence the occurrence and severity of these injuries.
Methods: Workplace injury data was obtained using a special query from the Bureau of Labor Statistics Workplace Injuries and Illnesses Nonfatal Cases Involving Days Away From Work: Selected Characteristics database. Data included injury incidence, incidence rate per 10,000 workers, and median days missed from work due to injury. The data was grouped by injury location (all injuries, ankle injuries, and foot injuries), type of injury (fracture, sprain, amputation), and industry. Spearman correlation, one-way ANOVA, and independent samples t-test were used to identify the industries, sex, and ages associated with the highest rates and median days missed from work for each of these groups. Regression analysis was used to analyze changes in incidence rate over time. Incidence rate data was obtained for a seventeen-year period (2003-2019) and days lost from work data was obtained for a nine-year period (2011-2019). Data analysis was performed using SPSS statistics software, version 25.0.
Results: The mining (44.85 foot,17.09 ankle), transportation/warehousing (16.82,16.29), and utilities (24.41,26.69) industries had three of the five highest average median days missed from work for both foot and ankle injuries. Of these, only transportation/warehousing (11.06,13.80) was among the five industries with the highest rates of foot and ankle injuries. There was a strong negative correlation (P<0.001) between age and rate of both foot and ankle injuries and a strong positive correlation (P<0.001) between age and median days missed from work. Males had significantly higher rates of foot injuries (5.31) than females (3.80; P<.0001). Males also had higher rates of ankle injuries (4.96) than females (4.88; P=.453). Regression analysis showed the incidence rate of ankle sprains, ankle fractures, foot sprains, and foot fractures decreased from 2003-2019.
Conclusion: This study demonstrates that the incidence rate and severity of workplace foot and ankle injuries are influenced by workers' age, gender, and the industry they work in. It shows that industries with higher days missed often did not have higher rates of injuries. Our results have the potential to be used to identify industries in need of additional safeguards to protect workers from injury and provide companies with information about the industry norm for rates of employee injuries and days missed from work for these injuries.
DOI: 10.1177/2473011421S00241
Assessing the Influence of Pain and Resiliency Scores on Post-Operative Outcomes
Caroline P. Hoch; Jonathan R. Pire; Jonathan R. Pire; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Introduction/Purpose: Resilience is defined as the ability to recover after stressful events and has been shown to correlate with surgical outcomes across multiple fields. To date, there has been minimal research on the impact of patient resiliency on outcomes of foot and ankle surgery. Thus, this study aimed to look for an association between resilience, as measured by the Brief Resilience Scale (BRS); pain, as measured by the Pain Disability Index (PDI) and Pain Catastrophizing Scale (PCS); and post-operative outcomes after foot and ankle surgery.
Methods: At a single academic medical center, a retrospective review of prospectively collected data was conducted on orthopaedic foot and ankle (n=201) and podiatric (n=7) patients who completed a pre-operative BRS and underwent surgery between 2019 and 2020 (N=208). The cohort consisted of 46 post-operative opioid users and 162 non-users. Data collected included demographics, comorbidities, diagnoses, procedure (i.e., removal of implant=22, Brostrom=15, tenolysis of flexor or extensor tendons=11, 1st MTP fusion=11, cheilectomy=10, etc.), PDI and PCS scores, complications, outcome markers, and pre- and post-operative opioid and benzodiazepine use. Data was analyzed with one-way ANOVA and linear and multivariate regressions formulated by SPSS software.
Results: The PDI score significantly correlated with post-operative benzodiazepine (p=.011) and opioid use (p=.006), the BRS score significantly correlated with post-operative benzodiazepine use (p=.007), and the PCS score significantly correlated with longer length of follow-up (p=.011). Pre-operative opioid use was associated with an increased rate of 30-day readmission (users=6.52%, non-users=2.47%; p<.001). The multiple regression analysis indicated that the BRS score remained significantly correlated to post-operative benzodiazepine use (p=.004). Results of the multiple regression analysis also indicated that higher PCS scores were significantly correlated with increased rates of 30-day readmission (p=.047) and longer length of follow-up (p=.005). No outcome measure was significantly correlated with PDI score, according to the multiple regression analysis.
Conclusion: In conclusion, the PCS was not shown to be an effective tool for measuring post-operative outcomes in orthopaedic foot and ankle patients, despite evidence of the contrary in other fields of orthopaedics. Additionally, the BRS and PDI were only valuable in their association with post-operative narcotic usage. Pre-operative opioid use was shown to correlate with worse higher rates of readmission and limited follow up, as corroborated by numerous previous studies. This study did not find the BRS, PDI, or PCS as useful indicators of surgical outcomes in foot and ankle patients.
DOI: 10.1177/2473011421S00242
Does Medicaid Expansion Improve Access to Care for Ankle Sprains?
Caroline P. Hoch; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Category: Ankle; Sports; Other
Keywords: Affordable Care Act; Health Care; Ankle Sprain
Introduction/Purpose: Prior research has found Medicaid patients face greater difficulty scheduling appointments with orthopaedic surgeons compared to those with other insurance. Recently, a number of states have expanded Medicaid coverage as part of the affordable care act, although it is unclear how this expansion impacts the ability of these patients to obtain access to orthopaedic surgeons. We questioned whether Medicaid patients face additional barriers to care for treatment of ankle sprains, an extremely common athletic injury. Our goal was to determine whether individual state Medicaid expansion status, as well as type of insurance accepted, affected access to care for ankle sprains.
Methods: Four pairs of Medicaid expanded (Kentucky, Louisiana, Iowa, Arizona) and unexpanded (North Carolina, Alabama, Wisconsin, Texas) states in similar geographic locations were chosen. Twelve foot and ankle practices from each state (N=96) were randomly selected from the American Orthopaedic Foot & Ankle Society directory. Each clinic was called twice to request an appointment for a fictitious 16-year-old with a first-time ankle sprain with either in-state Medicaid insurance or Blue Cross Blue Shield (BCBS) private insurance.
Results: An appointment was obtained at 63 (65.6%) clinics when calling with BCBS and 44 (45.8%) clinics with Medicaid (P=.006). There was a significant difference in appointment scheduling based on insurance status in Medicaid unexpanded states (Medicaid=21, 43.8% vs. BCBS=34, 70.8%; P=.007). However, this difference was not significant in Medicaid expanded states (Medicaid=23, 47.9% vs. BCBS=29, 60.4%; P=.219). In addition, in all states except Iowa, a Medicaid expanded state, more appointments were scheduled using BCBS than Medicaid. The three most common reasons for appointment denial were inability to provide an insurance identification number (47.1%), insurance status (23.5%), and lack of referral (17.6%). The waiting period for an appointment was not significantly different depending on insurance status or Medicaid expansion status (Medicaid=3.30 days, BCBS=3.43 days, P=.152).
Conclusion: For patients with first-time ankle sprains, access to care is more difficult using Medicaid insurance rather than private insurance, especially in Medicaid unexpanded states. However, when granted an appointment, Medicaid patients waited a comparable amount of time to the appointment as those using private insurance.
DOI: 10.1177/2473011421S00243
Effect of Preoperative Ulceration on Outcomes of Tibiotalocalcaneal Arthrodesis
Caroline P. Hoch; William Newton; William Newton; Christopher E. Gross, MD; Daniel J. Scott, MD, MBA
Introduction/Purpose: Tibiotalocalcaneal (TTC) arthrodesis is commonly performed for complex deformity, arthritis, or unstable Charcot about the hindfoot. In patients with neuropathy, hindfoot deformity, and preoperative hindfoot ulceration, management options can be limited and very challenging. Previously, some authors have advocated for fine wire circular frames and avoidance of internal fixation in an effort to decrease the risk of infection in patients with preoperative ulceration, however, there is very limited data on the outcomes of TTC arthrodesis with internal fixation in this patient population. We hypothesized that internal fixation of TTC arthrodesis in patients with preoperative ulceration would lead to higher infection rates compared to patients without ulceration.
Methods: A retrospective review was conducted on the TTC fusions performed from 2016-2020 by a single fellowship trained foot and ankle surgeon at an academic medical center. Preoperative diagnosis and indications, fixation method, clinical success, and complications were obtained from the patients' charts. Patients were excluded if their clinical or radiographic data were unavailable for review, or if they had less than 3 months of follow-up. 34 patients (34 ankles) underwent TTC arthrodesis Mean age was 60.7 years and mean follow-up was 1.3 years. Statistical analysis was performed using t-Student and Chi-squared tests with a p-value of 0.05 defining significance. Midline tibiotalar angle (MTA) was measured before and after surgery to assess position of fusion. Nine patients had preoperative ulcers at the time of surgery.
Results: Common surgical indications included Charcot neuropathy (n=17), post-traumatic (n=14), and cavovarus (n=3). All patients with preoperative ulcers underwent TTC fusion with an intermedullary rod. Of the patients without ulceration, 18 underwent intermedullary nailing, 5 underwent plating, and 1 had an external fixator placed. There was no difference in deep wound infection rates between patients with (2/9, 22.2%) and without (2/25, 8.0%; p=.386) preoperative ulceration; nor was there a difference in rate of fusion, wound healing, or radiographic alignment. One patient without preoperative ulceration underwent a below knee amputation due to infection.
Conclusion: TTC arthrodesis with internal fixation appears to be a reasonable consideration in patients with a preoperative hindfoot ulcer. There was no statistical difference in infection rate in patients undergoing TTC fusion with and without preoperative ulceration. Further, the rate of infection in those with an ulcer and internal fixation was acceptable, and internal fixation can be considered in these patients.
DOI: 10.1177/2473011421S00244
Increased Complication Rate Associated with Podiatric Surgery
Caroline P. Hoch; Daniel J. Scott, MD, MBA; Daniel L. Brinton; Lizmarie Maldonado; Christopher E. Gross, MD
Introduction/Purpose: Nationally, there has been an increase in the scope of practice between orthopaedic surgeons and podiatrists. However, there is a paucity of studies in the literature comparing outcomes between orthopaedic and podiatric surgeons in different areas of foot and ankle surgery.
Methods: A retrospective analysis was conducted using 2016-2017 5% US national sample of the Medicare limited dataset (LDS). This included a total of 527 patients undergoing one of 14 CPT foot and ankle specific codes. Basic demographics, medical comorbidities, and 1-year post-surgical complications were reviewed. One-hundred and eighteen patients were operated on by a podiatrist versus 409 who were operated on by a physician. Mean age was 69. Common procedures included gastrocnemius recession (n=168), ankle fracture open reduction internal fixation (168), and Achilles tendon repair (72). Continuous variables were compared using Wilcoxon-Mann Whitney test and categorical variables with chi-squared test. In addition, a multivariable regression was performed, evaluating the impact of various factors on odds of complication.
Results: Between cohorts, there were no statistically significant differences in demographics, Charlson Score, COPD, hypothyroidism, hypertension, or obesity. There was a higher rate of peripheral vascular disease in patients treated by a podiatrist versus a physician (8.5% vs. 2.4%; P=.0025). Univariate analysis showed complication rates were higher among podiatrist compared to physicians (29.7% vs. 18.8%; P=.0113). Specifically, there were high rates of complications for bunion correction (4.2% vs. 1.0%; P=.0160), diabetic wound infection (11.0% vs. 1.5%; P<0.0001), and plantar fascia release (7.6% vs. 0.1%; P=.0001). Multivariable logistic regression showed patients operated on by a podiatrist had 84.1% greater odds of suffering a complication than those operated on by a physician (OR: 1.84, 95% CI: 1.15-2.96).
Conclusion: Surgical treatment of multiple types of foot and ankle conditions by orthopaedic surgeons was associated with lower complication rates when compared with podiatrists. The reasons for these differences are likely multifactorial, but warrants further investigation. Our findings have important implications for policymakers, as well as for large healthcare systems and patients when selecting a treating provider for surgical problems.
DOI: 10.1177/2473011421S00245
Radiographic Characterization of Midfoot and Transverse Tarsal Joint Osteoarthritis
Caroline P. Hoch; Alexander Caughman; David E. Baxley; Katherine M. McGurk; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Category: Ankle Arthritis; Midfoot/Forefoot
Keywords: CT; Midfoot; Nonoperative
Introduction/Purpose: Midfoot osteoarthritis affects over 16% of adults over the age of 50, interfering with activities of daily living and leisure. Non-operative management includes anti-inflammatory, carbon fiber shank/custom orthotics, and cortico-steroid injections. To improve accuracy, these injections are often done under fluoroscopic guidance. Operative intervention with midfoot fusions is sometimes performed, though non-union rates and continued pain after surgery can be challenging. Sometimes, there can be difficulty in determining exactly which midfoot joints are most arthritic/symptomatic based on radiographs. This study aims to quantify how well surgeons are able to diagnose midfoot and transverse tarsal joint arthritis on standing radiographs versus advanced imaging.
Methods: We reviewed the records of 113 patients (144 feet) with midfoot arthritis, who were treated from 2015 to 2019 at an academic medical center by a single fellowship trained foot and ankle surgeon. The mean age was 63.0 years, the average BMI was 31.5, and 7 patients eventually underwent surgery. Each patient underwent both plain radiographs, according to a standardized protocol, and either a CT or MRI scan. Radiographs and advanced images were graded separately for the presence of joint space narrowing, subchondral cysts, and other signs of arthritis in the following joints: 1st tarsometatarsal (TMT), 2nd TMT, 3rd TMT, 4th TMT, 5th TMT, naviculocuneiforms (NC), talonavicular (TN), calcaneocuboid (CC), subtalar (ST), and 1st metatarsophalangeal (MTP). The sensitivity, specificity, precision, negative predictive value, and overall accuracy of radiographs compared to CT scans was calculated for each joint. Statistical significance was assessed using a paired t-test.
Results: The most common joints affected by arthritis were the 2nd TMT (radiograph=75.7%, CT=79.9%) and 3rd TMT (radiograph=65.5%, CT=70.4%). Advanced imaging showed a significantly higher rate of arthritis in the 1st TMT (P<0.01), 4th TMT (P<0.01), and 5th TMT (P<0.01), as compared to radiograph. Only 16.9% of patients' radiographs had a direct correlation with the results of their CT scan. A CT scan showed one or two additional affected joints by 19.7% and 13.0 %, respectively; and rarely showed one or two less joints affected by arthritis (8.1% and 3.2%, respectively). We found radiographic sensitivity and specificity to be highly variable (1st TMT=61.3% & 92.3%, 3rd TMT=79.5% & 69.3%).
Conclusion: Radiographs vary drastically in their sensitivities and specificities in diagnosing arthritic joints in the midfoot and transverse tarsal joints. When treating midfoot osteoarthritis surgically, we recommend obtaining advanced imaging preoperatively, rather than relying on plain radiographs alone to determine which joints may need to be managed surgically.
DOI: 10.1177/2473011421S00246
Risks of Preoperative Opioid Therapy on Ankle Surgery Success
Caroline P. Hoch; William Newton; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Category: Ankle; Hindfoot
Keywords: Preoperative risk factors; Total Ankle Arthroplasty; Hindfoot Fusion
Introduction/Purpose: Past studies have found that preoperative chronic opioid therapy correlates with increased opioid use post-operatively as well as potentially worse surgical outcomes; however, these trends have not been extensively studied in cases of hindfoot fusions or ankle replacement (TAA). Therefore, we aimed to fill this gap in the research and understand the relationship between preoperative opioid use and postoperative success in order to improve patient outcomes. We hypothesized that patients with chronic opioid use prior to surgery would have increased likelihood of postoperative opioid use, complications, and re-operation.
Methods: A retrospective review was conducted of ankle (AA), talo-navicular (TN), and tibio-talo-calcaneal (TTC) fusions, as well as TAAs from December 2014-August 2020 by a single fellowship trained foot and ankle surgeon. Pre- and postoperative opioid and other analgesic use, medical history, demographics, and surgical outcomes were reviewed. Statistical analysis was preformed using correlation, linear multivariate regression, independent-samples t-test, and one-way ANOVA. One-hundred and fifty-two patients (female=66, male=86) with mean BMI of 31.7 and mean follow-up of 1.35 years were included. Thirty-nine underwent isolated AA, 28 TTC, 85 TAA, 9 TAA + other hindfoot fusions, 1 pan-talar fusion, and 1 TN + ankle fusion. Seventeen had a history of substance abuse (i.e., EtOH, opioids, benzodiazepines, other substances). Records of preoperative opioid use were limited to 93 patients, 90-day postoperative opioid use to 81 patients, and 120-day postoperative opioid use to 73 patients.
Results: Preoperative opioid use was significantly associated with reoperation rate (P=.027) and continued postoperative opioid use at 90 (P<.001) and 120 days (P<.001). Preoperative benzodiazepine use was significantly associated with continued postoperative benzodiazepine use at 90 (P<.001) and 120 days (P<.001). There was no significant difference in postoperative opioid use, complications, or reoperation rate between substance abusers and other patients. Female sex (P=.029) and BMI (P=.013) were significant predictors of postoperative opioid use. Of comorbidities, mental illness was a significant predictor of postoperative opioid use (P=.022); substance abuse history (P=.006) and mental illness (P=.001) were significant predictors of postoperative benzodiazepine use. In addition, postoperative opioid use significantly differed by surgery type (fusion=64.5 MME, TAA=28.0 MME, TAA + fusion=859.6 MME; P<.001), but postoperative benzodiazepine use did not.
Conclusion: We found that patients with pre-operative opioid use have statically significantly higher rates of re-operation and continued post-operative opioid use. We also found that on average, patients undergoing hindfoot fusion require statically significantly more narcotics than those undergoing total ankle arthroplasty. Patients and surgeons should be aware of this data to help appropriately council patients on post-operative expectations.
DOI: 10.1177/2473011421S00247
Vancomycin Powder Associated with Decreased Surgical Site Infections in Lower Extremity Trauma
Caroline P. Hoch; Christopher L. Robinson, BS; Christopher L. Robinson, BS; Alex Rovner, BA; Raines M. Waggett, BS; Ryan Horn, MD; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Introduction/Purpose: The use of intraoperative topical vancomycin powder has recently increased in popularity as a method of theoretically decreasing post-operative surgical site infections; however, there is limited research in orthopaedic trauma to support its use. This study evaluates the use of topical vancomycin powder to decrease post-operative infections following lower extremity trauma. We also investigated socio-demographic factors and medical comorbidities that were associated with post- operative surgical site infections.
Methods: We conducted a review of 226 patients at a single Level 1 Trauma Center following surgery between the years 2015 and 2020. These patients were treated predominantly by a single fellowship trained foot and ankle orthopaedic surgeon. Demographic factors, medical comorbidities, postoperative infections, and use of vancomycin powder were reviewed. Analysis of 4 groups (no infection, superficial infection, deep infection, or both) was performed using Fischer’s exact test and Student t-test. A logistic regression model was utilized to identify independent demographic factors and medical comorbidities that were associated with surgical site infection.
Results: The final cohort included 221 patients, of which 26 received intraoperative vancomycin powder. There were 23 total post-operative surgical site infections. Of those, 14 infections were superficial, 3 were deep, and 6 were both superficial and deep. All but one of these infections were in patients without vancomycin powder applied. Patients who received intraoperative vancomycin powder were statistically significantly less likely to acquire post-operative surgical site infections than those who did not (1 vs. 22, p=0.031). The one postsurgical site infection with vancomycin use was a deep infection in a patient with chronic kidney disease that had previously undergone three irrigation and debridement surgeries for a gunshot wound. Male sex was the only demographic or comorbidity factor associated with postoperative surgical site infection (p=0.009, OR=4.006).
Conclusion: We found an association between topical vancomycin use and lower likelihood of developing postsurgical wound infections in lower extremity trauma. This is consistent with similar studies in spinal surgery. In contrast to previous studies, we did not find a significant association between medical comorbidities or demographic factors other than male sex and surgical site infection. Future studies should aim to identify which patients would have the greatest reduction of risk for postsurgical wound infections with the use of intraoperative topical vancomycin powder.
DOI: 10.1177/2473011421S00248
Effect of Achilles Tendon Repair on Performance Outcomes Following Return to Play in NCAA Division I Basketball Athletes
Blake H. Hodgens; Rafael A. Sanchez; Joseph S. Geller; Samuel R. Huntley, MD, MPH; Jonathan R. Kaplan, MD; Amiethab A. Aiyer, MD
Category: Sports; Ankle
Keywords: Achilles Tendon Rupture; Basketball; Return to Play
Introduction/Purpose: Achilles tendon ruptures are devastating injuries highly prevalent among athletes. Despite our understanding of the impact of Achilles tendon rupture in professional athletes, and in particular its relationship to basketball, no study has examined the effect of Achilles tendon rupture on performance metrics in National Collegiate Athletic Association (NCAA) Division I basketball players.
Methods: NCAA Division I basketball players who sustained a surgically repaired Achilles tendon rupture between the 2000 and 2019 seasons were identified by systematic evaluation of individual injury reports from the NCAA career statistics and individual school statistics databases. 65 male and 41 female players were identified. Athletes were included if they participated in at least one collegiate season before tearing their Achilles tendon, and at least one season after operative repair. A total of 50 male and 30 female athletes were ultimately included in the analysis. Each injured athlete was matched to a healthy control by conference, position, starter-status at time of injury, class year, and number of games played. Matched controls were healthy players and experienced no significant injuries during their NCAA careers.
Results: Following Achilles tendon rupture and subsequent surgical repair, male athletes played significantly more minutes per game (19.7 vs. 22.6, p=0.017), scored more points per game (6.7 vs 7.9, p=0.024), and had more assists per game (1.4 vs. 1.7, p=0.036), when compared to their pre-injury statistics. The only area of worsened athletic performance following injury was total blocks, which significantly decreased post-injury (18.1 vs. 10.2, p=0.004). Matched healthy controls demonstrated a higher percent change in assists per game (+39.0% vs +21.8%, p=0.036) and total blocks (+55.1% vs -43.5%, p=0.031) between the matched pre- injury and post-injury periods. Female athletes scored significantly more points per game after returning from injury (7.6 vs 6.3, p=0.032) but demonstrated a significantly lower 3-point shooting percentage (10% vs. 20%, p=0.047).
Conclusion: Male athletes who returned to play following Achilles tendon rupture demonstrated significant increases in various offensive performance metrics, while suffering a significant decrease in total blocks. Female athletes demonstrated a significant improvement in points per game following Achilles tendon rupture, but suffered a significant decline in 3-point shooting percentage. Despite suffering an Achilles tendon rupture, 14% of the male cohort reached the NBA, and 16.7% of the female cohort reached the WNBA.
DOI: 10.1177/2473011421S00249
Radiographic Evaluation of Isolated Continuous Compression Staples for Akin Osteotomy Fixation
Kevin Horner; Kyle Fiala, DPM; Benjamin Summerhays, DPM; Kyle M. Schweser, MD
Category: Bunion; Other
Keywords: Osteotomies; Staples; Clinical Outcomes
Introduction/Purpose: The use of continuous compression implants (nitinol staples) in orthopaedic surgery has increased secondary to advances in metal alloy engineering. Biomechanical studies provide useful data supporting the theoretical use of nitinol staples in the foot and ankle. However, clinical data is limited. The purpose of this study was to determine the overall effectiveness, both clinically and radiographically, of continuous compression implants (nitinol staples) to achieve bony healing in the medially based, closing-wedge osteotomy of the proximal phalanx of the great toe (Akin osteotomy).
Methods: A retrospective chart review was performed on 104 patients (107 feet) who underwent an Akin osteotomy using nitinol staples between January 1st, 2018 and February 20th, 2020. The primary outcome variable was radiographic evidence of healing on x-ray. X-rays were independently reviewed by three board-certified foot and ankle surgeons. All investigators were blinded towards the x-rays, and x-rays were randomized in terms of timing from surgery. Each investigator reviewed digital radiographs independently and recorded their radiographic finding responses. Osteotomies were deemed healed if greater than 50% of the osteotomy contained bridging bone. A partially healed osteotomy was defined as some bridging bone, but less than 50% of the overall osteotomy site, and a nonunion was defined as no healing seen radiographically, broken hardware, or loss of reduction.
Results: Radiographic union (partial or full) was seen in 95% of Akin osteotomies (96/101) based on our parameters, with no loss of initial reduction. Only 2.8% (3/107) of the patient population had unplanned return to the operating room for reasons associated with the Akin osteotomy: one infection (0.9%), one irritable hardware removal (0.9%), and one traumatic disruption of fixation (0.9%). None of the eligible staples (0/106) were found to be fractured upon radiographic analysis. Smokers and diabetics represented 4.8 and 8.7 percent of the patient population, respectively.
Conclusion: Since its inception in 1925, the Akin osteotomy has been described using several types of fixation methods. The results of this retrospective study show that continuous compression implants (nitinol staples) are a viable option for Akin osteotomy fixation, with low rates of complications (2.8%, 3/107) and high healing rates (95%, 96/101). Staples are lower profile, eliminating hardware irritation and potential secondary surgeries, are technically less demanding, and time of application is decreased when compared to other fixation methods. They offer the benefit of continuous compression of the fusion site, as well, and are rigid enough to maintain reduction.
DOI: 10.1177/2473011421S00250
Chopart Fractures and Dislocations: Case Series and New Algorithm of Treatment
Maximiliano Hube, MD; Gonzalo F. Bastias, MD; Felipe Amoedo; Matias Harmat; Camilo Piga, MD; Patricio A. Fuentes
Category: Trauma
Keywords: Midfoot; Trauma; Midfoot arthrodesis
Introduction/Purpose: Chopart fractures and dislocations are one of the most commonly overlooked injuries of the foot. These injuries are still challenging in both diagnosis and treatment and result in a high degree of long-term disability. Recent studies have shown that around 30 to 40% of these injuries are not adequately diagnosed on first consultation, mainly because of their low incidence and high clinical variability/spectrum of injuries. Anatomical reduction of Chopart injuries seems to be the most important prognostic factor of functional outcomes. However, there is still no consensus or clear evidence-based guidelines on the management of these types of injuries. We report the result of our current management protocol and propose a new algorithm of management of Chopart Injuries.
Methods: We present a case series of patients with Chopart fractures and fracture-dislocations admitted to a Level 1 Trauma center between March 2015 and April 2020. Demographic data, mechanism of injury, treatment and complications were obtained from clinical records. Classification of injuries according to Zwipp was performed. Standardized surgical management was performed in 1 or 2 stages, according to soft tissue status. Open reduction and internal fixation of associated fractures of the talus, navicular, calcaneus and cuboid was performed. In cases of severe articular comminution or presence of medial and/or lateral instability, transarticular bridge plating was indicated. Postoperative radiological assessment was performed with X-rays and CT scan. Outcomes were determined using the American Orthopaedic Foot & Ankle Society midfoot score (AOFAS), visual analogue scale (VAS), foot and ankle ability measure (FAAM) and the 12-item Short Form Survey (SF-12).
Results: Thirty four patients (12 women) were included in this study with a mean age of 37 years. Mechanisms of injury were: motor vehicle accidents (n=12), low energy midfoot torsion (n=12), crushing injuries (n=7), fall from height (n=2) and firearm injury (n=1). Mean follow up was 39 months (ranging from 8 to 71 months). The mean AOFAS score 84.8 (SD 12.9), mean FAAM of 84.4% (SD 15.4) and mean VAS score was 3/10. In terms of quality of life, the SF-12 physical component score was 43.59 (SD 9.3), with a mental component score of 51.98 (SD 12.1). Secondary procedures included: hardware removal (n=23), midfoot fusion (n=3) and skin coverage procedures by plastic surgery (n=5).
Conclusion: In this case series, a standardized strategy for the treatment of Chopart injuries including the use of external fixation, ORIF and transarticular plating is presented. Reestablishment of joint alignment of both columns (medial and lateral) is crucial to obtain acceptable functional outcomes. Transarticular fixation is a useful alternative to post-reduction residual instability and bridging of fractures with periarticular comminution. Functional and quality of life results on this series were acceptable and comparable to previous reports at minimum one year follow up. Long-term follow up is needed to further validate the proposed algorithm.
DOI: 10.1177/2473011421S00251
Effect of Medial Ligament Reconstruction in Flatfoot Deformity: How It Affects the Soft Tissue Improvement and Radiological Outcome of the Surgery?
Helen Huetteman; Seyed Alireza Mirghasemi, MBBS; Matthew S. Lipphardt; Stephanie Mrowczynski; Allan M. Grant, MD; Zachary M. Vaupel, MD; Paul T. Fortin, MD
Introduction/Purpose: Surgical treatment of adult flatfoot deformity has traditionally be driven by tendon transfers and osteotomy. In acquired deformity, injury to the spring ligament and superficial deltoid ligament is common. The procedures mentioned previously do nothing to restore the function of the medial ligament complex. Studies have shown that reconstruction of the medial ligament complex, and thus the medial talonavicular joint, has benefit to patient outcomes. The question still remains of how much correction the medial ligament reconstruction confers on its own. The purpose of this study is to compare isolated medial ligament reconstruction procedures to other flat foot correcting procedures in the treatment of acquired flat foot deformity.
Methods: 18 patients were identified that underwent procedure for flatfoot deformity. Of these patients there were 7 patients that underwent isolated medial ligament complex reconstruction and 11 patients that underwent non-tendon transfer procedure for correction of flat foot deformity. Imaging was performed on patient’s weight bearing (WB) and non-weight bearing (NWB) before and after surgery. Measurements included Angles: calcaneal pitch, talo-1st metatarsal, talocalcaneal, talar declination, calcaneal 1st metatarsal and Distances: talar height, navicular height, 1st cuneiform height, cuboid height, and 1st to 5th metatarsal distance in lateral X-ray, and Angles: talonavicular coverage, talar 1st metatarsal, talar 2nd metatarsal and Distances: talonavicular uncoverage distance in AP. The differences in measurement between the pre-op and post-op non-weight bearing are considered as bony correction effect while differences between pre-op and post-op weight bearingare considered as soft tissue correction
Results: For non-weight bearing; medial ligament reconstruction impact was seen on calcaneal pitch (19 to 35 degrees, p=0.007), 1st cuneiform height (21 to 28mm, p=0.016), talonavicular coverage (6 to 3 degrees, p=0.026), and Talar 1st metatarsal angle (14 to 7 degrees, p=0.008). Other corrections had an impact on calcaneal pitch (15 to 24 degrees, p=0.006), Talo-1st metatarsal angle (11 to 6 degrees, p=0.019), Calcaneal 1st metatarsal (139 to 129 degrees, p=0.044), Talar height (31 to 42mm, p=0.001), navicular height (24 to 34mm, p=0.002), and 1st cuneiform height (18 to 22mm, p=0.016). For weight bearing; reconstruction impact was seen on talocalcaneal angle (36 to 44 degrees, p=0.011), 1st-5thmetatarsal distance (12 to 18mm, p=0.047), and hindfoot moment arm (16 to 6mm, p=0.031). Other corrections had an impact on talar height (34 to 40mm, p=0.028), navicular height (26 to 30mm, p=0.031), cuboid height (p=0.021), and hindfoot alignment angle (17 to 7 degrees, p=0.003).
Conclusion: When compared to procedures that only address bony changes in the foot, it is clear from this study that medial ligament repair plays a different, but significant, role in correction of flat foot deformity. Interestingly, the non-weight bearing and weight bearing results show that medial ligament reconstruction affects different aspects of the correction in these two distinct phases. This study serves to suggest that medial ligament reconstruction has a role in the correction of flat foot deformity that is not completely addressed in the more common procedures performed.
DOI: 10.1177/2473011421S00252
Are Preoperative PROMIS Scores Associated with Postoperative ED Visits?
Austin Hughes; Nicholas A. Andrews; Jared R. Halstrom, BS; Aseel G. Dib, BS; David A. Patch, MD; Whitt Harrelson; Kenneth J. Fellows; James Pate, BS; Sameer Naranje; Ashish Shah, MD
Introduction/Purpose: Preoperative Patient-Reported Outcomes Measurement Information System (PROMIS) scores have been shown to be predictive of postoperative success in orthopedic foot and ankle patients. The purpose of this study was to determine if an association exists between pre-operative PROMIS scores and patients going to the emergency department (ED) in the first 60 days following their operation.
Methods: PROMIS scores, including physical function (PF) and pain inference (PI), were collected from 290 patients prior to foot and ankle procedures. Patients with presence of ongoing infection were excluded. Electronic medical record (EMR) data was retrospectively gathered for each patient to determine if they visited the ED for any reason during the first 60 days following their operation. A Backward Stepwise Logistic Regression analysis was conducted for postoperative ED visits with p<0.1 in univariate analysis required for entry into the model.
Results: The median age was 50.0 with an interquartile range (IQR) of 20.0, while the median BMI was 33.1 with an IQR of 11.6. In univariate analysis, Preoperative PROMIS PF and PI scores were significantly associated with ED visits within the first 60 days after surgery. Patients who visited the ED had lower preoperative PROMIS PF (median 34.9 (IQR 10.2)) and higher PROMIS PI (median 66.9 (IQR 9.1)) compared to patients who did not visit the ED, PROMIS PF (median 38.0 (IQR 10.2)) and PROMIS PI (63.6 (IQR 9.0)), respectively. In multivariate analysis, only PROMIS PF was associated with lower risk of ED visits OR 0.92 (95% CI.85-.99). Other factors independently associated with ED visits included non-traumatic surgical indication OR 3.7 (95% CI 1.1- 12.9), any pulmonary disease OR 4.2 (95% CI 1.4-12.8), ASA classification OR 4.4 (95% CI 1.3-14.9), and wound complications OR 10.2 (95% CI 2.6-39.9).
Conclusion: Patients with lower PROMIS PF scores preoperatively were significantly more likely to visit the ED postoperatively. While all of the factors found to be associated with ED visits are not modifiable by the surgeon, preoperative PROMIS scores could quickly and easily be used to identify patients for potential interventions. This study demonstrates the potential of the PROMIS outcomes system outside of quantifying surgical outcomes. Further study is being conducted to investigate the optimal PROMIS PF cutoff for best identifying patients at risk for ED visits.
DOI: 10.1177/2473011421S00253
Trends in Medicare Physician and Facility Fee Reimbursement in Orthopaedic Foot and Ankle
Clayton Hui; Haroon Kisana; John R. Martin; Chad Stecher; Joshua Hustedt, MD
Introduction/Purpose: The purpose of the study was to examine the trends in physician and facility reimbursement for the orthopaedic foot and ankle subspecialty utilizing the 23 most common foot and ankle surgeries based on national payment amounts.
Methods: The Current Procedural Terminology (CPT) codes and corresponding Medicare Severity - Diagnosis Related Group (MS-DRG) codes for the 23 most common orthopaedic foot and ankle surgeries were identified. With the CPT codes, physician reimbursement was obtained through querying the Medicare Physician Fee Schedule (MPFS) for the work, malpractice, and practice expense relative value units (RVU) and then multiplying the total RVUs by the yearly conversion factor. CPT codes were also utilized to gather hospital outpatient reimbursement data from the Hospital Outpatient Prospective Payment System (OPPS) database. Hospital inpatient reimbursement rates were obtained from the Hospital Inpatient Prospective Payment System (IPPS) database utilizing the MS-DRG codes. All amounts were then adjusted for inflation using the Consumer Price Index (CPI).
Results: From 2008 to 2021, physician reimbursement for the 23 most common orthopaedic foot and ankle surgeries decreased by 20%, with a mean Compound Annual Growth Rate (CAGR) of -1.7%. Hospital inpatient reimbursement increased by 34.7% with a mean CAGR of 2.3%; while outpatient hospital reimbursement increased by 97.2% with a mean CAGR of 5.1%.
Conclusion: Over the past 13 years, physician reimbursement for common orthopaedic foot and ankle surgeries has declined while hospital reimbursement has increased. The larger increase in outpatient reimbursement compared to inpatient reimbursement highlights how CMS aims to transition surgeries from the inpatient setting to the more efficient and less expensive outpatient setting. This downward pressure on physician reimbursement while incentivizing outpatient services could have many unintended consequences on the landscape of foot and ankle practice in the US.
DOI: 10.1177/2473011421S00254
Content Expert Lecturers and Their Related Peer Reviewed Publications: An Analysis of Foot & Ankle Societys' Annual Meetings from 2016 to 2020
Christopher F. Hyer, DPM; Dominick Casciato, DPM; Calvin J. Rushing, DPM; John M. Schuberth, DPM
Introduction/Purpose: Annual national society meetings for the American College of Foot and Ankle Surgeons (ACFAS) and American Orthopaedic Foot & Ankle Society (AOFAS) have long provided an important resource to disseminate the latest innovations, techniques, and research. However, unlike submitted research abstracts which are screened by a selection committee, there are scant guidelines for selected content experts to present educational content. To date, the ability to publish in a peer-reviewed journal bestows the ultimate validity of academic expertise on a particular subject matter and supports the expertise of the clinician. The purpose of this study was to evaluate for the first time, the incidence of scholarly publication in a peer reviewed journal for invited speakers from the ACFAS and AOFAS annual meetings from 2016 to 2020.
Methods: Annual meeting programs for the ACFAS and AOFAS from 2016 to 2020 were compiled by two reviewers. Faculty lists and assigned lecture tract topics from each meeting were entered into password protected databases. Oral and poster abstracts, industry/society sponsored presentations, 'competitions', and 'other events' held during the annual meetings were excluded. Speaker specific variables included: gender, number of peer reviewed journal publications on the assigned subject matter (publications preceding the meetings date), study design, weighted total topic publication citations, and H-index. The weighted total topic publication citations was obtained by dividing the total citation counts for each manuscript on a particular subject by the number of years since its publication. The H-index, an author specific metric of both productivity and citation impact was obtained from searches of an online resource (http://www.scopus.com/freelookup). For the purposes of the present study, only foot and ankle surgeons (DPM, MD, DO) were included for assessment.
Results: There were a total 1,028 invited presentations combined between AOFAS (158) and ACFAS (870) at the annual meetings fom 2016-2020. With combined data, 724 (70%) presentations were given by speakers with no publications in the subject matter while 300 (29.2%) were given by speakers with one or more publications. Lecture topics that had the highest percentage of speakers with publications in the subject matter included Wound Care/Limb Salvage (82.8%), Charcot (63.6%) and Total Ankle Replacement/Fusions (50%). Topics with the highest number of speakers without publications on the topic included Trauma (84%), Sports (80.3%) and Forefoot Elective (78.7%). Only the Trauma category of speakers had a statistically significant difference of predicted number of lectures by publication between no publications (3.7 lectures) and those with 1 or more publications (1.6 lecture) with p=0.04.
Conclusion: Content expert presentations at national society specialty meetings are a crucial source of continuing education. What makes a speaker a content expert has yet to be defined but is important to consider. Perhaps factors such as peer reviewed publications in subject matter or the speaker’s H-index are characteristics to consider in selecting content experts. In our survey of ACFAS and AOFAS annual meetings from 2016-2020, there were many topics were the vast majority of lectures were given by speakers without any publications and dispersed across the spectrum regardless of the speaker’s H-Index ranking. Further criteria development is likely needed.
DOI: 10.1177/2473011421S00255
Coronal Plane Deformity and Total Ankle Replacement: When to Stage with Cement Spacer Ankle Arthroplasty for Deformity Correction
Christopher F. Hyer, DPM; Antonio M. Malloy McCoy; John M. Thompson; Mitchell Thompson; Devon Consul, DPM
Introduction/Purpose: Degenerative ankle joint disease is a debilitating condition that causes significant pain, adversely affects function and quality of life. Though primary arthritis of the ankle can occur without deformity, frequently soft tissue imbalances or joint deformities complicate the clinical picture. Often, additional procedures are required to balance the foot and ankle during the index total ankle replacement procedure. When large deformities exist a staged approach to first, align the ankle joint to neutral as stage one and then implantation of the TAR as stage two can be deployed. This paper will further popularize the cement spacer staged TAR technique in correction of coronal deformities, share a clinical algorithm on approach, and depict a case series demonstrating its application.
Methods: A case series was performed of 7 patients and 8 ankles, who underwent staged primary TAR utilizing a cement spacer to assist with deformity correction, between the years 2016-2019.
Results: Patients' mean age 58.5 yrs., preoperative varus coronal plane deformity mean 19.1 degrees, preoperative valgus coronal plane mean 10.25 degrees. Mean time from stage 1 till 2 was 163.5, +-140.2 days. Stage 1 soft tissue procedures: Chrisman-Snook procedure with synthetic ligament graft, Brostrum-Gould with synthetic graft, Brostrum-Gould without graft, FDL transfer, and isolated medial release/peel. Osteotomies performed during stage one: Dwyer, MDCO, Cotton, and MDCO with medial malleolus osteotomy. Fusions performed during stage one consisted: Subtalar joint, talonavicular joint (TNJ), and STJ with 1st Metatarsophalangeal joint (MTPJ). Seven ankles were replaced with Cadence Total Ankle System (Integra), and one with INBONE II (Wright Medical Technology). Average follow-up time for included patients was 290.75 days (9.7 months). One revision was performed following index TAR procedure.
Conclusion: This paper describes a cement wedge spacer staged total ankle arthroplasty technique for correction and stabilization of deforming forces at the ankle joint. While not all ankle deformities necessitate a staged approach, the complexity of the malalignment and the extent of tissue disruption needed to achieve a neutral ankle should be considered when correcting a given deformity with a staged or non-staged approach.
DOI: 10.1177/2473011421S00256
Does a “Spot Weld” with a 1st to 2nd Metatarsal Base Screw Maintain Correction of the Modified Lapidus Procedure? A Retrospective Radiographic Review
Introduction/Purpose: The Lapidus 1st tarsometatarsal (TMT) arthrodesis has gained popularity for its ability to correct large deformities especially in cases of medial column instability. Even with solid fusion, instability between the 1st and 2nd columns can result in loss of intermetatarsal (IM) angle correction over time. Anecdotally, a ’spot weld' between the lateral 1stmetatarsal and medial 2nd metatarsal bases seems to predict long term maintenance of IM correction. The purpose of the study is to review cases of Lapidus 1st TMT arthrodesis with supplemental screw fixation from the 1stto 2nd metatarsal base for maintenance of IM correction and determine whether a ’spot weld' is predictive of maintenance and identify an optimum position of the 1st to 2nd metatarsal screw to achieve the ’spot weld.
Methods: A retrospective radiographic review of cases by a single surgeon over the past five years was performed. All cases of tarsometatarsal fusion were queried and reviewed. Inclusion criteria included primary arthrodesis of the 1st TMT joint with supplemental fixation between the 1st and 2nd metatarsal bases, availability of appropriate radiographic image and at least 4 months follow up. Exclusion criteria included 1st TMT fusion without 1st-2nd metatarsal screw fixation, multiple TMT or midfoot fusion, Charcot neuroarthropathy, and revision fusion. A standard surgical technique was utilized with an in situ joint debridement, specific preparation to the medial 2ndmetatarsal base and adjacent lateral 1st metatarsal base, autogenous bone grafting and hardware construct at the 1stTMT joint consisting of compression screw from the 1st metatarsal to the 2nd cuneiform, screw fixation from 1st to 2ndmetatarsal bases and either locking plate or compression staple fixation dorsally across the 1st TMT joint.
Results: 90 cases (77 patients) met the inclusion criteria with average follow up of 309 days. Fusion of the 1st TMT occurred in 87/90 (96.7%) cases with 76 dorsal plate, 10 with dorsal staple and 4 with all screws. There was no incidence of complications related to the 1-2 screw. The mean pre-operative IM 1-2 angle was 14.90 degrees, with mean correction to 6.22 degrees post operative and final maintained correction at 7.10 degrees with mean loss of 0.87 degrees. There were ’spot welds' in 65/90 (72.2%) with a mean loss of correction of 0.48 degree versus loss of 1.88 degrees in the 'no spot weld' subgroup (p<0.001). Cases with no spot weld and screw lucency lost 2.25 degrees (p<0.001).
Conclusion: Loss of IM 1-2 correction can occur due to instability between the 1st and 2nd columns even in cases of solid 1st TMT arthrodesis. The achievement of a ’spot weld' via careful preparation, bone grafting and use of a 1st to 2nd metatarsal base screw as part of a Lapidus construct was found to maintain correction with minimal loss (0.87 degree) versus cases where no ’spot weld' was achieved. Cases with no ’spot weld' that developed screw lucency had the greatest loss of correction. No statistical difference in screw position between groups was found.
DOI: 10.1177/2473011421S00257
Scope Assisted Ankle Arthrodesis in a Young Male with Hemophilic Arthritis: A Case Study
Christopher F. Hyer, DPM; Antonio M. Malloy McCoy; Kevin N. Nguyen; Devon Consul, DPM
Category: Ankle Arthritis; Arthroscopy
Keywords: Ankle Arthrodesis; Arthroscopy; Ankle
Introduction/Purpose: Arthritis is a debilitating condition that negatively affects an individual’s ability to carry out activities of daily living. While osteoarthritis is a term many have become familiar with, as it is the most common form of arthritis encountered, hemophilic arthritis is a condition not frequently seen or discussed. Hemophilia is a congenital bleeding disorder caused by the absence or decrease of clotting factor VIII (Hemophilia A) or XI (Hemophilia B). When severe, this X-linked disease commonly results in intra-articular bleeding which, can progress to joint destruction1-4. This subsequently leads to the progressive destruction of articular cartilage and bone6-7.
Methods: Arthroscopic assisted ankle arthrodesis with calcaneal autograft was performed. Calcaneal autograft was acquired through a small linear incision along the lateral wall of the calcaneus, a power graft harvester was introduced into the medullary bone to procure the graft. The left lower extremity was then placed into a non-invasive Gould Ankle distraction system and the standard anteromedial and anterolateral ankle scope portals were established. A scope and shaver were utilized to extensively debride all visualized hemorrhagic synovium. The shaver was then exchanged for a burr following debridement to remove the articular cartilage to both the talus and tibia. Following adequate preparation of the joint margins for fusion, the ankle joint was filled with the calcaneal autograft and rhPDGF-BB.
Results: Various treatments have been described for patients suffering from hemophilic arthritis. While the use of clotting factor concentrations (CFCs) may reduce the risk of hemarthrosis, the risk of bleeding cannot be completely avoided2. Arthroscopic or open synovectomies has been described to remove the pathogenic synovium. Chemical or radioisotopic synoviorthesis is an option for less severe cases, but the treatment of choice is joint fusion or arthrodesis for advanced stages of arthropathy3.
Conclusion: In patients with hemophilia, regular replacement therapy with clotting factor concentrates (prophylaxis) is effective in preventing recurrent bleeding episodes into joints and muscles. However, despite this success, intra-articular and intramuscular bleeding is still a major clinical manifestation of the disease. The pathogenesis of hemophilic arthropathy is multifactorial, with changes occurring in the synovium, bone, cartilage, and blood vessels. Our case report presents a unique pathology and the successful outcome that can be accomplished through surgical intervention and a multidisciplinary treatment approach.
DOI: 10.1177/2473011421S00258
Ankle-Hindfoot Reconstruction by Tibiotalocalcaneal (TTC) Arthrodesis Using Multiple Cannulated Screws: 32 Cases
Introduction/Purpose: Tibiotalocalcaneal (TTC) arthrodesis is a salvage procedure that can be used as an alternative to amputation for various pathologic conditions of the ankle-hindfoot. The aim of this study is to evaluate the clinical-radiological outcome of TTC arthrodesis performed using the multiple cannulated screws.
Methods: From 2003 to 2018, 32 ankles (31 patients) underwent TTC arthrodesis. The mean follow-up period was mean 32.5 (12-92) months and the average patient age at surgery was 59.6 years (43-75). The etiologies of TTC arthrodesis included posttraumatic osteoarthritis (18.8%), Charcot arthropathy (18.8%), paralytic deformity (21.9%), failure of total ankle arthroplasty (9.4%), and failure of arthrodesis (9.4%). For all of 32 cases, transfibular approach was used with or without auto fibular cancellous bone graft. 7.3mm cannulated screws were used for fixation of arthodesis for all of 32 cases, and in 23 of 32 cases (71.9%), screw- fixation was used exclusively without any additional plate or Ilizarov fixator. Especially for 11 of 32 cases with large bony defect, fresh-frozen allo-femoral head structural bone graft was used. Pre- and postoperative visual analog scale (VAS) pain, the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot functional score, and radiographs including CT images were assessed.
Results: Overall union rate was 81.3% (26/32). Mean VAS score decreased from 6.92 preoperatively to 1.46 postoperatively and the AOFAS score improved from 27.0 to 53.7 (Max=68) at the final follow-up. Complication of TTC arthrodesis included nonunion (18.8%, 6/32), infection (12.5%, 4/32), and one case of skin necrosis. Most frequent nonunion site was tibiotalar joint (6/32). For 3 of 7 cases with nonunion, patients were painless and could ambulate without severe functional impairment. There were two cases with infective nonunion and one case with active Charcot arthropathy after artrhdesis. Union rate of two groups with/without allo-femoral head bone graft were similar to each other (81.8%, 81.0%, respectively), however, final AOFAS scores were significantly superior in 'without' femoral head bone graft group.
Conclusion: This study achieved a fusion rate comparable to other previous studies and obtained favorable clinical outcomes. Realignment TTC arthrodesis using multiple cannulated screws is a valid surgical option as a salvage procedure for various deformed or arthritic conditions of ankle-hindfoot. Allo-femoral head structural bone graft can be selected as useful option for TTC arthrodesis with large bone defect.
DOI: 10.1177/2473011421S00259
Clinical and Radiological Outcomes of Modified Lapidus Procedures Using 2 Compression Cannulated Screws in Hallux Valgus Deformity
Introduction/Purpose: Hallux valgus is common disease. Surgical correction is usually required because, conservative treatment can not correct deformity and lacks evidence for prevention of progression of deformity. Among the various methods for the correction of hallux valgus deformity, the modified Lapidus procedure is known to be performed in less than 10%. The purpose of this study is to investigate the clinical and radiological outcomes of patients who underwent the modified Lapidus method.
Methods: From January 2010 to December 2019, 34 cases of patients who underwent the modified Lapidus procedure and followed up for at least 6 months were included in the study. For clinical evaluation, VAS score, AOFAS score, and patient satisfaction (very satisfied, satisfied, dissatisfied, very dissatisfied) were used. For radiological evaluation, hallux angle and 1-2 metatarsal angle on anterior and posterior foot x-ray of the weight-bearing were used. Furthermore, rate of bone union and the period until bone union were also evaluated.
Results: The mean follow-up period was 21.0 (6~108) months. The indications for surgery were: Severe hallux valgus in 30 cases, metatarsus adductus in 17 cases, recurrent hallux valgus in 4 cases, and hypermobility of the first tarso-metatarsal joint in 10 cases. In terms of VAS score, between pre-operation and the last follow-up was significantly improved from 5.8+-2.1 to 1.1+-1.4 (p<0.05), and the AOFAS score from 52.8+-15.0 to 92.3+-9.8 (p<0.05). In terms of patient satisfaction, 33 patients (97.1%) showed overall satisfaction (very satisfied and satisfied). Complications were nonunion in 3 cases (8.8%), incomplete union in 1 case, delayed union in 1 case, and hallux varus in 1 case. There was no additional surgery for these complications. At preoperative and last follow-up, the hallux angle improved from 46.0°+-10.7° to 5.9°+-11.7°, and the 1-2 IMA improved from 18.2°+-5.1° to 5.5°+-4.5°. In the cases excluding complications, the average period to bone union was 3.9(3-8) months.
Conclusion: In our study, the modified Lapidus method using 2 compression cannulated screws was showed satisfactory clinical, radiological outcomes and relatively satisfactory bone union (91.2%) in a short follow-up. The modified Lapidus method using 2 compression cannulated screws is a considerable option for severe hallux valgus deformity.
DOI: 10.1177/2473011421S00260
A Scoping Review Regarding the Treatment of Foot and Ankle Ganglia
Adil Iqbal; Zaki Arshad; Sofyan A. Shdefat; Maneesh Bhatia, MBBS, FRCS(Tr&Orth)
Introduction/Purpose: Ganglion cysts are a well documented phenomena occurring in a variety of joints. They are described as a tumour like lesion filled with mucopolysaccharides. The majority occur in the hand and wrist (88%) with a small yet significant minority occurring in the foot and ankle (11%). Currently, there is a lack of high-quality literature regarding the management of ganglia in the foot and ankle region. Therefore this scoping review aims to systematically map and summarise current evidence regarding the management of ganglia of the foot and ankle, whilst identifying areas for further research.
Methods: This scoping review follows the methodology outlined by Arksey and O'Malley, Levac, the Joanna Briggs Institute and PRISMA framework.. A detailed search strategy was used to identify relevant articles using free text terms such as 'foot' 'ankle' 'ganglion' 'ganglia' 'ganglionic cyst'. This was carried out in four electronic databases; PubMed, EMBASE, CINAHL and Ovid MEDLINE. A stage two-stage independent screening process based and title and/or abstract then full-text was carried our by two reviewers. The a-priori selection criteria included all primary research (observational studies and randomised control trials) whilst excluding (case reports, letters to editors, editorials, commentaries and review articles). Studies that did not separate the treatment of foot and ankle tumours from ganglia were excluded. The MINORS criteria were used to assess methodological quality of included studies.
Results: In total, 2286 unique articles were initially identified, from which 11 met the criteria for inclusion. A variety of conservative and surgical treatment strategies were reported. The use of surgical excision was reported in all 11 studies, ten of which via an open surgical approach, with only one study using an endoscopic approach. The use of conservative treatments, involving aspiration and/or steroid injection, were reported in only 5 studies. As for the recurrence rate, 7 studies reported a rate of 5.7% - 65.7%, with an overall pooled recurrence rate of 30.6%. Pooled recurrence rates showed that surgical excisions were associated with a lower recurrence rate than conservative treatments. Complications other than occurrence were described in 6 studies. Only 3 studies performed an analysis of outcomes based on the location or site of origin of ganglia.
Conclusion: The current literature regarding the treatment of foot and ankle ganglia is of a low-quality, as the articles included in this scoping review are level III or IV cohort or case series design. The literature alludes to the idea that a surgical approach provides greater efficacy than a conservative approach. There is also limited evidence to suggest that factors such as the origin or location of ganglia may affect treatment outcomes. Alternative approaches utilised in the treatment of wrist ganglia are yet to be investigated. Further research is required before more definitive conclusions into any such associations may be drawn.
DOI: 10.1177/2473011421S00261
Opioid Usage after Hallux Valgus Correction Surgery
J.B. Jackson, MD; Zachary T. Thier; Matthew E. Barfield, BS; Kenna C. Altobello, APRN; Tyler A. Gonzalez, MD, MBA
Category: Bunion; Other
Keywords: Bunion; Pain; Hallux Valgus
Introduction/Purpose: More than 200,000 surgeries for hallux valgus correction occur annually in the United States. Due to the post-operative pain associated with the procedure, opioids are often prescribed to help manage pain. Given the lack of objective data on opioid use and the difficulty of addressing a patient’s post-operative pain, we sought to quantify, through a prospective analysis, patient’s narcotic use after hallux valgus surgery. The purpose of our study was to determine the average quantity and type of post-operative opioids consumed after hallux valgus surgery and to assess potential predictive factors for increased opioid consumption.
Methods: Adult patients undergoing primary hallux valgus surgery were recruited from two foot and ankle fellowship trained orthopedic surgeons at a single institution. At the pre-operative visit, patients were consented and completed a demographical questionnaire. Data was collected from the operative and PACU record, as well as the 2, 6, and 12-week post-operative visits. A statistical analysis was performed to determine the average quantity of opioid and non-opioid pain medication consumed post- operatively, as well as any statistically significant correlations.
Results: For the 58 subjects who completed treatment and data collection in the PACU, 53 consumed opioids. Initial prescriptions for these patients included Hydrocodone, 39 (73.58%) Oxycodone, 13 (24.52%) and Meperidine, 1 (1.89%). The average number of opioid pills collectively consumed at the two-week and 12-week post-operative visit was 19.99 and 22.52, respectively. At the two-week postoperative visit, only patient BMI showed a statistically significant association with increased opioid use.
Conclusion: On average, patients consumed 22-24 narcotic pain pills after hallux valgus reconstruction surgery. If a physician prescribed 24 narcotics pills after surgery to patients that are not currently utilizing narcotic pain medication, there is a 95% chance they will not need additional pain medication during the two-week postoperative period.
DOI: 10.1177/2473011421S00262
Anterior-Inferior Tibiofibular Ligament Suture-Tape Augmentation for Isolated Syndesmotic Injuries
Marissa D. Jamieson, MD; Alex W. Brady; Kira Tanghe; Thomas O. Clanton, MD; Ingrid Stake
Introduction/Purpose: Aggressive surgical treatment of isolated syndesmotic injuries has recently gained some traction in the media and sports world. New developments in syndesmotic fixation aim to restore native syndesmotic stability and ankle motion with a goal of returning athletes to sport quickly. However, the best surgical technique is debated. Dynamic repair with a suture- button (SB) can provide an accurate reduction of the syndesmotic space but may alter the rotational kinematics of the fibula. Previous studies have suggested that repair or reconstruction of the anterior-inferior tibiofibular ligament (AITFL) may restore the dynamics of the syndesmosis better than other devices. The purpose of this study was to biomechanically compare SB fixation and augmented repair of the AITLF using suture and suture-tape (ST) in isolated syndesmotic injuries.
Methods: Twelve unpaired lower leg specimens underwent biomechanical testing in 6 states: 1) intact, 2) AITFL suture repair alone, 3) AITFL suture repair + ST augmentation, 4) AITFL suture repair + ST augmentation + SB fixation, 5) AITFL suture repair + SB fixation, and 6) complete syndesmotic injury. The testing consisted of subjecting the ankle joint to 6 cycles of 5 Nm internal and external rotation torque under a constant 750 N axial compression load in a dynamic tensile testing machine. A lower level of torque was chosen than in previous studies in order to replicate physiologic motion of everyday activities instead of injury level forces. The spatial relationship between the tibia and fibula and tibia and talus was continuously recorded using a 5-camera motion capture system.
Results: AITLF suture repair and suture repair + ST augmentation repair constructs showed no statistically significant change in fibula kinematics during testing compared to the intact state. The suture repair + SB construct showed increased external rotation of the fibula (p<0.001, mean 2.32 degrees) and medial translation (mean 0.72 mm, p= 0.007) or overtightening compared to the intact state. The suture repair + SB + ST augmentation state also showed increased external rotation of the fibula compared to the intact state (p<0.001). Sagittal plane motion of the fibula was not significantly different in the repair states compared to the intact state. None of the repair states restored talus rotation back to the intact state; however, the repairs that utilized suture tape reduced the talus external rotation laxity compared to the complete syndesmotic injury.
Conclusion: For isolated syndesmotic injuries without significant fibular displacement, augmentation of the AITFL with suture- tape best restored the rotational profile of the fibula and ankle joint. Suture-button constructs had a tendency to over-tighten and externally rotate the fibula when compared to the intact state. Suture-tape AITFL augmentation may be a good surgical option and alternative to suture-button fixation for isolated syndesmotic disruptions. Further clinical trials are needed to determine the role for suture-tape augmentation of the AITLF in syndesmotic injuries.
Introduction/Purpose: The cavovarus foot is a true challenge for both the patient and the surgeon. This complex deformity can be a result of many different causal factors including genetics, Charcot-Marie-Tooth disease, diabetes and spina bifida. It may also be caused or worsened by trauma or surgical procedures. The cavovarus foot is difficult to manage conservatively as it tends to be rigid, is not a good shock absorber and causes the joints of the foot to process abnormal stresses. The mechanical construct of a cavus foot makes it susceptible to a multitude of complications and injuries like inversion ankle sprains and metatarsal stress fractures.
Methods: While foot orthoses would likely be the most commonly considered conservative treatment option for the symptomatic cavus foot, other modalities like shoe modification, bespoke and/or therapeutic footwear and bracing have also proven effective. Oftentimes, a combination of the aforementioned options is employed. Given the individual complexities of each cavus foot, the conservative treatment plan is typically custom tailored to fit a particular patient’s foot structure, biomechanical and corrective needs, and occupational or recreational demands. A so-called 'cookie cutter' approach is not appropriate for management of the cavovarus foot.
Results: A review of published research demonstrates that foot orthoses - and other conservative modalities - are effective in the treatment of the cavus foot. These devices work by correcting the varus foot alignment (when applicable), offloading painful areas such as ball of the foot or the base of the fifth metatarsal, providing shock absorption and replacing lost motion. These applications work together to provide a more normal, safer and energy-efficient gait.
Conclusion: Conservative management, specifically pedorthics, is not only a viable treatment option for the cavovarus foot but should be considered integral to the overall management of the cavus foot patient. Pedorthic modalities are successfully used post-operatively or in lieu of surgical intervention. Modern pedorthics (technological advances in shoe and orthotic design, construction and materials) allows for cosmetically pleasing, affordable and comfortable management allowing patients to return to a healthy and active lifestyle in many cases.
DOI: 10.1177/2473011421S00264
Weight Bearing CT Analysis of the Transverse Tarsal Joint During Eversion and Inversion
Clifford L. Jeng, MD; Nicholas Rowe; Cassandra E. Robertson; Stuti Singh; John T. Campbell, MD
Category: Basic Sciences/Biologics; Hindfoot
Keywords: Biomechanics of the Foot and Ankle; Hindfoot; Weight Bearing CT
Introduction/Purpose: Current understanding of the kinematics of the transverse tarsal joint continues to evolve. Unfortunately, most prior studies have been in cadavers or under non-physiologic conditions. Weight bearing CT scans may provide more accurate in vivo information about the position of the transverse tarsal joint during eversion and inversion.
Methods: Institutional Review Board approval was obtained. Five normal volunteers underwent bilateral weight bearing cone- beam PedCAT scans (CurveBeam LLC, Hatfield, PA) while standing on platforms that positioned both hindfeet in 20o of valgus and then 20o of varus. The CT scans had a field-of-view diameter of 350 mm and a field-of-view height of 200 mm. The scan exposure time was 9 seconds, with a total scan time of 54 seconds. The datasets were reconstructed using filtered back projection with 0.37mm isotropic voxels. The resulting volumes were then segmented, identifying the [x, y, z] coordinates that comprised each bone. Each bone of the hindfoot was segmented on the scan images and the motion between the talus and calcaneus was analyzed. A similar analysis was done for motion between the navicular and cuboid. Two-tailed paired Student’s t- tests were used to compare the angle and distance measurements between valgus and varus positions.
Results: In the coronal plane, the axis of the talus rotated by 17.0° relative to the axis of the calcaneus as the hindfoot moved from eversion to inversion (p=0.03). The distance between the centers of the talar head and the anterior calcaneus also moved closer to each other by 7.1 mm (p=0.00005). There was no significant change in angle or distance between the navicular and cuboid when moving from eversion to inversion. The angle between the navicular and cuboid axes changed 2.1° (p=0.7), while the distance changed 0.8 mm (p=0.7)
Conclusion: Previous work proposed that the transverse tarsal joint locking mechanism occurs from the talonavicular and calcaneocuboid joint axes diverging (less parallel) as the hindfoot inverts. The current weight bearing CT data shows that not only do the talar and calcaneal axes rotate relative to each other during inversion, but the center of the talar head and anterior calcaneus translate to move closer together. Because the navicular and cuboid do not move, transverse tarsal joint locking may occur due to tightening of the joint capsules and ligaments. Further in vivo study is warranted, especially under dynamic weightbearing conditions.
DOI: 10.1177/2473011421S00265
Assessment of Midterm Functional Outcomes Following Talar Extrusion Injuries
Shilpa Jha, MBBS, MRCS; Kate Atkinson, MBBS, MRCS; Matthew R. McFegan; Amit Patel, FRCS(Orth); Alexandros Vris; Nima Heidari; Lee Parker, FRCS(Tr&Orth); Luckshmana A. Jeyaseelan; Francesc Malagelada Romans
Category: Ankle; Hindfoot; Trauma
Keywords: Talus; Talus Fractures; Trauma
Introduction/Purpose: Open talar dislocations with complete or partial extrusion of the talus are rare, high energy injuries associated with major complications including infection, avascular necrosis and post-traumatic arthritis. These are debilitating injuries with significant long-term effects including avascular necrosis and post traumatic arthritis. Functional outcome data in the literature is limited and predominantly consists of case reports and few single centre case series. Historically these injuries have been treated with talectomy and tibiocalcaneal arthrodesis, however there has been a subsequent trend towards debridement and reimplantation with preservation of the extruded talus. Our aim was to evaluate mid-term functional outcomes, assess complication profile and need for secondary surgery in a single-centre series of cases treated with reimplantation.
Methods: All talar extrusion injuries presenting between January 2015 and January 2018 were identified from the trauma database search at our major trauma centre. Inclusion criteria was defined as open talar dislocations associated with either complete or partial extrusion of the talus. Case-note review was performed collecting baseline demographic data including age, gender, injury mechanism, associated injuries, Gustilo-Anderson grade, smoking and diabetes status, and method and timing of surgical management. Twelve patients were identified with a mean follow-up of 3 years (minimum 26 months). Primary outcome measure was functional outcome assessed using the Manchester-Oxford Foot Questionnaire (MOxFQ). Results for each of the three domains were converted to a 0-100 scale for comparison. Secondary outcomes included complication rate and all cause re- operation rates
Results: Mean age was 37.8 years (17-74 years). Five patients (42%) had total talar extrusion without fracture and 7/12 (58%) sustained fracture-dislocation with partial talar extrusion. All were Gustilo-Anderson grade III. All underwent successful reimplantation with 8/12 (67%) treated with single stage surgery, and 4/12 (33%) in two stages. The mean MOxFQ scores for total talar extrusions versus partial talar extrusions with fracture were 79 (range 9-18) vs 41 (range 0-86) for walking domain, 65 (range 45-80) vs 42 (range 0-90) for pain domain, and 63 (range 38-75) vs 48 (range 19-51) for social domain. One patient (8%) developed avascular necrosis, 3/12 (25%) developed infection and 1/12 (8%) patient eventually required below knee amputation. One (8%) patient underwent secondary surgery fusion for post-traumatic arthritis.
Conclusion: Our series demonstrates the serious ramifications of sustaining talar extrusions. Patients who sustain these injuries should expect persistent functional deficit and pain at mid-term follow-up. Functional outcomes are relatively poor. The data demonstrates a trend towards better functional outcomes in patients who have partial extrusion of the talar dome with associated fractures, compared to ligamentous total talar extrusion injuries. The incidence of avascular necrosis, deep infection and secondary surgery in our cohort supports reimplantation as an effective treatment strategy.
DOI: 10.1177/2473011421S00266
Relative First Metatarsal Length Variation Following Hallux Valgus Surgery and Association with Postoperative Metatarsalgia
Pablo Justiniano, MD; Pablo E. Mocoçain Mac-iver, MD; Mario López; Ruben D. Radkievich, MD; Diego H. Zanolli de Solminihac, MD; Andres Keller Díaz, MD; Stephane Elgueta, MD
Category: Bunion; Midfoot/Forefoot
Keywords: Hallux Valgus; Metatarsalgia; Forefoot
Introduction/Purpose: The hallux valgus surgery can be associated with first metatarsal shortening increasing the occurrence of postoperative transfer metatarsalgia. There is no consensus regarding the acceptable degree of shortening and it relation with metatarsalgia. Besides shortening, there are other factors that could be associated with metatarsalgia like sagittal alignment, deformity correction and surgical technique. The primary objective of the study was to analyze the relative first metatarsal length variation following hallux valgus surgery and its association with postoperative metatarsalgia. The secondary objective was to analyze de first metatarsal length variation and postoperative metatarsalgia by type of surgical technique.
Methods: We performed a retrospective cohort study of all adult patients who underwent hallux valgus corrective surgery between 2017 and 2019 in our clinical center. The inclusion criteria were patients with at least 1 year follow up, without simultaneous lesser metatarsal procedures or referred preoperative metatarsalgia, and that could be contacted for the study. For the analysis we evaluated the incidence of post operative metatarsalgia via phone call and the relation with first metatarsal length variation which was determined by the relative first metatarsal length (RML) measurement according to Nilsonnne/Morton technique. All radiographs were measured by two foot and ankle surgeons. We analyzed the association of postoperative metatarsalgia according to the RML variation. A total of 85 feet were included in the study, with 5 different surgical techniques (16 promo, 19 chevron, 18 scarf, 14 lapidus and 18 MICA)
Results: The average preoperative and postoperative RML were + 0.03 mm and -2.92 mm, respectively. The average global postoperative RML shortening variation was -2.98 mm (min -10, max +5), and by surgical technique were -4.09 mm, -3.11 mm, - 3.05 mm, -2.93 mm and -1 mm for lapidus, chevron, scarf, promo and MICA, respectively. Only 9.1% of patients presented postoperative metatarsalgia, and the average postoperative RML shortening in those patients was - 4.63mm (min 0, max -10). There was a statistically significant correlation between RML shortening and postoperative metatarsalgia in patients with shortening higher or equal to 4 mm (p value <0.05). In relation to the 8 patients with metatarsalgia, 3 of them had a postoperative elevated first metatarsal (1 promo, 1 chevron and 1 lapidus) and 1 had recurrence of the deformity associated (lapidus).
Conclusion: We found a postoperative RML shortening in hallux valgus correction, regardless of the selected surgical technique. The RML shortening was associated with postoperative metatarsalgia in patients with shortening higher or equal to 4 mm. However, in some of those patients, we found other concomitant factors, such as first metatarsal elevation or recurrence of the deformity. Therefore, even though we consider that shortening of the first metatarsal is an important factor, it seems relevant to assess all other potentials factors in patients with postoperative metatarsalgia.
DOI: 10.1177/2473011421S00267
Diagnostic Accuracy of MRI in Diagnosing Plantar Plate Tear About Metatarsalgia: Incidental Finding of A Tear on Routine Magnetic Resonance Imaging
Amir R. Kachooei, MD; Rachel J. Shakked, MD; Johannes B. Roedl; David I. Pedowitz, MD, MS
Category: Lesser Toes; Midfoot/Forefoot
Keywords: Forefoot; Lesser Toe Metatarsophalangeal (MTP) Joint Instability; Metatarsalgia
Introduction/Purpose: This study aimed to assess the rate of plantar plate tear finding on MRI study of symptomatic versus asymptomatic patients. We secondarily aimed to determine the correlation between PP tear grading and symptoms and to assess the diagnostic accuracy of MRI.
Methods: Based on the physical examination report, patients were divided into Symptomatic and Asymptomatic groups. Data from the MRI reports were extracted for the second to fifth plantar plates. All MRIs were studied again by a musculoskeletal radiologist to measure the inter-rater agreement and MRI reports' reliability. MRI finding of the plantar plates was categorized as torn vs. intact. We used the anatomical grading system (AGS) to assess the plantar plate tear grading correlation with symptoms
Results: There was an excellent inter-rater agreement (Kappa=0.92). Calculating the odds ratio reveals that the odds of finding intact PP in a symptomatic patient is 16 times more than finding a tear in the same patient. Diagnostic accuracy of MRI shows that PP tear finding on MRI is highly specific and has a low sensitivity meaning that the chance of incidental finding of a PP tear is extremely low.
Conclusion: MRI is specific for diagnosing plantar plate tear and is suggested to confirm the diagnosis and plan for the surgery when the diagnosis is highly probable concerning the clinical examination.
DOI: 10.1177/2473011421S00268
Effect of Postoperative Ketorolac Administration on the Union Rate Following First Metatarsophalangeal Joint Arthrodesis
Amir R. Kachooei, MD; William Hester, III, MD; Tara Gaston, DO; Daniel O. Corr, BS; Joseph N. Daniel, DO
Introduction/Purpose: To decrease postoperative opioid consumption, nonsteroid anti-inflammatory drugs (NSAIDs), including ketorolac, is considered a proper substitute with few side effects. This study aimed to assess the nonunion rate after the first metatarsophalangeal (MTP) joint arthrodesis and five-day ketorolac administration. We secondarily aimed to compare the observed rate of nonunion in our study with the reported rate of 5.4% in a systematic review.
Methods: In a retrospective cohort study, we included 181 primary MTP arthrodeses from 2016 to 2020 in a single surgeon practice. The surgical technique was identical using a dorsal locking plate after preparing the joint with the cup-and-cone technique. Ketorolac was administered every 6 hours for five consecutive days postoperative. Patients were placed in a heel weight-bearing CAM boot for a minimum of 6 weeks. Union was determined radiographically at three months and the final follow- up. Nonunion was categorized as symptomatic versus asymptomatic.
Results: At three months postoperative, patient characteristics did not show any statistically significant difference between union and nonunion groups. However, at the final follow-up, hallux rigidus was significantly associated with a higher rate of the union in comparison to the preexisting hallux valgus deformity (odds=3.7; P=0.04). of 181 feet, 15 (8.3%) at three months and 12 (6.6%) at the final follow-up revealed nonunion. Of 15, 7 (45%) were asymptomatic, and 8 (55%) were symptomatic. Six (75%) of the ’symptomatic' nonunion underwent an unplanned secondary surgery. Almost 50% of the asymptomatic nonunions at three months healed by the final follow-up; however, none of the symptomatic nonunions healed. Comparing the observed proportion of nonunions at three months (8.3%) and the final follow-up (6.6%) in our study to the mean nonunion rate of 5.4% found in the literature revealed no significant difference between our results and the literature (P=0.067 and 0.27, respectively).
Conclusion: A short course of oral ketorolac does not seem to affect the union rate after MTP arthrodesis. Ketorolac can be used safely and effectively to decrease postoperative opioid consumption.
DOI: 10.1177/2473011421S00269
Soft Tissue Thickness as a Predictor of Wound Complications after Total Ankle Arthroplasty: A Retrospective Study
Jeremy J. Kalma, MD; Zein S. El-Zein, MD; Denise Koueiter; Paul T. Fortin, MD
Category: Ankle Arthritis; Ankle
Keywords: Ankle Replacement; Surgical Site Infection; Outcomes Measures
Introduction/Purpose: Periprosthetic joint infection following total ankle arthroplasty (TAA) is a serious complication often related to the surrounding soft tissue envelope which can lead to poor patient outcomes. The purpose of this study was to determine the relationship between wound complications following TAA and the overlying soft tissue envelope thickness using standardized radiographic soft tissue measurements. We hypothesized that a smaller soft tissue thickness would correlate with an increase in complications.
Methods: 197 patients who underwent primary TAA between October 2014 and December 2018 at a single institution with preoperative radiographs and 6 months of follow up were analyzed. We measured the horizontal distance from the posterior tibia to the overlying anterior skin surface and tibial width 2 cm above the tibiotalar joint on lateral ankle films. The ratio of the soft tissue thickness to the tibial width was calculated and named the ankle soft tissue thickness ratio (ASTR). The patients were divided into 2 groups based upon their ASTR. There were 102 patients in the low ASTR group (ASTR <1.38) and 95 patients in the high ASTR group (ASTR >1.38). Minor complications involved office-based treatment and/or oral antibiotics. Major complications involved surgical intervention. A chi-squared test determined complication incidence variance amongst patients in each ASTR group and an independent t-test determined mean ASTR difference.
Results: Twenty-nine wound complications (14.7%) were identified among 197 patients, 24 (82.8%) minor and 5 (17.2%) major. There were 19 wound complications in the low ASTR group (17 minor and 2 major) and 10 wound complications in the high ASTR group (7 minor and 3 major). Complications were more frequent in the low ASTR group compared to high ASTR group, though not statistically significant (18.6% vs. 10.5%, P=0.158). There was no difference in the mean ASTR measurement between patients with and without wound complications (1.36 vs. 1.40, P=0.093).
Conclusion: This study does not demonstrate a statistically significant difference in post-operative TAA wound complications based on standardized radiographic soft tissue thickness measurements. Though not statistically significant, complications were more frequent in patients with a lower ASTR. Lower surgical site soft tissue thickness may be a predictor of increased risk for wound complications following TAA however further research including studies with larger patient populations is needed to make this determination.
DOI: 10.1177/2473011421S00270
Return to Sports and Clinical Outcomes in Suture-Tape Augmentation for Ankle Instability: A Systematic Review
Ajay C. Kanakamedala; Nathaniel P. Mercer; Alan Samsonov; Raymond J. Walls, MD, FRCS; Eoghan T. Hurley, MB BCh BAO; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle; Sports
Keywords: Ankle Sprain; Broström; Sports
Introduction/Purpose: There is minimal literature on the use of suture-tape augmentation in the treatment of chronic lateral ankle instability (CLAI), prompting an investigation on its use and effect during surgery of the lateral ankle. The purpose of this systematic review is to evaluate the evidence for the use of suture-tape augmentation in the treatment of CLAI, and the outcomes following this technique.
Methods: A literature search was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies were included if they evaluated the use of suture-tape for CLAI. Quantitative and qualitative analysis was performed.
Results: There were 11 studies (LOE II: 2, LOE III: 1, LOE IV: 8) with 334 patients and 334 ankles, and 66.7% were females. The mean age of patients was 27.3 years. The mean follow-up was 27.6 months (range: 11.5-38.5). Overall, 9 recurrent instability events (4.1%) were reported for suture-tape augmentation, with no significant difference between Modified Broström repair and suture-tape augmentation (MD;.81, 95% CI,.19, 3.50, I2 = 0%, p = 0.78). There was no significant difference in talar tilt angle (TTA) improvement between Modified Broström repair and suture-tape augmentation (MD; -0.07, 95% CI, -0.68, 60.54, I2 = 0%, p = 0.82). There was no significant difference in anterior talar translation (ATT) improvement between Modified Broström repair and suture-tape augmentation (MD; -0.06, 95% CI, -0.69, 0.56, I2 = 0%, p = 0.84).
Conclusion: Suture-tape augmentation did not significantly improve clinical or radiological outcomes in the setting of Modified Broström repair for CLAI. Quicker return to play was the single most important advantage of the suture-tape augmentation procedure identified in the current study. This indicates that there is a role for suture-tape augmentation in ATFL repair for athletes and high-demand patients.
DOI: 10.1177/2473011421S00271
First Metatarsophalangeal Joint Fusion with Orthogonal Memory Staple Fixation
Sarang P. Kasture; Anna S. Walsh; Hari Sugathan; Rakesh Dalal
Category: Midfoot/Forefoot
Keywords: 1st MTP Joint; Fusion; Staples
Introduction/Purpose: First metatarsophalangeal joint (MTPJ) fusion is one of the most commonly performed procedure for painful symptomatic arthritis. The implants used for osteosynthesis are variable and depend on surgeon preference. The aim of this paper was to study the outcome of first MTPJ fusion surgery using fixation with orthogonal shape memory alloy (Nitinol) staples.
Methods: 75 consecutive patients who underwent first MTPJ fusion with orthogonal memory staples were included in the study. All patients underwent surgery using standard surgical technique with fixation of the arthrodesis with two 20 mm shape memory alloy (Nitinol) staples (Memo staples, Ortho Solutions Inc). The first staple placed medially and the second staple placed dorsally in orthogonal plane. The arthrodesis surfaces were prepared and temporarily fixed with K wire. Once the position and bone approximation was confirmed satisfactory under image intensifier guidance, a flat staple bed was prepared with saw blade to make sure the staples are not proud after fixation. All patients also received standard postoperative care with heel weight bearing shoe for six weeks and follow-up at 3,6 and 12 weeks as standard regimen. Patient demography, time to clinical and radiological union, early/late complications, rate of non-union, revision surgery and implant removal were noted.
Results: Average age was 64.6 years. 42 patients had severe radiologic arthritic changes while 27 patients had associated moderate to severe hallux valgus deformity. Five patients were known to have inflammatory arthritis. The average follow-up was 18.3 weeks. There were two early complication of superficial infection treated successfully with oral antibiotics. Average clinical union was 7.2 weeks and radiological union at 12 weeks. Five patients (6.6%) had radiological non-union of which four underwent revision surgery with plate fixation. One patient had delayed union while one had dorsal staple back-out but did not warrant removal. None required staple removal from hardware prominence. There was no significant difference in union or complication rates with regards to gender or presence inflammatory arthritis.
Conclusion: This study demonstrates that the outcome of 1st MTPJ fusion with two memory staples in orthogonal position is comparable with other modalities of fixation in terms of rate of union and resurgery. It is safe, simple and easily reproducible technique. Besides, none of the patients in this series required implant removal for hardware related complications. This could be advantageous compared to fewer other modalities like plate fixation, though larger studies are needed to confirm it.
DOI: 10.1177/2473011421S00272
Fifth Metatarsal Bunionette Correction Using a Stable Intramedullary Device
David B. Kay, MD; James A. Sabetta, PA-C
Category: Lesser Toes
Keywords: Fifth Metatarsal; Forefoot; K-Wire
Introduction/Purpose: Fifth metatarsal osteotomies for correction of a bunionette deformity are stabilized with a variety of techniques. The fifth metatarsal is a small bone with a unique blood supply and anatomy. Most of the described osteotomies are distal, making stable fixation technically demanding. The use of minimal incision surgery (MIS), also presents further challenges in the placement of stable fixation and current recommendations are to use either no fixation or intramedullary Kirschner wire fixation. Extensive translational osteotomies have not had documentation on healing as have first metatarsal osteotomies. This paper presents the results of 2 fellowship-trained orthopedic surgeons utilizing a new surgical implant that is both intramedullary and intramedullary. The patients were assessed with an endpoint of radiographic healing.
Methods: A consecutive series of 21 de-identified patients who underwent a fifth metatarsal osteotomy for bunionette correction were radiographically followed until healing. Each patient was pre-operatively classified following the Coughlin classification of bunionette deformity. Postoperative radiographic assessments were made to include: 1. Bridging bone 2. The formation of medial bridging from the metatarsal head to the shaft. 3. Change in the 4-5 Intermetatarsal angle. Also, there was made a notation of complications: Time to weight-bearing, pain, and function were not assessed. There was only a small sample of patients that were treated with an isolated bunionette procedure. The other procedures were impactful and would skew the functional results. We also evaluated for hardware complaints that would need removal.
Results: 19 patients, 21 feet were evaluated with ages ranging from 51-77 years (Avg 63 years). 17 women and 2 men. Only one patient was a revision of prior surgery. Only 4 patients had an isolated bunionette correction. The other surgical procedures including; double osteotomy bunionectomy, distal metatarsal osteotomies (MIS), phalanx osteotomies of the great and lesser toes, Lapidus bunionectomy, first metatarsophalangeal arthrodesis. Coughlin grading; one Grade one, ten Grade 2, ten Grade 3. The average time to radiographic healing was 8 weeks. 5 patients underwent a traditional open incision and a chevron osteotomy with a saw, the remainder of the osteotomies were percutaneous transverse osteotomies performed with a 2x12mm Shannon burr.
The mean 4-5 intermetatarsal angle improved from 10 degrees preoperatively to 3 degrees at follow-up. The amount of shift varied whether the lateral eminence was or was not excised. The numbers are not large and meaningful statistics are difficult to extrapolate.
Conclusion: This is the first documented use of a novel surgical implant designed specifically for fifth metatarsal osteotomies used for bunionette correction. The implant is simple to use, provides for stability to prevent malunion and nonunions. It is low profile and has not caused irritation requiring removal in this pilot group. It is versatile and can be used with either an MIS approach and a transverse osteotomy or a classic open incision with a chevron osteotomy.
DOI: 10.1177/2473011421S00273
Calcaneal Bone Morphology in Association with Bone Mineral Density Status: A Cadaveric Study
Introduction/Purpose: Displaced intra-articular calcaneal fractures are mostly treated by reduction and internal fixation. The calcaneal cortical thickness and regional bone density play an important role in the stability of the fixation construct. This study aims to assess the relationship between calcaneal bone morphology and bone mineral density (BMD) status.
Methods: Seventeen fresh cadaveric specimens underwent a BMD scan at the femoral neck and were later classified according to WHO criteria into three groups, including normal five specimens, osteopenic six specimens, and osteoporotic groups six specimens. The calcaneus bone of each specimen was then dissected and evaluated for the bone morphology. The sustentaculum tali of the calcaneus was divided into anterior, middle, and posterior segment. The superior, inferior, and posterior cortices of the calcaneus were equally divided from medial to lateral into five segments and from anterior to posterior into three segments (Figure 1). The cortical thickness (mm) was measured at the center of each divided fragment. The calcaneal bone density (g/cm3) was quantified at three regions of interest (ROI), including superior, inferior, and posterior ROI (Figure 2).
Results: The calcaneal cortical thickness and calcaneal bone density of each fragment or each ROI were demonstrated as the median and interquartile range (IQR) (Table 1-5, Figure 3). The overall cortical thickness and calcaneal bone density values were significantly lower in the osteopenic or osteoporotic group when compared with the normal BMD group. Notably, the cortical thickness of the normal group at the lateral one-fifth and/or lateral two-fifth fragment of the superior, posterior, and inferior cortices of the calcaneus were not significantly different when compared with the osteopenic or osteoporotic group. When focusing at the sustenaculum tali, the posterior cortical thickness was significantly different only when compared between the normal and osteoporotic groups. Inter and intra-rater reliability of the outcome measurements were all excellent (>0.80).
Conclusion: The cortical thickness of the posterior aspect of the sustenaculum tali, as well as the cortical thickness of the lateral one-fifth and lateral two-fifth of the calcaneus, were less likely effected by the decrease in BMD status. However, the anterior part of sustenaculum tali, anteromedial area of superior and inferior cortex and inferomedial area of posterior cortex are thicker than others.
DOI: 10.1177/2473011421S00274
A Historical Analysis of Randomized Controlled Trials in Pediatric Orthopaedic Foot and Ankle Surgery
Abdulaziz Khurshed; Monther Abuhantash; Jeffrey Kay; Anthony S. Habib; Waleed Kishta, PhD, MB BCh, FRCS(C), MSc(Orth); Darre De Sa
Introduction/Purpose: The primary objective of this systematic review was to comprehensively assess the quality of reporting of randomized controlled trials (RCTs) relating to pediatric orthopaedic foot and ankle conditions. Additionally, this current study looked at factors related to the quality of the RCTs and trends in the quality of reporting over time
Methods: This systemic review was performed according to an agreed predefined protocol and conducted according to Preferred Reporting Items for Systemic Reviews and Meta-analyses (PRISMA) statement standards. PubMed, Ovid (MEDLINE) and Embase were searched for all RCTs on foot and/or ankle surgery from the database inception until March 31, 2020. The quality of reporting was evaluated using the Detsky quality index and the Consolidated Standards of Reporting Trials (CONSORT) checklist for reporting trials of nonpharmacologic treatments. A multivariate regression analysis was used to assess predictors of quality reporting.
Results: The online search yielded 3,697 articles, 22 of which met the inclusion criteria and were assessed for quality of reporting. The earliest identified RCT was published in 1991. Close to 70% of all RCTs have been produced over the past 10 years (since 2010), and over 90% have been published in the past 20 years (since 2000). There has been a significant increase in the number of RCTs published over time (p=0.042). The mean (SD) Detsky score across all included studies was 69.2% (13.8%). Nine (41%) of the studies were considered 'high-quality' with a standardized Detsky score greater than or equal to 75%. The strongest predictor of quality reporting was the inclusion of a CONSORT flow diagram (β-coefficient: 18.4, p=0.0013).
Conclusion: Despite an increase in the quantity of pediatric F&A RCTs over time, the quality has not significantly improved. The use of a CONSORT flow diagram is a strong predictor of high-quality reporting. We encourage investigators to devote more efforts in conducting high-quality RCTs in pediatric orthopaedic foot and ankle, as these are scarce in the literature.
DOI: 10.1177/2473011421S00275
Is Arthroscopic Surgery Favorable for Freiberg’s Disease in Metatarsophalangeal Joint?
Do Yeon Kim; Kwang-Bok Lee, MD, PhD; Gun Joo Park, MD; Jong Kil Kim, MD
Introduction/Purpose: Freiberg’s disease is osteochondrosis involving the metatarsal heads. It is a rare disease, mostly found in the second or third metatarsal. The surgical treatment regimens for this disease have not yet been completely defined. We report the outcomes of cases of Freiberg’s disease treated with arthroscopic surgery. To assess the effectiveness of a minimally invasive procedure with arthroscopic surgery for the treatment of Freiberg’s disease.
Methods: From 2015 to 2019, 13 patients (15 feet) diagnosed with Freiberg’s disease were enrolled for arthroscopic surgery. Patients were divided based on the Smillie’s classification system; 2 stage I, 8 stage II, 3 stage III, 1 stage IV, and 1 stage V. Arthroscopic procedures included synovectomy, debridement, chondroplasty, microfracture, and loose body removal. For radiological evaluation, we obtained pre- and post-operative follow-up X-rays and MRIs. We evaluated clinical outcomes using the American Orthopaedic Foot & Ankle Society (AOFAS) lesser metatarsophalangeal (MTP)-interphalangeal score, and the Visual Analogue Scale (VAS) score. The MTP joint range of motion (ROM) was measured pre- and post-operatively.
Results: Radiological study showed no evidence of osteonecrosis progression in the post-operative follow-up X-ray images in any of the 15 cases. Postoperative 12-month MRIs showed reduction of bone-marrow edema, irregularity of subchondral bone, and cartilage defects in all cases. There were significant improvements in AOFAS scores and VAS scores at post-operative 2 weeks and 3 and 12 months over the pre-operative scores (p < 0.05). The MTP joint ROM improved at the last follow-up (p < 0.05).
Conclusion: Arthroscopic surgery applied to Freiberg’s disease showed excellent results regardless of grades (Smillie’s classification system) in radiological evaluation, clinical outcomes, and MTP joint ROM. We suggest it as a treatment of choice for surgeons when they encounter Freiberg’s disease.
DOI: 10.1177/2473011421S00276
Effect of Total Ankle Arthroplasty Implantation and Adaptive Gait on Ankle and Adjacent Joint Kinematics During Simulated Gait
Jaeyoung Kim, MD; Jeffrey W. Hoffman, MS; Brett D. Steineman; Daniel R. Sturnick, MS; Jonathan T. Deland, MD; Constantine A. Demetracopoulos, MD
Keywords: Ankle Arthroplasty; End-Stage Ankle Arthritis; Gait Study Range of Motion
Introduction/Purpose: Clinical and functional improvement after total ankle arthroplasty (TAA) in end-stage ankle arthritis has been well documented. However, despite the implantation of TAA devices designed to restore normal walking kinematics, patients with end-stage arthritis develop compensatory walking patterns which do not return to normal, postoperatively. This discrepancy between the normative and adaptive gait patterns could influence implant loading and intended function; however, the independent influence of implant constraints and adaptive gait on joint function is unknown. Therefore, this study aimed to isolate the individual and combined effects of TAA implantation and gait adaption from ankle arthritis on foot and ankle kinematics during simulated level walking. We hypothesized that foot and ankle kinematics would primarily be altered through adaptations in gait resulting from ankle arthritis.
Methods: Twelve mid-tibia cadaveric specimens were utilized. A validated six-degree of freedom robotic gait simulator was used to simulate the stance phase [3]. The specimen was first placed on the simulator in the intact condition, simulated with both healthy and adaptive gait inputs collected from healthy and post-surgical TAA subjects (average follow-up: 46 months), respectively. The TAA (Salto Talaris; Integra LifeSciences) was then implanted, and adaptive and healthy gait trials were conducted in the implanted condition. Four conditions were collected on each specimen: intact with a healthy walking trajectory (intact- healthy), intact with an adaptive walking trajectory (intact-adaptive), implanted with TAA with a healthy walking trajectory (TAA- healthy), and implanted with TAA with an adaptive gait trajectory (TAA-adaptive). Ankle, subtalar, and talonavicular joint kinematics in each condition were compared to intact-healthy to isolate the effects of implantation and adaptive gait on kinematics. Bias-corrected 95% confidence intervals were calculated for the difference between conditions.
Results: Significant differences were observed in the ankle, subtalar, and talonavicular joints across all comparisons. In the comparison between the intact-healthy and intact-adaptive conditions, to isolate the effect of adaptive gait (Figure 1A), ankle dorsiflexion and subtalar eversion increased late in stance, while talonavicular abduction increased in early and late stance. In the comparison between intact-healthy and TAA-healthy conditions, to isolate the effect of implant constraints (Figure 1B), ankle plantarflexion, subtalar eversion, and talonavicular abduction significantly increased in mid-stance after implantation. In the comparison between the intact healthy and the TAA-adaptive conditions, to evaluate the combined effect of adaptive gait and implantation (Figure 1C), ankle plantarflexion was increased during early stance and decreased in late stance, subtalar eversion increased during mid-to-late stance, and talonavicular abduction increased throughout most of the stance phase.
Conclusion: The results from this study indicate that both gait adaption and implant constraint contributed to changes in ankle and adjacent joint kinematics. The two factors appear to influence different aspects of the stance phase, where gait adaption appeared to influence early, and late stance and implantation influenced kinematics in mid-stance. The synergistic influence of both factors seemed to exaggerate deviations away from normal kinematics in the subtalar and talonavicular joints while negating deviations from normal in the ankle joint. This suggests that ankle implants designed to restore normative walking patterns may not account for the loading environment seen in patients.
DOI: 10.1177/2473011421S00277
Analyzing Risk Factors for Sequential Above Knee Amputation after Below Knee Amputation in Surgical Treatment of Ischemic and/or Infectious Foot Disease
Ki Chun Kim, MD; Sung-Jae Kim, PhD; Il-Hoon Sung, MD, PhD; Kiwon Young, MD; Kyung-tai Lee, MD, PhD; Hong S. Lee, MD
Introduction/Purpose: Some patients with below knee (BK) amputation for treatment of ischemic and/or infectious foot disease eventually further progress to above knee (AK) amputation. We aimed to analyze predictors for sequential AK amputation after BK amputation.
Methods: We retrospectively reviewed medical records and find 55 patients with BK amputation for surgical treatment of ischemic and/or infectious foot from 2013 to 2018. Twelve patients with sequential AK amputation after BK amputation were designated as group I, and 43 patients successfully treated with BK amputation only were designated as group II. Two groups were compared for various demographic, laboratory and physical state. Then, multivariate logistic regression analysis was done to find predictors for sequential AK amputation after BK amputation.
Results: In univariate analysis between two groups, only 'knee contracture' showed significant difference between two groups (p= 0.003). In multivariate logistic regression analysis performed with variables showing p <0.1 during univariate comparison, knee contracture was found to be predictor for sequential AK amputation after BK amputation (odds ratio= 34.740, p= 0.041).
Conclusion: Patients with intractable ischemic and/or infectious foot disease with knee contracture, optimal level of amputation may be above knee level. Careful decision on amputation level can reduce surgical burden for intractable ischemic and/or infectious foot patients.
DOI: 10.1177/2473011421S00278
Radiographic Evaluation of the Normal Distal Tibiofibular Syndesmosis in Neutral to Dorsiflexion on Weight-Bearing
Ki Chun Kim, MD; Kyung-tai Lee, MD, PhD; Kiwon Young, MD
Introduction/Purpose: Reliable landmarks of ankle syndesmosis change in various position is important for managing ankle injury. The purpose of our study was to investigate and compare radiographic landmarks of normal ankle in various positions.
Methods: The study involved both ankle radiographs of 30 subjects (15 males, 15 females) without clinical or radiographic abnormality. Tibiofibular clear space (TFCS) and tibiofibular overlap (TFO) were measured on anteroposterior (AP) and mortise radiographs in non-standing (NS) and standing (S) neutral and dorsiflexion 10 (DF10) and 20 degrees (DF20). The radiographic measurements were used to calculate means, standard deviations, and intra- and interobserver reliabilities, and compare TFCS and TFO in various positions and genders.
Results: On the AP view, the mean TFCS in NS, S, DF10, and DF20 positions were 4.00+-0.97, 4.00+-0.83, 4.35+-0.95, and 4.45+-0.89 and the mean TFO on the same positions were 6.58+-2.27, 4.27+-1.90, 3.44+-1.96, and 2.38+-1.91. On the mortise view, the mean TFCS in NS, DF10, and DF20 positions were 3.62+-0.88, 4.08+-0.86, and 3.88+-0.97 and the mean TFO on the same positions were 3.57+-2.13, 2.31+-1.77, and 3.57+-2.14. The reliabilities in all positions except TFCS on some positions were excellent. No measurement was significantly different between females and males except TFO in NS on mortise view (p=0.006) and DF10 on AP view (p=0.032).
Conclusion: Increase of TFCS and decrease of TFO on AP view reflects syndesmosis change from non-standing to DF20 on standing. Clinically, Effect of weight-bearing and reliability of TFO should be considered.
DOI: 10.1177/2473011421S00279
Comparison of the Distributions of Mechanoreceptors in the Three Parts of ATFL (Fibula Attach, Mid- Substance, Talar Attach)
Woo Jong Kim, MD; Young Koo Lee, MD, PhD; Young Cheol Hong
Category: Basic Sciences/Biologics; Ankle
Keywords: Ankle Instability; Ligament; Ankle
Introduction/Purpose: To investigate the functional characteristics of the anterior talofibular ligament (ATFL) in the ankle, we divided the ligament into three parts and compare the distribution of mechanoreceptors in each part by type.
Methods: The ATFL were obtained from 20 ankles of 10 fresh-frozen cadavers. The ligament was divided into three parts: fibula attach, mid-substance, and talar attach. Historically, mechanoreceptors were identified and classified as Ruffini (type I), Vater-Pacini (type II), Golgi-Mazzoni (type III) corpuscle, Free nerve ending (type IV). Difference in receptor density were compared.
Results: The ATFL were obtained from 20 ankles of 10 fresh-frozen cadavers. The ligament was divided into three parts: fibula attach, mid-substance, and talar attach. Historically, mechanoreceptors were identified and classified as Ruffini (type I), Vater-Pacini (type II), Golgi-Mazzoni (type III) corpuscle, Free nerve ending (type IV). Difference in receptor density were compared.
Conclusion: There were no significant differences in the densities of the four types of mechanoreceptors among the three parts of the ATFL.
DOI: 10.1177/2473011421S00280
Apoptosis Occurs in Anterior Talofibular Ligament of Chronic Lateral Ankle Instability: Biochemical Evidence from Bench to Bed
Introduction/Purpose: Chronic lateral ankle instability (CLAI) is a common entity that can result in degenerative arthritis if left untreated. CLAI is treated operatively, while acute ligament injury, so-called 'ankle sprain' is primarily treated nonoperatively with good clinical outcomes. This widely accepted opinion has been proved by clinical scoring system, physical examination, stress radiographs, ultrasonography, or magnetic resonance imaging. However, some surgeons often rush to perform the operative repair for acute ankle ligament injury. Apoptosis has been demonstrated as a considerable cause of ligament degeneration. Up to date, there are few reports of biomolecular and histochemical evidence focused on the 'apoptosis' that occurred in the torn anterior talofibular ligament (ATFL). The aim of this study is to elucidate the apoptosis that occurs within the ATFL of CLAI.
Methods: Ligamentous tissues were collected from 15 patients undergoing modified Broström operation (group C) and 10 patients undergoing distal fibular fracture surgery as controls (group A). We allocated distal fibular fracture patients as an alternative to acute lateral ankle ligament injury to harvest acutely injured ATFL tissue. In both groups, the tissue samples were harvested at ATFL. Apoptotic cells were determined by TUNEL (terminal deoxynucleotidyltransferase-mediated dUTP-biotin nick end labeling) assay. Caspase 3/7, 8, 9, and cytochrome c activities were measured to determine the intracellular apoptosis pathway using Western blot. Immunohistochemistry staining was also performed to detect the expression of caspases and cytochrome c.
Results: The TUNEL assay revealed a large number of positive staining cells in group C that included ATFL of CLAI. The apoptotic activities of ligaments from group C were significantly higher than those of group A (P < 0.05). Immunohistochemistry also revealed an increase in expression of caspase 3/7, 8, 9, and cytochrome c more in group C than in group A.
Conclusion: This study demonstrates that the degenerated ATFL following CLAI showed higher apoptotic activity than acutely sprained ligament. Based on our biochemical findings, we could remind previous understanding about surgical indication and timing of lateral ankle ligament injury. We suggest that a clinical relevance between our laboratory research and previous knowledge Further study should be conducted to focus on biological augmentation to reverse or prevent further apoptosis within the lateral ankle ligament complex including ATFL.
DOI: 10.1177/2473011421S00281
Development of A Risk Stratification Scoring System to Predict General Surgical Complications in Foot and Ankle Surgery Patients
Haroon Kisana; Clayton Hui; John R. Martin; Chad Stecher; Joshua Hustedt, MD
Introduction/Purpose: Preventing postoperative complications is crucial for patients, surgeons, and healthcare facilities. A risk stratification scoring system was created to help optimize risk factors for general surgical complications in foot and ankle surgery patients.
Methods: A total of 85,363 patients that underwent foot and ankle procedures from 2005 to 2017 were identified as part of the American College of Surgeons National Surgical Quality Improvement Program. Independent risk factors associated with postoperative complications within 30 days of surgery were identified and used to develop a point-scoring system to estimate the relative risk for experiencing complications. For validation, the system was tested on a subset of patients from the database who had foot and ankle surgery.
Results: The 30-day postoperative complication incidence after foot and ankle surgery was 19.1%. Risk factors associated with postoperative complications were tobacco abuse, age (>64), diabetes mellitus, hypertension, elevated creatinine (>1.3 mg/dL), hypoalbuminemia (<3.5 g/dL), and anemia (male hematocrit <42; female <38). Point scores from each factor were: anemia, +7; hypoalbuminemia, +4; hypertension, +4; elevated creatinine, +3; diabetes mellitus, +3; age over 64, +2; and tobacco abuse, +1. In the validation cohort, patients categorized as low risk (0-5), using the point scoring system had a 2.5% rate of 30-day complications; patients categorized as medium risk (6-10) had a 7.5% complication rate (relative risk = 2.0; 95% CI, 1.7-2.3 compared with low risk) and high risk (>=11), 33.1% (relative risk = 3.7; 95% CI, 3.2-4.3).
Conclusion: This point scoring system predicts risk for general postoperative complications after foot and ankle surgery. These data may help foot and ankle surgeons identify areas of clinical concern with patients to reduce the risk of experiencing postoperative complications.
DOI: 10.1177/2473011421S00282
The Circular Arc Curved Nail for Internal Fixation of Tibio-Talo-Calcaneal Arthrodesis
Introduction/Purpose: Normal anatomy demonstrates alignment of the heel, the subtalar facet, the talus, the ankle joint and the distal tibia on a regular curve. This curve lies on a vertical plane which is slightly angulated inwards in relation to the sagittal plane. Today’s hindfoot nails are either straight or bent. The hole which accommodates the implant is always straight and thus does not respect the normal alignment of the hindfoot. This technique may cause a plantar neurapraxia, the nail holds poorly the calcaneus and tends to create a hindfoot varus. Purpose of the study is to optimize the technique to
Methods: A circular arc bore hole crosses the heel, the posterior subtalar facet, the tibio-talar joint and the distal tibia metaphysis. The hole is bored using a motor driven end cutting flexible reamer which is seated within a rigid curved hull. The nail has the exact same shape than the hull and is impacted up to the distal tibia creating a bone-nail form fit. A distal locking screw crossing the subtalar joint and a proximal locking screw within the tibia concludes the central fixation. 47 patients (23 women and 24 men aging 30 to 84 y (mean 52y)) have been treated so far using this technique. The diagnosis was basically primary and post- traumatic arthritis and includes diabetic arthropathies (4 cases) and failed TAR (3 cases). After 2 weeks our patients did practise partial weight bearing using a cam walker for other 6 weeks.
Results: The mean follow-up time of the patient series is 3 years (16-78 months). Two patients with diabetic arthropathy died 2 years and 8 months and the other 8 months post-op after consolidation of the arthrodesis due to their primary disease. 3 cases sustained a deep infection which requested a below knee amputation in 2 cases and a calcanectomy in another case. Within the remaining 42 cases, 37 consolidated their arthrodesis within 2 months; 5 cases had a delayed union and 2 cases had to be revised for a non-union, one in the ankle, the other one in the subtalar joint. Patients with a good bone quality and anatomical hindfoot axes could bear their body weight entirely at 2 months. 1 patient reported remaining pain at 2 years post-op and another case was additionally operated to correct a remaining midfoot deformity (club foot).
Conclusion: The tibio-talo-calcaneal arthrodesis can be successfully treated using a central circular arc curved nail respecting a form fit interaction between bone and nail. The anatomical osteo-articular alignment of the hindfoot is corrected or preserved. Due to the safe approaches and the bone-nail form fit, the technique allows for primary stability and prevents shortcomings such as neurological complications and non-union. We expect a shorter period between surgical fixation and full weight bearing.
DOI: 10.1177/2473011421S00283
Lag Screw with Plantar Plating for Naviculocuneiform Arthrodesis in Progressive Collapsing Foot Deformity
Derek M. Klavas, MD; Austin E. Wininger; Stephanie S. Gardner, MD; Jason S. Ahuero, MD; Kevin E. Varner, MD
Introduction/Purpose: Medial column procedures are a common adjunct to progressive collapsing foot deformity (PCFD) correction. In particular, naviculocuneiform (NC) arthrodesis could be performed when degeneration or instability at the NC joint is contributing to arch collapse. Plantar plate fusion resists gapping along the tension side of the joint, potentially reducing risk of non-union and recurrent deformity. Additionally, by placing the hardware in a plantar location there is an increased soft tissue envelope to function in a protective matter and eliminate the possibility of hardware prominence and tendon irritation. The purpose of this study was to analyze short-term clinical and radiographic outcomes of NC fusion using a lag screw with plantar plating technique.
Methods: A single-surgeon retrospective case series was performed on patients with PCFD and medial arch collapse treated with NC arthrodesis using a lag screw plus plantar plating technique between January 2016 and December 2019, with a minimum six month clinical and radiographic follow up. Patients undergoing revision NC joint arthrodesis, patients with incomplete imaging, or an arthrodesis technique that did not utilize NC joint plantar plating were excluded. Demographic data, perioperative data, complications, and reoperations were recorded from electronic medical records. Pre-operative AOFAS midfoot scores were calculated at the initial clinic visit and then again at the patients' most recent follow-up. In the case of most recent follow up occurring prior to six months post-operatively, a telemedicine visit was performed. Anteroposterior (AP) and lateral talo-first metatarsal angles, talonavicular coverage angle, and calcaneal pitch were measured independently by three authors. Fusion was confirmed radiographically and computed topography when union was in question.
Results: Nineteen patients (15 female, 4 male; 11 right, 8 left) with a mean age of 56.6 years and a mean follow-up of 21.0 +- 13.4 months were reviewed. A mean 3.4 concomitant procedures were performed at the time of NC fusion. AP talo-first metatarsal angle (18.9° to 5.2°), lateral talo-first metatarsal angel (-18.7° to -4.4°), talonavicular coverage angle (28.1° to 7.4°), and calcaneal pitch (14.6° to 20.1°) all improved significantly (p<0.001). Fusion was confirmed in 15 (79%) patients at a mean 6.1 +- 3.5 months. Mean AOFAS midfoot scores improved from 51.7 +- 13.0 preoperatively to 82.6 +-12.8 (p<0.001) at an average 21.0 +- 13.4 months follow up. Two patients experienced broken hardware, one patient fractured through flexor digitorum longus (FDL) transfer site and experienced non-union requiring revision at 9.5 months, one patient experienced symptomatic lateral column hardware requiring removal, and one patient experienced non-union requiring revision at 13.5 months.
Conclusion: Lag screw with plantar plating is a technique for NC arthrodesis that is associated with a higher non-union rate (21%) than what is reported in the literature. Nonetheless, at short term (mean 21 months) follow up, the technique proved capable of correcting medial arch collapse through the NC joint when used in conjunction with adjunctive soft tissue and bony procedures. Plantar plating technique resulted in no instances of symptomatic hardware along the medial midfoot. Addressing medial arch collapse with NC arthrodesis resulted in significant improvement of both radiographic outcomes and patient reported clinical outcomes.
DOI: 10.1177/2473011421S00284
Elevated Body Mass Index Does Not Adversely Influence the Outcomes of Arthroscopic Treatment for Osteochondral Lesions of the Talus
Don T. Koh, MBBS, MRCS, BSc (Hons); Zhan Xia; Zongxian Li; Kae Sian Tay; Shi Ming Tan; Nicholas Yeo, MBBS, MRCS, MMed(Ortho), FRCS(Edin), FAMS; Inderjeet S. Rikhraj, FRCS
Category: Ankle; Arthroscopy; Hindfoot; Trauma
Keywords: Osteochondral Lesions of the Talus; Arthroscopy; Cartilage Defect
Introduction/Purpose: Osteochondral lesion of the talus (OLTs) is a common condition found in patients with chronic ankle pain after previous ankle sprains. Conservative measures such as analgesics, activity modification and immobilisation of the affected ankle are usually applied as first line treatments. Surgical management are indicated after conservative management have failed. This study evaluates the influence of body mass index (BMI) on the early clinical outcomes of arthroscopic debridement and microfracture of OLTs.
Methods: An IRB approved study was conducted between 2007 and 2017. A total of 252 patients with symptomatic OLTs who failed conservative management underwent arthroscopic debridement and microfracture of OLTs over the affected ankle. Postoperatively, all patients underwent a standardised postoperative rehabilitation protocol. Patients who underwent previous fractures, previous infections or associated ligamentous injury of the affected ankle were excluded from this study. Patients from this cohort were divided into two groups based on BMI. The normal BMI group (NB-Group) (BMI 18.5-25.0kg/m2) and raised BMI group (RB-Group) (BMI >=25kg/m2). Visual Analogue Score (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) Hindfoot Score as well as the Physical and Mental Components of the Short-Form 36 Questionnaire (PCS and MCS respectively) were prospectively collected from these cohort during their standard postoperative outpatient follow up.
Results: A total of 252 patients were reviewed. Patients from either group were otherwise well matched demographically (Table 1). The operative duration was significantly shorter for NB-Group compared to RB-Group. Patients from both groups had significant improvement VAS, AOFAS and PCS scores postoperatively at 6 months and 24 months after surgery (Table 2).Between both groups, patients had comparable VAS, AOFAS as well as PCS scores at preoperative, 6 months postoperative and 24 months postoperatively (p > 0.05). However, MCS in the RB-Group showed a gradual deterioration over 24 months postoperatively and was significantly poorer compared to the NB-Group at 24 months (p = 0.036) (Figure 1).
Conclusion: Arthroscopic debridement and microfracture is a reliable procedure, providing significant improvement in pain relief and functional improvement in patients. A raised BMI did not adversely affect pain and functional outcomes. However, patients with raised BMI required a longer duration of procedure and had significantly poorer MCS scores at 24 months after surgery.
DOI: 10.1177/2473011421S00285
Biomechanical Comparison of Fibertape Augmentation with Intercuneiform Adjunct and Cannulated Screws for Ligamentous Lisfranc Injuries: 3D Visualization of Complex Movement
Zachary Koroneos; Kristen M. Manto, BS; Brandon Martinazzi, BS; Chris M. Stauch, BS; Shawn M. Bifano, MD; Gregory I. Pace, MD; Gregory Lewis, PhD; Michael C. Aynardi, MD
Category: Midfoot/Forefoot; Sports; Trauma
Keywords: Lisfranc Injury; Lisfranc Ligament; Biomechanics of the Foot and Ankle
Introduction/Purpose: The preferred method of fixation for ligamentous Lisfranc injuries is controversial, with the traditional method being transarticular screws. Unfortunately screw removal is often required leading surgeons to seek alternative fixation methods including fibertape constructs. Our lab has published biomechanical results on the safety and efficacy of a fibertape construct for the treatment of ligamentous Lisfranc injuries demonstrating biomechanical superiority with the supplementation of an intercuneiform limb. The purpose of this biomechanical study is to compare transarticular screws to a fibertape construct under loading and utilizing 3D visualization software.
Methods: Three matched pairs of cadaveric specimens were dissected to allow for the placement of three screws on the dorsal aspect of the each bone involved in the Lisfranc complex. The diastasis between bones were measured at three midfoot joints in the Lisfranc articulation while each specimen was loaded to 75% of donor bodyweight. Measurements were obtained for the pre- injured specimens. The MC-2MT joint was sectioned under fluoroscopic imaging and re-measured to produce at least 2 mm of gapping. Specimens were then fixed with either transarticular screws or fibertape with an intercuneiform limb and computed tomography scans were performed. Post-fixation measurements were obtained for 250 N of axial loading with subsequent 100 N increases up to 650 N. CT scans were imported as DICOM images and the three bones were segmented to analyze the gapping that occurred at the dorsal, interosseous, and plantar portions of the ligament.
Results: There were no significant differences detected for the diastasis between bones in the Lisfranc complex between the fibertape and screws. After loading to 650 N, no specimens had reached a diastasis of 2 mm through coordinate digitized measurements (Figure 1A and B). At 650 N of loading the fibertape specimens displayed an average diastasis of 0.78 mm while the specimens fixed with screws also displayed an average diastasis of 0.78 mm. 3D diastasis measurements showed coordinate digitized measurements were within 0.2 mm of those measured from 3D reconstruction of CT scans. The largest diastasis occurred at the dorsal aspect of the ligament.
Conclusion: The use of a fibertape device involving a supplementary intercuneiform limb appears to provide a biomechanically viable alternative to screws for ligamentous Lisfranc injuries. Diastasis was verified using 3D computer models. Future efforts involve increasing the number of specimens, applying cyclic loading, and determining the effects on each portion of the ligament for each fixation type.
DOI: 10.1177/2473011421S00286
Establishment of a Neurodegenerative Mouse Model for Charcot Neuropathic Arthropathy
Zachary Koroneos; Anna Ptasinski; Chris M. Stauch, BS; Laura R. Luick, MD; Julie C. Fanburg-Smith; Michael C. Aynardi, MD
Category: Basic Sciences/Biologics; Diabetes
Keywords: Charcot Foot; Diabetic Foot; AAFD
Introduction/Purpose: Neuropathic arthropathy (Charcot) is a progressive and debilitating joint destruction and has neurovascular and neurotraumatic etiologies which are commonly observed in type II Diabetes. This stems from the loss of protective sensation through peripheral neuropathy, cartilage loss, and fragmentation. To model this condition, diabetic obese mice have demonstrated insulin resistance and peripheral neuropathy similar to that seen in type II diabetes in humans. We hypothesized that exposing these diabetic induced, neuropathic (DIN) mice to neuro-trauma through a regimented running protocol would produce a Charcot like, neurodegenerative state seen in human diabetic Charcot when compared to controls.
Methods: Following IAUCUC approval, 24 DIN wild-type C57BL/6J, and 24 wildtype control (WTC) C57BL/6J mice were obtained (Jackson Labs, Bar Harbor, ME) at 6-weeks-old. After a one-week acclimation period, DIN mice consumed a high-fat diet (60% fat by kcal) ad libitum to facilitate neuropathic diet-induced obesity while WTC mice consumed an age-matched standard low-fat control diet (10% fat by kcal). At 12-weeks-old, half of the animals from each group were subjected to a high-intensity inclined treadmill running protocol (+R), which has been previously shown to induce neurotrauma. The protocol involved 25 minutes of running 4 times per week for 10 weeks for both groups. Von Frey filament sensory testing, and radiographic analyses were performed at weeks 0,5 and 10. After 10 weeks, animals were sacrificed; histopathologic analyses were performed to evaluate the navicular-cuneiform joint articular cartilage, sub-chondral and cortical bone, distance to marrow space, and soft tissue including nerves, and vessels.
Results: DIN+R mice displayed significantly reduced sensory function in Von Frey filament testing in week 1 (P<0.05) and this worsened over time requiring 22.0% more force for paw withdrawal by week 10 (P<0.001). Radiographic analysis determined that DIN+R mice demonstrated greater midfoot subluxation & tarsal instability at all time points compared to WTC (P<0.001). Pathological analyses of DIN+R mice demonstrated a significant increase in neurodegenerative destruction of the hind paws compared to controls (P<0.001). Interestingly, DIN+R subjects demonstrated the presence of hyalinized arteriolosclerosis and intraneural vacuolization/myxoid/edematous changes with in hind paw nerves seen in human Charcot histopathologic analysis. Furthermore, these changes were not observed in controls.
Conclusion: Diabetic induced, neuropathic (DIN) mice, when exposed to a regimented running protocol, displayed a neurodegenerative state in their hind paws similar to that seen in human diabetic Charcot foot. In addition, DIN+R mice had both radiogahpic and pathologic changes akin to early diabetic Charcot changes seen in humans. This is the first mouse model which has successfully demonstrated that the combination of peripheral neuropathy and neurotrauma can consistently reproduce early Charcot like changes seen in humans. This model will serve as the basis for future testing of medical and surgical interventions for the treatment of diabetic Charcot in humans.
DOI: 10.1177/2473011421S00287
Histological Findings Upon Patients Undergoing Revision Surgery after AMIC of the Talus
Fabian Krause, MD; Helen Anwander, MD; Birgit Schaefer
Introduction/Purpose: Failure after AMIC (autologous matrix-induced chondroplasty) of the talus is relatively rare and ranges between 2-6%. The purpose of the study was to analyze the histologic quality of the repair cartilage and potentially identify the mode of failure in 3 patients that underwent revision surgery after primary AMIC procedures.
Methods: Out of 48 patients treated with AMIC for OLT between 2012 and 2018 at our institution, three patients (6.2%, average age 27.3 years) required revision surgery for various reasons. During revision, repair cartilage was evaluated about integration with the surrounding healthy cartilage and firmness, and specimen were taken for histologic assessment.
Results: Only one patient that had, next to revision AMIC, a lateral ligament reconstruction for a secondary supination sprain, improved clinically after revision surgery (patient no.3). Despite repair SMOT (no.1) or deltoid ligament repair (no.1), the two other patients did not benefit from revision. Supposed reasons for ongoing symptoms were progressive posttraumatic arthritis (no.1 and 2) and neuropathic pain (no.2). Three types of soft connective tissues could be identified: (i) non-vascularized fibrocartilaginous tissue (patient no. 1-3), (ii) fibrous tissue (patient no. 1 and 2), and (iii) hyaline like cartilage (patient no. 3).
Conclusion: Overall, data support the theory that patients with hyaline or hyaline-like repair cartilage tend to better clinical outcome over time. However, the growth of hyaline or hyaline-like repair cartilage appears to require ligamentous stability, neutral or even offloading hindfoot alignment, and absence of arthritis.
DOI: 10.1177/2473011421S00288
Epidemiology of Insertional Achilles Tendinosis in Patients Requiring Surgical Intervention
Bryce F. Kunkle; Nicholas A. Baxter; Alexander Caughman; John Barcel; Daniel J. Scott, MD, MBA; Christopher E. Gross, MD
Introduction/Purpose: While many patients benefit from non-operative treatment of insertional Achilles tendinosis (IAT), some require surgical debridement and reconstruction. While numerous studies have looked for factors that may contribute to the development of IAT, there is a lack of studies that identify factors that contribute to the need for surgical management.
Identification of these factors could better inform physicians on the progression of IAT and could help guide doctor and patient decision-making. The purpose of this study is to determine the relationship of patient demographic characteristics, comorbidity profiles, and radiological markers with the need for future surgical or non-surgical management of IAT.
Methods: A retrospective chart review was performed to identify patients who received either surgical or non-surgical treatment of IAT at an academic institution from September 2015 - June 2019. Patients were identified using ICD-10 diagnosis codes for Achilles tendinosis, and all cases of non-insertional tendinosis were excluded (N=226). This sample was further separated into patients who received surgical treatment (n=48) and those who were managed conservatively without surgery (178). Demographic and comorbidity data was collected and compared between groups. Additionally, the presence and magnitude of radiological markers including Haglund’s deformity, calcaneal enthesophytes, relevant calcaneal angles, and maximum cross- sectional tendon disease involvement on MRI were collected and compared between groups (Figure 1). A multivariate, binomial logistic regression model was then constructed in order to identify independent predictors of the need for surgical management.
Results: There were no significant differences between groups in regard to age, sex, race, BMI, tobacco or alcohol use, hypertension, diabetes, arthritis, previous arthroplasty, or previous platelet-rich plasma injection. The surgery group was significantly more likely to have evidence of Haglund’s deformity on clinical exam (83% vs. 69%; p=.005) and to have depression (27% vs. 12%; p=.012). Patients who received an ankle MRI were more likely undergo surgery (63% vs. 27%; p=.006), and patients treated surgically had a higher percentage of maximum cross-sectional tendon disease involvement on MRI (41% vs. 26%; p<.001). Multivariate logistic regression analysis showed that increased cross-sectional disease involvement was an independent predictor of the need for surgery, with involvement of at least 18% being significantly predictive of this need.
Conclusion: Patients who received surgery for IAT were significantly more likely to have evidence of Haglund’s deformity on clinical exam, have a previous diagnosis of depression, have received an MRI, and have a higher percentage of cross-sectional tendon disease involvement. Patients with at least 18% cross-sectional tendon involvement on axial MRI are more likely to go on to surgery and should therefore be counseled as such. Foot and ankle surgeons should use this information to facilitate shared decision-making regarding conservative versus surgical treatment of IAT.
DOI: 10.1177/2473011421S00289
Minimally Invasive Surgery for Severe Hallux Valgus with Severe Metatarsus Adductus: Case Reports
Toshinori Kurashige, MD
Category: Bunion; Lesser Toes
Keywords: Minimally Invasive; Metartus Adductus; Hallux Valgus
Introduction/Purpose: Metatarsus adductus (MA) is a congenital transverse plane deformity with an incidence of approximately 30% in patients with hallux valgus. Operative treatment of hallux valgus (HV) with MA can be clinically challenging, and the recurrence rate of HV has been reported as two times higher than in patients without MA. Minimally invasive surgery (MIS) for the correction of HV is growing in popularity; however, only one study has been published on MIS for HV with MA using percutaneous proximal metatarsal osteotomy. We presented our case reports using distal oblique metatarsal minimal invasive osteotomy (DOMMO) for severe MA.
Methods: We corrected two feet using DOMMO for severe MA. Minimally invasive chevron Akin osteotomy (MICA) was utilized to correct severe HV. The patient had subluxations in the second and third metatarsophalangeal joints and hammer toe deformities. Therefore, those deformities were concurrently corrected using percutaneous procedures. The patient was allowed immediate full weight bearing postoperatively in a flat rigid shoe for 6 weeks. Radiographic and clinical evaluations were performed preoperatively and one year after surgery. On the anteroposterior radiograph, the hallux valgus angles (HVA), the first intermetatarsal angles (IMA), tibial sesamoid positions (TSP) and metatarsus adductusangles (MAA) were evaluated. On the lateral weight-bearing radiograph, first metatarsal inclination angles were also evaluated. We also evaluate the Japanese Society for Surgery of the Foot (JSSF) hallux and lesser toes scales and the Self-Administered Foot Evaluation Questionnaire (SAFE-Q) both before and after MIS for HV with MA.
Results: In the first case, the HVA improved from 50° to 16°, the IMA from 15° to 11°, TSP from 7 to 5 using Hardy’s classification, and MAA from 27° to 14.5°, pre- to postoperatively. In the second case, the HVA improved from 45° to 11°, the IMA from 10° to 6.5°, TSP from grade 7 to 3, MAA from 30 to 12, pre- to postoperatively. The first metatarsal inclination angles changed from 16.9° and 18.8° to17.7° and 22.0°, respectively. All subluxations and hammer toe deformities were resolved. Although there were delayed unions in the lesser metatarsals, unions were achieved finally. Preoperative JSSF hallux scales and lesser toes scales were 59 points and 64 points, 67 points and 80 points, respectively. Both hallux and lesser toe scales improved to 100 points one year after surgery. All SAFE-Q subscores were also improved one year after surgery.
Conclusion: In conclusion, our MIS procedure, consisting of DOMMO of the second, third, and fourth metatarsals and MICA, could correct severe HV with severe MA. The patient was allowed immediate full weight bearing postoperatively in a flat rigid shoe. Although there were delayed unions in lesser metatarsals, unions were finally achieved and good results were demonstrated both radiographically and clinically.
DOI: 10.1177/2473011421S00290
Percutaneous Bunionette Correction without Fixation: Clinical Results and Radiographic Evaluations Including Rotation of Metatarsal Head and Sagittal Angular Change of Fifth Metatarsal
Introduction/Purpose: Bunionette has been treated as an analogy of hallux valgus, and the surgical techniques are similar. However, only the anteroposterior image is generally evaluated pre- and postoperatively. There are few studies that evaluated on the lateral radiograph, and to the best of our knowledge, no study that evaluated changes in rotation of fifth metatarsal head. In percutaneous bunionette correction using a burr, shortening of fifth metatarsal and elevation of metatarsal head are inevitable. In addition, there is also the possibility of rotational change of metatarsal head without fixation.
Methods: We evaluated 18 consecutive feet performed percutaneous bunionette correction without internal fixation. Mean age was 54.9 years. Mean follow-up was 10.1 months at least six months followup. On anteroposterior weightbearing radiograph, we measured the fifth metatarsophalangeal angle (MPA), fourth and fifth intermetatarsal angle (IMA), the fifth metatarsal head width (MHW), the lateral deviation angle (LDA) of the fifth metatarsal, and fifth metatarsal shortening. On the lateral weightbearing radiograph, we measured the lateral inclination angle (LIA) of the fifth metatarsal, the fifth distal metatarsal height (DMH), mid metatarsal height (MMH), proximal metatarsal height (PMH), and plantar bowing angle (PBA). To evaluate the rotation of the fifth metatarsal head, we devised a new original method measured at the medial tubercle location (MTL). Preoperatively and at the most recent follow-up visit, we applied the Japanese Society for Surgery of the Foot (JSSF) lesser scale and visual analogue pain scale (VAS).
Results: Except for MTL, DMH and PMH, all parameters showed significant changes postoperatively.MPA, IMA and LDA reduced from 17.3 degrees to 6.4 degrees, from 9.9 degrees to 4.5 degrees, and from 2.3 degrees to -10.0 degrees, respectively. Shortening of fifth metatarsal was 2.5 mm. Despite not performing partial head resection, MHW decreased from 12.1mm to 11.4 mm. LIA decreased from 9.2 degrees to 6.1 degrees. MMH decreased from 11.6 mm to 10.9 mm. PBA decreased from 7.0 degrees to -1.3 degrees. Union was obtained at 6.9 weeks. MTL reduced from 3.4 to 2.8 but not significantly. However, MTL changed in 15 of 18 feet (83.3%) postoperatively. JSSF lesser scale improved from 66.7 to 97.8 points. VAS also improved from 3.6 to 1.0. One foot had a delayed union and an occasional pain.
Conclusion: Percutaneous bunionette correction without fixation could achieved good clinical and radiographic results comparable with previously published outcomes of open and percutaneous surgery with fixation with less complication. The procedure could be adapted to different types of bunionette deformity. In this surgical method, bunionette is corrected in three dimensions.
DOI: 10.1177/2473011421S00291
Percutaneous Surgery for Interdigital and Lateral Fifth Toe Corns
Toshinori Kurashige, MD
Category: Lesser Toes
Keywords: Minimally Invasive; Intermetatarsal space; Joint Preserving Surgery
Introduction/Purpose: Lateral fifth toe corns (LFC) form as a result of extrinsic pressure from footwear. Interdigital corns (IDC) form over the condyles of the phalanx between the toes, and can be soft and very painful in most cases. When conservative treatment fails, surgical treatment is indicated. Partial condylectomy for interdigital cornsis difficult because of the narrow webspace and risk of painful postoperative scar. No prior study has been published on percutaneous surgery for lateral fifth toe and interdigital corns, with the exception of some publications on the explanation of the technique.
Methods: We performed percutaneous partial condylectomy for six toes in five patients with one LFC and five IDCs. The mean age was 71 years. The mean follow-up period was 16.2 months. All feet, except for one malalignment case after second proximal phalanx fracture, had both hallux valgus and bunionette. A small incision was made distal to the corn to allow the insertion of the entire cutting surface of a burr to avoid skin damage. The periosteum was removed from the eminence by a small rasp and provided an adequate working area. The bone eminence was then removed with 2-5 or 2-8 mm burrs. For hallux valgus and proximal phalanx malalignment after fracture, we also corrected them percutaneously. In some cases, the Japanese Society for Surgery of the Foot (JSSF) lesser toes scales and self-administered foot evaluation questionnaire (SAFE-Q) were evaluated pre- and postoperatively.
Results: There was no complication, except for one valgus deformity in the second proximal interphalangeal joint after partial condylectomy. At the final follow-up visit, all patients had no recurrence of corns and no symptoms, and were very satisfied with the results during the follow-up period of one year. In case of IDC, JSSF lesser toes scale improved from 45 points to 100 points at the final follow-up. All SAFE-Q subscores were improved with regard to 'Pain and pain-related' sensations from 36.7 to 99.6, 'Physical functioning and daily living' from 54.5 to 100, 'Social functioning' from 37.5 to 100, 'Shoe-related' from 25 to 100, and 'General health and well-being' from 25 to 95. The visual analog scale of pain improved from 7 to 0.4.
Conclusion: The percutaneous procedure consisted of partial condylectomy with correction of associated deformities achieved good results without major complications and recurrence over the one year follow-up period.
DOI: 10.1177/2473011421S00292
Percutaneous Tarsometatarsal Arthrodesis of the Lesser Ray with Autograft using a Cannulated Screw
Introduction/Purpose: Tarsometatarsal (Lisfranc) joint arthritis can be a painful condition caused by primary osteoarthritis, inflammatory, and posttrauma. When conservative treatment failed, tarsometatarsal arthrodesis is indicated. There has been no study on percutaneous tarsometatarsal arthrodesis previously. The purpose of this study is to report our percutaneous tarsometatarsal arthrodesis technique and the results of case series.
Methods: We report 11 joints from 6 feet with painful tarsometatarsal arthritis of lesser ray treated using percutaneous procedure using a wedge burr. The mean age at surgery was 67 years. The mean follow-up period was 12 months. Five feet of 4 patients had TMTj degeneration with hallux valgus. Another patient suffered from painful posttraumatic degenerative arthritis. Through 5-10 mm incision, a 2.9 mm-diameter wedge burr was introduced into the joint. Resection of subchondral bones was performed with the medial, lateral and plantar cortices preserved. The dorsal cortex except the burr insertion point was also remained. The iliac-crest bone grafts were taken using a 6-mm diameter trephine. Preoperatively and at the most recent follow-up visit, we applied the midfoot scale proposed by Japanese Society for Surgery of the Foot (JSSF). The validity and reliability of the JSSF scale has been confirmed in previous studies.
Results: Though there was one nonunion with screw breakage, we achieved successful results with no need of revision surgery during mean one year follow-up period. Bone unions were achieved in 10 of 11 joints (91%) at the most recent follow-up. JSSF midfoot scale significantly improved from 62 points preoperatively to 89.6 points at the most recent follow-up (p= 0.04).
Conclusion: Our percutaneous TMTj arthrodesis was achieved a union rate and clinical results comparable to other surgical technique. This procedure was an effective method for treatment of TMTj arthritis.
DOI: 10.1177/2473011421S00293
Radiographic and Clinical Results of Minimally Invasive Chevron Akin Osteotomy for Moderate to Severe Hallux Valgus Deformities
Introduction/Purpose: Some authors reported the results from the third-generation minimally invasive chevron Akin osteotomy (MICA) to treat mild to moderate hallux valgus recently. However, there have been few studies evaluating the results of MICA for moderate to severe hallux valgus. The purpose of this study was to evaluate the radiographic and clinical results of MICA for correction of moderate to severe hallux valgus.
Methods: A prospective review of 30 patients (40 feet) that underwent MICA for moderate to severe hallux valgus was conducted. The 28 feet (70%) were classified as severe deformity (hallux valgus angle (HVA) >= 40°and/or first intermetatarsal angle (IMA) >= 18°). Mean followup was 18.6 months. On the anteroposterior weightbearing radiographs, HVA, IMA, lateral shape of metatarsal head (round sign), tibial sesamoid position, and first metatarsal shortening were measured. On the lateral weightbearing radiographs, inclination angle of first metatarsal was measured. American Orthopaedic Foot & Ankle Society hallux metatarsophalangeal-interphalangeal (AOFAS) scores and Self-Administered Foot Evaluation Questionnaire (SAFE-Q) were evaluated preoperatively and at the most recent follow-up.
Results: Mean HVA reduced from 39.3° to 12.8°and mean IMA reduced from 18.6° to 8.4° postoperatively. Incidence of positive round sign of metatarsal head reduced from 57.5% to 5%. Tibial sesamoid position improved from 6.7 to 4.7 using Hardy’s classification. Average first metatarsal shortening was 2.8mm. Inclination angle did not changed significantly, from 20.5°to 21.1°. Mean AOFAS score improved from 65.3 points to 97.9 points. All SAFE-Q subscores also significantly improved postoperatively. There were 5 complications required surgeries: 2 metatarsal screw removals and 3 bone eminence resections. There were some other complications including 3 under-correction cases and one numbness for at least 6 months.
Conclusion: MICA could improve moderate to severe hallux valgus both radiographically and clinically. Accordingly, our results suggest that this procedure provides an effective means of correcting hallux valgus regardless of severity of deformity.
DOI: 10.1177/2473011421S00294
3D Assessment in Posttraumatic Ankle Osteoarthritis
Peter Kvarda; Lukas Heisler; Nicola Krähenbühl, MD; Caspar S. Steiner, MD; Roxa Ruiz, MD; Roman Susdorf, PhD; Yantarat Sripanich, MD; Alexej Barg, MD; Beat Hintermann, MD
Introduction/Purpose: Auto-generated 3-dimensional (3D) measurements based on weightbearing cone-beam computed tomography (CT) scan technology may allow for a more accurate hind- and midfoot assessment. The current study evaluated the reliability and clinical relevance of such measurements in patients with posttraumatic end-stage ankle osteoarthritis.
Methods: Seventy-two patients treated at our institution for posttraumatic end-stage ankle osteoarthritis, with available weightbearing conventional radiographs and a cone-beam CT scan, were analyzed. Twenty healthy individuals aged between 40 and 70 years served as controls. Seven variables were measured on the conventional radiographs (2D) and compared to 3D measurements that were based on reconstructions from cone-beam CT scans. The reliability of each measurement was calculated and subgroups formed according to commonly observed deformities.
Results: Inter- and intraobserver reliability was superior for 3D compared to 2D measurements. The accuracy of 3D measurements performed on osteoarthritic ankles was similar to 3D measurements performed on healthy individuals. Thirty-three of the 72 included patients (46%) evidenced an inframalleolar compensation of a supramalleolar/intra-articular ankle deformity (78% = varus compensation; 22% = valgus compensation), whereas 24 of those 72 patients (33%) showed no compensation or a further increase of a supramalleolar/intra-articular ankle deformity (67% = varus deformity; 33% = valgus deformity).
Conclusion: Auto-generated 3D measurements of the hind- and midfoot are reliable in both healthy individuals and patients with posttraumatic end-stage ankle osteoarthritis. Such measurements may be crucial for a detailed understanding of the location and extent of hindfoot deformities, possibly impacting decision making in the treatment of end-stage ankle osteoarthritis.
DOI: 10.1177/2473011421S00295
High Reliability for Weightbearing CT Based Automated 3D Measurements to Assess Progressive Collapsing Foot Deformity
Peter Kvarda; Nicola Krähenbühl, MD; Roman Susdorf, PhD; Arne Burssens; Roxa Ruiz, MD; Alexej Barg, MD; Beat Hintermann, MD
Introduction/Purpose: In progressive collapsing foot deformity (PCFD), hind- and midfoot deformities are paramount. However, an accurate assessment thereof, using weightbearing radiography, remains challenging. Automated three-dimensional (3D) measurements derived from weightbearing computed tomography (WBCT) scans may provide a more accurate approach for deformity assessment. In this study, automated 3D measurements based on WBCT were compared to two-dimensional (2D) measurements performed on weightbearing radiographs. Furthermore, it was investigated whether various stages of PCFD could be identified using automated 3D measurements.
Methods: Twenty patients treated at our institution with either a flexible (N=10) or rigid (N=10) PCFD were identified, retrospectively analyzed and compared to a control group of thirty healthy individuals. Four angles and two distances measured on weightbearing radiographs were compared to the automated 3D measurements derived from WBCT scans.
Results: In 5 out of 6 variables, the reliability of the measurements derived from weightbearing radiographs was lower than the automated measurements that derived from WBCT scans. The automated 3D measurements showed: the talar tilt in the ankle mortise was more valgus in patients with a rigid PCFD when compared to patients with a flexible PCFD; medial facet subluxation was present in all but one patient; patients with a sinus tarsi impingement evidenced a higher overlap between the talus and calcaneus (12.4+-2.6 mm) compared to patients without impingement (7.8+-3.9 mm; P=0.020).
Conclusion: A higher reliability of automated 3D measurements derived from WBCT scans, was evident for most variables when compared to measurements based on weightbearing radiographs. Besides being less prone to errors, automated 3D measurements may provide more reliable information regarding the hind- and midfoot alignment in patients with PCFD. Future studies may show to what extent 3D measurements could contribute to current diagnostic algorithms and treatment concepts of patients with PCFD.
DOI: 10.1177/2473011421S00296
Are SER-II Ankle Fractures Actually Anatomic? Bilateral CT Demonstrates Subtle Non-Anatomic Mortise & Syndesmotic Alignment in the Setting of Apparent Normal Radiographs
John Y. Kwon, MD; Bonnie Y. Chien, MD; Eitan M. Ingall; Steven Staffa, MS; Caroline Williams, BA; Christopher P. Miller, MD
Introduction/Purpose: Current treatment of ankle fractures is predicated on 1-2 mm of talar shift leading to abnormal contact pressures. Determination of anatomic alignment has conventionally been based on plain radiographs. The ability of x-ray to detect subtle mortise displacement however is unknown. The purpose of this investigation is to determine if CT scan can detect malalignment undetectable utilizing plain radiography when assessing injuries assumed to have anatomic mortise alignment. The findings have implications for utilizing higher resolution diagnostic imaging to assess malalignment and challenging the validity of previous literature in which conclusions of anatomic mortise alignment were determined based on plain radiography.
Methods: 24 patients with stress-negative, stable SER-II type ankle fractures were included. Contralateral ankle mortise radiographs were obtained in addition to static and gravity stress radiographs of the injured side. Bilateral CT scans were performed once patients were deemed to have achieved clinical/radiographic healing. Measurements of the medial clear space (MCS) and syndesmosis were performed by two blinded orthopedic surgeons at two different time points. Intraclass correlation coefficients (ICC) were calculated to evaluate the intra- and inter-rater reliability and consistency of measurements. Statistical analyses were performed to determine any differences between x-ray and CT scan measurements to detect discrepancies between the injured and normal ankle measurements. Statistical significance was defined as a two-sided alpha error of less than 0.05 (p < 0.05).
Results: Despite plain radiographs demonstrating no statistical side-to-side differences and achieving apparent final anatomic alignment in the majority of the cohort, CT MCS on coronal, axial planes and syndesmosis measurements were significantly different when comparing the injured to the normal contralateral ankle by on average of about 0.5mm. There was also excellent intra and interobserver agreement achieved for the measurements.
Conclusion: CT is superior to plain radiography in detecting subtle mortise/syndesmotic displacement and side-to-side differences undetectable by x-ray. These findings challenge conventional assumption of anatomic alignment for SER II injuries and reliance on x-rays to assess anatomic alignment. While injured ankles uniformly demonstrated non-anatomic alignment as compared to the uninjured side, the clinical implications of subtle malalignment are unknown. However, broad reaching implications of this preliminary study include challenging the validity of x-ray to detect possibly clinically-relevant mortise malalignment in patients presenting with isolated lateral malleolus fractures.
DOI: 10.1177/2473011421S00297
A Comparison Between the Bluman et al. Classification and the Progressive Collapsing Foot Deformity Consensus for Flatfeet Assessment
Matthieu Lalevée; Hee Young Lee; Nacime S. Mansur, MD; Edward O. Rojas; Mark S. Myerson, MD; Eric M. Bluman, MD, PhD; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Bluman et al. flatfoot classification (2007) is based on the posterior tibial tendon (PTT) rupture leading to a chronological appearance of several foot deformities. Since then, several discordances have been noted in this concept. An expert consensus met recently to update it. Emphasis on posterior tibial tendon rupture was shifted to a non-chronological approach focusing on five different independent foot and ankle deformations and each deformation’s flexibility or rigidity. This concept, named Progressive Collapsing Foot Deformity (PCFD), was approved with a strong consensus. The aim of this study was to compare Bluman et al. and PCFD classifications. We hypothesize that both classifications will be intra and interobserver reliable and that the PCFD classification will allow a better distribution of the different types of foot.
Methods: We performed a retrospective IRB approved study including 92 flatfeet. Three fellowship trained foot and ankle surgeons studied clinical information and X-rays and classified them in Bluman and PCFD classifications. One performed a blinded second assessment. Bluman classification was analyzed one time as initially described and a second time after removing the Angle of Gissane sclerosis sign. Bluman stage I represents isolated PTT dysfunction, stage II and III Flexible and Rigid Hindfoot Valgus, and stage IV Tibio-Talar Valgus. These stages are progressive and don't allow any combinations. PCFD classifies Hindfoot valgus (A), Midfoot Abduction (B), Forefoot Varus (C), Peritalar Subluxation (D), and Tibiotalar Valgus (E). Combinations of these deformities is allowed. Each deformity can be Flexible (1) or Rigid (2). Interobserver and Intraobserver reliabilities were determined with respectively unweighted Fleiss' and Cohen’s kappa values. Descriptive analysis was performed on the 276 readings to highlight discrepancies between classifications.
Results: Inter and Intraobserver reliabilities were respectively moderate (K=0.55) and substantial (K=0.62) for Bluman and moderate (K=0.56) and very good (K=0.85) for PCFD. The 276 readings were spread into 10 subgroups in Bluman and 64 in PCFD. 2.9% of the flatfeet were classified Bluman stage I, 31.5% stage II, 43.8% stage III and 21.7% stage IV. Bluman stages II and III were mainly composed of PCFD 1ABC (respectively 40.2% and 28.1%). The most represented Bluman subgroup was IIIB (32.6%) whereas after removing the Angle of Gissane sclerosis sign from the classification it was the IIC subgroup (44.2%). PCFD A, B and C were mainly composed of Bluman subgroup IIIB (respectively 35.7%, 43.6% and 36.2%) and PCFD D and E of Bluman subgroup IVB (31.9% and 73.3%).
Conclusion: Both classifications showed moderate reliabilities although the PCFD represented 6 times as many different choices by readers. Bluman stage I was rare, possibly because it is based on PTT dysfunction with little or no deformity. This entity is no longer considered in the PCFD. Bluman stage III, assumed to represent rigid hindfoot varus included numerous flexible PCFD. Main confusion could come from the Angle of Gissane sclerosis sign, which leads to Bluman stage III. This sign is however a sign of extraarticular sinus tarsi impingement which should not lead to a triple arthrodesis as recommended in the Bluman classification.
DOI: 10.1177/2473011421S00298
Comparison Between Cotton Test and Tap Test for the Assessment of Coronal Syndesmotic Instability: A Cadaveric Study
Matthieu Lalevée; Ivan C. Giarola; Victoria Vivtcharenko, BS; Fernando S. Martins; Nacime S. Mansur, MD; Vicenzo Giordano; Andre Wajnsztejn; Shuyuan Li, MD, PhD; Kevin N. Dibbern, PhD; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Diagnosis of subtle instability of the distal tibiofibular syndesmosis is challenging. In surgically treated rotational malleolar fractures, instability is typically assessed with the intraoperative Cotton test. However, this test can be unreliable due to its dynamic nature and uncontrolled distraction force. The Tap test is an alternative test where a cortical tap is advanced through the fibula with a progressive, stable, and unidirectional distraction force. The objective of this cadaveric study was to compare the DTFS widening when using the Cotton and Tap tests as diagnostic tools for coronal plane syndesmotic instability.
Methods: Ten below-knee cadaveric specimens were tested in intact non-stressed, intact stressed, injured non-stressed, and injured stressed conditions, with stressed conditions utilizing both Cotton and Tap tests. In injured conditions, the syndesmotic ligamentous complex was sectioned (anterolateral longitudinal approach). Perfect fluoroscopic Mortise images were acquired for all conditions. For the Tap test, a 2.5 drill bit was used to drill a hole through both distal fibular cortices. A blunt-edged 3.5mm cortical tap was advanced toward the tibia. For the Cotton test, a lateral distraction force was applied to the distal fibula with a towel clamp. Two observers measured Tibiofibular Clear Space (TFCS) 1cm proximal to the ankle joint line. Intra and interobserver reliabilities were assessed by Intraclass Correlation Coefficient (ICC). Syndesmotic TFCS values for all conditions were compared by paired Wilcoxon. Diagnostic performance of the Cotton and Tap tests was assessed (a relative increase of TFCS>2mm). P-values <0.05 were considered significant.
Results: The intraclass correlation coefficient (ICC) for intraobserver and interobserver reliability was respectively, 0.96 and 0.78.TFCS measurements were similar in intact non-stressed, intact stressed (both Cotton and Tap tests) and injured non- stressed conditions: intact non-stressed, 3.5mm (CI, 3.0 to 3.9mm); intact stressed, 3.6mm (CI, 3.1 to 4.1mm) (Cotton test) and 4.0mm (CI, 3.5 to 4.5mm) (Tap test); injured non-stressed, 3.8mm (CI, 3.3 to 4.3mm). TFCS was significantly increased (p<0.0001) in injured and stressed ankles for both Cotton and Tap tests, with values of respectively, 6.2mm (CI, 5.8 to 6.7mm) and 6.1mm (CI, 5.7 to 6.6mm). The Cotton test had 73.3% sensitivity, 100% specificity, and 86.7% diagnostic accuracy. The Tap test had 70% sensitivity, 90% specificity, and 80% diagnostic accuracy.
Conclusion: Our cadaveric study compared the Cotton and Tap tests for detection of coronal plane syndesmotic instability. Both tests demonstrated similar increases in TFCS measurements in stressed injured conditions when compared to intact and injured non-stressed conditions. Additionally, both tests demonstrated similar diagnostic accuracy for coronal plane syndesmotic instability, with slight favor for the Cotton test. In our experience, the Cotton test can be unreliable due to the difficulty in applying a steady distraction force while maintaining a perfect Mortise view. We recommend the Tap test as a more stable, controlled, and reproducible intraoperative diagnostic test for coronal plane syndesmotic instability.
DOI: 10.1177/2473011421S00299
Prevalence and Pattern of Lateral Impingements in the Progressive Collapsing Foot Deformity
Matthieu Lalevée; Nacime S. Mansur, MD; Hee Young Lee; Edward O. Rojas; Francois Lintz, MD MSc FEBOT; Alexandre L. Godoy-Santos, MD; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Lateral impingements, subdivided into Sinus Tarsi (STI), Talo-Fibular (TFI), and Calcaneo-Fibular (CFI) impingements, appear to be associated with the Peritalar Subluxation (PTS) component of the Progressive Collapsing Foot Deformity (PCFD). This is not yet confirmed, as the chronological place of the different types of lateral impingements in PTS is unknown. It is also unclear whether STI are associated with PTS or Midfoot Abduction. Our primary objective was to assess the amount of PTS in STI, TFI and CFI. Our secondary objective was to determine the position of STI among the PTS and Midfoot Abduction deformities. We hypothesized that STI and TFI will be associated with a lower amount of PTS than CFI and that STI will be part involved in both PTS and Midfoot Abduction deformities.
Methods: A retrospective study including 72 PCFD assessed with Weight Bearing Computed Tomography (WBCT) was realized. Patients under 15 or with a previous history of surgery were excluded. Lateral impingements were assessed on WBCT images and subdivided as STI, TFI and CFI. Both direct and indirect signs of impingement were considered positive. The amount of PTS was assessed by the percentage of uncoverage and the incongruence angle of the Middle Facet (MF). Midfoot-Abduction was assessed by Talonavicular coverage angle and global foot deformity by Foot and Ankle Offset (FAO). These data were collected by two independent observers and one performed a blinded second assessment. Interobserver and Intraobserver reliabilities were determined using unweighted Cohen’s kappa values for lateral impingements and using intraclass correlation coefficients for the measurements. Impingement groups were compared using Student’s T-tests for normal, and Mann-Whitney for non-normal variables.
Results: Interobserver and Intraobserver reliabilities ranged from substantial to almost perfect for all assessments. STI was present in 84.7%, TFI in 65.2% and CFI in 19.4% of PCFD cases. PCFD with STI showed significant increases of MF uncoverage (p=0.0001), FAO (p=0.0008) and Talonavicular coverage angle (p=0.0197) compared to PCFD without STI. PCFD with TFI did not show significant difference on measurements compared to PCFD without TFI. PCFD with CFI had associated STI in 100% and TFI in 64.2% of cases. PCFD with CFI showed significant decreases of MF incongruence (p=0.0398) and significant higher FAO (p=0.0058) compared to PCFD without CFI. PCFD with both STI and CFI showed significant decreases of MF incongruence (p=0.032) and significant higher FAO (p=0.028) compared to PCFD with isolated STI.
Conclusion: Our hypotheses have not been confirmed. STI was associated with both PTS and Midfoot Abduction deformities but neither TFI nor CFI were associated with PTS considering MF subluxation. Conversely, CFI was associated with a reduction of the MF incongruence angle despite being associated with a higher global deformity. STI may be associated with earlier PCFD with a concentration of the malignment forces in the subtalar joint whereas CFI may occur later and be associated with a failure of the deep layer of the deltoid ligament and a talar tilt. This could explain the relative reduction of the PTS in CFI.
DOI: 10.1177/2473011421S00300
Short-Term Outcomes of the Lapicotton Technique in the Treatment of Progressive Collapsing Foot Deformity
Matthieu Lalevée; Nacime S. Mansur, MD; Alan G. Shamrock, MD; Hee Young Lee; Eli Schmidt; Victoria Vivtcharenko, BS; Francois Lintz, MD MSc FEBOT; Kevin N. Dibbern, PhD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Medial column instability (MCI) in Progressive Collapsing Foot Deformity (PCFD) is not solely determined by forefoot varus (FV). First ray hypermobility, hallux valgus, midfoot arthritis, gapping at the tarsometatarsal joint and dorsal metatarsal migration are findings associated with MCI. Acknowledgement of this instability requires inclusion of a procedure to the medial column in order to correct the forefoot varus, stabilize the ray and bring the foot to a plantigrade tripod position. Cotton opening wedge medial cuneiform osteotomy and Lapidus tarsometatarsal arthrodesis are procedures of choice in these scenarios. We have combined these 2 procedures into one called Lapicotton. The purpose of this study was to present the short-term outcomes of this technique.We hypothesized that Lapicotton will improve both clinical and radiological outcomes.
Methods: We performed an IRB-approved retrospective study comprising 3 PCFDs having benefited from a Lapicotton procedure. Clinical outcomes were assessed with the European Foot and Ankle Society Score (EFAS), the Foot Function Index Score (FFI) and the Pain Catastrophizing Scale (PCS). Radiographic outcomes were assessed using weight-bearing computed tomography (WBCT) assessments. Middle Cuneiform Floor distance, Forefoot Arch Angle, Middle Facet uncoverage percentage, Talonavicular Coverage angle and the Foot and Ankle Offset (FAO) were measured. All these data were both preoperatively and postoperatively collected. Comparison between preoperative and postoperative results were done as described below. The Kruskal-Wallis H-test for independent groups was used to compare median values of the EFAS. The Wilcoxon signed-rank test for paired samples was used to compare preoperative and postoperative variables of FFI and PCS. For the radiographic measurements, normality was assessed using Shapiro-Wilk test. Comparisons were made using Student tests for normal variables and Mann-Whitney for non-normals.
Results: This small series included 2 female and 1 male, with a mean age of 56 and a mean BMI of 31.8 kg/m2. Mean follow up was 2.9+/-0.2 (range from 2.7 to 3.1) months. 2 out of 3 patients simultaneously benefited of a Medial Calcaneal Displacement Osteotomy (MDCO 10mm) and a Lateral Column Lengthening (LCL 8mm). The wedge sizes used for the Lapicotton were 8 mm in all cases. Regarding clinical outcomes, EFAS (p=0.79) and FFI (p=0.99) did not showed any significant improvement whereas PCS were significantly improved (Δ=-5.67[-9.2--2.2];p=0.03). Regarding radiological outcomes, fusion was present in all the cases at the maximal follow-up. Middle cuneiform floor distance and Forefoot Arch Angle were significantly increase (respectively Δ=6.9;CI95%=[6.4;7.4];p< 0.01 and Δ=7.5;CI95%=[4.3;10.8]p<0.05). Middle Facet uncoverage was significantly improved (Δ=- 28.8;CI95%=[-33.1;-24.5]p< 0.01). Statistical power of the serie did not allowed comparison regarding the Talonavicular Coverage Angle (Δ=-14;CI95%=[-24;-3.9]) and the FAO (Δ=-3.9;CI95%=[-10.7;2.9]).
Conclusion: The Lapicotton procedure showed encouraging outcomes with fusion in all cases at 3 months postoperatively, improvement in pain, correction of forefoot varus and of the of the Peritalar subluxation represented by the Middle Facet Uncoverage. These results should be moderate because other procedures (MDCO and LCL) were performed in 2/3 of the patients, and the outcomes were issued from a small cohort with short-term follow-up. Longer follow-up and a larger cohort are needed to confirm these results.
DOI: 10.1177/2473011421S00301
Functional Outcomes Following Operative Management of Ankle Fractures: Intermediate Length Follow-Up
Scott M. LaTulip, MD; Alexander S. Rascoe, MD; Megan Audet, MD; Heather Vallier, MD
Introduction/Purpose: Ankle fractures are among the most commonly surgically treated orthopaedic injuries, with debate regarding their long-term outcomes and the clinical benefit of contemporary fixation strategies. The purpose of this study was to retrospectively evaluate the functional outcomes of patients following surgical management of ankle fractures, and to determine what, if any, limitations and effects their injury has on their daily lives. The authors of this study hypothesized that despite patients having some degree of measurable impairments, these did not cause meaningful disruption in their everyday lives.
Methods: We retrospectively reviewed a total of 259 patients who underwent surgical management of their ankle fractures between 2004 and 2012. Two separate patient reported outcome measures, the Foot Function Index (FFI) and Short Musculoskeletal Function Assessment (SMFA) were obtained at a minimum of 5 years following time of surgery. Multivariate linear regression analysis was performed to compare FFI and SMFA against several patient and injury specific variables.
Results: A total of 259 patients with ankle fractures were included in the study population. 7 of the demographic and injury- related variables were found to have a statistically significant relationship to both the FFI and SMFA scores. The multivariate linear regression analysis using these 7 variables in addition to both sub-group components of the SMFA to predict the total FFI score yielded an output adjusted-r2 = 0.78. The SMFA dysfunction sub-category was found to correlate with FFI (standardized beta 0.85, p<0.001), but the SMFA bothersome sub-category did not (p=0.866). Ankle pain limiting function and Medicaid insurance status were also predictive of higher FFI scores.
Conclusion: Despite patients, at times, experiencing persistent issues with pain and mild activity limitations following surgical management of ankle fractures, these did not lead to measured burdens in daily activities. At a moderate-length follow-up, patients overall do well from a functional standpoint after sustaining ankle fractures treated surgically.
DOI: 10.1177/2473011421S00302
Correlation of Stress Radiographs to Injuries Associated with Lateral Ankle Instability
Gregory E. Lause, MD; Joshua Sy, DO; Andrew Lopez; J. Banks Deal, MD; Michael Lustik, MS; Paul M. Ryan, MD
Introduction/Purpose: Stress radiographs have demonstrated superior efficacy in the evaluation of ankle instability. The purpose of this study is to determine if there is a degree of instability evidenced by stress radiographs that is associated with pathology concomitant with ankle ligamentous instability.
Methods: A retrospective review of 87 consecutive patients aged 18-74 who had stress radiographs performed at a single institution between 2014 and 2020 was performed. These manual radiographic stress views were then correlated with MRI and operative findings.
Results: A statistically significant association was determined for the mean and median stress radiographic values and the presence of peroneal pathology (p=0.008 for tendonitis and p= 0.020 for peroneal tendon tears). A significant inverse relationship was found between the presence of an osteochondral defect and increasing degrees of instability (p=0.043).
Conclusion: Stress radiographs may assist the surgeon in clinical decision making.
DOI: 10.1177/2473011421S00303
Comparative Assessment of Hallux Rigidus using Conventional Radiograph and Weightbearing CT
Hee Young Lee; Matthieu Lalevee, MD; Nacime S. Mansur, MD; Kevin N. Dibbern, PhD; Amanda Ehret; Connor Maly; Walter C. Hembree, MD; John E. Femino, MD; Victoria Vivtcharenko, BS; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: The etiology of hallux rigidus (HR) is not well understood and Its association with first-ray hypermobility, hallux valgus and metatarsus primus elevatus (MPE) has not been clearly proven. MPE, elevated first metatarsal has been a topic of debate since Lambrinudi`s first description. Recent studies have supported MPE in hallux rigidus by measuring with various methods on wightbearing lateral radiographs, but there are limitations of conventional radiography due to variation in X- ray projection and superimposed metatarsals regardless of the methods of measurement. Our objective was to assess MPE and other associated parameters with hallux rigidus via radiography and WBCT for convergent validity and to evaluate the use of classification system used in conventional radiography with WBCT.
Methods: This is a single-center, retrospective study from prospectively collected data. 20 symptomatic hallux rigidus patient with weightbearing radiograph and WBCT were enrolled from October 2014 to December 2020. Measured parameters included hallux valgus angle (HVA), intermetatarsal angle (IMA), hallux interphalangeal angle (HIPA), distal metatarsal articular angle (DMAA), 1st TMT joint version, First and second metatarsal lengths, Metatarsus adductus angle, 2nd cuneiform-2nd metatarsal angle, Talus-1st Metatarsal Angel, First and second metatarsal declination angles, and MPE. MPE was measured as the direct distance between 1st and 2nd metatarsals (modified Horton index). All patients were graded according to the radiographic criteria of Coughlin and Shurnas classification on radiographs and WBCT, separately. Paired T-test was performed to compare radiographic measurements with WBCT.
Results: Mean age was 55.9, 12 males and 8 females. HVA (15.73 in X-ray vs 14.04 in WBCT), AP first TMT version (16.25 vs 16.47), 2nd cuneiform-2nd metatarsal angle (24.54 vs 26.60), Talus-1st Metatarsal Angel (-7.67 vs -7.89) were not different between radiograph and WBCT. MPE was measured higher in WBCT by 0.86 mm compared to radiograph. First metatarsal declination angle was lower in WBCT by 2.9° indicating increased MPE. When graded with radiographic findings, 5 (25%) patients were grade 1, 5 (25%) patients were grade 2 and 10 (50%) grade 3, when graded with WBCT, 1 (5%) patient had grade 1, 3 (15%) patients were grade 2 and 16 (80%) grade 3. Dorsal subluxation/translation of first metatarsal at first TMT joint was observed 3 (15%) in radiograph and 9 (45%) in WBCT.
Conclusion: HVA, AP first TMT version, 2nd cuneiform-2nd metatarsal angle, Talus-1st Metatarsal Angel demonstrated consistent measurements in radiograph and WBCT. MPE was measured higher in WBCT when measured with direct distance (0.86 mm) between the first and second metatarsals using modified Horton index and first metatarsal declination angle (2.9°). When graded with WBCT, the subchondral cyst in the proximal phalanx and metatarsal head were better delineated leading to higher grade in WBCT. Further studies are needed for inter-rater reliability and discriminant validity of the measurements determined by differences between different groups (HR vs control).
DOI: 10.1177/2473011421S00304
Intra and Inter-Observer Reliability of the New Classification System of Progressive Collapsing Foot Deformity
Hee Young Lee; Nacime S. Mansur, MD; Matthieu Lalevee, MD; Connor Maly; Kevin N. Dibbern, PhD; Mark S. Myerson, MD; Scott J. Ellis, MD; Jonathan T. Deland, MD; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Over the past three decades, the historical notion that adult acquired flatfoot was attributed to posterior tibial tendon dysfunction (PTTD) has been questioned. Advances in the understanding of arch stabilizers and biomechanics of the midfoot joints have led to the new concept of progressively collapsing foot deformity (PCFD). Most recently, the consensus group proposed a new classification system and recommended renaming PTTD to PCFD. The proposed PCFD classification system incorporates the latest understanding of the condition and provides a concise, standardized description of the deformity. To date, there has been no study reporting the frequency of each subclass of PCFD with various combination of deformity components and evaluating intra- and interrater reliability.
Methods: This was a single-center, retrospective study conducted from prospectively collected registry data. 84 patients (92 feet) were assessed between 2014 and 2020. Classification of each patient was made utilizing clinical and radiographic findings by three independent observers. Clinical aspects of the deformity included hindfoot valgus, forefoot/midfoot abduction, forefoot varus deformity, hypermobile medial column, sinus tarsi impingement, peritalar subluxation and valgus tilting of the ankle joint. Radiographic evaluation was focused on Hindfoot valgus (A), increased talar head undercoverage, significant sinus tarsi impingement (B), increased lateral talus-first metatarsal angle, plantar gapping at first TMT/NC joints (C), significant subtalar joint subluxation/subfibular impingement with obliterated joint space (D), and ankle joint valgus tilting with or without arthritic changes (E). Intra- and interrater reliabilities were analyzed with Cohen’s Kappa and Fleiss' kappa respectively.
Results: Mean age was 54.4, 38% male and 62% female. Mean BMI was 33.6 kg/m2. 1ABC (21 feet, 22.8%) was most common subclass followed by 1AC (12 feet, 13%) and 1ABCD (8 feet, 8.7%). Cumulative percent of frequency of 1ABC, 1AC, and 1ABCD was 44.5%. Only a small percentage of patients had an isolated deformity. 58.7% were flexible, 5.5% were rigid, and 35.8% were combined deformities with flexible and rigid components. A was most frequent component (93.5%) followed by C in 88% and B in 71.7%. D was in 29.4% and E was the least frequently observed component in 23.9%. Moderate inter-rater reliability (Fleiss Kappa=0.561, p<0.001, 95% CI 0.528-0.594) was found. E was the most reliable between raters (91.3%) followed by A (79.4%). D was least reliable between three raters (45.7%). Very good intra-rater reliability was found (Cohen`s Kappa=0.851, P<0.001, 95% CI 0.777-0.926).
Conclusion: Most cases predominantly involved hindfoot with various combinations of midfoot and forefoot deformity with/without subtalar joint involvement. This finding suggests most of PCFD exist in combined forms with various deformity components. Despite the limitation of inherent subjectivity, which may account for moderate inter-rater agreement, the new system potentially cover all possible combinations of the deformity in hindfoot, midfoot, forefoot and ankle. This provides a more comprehensive description of PCFD deformity and can guide treatment in a more systematic and individualized manner. Future studies in a larger cohort with advanced imaging are warranted to ascertain reliability and validity of this system.
DOI: 10.1177/2473011421S00305
Weightbearing CT Analysis of Hallux Rigidus: Does Metatarsus Primus Elevatus Really Exist?
Hee Young Lee; Nacime S. Mansur, MD; Matthieu Lalevee, MD; Kevin N. Dibbern, PhD; Connor Maly; Caleb J. Iehl; Walter C. Hembree, MD; Francois Lintz, MD MSc FEBOT; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: The etiology of hallux rigidus has been unknown. Metatarsus primus elevates (MPE), elevated first metatarsal has been controversial. Recent studies have supported significantly elevated first metatarsal in hallux rigidus patients. Bouaicha reported MPE greater than 5 mm could be a predictive factor of hallux rigidus. Lateral weightbearing radiographs has been used to evaluate MPE, However, there are limitations of conventional radiography including variation in X-ray projection angle and foot position and superimposition of metatarsals. Cheung assessed foot alignment utilizing 3D reconstructions from WBCT and concluded that hallux rigidus patients had increased MPE. Our objective was to assess MPE and anatomical characteristics in foot alignment of hallux rigidus patients compared to a control group using WBCT. This is the first study measuring MPE on WBCT.
Methods: This is a single-center, retrospective study from prospectively collected data. 20 patients with hallux rigidus and WBCT data were enrolled from October 2014 to December 2020. As a control group, 20 patients with various foot and ankle pathologies were selected. Measured WBCT parameters included 1st TMT joint version, HVA, IMA, DMAA, 1st and 2nd metatarsal lengths, Foot width, Sesamoid station and rotation angle, 1st-5th Metatarsal Angle, Metatarsus adductus angle, 2nd cuneiform-2nd metatarsal angle, Talus-1st Metatarsal Angel, 1st Metatarsal-Proximal Phalanx Angle, 1st and 2nd metatarsal declination angles and ratio, and MPE. MPE was measured as a direct distance between 1st and 2nd metatarsals using a line tangential to the first metatarsal and another perpendicular line at the metadiaphyseal junction to reach second metatarsal on parasagittal view. A Cut-off value of MPE was calculated using receiver operating characteristic curve. Two investigators independently assessed each WBCT.
Results: Mean age was 43.3 in control group (45% male, 55% female) and 55.9 in HR group (60% male, 40% female). Significant differences were found in several facets of foot anatomy between HR and control groups including HVA (7.57 in control vs 14.05 in HR), DMAA (3.89 vs 8.06), forefoot width (92.96 vs 95.47), 1st MT declination angle (20.17 vs 17.82), 1st/2nd MT declination ratio (83.52 vs 76.02), and MPE (3.24 mm vs 5.40 mm). MPE was significantly higher in hallux rigidus group in all three parasagittal views (unmodified, parallel to 1st metatarsal and 2nd metatarsal). Dorsal subluxation/translation of the first metatarsal was observed at 1st TMT joint in the parasagittal view of WBCT in 9 (45%) patients of hallux rigidus group suggesting sagittal instability. No patient in control group had dorsal subluxation/translation. A cut-off value of MPE was 4.56 mm with 80% sensitivity and 90% specificity.
Conclusion: To evaluate MPE on WBCT, we used a new direct measurement on parasagittal views. We found a significant difference in MPE in HR. Our WBCT results are consistent with other studies using conventional radiographs. A cut-off value of WBCT MPE for diagnosis of HR was 4.56 mm in our cohort. Considering 45% patients of the HR group had dorsal subluxation/translation of first metatarsal at 1st TMT and increased HVA, Hallux rigidus may be associated with first ray instability predominantly in sagittal plane with resultant MPE with varying degree of combined coronal plane instability resulting in increased HVA.
DOI: 10.1177/2473011421S00306
Additional Inferior Extensor Retinaculum Augmentation after All-Inside Arthroscopic Anterior Talofibular Ligament Repair for Chronic Ankle Instability is Not Necessary
Introduction/Purpose: Although several arthroscopic surgical techniques for the treatment of chronic ankle lateral instability (CAI) have been introduced recently, the effect of inferior extensor retinaculum (IER) augmentation remains unclear. The purpose of this study was to compare the clinical outcomes after arthroscopic anterior talofibular ligament (ATFL) repair according to whether additional IER augmentation was performed or not.
Methods: Between 2016 and 2018, we performed a retrospective review of consecutive patients who underwent arthroscopic ATFL repair surgery for CAI. The mean age of the patients was 35.2 years (range, 19-51 years), and the mean follow-up period was 32.6 months (range, 24-48 months). Patients were divided into two groups according to the surgical technique used for CAI: Arthroscopic ATFL repair (group A, n = 37), and arthroscopic ATFL repair with additional IER augmentation (group R, n = 45). The Pain Visual Analog Scale, American Orthopaedic Foot & Ankle Society (AOFAS) score, Foot and Ankle Outcome score (FAOS), and the Karlsson Ankle Functional Score were measured as subjective outcomes, and posturographic analysis was performed using a Tetrax device as an objective outcome. Radiologic outcome evaluations were performed preoperatively and at 2 years postoperatively using stress radiographs and axial view MRI.
Results: Out of 101 patients, 19 (18.5%) were excluded based on the exclusion criteria, and 82 patients were evaluated. We identified a total of six re-tears (7.3%) based on postoperative MRI evaluation. All patients who had ATFL re-tear on MRI (8.1% [3/37] in group A, and 6.7% [3/45] in group R) demonstrated recurrent CAI with functional discomfort and anterior displacement > 3 mm compared to the intact contralateral ankle. All clinical scores and posturography results were improved after surgery in both groups (P < 0.001). However, there were no significant differences in the clinical results and radiologic findings between the two groups.
Conclusion: The clinical and radiologic outcomes of patients with CAI improved after all-inside arthroscopic ATFL repair. However, additional IER augmentation after arthroscopic ATFL repair did not guarantee better clinical outcomes.
DOI: 10.1177/2473011421S00307
Noninvasive Skin Expansion Strips to Decrease Wound Issues after Total Ankle Replacement
James Lendrum; S. Blake Wallace, MD; Mary C. Hamati, MD; Lindsey Schultz; Joshua A. Metzl, MD; Daniel K. Moon, MD, MS, MBA; Kenneth J. Hunt, MD
Category: Ankle; Ankle Arthritis; Basic Sciences/Biologics; Other
Introduction/Purpose: Total ankle arthroplasty through the anterior approach (TAR-AA) is an increasingly popular treatment for ankle arthritis. This approach carries significant risk for wound complications. Several products have been investigated to mitigate this risk, but these are either costly or invasive. Noninvasive skin expansion strips (NSESs) have two nonelastic adhesive strips, one on either side of the incision, with an elastic band connecting them. These were designed to induce new skin growth at the edges of the strips for plastic surgery applications. In the postoperative setting, the NSES functions to transfer tension away from the site of the incision to the edge of the strips. We hypothesize that postoperative application of NSESs will decrease unplanned clinic visits and wound complications after TAR-AA.
Methods: This is a prospective cohort study with retrospectively identified historical controls designed to evaluate the effectiveness of NSESs. Prospectively enrolled patients undergoing TAR-AA at a single institution (3 surgeons) received application of NSESs in the operating room after routine wound closure. At their two-week postoperative visit, each wound was assessed and new NSESs were applied. No other changes were made to the surgeons' wound closure technique, immobilization, follow-up cadence, or rehabilitation protocols. Patients following up with providers outside the institution were excluded. Thirty five consecutive historical controls were identified for comparison. Primary outcomes included (1) Additional clinic visit required for wound assessment or suture removal, (2) superficial wound complication before 8 weeks, and (3) deep infection before 8 weeks. Z-score test was used to calculate statistically significant (p<=0.05) differences between the two groups.
Results: To date, 20 patients (62.5 +- 11.8 years; 6 females, 14 males) received application of NSESs. Baseline demographics did not differ significantly from our 35 consecutively identified historical controls (62.2 +- 13.3 years; 16 females, 19 males). Additional clinic visits for suture removal were needed for 15% (3/20) of patients in the treatment group compared to 46% (14/35) of patients in the control group (p=0.021). There were significantly fewer unplanned visits per patient in the treatment group compared to the control group (0.15 vs. 0.54, p=0.004). The superficial wound complication rate in the treatment group vs. control group was 0% and 11%, respectively (p=0.12). There were no deep infections in either group.
Conclusion: Noninvasive skin expansion strips are an effective means to improve early wound healing and decrease unplanned clinic visits for wound checks or delayed suture removal after TAR-AA. There was a trend toward significance for NSESs decreasing superficial wound complications. Further high volume studies are needed to clarify their cost effectiveness and effect on deep infections.
DOI: 10.1177/2473011421S00308
The Metatarsal Cortical Index as an Indicator of Insufficiency Fracture of the Foot
Christopher G. Lenz; Constance Raith; Lukas Urbanschitz; Timo O. Tondelli; Karim Eid; Richard Niehaus; Sandro Hodel
Introduction/Purpose: The diagnosis of metatarsal stress fractures is challenging. Standard imaging often shows false negative results. The aim of this study was to create reliable radiologic outcome parameters to predict insufficiency fractures of the metatarsals
Methods: We performed an age- and sex-matched case-control study of patients with (n = 18) and without insufficiency fracture (n = 18) of the foot. To measure the ratio between the outer cortical border and the endosteal diameter, the MCI was developed as a novel radiographic measurement on dorsoplantar images. The MT was divided into thirds, and the width from the outer cortical border to the endosteal diameter was measured at the junction of the proximal to the middle third (proximal), at the midshaft (middle), and at the junction of the middle to the distal third (distal). The metatarsal cortical index (MCI) for each metatarsal was developed to predict an insufficiency fracture. The MTs were sequentially numbered as MT I-V. To correct for potential bias due to MT length, the Coughlin index and Maestro method were used in all patients.
Results: The MCI of each metatarsal was significantly decreased in the insufficiency fracture group compared with the control group (p <.01). The MCI of the fourth ray yielded the highest area under the curve among the analyzed MCI values (area under the curve, 0.79; 95% confidence interval, 0.61-0.90). A cut-off value of 1.62 for the MCI of the fourth ray yielded a sensitivity of 78% and a specificity of 78% to predict insufficiency fracture of the foot (odds ratio, 12.25; 95% confidence interval, 2.54-58.97), and enabled accurate allocation to the insufficiency fracture group versus the control group in 74% of cases.
Conclusion: A decreased MCI is associated with metatarsal insufficiency fractures and enables an accurate diagnosis in three out of four cases. Despite the highly variable anatomy and morphology of the MTs, we were able to show that the MCI is a reliable tool to determine insufficiency fracture of the MT on plain radiography. The MCI might aid clinicians in identifying insufficiency fracture, and raise the suspicion of the diagnosis without additional imaging studies.
DOI: 10.1177/2473011421S00309
Does Sagittal Tibiotalar Alignment of TAR Predict Failure?
Anna-Kathrin Leucht, MD; Peter Salat; Phinit Phisitkul, MD; Annunziato Amendola, MD; John E. Femino, MD; Andrea N. Veljkovic, MD, MPH, FRCSC
Category: Ankle Arthritis
Keywords: Total Ankle Arthritis; Total Ankle Arthroplasty; Total Ankle Replacement
Introduction/Purpose: The long term outcome of total ankle replacement is contingent on restoring the anatomic tibiotalar alignment of the ankle joint. Prior studies have mainly looked at the effect of coronal and hindfoot alignment of TAR on outcome and failure with few studies focusing on the effect of sagittal tibiotalar alignment. From these, we know that sagittal alignment has a greater impact on joint mechanics and that proper positioning of the talar component in the sagittal plane results in greater postoperative pain relief and better functional outcome, especially ankle range of motion. The goal of this study was to define a sagittal radiographic value that predicts failure in TAR.
Methods: We analyzed the data of a retrospective patient cohort of consecutive TAR patients, which were treated from 2004 and 2011. Patients with two types of prosthesis were included, Salto Talaris (fixed bearing) and STAR (mobile bearing). All measurements were completed by two blinded observers, including the sagittal distal tibial articular angle (sDTAA), the lateral talar station (LTS) and the talar component inclination angle (γ angle). A total of 90 patients were included, 51 were male and 39 female patients. Seventy-seven patients received a Salto and 13 patients a STAR prosthesis. The average age was 63.7 years.
Results: The mean sDTAA was 83.9 degrees and the mean γ angle was 21 degrees, both without significant difference in the two different prosthesis designs. A significant association (p=0.03) between post-op LTS as a continuous variable per unit increase and clinical failure was demonstrated, which included all the revision cases, with an odds ratio of 1.25. In addition a significant association (p=0.03) between increased LTS and sDTAA change of >5°, which is indicative of anterior subsidence, was shown. This was associated with an odds ratio of clinical TAR failure of 1.27.
Conclusion: The abnormal radiographic post-op lateral talar station appears to predict clinical TAR failure and correlates with the abnormal sDTAA; the anterior translated talus loads the anterior tibia leading to anterior subsidence of the prosthesis. Limitation of this study is the inclusion of two different types of prosthesis designs.
DOI: 10.1177/2473011421S00310
Proximal Phalanx Osteotomy in Percutaneous Correction of the Lesser Toe Deformities: A Cadaver Study
Anna-Kathrin Leucht, MD; Martin J. Wiewiorski, MD; Miki Dalmau-Pastor, PhD; Alexandro Pellegrino, MD
Introduction/Purpose: The correction of lesser toe deformities has been traditionally performed in an open fashion. With minimal-invasive foot surgeries becoming increasingly popular, correction of lesser toe deformities via percutaneous soft-tissue procedures and osteotomies is frequently performed. The aim of this study was to evaluate the site of percutaneous proximal phalanx osteotomy of the lesser toes in relation to the metatarsophalangeal joint line when performed without fluoroscopy guidance.
Methods: In this experimental cadaver study, the metatarsophalangeal joints of the lesser toes of 20 cadaver samples (=80 toes) were palpated. A plantar skin stab incision was made just distal to the joint line without fluoroscopic control. Plantar closing osteotomies of the proximal phalanx were performed with a Shannon burr. Adorsoplantar view was taken with fluoroscopy. The location of the osteotomy and the relative distance from the metatarsophalangeal joint line was evaluated.
Results: The majority (78/80; 97.5 %) of the osteotomies were localized in the metaphyseal region. No osteotomy violated the metatarsophalangeal joint.
Conclusion: Percutaneous osteotomy of the proximal phalanx of the lesser toes guided by palpation without using the image intensifier is a safe procedure and does not violate the metatarsophalangeal joint.
DOI: 10.1177/2473011421S00311
Surgical Outcome of Hindfoot Fusion using a Retrograde Hindfoot Fusion Nail
Anna-Kathrin Leucht, MD; Andrea N. Veljkovic, MD, MPH, FRCSC; Kevin J. Wing, MD, FRCSC; Murray J. Penner, MD, FRCSC; Alastair S. Younger, MB ChB, ChM, FRCSC
Introduction/Purpose: TTC fusions are often performed as a salvage procedure in patient with severe hindfoot arthritis or hindfoot deformity. Comorbidities in this patient collective are frequent, leading to increased risk of postoperative complication. The purpose of this study was to evaluate the surgical outcome regarding union rate, reoperation rate and adverse events using a retrograde hindfoot fusion nail.
Methods: Patient records of a single center were retrospectively reviewed in which a retrograde hindfoot fusion nail was utilized for hindfoot fusion between July 1st, 2009 and August 31st, 2018. These records included age, gender, BMI, comorbidities, indications for surgery, non-union, re-operation rates and adverse events related to the surgery. The fusions were performed by 4 fellowship trained foot and ankle surgeons at a tertiary care teaching hospital. 58 cases were identified consecutively, in 51 cases a TTC fusion was performed, in 7 cases a tibiotalar fusion with preexisting talocalcaneal fusion. 22 fusions were arthroscopic and 36 open. The average age of patients was 59 years, the average BMI 29. Main indication for the hindfoot fusion were arthritis (55%) and complex hindfoot deformity (43%).
Results: An overall union rate of 89.66% was achieved, 5 non-union tibiotalar and 1 non-union tibiotalar + talocalcaneal was documented. In the group of arthroscopic fusion the non-union rate was 9.09%, in the open group 11.11% respectively. The non- union group included patient with elevated BMI (50%), Diabetes mellitus (33%) and smoking (33%). Adverse events were documented in 21%. The reoperation rate was 17%, mostly due to deep infection or wound complication requiring surgical debridement. No patient in the arthroscopic fusion group needed a reoperation due to deep infection or wound complication, whereas in open surgery this rate was 27.78%.
Conclusion: A union rate of 89.66% was achieved using a retrograde hindfoot fusion nail in a high risk patient population for non- union. Arthroscopic preparation of the tibiotalar and the subtalar joint seem to prevent postoperative wound complications.
DOI: 10.1177/2473011421S00312
What are the Risk Factors for Infection after Operative Treatment of Subtalar Fracture Dislocations?
Eli Levitt, MS; David A. Patch, MD; Michael D. Johnson, MD; Ryan McLynn; Henry DeBell, BS; James B. Harris; Clay A. Spitler, MD
Category: Ankle; Trauma
Keywords: Ankle Fracture; Wound Complications; Foot and Ankle Infection
Introduction/Purpose: Subtalar fracture dislocations are a rare hindfoot injury with relatively little evidence to inform surgeons about outcomes and risk factors for complications. Some previously documented poor prognostic factors include lateral and complicated dislocations, total talar extrusions, and concomitant fractures. The mechanism of injury often results from high energy trauma and has been reported as severe inversion (medial dislocation) or eversion (lateral dislocation) of the foot. The purpose of this study was to assess the risk factors associated with deep infection after operative treatment of subtalar fracture dislocations.
Methods: A retrospective cohort study at a single level 1 trauma center was performed to identify patients who had operative treatment of a subtalar fracture dislocation over an 11 year period (2008-2019). Patients were identified by review of the electronic health record and data collected included patient demographics, injury characteristics, and treatment choices. Deep infection was defined as return to the operating room for debridement. Minimum follow-up for inclusion was 3 months. Descriptive analyses (means, medians, standard deviations, ranges, frequency distributions) were used to assess and describe the group. Chi-square tests of association and independent-sample t tests were used to assess differences between the infected group and those without infection.
Results: A total of 154 met criteria for this study. The most common associated fractures were talus (47%) and calcaneus (33%). Approximately every 1 in 8 patients (12.3%) patients developed a deep infection. The infected group was older (47.2 vs 39.5 years, p=0.03). Tobacco users were found to have a significantly higher rate of postoperative deep infection (74 vs 34%, aOR=7.4, 95% CI, 2.3-24.1, p=0.001). There was a significantly higher proportion of infection in patients with Gustilo-Anderson type 3 open fractures (32 vs 12%, aOR=5.7, 95% CI, 1.6-20.3, p=0.007). The infected group had a higher proportion of below the knee amputation (47 vs 1%, p<0.001).
Conclusion: Infection after operative management of subtalar fracture dislocations can be devastating, with 47% of infected patients requiring amputation. Risk factors for infection after subtalar fracture dislocation include older age, smoking, type 3 open fracture, and freshwater contamination. Ultimately demographic and injury characteristics seem to drive the risk of infection in subtalar fracture dislocations.
DOI: 10.1177/2473011421S00313
Surgical Treatment Outcomes of Achilles Tendon Rupture and Tendinosis Augmented with Synthetic Graft
Jeffrey A. Levy, DO; Steven K. Neufeld, MD; Thomas H. Sanders, MD; Daniel J. Cuttica, DO
Introduction/Purpose: Surgical treatments for Achilles tendon ruptures (ATR) or insertional Achilles tendinitis (IAT) traditionally have prolonged postoperative recoveries. Patients are typically kept non-weight bearing or protected weight bearing on the operative extremity for weeks after surgery to protect the repairs. The purpose of this study is to show that augmentation of typical Achilles tendon repairs with a synthetic scaffold is safe, allows for early weight bearing while preserving functional outcome and has a high patient satisfaction.
Methods: A retrospective chart review was performed on all patients surgically treated for ATR or IAT from 2018 - 2020. The surgeries were performed by two fellowship trained Foot and Ankle Orthopaedic surgeons. All repairs were augmented with a synthetic scaffold made of polycaprolactone-based polyurethane urea (PUUR). Achilles tendon ruptures were direct end-to-end repairs and IAT repairs were performed with double row biocomposite anchors in the calcaneus after a calcaneus exostectomy. Exclusion criteria included flexor hallucis longus transfer, non-insertional achilles tendinosis, patients undergoing additional surgical procedures, and ATR or IAT repairs not treated with PUUR. Patients were evaluated as a cohort as well as acute ruptures, chronic ruptures (defined as more than 6 weeks old), and IAT subgroups. Primary outcomes were date of weight bearing and patient satisfaction. Secondary outcomes were final strength and ankle dorsiflexion. The Wilcoxon signed-rank test (WSR) was used to compare baseline and final follow-up NRS scores.
Results: A total of 33 patients met the inclusion criteria with 12 ATR (9 acute and 3 chronic) and 21 IAT. Mean follow-up length was 150 days (43 - 314). Mean weight bearing began on postoperative day (POD) 7.33 (6-13) for acute ruptures, 14.33 (6-19) for chronic ruptures, and 9.9 (5-42) for IAT. Patient satisfaction, based on a binary yes/no response at final followup, was obtained on 27 of 33 patients with 92.6% positive indicating satisfaction with surgical outcome. Final strength averaged 5/5 for 83.9% and 4/5 for 16.1% of all patients. Final active dorsiflexion of at least 10 degrees was obtained in 93.5%. Mean numerical rating scale (NRS) for pain significantly decreased from 5.2 to 0.6 for all patients (WSR p<0.001). No patients had loss of fixation or had a re-rupture. Complications included one patient with sural neuritis and another with minor wound breakdown that did not require surgical intervention.
Conclusion: Augmentation of Achilles tendon ruptures and insertional Achilles tendonitis with PUUR graft is safe, allows for early weight-bearing, has a high patient satisfaction and has acceptable functional outcomes in regards to strength and motion.
DOI: 10.1177/2473011421S00314
Five-Factor Modified Frailty Index as a Predictor of Complications Following Total Ankle Arthroplasty
Lauren Lewis, MD; Daniel Jupiter, PhD; Vinod K. Panchbhavi, MD, FACS; Jie Chen, MD, MPH
Introduction/Purpose: Ankle arthritis can significantly diminish the function and quality of life of affected individuals. Treatment options for end-stage ankle arthritis include total ankle arthroplasty (TAA). Ongoing research seeks to identify patient factors associated with a higher risk of post-operative complications following TAA. A 5-item modified frailty index (mFI-5) has been found to predict adverse outcomes of multiple orthopaedic procedures. The aim of this study was to evaluate the suitability of the mFI-5 as a risk stratification tool for patients undergoing TAA.
Methods: A retrospective review of the National Surgical Quality Improvement Program (NSQIP) database was performed on patients undergoing TAA between the years of 2011 and 2017. Data on patient demographics, post-operative complications, and length of stay were collected. Bivariate analysis and multivariate logistic regression were subsequently performed to investigate frailty as a possible predictor of post-operative complications.
Results: 1035 patients were identified (mean age = 63.9 years). Complication rates significantly increased with increasing mFI-5 score, from 5.24% in patients with no mFI-5 variables to 19.38% in patients with two or more mFI-5 variables present (P <0.0001). When comparing patients with an mFI-5 score of 0 to patients with an mFI-5 score of 2, 30-day readmission rate increased from 0.24% to 3.1% (P> 0.017), length of stay increased from 1.79 days to 2.18 days (P >0.007), adverse discharge rate increased from 3.81% to 15.5% (P <0.0001), and wound complications increased from 0.24% to 1.55% (> 0.02). After controlling for demographic factors, length of stay, and operative time, mFI-5 score remained significantly associated with patients' risk of developing any complication and 30-day readmission rate.
Conclusion: Frailty as defined by the mFI-5 is associated with adverse outcomes following TAA. Implementing the mFI-5 as a risk stratification tool may assist in identifying patients who are at an elevated risk of sustaining a complication, and may allow for improved informed decision-making and perioperative care when considering TAA.
DOI: 10.1177/2473011421S00315
Peritalar Subluxation: A Key Finding for Both Cavovarus and Flatfoot Deformities
Shuyuan Li, MD, PhD; Mark S. Myerson, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Peritalar subluxation in both the talonavicular and subtalar joints has been described as characteristic markers for adult acquired flatfoot deformity (AAFD). However, no study has reported these changes in in cavovarus deformity, and we postulated that peritalar subluxation would apply to both the AAFD as well as the cavovarus foot deformity but in different directions using the same markers. Furthermore, the use of calcaneocuboid (CC) joint subluxation as an additional marker for peritalar subluxation has never been investigated in either flatfoot or cavovarus deformities. This study used three dimensional images of weightbearing cone beam computed tomography (WBCT) to evaluate the alignment of the peritalar joints in feet with normal, varus and valgus hindfoot alignment.
Methods: WBCT scan images and medical charts of 400 patients were retrospectively reviewed. Thirty cavovarus and 15 flexible AAFD feet were chosen as the study groups. Fifteen feet without deformities and arthritis, a history of trauma or surgery in both the hindfoot and ankle were chosen as controls. Hindfoot moment arm (HMA), Foot and ankle offset (FAO) were used to assess hindfoot alignment. Middle facet subluxation (MFS), talonavicular joint coverage angle (TNCA), and calcaneocuboid joint subluxation (CCS) were used as markers of peritalar subluxation. The talocalcaneal (Kite’s) angle in the axial plane was used to demonstrate the relative position between the talus and the calcaneus. The arch height index in the sagittal plane was used to assess medial arch height. Positive was used to reflect lateral subluxations while negative for medial ones. Correlations between HMA, FAO and each of the above three peritalar subluxation parameters were assessed by bivariate linear regression.
Results: Patients in both the cavovarus and the AAFD groups showed totally different hindfoot alignment, peritalar subluxation and the height of the medial arch compared to the control group. In the order of Cavovarus, AAFD, and Control, the mean HMA- CR values were -20.43mm, 14.02mm, and 0.03mm, respectively; HMA-WBCT values were -6.34mm, 15.75 mm, and 3.19 mm; FAO values were -11.17%, 7.42%, and 2.63%; TNCA were -16.8 degrees, 22.11, and 6.45; The MFS values were -17%, 42%, and 22%; CCS values were -21% (IQR=-35%,-0.17%), -7% (IQR=-11%, 0) and 0 (IQR=-4%, 5%); The Kite’s angles were 22.19 degrees, 34.27 degrees, and 28.06 degrees; The arch height index values were 0.25, 0.71, and 0.44. There was a statistically significant difference among the three groups in all the above parameters. There was a strong positive linear correlation between each parameter of the peritalar subluxation marks with both hindfoot moment arm and FAO.
Conclusion: This is the first study to bring the concept of peritalar subluxation to cavovarus deformity assessment, proving that peritalar subluxation is a key characteristic in both flatfoot and cavovarus foot deformities. The two deformities are pathologically completely different, and as expected, markers of peritalar subluxation were in opposite directions. The use of calcaneocuboid joint subluxation as additional marker of perisubtalar subluxation is novel to assess both deformities. The findings of this study will provide useful guidelines for future clinical evaluation and decision making in treating patients with either varus or valgus hindfoot deformities.
DOI: 10.1177/2473011421S00316
Validation and Reliability of the Progressive Collapsing Foot Deformity (PCFD) Classification
Shuyuan Li, MD, PhD; Mary C. Hamati, MD; Mingjie Zhu; Kenneth J. Hunt, MD; Cesar de Cesar Netto, MD, PhD; Mark S. Myerson, MD
Category: Midfoot/Forefoot; Other
Keywords: AAFD; PTTD; Cavovarus Foot Deformity
Introduction/Purpose: Recently, a group of experts proposed Progressive Collapsing Foot Deformity (PCFD) as a new terminology to describe better the complexity of this pathology, as well as a new staging system based on rigidity and different patterns of deformity. The proposed system (Table 1) better incorporates recent data and understanding of the condition, better allowing for standardization of reporting, and guiding treatment decision-making to achieve optimal outcomes. The classification includes two Stages: flexible (1) and rigid (2) deformity each of which may or may not be associated with five subclasses of deformity including hindfoot valgus (A), midfoot abduction (B), forefoot supination (C), peritalar subluxation (D), and ankle valgus instability (E). This paper aims to determine the reliability and the validity of the PCFD classification system.
Methods: This is a survey-based study distributed through REDCap. Participants were provided with video and case examples explaining how the classification system is used. Three groups of surgeons (Group 1 fellows in training, Group 2 surgeons in practice for 1-4 years, and Group 3 in practice 5 years or more) classified 20 cases of PCFD. Correct response rates for the 20 cases, and subclasses and substages of each individual case were calculated. The mean and 95% confidence interval were used to describe normally distributed numerical data. Values of the above parameters were compared among the three different groups using Tukey-Kramer HSD test of Oneway ANOVA. P<0.05 was considered statistically significant.
Results: Ninety-four of 113 returned surveys were completed and included in the analysis. There were 18 in Group 1, 23 in Group 2, and 53 in Group 3, with significantly different overall correct diagnosis rates (75.8%, 51.7%, and 37.6% respectively). There was no significant difference among the three groups with regard to the correct response ratio of different Stages. The correct response rates for each Class of deformity were 96.62% (95% CI=94.02%, 99.23%) for Class A (hindfoot valgus); 77.66% (95% CI=75.06%, 80.26%) for Class E (ankle instability); 87.98% (95% CI=85.38%, 90.58%) for Class B (midfoot abduction), 87.99% (95% CI=85.39%, 90.60%) for Class C (forefoot supination) and 57.29% (95% CI=54.70%, 59.90%) for Class D (peritalar subluxation), with the correct response rates of Class A, B, C and E being significantly higher than that of Class D.
Conclusion: Three groups of surgeons with varied experience demonstrated a higher accuracy of responses for hindfoot valgus, and ankle instability and a lower accuracy for midfoot abduction, forefoot supination and peritalar subluxation. The classification as presented to the reviewers provided sufficient information to guide accurate decision making for correct responses, however some classes of deformity, in particular peritalar subluxation may have been poorly defined in the clinical presentations and may require more clinical and radiographic information to guide decision making for correct classification.
DOI: 10.1177/2473011421S00317
Ankle/Hindfoot Arthrodesis as a Salvage Procedure for Failed Total Ankle Arthroplasty
Jung-Won Lim, MD; Won Tae Song, MD; Hong-Geun Jung, MD, PhD; Jemin Im
Category: Ankle; Hindfoot
Keywords: TTC; Tibiotalocalcaneal Arthrodesis; Total Ankle Arthroplasty
Introduction/Purpose: High failure rate after total ankle arthroplasty (TAA) in 10-year follow-up has been reported, ranging from 10 to 20%. Massive bony destruction after TAA often caused by periprosthetic osteolysis, implant subsidence or loosening, or periprosthetic infection, and it would be considerable challenge to many orthopedic surgeons. In some cases, it is difficult to perform revision arthroplasty. For failed TAA, ankle/hindfoot arthrodesis can be performed as a salvage procedure. In this study, we evaluate the clinical and radiologic outcomes of the ankle/hindfoot arthrodesis in patients with failed TAA.
Methods: Ankle/hindfoot arthrodesis was performed in 10 ankles with failed TAA from October 2003 to March 2019 (at least 6- month follow-up). As for the clinical evaluation, visual analogue scale (VAS) pain scores, and American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scores were assessed. Postoperative complications such as skin necrosis, surgical site infection (SSI), or non-union were reviewed through medical records. Radiographs including CT images at last follow-up were assessed to confirm bone union.
Results: The average follow-up was 49.1 months (range, 7-89). There were 6 cases performed with tibiotalocalcaneal (TTC) arthrodesis, and 4 cases with ankle arthrodesis. The operations were performed at mean postoperative 46.6 months (range, 8- 178) from index TAA. Allo-femoral head structural bone graft was used in 9 cases, and auto proximal tibia cancellous bone graft was used in 5 cases. Mean VAS pain score decreased from 7.6 pre-operatively to 2.2. AOFAS score increased from 15.6 to 42.0 (subjective assessment only; maximum score=68). 3 revision surgeries had been performed after initial arthrodesis (1 case for SSI, 2 cases for non-union), and bone union was obtained in 2 cases (1 case of SSI, 1 case of non-union).
Conclusion: Ankle/hindfoot arthrodesis after failed TAA can be optimal surgical option for the patients with massive bony destruction which compromises revision arthroplasty. It acts as a salvage procedure for failed TAA and could yield favorable outcome.
DOI: 10.1177/2473011421S00318
Comparison of the Outcome of the 3-Component Salto Total Ankle Arthroplasty for Ankle with Preoperative Varus, Valgus and Neutral Alignment in End-Stage Osteoarthritis
Jung-Won Lim, MD; Hong-Geun Jung, MD, PhD; Jemin Im
Category: Ankle; Ankle Arthritis
Keywords: Ankle Arthritis; Total Ankle Arthroplasty; Total Ankle Replacement
Introduction/Purpose: As the popularity of total ankle arthroplasty (TAA) increases, indication of TAA also expands. Recently, the ankles more than 20° of varus or valgus deformity in the coronal plane are treated with TAA. However, severe varus or valgus deformity should be corrected in the coronal plane to avoid residual mal-alignment that leads to instability, insert wear, and clinical failure. In this study, we compare the clinical and radiologic outcome of the Salto mobile bearing 3-component total ankle prosthesis for ankles with preoperative varus, neutral, and valgus alignment.
Methods: TAA was performed in 101 consecutive ankles (99 patients) by a single surgeon using 3-component Salto total ankle implant from June 2014 to October 2019. A prospectively collected database was used to identify all patients who underwent primary TAA with a minimum 1-year follow-up. We classified the enrolled ankles as neutral, varus, or valgus groups. More than 10° of tibial anterior surface angle, talta tilt angle, tibial axis-talar dome angle, talar dome-ground surface angle (TD-GSA), or tibio- calcaneal angle was defined as varus or valgus groups. All patients were followed up at postoperative three months, six months, at one year and yearly thereafter. Clinical outcome scoring was done pre-operatively and post-operatively. American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot functional score, pain VAS, satisfaction score and clinical range of motion (ROM) were collected along with weight-bearing radiographs of the ankle. Post-operative coronal alignment of the component were evaluated with radiographs.
Results: The average follow-up was 21.6 months (range, 12-71). Preoperatively, there were 63 ankles (62%) with varus deformity, 27 ankles (27%) with neutral alignment, and 11 ankles with valgus deformity. In preoperative varus group, 13 ankles (21%) were performed with concomitant lateral sliding calcaneal osteotomy, and 23 ankles (37%) with deltoid release. No additional procedures for the correction of ankle and hindfoot deformity were performed in preoperative neutral and valgus groups. VAS pain score and AOFAS score were significantly improved in all groups (p < 0.05). Overall satisfaction rate was 88%. After TAA, there were no significant radiologic alignment among the groups (3.9° (range, 0.7°~9.7°) in varus group, 4.1° (range, 0.4°~6.8°) in neutral group, and 2.2° (range, -0.4°~4.4°) in valgus group; p > 0.05).
Conclusion: There was no significant difference in outcome among the varus, neutral, and valgus groups postoperatively in the TAA series using single Salto 3-componenet implant. Postoperative neutral alignment was achieved in all ankles. For favorable long-term outcomes, coronal alignment should be corrected with proper additional procedures in TAA.
DOI: 10.1177/2473011421S00319
Suture Pullout in Human Cadaveric Skin: Evaluation of HEMIGARD® Augmentation vs Suture Alone
Introduction/Purpose: Closure of high-tension surgical wounds is a challenge frequently encountered during surgical procedures. The use of a novel adhesive augmentation device, HEMIGARD, has been proposed to decrease tension on wound closure and thereby increase the amount of force needed for suture pullout. In principle, this may help prevent wound dehiscence, skin edge necrosis and the sequelae thereof. We hypothesized that HEMIGARD augmentation of suture placement would require more force for suture pullout from human cadaveric lower extremity skin when compared to suture alone.
Methods: In this study, HEMIGARD with suture was compared to suture alone on leg and foot measurements from four cadavers. One side of the incision was used to test the HEMIGARD according to the manufacturer’s instructions. The other side of the same incision was used to test the same suture material, passed without HEMIGARD, to allow for direct comparison. A force gauge was used to measure the Newtons of force required for suture pullout. A total of 30 measurements were recorded per cadaver; 15 using HEMIGARD and 15 using suture alone.
Results: No difference was observed between HEMIGARD and suture alone in the amount of force required for suture pullout. When excluding instances of HEMIGARD adhesive failure, which occurred in 67% of measurements, the HEMIGARD was found to be superior to suture alone in the cadaveric foot, but not in the leg.
Conclusion: The amount of force required for suture pullout from human cadaveric lower extremity skin did not significantly differ when using HEMIGARD augmentation of suture placement versus using suture alone. However, when excluding instances of HEMIGARD adhesive failure, the HEMIGARD may be superior to suture alone in the cadaveric foot, but not in the cadaveric leg.
DOI: 10.1177/2473011421S00320
A Systematic Review of Third-Generation Total Talus Replacements
Benjamin B. Lindsey, MD; Benjamin B. Lindsey, MD; Shumaila Sarfani, MD; Clayton C. Bettin, MD
Introduction/Purpose: Total talus replacement (TTR) has emerged as a novel treatment for talar avascular necrosis and severe trauma to the talus. Despite TTR first being described over 35 years ago, many questions still remain regarding the procedure.
The objective of this study was to summarize the evidence on third-generation TTR’s, focusing on surgical indications, surgical technique, prosthesis design, clinical outcomes, and postoperative complications.
Methods: MEDLINE and EMBASE were queried and data abstraction was performed by 2 independent reviewers. Inclusion criteria for the articles were (1) peer-reviewed clinical studies with levels of evidence from I to IV, (2) with at least 5 patients, (3) reporting clinical outcomes of third-generation TTR’s that were not done in conjunction with a total ankle arthroplasty, and (4) with a minimum clinical follow-up of at least 6 months.
Results: Five studies met inclusion criteria for analysis including 101 ankles in 97 patients. The mean reported patient age was 52.8 years. The most common indication for TTR was avascular necrosis (86%), followed by trauma (10%), and tumor (4%). The mean follow up was 40 months. 98% of TTR’s were performed through an anterior approach. There was significant variation in implant material, with 60% alumina ceramic, 27% cobalt chromium, 9% titanium, and 4% stainless steel. Only 3 studies obtained preoperative outcome measures, but these all demonstrated improvement at final follow up. Average dorsiflexion after TTR was 6.1 degrees and average plantarflexion was 35.1. Only 5% of ankles had complications requiring return to the operating room and only 2% of the total taluses were revised.
Conclusion: While evidence is limited, short-term and mid-term results are promising for TTR as it demonstrates improvement in ankle function and has a low rate of revision. As the consequences of failure of a TTR are significant, including pantalar fusion or below knee amputation, higher quality studies and long-term results are needed to further evaluate this procedure.
DOI: 10.1177/2473011421S00321
Biomechanics of Ankle Sprains: A 3D Dynamic Analysis of Lateral Tensile Load
Francois Lintz, MD MSc FEBOT; Cesar de Cesar Netto, MD, PhD; Maryama S. Dufrénot, MSc; Matthieu Lalevée; Ronny Lopes; Céline Fernando; Alessio Bernasconi, MD, PhD FEBOT
Category: Ankle; Sports
Keywords: Ankle Instability; Alignment Weight Bearing CT; Biomechanics of the Foot and Ankle
Introduction/Purpose: Lateral ankle sprains are the most frequent ankle trauma and may lead to chronic lateral ankle instability (CLAI). Studies have reported anterior talofibular (ATFL) and calcaneofibular (CFL) ligaments tensile strengths around 200N and 300N. Cone Beam Weight Bearing CT (WBCT) allows visualization of 3D bony anatomy in different functional positions. The primary objective of this study was to calculate 3D ATFL and CFL tensile loads in patients diagnosed with CLAI performing Forced Inversion stance during WBCT imaging (FI-WBCT) and wearing shoes, and to compare them with a population of non-CLAI ankles. The secondary objective was to evaluate the relative contribution of shoes. We hypothesized that ATFL and CFL calculated tensile loads (CTLs) would be close to previously published data with minimal contribution of shoes.
Methods: This retrospective comparative Level III study included 20 CLAI ankles and 20 controls with known demographics and available FI-WBCT datasets. Patients under 18 or with a previous history of trauma or surgery which could affect ankle architecture were excluded. A mechanical lever arm model was calculated for each case using the spatial coordinates of the weight bearing surfaces of the shoe and foot (bony landmarks: 5th metatarsal head, base and calcaneus lowest points, distal tip of the medial malleolus, ATFL and CFL distal insertion points, distal tip of the fibula). The ATFL and CFL CTL were calculated respectively as the coronal force applied at the distal insertion landmarks of the ATFL on the talus and CFL on the calcaneus. Normality was assessed using the Shapiro-Wilk test, then variables were compared using the Student t-test (normally-distributed) or the Wilcoxon rank sum test (non normally-distributed variables). Chi-2 was used for categorical variables.
Results: Mean age [42.4+-10.9 vs 40.8+-10.7 years; p=0.317], Body Mass Index [24.4+-3.3 vs 24.9+-4 kg.m-2; p=0.34], sex (p=0.75), side (p=0.75) and foot alignment (FAO -1.05%+-5.5 vs 0.08%+-3.6; p=0.22) were not different between CLAI ankles and controls. CTLs for ATFL were 194N+-149 in CLAI and 192N+-183 in controls (p=0.85), while for CFL they were 311N+-286 and 311N+-361, respectively (p=0.79). Using footwears, CTLs were 406N+-360 in CLAI vs 608N+-380 in controls (p<0.05) for ATFL, and 703N+-741 vs 958N+-779 (p=0.11) for CFL. Comparing barefoot and shod values, mean CTLs in the ATFL (193N+-164.8 vs 507N+-379.1, respectively; p<0.001) and in CFL (311.3N+-321 vs 830.8N+-761.5, respectively; p<0.001) were significantly different.
Conclusion: We found that the Calculated Tensile Loads for ATFL and CFL using Forced Inversion-WBCT considering the barefoot weightbearing surface were close to values described in previous cadaveric studies for those ligaments' tensile strength. A 2.6 and 2.7 fold increase was found when the weight bearing surface of the shoe was considered, indicating a possible aggravating role of shoewear. The reduced shod ATFL-CTL values found in unstable cases as compared to controls could suggest a possible active self-protection mechanism during FI-WBCT in CLAI.
DOI: 10.1177/2473011421S00322
Distribution of Bone Mineral Density in the Ankle Joint: Correlation with Hindfoot Alignment
Francois Lintz, MD MSc FEBOT; Matthew J. Welck, MD, FRCS(Orth); Kristian Buedts, MD; Céline Fernando; Cesar de Cesar Netto, MD, PhD; Alessio Bernasconi, MD PhD FEBOT
Keywords: Bone Mineral Density; Alignment Weight Bearing CT; Ankle Osteoarthritis Risk Factor
Introduction/Purpose: Abnormal Hindfoot Alignment (HA) has been correlated with increased failure rates in ankle fusion or replacement for osteoarthritis (OA). An altered stress distribution in the surrounding bone and abnormal Bone Mineral Density (BMD) around the native ankle may be predisposing factors for those unwanted outcomes. Cone Beam Weight Bearing CT (WBCT) has recently been used to investigate BMD and to correlate the localization of periprosthetic cysts and alignment in ankle arthroplasty. The objective of this study was to assess the spatial distribution of BMD around the ankle joint in patients with normal or abnormal HA. We hypothesized that BMD would be evenly distributed in normally-aligned ankles whilst increased medially in varus and laterally in valgus configurations.
Methods: In this retrospective comparative Level III study, 60 ankles (41 adults),without any trauma or surgery affecting HA, with WBCT datasets (PedCat, Curvebeam LLC, PA-USA) were allocated to 3 groups (comparable by age, p=0.79; BMI, p=0.24; and side, p=0.93), based on the Foot Ankle Offset (FAO) values: 20 normal (0%-2), 20 varus (FAO< 0%; 35% female, age 48.8+-13 years, BMI 26.2+-2.9 kg.m-2), and 20 valgus (FAO>5%; 40% female, age 58.9+-14.6 years, BMI 28.6+-4.2 kg.m-2). Semi-Automatic Segmentation (BoneLogic, Disior Oy, Helsinki-Finland) was applied to identify bones of interest. The tibia and talus were digitally compartmented in medial (M) and lateral (L) volumes relative to the median sagittal plane. Mean Hounsfield Unit (HU) value per compartment was used to assess BMD. The primary outcome measure was the Medial over Lateral HU ratio (M/L-HU).
Comparisons were performed using one-way ANOVA, Kruskal-Wallis and Chi2 tests.
Results: All values of BMD were normally distributed but M/L-HU ratios were not. Mean +- standard deviation HU values in the compartments in normal cases were 523+-103 (medial tibia), 519+-115 (lateral tibia) 421+-81 (medial talus), 470+-92 (lateral talus) and 725+-109 (fibula). The mean BMD was significantly lower in all compartments in valgus cases compared to normal (all p<0.05). It was decreased in valgus vs varus in the talus (p<0.04), specifically in the medial compartment (p<0.01). The tibia M/L- HU ratio was decreased in valgus vs normal (0.87+-0.16 vs 1.01+-0.07; p=0.001) and vs varus (1.04+-0.09; p<0.001). The talus M/L-HU ratio was increased in varus cases vs normal (1+-0.22 vs 0.83+-0.09; p<0.01) and valgus (0.07+-0.19; p<0.001).
Conclusion: We found that BMD in distal tibia, fibula and the talus varies with hindfoot alignment. In valgus configuration, all bone compartments were less dense compared to normal and varus. The medio-lateral ratio increased in the tibia and in the talus in varus cases, suggesting medial concentration of bone, and decreased in valgus cases, suggesting a more lateral concentration. This data supports the role of WBCT in analyzing BMD distribution. This method could be clinically useful in ankle OA to evaluate bone quality for such considerations as surgical indications or implant positioning.
DOI: 10.1177/2473011421S00323
Anatomic Considerations of the Distal Fibula: A Computed Tomography Guided Analysis
Philip H. Locker; Leah Waldman; Max Michalski, MD
Category: Ankle; Basic Sciences/Biologics; Trauma; Other
Keywords: Anatomic Plating; Ankle Fracture; Structural Anatomy and Biomechanics
Introduction/Purpose: Ankle fractures are a common injury in the general population with nearly sixty thousand operations performed in California for fractures involving the tibiotalar joint over a 10-year span. Reestablishing anatomic fibular alignment after fracture reduction leads to improved patient outcomes by restoring ankle mortise congruence. An in-depth understanding of fibular morphology may aid in fracture reduction, preoperative planning, plate positioning and intra-operative contouring. The goal of this study is to perform quantitative morphologic analysis of distal fibular anatomy using computed tomography (CT).
Methods: Using Nuance mPower Clinical Analytics software, a database of CT tibia-fibula reports for patients ages 18 through 35 performed at our institution were searched for the term 'normal.' Inclusion criteria was absence of any reported osseous pathology. Examinations were excluded if the fibula was incompletely imaged. Twenty CTs were collected and analyzed. Measurements were performed at 5 mm increments from the tip of the fibula extending proximally to 10 cm. At each level the following measurements were obtained: lateral and posterior border lengths, lateral to medial (LM) bicortical distances at ¼, ½, and ¾ the length of the lateral border, posteroanterior (PA) bicortical distance at the center of the posterior border, and the angles of the lateral and posterior borders relative to the PA axis of the tibia (figure 1). The location of the maximal bicortical distance in the LM direction was recorded at each level.
Results: The posterior border of the fibula broadens from an apex distally to 8.4+-1.6 mm at 10 cm proximal while rotating an average of 97.5 degrees. The lateral border of the fibula rotates 6.3 degrees from distal to proximal and begins with a width of 12.8+-3.1 mm and comes to an apex at 9 cm. In the distal fibula, the ratio of the maximal LM to PA bicortical length is 0.56. By 3 cm proximal, the ratio approaches 1 and is 1.6 at 10 cm. The distal 1 cm of the fibula has the largest LM diameter anteriorly and medially but from 1.5 cm to 10 cm proximal the posterior ¼ has the largest LM diameter.
Conclusion: The fibula has a complex distal geometry which changes with progression from the distal tip to 10 cm proximal. The posterior border of the fibula broadens and rotates over 90 degrees to become the lateral border proximally. The lateral border distally is broad but comes to an apex proximally with minimal rotation. The ratio of bicortical distances changes from distal to proximal as the distal posterior border rotates to face in a LM direction proximally. This information may aid in surgeons' understanding of the complex distal fibular morphology and assist with intra-operative decision making regarding hardware size, placement and manipulation.
DOI: 10.1177/2473011421S00324
Cost of Operative Fixation of Ankle Fractures: Comparing Orthopaedics and Podiatry
Joshua C. Luginbuhl, MD; Alexa R. Deemer; Eric C. Gokcen, MD
Category: Trauma; Other
Keywords: Ankle Fracture; Cost; ORIF
Introduction/Purpose: Ankle fractures pose a unique situation as both podiatrists and orthopaedic surgeons are licensed to treat them. Despite increasing emphasis on value-based medical care, there are few cost analyses focused on the treatment of ankle fractures. The goal of this study is to determine if there are cost differences between an orthopaedic surgeon and podiatrist to operatively manage an ankle fracture.
Methods: Retrospective cohort study of patients who underwent ankle fracture fixation over a 22 month period at an academic level 1 trauma center. Patient data was subcategorized by surgeon type and treatment groups. Four treatment groups were included: lateral malleolus open reduction and internal fixation (ORIF), bimalleolar/trimalleolar ORIF (no posterior malleolus fixation), lateral malleolus ORIF with syndesmotic fixation, bimalleolar/trimalleolar ORIF (no posterior malleolus fixation) with syndesmotic fixation. Primary outcome was total (OR time cost + Implant cost) cost per case.
Results: A total of 134 cases met criteria. Eighty-five cases were treated by a total of 4 orthopaedic surgeons while 49 were treated by 8 podiatrists. There was significantly longer OR time (minutes) for lateral malleolus ORIF (111 vs 134.92), lateral malleolus ORIF with syndesmotic fixation (130.53 vs 156.7), and bimalleolar/trimalleolar ORIF (no posterior malleolus fixation) with syndesmotic fixation (162.13 vs 208) when podiatry was the treating team. Average total cost per case was significantly more for lateral malleolus ORIF (+$1188.45), lateral malleolus ORIF with syndesmotic fixation (+$2259.16), and bimalleolar/trimalleolar ORIF with syndesmotic fixation (+$2837.29) when podiatry was the treating team.
Conclusion: Lateral malleolus ORIF, lateral malleolus ORIF with syndesmotic fixation, and bimalleolar/trimalleolar ORIF with syndesmotic fixation costs less per case when performed by an orthopaedic surgeon based on OR time costs and implant costs.
DOI: 10.1177/2473011421S00325
Accuracy of Tibia Deformity Correction with a Hexapod Multiplanar External Fixator with Measurements Taken from Radiographs, CT Scan, and Imaging Software: A Cadaveric Study
Gregory A. Lundeen, MD, MPH; Abrianna S. Robles; Erin K. Haggerty, MD; Tyler W. Fraser, MD; Spenser J. Cassinelli, MD; Julie Smith-Gagen; Ally Abbatangelo; Scott R. Whitlow, MD
Introduction/Purpose: The success of hexapod multiplanar external fixators for correction of tibial deformity has been well described. The ability to correct deformity is based on the accuracy of the reference and deformity data inputted into the prescription program. If the data is not accurate, multiple residual programs may be required for final correction. There are limited papers evaluating i accuracy of intraoperative measurements. We are unaware of any analysis on the use of CT scan to determine deformity and reference points. Newer software program allows surgeons to incorporate radiographs into the correction program to determine deformity and reference points. Our study objective was to compare deformity and reference point measurements taken from radiographs, CT, and imaging software to determine which method most accurately corrects tibia deformities.
Methods: Hexapod external fixators were orthogonally applied on four full length tibia cadavers. Strut lengths were set to the same length. Each cadaver was assigned a different deformity: proximal quartile, distal quartile, midshaft, and segmental. An osteotomy was performed and the hexapod struts were loosened to create a multiplanar deformity. Radiographs and CT were taken orthogonal to the reference ring. Deformity and reference points were measured off each according to correction software data points. Pictures of the radiographs were imported into the software program (Stryker, Mahwah, NJ) and the correction reference points were determined with imaging software. All cadavers had a correction program for each method. Two surgeons performed the measurements twice to determine inter and intra-observer accuracy. Corrections were performed and post reduction radiographs were measured to determine length, angulation and translation. In addition, the total number of millimeters each strut was off from the pre-deformity position was recorded.
Results: Line technique on software program was significantly better at measuring segmental deformity and the Image technique was statistically more accurate to correct proximal, midshaft and distal deformities (p<0.05). Overall, all methods were more accurate correcting Midshaft and Proximal deformities (44.8mm and 50.4mm, respectively) significantly better than Distal and Segmental deformity correction (88.9mm and 121.7mm, respectively (p<0.001). There was no difference in absolute measurements or intra-observer error between the four surgeons (p>0.05).
Conclusion: Compared to the traditional method of measuring deformity and frame reference using radiographs, new imaging software appears to be superior and more reproducible in correcting tibia deformities. Surgeons should recognize the increased difficulty in correcting segmental and distal deformities regardless of the method used. Accuracy of determining deformity and frame reference points has the potential to decrease time patients are in a frame and reduces the potential for malunions. Further investigation is needed to determine sites of variation to further improve the process of correcting complex deformities of the tibia.
DOI: 10.1177/2473011421S00326
Effect of Packaging on Polyethylene Fractures, Implant Survivorship and Cyst Formation in Mobile Bearing Total Ankle Replacements
Gregory A. Lundeen, MD, MPH; Tyler W. Fraser, MD; Erin K. Haggerty, MD; Braden Matthews; Ally Abbatangelo; Scott R. Whitlow, MD; Spenser J. Cassinelli, MD
Category: Ankle Arthritis; Ankle
Keywords: Total Ankle Replacement; Ankle Replacement; Total Ankle Arthroplasty Prostheses
Introduction/Purpose: The Scandinavian Total Ankle Replacement (STAR) is the most widely used mobile bearing total ankle arthroplasty (TAA) in the US. The polyethylene component is ultrahigh molecular weight polyethylene and is designed to articulate with both the tibial and talar component. Initial data on the STAR in the US reported polyethylene fracture rates of greater than 10% as well as a concern for cyst formation due to osteolysis. The manufacturer changed the packaging to foil to prevent potential oxidation of the polyethylene, which could predispose the polyethylene to failure. The objective of the study was to evaluate a cohort of patients with STAR performed before and after converting to foil packaging to determine if there is a difference in polyethylene survivorship and cyst formation.
Methods: All primary TARs performed by the senior author from 2010-2017 were reviewed. Patients with a minimum 48 month follow up were included in the study. The two groups were stratified by those performed prior to August 2014 (PRE) and those performed after August 2014 (POST). Preoperative and most recent postoperative alignment was determined on weight bearing radiographs. The outcomes included polyethylene fractures and cyst formation in the two groups. Cysts were defined as those measuring greater than 1cm2 on plain radiographs. Patients were recommended to have surgery if cyst volume was greater than 2cm2. Chi-squared tests were used to detect significant differences in the rate of cyst formation between the two groups. Paired t- tests were used to determine difference in preoperative versus postoperative alignment, follow up length, and polyethylene component thickness and patient age at time of procedure between the two groups.
Results: The PRE group had 35 patients with an average follow up of 75 months (range 48-118). The POST group had 15 patients with average follow up 55 months (range 48-60). There was no difference in preoperative versus postoperative radiographic alignment between the groups (p>0.05). Cysts were present in 9 (26%) patients in the PRE group versus 4 patients (26%) in the POST group. Nine patients (26%) needed a second surgery due to cyst formation in the PRE group versus two (16%) in the POST group (p>0.05). Four patients (11%) had a fracture of the polyethylene in the PRE group with an average thickness of 6.7mm (range 6-9) and 77 months (range 68-84) versus zero in the POST group. The average time to polyethylene exchange for cyst(s) or polyethylene fracture was 58.3 months.
Conclusion: This study suggests that changes in packaging to limit oxidation of the polyethylene from plastic to foil did not appear to represent a difference in periprosthetic cyst formation. However, there was a trend for additional surgery related to periprosthetic cysts and increased risk for polyethylene fracture in the PRE group. These results could suggest the potential for oxidation changes that alter the wear characteristics and fragility of the polyethylene component. Confounding factors could include postoperative time and component thickness. Further investigation and longer follow-up will be needed to further delineate oxygenation impacts on TAA polyethylene components.
DOI: 10.1177/2473011421S00327
Motion is Maintained at the Tibial and Polyethylene Component Interface in a Mobile-Bearing Total Ankle Arthroplasty at Mid and Long-Term Follow-Up
Gregory A. Lundeen, MD, MPH; Erin K. Haggerty, MD; Tyler W. Fraser, MD; Braden Matthews; Scott R. Whitlow, MD; Spenser J. Cassinelli, MD
Category: Ankle Arthritis; Ankle; Hindfoot
Keywords: Total Ankle Arthroplasty; Total Ankle Arthroplasty Prostheses; Total Ankle Replacement
Introduction/Purpose: Normal biomechanics of the ankle joint includes sagittal motion, but also anterior-posterior (AP) translation (1mm) as well as axial rotation (5-8 degrees). Sagittal motion is well described in total ankle arthroplasty (TAA), however, current understanding of mobile-bearing motion at the tibial-polyethylene interface in TAA is limited to AP motion and short-term data on axial rotation. The purpose of our study was to determine if polyethylene components maintain mobility adjacent to the tibial component in mobile bearing TAA at mid and long-term follow-up in both the sagittal and axial planes in patients more than 48 months post-operatively.
Methods: Patients who were a minimum of 48 months postoperative from a third-generation mobile-bearing TAAwere identified. Fluoroscopic images perpendicular to the tibial component were saved at maximum internal and external rotation on AP, and the lateral images were saved in maximum plantarflexion and dorsiflexion. Sagittal range of motion and AP translation of the polyethylene component were measured from the lateral images. Axial rotation was determined by measuring the relative position of the two wires within the polyethylene component on AP internal and external rotation imaging. This relationship was compared to a table previously developed from fluoroscopic images taken at standardized degrees of axial rotation of a nonimplanted polyethylene with the associated length relationship of the two imbedded wires. Total axial motion was determined by the difference between angle value determined for maximum internal and external rotation.
Results: Eight patients were included in this investigation, 5 (62.5%) were female and average age was 72.6 (range, 59-83) years. Time from surgery averaged 94.2 (range, 54.7-118.6) months. Total sagittal range of motion between the talar and the polyethylene component averaged 20.3 (range, 10-30) degrees. All patients (100%) maintained motion at the tibia-polyethylene interface. Axial motion for total internal and external rotation of the polyethylene component articulation on the tibial component averaged 5.3 (range, 2-12) degrees. AP translation of the polyethylene component relative to the tibial component averaged 1.1 (range, 0.4-2.6) mm during plantarflexion and dorsiflexion. There was no relationship between axial rotation or AP translation of the polyethylene component and ankle joint range of motion (P >.05).
Conclusion: To our knowledge, this is the first investigation to measure axial and sagittal motion of the polyethylene component in mobile bearing TAA at the tibial implant interface in patients at mid and long-term follow-up. Based on our results, motion is maintained an average of 8 years post-operatively and concludes that a mobile-bearing TAA has the potential to fall within the parameters of normal polyaxial ankle motion several years after implantation. Such maintenance of motion may have a positive influence on gait pattern, polyethylene wear, joint reaction forces and implant longevity.
DOI: 10.1177/2473011421S00328
Return to Driving after Elective Foot & Ankle Surgery: A Systematic Review
Alexander Lundy; Andres S. Piscoya; Michael D. Bedrin; Daniel L. Rodkey; Sarah Nelson; Tobin T. Eckel, MD
Category: Ankle; Arthroscopy; Midfoot/Forefoot; Other
Keywords: Clinical Outcomes; Patient Education; Elective Surgery
Introduction/Purpose: Studies investigating when patients can safely return to driving are becomingly increasingly numerous in the orthopedic literature because of the recognition of the importance of the activity to the lives of most adults. Previous systematic reviews have proven helpful by collecting and summarizing these studies to establish concise guidelines that can be presented to patients during the counseling surrounding a procedure. Having these guidelines can be even more crucial when discussing elective procedures. This systematic review summarizes the available studies investigating when it is safe to return to driving following elective foot and ankle procedures.
Methods: A systematic review of the literature was performed using PubMed, Embase, and CINAHL to identify English-language studies from 1999 to present that investigate return to driving after right-sided elective foot and ankle procedures. Qualitative assessment of each of the included studies was performed independently by two authors. Then data from each study was extracted and broken down into distinct categories for comparison: study details, population, control group, method of evaluation, and results.
Results: Eight studies met inclusion criteria. All of the studies investigate brake reaction time (BRT), via a driving simulator, as their primary outcome. A variety of objective and subjective secondary outcomes were collected. Patients undergoing right ankle or subtalar arthroscopic procedures have no significant difference in BRT compared to controls at 2 weeks post-operatively. 92% of patients undergoing right ankle arthroplasty had a BRT that was not significantly different to the control group at 6 weeks post- operatively. Patients who had an ankle arthrodesis had significantly delayed BRT compared to controls even past 1-year post- operatively. The majority of patients after corrective hallux valgus surgery have no significant difference in BRT at 6 weeks post- operatively compared to their pre-operative baselines depending upon how they are doing clinically. The included studies used a variety of patient reported outcomes that were helpful in predicting which patients would fail the driving simulation at the various timepoints.
Conclusion: The recommendations from these reviewed studies can guide physicians when counseling their patients on when they can expect to safely return to driving after a specific, elective foot and ankle procedure. However, these recommendations are reliant on routine healing post-operatively and may need to be adjusted if a patient is experiencing any complications. A variety of patient surveys and other subjective scores can be very helpful in assuring a routine post-operative course.
DOI: 10.1177/2473011421S00329
Risk Reduction and Perioperative Complications in Diabetics with Multiple Medical Comorbidities Undergoing Charcot Foot Reconstruction
Madeline M. Lyons, MD; Michael S. Pinzur, MD; Patrick C. McGregor, MD; William Adams; Lynette Wilkos-Prostran, RN
Introduction/Purpose: Modern Patient Safety Programs focus on medical optimization prior to surgery, regional anesthesia and hospitalist-orthopaedic co-management during the perioperative period.
Methods: Eighty-five consecutive diabetic patients with multiple medical co-morbidities underwent surgical reconstruction for acquired deformities secondary to Charcot foot arthropathy with circular ring fixation between 2016 and 2019. All patients participated in a standardized perioperative medical optimization program, which included medical optimization prior to surgery, regional anesthesia whenever possible and hospitalist-orthopaedic comanagement during hospitalization. Charts were retrospectively reviewed for medical comorbidities, complications, and length of stay. The National Surgical Quality Improvement Program (NSQIP) Risk Calculator was used to retrospectively calculate their predicted perioperative risk.
Results: On multivariable analysis, longer lengths of stay were associated with low preoperative hemoglobin values (RR = 1.36; P =.01) and congestive heart failure (RR = 1.42; P =.02). There were 22 (27%) complications, though only 10 (12%) were serious. These included acute kidney injury (n = 6), sepsis (n = 2), one cardiac event, and one pulmonary embolism. Overall, the accuracy of predicting a complication using the NSQIP risk calculator was 74% (95% CI: 63% - 85%) which was comparable to the accuracy of predicting a complication using only patients' congestive heart failure and pin-tract infection statuses (c = 74%, 95% CI: 62% - 86%).
Conclusion: Medical optimization of diabetic patients with multiple medical co-morbidities prior to elective complex reconstruction orthopaedic surgery leads to improved clinical outcomes. Preoperative anemia and congestive heart failure are associated with longer hospitalizations in this patient group. The American College of Surgeons NSQIP Risk Calculator is a reliable predictor of complications in the perioperative period. This study demonstrates that reconstructive surgery in this complex patient population can be accomplished with a reasonable exposure to risk for complication.
DOI: 10.1177/2473011421S00330
Screws Only Primary Subtalar Arthrodesis for Calcaneus Fractures
David M. Macknet, MD; Ainsley Bloomer, BS; Richard Mcknight, MD; Nicholas Johnson; Ziqing Yu; Rachel Seymour; Joseph R. Hsu, MD
Introduction/Purpose: The initial management of displaced intraarticular calcaneus fractures (DIACFs) is a difficult problem. The results of open reduction internal fixation (ORIF) have been disappointing. Alternatively, ORIF with primary subtalar arthrodesis (PSTA) has gained increasing popularity. The purpose of this study is to review patient-centered and radiographic outcomes of ORIF plus PSTA using screws alone through a sinus tarsi approach.
Methods: A retrospective study of all patients from 2013-2019 who underwent ORIF+PSTA for DIACFs was conducted. The same surgical technique was utilized in all cases consisting of only screws, no plates were utilized. Delayed surgeries past 8 weeks were excluded. Demographic and radiographic data was collected. Worker’s compensation (WC) claims were noted and analyzed separately. Plain radiographs were assessed preoperatively and post-operatively and Sander’s classification was used to characterize injuries. Patient reported outcomes (PROs), complications, and need for revision surgeries was also noted and analyzed at final follow-up.
Results: In total, forty-eight DIACFs underwent PSTA with a median follow-up of 194 days. Median time to weight-bearing was 60 days post-operatively. Three fractures were documented as Sanders II, 22 as Sanders III, and 23 as Sanders IV. Seventy-five percent of the WC group returned to work compared to just 58.3% in the non-WC group (p=0.0003). Patients in the WC group were more likely to have had an abnormal pre-operative Bohler’s angle (p=0.047) but the two groups did not differ significantly in postoperative Gissane or Bohler angles. Nearly 85% (N=41) achieved >=2 zones of fusion on radiographs by final follow up and 95.8% (N=46) had at least one. Four patients had a complication and 3 required a return to the operative room.
Conclusion: Utilizing Screws only primary subtalar arthrodesis for the treatment of DIACFs through a sinus tarsi approach shows promising results with high rates of return to work and fusion, even in the workers' compensation population.
DOI: 10.1177/2473011421S00331
Complications of Calcaneal Osteotomy: Are They Equal Between Different Osteotomy Types?
N. Jane Madeley; Chinnasamy Senthil Kumar, MBBS,FRCS(Tr&Orth); Alia Alenezi
Introduction/Purpose: Calcaneal osteotomy is regularly performed as part of the surgical management of a number of conditions. Complication rates are thought to be low, however are these risks the same for different osteotomy types? In our institution a Lateralising Closing wedge osteotomy is performed for Cavus foot correction and Varus alignment with instability, whilst Lateral Column Lengthening Osteotomy and Medialising Displacement Calcaneal Osteotomy (MDCO) are performed for Pes Planus with and without forefoot abduction respectively. In severe Pes Planus deformities both may be utilised. The purpose of this study was to examine complication rates in each group.
Methods: This is a retrospective case series of consecutive calcaneal osteotomies performed at our institution between January 2010 and December 2019. The primary outcome measures were healing of the osteotomy, metalwork removal and any other reported complications related to the calcaneal osteotomy including infection and wound problems. Patient demographics, associated procedures, indication for surgery, incision, and fixation method were also recorded.
Results: There were 141 patients in the series. 77 patients underwent a lateralising osteotomy, 55 underwent MDCO and 12 Lateral column lengthening (LCL) with opening wedge osteotomy of the anterior process of the Calcaneus. Fixation was with cannulated screws, or specific purpose locking plates. Patients were followed up for a minimum of three months and discharged from follow-up once a satisfactory level of recovery was reached..One non-union was seen in each of the Lateralising, MDCO and LCL groups. Delayed union was seen in 3 lateralising osteotomies, and 1 MDCO. Metalwork irritation requiring surgery for metalwork removal was 6.5% (4 with screws, 1 plate), 9.1% (all screws) and 0% for Lateralising, MDCO and LCL osteotomies respectively. Wound problems or sural nerve irritation were noted in 11.7%, 3.6% and 8.3% of Lateralising and MDCO and LCL osteotomy respectively. 1 superficial infection was seen in the Lateralising osteotomy group
Conclusion: One non-union was seen in all groups, with a trend for bone healing to be slower in those having lateralising procedures. Patients should be advised of this possibility if undergoing calcaneal osteotomy. Wound problems and sural nerve irritation were also more common with lateralising procedures. Metalwork removal due to hardware irritation was common (7% overall), and fixation method rather than osteotomy type appears to influence this with 9 cases following cannulated screws and 1 following lateral locking plate fixation. Screw fixation is associated with higher hardware removal rates.
DOI: 10.1177/2473011421S00332
Middle Facet Subluxation Correlation with Foot and Ankle Offset in the Assessment of Progressive Collapsing Foot Deformity
Connor Maly; Nacime S. Mansur, MD; Matthieu Lalevee, MD; Christian VandeLune; Chris Cychosz, MD; Edward O. Rojas; Kevin N. Dibbern, PhD; Scott J. Ellis, MD; Francois Lintz, MD MSc FEBOT; Alessio Bernasconi, MD PhD FEBOT; Cesar de Cesar Netto, MD PhD
Introduction/Purpose: Identifying markers of severity and progression in Progressive Collapsing Foot Deformity (PCFD) provides surgeons with critical information, possibly aiding in the decision making along the treatment algorithm. Subtalar middle facet subluxation (MFS), the percent undercoverage of the talus in relation to its calcaneus counterpart, was recognized as a reliable marker in weight-bearing computerized tomography (WBCT) for PCFD diagnosis. The Foot and Ankle Offset (FAO), the relative position between the center of the ankle joint and the foot tripod, is a three-dimensional WBCT tool predictive of disease severity. Our objective is to assess the relationship between the amount of MFS and FAO in flexible PCFD patients. We hypothesize that MFS is a reliable assessment of disease severity and correlates with FAO.
Methods: In this retrospective IRB-approved comparative study, a total of 56 individuals with PCFD (74 feet) who underwent WBCT for baseline assessment were analyzed. Two blinded fellowship-trained foot and ankle surgeons performed the measurements. MFS was executed in the coronal-plane, at the midpoint (on sagittal-plane) of the middle facet (see attached figure). Dedicated software was utilized to perform the FAO, using the most plantar voxels of the first metatarsal, fifth metatarsal, calcaneal tuberosity and centre of the ankle. Interobserver agreement was quantified for MFS and FAO using intraclass correlation coefficient (ICC). Intermethod agreement between MFS and FAO was assessed by Spearman’s correlation. Bivariate linear regression analysis was used to assess the relationship between MFS and FAO. A partition prediction model and multivariate analysis were utilized to assess influence of MFS measurements on FAO values and vice versa.
Results: A total of 56 patients (74 feet) were included in the study. The ICCs for interobserver reliability was 0.87 for MFS and 0.95 for FAO. In a bivariate analysis, MFS and FAO were found to be significantly and linearly correlated (P< 0.0001, R2 0.26). Foot Angle Offset = 2.22 + 0.12*Medial Facet Subluxation (%). In multivariate analysis, FAO and body mass index (BMI) were significantly correlated with MFS (<0.001 and 0.02, respectively). The partition prediction model demonstrated that an MFS of 27.5% was an important threshold for increased FAO, with FAO of 3.4% +-2.4% when MFS was below threshold and 8.0% +-3.5% when above threshold.
Conclusion: We found a positive linear correlation between MFS and FAO measurements. An MFS of 27.5% was an important threshold for higher FAO values, which corresponded to a worst overall alignment. Our results are consistent with the idea that MFS is a reliable marker for PCFD diagnoses and severity, correlating well with the FAO. This data may support clinical decisions in PCFD patients. Also, BMI was found to be positively correlated with MFS. Future prospective and longitudinal studies are needed to confirm the findings of this study.
DOI: 10.1177/2473011421S00333
Arthroscopically Assisted Particulated Juvenile Allograft Cartilage Implantation and Bone Grafting for Treatment of Large Cystic Osteochondral Lesions of the Talus: A Case Series
Kshitij Manchanda, MD; Joseph E. Manzi; Cary B. Chapman, MD
Keywords: Ankle Arthroscopy; Osteochondral Lesions of the Talus; Cartilage Allografts
Introduction/Purpose: Osteochondral lesions of the talus (OCLT) are common traumatic injuries and can be difficult to treat. Conventional methods consist of arthroscopic debridement and bone marrow stimulation techniques including microfracture, curettage, abrasion chondroplasty and antegrade/retrograde drilling predominantly leading to fibrocartilage formation. These methods have proved effective for small lesions; however, larger lesions with accompanying subchondral bone cysts require more invasive treatment with osteochondral allografts or autologous chondrocyte implantation. These procedures can require harvesting of osteochondral grafts from the knee or malleolar osteotomies, which have associated donor site morbidities and complications of osteotomy healing. We describe an alternative method, an all-arthroscopic technique to treat these large cystic OCLTs, and sought to determine long-term quality of life metrics for a cohort of patients.
Methods: From 2010-2012, six patients with difficult to treat OCLTs underwent arthroscopic-assisted implantation of particulated juvenile allograft cartilage with viable chondrocytes (DeNovo NT) along with autogenous bone grafting from the calcaneus by a single surgeon. These lesions all had associated cystic changes requiring bone graft to fill the defect. Other inclusion criteria included at least two of the following: 1) shoulder lesions, 2) lesion size > 200 mm2, 3) failed previous microfracture treatment, or 4) age > 40 with a Body Mass Index (BMI) > 25 kg/m2. These six patients were fully evaluated using physical examination, patient interviews, and outcome score measures. Follow-up was completed at 2 years, 4 years, and between 6-9 years at their most recent visit. Pre-operative and post-operative functional outcome scores were compared with Wilcoxon Signed Ranked Test.
Results: Six patients (age: 43.8 + 14.0 years, BMI: 28.4 + 6.7 kg/m2) had average lesion sizes of 188.5 + 50.9 mm2 (range: 125-260 mm2) and most recent follow-up of 8.4 + 1.2 years (range: 6.0-9.3 years). Post-operatively, average VAS pain scores decreased by 4.2 points, 95% CI [1.6-6.8]. FAAM ADL scores improved from 41.8 to 72.5, 95% CI [11.3-50.1]. SF-36 Physical Component Scores also showed significant improvement by 37.8 points, 95% CI [20.8-54.8]. FAAM Sports (p = 0.055) and AOFAS (p = 0.066) scores clinically improved from 13.3 to 39.2 and 57.7 to 86.3, respectively, and approached statistical significance. There were no intraoperative or perioperative complications with calcaneal bone grafting.
Conclusion: A small cohort of patients followed over the course of ~8 years after implantation of particulated juvenile allograft cartilage (DeNovo NT) and autogenous calcaneal bone graft for cystic OCLTs had positive post-operative, self-reported functional outcomes. Patients significantly improved compared to pre-operative measures, with no complications observed. This may be an effective long-term treatment for patients with difficult to treat OCLTs.
DOI: 10.1177/2473011421S00334
Characterization of Motor Performance in 200 Normal Ankles Through Isokinetic Evaluation
Nacime S. Mansur, MD; Lucas Fonseca; Eduardo S. Maciel; Thiago Inojossa; Cesar de Cesar Netto, MD, PhD; Diego C. Astur
Category: Ankle; Sports
Keywords: Ankle; Biomechanics of the Foot and Ankle; Functional Rehabilitation
Introduction/Purpose: The isokinetic test has been used diffusely as a way to evaluate the functional results after the rehabilitation of musculoskeletal injuries. In the ankle, in particular, most studies are related to lateral ligament injuries and Achilles tendon’s injuries. However, different protocols are used and a lack of normative values is observed in the literature. The aim of this work is to perform a global isokinetic evaluation on healthy ankles in order to propose reference values for future patients.
Methods: We evaluated 100 participants (200 ankles) using the Biodex 3 System for the eversion, inversion, dorsiflexion and plantar flexion movements of the ankle. The sample consisted of individuals aged 20-60 years, with an active life and practice of recreational physical activity (non-athlete) and without previous injuries. Five repetitions for strength (N / m) and work (J) at a speed of 30° / sec and 10 repetitions for power (W) at a speed of 120° / sec were performed in our protocol. Agonist / antagonist ratio and the Muscle Deficiency Index, which globally assesses the balance between the sides for each movement, were also evaluated, as well as the demographic variables. Different statistical analyzes were performed for each parameter.
Results: The mean age was 38.5 years and BMI 25.8 (CI 2.7 and 0.8 respectively). The non-dominant side was consistently stronger (higher peak torque) in all movements (p <0.001 -). The mean values obtained for force in each movement were 29.9N / m (CI 1.4) for eversion, 34.8N / m (CI 1.6) for inversion, 48.6N / m (2.0) for dorsiflexion and 140.2 N / m (CI 6.1) for plantar flexion. There was no correlation between age or BMI with the maximum torque (N / m). The ratio of eversors / inverters was 88.8% (CI 3.1) and that of dorsiflexors / plantar flexors was 36.1% (1.3). The Muscle Deficiency Index showed a balance between the sides for each movement (p 0.062), with an average global difference of less than 10% between them (eversion 8.66 [CI 3.17], inversion 4.2 [3, 48], dorsiflexion 3.41 [3.04] and plantar flexion 5.18 [2.51].
Conclusion: As far as we know, this is the largest isokinetic assessment of normal ankles ever performed. The sample, although not stratified, was considered homogeneous (coefficient of variation <50%), which allows to propose several normative values for a non-athlete population in the isokinetic evaluation. It would be interesting to compare these data in the future with the functional results in patients after the treatment of certain injuries.
DOI: 10.1177/2473011421S00335
Computerized Tomography Scans for Ankle Fracture: Diagnosis, Management and Surgical Plan Modifier
Nacime S. Mansur, MD; Fausto Santana Celestino; Caroline Neves; Vinícius F. Pereira; Pedro Debieux Vargas Silva; Fabio Teruo Matsunaga, MD, PhD; Caio A. Nery; Diego C. Astur
Introduction/Purpose: Ankle fractures are one of the most operated injuries in orthopedic practice. The decision upon the best management is based on the displacement of the bone fragments and the presence of associated lesions (osseous and/or soft tissues). The therapeutic decision is classically established upon plain radiographs, which might be temerarious due to the usual difficulty in analyzing those exams. In recent years, some authors have advocated that computed tomography could be used as an assistant instrument on the decision-making. Our study aims to demonstrate the superiority of the association between both methods on diagnosis, therapeutic decision, and surgical plan for these injuries.
Methods: Patients diagnosed with an ankle fracture, between 2011 and 2016, and assessed with CT and X-ray were included in our investigation. Seven examiners with different degrees of experience analyzed the exams, determined the injuries, chose how they would treat, and the defined surgical strategy when applicable. This was done, at first, only with radiographs and after with the combination of CT and radiographs. The data were statistically compared.
Results: Fifty-three patients were included. The medial malleolus fractures characteristics (posteromedial fragment and anterior colliculus), the presence of posterior malleolus fracture and its characteristics (displacement, bone fragment greater than 25%, posteromedial or posterolateral segment), syndesmosis injury, and the absence of deltoid ligament lesion were more noticeable from the combination of CT and radiography. Concerning surgical treatment, the prone position, the posterolateral surgical approach (rather than anterolateral) on lateral malleolus osteosynthesis, the decision to surgically treat the posterior malleolus fracture (through posterolateral approach with posterolateral plate), the option to include the syndesmosis approach in the treatment, and not to include deltoid ligament repair were more noticeable from the combination of CT and radiography, among all groups of expertise, with high inter-observer reliability.
Conclusion: The usual radiographs may fail to demonstrate subtle lesions, as posterior malleolus fractures and syndesmotic injuries. The tomographic evaluation increases the precision of diagnosis and improves the quality of information that the surgeon receives, providing data that can positively affect patient care.
DOI: 10.1177/2473011421S00336
Deltoid Ligament Arthroscopic Repair in Ankle Fractures: Case Series
Nacime S. Mansur, MD; Andre Vitor Lemos, MD, MSc; Daniel Baumfeld, MD; Gustavo T. Sanchez; Fernando C. Raduan, MD; Marcelo P. Prado, MD, PhD; Caio A. Nery
Introduction/Purpose: Diagnosis and treatment of ankle medial ligament lesions in malleolar fractures has always been a matter of controversy. Even when deltoid involvement is clear, the direct repair of this structure is not a consensus. Recently, deltoid reparation through an arthroscopic technique was described aiming to potentialize better clinical results and minimize complications. We intend to demonstrate safety and functional results of operated ankle fractures that had an arthroscopic deltoid repair.
Methods: This is a retrospective study in patients diagnosed with ankle fractures associated with acute deltoid injuries submitted to malleolar fixation and deltoid arthroscopic repair between June 2016 and January 2020. All patients were evaluated for pain and function according to the Visual Analogue Scale (VAS) and the American Orthopaedic Foot & Ankle Society Score (AOFAS) at a minimum of 6 months in follow-up.
Results: Between January 2016 and January 2020, 20 ankles with fractures or dislocations were operated and the deltoid ligament rupture was repaired arthroscopically. A mean follow-up of 14.45 months (6-48) was observed, and patients presented an average AOFAS of 93.5 (SD 7.25) and a VAS of 0.75 (SD 1.05). Three minor complications were noticed and no signs of medial chronic instability, loss of reduction or osteoarthritis were observed.
Conclusion: The repair of the deltoid complex and the low morbidity of the arthroscopic technique used may improve the clinical outcomes of these patients. Additional studies, with a prospective and comparative methodology are required to sustain this proposal.
DOI: 10.1177/2473011421S00337
Diagnosis of the Achilles Insertional Tendinopathies by Algometry
Nacime S. Mansur, MD; Vinícius F. Pereira; Henrique C. Monteiro Cunha, MD; André F. Yamada, MD, PhD; Fabio Teruo Matsunaga, MD, PhD; Marcel J. Sugawara Tamaoki, MD, PhD
Introduction/Purpose: Diagnosis of Achilles insertional tendinopathies (AIT) is based on pain by tendon palpation. However, there is no consensus or standard regarding the amount of force to be used during the evaluation. The algometry is a method of measuring the pressure applied in a specific region and can be a method for determining diagnosis values. Goal: To determine a cut-off value for Pain Threshold (PT) in the assessment of AIT.
Methods: Design: This is a prospective case-control study of diagnostic accuracy, to develop a diagnostic criterion. Methods: Forty asymptomatic individuals and forty patients with insertional Achilles tendinopathy, matched by age and sex, were evaluated, and submitted to algometry for PT and for Visual Analogical Scale (VAS) levels with 3kg/f at the insertion of the calcaneal tendon by two different evaluators. Inter-observer reproducibility was accessed through the interclass correlation index (ICC). Sensitivity and specificity calculation of PT and of VAS were calculated and plotted on a ROC (Receiver Operator Characteristic) curve.
Results: The lowest ICC found was 0.788. Regarding the diagnosis through TP, the 4.08 kg/f mark showed the best relation between sensitivity and specificity (92.5% and 92.5%, respectively). Algometry values lower than 4.08 were considered positive for disease. For the diagnosis of TIA through VAS with 3kg/f, the value of 2.98 was determined (sensitivity of 92.5% and specificity of 97.5%).
Conclusion: This study showed that algometry is a reliable method in the assessment of Achilles insertional tendinopathies, having a high intra-observer reproducibility. The painful threshold for establishing the diagnosis of Achilles insertional tendinopathies was 4.08 kg/, with values below this number considered altered.
DOI: 10.1177/2473011421S00338
Does the Radiographic Lateral View of the Lesser Toe Matter in A Trauma? A Retrospective Analyses of 378 Radiographs
Nacime S. Mansur, MD; Danilo P. Kitagaki; João P. Gonçalves; Noel O. Foni; Caio Augustus F. Araujo; Gustavo T. Sanchez
Category: Lesser Toes; Trauma
Keywords: Fractures; Forefoot; Trauma
Introduction/Purpose: To evaluate the importance of a radiographic lateral view in diagnosing lesser toes traumatic conditions.
Methods: Between January 2018 and March 2018, 378 radiographs of 126 patients evaluated in an emergency care hospital for trauma in the lesser toe were retrospectively evaluated for presence of lesser toes traumatic conditions. Patients were selected if a complete series of radiographs were performed, anteroposterior (AP), lateral (LA) and Oblique (OB). Radiographs of the same patient were duplicated and divided in two groups: standard group (AP and OB) and complete group (AP + LA + OB). Images were examined by four independent examiners with different degrees of experience. Each examiner randomly evaluated the same patient twice (one for each group). Kappa index was used to evaluate intra and inter-examiner concordance, and the two- proportion equality test was used to calculate statistical significance.
Results: Mean age of patients was 37.2 years (4-85yr), 144 injuries were diagnosed in standard group (28.6%) and 266 injuries (52.8%) in complete group (p<0.001). Individually, each examiner had an improvement in the number of lesions diagnosed when comparing group assessment (p<0.001). Kappa index was superior to 0.60 for all examiners in standard group.
Conclusion: In conclusion, the addition of true lateral view was able to detect misdiagnosed injuries in lesser toes trauma and improved the number of diagnosed lesions in 84.6%.
DOI: 10.1177/2473011421S00339
Influence of Weight-Bearing Computed Tomography in the New Staging System of Progressive Collapsing Foot Deformity Classification
Nacime S. Mansur, MD; Hee Young Lee; Amanda Ehret; Matthieu Lalevee, MD; Caleb J. Iehl; Mark S. Myerson, MD; Alessio Bernasconi, MD PhD FEBOT; Kristian Buedts, MD; Francois Lintz, MD MSc FEBOT; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: The same Consensus that proposed a new nomenclature for Flatfoot, Progressive Collapsing Foot Deformity (PCFD), also introduced a new classification system for the disease. The idea of staging was supplemented by the construction of a system combining deformity classes and its flexibilities, using clinical and radiographic signs. The capacity of the weight-bearing computed tomography (WBCT) in evaluating PCFD and all components of peritalar subluxation has been established. The objective of this study was to compare PCFD classifications performed utilizing clinical and conventional radiographs (CR) findings with classifications established using clinical and WBCT findings. We hypothesized that evaluations considering WBCT would significantly change PCFD classifications, portraying a different picture of the disease.
Methods: This retrospective IRB-approved case-control diagnostic study evaluated 89 consecutive PCFD feet (84 patients) with different presentations of the disease. Three fellowship-trained foot and ankle surgeons performed chart reviews and CR evaluations, determining PCFD classifications for the studied subjects. After a two-week washout period, the sequence was randomized, and a new classification was executed using clinical data and WBCT assessment. One of the readers repeated the WBCT evaluation two weeks later for intrarater reliability purposes. Assessments included presence or absence of classes, such as hindfoot valgus (A), midfoot abduction/sinus tarsi impingement (B), medial column instability (C), subtalar joint subluxation/subfibular impingement (D) and valgus of the ankle joint (E) as well as flexibility (1) and rigidity (2) of existing deformities. Fleiss kappa was used for interrater and Cohen’s kappa for intrarater agreements. Differences between studied groups were determined by distribution comparison.
Results: Mean BMI and age were 54.4 (+-17.1) and 33.6 (+-7.6) respectively. Interrater reliability was found to be moderate (0.55) and intrarater to be excellent (0.98). Evaluation using CR produced 22.8% of 1ABC, 13% of 1AC, 8,7% of 1ABCD and 7% of 2EABCD as most prevalent classifications. WBCT assessment found 31.5% of 1ABC, 11.2% of 1ABCD, 10.1% of 2ABCDE and 5.6% 1ABCDE. Class A was the most frequent component in CR (93.5%) and WBCT (94.5%). Class B had a higher prevalence in WBCT (94.38%) than in CR (71.7%) as well as Classes C (89.9% and 88.0%), D (44.9% and 29.3%) and E (31.5% and 23.9%). The percentage of combined flexible (1) and rigid (2) deformities was also higher in the WBCT evaluation (39.3% compared to 35.8%).
Conclusion: As the new classification proposes the combination of different PCFD components to better support clinical decisions, proper identification of the classes is mandatory for a complete diagnosis. WBCT showed a different rate of deformity recognition, which increased the incidence of all classes, especially B (midfoot abduction/sinus tarsi impingement) and D (peritalar subluxation/subfibular impingement). An excellent intrarater agreement was found, which infers reliability of patient assessment combining clinical and WBCT evaluation. The obtained information could help providers to enhance comprehension of the disease and to supply patients with the most precise individual care.
DOI: 10.1177/2473011421S00340
Medial and Lateral Combined Ligament Arthroscopic Repair for Multidirectional Ankle Instability: Case Series
Nacime S. Mansur, MD; Andre Vitor Lemos, MD, MSc; Daniel Baumfeld, MD; Tiago S. Baumfeld, MD; Marcelo P. Prado, MD, PhD; Fernando C. Raduan, MD; Caio A. Nery
Category: Arthroscopy; Sports
Keywords: Ankle Arthroscopy; Ligament; Deltoid
Introduction/Purpose: The high prevalence of ankle sprains in the population produces a significant number of patients with lateral instability. Maintenance of this condition may lead to the progressive involvement of medial structures, causing a multidirectional rotational instability.
Methods: This is a retrospective study with patients diagnosed with multidirectional instability, submitted to an ankle arthroscopy with medial (arthroscopic tensioning) and lateral repair (arthroscopic Bröstrom) between January 2018 and January 2020. All patients were evaluated for pain and function according to the VAS and the AOFAS Score at a mean of 14.8 months (5-27 months) in follow-up.
Results: A total of 30 ankles (29 patients) were included in the study. AOFAS score increase from a 49.7 (CI 5.8) to a 91.9 (CI 2.4) mean (p=0.001) and was followed by significant improvement in the mean VAS (6.83; CI 0.37 to 0.95; CI 0.31). The majority of patients had associated procedures (53.3%) and a low complication rate was found (16.6%).
Conclusion: Combined medial and lateral arthroscopic repair might be an effective and safe alternative in the treatment of multidirectional instability. Inclusion of the deltoid ligament complex and the low invasiveness of the arthroscopic technique can improve the clinical outcomes of these patients.
DOI: 10.1177/2473011421S00341
Percutaneous Distal Metatarsal Mini-Invasive Osteotomy: Comparison Between Standard vs Modified Intraosseous Approach: A Cadaveric Study
Nacime S. Mansur, MD; Fernando S. Martins; Elijah Auch; Ivan C. Giarola; Shuyuan Li, MD, PhD; Matthieu Lalevée; Kevin N. Dibbern, PhD; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Minimally invasive surgery (MIS) of the forefoot has gained popularity as an alternative to traditional open procedures for the treatment of metatarsalgia and hammertoe deformity. Distal metatarsal mini-invasive osteotomy (DMMO) is an extraarticular osteotomy done in a percutaneous manner, with minimal soft tissue dissection that permits elevation as well as shortening. However, there is concern for damage to vital structures due to lack of direct visualization. The objective of the study was to evaluate the structures at risk in standard versus modified DMMO.
Methods: 11 thawed fresh-frozen cadaveric specimens underwent minimally invasive DMMO using both the standard and modified approach. The standard technique was performed by moving the burr in a circular motion with an angle of 45° (right- handed surgeon), which cut sequentially the left, plantar, right and dorsal cortices. It was compared to a modified intraosseous technique requiring less wrist supination while remaining intraosseous. After completion of the procedures, the cadavers were fully dissected and analysed to identify unintentional injury to soft tissue structures and to verify if cuts were completely extraarticular and performed with proper angulation.
Results: In the standard group the most commonly injured structures were the metatarsal joint capsules (MJC) (27%), extensor digitorum longus (EDL) (18%), and extensor digitorum brevis (EDB) (9%). The modified intraosseous group demonstrated injury to the EDL (27%), while MJC (0%) and EDB (0%) were not damaged. Distances between osteotomies and structures were 6.08 +- 3.99 mm from the dorsal metatarsal head articular surface (DMHAS), 4.85 +- 2.45 mm from EDB and 0.76 +- 1.72 mm from the EDL in the standard group and 9.92 +- 3.42 mm from the DMHAS, 4.71 +- 3.24 mm from EDB and 1.24 +- 1.84 mm from the EDL in the modified group. Statistically significant difference was found among osteotomy site and DMHAS (p=0.02).
Conclusion: The most frequently injured structure was the EDL tendon with both DMMO techniques used. Intra-articular positioning of the osteotomy was more frequently observed in the standard technique. There was also a statistically significant difference between the distance of the osteotomy site and the dorsal metatarsal head articular surface when comparing the standard group and the modified group. Overall, it appears that the modified method could be a safer, less complex alternative to the standard DMMO technique, especially for the inexperienced surgeons.
DOI: 10.1177/2473011421S00342
Predictors of Deformity in Patients with Progressive Collapsing Foot Deformity and Valgus of the Ankle
Nacime S. Mansur, MD; Matthieu Lalevee, MD; Victoria Vivtcharenko, BS; Kevin N. Dibbern, PhD; Scott J. Ellis, MD; Jonathan T. Deland, MD; Alexandre L. Godoy-Santos, MD; John E. Femino, MD; Elijah Auch; Cesar de Cesar Netto, MD, PhD
Introduction/Purpose: Markers of diagnosis and severity are well studied in patients with Progressive Collapsing Foot Deformity (PCFD). Medial facet subluxation (MFS) in weight-bearing computerized tomography (WBCT) has been established as an indicator of peritalar subluxation and an earlier detector of the disease. When the disease affects the ankle leading to a valgus talar tilt (class E), structures distal to this topography may behavior differently, trying to compensate proximal deformity. The aim of this study is to assess predictors of deformity in PCFD patients with and without valgus of the ankle. Our hypothesis is that MFS could not be used in class E patients as an accurate value for estimation and staging of PCFD.
Methods: In this IRB-approved retrospective case-control study we analyzed WBCT acquisitions of 21 consecutive patients with PCFD presenting valgus of the ankle and 64 controls (flexible PCFD with no ankle involvement). MFS (percentage of uncoverage), middle facet incongruence angle, middle cuneiform-to-floor distance, forefoot arch angle, talonavicular uncoverage angle, hindfoot moment arm (HMA), Foot and Ankle Offstet (FAO) and talar tilt angle (TTA) were obtained and compared between groups using oneway ANOVA. A multivariate regression analysis was performed to evaluate which of the measurements influenced the alignment. A partition prediction model was also constructed to find how the variables contributed to the deformity and its aspects. Statistical significancy was set in p values <0.05.
Results: We found differences among groups only for MFS, HMA, FAO and TTA, with a lower mean value of MFS in patients with valgus of the ankle. An inverse relation between MFS and TTA was obtained in this group, demonstrated by increase in the talar tilt and decrease in middle facet uncoverage. MFS affected FAO values in the control group (R2: 0.25) but not in the ankle valgus group (R2: 0.001), being that this last one was influenced mainly by the TTA (R2: 0.53). A FAO value higher than 12.14 was found to be a strong predictor of deformity at the ankle.
Conclusion: MFS was lower in patients with PCFD and valgus of the ankle, demonstrated as a weak predictor of deformity severity. In this group of patients (class E), talar tilt angle and Foot and Ankle Offset should be used as disease markers. A FAO value above 12.14 must be appreciated as a possible sign of ankle involvement in PCFD patients.
DOI: 10.1177/2473011421S00343
Shock Wave Therapy Associated with Eccentric Strengthening vs Isolated Eccentric Strengthening for Achilles Insertional Tendinopathy Treatment: A Double Blinded Randomized Clinical Trial
Nacime S. Mansur, MD; Oreste L. Carrazzone; Fabio Teruo Matsunaga, MD, PhD; Flávio Faloppa, MD, PhD; Marcel Jun Sugawara Tamaoki
Introduction/Purpose: Lack of consensus inhibits Achilles insertional tendinopathy (AIT) management. The condition is usually treated with eccentric exercises (EE), despite its absence of satisfactory and standing results. Shock wave therapy (SWT) was presented as an alternative, but it is still supported by a paucity of studies that shows moderate outcomes. The purpose of this study is to determine if the association of shock wave therapy (SWT) with the eccentric exercises (EE) protocol improve rates of pain and function in patients with AIT.
Methods: This was a single-centre, double blind, placebo-controlled, in parallel groups, randomized clinical trial. 119 patients diagnosed with AIT, were evaluated, and enrolled in the study from February 2017 to February 2019. They were divided in two treatment groups, SWT associated to EE (SWT group) and EE associated to sham (CON group). Three sessions of radial shockwaves (or sham) separated by 2 weeks and eccentric training for three months were applied. The primary outcome was the Victorian Institute of Sport Assessment-Achilles questionnaire (VISA-A) at 24 weeks. Secondary outcomes included the Visual Analogue Scale (VAS), Algometry, the Foot and Ankle Outcome Score (FAOS) and the 12 Item Short Form Health Survey (SF-12).
Results: Both groups showed significant improvement with the corresponding treatment in the study period. However, there were no between-group differences (all ps > 0.05) in any of the outcomes. At the 24th week evaluation, the SWT group exhibited a mean VISA-A of 63.2 (CI 8.0) and the CON group of 62.3 (CI 6.9), p=0.876. Failures were higher in the SWT (38.3% to 11.5%, p=0.002) and recurrences were superior in the CON side (34.6% to 17.0%, p=0.047). There were no complications.
Conclusion: Extracorporeal shockwave therapy does not potentialize the effects of eccentric strengthening in the management of Achilles insertional tendinopathy.
DOI: 10.1177/2473011421S00344
Calculation of Minimally Clinically Important Difference in VAS, SF-36, and LSA Scores for Hallux Rigidus Correction Via MTP Fusion
Wesley J. Manz; Matthew Lunati; Joel Greenshields; Joel A. Zaldumbide; Rishin J. Kadakia, MD; Michelle M. Coleman, MD, PhD; Jason T. Bariteau, MD
Introduction/Purpose: Hallux rigidus is a mobility limiting disease commonly seen in elderly patient populations. Correction via metatarsophalangeal (MTP) fusion has been shown to be a safe and effective means of treatment in these populations relative to younger cohorts. An increasingly important measure of surgical efficacy is the establishment of patient-reported outcomes for achieving meaningful change through a procedure. Calculation of a minimally clinically important difference (MCID) has been established to illuminate these thresholds. The objective of this study was to calculate MCID thresholds for visual analogue pain (VAS), Short Form 26 Health survey (SF-36), and LifeSpace Mobility Assessment (LSA) following first MTP fusion.
Methods: A prospective study of all patients undergoing MTP fusion between August 1, 2015 and July 1, 2018 by a single surgeon was conducted following IRB approval. A total of 143 patients were included in the study. Demographics and surgical data were collected from review of the electronic medical record. Patient reported VAS, SF-36, and LSA scores were collected at routine 6- month and 12-month follow-up clinic appointments, as well as preoperatively. This study utilized a distribution-based approach for calculation of MCID for each of the patient reported outcomes. The MCID was defined as 0.5 times the standard deviation of the pre-operative score, 95% bootstrap confidence intervals were creating using the bias corrected and accelerated method.
Results: The average age of patients undergoing first MTP fusion was 63.4 years (SD 10.6). Patient demographics were recorded, 25.9% of patients were current or former smokers, 60.8% had clinically managed hypertension, 9.8% had diabetes, and 31.5% carried a diagnosis of osteoarthritis. The average patient had 1.9 (SD 1.1) toes operated on during the procedure, including their MTP fusion. Mean tourniquet time was 65.6 (SD 24.8) minutes and mean operative time was 89.9 (SD 31.4) minutes. Mean (SD): VAS, 4.7 (2.8); LSA, 86.4 (35.1); SF-36 physical component score, 63.00 (19.9); SF-36 component score, 77.4 (19.8). MCID: VAS, 1.4 (95% CI 1.3 to 1.5); LSA, 17.6 (95% CI 14.4 to 21.4); SF-36 physical component score, 9.9 (95% CI 9.1 to 11.0); SF-36 mental component score, 9.8 (95% CI 8.7 to 11.4).
Conclusion: This study identifies the MCID for VAS, SF-36, and LSA following first MTP fusion. The MCID of VAS reveals minimal improvements in pain (>1.5) are clinically significant. Both SF-36 physical and mental component scores reveal narrow 10- point differences have clinically significant changes. In contrast, LSA appears to have a relatively wide MCID value for patients undergoing first MTP fusion, highlighting the need for a large increase in mobility for significant improvement.
DOI: 10.1177/2473011421S00345
Elective Foot & Ankle Procedures in the Geriatric Populations: Worth the Mobility Gains
Wesley J. Manz; Ryan Patton; Philip Oladeji; Joel A. Zaldumbide; Michelle M. Coleman, MD, PhD; Rishin J. Kadakia, MD; Jason T. Bariteau, MD
Introduction/Purpose: Chronic, non-traumatic pathologies of the foot and ankle can be mobility-limiting for patients of all ages. Given increased rates of perioperative comorbidities and the heightened risks of intraoperative complications, physicians may be more inclined to manage elderly patients with longer periods of conservative treatment for similar pathologies. However, previous work has shown that decreased mobility of elderly patients affects longevity and is linked to increased rates of all-cause and non- cancerous morbidity and mortality. Currently, little is known about the effect of elective foot and ankle procedures on mobility in patients of all ages. Therefore, the objective of this study was to compare posteroperative changes in LifeSpace Mobility Assessment (LSA) scores of adult and elderly patients following foot and ankle surgery.
Methods: A prospective study of 184 patients undergoing elective ankle, hindfoot, and midfoot procedures conducted by a single surgeon between September 1, 2015 and August 31, 2019 was undertaken following IRB approval. Patient-reported LSA scores were collected at preoperative and routine 6-month and 12-month follow-up clinic appointments. Patient demographic and surgical data were recorded, and they were divided into groups by age over and under 65 years. Demographics and surgical characteristics were compared utilizing an independent sample t-test for continuous, normally distributed data and a chi-squared or Fischer’s exact test for categorical data. Alpha and beta were assumed to be 0.05 and 0.8, respectively.
Results: The younger (<65) group included 140 patients (mean age 44.1, SD 13.2), while 44 patients were observed in the elderly (>=65) age group (mean age 70.4 years, SD 8.4 (p<0.0001). The elderly group had significantly more patients with hypertension requiring medical management (p=0.012), but no other differences in perioperative comorbidities or demographics were observed. A higher proportion of elderly patients underwent surgery for conditions of osteoarthric origin, while younger patients underwent surgery more frequently for soft tissue pathology (p=0.033). The average LSA score of elderly patients at the preoperative visit was 58.3 (SD 38.0) versus 79.3 (SD 38.8) in the younger cohort (p=0.041). Both the young and elderly patient cohorts regained and surpassed their preoperative mobility scores by 6 months and 1-year postop. No difference in average mobility score was observed between young (85.6, SD 36.1) and elderly (90.1, SD 34.3) cohorts at 1-year follow-up.
Conclusion: This study demonstrates that while elderly patients may begin with lower mobility than younger patients with foot and ankle pathology, operative treatment can improve their mobility dramatically up to comparable levels of operatively-treated younger patients. Our results, in tandem with literature showing the drastic deleterious effects of decreased mobility in the elderly, suggest that the discussion to pursue or hold on surgical correction of chronic foot and ankle disease in the patients over the age of 65 must take into account the mobility benefits of surgery.
DOI: 10.1177/2473011421S00346
Improvement of Depressive Symptoms Following Surgical Correction of Hallux Valgus and Hallux Rigidus via 1st MTP Fusion
Wesley J. Manz; Rahul K. Goel; Joel A. Zaldumbide; Rishin J. Kadakia, MD; Michelle M. Coleman, MD, PhD; Jason T. Bariteau, MD
Category: Bunion; Midfoot/Forefoot
Keywords: 1st MTP Joint; Hallux Rigidus; Hallux Valgus
Introduction/Purpose: Psychiatric comorbidity has been shown to significantly impact postoperative course, leading to increasingly complicated hospitalizations, increased pain, and worse overall patient outcomes. Achieving adequate pain management is paramount in restoring mobility and ultimately reaching treatment goals, making an understanding of the interplay between psychiatric conditions and orthopedics vitally important. Specifically, deformity of the first MTP joint has been associated with increased psychiatric symptoms preoperatively. However, despite this particular population’s vulnerability to depressive symptoms, the effects of surgical correction on mental function outcomes have not been well observed. The purpose of this study was to assess the association of psychotropic medication use in patients with diagnoses of hallux rigidus and hallux valgus undergoing first MTP fusion and differences in patient-reported pain and functionality scores.
Methods: A retrospective analysis of prospectively collected patient outcomes for those undergoing MTP fusion for hallux valgus and hallux rigidus between August 1, 2015, and July 1, 2018, was conducted. A total of 95 patients were included in the study. Demographics and surgical data were collected from a review of the electronic medical record, and patients were grouped based on chronic use of psychotropic medications at the time of surgery. Patient-reported VAS, SF-36 Mental Component Scores (MCS), and Physical Component Scores (PCS) scores were collected at preoperative and routine 6-month and 12-month postoperative follow-up clinic appointments. Categorical variables were compared using Pearson’s chi-squared test. For normally distributed data outcome scores were compared using the independent sample t-test while non-normal data comparisons were made with the Mann-Whitney U test. For all statistical tests, assumptions of α <.05 and β =.8 were made.
Results: The average age of the patients in our cohort was 63.3 (range, 39 - 83), with 42 patients in the psychotropic medication (MED) and 53 patients non-psychotropic medication (NO MED) cohorts. Mean time to final follow-up was similar between NO MED and MED groups (p=.987). No differences in mean VAS scores were detected at preoperative (p=.455), 6-month (p=.505), nor 1-year (p=.269) visits. Similarly, no differences in SF-36 PCS were detected at preoperative (p=.087), 6-month (p=.314), nor 1- year (p=.103) postoperative visits. Patients taking psychotropic medications had significantly lower mean SF-36 MCS at preoperative and 6-month postoperative visits (p=.004, p=.033, respectively). No difference in mean mental component score was detected at the 1-year postoperative visit (p=.184).
Conclusion: This study is the first to examine the surgical outcomes of patients undergoing 1st MTP fusion for hallux rigidus and hallux valgus while concurrently taking psychotropic medications. SF-36 mental component scores were depressed at preoperative baseline in the psychotropic medication cohort and improved postoperatively to a level similar to that of their non- psychotropically medicated peers. These findings suggest that psychiatric diagnoses should be considered in the discussion of conservative vs. surgical management of hallux valgus and rigidus, as a secondary benefit of surgical correction may be partial relief of depressive symptoms.
DOI: 10.1177/2473011421S00347
Marked Mobility Improvement: Men and Women Respond Similarly to Operative Treatment of Foot & Ankle Pathologies
Wesley J. Manz; Philip Oladeji; Ryan Patton; Joel A. Zaldumbide; Michelle M. Coleman, MD, PhD; Rishin J. Kadakia, MD; Jason T. Bariteau, MD
Introduction/Purpose: Differences between men and women in the perception, incidence, and outcomes of various orthopaedic injuries are well-documented. Recent studies have noted that women display increased ankle ligamentous laxity and double the rate of ankle sprains in relation to their male peers. Current studies indicate that, in general, women and men respond similarly to surgical correction of such pathologies. However, a gender difference in mobility has not been investigated. Given the mobility implications associated with chronic foot and ankle conditions, a need exists to better characterize baseline and postoperative functionality in men and women. The objective of this study was to assess changes in LifeSpace Mobility Assessment (LSA) scores of male and female patients following surgical correction of non-traumatic ankle, hindfoot, and midfoot conditions.
Methods: A prospective study of elective ankle, hindfoot, and midfoot procedures conducted by a single surgeon between September 1, 2015 and August 31, 2019 was undertaken following IRB approval. LSA scores on 184 patients - 137 women and 53 men - were collected at preoperative, 3-month, 6-month, and 12-month clinic visits. The electronic medical record was queried for patient demographic and surgical data. Demographics, surgical factors, and patient-reported LSA scores were compared utilizing an independent sample t-test for continuous, normally distributed data. All categorical data was analyzed with a chi- squared or Fischer’s exact tests. Alpha and beta were set at 0.05 and 0.8, respectively.
Results: The average age of female participants was 51.2 (SD 16.4) years and 48.2 (SD 17.1) years for male participants (p=0.273). There were no significant differences in frequencies of comorbidities (p>0.05). Men and women in this cohort underwent elective foot and ankle surgery for a similar diseases processes, most commonly soft tissue pathology, followed by osteoarthritis (p=0.440). Women had significantly lower LSA scores at preoperative (63.7 [SD 38.1] vs. 84.8 [SD 35.9], p=0.002), 3 month postoperative (52.5 [SD 33.8] vs. 69.9 [SD 34.5], p=0.006), and 1 year postoperative (81.2 [SD 37.2] vs. 105.5 [SD 18.2], p=0.019) timepoints relative to their male peers. No differences in mobility at 6 months postop were observed (p=0.714). Overall, women and men had similar absolute increases in postoperative mobility at 1-year after surgery (17.5 vs. 20.7, p>0.05) as well as similar percentage of increased mobility (27% vs. 24%, p>0.05).
Conclusion: The present study provides further evidence of the gender differences in chronic foot and ankle pathologies. Both sexes improved similarly pre to postoperatively, however, women did not reach the same level of absolute mobility as their male counterparts. Prior studies have shown that women characterize a greater degree of limitation with foot and ankle conditions as 'normal' relative to men, making it plausible that they delay treatment until they become more severely symptomatic than men. This persistent deficit highlights the importance of early recognition of mobility impairment in order to preserve function among the sexes in foot and ankle care.
DOI: 10.1177/2473011421S00348
Complications Associated with Anesthetic Choice for Elective Foot and Ankle Surgery
John R. Martin; Haroon Kisana; Clayton Hui; Chad Stecher; Joshua Hustedt, MD
Introduction/Purpose: Wide-awake anesthesia (local anesthesia without sedation) is rarely utilized during elective foot and ankle surgery. As such, the rate of post-operative complications following wide-awake foot and ankle surgery is unknown. The aim of this study was to compare rates of early post-operative complications for wide-awake anesthesia to general/local anesthesia with sedation for elective foot and ankle procedures conditional on a wide range of observable patient characteristics and risk factors.
Methods: Patients that underwent an elective foot or ankle surgery were identified in the American College of Surgeon’s National Surgical Quality Improvement Program (NSQIP) dataset. The rate of thirty-day post-operative complications was compared between patients who received wide-awake anesthesia and those who received general/local anesthesia with sedation using logistic regressions that controlled for patient risk factors.
Results: Between 2005 and 2017, 85,363 patients were identified has having any foot and ankle procedure. After excluding observations with missing anesthesia type data information and non-elective foot and ankle procedures, the analytic cohort had 16,743 patients. There were 1,401 (8.4%) patients who underwent wide-awake anesthesia and 15,342 (91.6%) patients who underwent general/local anesthesia with sedation over the entire sample. Starting in 2007, there was an annual increase in the likelihood of using general/local anesthesia with sedation for foot and ankle procedures of 0.7 percentage points (p = 0.001). Overall, general/local anesthesia with sedation increased the odds of experiencing any complication within the first thirty days by 1.523 (95% CI 1.152 - 2.014).
Conclusion: Although wide-awake surgery is rarely performed for elective foot and ankle procedures, utilization of local anesthesia without sedation may result in fewer post-operative complications in the first thirty days. Existing trends in the use of sedation for foot and ankle procedures show that physicians are increasingly favoring general/local anesthesia with sedation, but our findings caution against this choice and suggest that post-operative complication rates may correspondingly increase.
DOI: 10.1177/2473011421S00349
Arthroscopic Reduction and Internal Fixation of Talus Fractures: An All-Inside Soft-Tissue Preserving Technique
Kevin D. Martin, DO; Adam T. Groth, MD
Category: Ankle; Hindfoot; Trauma
Keywords: Talus; Arthroscopic; Talus Fractures
Introduction/Purpose: Talus fractures, although rare, can lead to devastating complications of posttraumatic osteoarthritis (PTA), mal-union, non-unions and avascular necrosis (AVN). The timing and method of fixation has been controversial, especially for open and extruded fractures. The purpose of this study is to present short term outcomes using a posterior talus arthroscopic reduction internal fixation (TARIF) technique.
Methods: We performed a retrospective study on 12 consecutive patients undergoing primary posterior arthroscopic reduction internal fixation for talus fractures from August 2020 to January 2021. All cases were performed completely arthroscopically, utilizing a posterior approach and cannulated screws. Patient demographics, fracture pattern, perioperative complications, and radiographic findings were collected.
Results: The mean age of our cohort was 37.3 years (range, 19-75), including 6 males and 6 females, with 58% utilizing nicotine. Motor vehicle accidents accounted for 58% of injuries, followed by falls and gunshot wounds. Fracture location included 7 body fractures, 5 neck fractures Hawkins type 2 (1), 3 (3), and 4 (1). Five fractures were open injuries, 2 of which had vascular injuries that underwent irrigation and debridement followed by external fixation. Intraoperatively, all patients had 2-3 anterior to posterior 3.5mm cannulated headless screws placed with a mean tourniquet time of 87 minutes (range, 0 - 88). Postoperatively, all fractures had the articular surface restored to within 2mm on radiographs. No patients required antibiotics and no debridement’s were performed. No acute AVN has been recorded.
Conclusion: Our short-term results indicate posterior arthroscopic reduction internal fixation of talus fractures are safe and able to restore the articular surfaces. It also suggests that an all-inside soft-tissue preserving technique may reduce short term complications.
DOI: 10.1177/2473011421S00350
Austere Lower Extremity Splinting: A Head-To-Head Comparison of A New Novel 1-Step Spray-On Splint Verse Standard Splinting
Kevin D. Martin, DO; Tyler Webb; Thuan Ly; Adam T. Groth, MD
Introduction/Purpose: Fracture immobilization in low resource environments is a critical and common aspect of austere medical care. However, there are few studies that critically investigate the efficacy and consistency of current practices. The purpose of this study was to compare austere immobilization techniques for lower extremity fractures while validating a splint application evlauation score sheet.
Methods: Six orthopaedic surgical residents and 2 medical students participated in a prospective analysis of austere splinting techniques that utilized a cadaveric model with a distal third tibia-fibula fracture. Each participant was observed and scored by 3 Orthopaedic surgeons. All scoring was independent using a Likert scale based on 10 splinting criteria, including quality of radiographic reduction and time to completion. The participants utilized standard equipment that included structural aluminum malleable (SAM) splints and 6-inch ACE wraps in their first attempt. A second immobilization attempt was done with a 1-step spray-on foam splint. After each splinting attempt the reduction was verified with radiographic imaging.
Results: The 1-step spray-on foam splinting technique was significantly superior (P <.05) in all parameters. Respectively yielding a mean score of 42.3 (range: 38-50), safety 4.7 (range: 3-5), longitudinal traction 4.5 (range: 3-5), time 136 seconds (range: 99-162). The standard splinting resulted in a mean score of 34.2 (22 - 46), safety 2.8 (range: 1- 5), longitudinal traction 4.1 (range: 3-5), time 169.5 seconds (range: 94-254). No catastrophic failures were noted in either group. A strong interobserver reliability was established.
Conclusion: A 1-step spray-on foam splinting technique demonstrated consistent superiority in reducing fracture motion, potential soft-tissue damage, and sustained longitudinal traction as compared to the standard technique. Secondly, our results validate our splinting evaluation criteria allowing for further utilization in training austere splinting.
DOI: 10.1177/2473011421S00351
Rates of Complications Following Lower Extremity Amputations: A Retrospective Chart Review
Brandon Martinazzi, BS; Zachary Koroneos; Chris M. Stauch, BS; Kristen M. Manto, BS; Anna Ptasinski; Michael C. Aynardi, MD
Category: Ankle; Diabetes; Hindfoot; Lesser Toes; Midfoot/Forefoot; Trauma; Other
Introduction/Purpose: Lower extremity amputations are commonly used in the field of orthopaedics to treat infections, trauma, and severe complications associated with diabetic foot ulcers. These procedures are often associated with high rates of unplanned reoperations, hospitalizations, and numerous postoperative complications. As a result, lower extremity amputations place added physical, emotional and financial stress on patients which can negatively impact outcomes. The aim of this study was to evaluate types of postoperative complications and the rate at which they occurred in an effort to improve future patient outcomes.
Methods: Following institutional board approval, all patients at a single academic institution that underwent lower extremity amputation, by a single surgeon, from January 2017 to December 2020 were queried using hospital electronic medical records. Patient charts were followed from the date of surgery until their last follow up appointment in order to identify potential complications.
Results: 135 patients underwent lower extremity amputation from 2017-2020. 102 were male (75.5%) and 33 were female (24.4%). The average age of the patients identified was 61.1. The oldest patient was 95 and the youngest patient was 13. The average number of days to a noted complication following amputation was 93.3. The earliest complication occurred 11 days after surgery, while the longest occurred 396 days. Of the 135 patients, 7 patients had revision of their amputation (5.2%), 4 had significant wound dehiscence (3%), 7 had delayed wound healing and excess fluid drainage (5.2%), 4 had postoperative infection (3%), and 4 were noted to have developed phantom limb (3%).
Conclusion: Lower extremity amputations continue to be associated with high rates of postoperative complications. This data demonstrates that additional surgical revisions and delayed wound healing were the most common postoperative complications in our cohort.
DOI: 10.1177/2473011421S00352
Mini-Invasive Approach and Minor Amputation in the Management of Diabetic Foot Ulcer: A Retrospective Study of 110 Cases
Fabrizio Marzano; Paolo Ceccarini, MD; Rosario Petruccelli; Lorenzo di Giacomo; Giuseppe Rinonapoli, MD; Auro Caraffa
Introduction/Purpose: The diabetic foot is an increasing issue over the last years. The 25% of diabetic patients have a risk to develop a diabetic foot ulcer (DFU) in their lifetime, among these, the 28% of patients will result in an amputation. The amputation is associated with a high rate of complications. Therefore, percutaneous mini-invasive (PMI) approaches and minor amputations (MA) have a widespread use in the last years. The aim of our work is to evaluate the clinical and functional outcomes of PMI and MA in the treatment of recurrences and unhealed DFU after conservative treatment.
Methods: We retrospectively enrolled 110 patients treated in our orthopedic department in Perugia between January 2012 and October 2019. Included were the patients underwent to a PMI or MA treatment after failed conservative treatment for 12 weeks. The PMI technique consist of flexor tenotomy, metatarsal osteotomy and resection arthroplasty sec. Kessler. DFU were classified according to the Texas Foot Ulcer Classification. Exclusion criteria were: patient affected by peripheral vasculopathy disease, previous major amputation, psychiatric disease. The patients were divided in 2 groups. The group A included 57 patients treated with PMI, mean age 62.8 y.o. (range 50-80). The group B included 53 patients treated with MI, mean age 66.2 y.o. (range 53-85). The mean follow up was 18 months (range 4-40 months). Clinical outcomes, complication’s rate, functional scores (FFI and VAS- FA) were assessed. The statistical analysis was performed with the t-student test, the significativity value was set p<0.05.
Results: In the group A, the patients had a healing’s rate in 90,7 % of cases, the ulcer was healed in average in 5.77 weeks ( range 4-8.1). The postoperative complications accounts 35% of cases, including 2 cases of osteomyelitis, 1 acute Charcot foot, 1 case of acute renal insufficiency and pneumonia. Transfer ulcer occurred in 12.96%. Overall a reintervention with a mini-invasive approach was performed in 2 cases. Group B healed in 77% of cases, in a mean time of 9.11 weeks (range 8-13.3), no postoperative complication occurred. In 23% of patients occurred a transfer ulcer after an average time of 30 months, in 1 case a major amputation was mandatory. The mean value at postoperative follow-up was 78 for VAS-FA for group A and 72.2 for group B, the FFIindex was 70% for group A and 68% for group B.
Conclusion: The PMI and AM are effective procedures for the treatment of DFU, associated with low complications rate, fast recovery and ulcer’s healing process, low rate of recurrences and ulcer transfer. Overall the percutaneous technique show encouraging results, however, these procedures must be addressed to the patient’s feature. As prospective, in the future percutaneous treatments might play a role in prevention’s strategy.
DOI: 10.1177/2473011421S00353
The UK Foot and Ankle COVID-19 National (FAlCoN) Audit – Regional Variations in COVID-19 Infection and National Foot and Ankle Surgical Activity
Lyndon W. Mason; Karan Malhotra, MRCS; Jitendra Mangwani, MBBS,MS(Orth),FRCS(Tr&Orth)
Introduction/Purpose: Aims: This paper details the impact of COVID-19 on foot and ankle activity in the UK. It describes regional variations and COVID-19 infection rate in patients undergoing foot and ankle surgery before, during and after the first national lock-down.
Methods: Patients & Methods: This was a multicentre, retrospective, UK-based, national audit on foot and ankle patients who underwent surgery between 13th January and 31st July 2020. Data was examined pre- UK national lockdown, during lockdown (23rd March to 11th May 2020) and post-lockdown. All adult patients undergoing foot and ankle surgery in an operating theatre during the study period included from 43 participating centres in England, Scotland, Wales and Northern Ireland. Regional, demographic and COVID-19 related data were captured.
Results: 6644 patients were included. In total 0.53% of operated patients contracted COVID-19 (n=35). The rate of COVID-19 infection was highest during lockdown (2.11%, n=16) and lowest after lockdown (0.16%, n=3). Overall mean activity during lockdown was 24.44% of pre-lockdown activity with decreases in trauma, diabetic and elective foot and ankle surgery; the change in elective surgery was most marked with only 1.73% activity during lock down and 10.72% activity post lockdown as compared to pre-lockdown. There was marked regional variation in numbers of cases performed, but the proportion of decrease in cases during and after lockdown was comparable between all regions. There was also a significant difference between rates of COVID- 19 and timing of peak, cumulative COVID-19 infections between regions with the highest rate noted in South East England (3.21%). The overall national peak infection rate was 1.37%, occurring during the final week of lockdown
Conclusion: National surgical activity reduced significantly for all cases across the country during lockdown with only a slow subsequent increase in elective activity. The COVID-19 infection rate and peaks differed significantly across the country.
DOI: 10.1177/2473011421S00354
The UK Foot and Ankle COVID-19 National Audit – Rate of COVID-19 Infection and 30 Day Mortality in Foot and Ankle Surgery in the UK
Lyndon W. Mason; Jitendra Mangwani, MBBS,MS(Orth),FRCS(Tr&Orth); Karan Malhotra, MRCS
Introduction/Purpose: The primary objective was to determine the incidence of COVID-19 infection and 30-day mortality in patients undergoing foot and ankle surgery during the global pandemic. Secondary objectives were to determine if there was a change in infection and complication profile with changes introduced in practice.
Methods: Design: Multicentre retrospective national audit. Setting: UK-based study on foot and ankle patients who underwent surgery between the 13th January to 31st July 2020 - examining time periods pre- UK national lockdown, during lockdown (23rd March to 11th May 2020) and post-lockdown. Participants: All adult patients undergoing foot and ankle surgery in an operating theatre during the study period included from 43 participating centres in England, Scotland, Wales and Northern Ireland. Main Outcome Measures: Variables recorded included demographics, surgical data, comorbidity data, COVID-19 and mortality rates, complications, and infection rates.
Results: 6644 patients were included. In total 0.52% of operated patients contracted COVID-19 (n=35). The overall all cause 30- day mortality rate was 0.41%, however in patients who contracted COVID-19, the mortality rate was 25.71% (n=9); this was significantly higher for patients undergoing diabetic foot surgery (75%, n=3 deaths). Matching for age, ASA and comorbidities, the OR of mortality with COVID-19 infection was 11.71 (95% CI 1.55 to 88.74, p=0.017). There were no differences in surgical complications or infection rates prior to or after lockdown, and amongst patients with and without COVID-19 infection. After lockdown COVID-19 infection rate was 0.15% and no patient died of COVID-19 infection.
Conclusion: COVID-19 infection was rare in foot and ankle patients even at the peak of lockdown. However, there was a significant mortality rate in those who contracted COVID-19. Overall surgical complications and post-operative infection rates remained unchanged during the period of this audit. Patients and treating medical personnel should be aware of the risks to enable informed decisions.
DOI: 10.1177/2473011421S00355
Does Industry Sponsorship Influence Research Productivity Among Foot and Ankle Surgeons?
Prashant Matai ; Nicholas Frane; Nick Piniella; Michael Katsigiorgis; Nick Scelzi; Gus Katsigiorgis; Adam D. Bitterman, DO
Category: Ankle; Basic Sciences/Biologics; Other
Keywords: Research Grant Funding; Ankle; Foot and Ankle Literacy Survey
Introduction/Purpose: Research productivity and success drive academic promotions in surgeons' careers. While previous studies have shown a strong relationship between research funding and academic productivity, few have analyzed that relationship in Foot and Ankle surgery. Furthermore, they have primarily used bibliometric data, such as the Hirsch index (h-index), which although is representative of an author’s impact, heavily favors physicians who have been in practice longer. There is a need for more pragmatic variables that take into account career longevity. Because there is deficient literature in the analysis of the association between industry sponsorship and research productivity among foot and ankle surgeons, we sought to narrow the gap.
Methods: A retrospective review of all articles from the 2018 issues of Foot and Ankle International Journal, Journal of Foot and Ankle Surgery and Clinical Research on Foot and Ankle Journal were queried for authors. 303 unique United States-based non trainee Foot and Ankle authors were identified, and ultimately included in the study. They were analyzed for demographic data including sex, academic title, years in practice, and specialty. We also collected bibliometric data from Scopus, including total publications, Hirsch index (h-index), m-index, and publications-to-years in practice ratio. The Center for Medicare & Medicaid Services Open Payments Database was reviewed, and total payments were collected for each author. Authors were divided into quartiles based on payment data (i.e., Quartile 1: 0-25%, etc.) for analysis. Kruskal Wallis and Mann-Whitney U tests were performed to identify significant differences between groups. A Multivariate logistic regression was performed to identify independent predictors of high research productivity.
Results: A total of 253 (83.5%) of authors had received at least one payment. The payments received by the authors were broken down in the following quartiles.: Quartile 1, (n=77) who had payments of 0 to $171.41; Quartile 2: (n=76) $171.42 to $2515.15; Quartile 3: (n=76): $2515.16 to $34,577.36; and Quartile 4: (n=74) $34,577.37 to $8,530,326.50. Total Publication Count, H- index, M-index and publications to years in practice ratio all were significantly different and increasing between quartiles (p<0.001 for all). Multivariate logistic regressions identified both Academic status (p<0.001) and Total payments (p<0.05) as contributing factors to total number of publications, publications per year ratio, h-index and m-index, while Author order also contributed to higher h-index. Physician Sex or Level of Evidence were not significant independent contributors to the total number of publications, H-Index, M-Index or publications per year ratio in our study.
Conclusion: We identified that both industry payments and academic status are significantly correlated with higher research productivity among Foot and Ankle authors. Being the last author on a research also correlated with increased productivity. While h-index and total publications measure the research output, they fail to account for time as a confounding variable, where an individual who has been active longer in research can potentially have a higher research output. The m-index, (which is H-index divided by number of years that an author has been active) and publications-per-year ratio takes that into account, and yet our findings remained significant.
DOI: 10.1177/2473011421S00356
Hammertoe Correction with Wire Fixation of Varying Length
Patrick Mayolo; Kristin L. Kress; Paul Kang; David E. Jaffe, MD
Introduction/Purpose: Hammertoe deformities are commonly encountered and frequently require surgical intervention for pain relief and shoewear accommodation. Various techniques exist for surgical management, but proximal interphalangeal (PIP) joint fusion with Kirschner (K) -wire fixation remains an inexpensive, popular treatment. The decision to place a K wire that spans the metatarsophalangeal (MTP) joint versus only fixating the digit through the proximal phalanx is entirely dependent on provider preference and situational context. This study was performed to evaluate the effect of length of wire fixation on clinical outcomes after hammertoe reconstruction.
Methods: A retrospective review of all hammertoe reconstructions by a single fellowship trained foot and ankle surgeon from 2017-2021 was performed. Hammertoe reconstructions involved PIP arthrodesis with double wire fixation and other supplemental balancing procedures as indicated. Pins were routinely removed at between 5-6 weeks and protected heel weightbearing was generally advised. Wire length was chosen at the discretion of the surgeon intraoperatively. Patients were excluded if no radiographic follow-up was available after pin removal. Patient outcomes were evaluated with radiographs and clinic notes to assess pin length, pin complications/breakage, return to the OR, MTP congruency, and PIP union rate. A logistic regression was performed to determine the odds ratio for digit congruency and non-union status.
Results: 88 toes (45 patients) underwent hammertoe reconstruction with K wire fixation. Of these toes, 47 had wires that spanned the MTP and 41 that did not. There were 65 congruent MTP joints and 23 incongruent joints. 16 of the incongruent joints were pinned across the MTP while 31 in the congruent group were pinned. One toe in the MTP group required return to the OR for removal of a broken wire, compared to zero in the phalanx group (p=1.0). No pins broke in the phalanx group, compared to 3 in the MTP group (p=0.25). One toe in the proximal phalanx group had their pins pull out early but no return to the OR was needed. There were 26 (63.4%) PIP radiographic nonunions, compared to 21 (44.7%) in the MTP group (p=0.12).
Conclusion: Wire failure was a rare occurrence in either group. Breakage only occurred in the MTP group, but only required one surgical intervention for removal. Pinning the MTP may allow for improved deformity correction and increased stability of the hammertoe reconstruction. Pin breakage can occur, but it may be of little clinical significance. The increased stability and control of MTP correction may be worth the potential risk of pin breakage. Pin breakage may be avoided potentially by using thicker wires, earlier removal, and protected weightbearing.
DOI: 10.1177/2473011421S00357
Quality of Life Improvement Following Reconstruction of Midtarsal Charcot Foot Deformity: A Five Year Follow-Up
Patrick C. McGregor, MD; Madeline M. Lyons, MD; Michael S. Pinzur, MD
Introduction/Purpose: Previous data has suggested that patients have significant clinical improvement after reconstruction of diabetes-associated Charcot foot arthropathy at one year postoperatively. The purpose of this study is to re-evaluate a cohort of patients who were previously surveyed pre-operatively and 1 year post-operatively following Charcot foot reconstruction to determine if improvements in quality of life measures were sustained at a 5-year interval post-operatively.
Methods: Twenty-four patients were contacted to repeat the Short Musculoskeletal Function Assessment (SMFA) 5 years after their index Charcot foot reconstruction. The same cohort of patients had completed the SMFA pre-operatively and at 1 year post-operatively. The response to items were summated to establish scores on the dysfunction and bother indices. The scores were then standardized to range from 0 to 100 with use of the published scoring formula. Poorer function is indicated by higher scores. Descriptive statistics were utilized to analyze the differences between the preoperative and five year data for the group. Sixteen of the initial 24 study patients (66.6%) were successfully contacted and completed the SMFA survey at five years postoperatively; 2 of the 16 had subsequently undergone amputation.
Results: Fourteen patients who had previously completed the SMFA preoperatively and 1 year postoperatively after Charcot foot reconstruction in a circular frame were contacted and again completed the SMFA instrument. Improvement was noted in all domains measured by the SMFA between preoperative scores and five years postoperative scores; there was a 17-point decrease in the SMFA standardized functional index and a 3.6-point decrease in bother index. Similarly, when looking at individual domains, there was a 8.7-point decrease in difficulty with daily activities, 4-point improvement in emotion, and 5.7-point improvement in mobility. There was a statistically significant improvement in difficulty with daily activities at five years (p = 0.037), All other domains assessed by the SMFA demonstrated improvement between the two time periods, but did not reach significance due to the limited sample size.
Conclusion: Successful correction of non-plantigrade midtarsal Charcot foot arthropathy is associated with a clinically meaningful improvement in health-related quality of life at both one and five years postoperatively, including independence with daily activities. This further supports the modern paradigm shift towards operative correction of this deformity.
DOI: 10.1177/2473011421S00358
The Influence of Sex on Outcomes at Various Time Points after Total Ankle Arthroplasty
Katherine M. McGurk; Daniel J. Scott, MD, MBA; Caroline P. Hoch; Luigi Manzi, MD; Federico Giuseppe Usuelli, MD; Christopher E. Gross, MD
Introduction/Purpose: Total ankle arthroplasty (TAA) is regarded as an increasingly accepted alternative to ankle arthrodesis in patients with ankle arthritis that have failed conservative management. While significant focus within orthopedic literature has been placed on determining various risk factors for particular outcomes, the stratification of outcomes based on sex has been insufficiently investigated. Moreover, as the number of TAAs performed continues to increase, there is a growing need to examine the effects of sex on outcomes after TAA. We sought to compare patient reported outcome measures (PROMs), ankle range of motion (ROM), and complications at multiple time points in the post-operative period after TAA as stratified by sex.
Methods: undergoing TAA during the years 2013 to 2018 at a single academic institution who had minimum follow-up of two years. A total of 133 patients met inclusion criteria, comprising 55.6% males and 44.4% females. Patients were evaluated pre- operatively and at 6 months, 1-year, and 2-years post-operatively. PROMs, including the American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot Score, Visual Analog Scale (VAS) score, and the Short Form - 12 (SF-12) were administered, and ROM was assessed at all time points. Post-operative complications were also recorded. Student t-test were used to determine differences between the outcome measures. Eighty-nine patients received the Zimmer total ankle (39 females), whereas 44 patients (20 females) received the mobile bearing Hintegra.
Results: The average age was 53.6 in the male cohort as compared to 53.8 in the female cohort (p=0.93). Both pre-operatively and at 6-months post-operative, the cohorts did not differ statistically in any of the measured outcomes. At 1-year post-operative, females had a lower SF-12 PCS score (44.1 versus 47.1, p=0.019) and less plantarflexion (20.5 versus 23.5, p=0.029) as compared to males. While both cohorts saw a significant step-wise increase in AOFAS scores between pre-operative, 6-months, and 1-year post-operative (p<0.001), the AOFAS score of the female cohort plateaued at 1-year while the male cohort continued to improve significantly (<0.015). Ultimately by 2-years post-operative, females had a statistically significant lower AOFAS score as compared to males (80.3 versus 85.4, p=0.04).
Conclusion: Our results show that while both cohorts experienced significant improvement in all measured outcomes, women have lower SF-12 PCS scores and AOFAS score at 1- and 2-years post-operative, respectively, as well as less plantarflexion at 1- year post-operative with a trend towards increased complication rate after TAA. While our results add to the growing body of literature supporting TAA as a reliable means of treating ankle arthritis, our results are novel in that they were stratified and analyzed based on sex. Understanding these differences in outcomes is critically important for effectively managing expectations and treating both male and female populations.
DOI: 10.1177/2473011421S00359
The Anatomic Reconstruction for Chronic Lateral Ankle Instability Utilizing Absorbable Synthetic Graft (ATLAS Procedure): Description and Short Term Follow Up
Bryon J. McKenna, DPM; Antonio M. Malloy McCoy; Bryon J. McKenna, DPM; Calvin J. Rushing, DPM; Christopher F. Hyer, DPM; Gregory C. Berlet, MD; Tyler Tewilliager
Category: Ankle
Keywords: Ankle Instability; Ankle; Ligament
Introduction/Purpose: The traditional modified Brostrom-Gould has long been the procedure of choice for addressing chronic lateral ankle instability. However, more robust techniques including anatomic reconstruction are favored for larger deformity, poor tissue quality and revision surgery. Given the inherent disadvantages of allograft and non-elastic synthetic materials, material science has sought to impact the graft choice providing alternative load sharing, permeable materials with high strength. Our institution has performed anatomic lateral ligament stabilization, termed the 'ATLAS' procedure, using a novel synthetic graft (Artelon, Marietta, GA) with anecdotal success in recent years. In this study, we present our surgical technique and early experience.
Methods: A retrospective cohort review was performed, evaluating the failure rate, complications and radiographic changes in anatomic alignment. A review of all patients undergoing the ATLAS procedure was performed, a total of 27 patients were included. The study included only those patients with at least 1 year follow up from the procedure.
Results: Only one patient had symptoms of early failure of the procedure, while none of the patients required a revision procedure. The most common complication was minor wound dehiscence (11.1%). Overall, our short-term results with this procedure were excellent.
Conclusion: We conclude that the ATLAS procedure is a predictable and effective lateral ligament reconstruction technique with no donor site morbidity, no donor tissue transmission risk, low risk of over-constraint and accomplished with a predictable technique.
DOI: 10.1177/2473011421S00360
Changes in Plantar Forces and Pressures During Functional Movement with an Intrepid Dynamic Exoskeletal Orthosis Brace
James E. Meeker, MD; Jason Weiss; Austin R. Thompson, BS; Jing Feng
Introduction/Purpose: Non-surgical interventions such as bracing using ankle foot orthoses (AFO) aim to assist, restore and redirect weightbearing forces with immobility in mind. We identified a custom carbon fiber specific energy storing AFO that was created to improve functional performance in veterans after limb salvage procedures. While being evaluated exclusively in a veteran population, the Intrepid Dynamic Exoskeletal Orthosis (IDEO) has also been indicated to be a conservative treatment option for veterans with posttraumatic osteoarthritis of the tibiotalar and subtalar joints. To evaluate the off-loading properties of the IDEO brace in a civilian population with osteoarthritis of the ankle.
Methods: Eight civilian patients 18-years or older who were prescribed an IDEO brace by a single surgeon participated in the study. Foot pressure data were recorded using Tekscan F-Scan system, an ultra-thin, in-shoe sensor that provides force and pressure information. Participants were instructed to walk at a self-selected pace along a 20 meter walkway under three conditions. Using F-Scan Research software, the stances were identified and averaged. Then, the forefoot and heel areas were identified. Next, the maximal force, force*time integral (FTI), maximal contact area, maximal contact pressure, pressure*time integral (PTI), and center of force (COF) excursion were calculated. One-way ANOVA with repeated measures was performed to detect effects of the condition (three levels: Without, Under and Over). Pairwise comparison with least significant difference (equivalent to no adjustments) was performed to detect difference among the conditions.
Results: Compared to the Without condition, the Under condition showed higher pressure in both the heel and the forefoot areas (especially in the forefoot) in most subjects; COF excursion was increased in some subjects. Compare to the Without condition, the Over condition showed reduced pressure in both the heel and the forefoot areas (especially in the forefoot) in most subjects. The statistical results below only included the involved side of the six subjects who were tested in all three conditions. Table 1 showed the results of one-way ANOVA with repeated measures of the six subjects.
Conclusion: The results of this study showed that the IDEO is effective in improving gait function and relieving forefoot pressure in the civilian population. IDEO generated force (and thus power), especially in the forefoot area in late stance, to provide more push-off power and propel the body moving forward. While acting as a functional foot, the IDEO reduced force by 66% and reduced pressure by 49% in the forefoot area, which helped to relieve pain. IDEO creates functional foot by storing power in the early stance and release power in late stance.
DOI: 10.1177/2473011421S00361
Clinical and Radiological Outcomes of Autologous Osteochondral Transplantation with and without Micronized Allograft Cartilage Matrix Augmentation for Osteochondral Lesions of the Talus
Nathaniel P. Mercer; Alan Samsonov; John Dankert, MD, PhD; John G. Kennedy, MD, FRCS(Orth)
Category: Ankle; Basic Sciences/Biologics; Trauma
Keywords: Osteochondral Lesions of the Talus; Clinical Outcomes; Biologics
Introduction/Purpose: Autologous osteochondral transplantation (AOT) using a cylindrical graft, in the treatment of osteochondral lesions of the talus (OLT) is typically indicated for patients with larger lesions. However, with lesions that are irregular in shape, the AOT graft may not completely replace the lesion. For these lesions, we utilize Extracellular Matrix Cartilage Allograft (EMCA) augmentation in AOT to act as a physiologic grout between the host and graft interface. The purpose of this study was to evaluate the clinical and radiological outcomes of AOT with concentrated bone marrow aspirate (CBMA) and EMCA augmentation in the treatment of OLT.
Methods: A retrospective analysis comparing patients treated with AOT/CBMA alone and AOT with CBMA/EMCA was performed. Clinical outcomes were evaluated with the use of the Foot and Ankle Outcome Score (FAOS). Magnetic resonance imaging (MRI) was evaluated with the use of the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score. Cyst formation was also evaluated on postoperative MRI.
Results: Twenty-six patients were included in the AOT + CBMA/EMCA group, with 10 males and 16 females. Thirty-four patients were included in the AOT/CBMA group, with 17 males and 17 females. The mean symptoms, pain, ADL, sports activities, and QOL scores in FAOS significantly improved in both groups (p<0.001), but there was no significant difference between groups at final follow-up. There was no significant difference between the mean MOCART scores between groups (p=0.118). In the AOT/CBMA group, 2 patients (7.7%) complained of knee pain and 5 patients (19.2%) required additional surgery (2 hardware removals and 3 arthroscopic debridements of scar tissue in the ankle). In the AOT + CBMA/EMCA group, 3 patients (8.8%) complained of knee pain, and one patient (2.9%) required hardware removal.
Conclusion: The current study demonstrated that AOT combined with CBMA and EMCA was an effective surgical treatment for OLT, providing good clinical and radiological outcomes. However, the benefit of combining ECMA with CBMA in small chondral defects at the host graft interface may be marginal as the biologic effect is induced by the CBMA and the mechanical scaffold effect of ECMA may not be required in such small defects.
DOI: 10.1177/2473011421S00362
Clinical Outcomes of Nano Arthroscopy in the Office Setting for the Treatment of Posterior Ankle Impingement
Nathaniel P. Mercer; Alan Samsonov; John Dankert, MD, PhD;; Rick J. Delmonte; Tobias Stornebrink, MD; Arianna L. Gianakos; Gino Kerkhoffs, MD; John G. Kennedy, MD, FRCS(Orth); Jari Dahmen, BSc, BSc(Med)
Introduction/Purpose: The hypothesis of the current study was that IONA in the treatment of posterior ankle impingement would provide the patient with a unique experience of their pathology and facilitate their rapid recovery through an awareness of their own condition and that using IONA would accelerate recovery to sports-specific activities compared to standard arthroscopic procedures.
Methods: This was a retrospective cohort study investigating patients who underwent IONA for posterior ankle impingement between 2019 and 2020. Clinical outcomes were evaluated using the following methods preoperatively and at final follow-up: The Foot and Ankle Outcome Scores (FAOS) and Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Interference and Pain Intensity domains. A five-point Likert scale regarding patient satisfaction was evaluated at final follow-up. Wilcoxon signed-rank test was performed to compare preoperative and postoperative outcome scores.
Results: Ten patients were included in this study, which included 4 males and 6 females with a mean age of 41.9 +- 15.5 years (range, 24-66 years) and a mean body mass index (BMI) of 28.3 +- 6.3 kg/m2 (range, 17.1 - 39.9). The mean follow-up time was 13.3 +- 2.9 months (range, 11-17 months). The mean PROMIS Pain Intensity T-score significantly decreased from 57.5 +- 8.4 preoperatively to 49.5 +- 5.5 at final follow-up (p<0.001). The mean PROMIS Pain Interference T-score decreased from 69.0 +- 5.8 preoperatively to 63.1 +- 5.8 at final follow-up (p<0.001). There were 7 patients who participated in sports activity prior to the IONA-arthroscopy procedure. Of those, 7 patients (100%) returned to their sports activities. The median time to return to sports was 4.1 weeks (range, 1 to 14 weeks). Lastly, 10 patients (100%) expressed willingness to undergo the same procedure again.
Conclusion: The current study demonstrates that IONA treatment of posterior ankle impingement results in significant pain reduction, a low complication rate and excellent patient-reported outcomes with high rates of return to work/sport. Additionally, IONA for posterior ankle impingement leads to high patient satisfaction with a significant willingness to undergo the same procedure again.
DOI: 10.1177/2473011421S00363
Clinical Outcomes of Peroneal Tendon Tears: A Systematic Review
Nathaniel P. Mercer; Arianna L. Gianakos, DO; Angela M. Mercurio; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: The purpose of this study was to provide an overview of the available evidence on peroneal tendon tears and the outcomes after surgical intervention.
Methods: A systematic review of the literature was performed using MEDLINE, Embase, and Cochrane. Criteria for inclusion were clinical studies reporting outcomes after treatment for peroneal tendon tear from August 2010 to August 2020.
Results: Nine studies evaluating 336 patients (146 males/190 females) and 336 ankles were included in this review. The mean age of included patients was 46.3 years (range, 46.0 - 56.9 years). The weighted mean follow-up was 23.8 months (range 9.2 - 78.0 months. Five surgical interventions were reported: primary repair with tenodesis, primary repair without tenodesis, FDL tendon transfer, FHL tendon transfer, and allograft reconstruction. Four studies recorded the AOFAS score, with a weighted mean preoperative score of 69.6 and a weighted mean postoperative score of 88.8. FAAM score was measured in 3 studies, which showed an improvement from 41.1 preoperatively to 84.4 postoperatively. The average overall complication rate was 38.7% (130/336) with the most commonly reported minor complication being ankle pain, which made up 46.2% of all minor complications (56/121). Primary repair without tenodesis was associated with a higher complication rate compared to any other surgical intervention (p=.001176).
Conclusion: The current systematic review showed that overall clinical outcomes were positive in lieu of the different modalities of surgical intervention for peroneal tendon tears.
DOI: 10.1177/2473011421S00364
Outcomes of Endoscopic Treatment for Plantar Fasciitis: A Systematic Review
Nathaniel P. Mercer; Leona Ward; Alexander Hoberman; Joseph J. Cronin; Eoghan T. Hurley, MB BCh BAO; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: Endoscopic plantar fascia release (EPFR) is an established operative treatment for recalcitrant plantar fasciitis. The purpose of this systematic review is to provide a comprehensive review on the outcomes of endoscopic plantar fascia release in the treatment of plantar fasciitis at mid- and long-term follow-up.
Methods: A systematic review was performed using, MEDLINE, EMBASE, and Cochrane library databases in May 2020 based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies included were evaluated with regards to the level of evidence (LOE) and quality of evidence (QoE) using the Coleman methodological score. Clinical outcomes and complications were also evaluated.
Results: Twenty-five studies including 729 feet were included in this systematic review with a mean follow-up of 25.1 months. 18 papers used the American Orthopaedic Foot & Ankle Society (AOFAS) score. The weighted mean preoperative AOFAS score was 55.6 and the postoperative score was 89.6 out of 100. The total number of patients who had complications was 117 of 729 (16.1%). The most common complication was a recurrence of pain experienced by 6.5% of patients (47 of 117).
Conclusion: Endoscopic plantar fascia release provides good clinical and functional outcomes in patients with refractory plantar fasciitis. However, this procedure is associated with a moderately high complication rate.
DOI: 10.1177/2473011421S00365
Return to Play and Clinical Outcomes in the Surgical Treatment of Peroneal Tendon Dislocation and Subluxation
Nathaniel P. Mercer; Arianna L. Gianakos, DO; Pim van Dijk, BSc(Med); Angela Mercurio; Gino Kerkhoffs; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: To provide an overview of the available evidence on peroneal tendon dislocation and subluxation as well as the outcomes after surgical intervention.
Methods: A systematic review of the literature was performed using MEDLINE, Embase, and Cochrane. Criteria for inclusion were clinical studies reporting outcomes after surgical treatment for peroneal tendon dislocation and subluxation within the last 10 years
Results: Fourteen articles evaluating a total of 321 patients were included in this review consisting of 240 males and 81 females. The weighted mean age of patients was 28.7 years (range 18-47). The weighted mean follow-up was 38.1 months (range 18 - 58). The weighted mean time to surgery was 5.32 months (range 3 - 9.5). Surgical treatments were categorized into 4 groups which comprised 13 of the 14 studies. Eleven studies recorded the AOFAS score with a weighted mean preoperative score of 65.97 and a weighted mean postoperative score of 92.9. Overall, 90% (145/162) of patients reported their satisfaction as either 'excellent' or 'good'. Time to return to play (RTP) was faster for patients who underwent SPR repair alone compared to SPR repair with groove deepening (p=0.001)
Conclusion: The current systematic review showed that overall clinical outcomes were positive in lieu of the different modalities of surgical intervention for peroneal tendon dislocation and subluxation. However, patients who received SPR repair with groove- deepening returned to sport faster than patients who received SPR repair alone.
DOI: 10.1177/2473011421S00366
The Plantar Fascia Talar Head Correlation: A Radiographic Parameter with a Distinct Threshold to Validate Flatfoot Deformity and Its Corrective Surgery on Conventional Weightbearing Radiographs
Introduction/Purpose: Corrective surgery for flexible flatfoot deformity (FD) remains controversial, and one of the main reasons for this is the lack of standardised radiographic measurements to define an FD. Previously published radiographic parameters to differentiate between a specimen with and without FD do not have a commonly accepted and distinct threshold. Such a parameter would help validate FDs and the required corrective surgery. The purpose of this study was to assess a new conventional radiographic parameter with a distinct threshold that allowed the differentiation between feet with and without an FD and evaluate its application in corrective surgery for FD.
Methods: The plantar fascia-talar head correlation (PTC) with its defined threshold was assessed by measuring the distance between the medial border of the plantar fascia [a connecting line between the medial border of the tibial sesamoid and the calcaneal insertion of the plantar fascia (mPCal)] and the centre of the talar head (DPT) on conventional dorsoplantar and lateral weightbearing radiographs; the authors were blinded to the clinical diagnosis of the 189 patients' first visits. Feet were grouped into specimens with and without an FD based on clinical examination. Then, the effect of surgical correction of FD on PTC was retrospectively evaluated on 38 patients. The intra-class correlation (ICC2) of the intra-observer reliability and the ICC2 of the inter-observer reliability of DPT measurement of 50 randomly selected specimens were calculated. The results of PTC were compared to the measurements of the lateral talar-1st metatarsal angle and the talonavicular uncoverage angle.
Results: The intra-class correlation (ICC2) of the intra-observer reliability of DPT measurement was 0.95 (95%-confidence interval CI95[0.92, 0.97]), the ICC2 of the inter-observer reliability was 0.93 (CI95 [0.89, 0.95]). PTC, lateral talar first metatarsal angle and talonavicular uncoverage angle showed a statistically significant difference between the specimens with and without a FD (Wilcoxon test p-values <0.001). However, only the discriminatory power of PTC was distinct. The sensitivity and specificity of PTC was 0.88 (95%CI: 0.77-0.95) and specificity 0.96 (95%CI: 0.92-0.98), respectively, to identify an FD, consistent with the clinical examination. The identification of a sagittal plane FD caused by midfoot osteoarthritis on a lateral conventional weightbearing radiograph before measuring DPT increased the sensitivity for the combined method to 0.98 (95%CI: 0.9-1). Thirty-five of 38 surgeries successfully corrected the FD and PTC comparable to that in subjects without an FD. The unsuccessful corrections did not adequately correct the PTC.
Conclusion: PTC is a unique and reliable radiographic parameter with an excellent threshold to confirm an FD, can be used intraoperatively to titrate the required amount for correction of FD under simulated weightbearing fluoroscopic imaging and is therefore useful to monitor and validate sufficient correction of its reconstructive surgery.PTC is an objective radiographic measurement to reliably describe the clinical subjective conclusion of any kind of FD with the exception FDs caused by an explicit midfoot pathology.
DOI: 10.1177/2473011421S00367
Isolated Gastrocnemius Recession for Flexible Adult Acquired Flatfoot Deformity
Max Michalski, MD; Christopher P. Chiodo, MD; Brady D. Greene; Kimberly K. Broughton, MD; Eric M. Bluman, MD, PhD; Jeremy T. Smith, MD
Introduction/Purpose: Adult acquired flatfoot deformity (AAFD) frequently has an associated gastrocnemius contracture, which is a primary focus of most non-operative treatment protocols. When conservative measures fail, AAFD reconstruction often includes a gastrocnemius recession. Most reconstruction procedures involve a period of post-operative non-weight-bearing, which can be difficult for elderly patients. Beginning in 2011, patients with flexible AAFD patients and at risk of non-compliance with weight-bearing restrictions, were offered a staged approach with initial isolated gastrocnemius recession followed by reconstruction, if required. Gastrocnemius recession may allow passive correction of the deformity, improve orthotic fit and obviate the need reconstruction (Figure). The goal of this study was to retrospectively evaluate patient reported outcomes following an isolated gastrocnemius recession for flexible AAFD.
Methods: A total of 49 patients met the inclusion criteria: isolated gastrocnemius recession for flexible AAFD, no previous ipsilateral surgery and >6 months follow-up. Of 49 eligible patients, 29 (31 feet) participated. Pre-operative and post-operative outcomes were compared for Foot and Ankle Ability Measure activities of daily living subscale (FAAM-ADL), visual analog scale (VAS), and the PROMIS Physical Function Short Form 10a (PROMIS PF SF 10a). Additionally, patients were asked about satisfaction, willingness to undergo the procedure again and whether orthotic provided better relief. Mean and standard deviation were compared using a two-tailed paired t-test with significance.
Results: FAAM-ADL and PROMIS PF SF 10a significantly improved from 55.9 and 37.3 pre-operatively to 71.6 and 42.0 (p=0.01, p=0.046) respectively. 70% of patients were either satisfied or very satisfied, 67% would undergo the procedure again, and 64.5% of patients had improved relief with use of orthotics post-operatively.
Conclusion: A staged approach with initial isolated gastrocnemius recession for the management of flexible AAFD in elderly patients can be effective. These results for patient recorded outcomes, patient satisfaction, willingness to undergo the procedure again and improvement in orthotic relief may guide the shared decision-making process with elderly patients when offered a reconstruction versus staged approach.
DOI: 10.1177/2473011421S00368
Endoscopic Insertional Achilles Reconstruction with Double Row Suture Bridge Reconstruction: A Technique Tip
Christopher P. Miller, MD; Jorge I. Acevedo, MD; James R. McWilliam, MD; Max Michalski, MD
Introduction/Purpose: Insertional Achilles tendinopathy can be a debilitating condition that often fails to improve with non- surgical management such as bracing and physical therapy. Traditional surgical techniques include an open debridement of the diseased tendon and resection of calcaneal spurs. This is followed by repair of the tendon. Suture anchors are often used to secure the tendon, but recent advances in tendon fixation, including the advent of double row repairs, has allowed better biomechanical repairs and faster rehabilitation. Additionally, minimally invasive surgery (MIS) and endoscopic techniques have advanced to allow successful treatment of all aspects of the condition while minimizing wound complications and infection
Methods: The authors present a technique to treat insertional Achilles tendinopathy and calcaneal bone spurs using MIS techniques while also incorporating a percutaneous double row suture anchor repair. The technique utilizes four portals to access two endoscopic working planes. The burr is inserted deep to the tendon and the calcaneoplasty is performed. Subsequently, the endoscope is inserted alongside a shaver to remove bony debris and debulk the anterior aspect of the Achilles areas of tendinopathy. Following this, the portals are used to place a double row suture anchor repair.
Results: With over 75 surgeries performed, there have been zero wound complications and patients have been able to return to full weight bearing within 10 days after surgery. Follow up outcome data is currently being collected and will be reported as a case series once sufficient patients have completed their follow up.
Conclusion: This study presents double-row repair following an endoscopic assisted MIS calcaneoplasty and Achilles debridement. The technique combines the benefits of the double row suture bridge repair with a minimal incision technique to debride the insertional tendinosis. In order to adequately debride the tendon and the posterior calcaneal tuberosity, the tendon foot print is elevated as the burr removes the bone at the insertion. The anterior portion of the tendon, which may be a pain generator as well, isdebrided endoscopically with the shaver. Finally, a double row suture bridge repair is performed in order to allow early weight bearing and rehabilitation.
DOI: 10.1177/2473011421S00369
Evaluation of the Soft Tissue Correction Improvement with Tendon Transfer in Flatfoot Deformity Reconstruction
Seyed Alireza Mirghasemi, MBBS; Helen Huetteman; Stephanie Mrowczynski; Allan M. Grant, MD; Zachary M. Vaupel, MD; Paul T. Fortin, MD
Category: Midfoot/Forefoot
Keywords: AAFD; Autograft Tendon Transfer; Tendon Transfer
Introduction/Purpose: An adult flatfoot deformity is a complex pathology that has been attempted to be addressed surgically with a variety of different procedures. Transfer of the flexor tendon has been a cornerstone of the treatment of flatfoot deformity for years. After the procedure, the appearance of the bony correction of the foot is noticeable on radiography, but after surgery when the patient begins to bear the weight the soft tissue laxity affects the achieved bony correction when compared to non- weight bearing images. This study aims to identify the effects of tendon transfer on bony and soft tissue after weight-bearing to better predict what the outcomes of surgery will be.
Methods: 29 patients were included. there were 18 patients that underwent tendon transfer as part of their flat foot correction and 11 patients that underwent non-tendon transfer procedure for correction of flat foot deformity. Imaging was performed on patient’s weight bearing (WB) and non-weight bearing (NWB) before and after surgery. X-ray measurements included Angles: calcaneal pitch (ML-CP), talo-1st metatarsal (ML-T1MT),talocalcaneal (ML-TC), talar declination (ML-Tdec), calcaneal 1st metatarsal (ML-C1MT) and Distances: talar height (ML-Tal-h), navicular height (ML-Nav-h), 1st cuneiform height (ML-1CN-h), cuboid height (ML-Cub-h), and 1st to 5th metatarsal distance (ML-1CN/5MT) in lateral X-ray and Angles: talonavicular coverage (AP-TN), talar 1st metatarsal (AP-T1MT), talar 2nd metatarsal (AP-T2MT) and Distances: talonavicular uncoverage distance in AP. The differences in measurement between the pre op post op non weight bearing considered as bony correction effect The differences in measurement between the pre op post op weight bearing considered as soft tissue effect.
Results: the results from non-weight bearing imaging, tendon transfer had a statistically significant impact on calcaneal pitch (, p=0.026), Talo-1st metatarsal (p=0.048), talar declination ( p=0.038), talar height (p=0.016), navicular height ( p=0.014), 1st cuneiform height (p=0.001), talonavicular coverage (p=0.019), talar-1st metatarsal angle (p=0.015), and talar to 2nd metatarsal angle ( p=0.001). the results from WBimaging, tendon transfer had a statistically significant impact on calcaneal pitch ( p=0.000), calcaneal 1st metatarsal (p=0.02), talar height (35 to 39, p=0.003), navicular height ( p=0.002), 1st cuneiform height (p=0.016), cuboid height ( p=0.016), 1st to 5th The post-op effect calcaneal pitch was 12 degrees of difference in NWB compared to 6 degrees of difference in WB The effect on talar height, navicular height, and 1st cuneiform height was 10mm, 9mm, and 8mm, respectively, in NWBimages. This compares to an effect of 4mm, 6mm, and 4mm, respectively, WB imaging.
Conclusion: When comparing NWB to WBimages, the effect of surgery on flat foot correction is consistently less pronounced inWB. there will be a difference between the bony correction and soft tissue correction. there is still a significant soft tissue effect seen in WBimaging. The comparison between NWB, WB changes shows that the soft tissue effect is around 50% of the bony correction on several key measurements. These include calcaneal pitch and talar, navicular, and 1st cuneiform height. These results provide a framework for establishing the soft tissue effect that tendon transfer surgery provides for flat foot correction surgery.
DOI: 10.1177/2473011421S00370
Comparing Infection Rates from Using Different Surgical Preparation Solutions and Techniques in Foot & Ankle Elective Surgery
Andrew P. Molloy, MB ChB, FRCS(Tr&Orth); Ravishanker Tangirala; Shirley A. Lyle, MBBS, MPhil, BSc; Gavin Heyes
Introduction/Purpose: Surgical site infection (SSI) after Foot & Ankle surgery ranges from 1.2% to 13.2%, higher than any other elective orthopaedic procedure. Infection is of concern for the patient and expensive for the healthcare system. SSI is multifactorial and can be divided into host-related and perioperative factors. Skin preparation is one of the key peri-operative factors in reducing SSI. The current literature supports a combined chlorhexidine and alcohol preparation technique, although there is some conflicting evidence. Most studies to date have used proxy outcomes such as growth from swabs shortly after skin preparation. There are no large scale studies which have looked at definitive clinical outcomes such as the rate of postoperative SSI.
Methods: A retrospective review of data was undertaken for two longitudinal cohorts which were using two different skin preparation solutions and techniques due to a change in hospital protocol. Each cohort was continuous and derived from the same overall populationIn cohort 1, Povidine-Iodine (Betadinetm) followed by Alcoholic Chlorhexidine was used on swabs (Double prep group). In cohort 2, 2 Alcoholic Chlorhexidine was used in a prep stick applicator. Standard criteria for diagnosing surgical site infection were used. All open injuries, procedures for ongoing infection, amputations for osteomyelitis /diabetic foot and COVID- 19 positive cases were excluded.
Results: After applying standard exclusion criteria, 919 elective F&A procedures in the Double prep group and 491 procedures were included for the Single prep groupAs these were continuous longitudinal cohorts of large scale from the same population, there is a justifiable presumption of group matchingIn cohort 1 there were 15 superficial infections (1.6%) and 3 deep (0.3%). In cohort 2 there were 18 superfical infections (3.6%) and 1 deep (0.3%). The total infections in cohort 1 were 18 (2%) and 19 in cohort 2 (3.9%)There was an increase in superficial, and therefore total infection rates, in the single prep group compared to the double prep group. These increases were statistically significant; p <0.05 with regards to superficial infection and total infection rates in the single prep group.
Conclusion: Double skin preparation, with Povidone-Iodine followed by alcoholic Chlorhexadine, statistically significantly decreases foot and ankle surgical infection rates as compared to a single alcoholic chlorhexidine skin preparation
DOI: 10.1177/2473011421S00371
Cadaveric Analysis of Plantar Fascia Tension and Windlass Mechanism and Development of Plantar Fascia-Specific Stretching Device
Kaveh Momenzadeh, MD; Caroline Williams, BA; Patrick M. Williamson; John Y. Kwon, MD; Ara Nazarian; Christopher P. Miller, MD
Introduction/Purpose: Plantar fasciitis is the most common cause of heel pain in adults, affecting 1 out of 10 of the population at some point during their lifetime. Plantar specific stretching programs are popularity among foot and ankle surgeons consisting of passively dorsiflexing foot and using thumb to apply pressure. This technique is not without limitations. Certain patients are unable to properly perform the stretching techniques, such as limited mobility from advanced age, disability, or simply from performing stretching exercises incorrectly. The aims of this study are; first, identify what configuration of plantar-specific stretching combined with applied pressure to the plantar aponeurosis generates the greatest tensional force in the plantar fascia. And second, to construct a prototype device that could simulate these forces in a hands-free technique.
Methods: Six (will be 10) fresh-frozen, morphologically normal cadaver feet (Medcure, RI) were utilized. Plantar fascia was exposed, ankle was fixed at 90-degree dorsiflexion using Calcaneo-Tibial Schanz Pin, specimen was then inverted and potted in a custom-made box (Smooth-Cast 300q, PA). Using an electromagnetic motion tracking system (Liberty, Polhemus, VT), the motion of sensors was recorded at 120 Hz. Utilizing tissue adhesive glue (Vetbond, 3M, Minnesota), the first sensor was attached to medial calcaneal tuberosity, and the second sensor was placed 5 cm distal to the first sensor on the plantar aponeurosis. Custom- built testing apparatus was made for induction of MTP dorsiflexion application of pressure on the plantar aponeurosis to mimic current conservative treatments. Weights were added to the custom build stretcher device in 10Lb increments. Strain percentage was calculated as the change in length divided by the baseline length position (condition 1) using the formula: ([L − Lo]/Lo) × 100
Results: Dorsiflexion of 2nd-5th MTPs increases strain percentage more in comparison with 1st MTP dorsiflexion (Condition 3>4>2). This might show that dorsiflexing of 1st metatarsal is less effective at straining the plantar fascia because of the midfoot motion. By adding thumb pressure, strain percentages go higher, up to a point that in condition 7 (dorsiflexing all MTPs in combination of thumb pressure) it is significantly higher than our baseline condition (P=0.0385). It is noteworthy that, stretcher device itself (condition 8), cannot replicate conditions 4 or 7 strain percentages. When adding direct pressure and weight to the stretcher device (conditions 12 and 13), strains are even higher than condition 7 and also are significantly higher than the baseline (P= 0.0090 and 0.0291 respectively).
Conclusion: The stretcher device itself is insufficient for stretching the plantar fascia, supporting the hypothesis of this study that we need a direct forceful pressure on the plantar aponeurosis as well. Our customized plantar stretcher not only can replicate the conventional stretching program, but also can produce higher strains on the plantar aponeurosis than the current manual application of plantar specific stretching. This device may impact the rehabilitation process in patients with advanced age as well as patients with spine mobility limitation who cannot perform manual stretching programs.
DOI: 10.1177/2473011421S00372
Do Closed Suction Drains Affect Postoperative Wound Healing after Total Ankle Arthroplasty?
Tara G. Moncman, DO; Brian E. Fliegel; Daniel Hameed; Joseph T. O'Neil, MD; David I. Pedowitz, MD, MS; Joseph N. Daniel, DO
Introduction/Purpose: Although most studies demonstrate no clear benefit of closed suction drains after total joint arthroplasty of the hip, knee, and shoulder, there is no study that has specifically looked at ankle arthroplasty. Despite the paucity of information regarding the potential benefit or lack thereof with postoperative closed suction drains after total ankle arthroplasty, they are still utilized in practice. The purpose of this study is to determine whether or not the use of closed suction drains after total ankle arthroplasty have an affect on wound complications in the first postoperative year.
Methods: Following a 3:1 match of patients with-drains to those without-drains, 78 patients with-drains and 28 without-drains were included for analysis. The drain group consisted of patients who had drains placed in the immediate postoperative period and removed prior to discharge from the hospital. The without-drains group acted as the control. Demographic data including age, sex, tobacco use, alcohol use, and medical comorbidities (diabetes, bleeding disorders, anemia, neuropathy, kidney disease, peripheral vascular disease, rheumatoid arthritis, history of leg ulcers or staphylococcus infection) were obtained. Follow-up data was collected and reviewed at 2 weeks, 6 weeks, 12 weeks, 6 months, and 1 year postoperative, for minor and major wound complications, as well as wound-related re-operations.
Results: At 2 weeks, 6 weeks, 12 weeks, 6 months, and 1 year postoperative, there was no statistically significant difference in wound complications with or without the use of a drain. Within the first postoperative year, a total of 4 (14.3%) patients with- drains and 24 (30.8%) patients without-drains had a wound complication. This was not statistically significant (p=0.148). The majority of wound complications were minor. A single superficial infection and two reoperations for major wound complications were noted, all of which were in patients who had a drain placed. Age, sex, tobacco use, alcohol use, as well as a history of diabetes, bleeding disorders, neuropathy, kidney disease, peripheral vascular disease, rheumatoid arthritis, and history of leg ulcers or staphylococcus infection were similar between both groups. A history of anemia was significantly higher in the drain group, however this was not associated with an increased risk of postoperative wound complications.
Conclusion: The use of a closed suction drain did not have an effect on postoperative wound complications in the first year after total ankle arthroplasty surgery. Based on the equivocal results in this study and that there is no clear consensus on the use of drains after total ankle arthroplasty surgery, the authors feel it is up to the individual surgeon to determine the necessity of use on a case-by-case basis.
DOI: 10.1177/2473011421S00373
Single Biotenodesis Screw vs Biotenodesis Screw with Cortical Button Tension Slide Technique for Flexor Hallucis Longus Transfer: A Biomechanical Analysis
Kaitlin C. Neary, MD; Sarah J. McClish; Anthony N. Khoury; Nick Denove; Coen A. Wijdicks
Introduction/Purpose: Restoration of functional plantarflexion of the ankle joint following chronic Achilles injury is achieved through transfer of the flexor hallucis longus (FHL) tendon. Fixation of the FHL tendon transfer with a cortical button tension slide technique is an advancement that has not been measured against traditional methods. The purpose of this study is to evaluate the biomechanical differences between a single biotenodesis screw versus biotenodesis screw with cortical button tension slide technique for the fixation of FHL transfer. The authors hypothesize a biomechanical advantage for the tension slide technique compared to the biotenodesis screw alone for fixation of the flexor hallucis longus in chronic Achilles pathology.
Methods: 12 pairs (n=24) of fresh-frozen cadaveric tibia-to-toe samples (6 male, 6 female) were utilized to assess the biomechanics of FHL tendon transfer fixation. All specimens underwent bone density analysis. Each pair of cadaveric samples were randomized to receive either the biotenodesis screw or the tension slide technique. FHL tendon transfer was performed via standard technique using a 6.25x15mm biotenodesis screw with the foot in 20 degrees plantarflexion. A 2.6x12mm cortical button was inserted and FHL tendon was introduced with a tension-slide technique. Biomechanical loading was applied between 20N and 60N at a rate of 1Hz for 100 cycles. Post-cyclic load to failure occurred at 1.25mm/sec. Cyclic displacement, structural stiffness, and ultimate load were derived from resultant load-displacement curves. Student t-tests were used to evaluate significant effects between both FHL tendon transfer techniques. Linear regression analysis was performed to assess interactions between bone density and strength of FHL tendon transfer.
Results: Average tendon diameter of the 24 FHL samples was 5.44+-0.46 mm. Average bone density for all 24 calcaneus samples was determined to be 1.06+-0.08 g/cm2. Loading data was normalized with respect to bone density and tendon diameter to account for inherent anatomical differences between cadaveric specimens. The addition of a cortical button for FHL transfer to the calcaneus did not significantly affect cyclic displacement (0.78+-0.52mm vs 0.87+-0.80mm) or structural stiffness (162.11+- 43.34N/mm vs. 167.57+-49.19N/mm). Addition of the cortical button to the FHL tendon transfer construct resulted in a 34% significant increase in ultimate load (343.72+-68.93 N) compared to biotenodesis screw alone (255.62+-77.17 N) (p=0.0002). Linear regression analyses did not reveal any significant interactions between bone density and FHL tendon transfer technique.
Conclusion: Enhanced strength can be achieved for Achilles pathology repaired with FHL tendon transfer utilizing a biotenodesis screw and cortical button tension slide technique demonstrated by a statistically significant 34% increase in ultimate load, subsequent to cyclic loading. Cortical buttons in the setting of FHL tendon transfer to the calcaneus offers an additional level of support in the case of extreme tendon transfer failure.
DOI: 10.1177/2473011421S00374
Plantar Plating in the Modified Lapidus Procedure: Evaluation of Function and Impairment of the Tibialis Anterior Tendon
Richard Niehaus; Sandro Hodel; Karim Eid; Christopher G. Lenz
Introduction/Purpose: Plantar Plating in the Modified Lapidus Procedure (MLP) to treat severe Hallux Valgus deformities (HVD) or hypermobility of the first ray has become more popular. Due to biomechanical considerations, early weightbearing can be achieved. The surgical procedure and some plate designs make a release of the Tibialis Anterior tendon (TAT) necessary and screws have to be placed through or close to its insertion. We investigate if there are detectable changes of the tibialis anterior tendon or the function of the tibialis anterior muscle (TAM).
Methods: We retrospectively reviewed 22 Feet (17 patients) after plantar plating for a modified Lapidus procedure. All patients underwent a MRI at an average of 27 months (range 12-49 months) postoperatively for evaluation of the tendon. Clinical outcome was evaluated using the EFAS score. Dorsiflexion strength was measured and compared to the healthy contralateral extremity. Complications and union rates were assessed.
Results: The subjective satisfaction was rated at a mean of 8.2 (range, 5 - 10; SD +-1.5) on a scale from 0 to 10. Fourteen (82%) patients would undergo the same surgical treatment again. MRI images showed signs of tendinopathy of the TAT in 13 feet (59%). There were no ruptures, signs of thinning of the tendon or fatty infiltration detected. Complication rate was low with only on case with performed revision surgery. Regarding the Range of Motion, the force data comparing both feet of the patients is statistically close in comparison to the other side without any statistical differences.
Conclusion: The MLP using a plantar-positioned locking plate leads to high patient satisfaction rates and provides significant improvement of preoperative deformity in severe HVD at midterm follow-up. Inversion strength was reduced, and MRI showed signs of tendinopathy in more than half of the cases. However, these findings did not seem to have any effect on the clinical outcome. None of the present patients had a high degree of fatty infiltration of the TAM in accordance with the Goutallier grading. Plantar-positioned locking plates do not seem to impair the TAM or the TAT.
DOI: 10.1177/2473011421S00375
Correlation of First Metatarsal Sagittal Alignment with Clinical and Functional Outcomes Following the Lapidus Procedure
Danilo Ryuko Nishikawa, MD; Fernando A. Duarte, MD; Guilherme H. Saito, MD; Bruno R. Miranda, MD; Cesar de Cesar Netto, MD, PhD; Marcelo P. Prado, MD, PhD
Introduction/Purpose: Lapidus procedure (LP) for hallux valgus (HV) requires an adequate control of first metatarsal (M1) sagittal alignment to avoid dorsiflexion. Otherwise, clinical and functional impairment, including transfer metatarsalgia may occur. This study aimed to evaluate the effects of pre- and postoperative measurements of M1 sagittal alignment on clinical and functional outcomes, and whether these variations would lead to transfer metatarsalgia or not.
Methods: 29 patients (36 feet) with a mean follow-up of 20 months after LP were reviewed. Clinical and functional data were assessed with the VAS for pain, AOFAS, LEFS and SF-12. SF-12 comprises physical and mental health scales (PCS-12 and MCS-12, respectively). Transfer metatarsalgia diagnosis was based on the clinical exam. M1 sagittal alignment analysis was based on the first metatarsal declination angle (FMDA) and Meary Angle (MA). Decrease of FMDA means that the M1 dorsiflected (Figure 1). Intermetatarsal angle (IMA) and hallux valgus angle (HVA) were assessed. Radiographic, clinical and functional measurements were compared. Intraclass Correlation Coefficients (ICC) were calculated for FMDA and MA. Linear regression was used to assess the association of Δ-FMDA and Δ-MA with clinical and functional questionnaires. Based on that, we assessed our sample at different cut-off points to evaluate whether a given Δ-FMDA and/or Δ-MA measurement was significantly related to the Δ-Questionnaires.
Results: Pre- and postoperative ICC of FMDA was 0.90 and 0.91 and MA was 0.94 and 0.88, respectively. FMDA showed significant variation after the LP, but MA did not. IMA and HVA improved significantly. Significant clinical and functional improvement were observed, except in MCS-12. No patient developed transfer metatarsalgia. A direct correlation was found between ΔFMDA with Δ-PCS-12 and Δ-LEFS (p=.028 and p=.02, respectively), meaning that excessive dorsiflexion of M1 as measured by FMDA led to a decrease in PCS-12 and LEFS. We found that at the cut-off point of quartile 50%, in which our sample was divided equally, patients with Δ-FMDA below 3.2 degrees of dorsiflexion had significantly improved results on Δ-PCS-12 compared to those with greater values (p=.029) (Figure 2).
Conclusion: The present study showed that excessive dorsiflexion of M1 led to decreased outcome scores as measured by PCS- 12 and LEFS. It supports that M1 dorsiflexion should be avoided after the LP. However, slight dorsal deviation can occur and, even so, satisfactory outcomes can be obtained. Further prospective and comparative studies with larger populations are required to evaluate the effects of M1 inclination on clinical and functional outcomes.
DOI: 10.1177/2473011421S00376
Is First Metatarsal Shortening Correlated with Clinical and Functional Outcomes Following the Lapidus Procedure?
Danilo Ryuko Nishikawa, MD; Fernando A. Duarte, MD; Guilherme H. Saito, MD; Bruno R. Miranda, MD; Emanoel Jefferson A. Fenelon, MD; Marcelo P. Prado, MD, PhD
Introduction/Purpose: Lapidus procedure (LP) is a powerful technique to correct hallux valgus (HV) deformities, with good long-term outcomes. However, postoperative complications may arise, as undercorrection of the deformity, nonunion, elevation and shortening of the first metatarsal (M1). The objective of this study was to correlate M1 shortening with transfer metatarsalgia, and clinical and functional outcomes in patients who underwent the LP.
Methods: a retrospective review of 29 patients (36 feet) who were submitted to the LP for HV correction was performed. The average follow-up was 20 months. M1 length was analyzed using the Relative First Metatarsal Length (RML) measurement (Figure 1). When M1 shortens in relation to the second metatarsal, the RML measurements increase. The intermetatarsal angle (IMA) and hallux valgus angle (HVA) were also measured. Clinical and functional analyses were based on the VAS for pain, AOFAS, LEFS and SF-12 health survey. SF-12 is divided into physical and mental health composite scales (PCS-12 and MCS-12, respectively). Transfer metatarsalgia diagnosis was based on the clinical exam. Radiographic, clinical and functional measurements were compared using paired Wilcoxon signed-rank test and Student t test. Interobserver reliability of RML measurements was calculated using Intraclass Correlation Coefficients (ICC). A linear regression was performed to assess the correlation between RML and the clinical and functional questionnaires.
Results: There was a significant M1 shortening of 2.28mm after the LP (p<.001), with mean preoperative RML of 3.06 mm and mean postoperative of 5.34 mm (Table 1). No patient developed transfer metatarsalgia. Intraclass Coefficient Correlation (ICC) of the RML measures showed a excellent reliability of 0.94 and 0.98 in the pre- and postoperative setting, respectively. IMA and HVA presented significant improvements (p<.001) (Table 1). Clinical and functional improvements were observed in all questionnaires applied, except in the MCS-12 (Table 2). In the linear regression, RML was inversely correlated to LEFS (p=<.05), which means that LEFS scores increased as RML measurements decreased (Table 3). There was no significant correlation with the other questionnaires.
Conclusion: The present study demonstrated that M1 shortening led to a decreased LEFS following the LP. Comparative studies with prospective design and larger populations are required to assess the role of M1 shortening on clinical and functional outcomes.
DOI: 10.1177/2473011421S00377
Porous Titanium Wedges in Revision First Metatarsophalangeal Arthrodesis
David M. Noble; Benjamin Small; M. Truitt Cooper, MD; Joseph S. Park, MD; Venkat Perumal, MD
Category: Midfoot/Forefoot; Other
Keywords: 1st MTP Joint; Fusion; Arthrodesis
Introduction/Purpose: First metatarsophalangeal (MTP) arthrodesis is a common procedure for hallux MTP pathology. In the setting of prior procedures with resultant bone loss, porous titanium wedges provide an alternative to allograft or autograft. The purpose of this study was to report clinical and radiographic outcomes achieved with titanium wedges used in 1st MTP arthrodesis in a revision setting.
Methods: A retrospective analysis was performed in 10 patients (mean age 65.8) with prior 1st MTP procedures who underwent 1st MTP arthrodesis with use of porous titanium wedges from February 2014 to March 2020. Outcomes were assessed using both clinical (Visual Analogue Scale, Foot and Ankle Ability Measure, Mental Health Continuum Short Form, 36-Item Short Form Survey, need for revision) and radiographic parameters. Patients were followed from a minimum of 6 months up to 6 years (mean
31.4 months).
Results: Average Foot and Ankle Ability Measure (FAAM) score was 91.1 +/- 14.7 (75.1 +/- 5.3 FAAM Activities of Daily Living; 17.9 +/- 9.9 FAAM Sports). Average pain visual analogue scale was 1.9 +/- 1.7. Average Mental Health Continuum-short form score was 34.2 +/- 8.5. Postoperative computed tomography (CT) imaging demonstrated lack of osseous integration in two of six CT scans obtained. Four patients underwent subsequent revision procedures, 3 for hardware prominence and 1 for failure of fusion.
Conclusion: To our knowledge, these data represent the first reported clinical and radiographic outcomes in patients undergoing revision 1st MTP arthrodesis with use of porous titanium wedges. Further research should focus on comparative data with other commonly performed operative techniques.
DOI: 10.1177/2473011421S00378
Pre-Visit Patient Instructional Video for the Virtual Orthopedic Foot and Ankle Examination: Technique Tip
Naudereh B. Noori, MD; Bonnie Y. Chien, MD; Walter C. Hembree, MD; Zijun Zhang; Jason Schon; Lew C. Schon, MD
Keywords: Practice Models; Clinical Outcomes; Patient Education
Introduction/Purpose: The COVID-19 pandemic has brought a major increase in telemedicine utilization to conserve resources and maintain social distancing. The rapid transition over a short period of time has exposed challenges and limitations of virtual visits, especially with regards to performing an effective and efficient physical examination. Within months, orthopedic telemedicine guides were published for patient education and facilitating the musculoskeletal examination. These publications, however, included only a short video clip to explain to the patient how to participate in the examination during a telemedicine visit. In the foot and ankle subspecialty, the closely adjacent complex anatomy compared to other areas of the body presents unique challenges for physical exam.
Methods: To optimize the efficiency and efficacy of the examination portion of the visit for both patients and providers, we designed and recorded an instructional video that is sent to all patients by email a minimum of 1 week prior to their appointment. This video consists of a step-by-step guide on how to take suitable photos and videos of their feet and ankles for the physical examination portion of their visit. These media files are then directly uploaded by the patients into their EMR or emailed to the physician’s office to be uploaded for access by the provider before and during the virtual visit. Along with the video, patients are given a link to test their microphone and camera in advance of the visit to ensure adequate functionality and positioning.
Results: Our pre-appointment instructional video has been effective to methodically replicate the most important aspects of an in-person foot and ankle evaluation. Both physicians and patients appear to benefit from the tutorial video by having more time during the telemedicine visit to focus on history, assessment, and plan. Patients are more actively involved in the clinical data collection process because they are educated on what to expect and how to best prepare and participate in telemedicine visits. Moreover, having a set of systematic and detailed photos and recordings of the patient’s foot and ankle beforehand better focuses interaction and discussion with the patient during the telemedicine encounter. Additionally, these are saved into the patient’s electronic medical record, available for reference and later review.
Conclusion: Physical examination plays a critical role in diagnosis and treatment in the orthopedic foot and ankle subspecialty. More research is needed to discern how best to utilize virtual modalities as they become more commonplace, not just from the imposition from the COVID pandemic but also from the standpoint of patient convenience and time efficiency. Here we have described our creation of a pre-visit educational video to guide and engage patients on acquiring invaluable physical examination information for the orthopedic foot and ankle telemedicine encounter.
DOI: 10.1177/2473011421S00379
Ultrasound Stress-Imaging is a Promising Tool to Detect Achilles Tendon Damage
Kathryn O'Connor, MD; Elaine Schmidt; Todd J. Hullfish; Michael W. Hast; Josh R. Baxter
Introduction/Purpose: Achilles tendon disorders are among the most common conditions observed by sports medicine physicians and among the most difficult to diagnose using current clinical tools. While qualitative imaging is a validated method to grade the severity of tendinopathy, predicting the risk of these patients progressing or suffering tendon ruptures remains a major clinical need. Therefore, the purpose of this study was to determine the efficacy of quantitative ultrasound imaging to explain in vitro fatigue-induced degradation of Achilles tendon mechanical properties. We hypothesized that decreases in mean echogenicity would be linked to in vitro tendon fatigue characterized by decreased mechanical properties.
Methods: In this cadaveric tendon study, we cyclically fatigued 10 cadaveric Achilles tendons (7 donors; sex: 4M, 3F; age: 60+-15 years) and acquired b-mode ultrasound images to determine if stress-imaging biomarkers provide new insight into tendon status. We cut dog-bone shapes to concentrate tendon damage at the mid-substance where we acquired ultrasound images. In a custom- built testing bath, we cyclically applied 10-20 MPa of tendon stress at 1 Hz for 150,00 or until the specimen failed. Every 500th cycle, we applied 2 slow (0.25 Hz) tendon stresses of 10-20 MPa while acquiring ultrasound images using an 18MHz transducer. We calculated the change in tendon echogenicity caused by the applied stress to determine if this stress-imaging biomarker was associated with tendon failure. We compared these stress-imaging biomarkers from the tendons that failed (N=6) and the tendons that survived (N=4) cyclic fatigue damage using an unpaired t-test (p < 0.05).
Results: Quantitative analysis of the ultrasound images indicated 2 key differences between tendons that failed during the cyclic loading protocol and those that did not (Figure 1 shows representative data of tendons with similar demographics but one tendon exhibited increased change in echogenicity before failing while the other tendon exhibited smaller changes in echogenicity and did not rupture). First, mean echogenicity decreased before failure. Second, the average change in mean echogenicity was significantly greater in tendons that failed (p = 0.031). For most tendons that did fail, mean echogenicity decreased during the third phase of fatigue life. For the tendons that did not fail, mean echogenicity plateaued along with strain during the second phase of fatigue.
Conclusion: This study found detectable differences in image echogenicity during a stress test between tendons that fail during cyclic loading and those that do not. While preliminary, our findings indicate that B-mode ultrasound has potential as a clinically viable tool to predict severe tendon injuries. Our future work is focused on developing computer-based predictive tools to assess Achilles tendon fatigue in patients with tendinopathy following prolonged tendon loading to establish quantitative imaging thresholds that can serve as clinical benchmarks.
DOI: 10.1177/2473011421S00380
Comparison of Physical Function and Pain Levels of Hallux Rigidus Patients before and after Synthetic Cartilage Implant vs Arthrodesis Surgery
Irvin Oh, MD; Peter Joo, BS; Judith F. Baumhauer, MD, MS, MPH; Jeffrey Houck, PT, PhD; Jessica M. Kohring, MD; Adolph S. Flemister, MD; John P. Ketz, MD; Benedict F. DiGiovanni, MD
Category: Bunion; Midfoot/Forefoot
Keywords: Hallux Rigidus; PROMIS Physical Function; Synthetic Cartilage Bone Implant
Introduction/Purpose: Hallux rigidus is a common and painful degenerative condition of the great toe limiting a patient’s physical function and quality of life. The purpose of this study was to investigate pre- and postoperative physical function (PF) and pain interference (PI) levels of patients undergoing synthetic cartilage implant hemiarthroplasty (SCI) versus arthrodesis (AD) for treatment of hallux rigidus using the Patient Reported Outcome Measurement Information System (PROMIS).
Methods: Pre- and postoperative PROMIS PF and PI t-scores were analyzed for patients who underwent either SCI or AD. Postoperative final PROMIS t-scores were obtained via phone survey. Linear mixed model analysis was used to assess differences in PF and PI at each follow up point. Final follow-up scores were analyzed using independent sample t-tests.
Results: Total 181 (59 SCI, 122 AD) operatively managed patients were included for analysis of PROMIS scores. Final phone survey was performed at mean 33 (14-59) months postoperatively, with 101 patients (40 SCI, 61 AD) successfully contacted. Mean age of the SCI cohort was younger than the AD cohort (57.5 versus 61.5 years-old, p = 0.01). Average PF t-scores were higher in the SCI cohort compared to AD cohort at baseline (47.1 versus 43.9, respectively; p = 0.01) and at final follow up (51.4 versus 45.9, respectively; p < 0.01). A main effect of superior improvement in PF was detected in SCI group (+4.3) versus AD group (+2) across time intervals (p < 0.01). PI t-scores were similar between the two procedures across time points.
Conclusion: The SCI cohort reported superior PF t-scores at all follow-up time points compared to the arthrodesis group. No differences were found for PI or complication rates between the two treatment groups during this study timeframe.
DOI: 10.1177/2473011421S00381
Gender and Geographic Trends Amongst Foot & Ankle Surgeons: Where Are We and Where Do We Need to Improve?
Introduction/Purpose: Clinical and elective experiences as well as the guidance of mentors are all critical factors in the pursuance of orthopedic residencies and fellowships. Women have historically been underrepresented in orthopedics. Some propose that the root cause lies in the lack of availability in the aforementioned factors. Previous studies demonstrated geographic differences in sex representation in orthopedic residency programs. Studies over geographic distributions of orthopedic foot and ankle (OFA) surgeons showed high variation in geographic density of OFA surgeons throughout the U.S. This study seeks to determine both the gender and geographic distributions of OFA surgeons as well as to determine geographic patterns between their training locations and current practices.
Methods: AOFAS data regarding fellowship completion from 1988 through 2021 was analyzed with regards to gender and fellowship location. Internet searches were performed for all those identified within the database for their medical school, residency, and current practice location. This biographical data was obtained from their front-facing biographical webpage or hospital affiliation. States were placed into regions and subsequent divisions as defined according to the US Census Bureau definition: Northeast (New England and Middle Atlantic), Midwest (East North Central and West North Central), South (South Atlantic, East South Central, and West South Central) and West (Mountain and Pacific).
Results: 1,088 OFA surgeons were analyzed. 168 (15.3%) were female and 922 (84.7%) were male. Female-held OFA fellowship positions increased over time, currently sitting at 13 (22% of all fellowship positions), with a maximum of 15 (25%) in 2017. Geographically, the Pacific had most females (n=26, 15.6% of females), while East South Central had least (n=10, 6.0%). The South Atlantic had most males (n=193, 20.9% of males) while East South Central had least (n=59, 5.3%). The region with the most OFA surgeons in total was the South Atlantic (n=218, 20.0% of the total) whereas the regions with the least were East South Central and New England (n=59, 5.4% in each).
Conclusion: Although the amount of female OFA surgeons has increased, the numbers are still low. Geographically, the East South Central division of the U.S consistently had the least number of OFA surgeons whereas the South Atlantic division had the highest.
DOI: 10.1177/2473011421S00382
Functional Outcomes of Dorsal Bridge Plating for Lisfranc Injuries with Routine Metalwork Retention: A Major Trauma Centre Experience
Elliot I. Onochie; Nelson Bua; Amit Patel, FRCS(Orth); Shilpa Jha, MBBS, MRCS; Nima Heidari; Alexandros Vris; Lee Parker, FRCS(Tr&Orth); Francesc Malagelada Romans; Luckshmana A. Jeyaseelan
Introduction/Purpose: Lisfranc injuries represent a significant disruption to the complex articulations of the midfoot. Many of these injuries are unstable with displacement and articular incongruity. This necessitates surgical intervention with the primary goals of anatomic reduction and midfoot stability. Evidence around surgical treatments for Lisfranc complex injuries is limited by heterogeneity in outcome measures and small patient numbers. Dorsal bridge plating is a well-recognized surgical technique with the benefits of rigid stability and joint preservation. The primary aim of this study is to assess the midterm functional outcomes for patients treated with this technique at our major trauma centre. Additionally, we assess the complication profile and review for risk factors that influence the functional outcome.
Methods: Eighty-five adult patients were identified as undergoing open reduction and dorsal bridge plate fixation for displaced, unstable Lisfranc injuries at our major trauma centre between January 2014 and January 2018. Supplemental Kirschner wire stabilization was used for the lateral column if necessitated by the injury pattern. Importantly, metalwork was not routinely removed. A retrospective review of case notes and imaging was conducted in order to collate demographic data including co- morbidities and smoking status. Patient-reported outcome measures were collected at final follow-up, with a minimum follow-up of 24 months. The Manchester-Oxford Foot Questionnaire summary index (MOXFQ-Index) was the primary patient-reported outcome. The American Orthopaedic Foot & Ankle Society (AOFAS) midfoot scale, complications, and all-cause re-operation rates were secondary outcome measures. Univariate and multivariate analyses were used to identify risk factors associated with poorer functional outcomes.
Results: The mean follow-up in this study was 40.8 months (24 - 72). 61/85 patients (72%) had high-energy or crush mechanisms of injury. The mean MOXFQ-Index was 27.0 (SD 7.1). The mean AOFAS score was 72.6 (SD 11.6). 48/85 patients (56%) had injury patterns that included an intra-articular fracture and this was associated with poorer outcomes, with worse MOXFQ and AOFAS scores (both p<0.001). There were trends towards poorer outcomes in diabetic patients (p=0.07), those patients needing supplementary Lisfranc or intercuneiform screws (p= 0.39 and 0.45 respectively), and as a greater number of tarsometatarsal joints were stabilized (p=0.12). Overall, eighteen patients (21%) underwent removal of metalwork for either prominence or stiffness. Female patients were more likely to require metalwork removal (OR 3.89, 95% CI 1.27 to 12.0, p=0.02). Eight patients (9%) required secondary arthrodesis for post-traumatic osteoarthritis.
Conclusion: This is the largest series of Lisfranc injuries treated with dorsal bridge plate fixation reported to-date. Bridge plating is safe and effective in stabilizing this complex midfoot injury. The presence of an intraarticular fracture is a poor prognostic indicator. This is the first study to report on outcomes with routine retention of bridge plates. 21% of patients required removal of metalwork and this was more likely in female patients. Patient-reported outcomes and secondary arthrodesis rates were comparable to the existing literature in which bridge plates are routinely explanted. This suggests that routine removal may not be a necessity.
DOI: 10.1177/2473011421S00383
The Triplanar Hallux Abducto Valgus Classification System: Is it Valid?
Alexander G. Padovano; Trapper Lalli, MD; Joshua N. Tennant, MD, MPH; Kevin D. Martin, DO; Robert D. Santrock, MD
Introduction/Purpose: Historically, two-dimensional radiographic study techniques have been used to classify and describe hallux valgus deformities and guided treatment based on severity of deformity in the transverse plane only. These two-dimensional radiographic studies and were not able to assess rotational deformity and may explain the high recurrence and dissatisfaction rates which have been reported. Recently, a triplanar hallux abducto valgus classification (THAVC) system was proposed. This key elements of this classification system are the pathologic alignments in all three anatomic planes. The THAVC system is intended to clarify the deformity and apply a triplanar anatomic algorithm for treatment. To our knowledge, this classification system has not been validated. Our objective was to assess the intra-reader and inter-reader reliability of the THAVC.
Methods: After approval by the Institutional Review Board, patients with hallux abducto valgus (HAV) were identified from a foot and ankle registry. Electronic medical records and digital radiographs were reviewed by the principal investigator (PI). Selected radiographs were then deidentified of patient information and assembled in a digital slide presentation and presented to the reviewers. The eligibility criteria required complete weightbearing radiographic studies and represented varying degrees of HAV. The reviewers included three board certified, fellowship trained orthopaedic foot and ankle surgeons. Images of twenty cases of hallux valgus and five normal cases were distributed electronically, who independently classified all 25 cases according to the THAVC system for a total of 75 observations. After an eight week washout period, the order of the HAV cases was randomized and redistributed to the reviewers. The three reviewers were blinded to the results of the both radiographic reviews until after statistical analysis had occurred.
Results: We evaluated the intra-reader consistency by Cohen’s kappa for the agreement between two measurements from the same reader. The average kappa value from three readers was 0.241 with 95% CI (0.093-0.374), indicating a fair agreement. The inter-reader agreement was 0.046 with 95% CI (-0.041-0.112), showing poor agreement between readers.
Conclusion: The Triplanar HAV Classification is the first classification system that utilizes anatomic, multi-plane evaluation. Our results indicate while this is the first known HAV classification system, by this analysis it lacks reliability. This study shows that the reading of 2D radiographs still present a difficulty in assessing a 3D problem. Perhaps a scoring system utilizing advanced imaging such as 3D WBCT could prove more reliable and applicable.
DOI: 10.1177/2473011421S00384
Ankle Approach Selection: Defining Eight Ankle Approaches Exposure Segment and Area
Introduction/Purpose: Ankle and tibial plafond fractures are a frequent problems in everyday practice. To achieve the best possible outcome, proper soft tissue handling and joint surface restoration is mandatory, therefore, approach selection is of vital importance. Currently, there is no consensus nor evidence-based data regarding this critical planning step, and published guidelines are based on expert opinion. The aim of this study was to measure exposure segment and amount of area exposed by 8 different approaches and to provide objective data to be used as a tool in approach selection.
Methods: We performed a descriptive cadaveric study. We included the following approaches: anteromedial, anterolateral, direct lateral, posterolateral, posterior paramedian, posterior modified posteromedial, anterior modified posteromedial and direct medial approach. Each approach was performed four times. All incisions where standardized in length and centered 1cm proximal to the tibiotalar joint. After retracting flaps, we took one picture of each approach at a standardized distance, using a 1cm mark as a witness and calculated bone exposure area. On a second stage, all specimens where frozen and used to perform an axial cut 1cm proximal to the tibiotalar joint. A new picture was then obtained of each approach at a standardized distance. The amount of segment exposed by each approach was expressed in degrees, using two reference axes: the mediolateral malleolar axis and an anteroposterior axis at it center. 0° was stablished at the medial malleolus and 90° at the anterior edge.
Results: We obtained the following median exposed area for the studied approaches: anteromedial: 18,36cm2, anterolateral: 8,52cm2, direct lateral: 12,72cm2, posterolateral: 9,40cm2, posterior paramedian: 12,18cm2, posterior modified posteromedial: 10,42cm2, anterior modified posteromedial: 12,37cm2 and direct medial: 15,66cm2. The median exposed segment of each approach was: anteromedial: 4°-99°, anterolateral: 50°-170,5°, direct lateral: 137°-200°, posterolateral: 187°-258°, posterior paramedian: 202°-297°, posterior modified posteromedial: 215°-305°, anterior modified posteromedial: 242°-311° and direct medial: 21°- 309,5°. The biggest area of exposure was provided by the anteromedial approach (18,36cm2) and the greatest exposed segment was that of the anterolateral approach (120°). On the other hand, the smallest exposed bone area was that of the anterolateral approach and the smallest segment with the direct lateral approach (63°). A comparative view of the exposed segments is showed in Figure 1.
Conclusion: When comparing results focused on posteromedial approaches, the posterior paramedian approach is the one that best combines exposure area and segment. Posterior paramedian approach also allows good access to the posterolateral tibial surface. Based on our results, we propose combining posterior paramedian and posterior modified posteromedial approach, using a single incision and the FHL tendon as a mobile window to manage complex posterior tibial fractures with posteromedial and posterolateral extension. We believe that by defining area and segment exposed by different ankle approaches we provide surgeon with objective data that could help in approach or approaches selection.
DOI: 10.1177/2473011421S00385
Medial Approaches to the Posterior Malleolus: A Comparative Cadaveric Study
Joaquin Palma, MD; Tomas Urrutia; Sergio Morales
Category: Ankle; Trauma
Keywords: Structural Anatomy and Biomechanics; Posterior Malleolus Fracture; Ankle Fracture
Introduction/Purpose: Ankle fractures are the most common fractures of the lower extremity. In spite of that, there is still no consensus regarding the best way to approach posterior malleolus (PM) fractures. The aim of this study is to compare the degree of PM exposure, tension of the flap containing the medial neurovascular bundle (NVB) and distance between the surgical incision and the NVB using three different posteromedial ankle approaches.
Methods: Three different posteromedial approaches were compared: direct medial (DM) modified posteromedial (MPM) and posterior paramedian (PPM). Each approach was performed four times using a standardized technique. With a digital tensiometer, the minimal tension of the flap containing the NVB that allowed proper exposure of the PM was measured. In a second stage, an axial cut 1cm proximal to the tibiotalar joint was performed in nine frozen pieces and PM exposure degree and distance between the incision and the NVB was measured.
Results: The median minimal tension was DM: 14,78 N, MPM: 8N and PPM: 5,75N. The median distance between the incision and the NVB was DM: 17mm, MPM: 6mm and PPM: 28mm. The median degree of exposure was DM: 51%, MPM: 58% and PPM: 72%.
Conclusion: The PPM approach achieved the highest degree of PM exposure, with the lowest tension applied to the NVB and allowing the greatest distance between the incision and the NBV. Thus, we believe it should be considered the approach of choice for large fractures compromising the posteromedial and posterolateral aspect of the PM.
DOI: 10.1177/2473011421S00386
Are Outcomes Following Crossed Lag-Screw Modified Lapidus Technique for Hallux Abductovalgus Comparable to Plate-Screw Fixation Technique? A Study of Costs, Radiographic and Patient Reported Outcomes
Chinmay S. Paranjape, MD; Trapper Lalli, MD; Joshua N. Tennant, MD, MPH
Introduction/Purpose: The modified Lapidus (ML) for tri-planar HAV correction is a powerful procedure for correcting hallux valgus (HV) and metatarsal rotation. We assessed implant costs, radiographs, and pre and postoperative patient reported outcome measures of Patient Reported Outcome Information System Physical Function (PROMIS-PF) Computerized Adaptive Test scores (CAT) at an average of 20.2 months followup.
Methods: We examined patients retrospectively from January 2014 to December 2019. Pre and postoperative PROMIS-PF, radiographic parameters (intermetatarsal angle, IMA and HV angle, HVA), complications, and total surgical time were reviewed from the medical chart. Estimated surgical implants costs were obtained from manufacturers.
Results: 83 patients underwent lag screw lapidus. All had radiographs, 71 had complete PROMIS-PF. Patients were a median age 55.80 (45.55, 53.85), 6.7% male, and 20% diabetic (median A1c 6.4%). Complications included 6.7% delayed wound healing, 13.3% painful hardware, 13.3% superficial infections. Others (7/83 or 8.4%) included complex regional pain syndrome in one, overcorrection in two, paresthesia in one and symptomatic nonunion in three. Preoperative angles were hallux valgus angle 33 (30, 40), IMA 15 (12, 16) which improved at final postoperative follow up to HVA 9 (5, 15) and IMA 7 (6, 9). PROMIS-PF was 43 (37,52) preoperatively, 37 (31, 39) at six weeks, 46 (42, 51) at three months, and 49 (41, 53) at > 360 days. The drop in PROMIS- PF between preop and 6 weeks and the rise from 6 weeks to 3 months were significant. There was no difference between pre and postoperative PROMIS-PF. Implants averaged $140 USD.
Conclusion: Patients achieved good radiographic correction of HV following ML by our technique. While physical function, measured by the PROMIS-PF, decreased in the acute postoperative period, it increased to near final levels by three months postoperatively. Low complication rate, low cost, and high patient postoperative functional expectations with excellent radiographic correction were demonstrated.
DOI: 10.1177/2473011421S00387
Red Blood Cell Distribution Width: A Novel Predictor of Mortality Following Amputation in Diabetic Foot
Jae Han Park, MD; Kwang Hwan Park, MD, PhD; Yeo Kwon Yoon, MD; Seung Hwan Han, MD, PhD; Jin Woo Lee, MD, PhD
Introduction/Purpose: Red blood cell distribution width (RDW), reflects the degree of heterogeneity of erythrocyte volume, has been found to be a significant prognostic factor in various human disorders. Herein, we assessed the value of RDW as a prognostic factor in diabetic foot amputation.
Methods: Data of 415 patients with diabetic foot underwent amputation between January 2009 and January 2019 were analyzed retrospectively. After establishing a cut-off point of preoperative RDW for all-cause mortality, Cox proportional hazard model for mortality and logistic regression analysis for length of hospital stay more than 1 month were performed with other variable
Results: RDW >14.5% was a significant risk factor for mortality (hazard ratio, 2.55; 95% confidence interval [CI], 1.55 to 4.19) on multivariable-adjusted regression analysis. Other significant factors associated with mortality were age and kidney disease. High RDW was also associated with longer hospitalization over 30 days (odds ratio, 2.17; 95% CI, 1.29 -3.66).
Conclusion: High preoperative RDW over 14.5% is an independent prognostic factor with increased mortality and longer hospitalization, implying that RDW may be a simple and inexpensive laboratory parameter for risk stratification in diabetic foot amputation.
DOI: 10.1177/2473011421S00388
The Course of Tarsal Tunnel Syndrome after Ultrasound-Guided Injections
Joseph S. Park, MD; Kivanc Atesok, MD, MSc; Jennifer Pierce, MD; Benjamin Small; Venkat Perumal, MD; M. Truitt Cooper, MD
Introduction/Purpose: Local ultrasound (US)-guided injections of anesthetics with corticosteroids are commonly performed for the conservative treatment of tarsal tunnel syndrome (TTS). This retrospective study aimed to investigate the course of TTS after US-guided injections.
Methods: The study included patients who were diagnosed with TTS and received US-guided injections as their initial conservative treatment. The patients' pain levels were noted on a scale between zero and ten before and after each injection. The patients were divided into two groups: nonsurgical and surgical groups. The nonsurgical group included patients who had received US-guided injections and were not treated surgically, and the surgical group included those who received US-guided injections and ultimately underwent surgical tarsal tunnel release (TTR). The two groups were compared in terms of age, gender, post-injection follow-up time, and the amount of pain reduction immediately after injection (ΔPN). In the surgical group, the presence or absence of additional foot and ankle pathologies requiring operative treatment during TTR, and outcomes of surgical treatment were also assessed.
Results: 218 patients were diagnosed with TTS and received US-guided injections as their initial treatment. After the injections, 169 patients (77.5%) required no TTR (nonsurgical group) and 49 patients (22.5%) underwent TTR (surgical group). The average ages for the nonsurgical and surgical groups were 53.8 and 48.9 years (P = 0.03). The average time between the injection and final follow-up for the nonsurgical group was 339 days. The average time between the injection and TTR for the surgical group was 145 days. There were no differences in pain relief after the injections between the nonsurgical and surgical groups (mean ΔPN: 3.6 and 3.8, respectively). In the surgical group, 16 patients (32%) presented with additional foot and ankle pathologies that were surgically treated during TTR. The average post-surgical follow up time was 117 days. At final follow up, 41 patients (84%) in the surgical group had no pain or functional impairment.
Conclusion: US-guided injection can be an effective conservative treatment option for patients with TTS. Surgical release of tarsal tunnel may improve and resolve the overall symtoms of TTS in majority of the patients who do not respond to nonsurgical treatment. Younger age and additional foot and ankle pathologies appear to be associated with greater likelihood of undergoing TTR.
DOI: 10.1177/2473011421S00389
Comparison of Medial and Dorsal Approach for Talonavicular Fusion: A Cadaver Study
David A. Patch, MD; Nicholas A. Andrews; Timothy. Torrez; Charles R. Sutherland; Whitt Harrelson; Abhinav Agarwal, MBBS; Ashish Shah, MD
Category: Basic Sciences/Biologics; Hindfoot; Other
Keywords: Arthrodesis; Degenerative - Wear and Tear; Midfoot
Introduction/Purpose: Talonavicular (TN) joint arthrodesis is a common procedure for end stage arthritis. There are two common operative approaches used to expose the TN joint for articular preparation, the medial and dorsal. Classically, the medial approach has been the preferred method of TN joint fusion, but recent arguments have been made for the use of the dorsal approach. Articular surface preparation is a key tenant required for any joint fusion. To date no physical preparation studies have been done to compare the two approaches in terms of articular surface preparation.
Methods: Ten fresh frozen cadaver specimens were obtained. Fluoroscopic radiographs were used to rule out any pre-existing pathology of the talonavicular joint. Specimens were assigned to receive either a dorsal or medial operative approach to the talonavicular joint. After joint preparation, the talonavicular joint was disarticulated and the amount of articular surface preparation was recorded using ImageJ software.
Results: A total of 8 male and 2 female specimens were utilized with an average age of 64.5 +- 13.1. The dorsal approach had a higher average percentage of talar, navicular, and total talonavicular joint surface prepared. When examining joint surface area preparation regardless of approach used, the talar head was significantly less prepared than the navicular. The inter-observer correlation coefficient was excellent for both navicular and talar surface area prepared.
Conclusion: The amount of articular surface preparation in the dorsal approach was consistently higher on average. Given the high rate of nonunion in isolated talonavicular and triple arthrodesis, surgeons should be aware that the dorsal approach may offer an increased amount of articular surface preparation. Our study adds to the growing body of evidence supporting the investigation and use of the dorsal approach when attempting talonavicular arthrodesis.
DOI: 10.1177/2473011421S00390
Treatment of Complex Hindfoot Trauma with Hindfoot Nail
David A. Patch, MD; Megan Lameka; Jared R. Halstrom, BS; Jonathan H. Quade, MD; Clay A. Spitler, MD; Michael D. Johnson, MD
Category: Hindfoot; Trauma
Keywords: Arthrodesis; Pilon Fracture; Trauma
Introduction/Purpose: Pilon fractures are often associated with severe bone comminution and soft tissue compromise. As a result, surgical salvage procedures such as hindfoot nailing may be indicated for patients who are not candidates for standard fixation techniques such as open reduction and internal fixation (ORIF). The purpose of this review was to access outcomes associated with complex hindfoot trauma acutely treated with hindfoot nailing.
Methods: A case series at a Level I trauma center was performed to identify trauma patients with complex hindfoot fractures who underwent hindfoot nailing as definitive treatment after initial external fixation between 2012 and 2020. Indications included a combination of patient comorbidities, fracture severity, and soft tissue injury. Exclusion criteria included follow-up less than 3 months. Post-operative radiographs were interpreted by a fellowship-trained foot and ankle surgeon. Primary outcome measures included unplanned reoperation/revision and deep infection. Deep infection was defined as any patient requiring surgical debridement after definitive fixation with positive cultures or the presence of positive cultures at the time of planned surgery. Fractures were classified using the AO/OTA classification and injury characteristics and postoperative complications were recorded via chart review.
Results: Twenty-six of 29 of identified patients met inclusion criteria. The most common AO/OTA classification was 43C (62%). The average age was 55 years (range, 31-94) and the most common mechanism of injury was motor vehicle crash (38%). Thirteen fractures (50%) were open with Gustilo Anderson grade IIIA fractures being the most common (38%). The overall deep infection rate was 15% with fifty percent of cases positive for a history of diabetes mellitus or smoking. Unplanned reoperations occurred in seven (27%) cases. Among these, a total of four (57%) occurred due to the development of deep infection, two (29%) were nonunions, and one (14%) was indicated for hardware failure. Below the knee amputation occurred in one patient with nonunion (4%), which was a grade IIIA open pilon fracture with significant bone loss. Union was achieved in the majority of patients (92%).
Conclusion: Treatment of complex hindfoot trauma with intramedullary nailing has a high union rate as a salvage procedure in a poor host. Surgeons should consider this treatment in patients that are not candidates for standard open reduction and internal fixation techniques.
DOI: 10.1177/2473011421S00391
Union Rates of Talar Neck Fractures with Critical Bone Defects Treated with Autograft
David A. Patch, MD; James T. McMurtrie, MD; Mason Frazier; Bradley Wills; John C. Prather, MD; Gean C. Viner; Margie J. Hill; Michael D. Johnson, MD
Introduction/Purpose: The purpose of this study was to evaluate union of talar neck fractures with critical bone defects treated acutely with autologous tibial bone graft during primary osteosynthesis. We hypothesized that acute autografting leads to reliable union rates.
Methods: A case series at a Level I trauma center was performed to identify patients who underwent open reduction and internal fixation of talar neck fracture with proximal tibial autograft between 2015 and 2018. Inclusion criteria were age greater than 18 years and displaced talar neck fracture with critical bone defect treated with tibial autograft. Critical bone defect was defined as a gap greater than 5mm in the sagittal plane and greater than 1/3 of the width of the talar neck in the coronal plane. Post-operative foot CT scans were obtained for all patients to assess for union. Primary outcome was union and secondary outcomes were malunion, avascular necrosis, post-traumatic arthritis, and patient-reported outcomes (PRO) including PROMIS (Patient Reported Outcomes Measurement Information System), Foot and Ankle Measurements: Activity of Daily Living and Sports (FAAM ADL/Sports), Visual Analogue Scale for feet (VAS), Foot Function Index (FFI), and Short Form-36 (SF-36).
Results: Twelve patients were included in the series. The average age was 34 years (17-59). The Hawkins classification of the fractures were four type II (33%) and eight type III (67%). Five fractures (42%) were extruded tali. Four fractures (33%) were open fractures, all being type III fractures. Union was achieved in eleven patients (92%). Nonunion occurred in one patient (8%), who had an open, extruded talus fracture and was a heavy smoker. Avascular necrosis occurred in 11 patients (92%). Ten patients (83%) had radiographic tibiotalar post-traumatic arthritis (PTA), and 12 patients (100%) developed subtalar PTA. Average PROMIS score was 37 (32-45) and average FAAM ADL and Sports was 61 (31-87) and 31 (0-71), respectively. Average VAS was 5 (0-10) and average FFI was 49 (7-89). SF-36 scores showed fair to poor outcomes in the majority of patients.
Conclusion: Tibial autograft in primary osteosynthesis of comminuted talar neck fractures with critical bone defects leads to reliable union rates and is an operative strategy that should be considered when treating these difficult fractures. Despite high union rates, secondary outcomes of AVN, PTA, and below-average PRO still occurred in the majority of patients.
DOI: 10.1177/2473011421S00392
Research During Foot and Ankle Orthopaedic Fellowship and Association with Careers Following Fellowship
Tamanna Patel, BA; Benjamin R. Williams, MD; Scott J. Ellis, MD
Category: Other
Keywords: Patient Education; General Principles / Context; Practice Models
Introduction/Purpose: Performing research during fellowship continues to develop vital critical thinking skills for orthopaedic surgeons as they move into their careers. As fellowships and academic careers become more competitive, research plays an important role in fellow selection and future academic appointments. The purpose of this study was to assess if research during fellowship, measured through journal publications, was associated with careers in academic medicine and if those who published early in their training continued to do so into their careers.
Methods: A list of foot and ankle fellows, from 2008-2013, were collected from the AOFAS website. In February 2021, all collected fellows were searched on pubmed.gov to generate all orthopaedic publications with a PubMed identifier published before residency, during residency, during fellowship and after fellowship. Each publication’s 2020 Thomson Reuters 5-Year Journal Impact Factor and fellows first authorship were noted. The collected fellows were searched through Doximity.com for the name of their medical school, residency and fellowship. The fellows were further searched for their current location of employment and whether it was academic or not. An employment location was considered academic if they were listed on a department website that also was involved in teaching residents. The number of publications, journal Impact Factor and number of first authorships were compared between the academic and non-academic groups during their time before residency, during residency, during fellowship and after fellowship.
Results: A total of 246 fellows were included, with a mean (+- SD) of 0.8 +- 1.4 publications per fellow during fellowship. During the years in review, 27% (67/246) of fellows entered a career in academics. Before residency, there was no difference in the number of publications between those that went into academic and those that did not [academics 0.54 +- 1.85, non-academic 0.27 +- 1.05 (p=0.154)]. During residency and fellowship, those that went into academics were statistically significantly more likely to publish than those that did not go into academics [during residency: academic 2.82 +- 4.53, non-academic 1.24 +- 2.00 (p=0.0002); during fellowship: academic 1.10 +- 1.57, non-academic 0.69 +- 1.34 (p=0.038)] as well as more first authorships and in journals with higher impact factors.
Conclusion: As fellowships and academic positions become more competitive, the quality and number of journal publications are likely to become increasingly more important. This study noted that an interest in academics likely develops during orthopaedic residency. This study may help improve mentorship earlier on to those who are more likely to pursue a career in academics.
DOI: 10.1177/2473011421S00393
Early Failure of Paragon28 Phantom Hindfoot Fusion Nail: A Case Report
Naveen Pattisapu, MD; Clayton C. Bettin, MD; Elizabeth Friedmann, MD; Michael L. Sims, MD
Introduction/Purpose: Tibio-talar-calcaneal (TTC) fusion nails are commonly used to treated acute ankle fractures in patients with diabetes, Charcot arthropathy or other comorbidities. Recently, Paragon28 released the Phantom Hindfoot Fusion Nail (Phantom nail) with a unique design feature-a proximal coil.
Methods: We present the case of a diabetic patient with an ankle fracture-dislocation treated with the Paragon28 nail who experienced early implant failure.
Results: A 48-year-old male with HIV, end-stage renal disease requiring hemodialysis, and insulin-dependent diabetes mellitus with severe peripheral neuropathy presented a trimalleolar ankle fracture-dislocation treated with a TTC nail. At his first follow- up, he presented with early implant failure at the nail-coil interface.
Conclusion: The integrity of the Phantom nail, appropriate length, and placement of the flex coil require further evaluation. Unstable pathologies such as fractures may be better stabilized with a solid nail construct.
DOI: 10.1177/2473011421S00394
Reconstructive Surgical Management of Charcot Neuropathy of the Foot and Ankle: A Retrospective Study
Naveen Pattisapu, MD; Clayton C. Bettin, MD; Jane C. Yeoh, MD; Shumaila Sarfani, MD
Introduction/Purpose: Treatment of Charcot neuropathy (CN) of the foot and ankle remains a challenge for both patient and surgeon. Non-operative treatment with immobilization in a cast/orthosis has long been the mainstay of treatment, but more recently surgical intervention-with attention to internal fixation-has gained interest because of the poor long-term outcomes with non-operative care.
Methods: To assess long-term outcomes between CN patients managed with reconstructive surgeries at a tertiary referral center; a retrospective chart review analyzed comorbidities, demographics, and complications (ulceration, infection, and below the knee amputation).
Results: Over the last 16 years, 31 patients with CN were treated with internal fixation (midfoot fusion, open reduction, or hindfoot fusion nail). Average BMI was 33.5, average number of comorbidities was 2.93, and the percentage of patients with a vascular deficit was 19.3%. The rate of infection and ulceration prior to surgery was 19.4% (6/31 patients) and 45.2% (14/31 patients) respectively. After surgery, the rate of new infections was 38.7% (12/31 patients). The rate of new ulcerations was 41.9% (13/31 patients). The rates of below the knee amputation was 19.4% (6/31 patients).
Conclusion: A 16-year retrospective review of operative management of Charcot neuropathy in 31 patients at a tertiary referral center found high rates of ulceration, infection, and amputation in patients treated with internal fixation. This study could prove valuable in counseling CN patients regarding reconstructive surgery.
DOI: 10.1177/2473011421S00395
Fusion Rates Following First Metatarsophalangeal Arthrodesis using a Dynamic Nitinol Staple-Plate Construct, Minimum 1-Year Follow-Up
Terrence M. Philbin, DO; Antonio M. Malloy McCoy; Amar Chandra; Devon Consul, DPM; Mitchell Thompson; Kevin N. Nguyen
Category: Midfoot/Forefoot
Keywords: First MTP Arthrodesis; Arthrodesis; Staples
Introduction/Purpose: Arthrodesis has long been the procedure of choice for end-stage arthritis of the first metatarsophalangeal joint (MTP). Multiple constructs have been described through literature with good fusion rates and patient outcomes. Methods allowing for ease of application and reduction of OR time without sacrificing surgical outcomes and fusion rates are therefore of considerable interest.
Methods: In this study, we retrospectively reviewed a cohort of 33 patients undergoing arthrodesis of the first MTP utilizing a dynamic Nitinol staple and plate construct. The primary focus of our study was to evaluate the fusion rates following the aforementioned procedure. All patients within the study received a compression staple-plate construct placed across the first MTP and underwent the same post-operative protocol with radiographs taken at set intervals to evaluate fusion across the joint.
Results: Our results demonstrated a 100% fusion rate with 3 delayed unions and no incidences of hardware failure. The time to fusion and fusion rates seen in this study are comparable to those previously reported in literature.
Conclusion: We conclude that utilization of this construct is a viable option for arthrodesis of the first MTP, and its ease of application may decrease overall operating time which could prove advantageous over other, more commonly used methods.
DOI: 10.1177/2473011421S00396
Delayed Surgery for Ankle Fractures is Associated with Poor Patient Reported Outcome
Kristian Pilskog, MD; Eivind Inderhaug; Heid Elin J. Odland, MD; Teresa B. Gote; Knut Fjeldsgaard; Håvard Dale; Jonas M. Fevang
Introduction/Purpose: Several studies discuss the relation between prolonged time to surgery and postoperative complications in ankle fractures, but little is known about how a longer wait affects clinical outcomes. The present study, therefore, aims to assess the association between time from injury to surgery and patient-reported outcomes after operative treatment of severe ankle fractures.
Methods: Patients treated operatively for low-energy ankle fractures which also involve the posterior malleolus from 2014 to 2016 were included. Patient charts were reviewed for patient demographics, type of trauma, fracture characteristics, treatment given, and complications. Ankle function was evaluated on a follow-up visit by clinical examination, radiographs and patient- reported outcome measures (SEFAS, RAND-36, VAS of Pain, VAS of Satisfaction). For analyses, patients were stratified based on time from injury to definitive surgery; Group 1: within the same day, Group 2: 1 to 7 days after injury, and Group 3: later than 7 days after injury.
Results: Follow-up visits of 130 patients were performed at median 25 (Interquartile range (IQR), 19-34) months after surgery. Patient demographics and fracture characteristics were similar between groups. Median SEFAS was 40 in Group 1 (IQR 33-43), 41 (IQR 33-44) in Group 2, and 33 (IQR 27-42) in Group 3. The difference between Group 1 and 3 (p =.03), and between Group 2 and 3 (p =.04) was statistically significant. Group 1 had the highest rate of mechanical irritation and secondary surgery following malreduced fractures or missing syndesmotic fixation. Patients operated later than seven days from injury reported more pain than those treated earlier (p =.03).
Conclusion: Time from injury to final surgery influenced clinical outcomes after these severe ankle fractures. Patients who waited more than seven days until definitive surgery had poorer clinical outcomes and more pain compared to those who had surgery within a week.
DOI: 10.1177/2473011421S00397
Association of Length of Stay and COVID-19 in Rotational Ankle Fracture Surgery in the National COVID Cohort Collaborative (N3C)
Charles C. Pitts, MD; Eli Levitt, MS; David A. Patch, MD; Alfredo Terrero, MD; Reed Butler, MD; Brent A. Ponce; Steven M. Theiss, MD; Clay A. Spitler, MD; Michael D. Johnson, MD
Category: Ankle; Trauma
Keywords: Ankle; Fractures; Outcomes Measures
Introduction/Purpose: Coronavirus (COVID-19) is an emerging, rapidly evolving situation. The National COVID Cohort Collaborative (N3C) is an innovative approach to integrate real-world clinical observations into a harmonized database. To investigate the outcomes of adults with ankle fracture surgery during the (COVID-19) pandemic, we had the following research question: What are the outcomes of ankle fracture patients with COVID-19 (invasive ventilation, length of stay, death)? The purpose of this abstract is to introduce the largest cohort of ankle fracture patients to date with a comparison between lab- confirmed COVID-19-positive and COVID-19-negative.
Methods: A retrospective cohort of adults with ankle fracture surgery in the N3C Data Enclave. The N3C Data Enclave is an NIH-funded, secure platform through which the harmonized clinical data from electronic health records is stored (https://covid.cd2h.org/). COVID-19 status was determined using a set of 55 SARS-CoV-2 polymerase chain reaction and antigen lab tests. Ankle fracture surgery was defined using SNOMED codes for 'fracture of bone' and one of the following CPT codes '27766, 27769, 27792, 27814, 27822, 27823, 27829' for 'ankle fracture surgery.'
Results: A total population of 3.4 million patient records was queried in the National COVID Cohort, identifying 2,032 participants with ankle fracture surgery. The age range of the overall group was 18-98 years. Comparing COVID-19-positive to COVID-19-negative, the age (48.9 years vs 47.7 years) and gender (66.7% female vs 55.1% female) distribution of each group were comparable (both p>0.05). COVID-19-positive comprised 2.4% of the group (n=48). The length of stay was 4.7 days longer in the COVID-19-positive group (8.7 days vs 4.0 days, p<0.001). Higher proportions of COVID-19-positive patients who required invasive ventilation (12.5% vs 3.2%, p<0.002). The number of outcomes for mortality was too few to report.
Conclusion: Based on the initial results, rotational ankle fractures requiring surgery necessitated longer hospitalizations in COVID-19-positive patients during the COVID-19 pandemic than in patients without the virus. The average increased length in hospitalization was, on average, about 6 days. When treated in isolation, ankle fractures can often be treated on an outpatient basis, and a multiple-day increase in average hospital stay is substantial. Though the overall complication profiles (with the exception of pulmonary disease) were similar, lengthy hospital stays could lead to delays in the recovery and rehabilitative process, and functional outcomes could not be determined in our study.
DOI: 10.1177/2473011421S00398
Diabetic Kidney Disease is Associated with Increased Complications Following Operative Management of Ankle Fractures
William S. Polachek; Hayden P. Baker; James S. Dahm, MD; Jason Strelzow; Kelly K. Hynes, MD
Category: Trauma; Ankle; Diabetes
Keywords: Ankle Fracture; Diabetes; Complications
Introduction/Purpose: Diabetes mellitus and peripheral neuropathy are established risk factors for complications in operatively treated ankle fractures. Generally, the presence of peripheral neuropathy and diabetic nephropathy have been used as dependent variables in studies of diabetic ankle fracture cohorts, but these factors are typically treated as binary risk factors. Thus, we sought to quantify additional risk factors for complication specific to diabetic patients undergoing fracture fixation.
Methods: We identified 617 rotational ankle fractures treated operatively at a single academic medical center from 2010-2019, of which 160 were identified as diabetic. Of these, 91 ankle fractures in 90 diabetic patients met criteria for retrospective review of clinical and radiographic data. Criteria included perioperative laboratory studies, including Hemoglobin A1c and estimated glomerular filtration rate (eGFR), as well as follow-up radiographs in the electronic record. We defined complications in this surgical cohort as deep surgical site infection, unplanned return to the OR and failure of fixation. Logistic regression was performed, and odds ratios (OR) calculated.
Results: The overall the complication rate was 24.2% (22/91) in this cohort. Median follow-up was 29 weeks (range: 5-520 weeks). Mean perioperative Hemoglobin A1c in patients who experienced postoperative complications was 7.6% (Range: 5.1%- 14.2%) compared to 7.8% (Range:5.6%-13.5%) who did not (p=0.69). Diabetic patients with chronic kidney disease (eGFR<60 ml/min/BSA) (OR=5.29, p=0.006) and peripheral neuropathy (OR=4.61, p=0.003) were at significantly higher risk of all complications compared to diabetic patients without these comorbidities. Of note, we did not find an association between perioperative Hemoglobin A1c or Body Mass Index and complication rate.
Conclusion: Patients with diabetes complicated by chronic kidney disease are at significantly higher risk of complications following operative management of ankle fractures. Our study also corroborated previous reports that within this high-risk cohort, the presence of peripheral neuropathy is a significant risk factor for complications. These sequalae of diabetic disease extends beyond simple glycemic and are manifestations of microvascular disease, glycosylation of soft tissues and impaired metabolic pathways. Identifying these risk factors in diabetic patients allows for patient specific risk stratification, education, and management decisions of ankle fractures.
DOI: 10.1177/2473011421S00399
Preoperative Opioid Prescription is a Risk Factor for Extended Opioid Filling After Ankle Arthroscopy
William S. Polachek; Cody Lee; Bryan L. Scott; Kelly K. Hynes, MD
Introduction/Purpose: Opioids can be an important tool in the management of postoperative pain, however, increased prescribing of these medications following orthopaedic procedures has significantly contributed to the current opioid crisis. Post- operative opioid utilization and duration varies greatly among surgeons, procedures, and patients. We sought to investigate patterns of opioid prescription following ankle arthroscopy and determine patient factors associated with increased postoperative opioid prescribing.
Methods: A national claims-based database was queried for patients undergoing first-time ankle arthroscopy. Only patients with continuous database inclusion for at least one year prior to and one year after index ankle arthroscopy were included. Patients carrying an International Classification of Diseases (ICD)-9 or ICD-10 code(s) for diagnosis of septic ankle joint or a CPT code for total ankle arthroplasty prior to index ankle arthroscopy were excluded from the study. Patients who filled at least 1 opioid prescription between 1 and 4 months prior to surgery were defined as preoperative opioid-use group. Monthly relative risk ratios for filling an opioid prescription were calculated for the first year after surgery. Multiple logistic regression analysis was performed to identify factors associated with opioid prescription refills at 3, 6, 9, and 12 months after ankle arthroscopy. For analysis, P<0.05 was defined as significant.
Results: We identified 6,039 patients who underwent primary ankle arthroscopy. The preoperative opioid-use group consisted of 1,514 patients (25.1%), of which 24 (1.6%) filled opioid prescriptions at 6 months postoperatively compared to 39 (0.9%) of opioid-naive patients (relative risk [RR], 1.84 95% confidence interval [CI], 1.11-3.05). Multivariate analysis determined that the preoperative opioid-use group was at increased risk of filling prescriptions at 3 (odds ratio [OR], 2.22; 95% CI 1.42-3.48) and 6 months (OR, 1.74; 95% CI, 1.01-2.95) postoperatively. Patients with Body Mass Index (BMI) > 30 were also at increased risk at 3 months (OR, 1.65; 95% CI, 1.04-2.62) and 6 months (OR, 2.01; 95% CI, 1.17-3.49) postoperatively. Comorbidities such as diabetes, hypertension, fibromyalgia, alcohol, and tobacco abuse were not associated with opioid filling (P>0.05).
Conclusion: Preoperative opioid prescription filling and BMI 30 were associated with an increased risk of extended opioid prescription utilization following ankle arthroscopy. Overall, prolonged opioid prescribing was not widespread in either group postoperatively. This may represent the indications and outcomes of ankle arthroscopy. Patients presenting with preoperative opioid-use and increased BMI may benefit from multimodal pain management and additional perioperative education around non- pharmacologic pain-management strategies to decrease risk of prolonged opioid use.
DOI: 10.1177/2473011421S00400
The STAMP Test: A Novel Clinical Test in Diagnosing Achilles Tendon Ruptures
Giselle M. Porter; Edward T. Haupt, MD; Jonathan R. Kaplan, MD; Timothy P. Charlton, MD
Introduction/Purpose: Achilles tendon ruptures are common injuries, and an estimated 20-25% injuries are missed acutely. Chronic and acute Achilles tendon rupture patients typically present with nonspecific complaints and physical exam findings. Commonly used physical exam maneuvers such as the Thompson test have variable sensitivity and reliability for the examiner. The patient with an Achilles tendon rupture will have expected plantar-flexion weakness, however clinical data utilizing plantarflexion weakness to develop a physical exam maneuver is lacking. We propose two new tests with sensitivity and specificity analysis to evaluate this understanding in the clinical setting: the Stand and Maintain Plantarflexion (STAMP) and Tendo-Achilles Rise (TAR) tests. We hypothesize that the STAMP and TAR exams maneuvers will have high sensitivity for diagnosis of acute and chronic Achilles tendon rupture.
Methods: Data was collected from a single surgeon’s practice at two large urban treatment centers. Data was retrospectively acquired over a period of 7 years and then prospectively acquired over a period of 5 years. Patients with mid-substance Achilles tendon rupture confirmed with MRI imaging or operative treatment were included. We examined clinical data regarding ambulation, resting tension, palpable Achilles gap, Thompson test, and STAMP and TAR tests on initial presentation. The STAMP test is performed by the patient attempting a wall assisted double leg heel rise and lifting the uninjured foot off the ground. It is consistent with an Achilles tendon rupture if the patient is unable to maintain this position for five seconds. The TAR test is performed by the patient attempting a wall assisted single leg heel rise. It is consistent with an Achilles tendon rupture if the patient is unable to maintain this position for five seconds.
Results: 71 patients with complete mid-substance Achilles tendon ruptures that met inclusion criteria were identified. 45 (63%) presented acutely and 26 patients (37%) presented chronically. The Thompson test displayed a diagnostic sensitivity of (12 26 46%) for chronic ruptures and (38 45 84%) for acute ruptures. The STAMP and TAR tests displayed a diagnostic sensitivity of (22 26 85%) for chronic ruptures and (45 45 100%) for acute ruptures with a diagnostic specificity of (89%).
Conclusion: Achilles tendon ruptures can be difficult to diagnose due to inconsistent symptoms and clinical exam findings. The STAMP and TAR physical exam tests have high sensitivity to clinically diagnose Achilles tendon rupture both in the acute and chronic setting and are superior to well-described physical exam tests. The findings support that the addition of the STAMP and TAR diagnostic protocol may be clinically beneficial when diagnosing Achilles tendon ruptures in both the acute and chronic setting. Future work should be focused on providing direct comparison to other exam maneuvers as well as identifying data reliability.
DOI: 10.1177/2473011421S00401
“In-Situ” Joint Preparation Technique for First Metatarsophalangeal Joint Arthrodesis: A Retrospective Comparative Study with “Flat-Cuts” Technique
Dan Prat, MD; Brandon A. Haghverdian, MD; Eric Pridgen; Wonyong Lee, MD; Keith L. Wapner, MD; Wen Chao, MD; Kathryn O'Connor, MD; Daniel C. Farber, MD
Category: Midfoot/Forefoot; Bunion
Keywords: 1st MTP Joint; Hallux Rigidus; First MTP Arthrodesis
Introduction/Purpose: The most common joint preparation techniques mentioned in literature for 1st metatarsophalangeal (MTP) joint arthrodesis are 'cup and cone' and 'flat-cuts'. A third option of an 'in-situ' technique, has rarely been studied. This study compares the clinical, radiographic, and patients-reported outcomes of 'in-situ' joint preparation with a traditional 1st MTP joint preparation technique.
Methods: The 'in-situ' technique utilizes the same dorsal surgical incision as traditional techniques. Cartilage and osteophyte removal are carried out using standard techniques without the use of specific reamers or a sagittal saw. The arthrodesis is performed in-situ with the similar freedom of joint positioning as the cup and cone technique, and traditional fixation constructs are applied. In this study, A retrospective chart review was performed for patients who underwent 1st MTP joint arthrodesis between January 2015 and December 2019. The complication, revision and non-union rates were examined in a multivariable logistic regression model. Patient reported outcome were analyzed in a repeated measures general linear model. Analysis of variance and Receiver Operating Characteristic were used to assess radiographic measurements.
Results: Total of 388 1st MTP joint arthrodesis cases were included. Overall, 262 'Flat-Cuts' and 126 'In-Situ' cases were analyzed. Mean follow-up time was 292 days (median 174, SD 305). Joint-preparation technique did not have statistically significant impact on union rates (p=0.311) or revision rates (p=0.898). Diabetes-Mellitus was the most powerful predictor of non-union (p<0.001, OR 6.558, 95% CI: 2.534-16.969) and revision (p=0.02, OR 3.662, 95% CI: 1.230-10.905). The rate of transfer- metatarsalgia was significantly higher in 'flat-cuts' (p=0.015, OR 6.808, 95% CI: 1.460-31.744). Visual-Analogue-Scale and PROMIS- CAT-Physical significantly improved at 6-weeks, 3-months, and at last follow-up in both techniques (p<0.001, p=0.001), and the improvement was comparable between the techniques (p=0.078, p=0.100).'In-situ' technique resulted in significantly less mean 1st- ray shortening (3.05mm vs 7.64mm, p<0.001). In a Receiver-Operating-Characteristic analysis of transfer metatarsalgia and 1st ray shortening, the optimal diagnostic cut-off was 6.87 mm (LR 1.67, AUC 0.652, p=0.005, 95% CI: 0.56-0.74).
Conclusion: 'In-situ' joint preparation technique is a simple, safe, and cost-effective technique for 1st MTP joint arthrodesis. In our series, 'in-situ' technique had a similar or better complication profile than the 'flat-cuts', while providing similar patient- reported outcomes. 'In-situ' technique resulted in significantly less 1st ray shortening, which was a predictor of transfer metatarsalgia.
DOI: 10.1177/2473011421S00402
Revision First Metatarsophalangeal Joint Fusion for Non-Union, Implant Failures, and Failed Hallux Valgus Correction: Does the Indication Matter?
Dan Prat, MD; Brandon A. Haghverdian; Eric Pridgen; Wonyong Lee, MD; Keith L. Wapner, MD; Wen Chao, MD; Daniel C. Farber, MD
Category: Midfoot/Forefoot; Bunion
Keywords: 1st MTP Joint; First MTP Arthrodesis; Complications
Introduction/Purpose: The most common indications for revision of 1st Metatarsophalangeal (MTP) joint surgery are symptomatic failures of prior fusion, failed hallux valgus correction, and failed MTP arthroplasty implants. The outcome of revision 1st MTP fusion has rarely been studied. The purpose of this study was to compare the clinical, radiographic, and patient-reported outcomes of revision MTP fusion for different indications.
Methods: A retrospective chart review was performed for patients who underwent revision 1st MTP fusion between January 2015 and December 2019 in a single-center, by 4 fellowship-trained foot and ankle surgeons. The complication, revision, and non- union rates as well as VAS and PROMIS scores and pre-operative and post-operative radiographs were analyzed and compared between the different indication groups. Univariate and multivariate analysis and logistic regression models were used to obtain odds ratio of the explanatory variables for outcome measures.
Results: A total of 79 cases of revision MTP fusion were included. Thirty-eight cases of hallux valgus corrections salvage, 22 failed MTP arthroplasty implants, 6 failed polyvinyl alcohol hydrogel implants, 13 prior MTP fusion non-unions. The mean follow-up time was 350 days (Median 226, SD 306). Seven cases (8.9%) required structural iliac-crest bone graft during the revision. Seven cases (8.9%) required allograft augmentation. The overall complication rate was 40.7%. Fifteen patients (18.5%) were classified as Clavien-Dindo grade 3, which represents a complication that may require a revision surgery (i.e. non-union, deep infection, loss of correction). Eventually, 7 cases (8.9%) underwent further revision surgery. The logistic regression model demonstrated that indication for revision was not significantly related to union rate (p=0.280). Visual-Analogue-Scale significantly improved at 6 weeks, 3 months, and at last follow-up in all indications for revision (p=0.001). PROMIS-10 Physical and PROMIS-10 Mental did not change significantly during follow-up (p=0.860, p=0.589).
Conclusion: Treatment of 1st MTP joint surgery failures is a clinical challenge in orthopaedic surgery. In our study, revision of 1st MTP joint surgery with MTP fusion had higher non-union rates and higher overall complication rates compared to primary 1st MTP fusion. Nevertheless, revision rates remained comparable to primary 1st MTP fusion. Complication rates and patient- reported outcomes were similar between the different indications for revision groups. Visual-analogue-scale improved significantly during follow-up in all groups. Diabetes mellitus had a significant impact on non-union rates and overall complication rates.
DOI: 10.1177/2473011421S00403
Mortality in Patients after Diabetic Charcot Foot-Related Procedures
Anna Ptasinski; Zachary Koroneos; Chris M. Stauch, BS; Brandon Martinazzi, BS; Michael C. Aynardi, MD
Introduction/Purpose: Diabetic Charcot foot is a chronic and progressive disease, following neuropathic loss of protective sensation and causing destruction of the joints. It is classically identified through a rocker-bottom deformity and may also present with a collapse of the medial arch, bony prominences, and ligamentous instability. Charcot leads to further morbidities, and patients may require surgeries including below the knee amputations or limb salvage reconstruction to treat the disease if conservative treatments fail. Previous literature demonstrated that foot ulceration is associated with mortality in diabetic patients, but no clear association between Charcot diagnosis and mortality has been identified. The purpose of this study was to investigate the mortality in patients diagnosed with acute diabetic Charcot foot.
Methods: After institutional review board approval, all patients at a single institution that underwent an orthopaedic surgery for the treatment of Charcot during 2015-2020 were queried using hospital and public records. Demographic data, as well as the 30- day, 90-day, 1-year, and 5-year mortality were recorded.
Results: 79 patients were identified, with 57 (72%) males and 22 (28%) females with Charcot-related surgeries between 2015 and 2020. At the time of surgery, the average age was 58.2 (28-83) years. At the time of analysis, 61 (77%) patients were still living, but 18 (23%) patients were deceased with mortality within 30 days (1), 90 days (5), 1 year (9), and 5 years (18) of the Charcot-related procedure. For deceased patients, the average age of death was 59.6 years (30-83 years). The average number of days post- operation until death was 460 days (23-1613 days).
Conclusion: Diabetic Charcot foot is a serious and debilitating complication of diabetic neuropathy. This data demonstrates that 23% of patients analyzed expired an average of 1.26 years after Charcot-related surgery. In addition, patients that were deceased were an average of 59.6 years of age, suggesting that Charcot may be associated with early mortality. Future studies will include an analysis of possible predictors of mortality for patients diagnosed with Charcot foot to evolve clinical and surgical management of patients.
DOI: 10.1177/2473011421S00404
Anatomy of the Intermetatarsal Facets of the Fourth and Fifth Metatarsals
Mossub Qatu, MD; James R. Jastifer, MD
Category: Basic Sciences/Biologics
Keywords: Fifth Metatarsal; Jones Fracture; 5th Metatarsal Fractures
Introduction/Purpose: The intermetatarsal joint between the fourth and fifth metatarsals (4-5 IM) is important in defining fifth metatarsal fractures. The purpose of the current study was to quantify this joint in order to determine the mean cartilage area, the percentage of the articulation that is cartilage, and to give the clinician data to help understand the joint anatomy as it relates to fifth metatarsal fracture classification.
Methods: Twenty cadaver 4-5 IM joints were dissected. Digital images were taken and the articular cartilage was quantified by calibrated digital imaging software.
Results: For the lateral fourth proximal intermetatarsal articulation, the mean area of articulation was 188 + 49 mm, with 49% of the area composed of articular cartilage. The shape of the articular cartilage had 3 variations: triangular, oval, and square. A triangular variant was the most common (80%, 16 of 20 specimens). For the medial fifth proximal intermetatarsal articulation, the mean area of articulation was 143 + 30 mm, with 48% of the joint surface being composed of articular cartilage. The shape of the articular surface was oval or triangular. An oval variant was the most common (75%, 15 of 20 specimens).
Conclusion: This study supports the notion that the 4-5 IM joint is not completely articular and has both fibrous and cartilaginous components.
DOI: 10.1177/2473011421S00405
A New Approach for Stage 2 Adult Acquired Flatfoot Deformity
Fernando C. Raduan, MD; J. Chris Coetzee, MD; Bryan D. Den Hartog, MD; Jeffrey D. Seybold, MD; Paul M. Cammack, MD; Rebecca M. Stone, MS; Jacquelyn E. Fritz, BS; Kayla Seiffert
Category: Hindfoot
Keywords: Flexible Flatfoot; Arthrodesis; PTTD
Introduction/Purpose: Adult Acquired Flatfoot Deformity (AAFD) is a common progressive pathology that mainly affects patients after their 50s. Even though it is not clear yet what causes AAFD, the great majority of patients have their talonavicular (TN) joint sub dislocated in one or more planes. According to the severity of the deformity and its flexibility, different surgical procedures can be performed to realign the foot. The deformities usually happen around the TN joint, making it the center of rotation and angulation (CORA). Corrections on the CORA realign deformities in different planes and his concept can be applied to mostly any deformity. The objective of this study is to evaluate clinically and radiographically patients with stage 2 AAFD submitted to isolated TN fusion.
Methods: Fifty-four patients (59 feet) from July 2013 to December 2019 with stage 2 AAFD were submitted to isolated TN fusion. All patients had clinical deformity and arch foot collapse associated with pain along the medial hindfoot. Weight-bearing x- rays were performed pre-operatively, the Meary’s and calcaneal pitch angles were measured on lateral view and the Talar coverage and Simmon’s angle were measured on antero-posterior view. Angles were measured by a fully trained foot and ankle surgeon. Post-operative measurements were done with the same set of images by the same surgeon, one month after the initial measurements. FAAM and VR12 were used to compare patient’s clinical status. Patients with previous surgeries on the foot or ankle and patients submitted to other fusions or hindfoot osteotomies were excluded from the study. Gastrocnemius lengthening and toes corrections were not an exclusion criterion.
Results: Thirty-seven females and seventeen males were evaluated with a mean age 61 years at the time of surgery. Only the FAAM score significantly improved from pre-operative (FAAM = 48.48, VR-12 Mental = 55.73, VR-12 Physical = 37.25) to most recent mean follow-up of 16.2 months (FAAM = 58.45 (p<.001), VR-12 Mental = 57.19 (p=.179), VR-12 Physical = 37.53 (p=.832). The lateral view X-Rays showed Meary’s and calcaneal pitch angles mean improving from 27 and 15 degrees pre-operatively to 9 and 18 degrees post operatively (p<.001), whereas Front view foot X-Rays showed Talo-Naviciular coverage angle and Simmon’s angle going from 35 and 20 degrees to 5 and 6 degrees respectively (p<.001)
Conclusion: Isolated talonavicular fusion can correct the deformity on its multiple planes providing not only significant improvement on radiographic alignment but also the FAAM clinical outcome score. Comparative studies should be performed to determine which is the best technique for patients with stage 2 AAFD.
DOI: 10.1177/2473011421S00406
Weber C Fractures Treated with ORIF, Syndesmotic Dynamic Fixation and Open Deltoid Repair: Clinical and Radiographic Evaluation after Minimum 12 Months
Fernando C. Raduan, MD; Bryan D. Den Hartog, MD; J. Chris Coetzee, MD; Jeffrey D. Seybold, MD; William M. Engasser, MD; Paul M. Cammack, MD; Rebecca Stone McGaver; Jacquelyn E. Fritz, BS; Kayla Seiffert
Introduction/Purpose: Ankle fractures are among the most common fractures in the body and it can affect not only professional athletes but also lower activity level and sedentary patients. The standard treatment for displaced fractures is open reduction and internal fixation. Even though the management for Weber B and C fractures is well stablished in the literature, deltoid ligament repair is still debatable. Medial ligament instability is a result of deltoid ligament failure and usually leads to valgus deformity of the ankle and severe morbidity over time. The primary objective of this study is to analyze clinically and radiographically, patients with Weber C fractures and deltoid ligament injury who were submitted to fibular fracture and syndesmotic fixation, associated with deltoid ligament repair.
Methods: Forty one patients who had Weber C fractures with deltoid ligament lesion from January 2013 to December 2019 had their medical records and X-Rays reviewed by a fully trained foot and ankle surgeon. The patients were between 14 and 69 years old and had their medial clear space wider than 4mm on initial X-Rays (our criteria for deltoid ligament lesion). Patients with Weber A or B, diabetics and with previous surgeries on the ankle were excluded. Patients were submitted to open anatomic reduction and fixation of the fibula, the syndesmosis was fixed with dynamic fixation system and the deltoid was reattached to the tip of the medial malleolus with one suture anchor. Medial Clear Spcace, Tibiofiluar clear space and Tibiofibular overlap were measuresd on weight bearing X-Rays done on the last follow up visit. FAAM sports Subscale17 and VR12 were used to evaluate clinical status of our patients.
Results: Forty one patients were analyzed on this series after 22 months on average. The mean age at operation was 37.7 years old. There were 32 males and 9 females. Mental and Physical VR-12 scores went from 56 and 37 pre-operatively to 57 and 50 on their final evaluation. Activity Daily Living and Sports FAAM scores improved from 27 and 7 to 19 and 88 respectively. Post- operative mean medial clear space was 3mm, and mean tibio-fibular clear space was 5mm. The average tibio-fibular overlap percentage was 46%. Patient’s overall satisfaction rate was 86.7%.
Conclusion: Weber C fractures with Deltoid ligament lesion can be successfully treated with anatomic reduction, syndesmotic fixation (dyanamic systems) and open deltoid repairs. Patients show excellent reduction parameters on weight-bearing X-Rays and good clinical outcomes after a minimum 12 months follow up. Comparative studies with and without deltoid ligament repair should be performed to compare two techniques. Weight-bearing CT scan could be used in future studies for more accurate evaluation of the syndesmotic reduction and medial clear space.
DOI: 10.1177/2473011421S00407
Surgical Treatment for Septic Ankle Arthritis: A Comparison of Arthrotomy and Arthroscopy
Pradip Ramamurti; Amil R. Agarwal; Alex Gu, MD; William V. Probasco, MD, MS; Savyasachi C. Thakkar; Marc D. Chodos, MD
Introduction/Purpose: Ankle joint septic arthritis can result in substantial morbidity involving cartilage destruction, bone erosion, osteomyelitis and loss of function. Operative intervention is the preferred method of irrigation and debridement, and options include both open arthrotomy and arthroscopic debridement. Prior studies have established both ankle arthroscopy and arthrotomy as effective management strategies for the treatment of ankle septic arthritis. However, no prior research has compared open arthrotomy verses arthroscopy to treat septic arthritis of the ankle, and it is unclear if one approach is superior to the other. The purpose of this study is to compare the rate of reoperation and 90-day perioperative complications between arthroscopy and open arthrotomy for the treatment of septic ankle arthritis using a national all-payer claims database.
Methods: Patients who were diagnosed with septic arthritis in a native ankle and underwent irrigation and debridement through arthroscopy or arthrotomy were identified in the 2010-2019 PearlDiver database using International classification of diseases (ICD) and current procedural (CPT) codes. Demographic characteristics including age, gender and Elixhauser comorbidities were obtained for each cohort. The rate of reoperation, defined as a proxy for failure of initial intervention, was the primary outcome. Secondary outcomes including readmission, surgical site infection (SSI) and other 90-day complications were compared between the two cohorts. Univariate analysis using chi-square tests and student T-tests were performed to analyze any differences in patient demographics, comorbidities and complications. Multivariate analysis through logistic regression was subsequently conducted to account for any confounding variables and covariates.
Results: In total, 331 patients undergoing arthroscopy and 886 patients undergoing arthrotomy for septic ankle arthritis were identified. On univariate analysis, the incidence of reoperation was higher in the open arthrotomy cohort (12.30%) compared to the arthroscopy cohort (9.37%), however this result was not statistically significant (p=.153). There was also no statistically significant difference between the two cohorts in superficial SSI incidence (3.95% vs. 2.42%, p=.197), readmission rates (36.79% vs. 34.14%, p=.0.391). However, the incidence of renal failure was higher in the open arthrotomy cohort (17.83%) compared with the arthroscopy cohort (12.39%) (p=.022). On multivariate analysis, the incidence of reoperation was higher for those undergoing ankle arthrotomy (OR 1.421; 95% CI 0.937-2.255; p=.108) relative to arthroscopy, however this result was not statistically significant (Table 1). The incidence of renal failure was higher in the open arthrotomy cohort after multivariate analysis (OR 1.615; 95% CI 1.113-2.393; p=0.014).
Conclusion: This study demonstrated similar 90-day rates of reoperation, postoperative complications and readmissions, suggesting that arthrotomy and arthroscopy have similar efficacy in treating septic ankle arthritis. Although renal failure was more prevalent in the cohort undergoing open arthrotomy, differences in the primary endpoint of reoperation/repeat washout rates were non-significant. Based on these findings, deciding between these two operative approaches may be determined by patient specific risk factors and factors not elicited by this study including surgeon comfort with the technique, rather than the treatment modality itself.
DOI: 10.1177/2473011421S00408
Ankle Fractures Involving the Posterior Malleolus: 7-Year Results in 100 Cases
Introduction/Purpose: The presence of a posterior malleolar (PM) fragment has a negative prognostic impact in ankle fractures. The best treatment is still subject to debate and new concepts continue to emerge. The aim of this study was to assess the medium- to long-term clinical and functional outcome of ankle fractures with a PM fragment in a larger patient population treated with an individualized treatment approach.
Methods: One hundred patients with ankle fractures involving the PM were identified retrospectively and reevaluated at an average follow-up of 7.0 years. Fixation of the PM was tailored to the individual fracture pattern. Bartoníček-Rammelt type I PM fractures (extraincisural shell-like fragments) were not fixed surgically. Displaced Type II (posterolateral fragments) and type III PM fractures (two-part with medial extension) were mostly fixed with direct posterior screw or plate fixation. Intercalary joint fragments were fixed with lost K-wires or resorbable pins. Type IV PM fractures (large triangular fragments) were treated with either posterior screw / plate fixation or indirect anteroposterior screw fixation with direct transfibular control of reduction, if feasible.
Results: Internal PM fragment fixation was negatively correlated with the need for syndesmotic screw placement at the time of surgery (p=0.010). At 7 years, the mean Foot Function Index was 16.5, the Olerud Molander Ankle Score averaged 80.2 and the American Orthopaedic Foot & Ankle Society ankle/hindfoot score averaged 87.5. The physical (PCS) and mental health component summary (MCS) scores of the SF-36 averaged 47.7 and 50.5, respectively. Range of motion was within 3.4 degrees of the uninjured side. The size of the PM fragment had no prognostic value. There was a trend to lower outcome scores with anterior or posterior shift of the distal fibula of 1 mm within the tibial incisura. Patients who underwent primary internal fixation had significantly superior SF-36 MCS than patients who underwent staged internal fixation (p=0.031). Two patients (2%) needed secondary ankle fusion following deep infection.
Conclusion: With an individualized treatment protocol, tailored to the CT-based assessment of PM fractures, favorable medium and long-term results can be expected. The mere size of the PM fragment is just one of the factors guiding treatment, other important criteria are fragment displacement, impaction of the tibial plafond and incisura involvement. PM fixation provides direct bone-to-bone fixation of the syndesmosis and significantly reduces the need for additional transsyndesmotic fixation with a screw or flexible implant.
DOI: 10.1177/2473011421S00409
Quadrimalleolar Fractures of the Ankle: Principles and Medium-Term Results of Surgical Fixation
Stefan Rammelt, MD, PhD; Livia Kroker; Annika P. Neumann
Introduction/Purpose: Over the last decade, much attention has been paid to the fractures of the posterior malleolus as it became obvious that the mere presence of a posterior tibial fragment is associated with a less favorable prognosis in malleolar fractures. It seems logical to pay the anterior restraints of the ankle joint a similar attention as to the posterior ones. The anteriolateral distal tibia may be considered a 'fourth' or anterior malleolus. Here, we present a technique of fixation of trimalleolar fractures with additional fracture of the anterior tibial tubercle ('quadrimalleolar') or anterior fibular rim ('quadrimalleolar equivalent').
Methods: Twenty-four patients with a mean age of 60 years were treated with open reduction and internal fixation of all 4 malleoli. There were 17 quadrimalleolar and 6 quadrimalleolar equivalent fractures. One patient had both anterior tibial and fibular avulsion fractures in addition to a trimalleolar ankle fracture. Surgical approaches and internal fixation were tailored individually. Twenty patients were operated in prone position with direct fixation of the posterior malleolus and 4 patients in supine position with indirect anterior to posterior screw fixation of the posterior malleolus under transfibular control of reduction.
Results: After fixation of al 4 malleoli, only one patient (4%) required a syndesmotic screw for residual syndesmotic instability on intraoperative testing. There were no infections, and no wound healing problems. All patients went on to solid union. No late fusions were needed. Nineteen patients (79%) could be reevaluated after a mean of 77 months (range, 15 to 156 months) follow- up. The Foot Function Index averaged 15 (range, 50 to 0), the Olerud and Molander Score averaged 79 (range, 45 to 100) and the AOFAS Ankle and Hindfoot Scale averaged 87 (range, 39 to 100).
Conclusion: Fixation of the anterior and posterior tibial fragments increases syndesmotic stability by providing a bone-to-bone fixation. Reduction of displaced anterior and posterior tibial rim fractures restores the physiological shape of the tibial incisura and therefore facilitates fibular reduction. In the majority of cases, this also restores articular congruity of the lateral tibial plafond. Anatomic reduction of the anterior and posterior malleolus in addition to medial and lateral malleolar fixation leads to favourable functional results despite a complex (quadrimalleolar) fracture pattern.
DOI: 10.1177/2473011421S00410
Clinical Management and Functional Outcomes of Postoperative Achilles Tendon Infections: How Do These Really Do?
Carson M. Rider, MD; Oliver B. Hansen; Mark C. Drakos, MD
Introduction/Purpose: Achilles tendon repairs and reconstructions have historically been associated with high wound infection rates due to poor vascularity in this region. The risk of postoperative infection, a potentially devastating complication, has led surgeons to pursue non-operative treatment when possible for a range of Achilles tendon pathology. However, new surgical techniques have allowed for smaller incisions and modern, aggressive infection control strategies have limited the morbidity associated with these complications. The present study will review a large case series of Achilles infections, evaluating treatment strategies and outcomes for patients who developed a postoperative infection following treatment for Achilles pathology.
Methods: This is a retrospective case series including all patients who experienced a postoperative Achilles tendon infection at a single hospital. Cases from 11 surgeons performed between 2011 and 2020 were reviewed for infection requiring a return to the operating room for irrigation, debridement, and any other necessary interventions. Cases that presented to our institution with an existing infection were also included. Thorough chart review was performed for all patients to determine pathology and initial treatment method, infection management, and clinical outcomes. For patients undergoing Achilles reconstruction with a graft, operative notes were reviewed to determine whether the graft was infected and thus removed during debridement. Clinical follow-up was performed and Patient-Reported Outcomes Measurement Information System (PROMIS) surveys were sent to all patients who were over 1 year out from surgery.
Results: 33 patients experienced a postoperative Achilles infection, including 10 who developed infection after surgery at an outside hospital. For patients treated initially at our institution, 8 presented with an acute rupture and 15 with chronic pathology. 12 of 15 chronic cases underwent reconstruction with a graft. For 3 reconstructions and 1 acute repair (12%) the entire Achilles was infected and removed. The graft was partially removed in 2 reconstruction cases (6%) and remained fully intact in the remaining 27 cases (82%). In 2/4 cases in which the Achilles was removed, it ultimately reconstituted as confirmed on MRI. A skin graft or flap was required in 5 of 33 cases (15%) for adequate soft-tissue coverage. In 14 cases (42%), the infection was controlled after a single debridement, 17 cases (52%) required a second debridement, and 2 cases (6%) a third. Postoperative PROMIS scores were available for 17 patients (Table 1).
Conclusion: To our knowledge, this case series represents the largest number of postoperative infections analyzed following Achilles tendon surgery. Relatively high postoperative PROMIS scores indicate that infected patients can ultimately reach high levels of physical function with minimal pain when managed appropriately. In many cases the Achilles or graft could be salvaged and in those where it was not, the tendon did at times reconstitute.
DOI: 10.1177/2473011421S00411
Differences in the 30 Days vs One-Year Complications and Reoperations after Total Ankle Replacement and Ankle Arthrodesis: A Large Database Study
Dietrich Riepen, MD; Senthil Sambandam; Varatharaj Mounasamy; Dane K. Wukich, MD
Introduction/Purpose: Total ankle replacement (TAR) and Ankle arthrodesis (AA) are two commonly performed procedures for end stage arthritis of ankle joint. Aim of this study was to analyze the characteristics of the complications and reoperations at 30 days and 1 year in a matched sample of TAR and AA in a large database population
Methods: Commercially available patient database record (PearlDiver) was used for this study. Patient undergoing TAR and AA were identified using CPT code. After matching two groups for diabetes, smoking, obesity and comorbidities scores, the differences in the risk of complications at 30 days and 1 year and the risk of reoperation at 1 year were noted in both groups.
Results: There were 1287 patients in each matched group. Four hundred and thirty patients were diabetic, 102 patients were smokers and 543 patients were obese. The risk of surgical site infection and wound dehiscence were higher at 30 days in the AA group. Vast majority of observed complications (More than 50% of complications) happened after 30 days. AA group showed higher risk of SSI, wound dehiscence, mechanical complications and pneumonia at 1 year. The risk of reoperation was also higher in the AA group at 1 year.
Conclusion: Ankle arthrodesis is associated with higher risk of local and systemic complications at 30 days and 1 years and higher reoperation rate at 1 year. Most complications happened after 30 days which highlights the fact that studies reporting 30 days complications after AA and TAR may underestimate the complications.
DOI: 10.1177/2473011421S00412
Thirty Days vs One-Year Complications and Reoperations after Foot Amputation and Below Knee Amputation: A Large Database Study
Dietrich Riepen, MD; Senthil Sambandam; Varatharj Mounasamy, MD; Dane K. Wukich, MD
Introduction/Purpose: Below knee amputation (BKA) and Foot amputation (AA) are two commonly performed procedures for diabetic foot conditions. Aim of this study was to analyze the characteristics of the complications and reoperations at 30 days and 1 year in a matched sample of BKA and FA in diabetic patients in a large database population.
Methods: Commercially available patient database record (PearlDiver) was used for this study. Diabetic Patient undergoing BKA and FA were identified using CPT code. After matching two groups for smoking, obesity and comorbidities scores, the differences in the risk of complications at 30 days, 90 days and 1 year and the risk of reoperation at 1 year were noted in both groups.
Results: There were 8555 patients in each matched group. Most patients were male (71.6%) and 6891 patients were smokers and 5292 patients were obese. More than 50% of general and systemic complications happened after 30 days. Incidence of 30 days, 90 days and 1 year general complications including Acute kidney injury, cardiac arrest, Cerebrovascular event, myocardial infarction, Pulmonary embolism, Pneumonia, sepsis and transfusion were higher in the BKA group. AKI was the most common general complication and PE was the least common general complication observed at 30 days, 90 days and 1 year. The risk of wound dehiscence, surgical site infection and overall wound complications were higher in FA group. One year reoperation for infection and dehiscence were higher in the FA group and reoperation for hematoma formation was higher in BKA group. The risk of revision to a BKA in the FA group at 1 year was 16.4% (1410 patients).
Conclusion: FA is associated with higher risk of local complications at 30 days, 90 days and 1 years and higher reoperation rate at 1 year for local complications. However, BKA is associated with higher systemic major complications and higher risk of reoperation for hematoma formation. Most complications in the FA and BKA group happened after 30 days which highlights the fact that studies reporting 30 days complications after FA and BKA may underestimate the complications.
DOI: 10.1177/2473011421S00413
Arthroscopic Bone Marrow Stimulation or Non-Operative Treatment for Osteochondral Lesions of the Tibial Plafond
Quinten Rikken; Jari Dahmen, BSc,BSc(Med); Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Category: Ankle; Arthroscopy
Keywords: Cartilage Defect; Ankle; Arthroscopy
Introduction/Purpose: A paucity of clinical results from osteochondral lesion of the tibial plafond (OLTP) treatment exists in the literature. The primary purpose of this study was therefore to compare the patient reported outcomes of OLTPs treated with arthroscopic bone marrow stimulation (BMS) and non-operative treatment. The secondary purpose was to compare the reintervention- and complication rates.
Methods: Patients treated either with BMS (BMS group) or any form of non-operative treatment (non-operative group) at a minimum follow-up of 12 months were selected from a retrospective database query of patients treated between 1990 and 2020. Eligible patients were contacted by phone and cross-sectionally included. The primary outcome was the Numeric Rating Scale (NRS) during weightbearing. Secondary outcomes included; the NRS in rest, the Foot and Ankle Outcome Score (FAOS), and the Short Form Health Survey (SF-36) general health questionnaire. Additionally, the reintervention- and complication rates were collected.
Results: A total of 55 patients were included, which consisted of 15 patients for the non-operative group and 40 patients for the BMS group were analyzed at a mean 73.2 +- 62.9 and 100.5 +- 72.1 months respectively (Table 1). The median NRS during weightbearing was 2 (IQR: 1-5) for the non-operative group and 1.5 (IQR: 0-4) for the BMS group (P= 0.43). The NRS in rest was, similarly, not significantly different between groups. None of the FAOS subscales were found to be significantly different between treatment groups. No reoperations or major complications after follow-up treatment were recorded.
Conclusion: Clinical outcomes following arthroscopic BMS and non-operative treatment yield moderate to good clinical results in this cross-sectional cohort OLTP patients. Although this study was the first to report outcomes of non-operative treatment of OLTPs and to compare these to BMS, prospective studies are highly needed for these understudied lesions.
DOI: 10.1177/2473011421S00414
Incidence of (Osteo)Chondral Lesions Concomitant to Chronic Lateral Ankle Instability: Systematic Review and Meta-Analysis
Quinten Rikken; Emma Wijnhoud; Jari Dahmen, BSc,BSc(Med); Inger Sierevelt, MSc; Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Introduction/Purpose: To determine the incidence of (osteo)chondral lesions ((O)CLs) in patients with chronic lateral ankle instability (CLAI).
Methods: A literature search was conducted in PubMed (MEDLINE), EMBASE (Ovid), and the Cochrane Library databases for articles published from January 2000 until December 2020. Two authors independently screened the search results and conducted the quality assessment using the MINORS criteria. Clinical studies that reported findings on (O)CLs of the ankle as per preoperative or intraoperative diagnostic measures in patients with CLAI (> 6 months of symptoms) were included. Chondral and osteochondral lesions were analyzed altogether for the primary outcome, namely, the incidence of (O)CLs in ankles with CLAI. Additionally, a subgroup analysis for the incidence of (O)CLs located on the talus. Secondary outcomes included the study-, patient, and lesion characteristics. Lesions characteristics included lesion localization and chondral- or osteochondral involvement. A random-effects model with 95% confidence intervals (95% CI) was used to analyze the primary outcome and subgroup analysis. Secondary outcomes were pooled using a simplified pooling method.
Results: 12 studies with a total of 2145 patients with 2170 ankles with CLAI were included. The overall pooled incidence of (O)CLs in ankles with CLAI was 32.2% (95% CI 22.7 - 41.7). The pooled incidence of talar (O)CLs was 26.5% (95% CI 19.0 - 34.0). Overall the most common location of OCLs in patients with CLAI is the talus with 85%, of which 68% of (O)CLs are located on the medial talus and 32% are located laterally. 43% of lesions were chondral lesions and 57% of lesions were osteochondral in nature.
Conclusion: (O)CLs were found in up to 32% of ankles with CLAI. Furthermore, most lesions are located on the medial talar dome. These findings will aid physicians in the early recognition and treatment of ankle (O)CLs in the context of CLAI.
DOI: 10.1177/2473011421S00415
Long-Term Clinical Results of Arthroscopic Lift-Drill-Fill and Fixation (LDFF) Treatment for Osteochondral Lesions of the Talus
Quinten Rikken; Jari Dahmen, BSc,BSc(Med); Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Introduction/Purpose: The purpose of this study was to describe the long-term (> 5 years) clinical results of a novel arthroscopic fixation technique for osteochondral lesions of the talus (OLT), named the Lift, Drill, Fill and Fix (LDFF) technique.
Methods: 18 ankles (17 patients) underwent an arthroscopic LDFF procedure for a primary OLT. The mean follow-up was 6.8 years (range: 68 - 96 months). Pre- and postoperative clinical assessment was prospectively performed by measuring the Numeric Rating Scale (NRS) of pain at rest, during walking, and when running. Additionally, the Foot and Ankle Outcome Score (FAOS) including its subscores of pain, symptoms, activities of daily living, sports, and quality. Additionally, the Short Form-36 (SF-36) was assessed.
Results: The mean NRS during running significantly improved from 7.8 pre-operatively to 3.7 post-operatively (p = 0.006), the NRS during walking from 5.7 to 1.5 (p < 0.001), and the NRS in rest from 2.3 to 1.0 (p = 0.015). The median FAOS at final follow- up was 80 for pain, 57 for other symptoms, 90 for activities of daily living, 70 for sport, and 55 for quality of life. A pre- and post- operative score comparison was available for fifteen patients, and improved significantly in most subscores. The SF-36 physical component scale significantly improved from 42.9 pre-operatively to 50.1 post-operatively.
Conclusion: Arthroscopic LDFF of fixable primary OLTs results in excellent pain reduction and improvement of functional outcomes, with sustained results at long-term follow-up. These results indicate surgeons should consider fixation for a fixable OLT.
DOI: 10.1177/2473011421S00416
Outcomes of Bone Marrow Stimulation for Secondary Osteochondral Lesions of the Talus Equal Outcomes for Primary Lesions
Quinten Rikken; Jari Dahmen, BSc,BSc(Med); Christiaan v. Van Bergen; Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Introduction/Purpose: To compare clinical, sports, work, and radiological outcomes between primary and secondary OLTs (<15mm) treated with arthroscopic BMS.
Methods: Ethical approval was obtained before the start of the study. A power analysis was performed for the primary outcome measure, the Numeric Rating Scale (NRS) during activities. Secondary OLTs were matched to primary OLTs in a 1:2 ratio using lesion size, patient age, body mass index, and sex as prognostic covariates to control for confounding. Secondary outcomes included pre- and one-year postoperative clinical assessment of the NRS at rest, American Orthopaedic Foot & Ankle Society (AOFAS) score, Foot and Ankle Outcome Score (FAOS) subscales, and the EQ-5D general health questionnaire. The rates and time to return to work and sports were collected. Radiological examinations were performed preoperatively and at final follow-up using computed tomography (CT). The postoperative outcomes were compared with a Wilcoxon rank-sum test; a univariate linear regression analysis was used to investigate the influence of covariates on clinical outcome scores.
Results: After matching, 22 and 12 patients with smaller (<15 mm) OLTs were included in the primary and secondary group, respectively. The NRS during activities was not different between primary cases (median: 2, IQR: 1 - 4.5) and secondary cases (median: 3, IQR: 1 - 4), P= 0.5. Both groups showed a significant difference between all pre- and postoperative clinical outcome scores, except for the FAOS symptoms subscale in the primary group and NRS at rest in the secondary group. No significant differences in any clinical outcome scores were found between both groups at one-year follow-up, nor did any covariate significantly influence the clinical outcome scores. The return to sport rate was 90% for primary cases and 83% for secondary cases (P= 0.6). All patients returned to work. Lesion filling on CT was complete (67% - 100%) in 59% of primary cases and 67% of secondary cases (P= 0.6).
Conclusion: No differences in outcomes were observed between arthroscopic bone marrow stimulation in primary and secondary OLT at one-year follow-up. Repeat BMS may therefore be a viable treatment option for failed OLTs in the short term.
DOI: 10.1177/2473011421S00417
Three-Dimensional Fluoroscopy Influence in Intraoperative Decision-Making Concerning Syndesmotic Reduction
Maximiliano Rivera, MD; Natalio R. Cuchacovich Mikenberg, MD; Gonzalo F. Bastias, MD; Patricio A. Fuentes
Introduction/Purpose: The use of intraoperative three-dimensional fluoroscopy to evaluate syndesmotic and articular reduction in ankle fractures is a relatively new tool demonstrating usefulness in the literature. It has been described that it can detect up to 32.7% of intraoperative malreduction. The objective of this prospective study is to observe if surgeons, when performing operative treatment in ankle fractures with three- dimensional fluoroscopy assistance, modify the syndesmotic reduction and/or fixation. The definitive syndesmotic reduction was assessed with bilateral ankle CT-scan postoperatively.
Methods: Sixteen patients with ankle fracture and syndesmotic instability were analyzed. After malleolar and syndesmotic fixation, intraoperative three-dimensional fluoroscopy was performed. The surgeon then analyzed cross-sectional images to evaluate the reduction of the fracture and syndesmosis. In this scenario, the surgeon decided whether to make any changes in the reduction of the syndesmosis or in the configuration of the fixation strategy. Postoperative bilateral computed tomography was carried out to corroborate in detail if there was any syndesmotic malreduction.
Results: Sixteen patients were included in this study (10 men) with a mean age of 40 years (range 25-60 years). 62% were supination-external rotation fractures according to Lauge-Hansen classification. Of all the patients evaluated, only 4 underwent any modification after performing intraoperative three-dimensional fluoroscopy. From the previous group, in 3 patients (19% of the total) there was a change in syndesmal reduction and in only one there was a change of any element of osteosynthesis. When evaluating syndesmal reduction with postoperative bilateral CT, there were 6 patients in the total group who presented syndesmal malreduction. In patients in whom a modification to syndesmal reduction was made, it persisted in 2 of the 3 cases.
Conclusion: In our series, the use of intraoperative three-dimensional fluoroscopy did not motivate most surgeons to make changes in syndesmotic reduction, unlike other previously published studies. Even despite making changes in syndesmotic reduction, the percentage of patients who persists with poor reduction is considerable. In this study, the percentage of poor syndesmotic reductions was 32.7%. Despite being a figure that is within what is expected according to the literature, we consider that it is high even using intraoperative fluoroscopy as support.
DOI: 10.1177/2473011421S00418
Weightbearing Computed Tomography for Assessment of Foot and Ankle Deformities: The Iowa Experience
Edward O. Rojas; Nacime S. Mansur, MD; Kevin N. Dibbern, PhD; Eli C. Auch, BS; Eli Schmidt; Victoria Vivtcharenko, BS; Shuyuan Li, MD, PhD; Phinit Phisitkul, MD; John E. Femino, MD; Cesar de Cesar Netto, MD, PhD
Category: Ankle; Ankle Arthritis; Other
Keywords: Weight Bearing CT; Ankle; CT
Introduction/Purpose: Weightbearing computed tomography (WBCT) is a reliable and precise modality for the measurement and analysis of bone position in the foot and ankle, as well as associated deformities. WBCT to assess three dimensional relationships among bones allowed the development of new measurements, as the Foot and Ankle Offset (FAO), which has high inter-rater and intra-rater reliability. This study reports our institution’s experience utilizing WBCT for the care of foot and ankle patients by describing its utility across different orthopedic diseases in improving diagnostic assessment, aiding surgical planning, and expanding the use for objective clinical follow-up.
Methods: The medical records of consecutive patients with various foot and ankle disorders that underwent WBCT examination as part of the standard of care at a single institution between November 2014 and August 2020 were retrospectively reviewed. Patient factors, including body mass index (BMI), sex, and patient comorbidities were collected. 3D coordinates for calculation of FAO were harvested using the Multiplanar Reconstruction (MPR) views were calculated from the obtained exams. Descriptive statistics were performed with Shapiro-Wilk test and the Anderson-Darling tests.
Results: 1175 feet and ankles (820 patients) had a WBCT performed over the studied 68 months. 53% of the subjects were male and 47% female. 588 of the acquisitions were from the right side (50.04%) and 587 from the left side (49.96%). Diabetes was present in 15.47% of, Rheumatic diagnoses in 4.52% and smoking habits in 44.10% of patients. Mean BMI of the sample was found to be 32.47 (32.03-32.90, 95% CI). The mean Foot and Ankle Offset (FAO) encountered in the study’s population was 2.43 (2.05- 2.82, 95% CI; min -30.8, max 37.65; median 2.39).
Conclusion: This study contains the largest cohort of WBCTs with accompanied FAO measurements to date, which can aid with establishing a new baseline FAO measurement for multiple pathological conditions. Acquiring WBCTs resulted in more specific diagnoses for patients with foot and ankle complaints. The ability to utilize WBCT for presurgical planning, its capability to provide a 3D reconstruction of patient anatomy, and use for assessment of advanced relational foot and ankle measurements, like FAO, demonstrate how WBCT may serve as a remarkable utility in clinical practice and has become a standard of care in our practice at the University of Iowa.
DOI: 10.1177/2473011421S00419
Foot and Ankle Injury Surveillance of Collegiate Student-Athletes Utilizing the Pac-12 Health Analytics Program
Lexie Ross; Mary C. Hamati, MD; Michael Tuffiash; Kevin Robell; Kenneth J. Hunt, MD
Category: Ankle; Sports; Other
Keywords: Sports; Return to Play; Outcomes Measures
Introduction/Purpose: In order to monitor student-athlete health, identify risk factors associated with sports injuries, and develop and evaluate injury prevention programs at the collegiate level, it is necessary to implement and utilize high quality sports injury surveillance systems. The Pac-12 Health Analytics Program (HAP) addresses this need by standardizing electronic medical record entries and common data elements across all Pac-12 institutions. The literature suggests that collegiate student-athletes are at higher risk for certain injuries that have chronic effects on their health-related quality of life. Previous investigations utilizing the HAP database found ankle injuries to be the second most prevalent lower extremity injury in this population. This study aims to build upon these previous findings and further characterize below-knee injuries using the HAP database.
Methods: We retrospectively reviewed archival data from Pac-12 student-athletes followed in the HAP database, a deidentified Pac-12 conference-wide sports injury surveillance system used to study the epidemiological characteristics of varsity student- athletes from 2017-2020. Data collection is part of the standard of care provided by varsity athletic trainers and entered into the Presagia Sports electronic medical record. This data is then deidentified and automatically sent to the Pac-12 for inclusion in the HAP. Individual authorization forms were obtained from student-athlete participants prior to deidentification and inclusion in the HAP database. Student-athletes who sustained a lower extremity (LE) injury below the knee were included. Data on demographics and injury characteristics were analyzed.
Results: Foot and ankle injuries account for 20.3% (6,776/33,432) of all database injuries, representing 23.4% (2,214/9,444) of all student-athletes. Female-athletes (26.8%) had a higher injury rate than male-athletes (20.9%) (p<0.00001). Lower leg injuries were categorized as ankle (43.1%), foot (25.3%), lower leg (18.4%), and ankle/heel (13.2%). Ligament sprain was the most common injury type (38.1%) followed by tendinopathy (14.4%) and inflammation (7.9%). Males were more likely to sustain an acute injury (81.8%) than females (63.7%). Injuries most commonly occurred on synthetic (46.0%). Common mechanisms of injury (MOI) included running (21.6%), contact with another player (18.4%), and contact with a hard object (14.8%). Injuries most commonly occurred during in-season (48.9%) compared to off-season (25.5%) and pre-season (20.9%) segments of the competitive year. Half of injuries (50.0%) resulted in lost time from sport, however only 6.7% of injuries were season ending and only 2 injuries (<0.01%) resulted in medical retirement.
Conclusion: Most ankle injuries occurred on synthetic surfaces, suggesting an opportunity for enhanced monitoring and prehabililitation programs for sports that utilize these types of surfaces. Further investigations accounting for covariates and risk factors may inform injury prevention strategies and improve student-athlete wellness. While the Pac-12 HAP database is early in development, this report demonstrates the potential value that injury surveillance systems can provide for student-athlete health. The Pac-12 HAP is a collaborative and effective injury database, setting the standard for other regional conferences.
DOI: 10.1177/2473011421S00420
Syndesmotic Overload in 3-Component Total Ankle Replacement
Roxa Ruiz, MD; Peter Kvarda; Roman Susdorf, PhD; Nicola Krähenbühl, MD; Alexej Barg, MD; Beat Hintermann, MD
Introduction/Purpose: Mobile-bearing total ankle replacement (TAR) potentially enables motion at the tibial implant- polyethylene insert (PI) interface. Such additional freedom of movement may overload periarticular ligaments and subsequently result in coronal translation of the talus. The aim of this study was to assess whether syndesmotic overload affects clinical and radiographic outcomes following mobile-bearing TAR and whether tibiofibular fusion is an effective treatment option.
Methods: Thirty-one patients who underwent revision surgery for syndesmotic overload after mobile-bearing TAR were retrospectively analyzed. Clinical and radiographic outcome, including computed tomography scans, were assessed before and after index TAR, preoperatively to revision surgery, and at the last follow-up after revision surgery. Additionally, available computed tomography scans were analyzed.
Results: Ankles with lateral talar translation prior to revision surgery were about 10 times more likely to have valgus tibial implant position (P =.003). A wide tibiofibular distance at the level of the syndesmosis after index TAR was associated with an increased hindfoot moment arm at revision surgery (P =.025). Decrease of PI height at revision surgery and a PI fracture were evident in 10 (32%) and 4 (13%) cases, respectively. Talar cyst formation at revision surgery was evident in 12 (39%) cases. Tibiofibular fusion was effective in restoring function of the replaced ankle and providing pain relief.
Conclusion: Syndesmotic overload impaired clinical and radiographic outcomes after mobile-bearing TAR. Proper implant positioning and additional realignment procedures may prevent overload of periarticular soft tissue structures after mobile-bearing TAR.
DOI: 10.1177/2473011421S00421
Heterotopic Ossification Following Total Ankle Arthroplasty with Fourth- Generation Prostheses
Calvin J. Rushing, DPM; Antonio M. Malloy McCoy; James M. Steriovski, DPM; Christopher F. Hyer, DPM; Gregory C. Berlet, MD
Introduction/Purpose: The purpose of the present study was to assess the radiographic incidence, location, and classification of heterotopic ossification (HO) in patients who underwent total ankle arthroplasty (TAA) with a 4th generation prostheses at a minimum of 1-year follow up. Baseline demographic, radiographic, and operative factors between patents with and without HO were compared.
Methods: Ninety ankles that underwent TAA with a 4th generation protheses, INFINITY (n = 62) or CADENCE (n = 28) were followed for an average of 23.7 (range, 12-49) months. Incidence and location of HO was assessed on weight bearing radiographs, and severity graded according to the modified Brooker classification. Data was compared between patents with and without HO to identity any predisposing factors.
Results: In 90 ankles that underwent 4th generation TAA, HO incidence was 55.6% (n = 50); 56.5% (n = 35) for INFINITY, and 53.6% (n = 15) for CADENCE. Twenty-five cases of HO were observed posteriorly, 16 anteriorly, and 9 combined. Severity was as follows; class I in 19 cases (38%), class II in 20 (40%), class III in 9 (18%) and class IV in 2 (4%). A single ankle required a non- revisional reoperation for HO debridement; reoperation rate of 2%.
Conclusion: The present study suggests a similarly high incidence of HO after TAA with two different 4th generation prostheses (INFINITY 56.5%, CADENCE 53.6%). A trend for differences in location and severity between the prostheses may also be present. Given the paucity of literature, additional studies with longer follow-up are warranted to discern the significance of HO following TAA with 4th generation prostheses.
DOI: 10.1177/2473011421S00422
The INBONE-2 Total Ankle Prosthesis: Outcomes At 5 to 9 Years Follow-Up
Calvin J. Rushing, DPM; Antonio M. Malloy McCoy; Gregory C. Berlet, MD; Christopher F. Hyer, DPM
Category: Ankle; Hindfoot; Other
Keywords: Ankle Arthroplasty; Total Ankle Arthroplasty; Hindfoot
Introduction/Purpose: Short and medium term outcomes of the INBONE I and INBONE II tibial stems have been favorable. The INBONE-2 talus has been shown to have lower reoperation and failure rates compared to its predecessor, INBONE-1 at short term follow-up. The purpose of the present study was to assess mid-term outcomes for the INBONE-2 prosthesis at 5 to 9 years follow-up considering both the tibial and talar components.
Methods: All patients who underwent primary total ankle arthroplasty (TAA) with INBONE-2 between July 2010 and July 2014 at a single institution and who were at least 5 years postoperative were included. A total of 15 ankles with a mean follow up 85 (range, 61-113) months met the criteria. Radiographs were assessed using coronal and sagittal alignment parameters preoperatively, at 6 weeks postoperative, and at the most recent follow-up. Medical records were reviewed and revisions, reoperations, and complications were classified according to the criteria established by Vander Griend et al. and Glazebrook at el., respectively.
Results: Survivorship for the INBONE-2 at a mean of 85 months was 93.7%. Coronal and sagittal tibiotalar alignment improved after surgery (p=0.081, p=0.15), and was maintained at the most recent follow-up (p=0.684, p=0.837). One ankle (6.7%) required early component revision; while 4 (26.7%) required a non-implant related revision. Six complications (2 high grade, 1 intermediate, and 3 low) in 5 ankles (33.3%) were recorded according to the Glazebrook classification system.
Conclusion: The present study is the first to report midterm follow-up after TAA with the INBONE-2. High survivorship, maintenance of correction, and a low incidence of major complications was observed. The most common complication overall was lateral gutter impingement, which accounted for the majority of the non-revisional reoperations.
DOI: 10.1177/2473011421S00423
Total Ankle Arthroplasty with Anatomic Lateral Ankle Stabilization (ATLAS) using Synthetic Graft for Instability in Moderate and Severe Pre-Operative Varus Alignment
Calvin J. Rushing, DPM; Antonio M. Malloy McCoy; Bryon J. McKenna, DPM; Gregory C. Berlet, MD
Introduction/Purpose: More than 50% of patients undergoing Total Ankle Arthroplasty (TAA) have some degree of coronal deformity, which is the most common reason for additional procedures. The purpose of the present study was to assess the early clinical and radiographic outcomes for patients who underwent TAA and Anatomic Lateral Ankle Stabilization (ATLAS) using synthetic graft for instability in moderate and severe preoperative varus alignment.
Methods: Seven ankles with moderate or severe varus alignment underwent TAA with a 3rd generation prosthesis (INBONE-2) and ATLAS using synthetic graft between September 2018 and February 2019 at a single institution, and were at least 1 year postoperative (mean 13.3 months, range 12-15). Medical records and charts were reviewed for any revisions, reoperations, or complications. Weight bearing radiographs were assessed using coronal and sagittal alignment parameters preoperatively, and during the latest follow-up.
Results: Survivorship for INBONE-2 with ATLAS was 100%; recurrent instability was not observed. Symptomatic talonavicular joint arthritis was recorded for a single patient 12 months postoperatively; there were no revisions, or reoperations. Tibiotalar coronal alignment improved significantly from 17.7 +- 9.3 (range, 10.1-33.6) to 2.3 +- 1.2 (range, 0.9-4.4) degrees (p<0.006), and all ankles achieved neutral alignment in single stage. Regarding sagittal tibiotalar alignment, preoperatively 2 ankles (28.5%) were translated anteriorly and the rest were neutral (71.5%). Significant posterior translation was observed and during the latest follow- up, 4 ankles were neutral (57.1%) and 3 posterior (42.9%) (p<0.009).
Conclusion: Satisfactory outcomes were observed at a minimum of 1-year follow-up for patients with moderate or severe varus alignment who underwent TAA with INBONE-2 and ATLAS. ATLAS using synthetic graft may afford advantages over previously described repair techniques. Comparative studies between the Brostrum-Gould and ATLAS are warranted in the TAA population.
DOI: 10.1177/2473011421S00424
A Comparison of Portable Ultrasonography and the Fluoroscopy for Evaluating Medial Ankle Instability: A Cadaveric Study
Jirawat Saengsin, MD; Go Sato, MD; Pongpanot Sornsakrin, MD; Bart Lubberts, MD, PhD; Gregory R. Waryasz, MD; Daniel Guss, MD, MBA; Christopher W. DiGiovanni, MD
Introduction/Purpose: Diagnosis of destabilizing deltoid ligament injuries remains challenging and is best identified with dynamic imaging techniques. This study aims to assess and compare medial clear space (MCS) distances in various stages of sequentially created supination external rotation (SER) ankle injury model using portable ultrasound (P-US) and fluoroscopy. We hypothesize that there is a strong correlation between the P-US and fluoroscopic measurements for the assessment of medial ankle instability in SER type ankle injury during the gravity stress test (GST), weight-bearing, or external rotation stress test.
Methods: Ten cadaveric specimens were used for assessing medial ankle instability. The assessment was performed with all structures intact, and later with sequential transection of the anterior inferior tibiofibular ligament (Stage I), fibular (Weber-B fracture) (Stage II), posterior inferior tibiofibular ligament (Stage III), superficial deltoid ligament (Stage IVa), and deep deltoid ligament (Stage IVb). In all scenarios, the GST, external rotation stress test(45N), and Simulated weight-bearing condition(750N) were performed. The P-US measurement of the MCS was assessed at the anteromedial and inferomedial aspect of the ankle joint. Three different MCS distances were measured, as demonstrated in Figure 1. The fluoroscopic MCS measurements were assessed on a true mortise ankle view achieved during each loading condition. Spearman rank correlation was used to investigate the relationship between the P-US and fluoroscopic measurements. The inter- and intra-observer agreement was assessed using the intraclass correlation coefficient (ICC) through a two-way mixed-effects model with absolute agreement.
Results: The P-US and fluoroscopic assessed medial ankle instability values during the GST, weight-bearing, and the external rotation stress test increased as the SER ankle injury stage progressed. The P-US values measured during all stress tests demonstrated a moderate to strong positive correlation with those measured with the fluoroscopy (Spearman’s rank correlation ranged from 0.61-0.93, p-values <0.001). Inter-rater (P-US: 0.97, 95%CI: 0.96-0.98) and intra-rater reliability (P-US, 0.95, 95%CI: 0.94-0.96) for the P-US measurements were all substantial.
Conclusion: The use of dynamic P-US to measure the MCS appears to be a reliable and repeatable technique. The P-US MCS measurement values measured in the SER ankle injury model during the GST, weight-bearing and the external rotation stress test are well correlated with those values measured with fluoroscopy. Therefore, the dynamic P-US with stress examination of the ankle has the potential to quantify medial ankle instability in a radiation-free, non-invasive, low cost, and point of care setting.
DOI: 10.1177/2473011421S00425
Diagnosing Medial Ankle Instability with Gravity Stress, Weight-Bearing, and External Rotation Stress Ultrasonography: A Cadaveric Study
Jirawat Saengsin, MD; Pongpanot Sornsakrin, MD; Go Sato, MD; Bart Lubberts, MD, PhD; Gregory R. Waryasz, MD; Daniel Guss, MD, MBA; Christopher W. DiGiovanni, MD
Introduction/Purpose: Destabilizing injuries to the deltoid ligament have historically relied on radiographic stress examination for diagnosis, with a focus on medial clear space (MCS) widening. Increasingly, Portable ultrasound (P-US) has increasingly been used in the clinical setting, allowing dynamic and non-invasive evaluation at the point of care. This study aims to determine whether the P-US assisted MCS evaluation during the gravity stress (GST), weight-bearing, and external rotation stress test can detect medial side instability in supination-external rotation (SER) type ankle injuries with sequential disruption of the anterior inferior tibiofibular ligament (AITFL) (stage I), the fibula (Weber B fracture) (stage II), the posterior inferior tibiofibular ligament (PITFL) (stage III), the superficial deltoid ligament (stage IVa) and the deep deltoid ligament (stage IVb).
Methods: Ten fresh-frozen cadaveric specimens were used. Medial ankle instability was assessed by the P-US. The assessment was performed with all structures intact and later with sequential transection of the AITFL, Weber-B fibular fracture, the PITFL, the superficial and deep deltoid ligament. In all scenarios, three loading conditions were considered, including the GST, the external rotation stress test (45N), and the simulated weight-bearing (750N). The P-US measurement of the MCS was assessed at the anteromedial aspect and inferomedial aspect of the ankle joint. Three different MCS distances were measured, as demonstrated in Figure 1. To investigate the correlation between the P-US measurements and the staging of SER ankle injuries, a Spearman rank correlation was used. To detect a difference in MCS distances between each injured stage and the intact stage for each stress test, a Wilcoxon signed-rank test was used. P-values were adjusted for multiple comparisons using the Holm- Bonferroni method.
Results: MCS values measured with the P-US increased as the SER ankle injury stage progressed. The Spearman’s rank correlation coefficient ranged from 0.43 to 0.90 (p-values <0.001), which represent moderate to strong positive correlations between the ultrasonographic MCS measurements, and the sequentially created supination-external rotation ankle injury model. All MCS values measured with the P-US during; 1) the GST in neutral ankle position, 2) the GST in plantarflexed ankle position, 3) weight-bearing, and 4) the external rotation stress test, were significantly different between intact stage vs. stage IVb (p ranged from 0.02-0.03). When compared between SER ankle injury stage IVa vs. IVb, the P-US MCS values measured in SER stage IVb were significantly larger (p ranged from 0.005-0.03). Inter-rater (0.97; 95% confidence interval: 0.96-0.98) and intra-rater reliability (0.95; 95% confidence interval: 0.94-0.96) for the P-US MCS measurements were all substantial.
Conclusion: Portable ultrasonography is a feasible tool for diagnosing medial ankle instability in SER ankle injury. The MCS measurements assessed with P-US during the GST, weight-bearing, and the external rotation stress test well correlated with the SER ankle injury staging. Besides, the P-US method is capable of differentiating the SER ankle injury stage IVb from the intact stage, as well as differentiating the stable SER ankle injury stage from the unstable stage. Therefore, the P-US can be a valuable diagnostic tool at the point of care due to its ability to dynamically evaluate suspect medial ankle instability in SER type injury.
DOI: 10.1177/2473011421S00426
Dynamic Portable Ultrasound Cutoff Values for Diagnosing Medial Ankle Instability in Supination External Rotation Ankle Injury: A Cadaveric Study
Jirawat Saengsin, MD; Bart Lubberts, MD, PhD; Pongpanot Sornsakrin, MD; Soheil Soashkani, MD; Gregory R. Waryasz, MD; Daniel Guss, MD, MBA; Christopher W. DiGiovanni, MD
Introduction/Purpose: In the setting of an isolated lateral malleolar fracture, stability is predicated by whether the deep deltoid ligament is intact. Portable ultrasound (P-US) has also been used in the clinical setting, allowing dynamic and non-invasive evaluation at the point of care. This study aimed to determine the cutoff values, as well as its sensitivity and specificity for diagnosing supination external rotation (SER) ankle injury stage IVb (with complete deltoid ligament rupture) using the P-US.
Methods: Ten fresh-frozen cadaveric specimens were used. Medial ankle instability was assessed by the P-US. The assessment was performed with all structures intact and later with sequential transection of the AITFL, Weber-B fibular fracture, the PITFL, the superficial and deep deltoid ligament. In all scenarios, three loading conditions were considered, including the GST, the external rotation stress test (45N), and the simulated weight-bearing (750N). The P-US measurement of the MCS was assessed at the anteromedial aspect and inferomedial aspect of the ankle joint. The P-US measurement of the MCS was assessed by placing the ultrasound probe perpendicularly to the medial gutter at the anteromedial aspect and inferomedial aspect of the ankle joint. Three different MCS distances were measured, as demonstrated in Figure 1. To determine the sensitivity and specificity of the diagnosis of SER injury type IV using the P-US, a receiver operating characteristic (ROC) curve analysis was performed.
Results: The MCS optimal cutoff point to distinguish SER ankle injury stage IVb from other injury stages ranged from 10.4 to 13.8 during the GST, 4.2 to 7.9mm during the weight-bearing stress, and 10.6-17.9mm during the external rotation stress test (Table 1). All P-US cutoff values provided acceptable sensitivity (60-100%), specificity (84-100%), and the area under ROC curve (0.8-1.0) for diagnosing SER ankle injury stage IVb.
Conclusion: MCS cutoff points assessed with the P-US under the GST, weight-bearing, and the external rotation stress test demonstrate high sensitivity and specificity for detecting SER ankle injury stage IVb. The cutoff values vary depending on which loading condition is being used. Additional clinical studies are necessary in the in vivo setting to better understand the implications of these test conditions.
DOI: 10.1177/2473011421S00427
A Systematic Review of Charcot Neuroarthropathy Misdiagnosis
Kiya Shazadeh Safavi, BS; Joseph S. Torian; Raliat O. Jimoh; Daniel Jupiter, PhD
Introduction/Purpose: Charcot neuroarthropathy (CN) is a disabling condition of the foot and ankle with a prevalence of up to 13% of patients with Diabetes Mellitus (DM). In the acute phase, CN presents as a hot, swollen foot, with mild destruction of bone and joint structure. If left untreated it can progress to a chronic stage, with bone and joint destruction, presenting with a classic rocker bottom foot deformity. CN is often misdiagnosed in its acute phase; as a result the diagnosis is usually made once CN has progressed to the chronic phase. This delay causes prolonged treatment regimens and poorer outcomes. This systematic review examines the misdiagnosis of CN and the timeline preceding a correct diagnosis.
Methods: A review of the literature was performed by searching Ovid Medline, CINAHL, and Scopus for articles published within the last five years that contained the terms Charcot and misdiagnosed, antibiotics, deep vein thrombosis, or osteomyelitis. The database search produced 110 articles, once duplicates were removed. 49 articles were screened out by title and 18 were screened by abstract; leaving 43 eligible articles. During the review of the 43 articles an additional 41 articles were added from references because they provided relevant information. Time of symptom onset to diagnosis was calculated in days, with 30 days counting as one month.
Results: In total, 230 patients were included in analysis; of these, 27 (12%) presented with bilateral CN for a total of 257 affected extremities. Type 1 DM was present in 112/210 (53%) of patients, Type 2 DM in 98/210 (47%) of patients, and an unreported DM status in 20/230 (9%) patients. The average time from symptom onset to final diagnosis of CN was 84.8 days, with a range of 25 days to 203 days. Nearly half (110/230; 48%) of the patients experienced CN misdiagnosis. Of these, 99 specific misdiagnoses were reported, with the most common including cellulitis (22/99; 22%), fracture/sprain (18/99; 18%), deep vein thrombosis (13/99; 13%), osteomyelitis (11/99; 11%), and erysipelas and gout (10/99; 10%) each. A total of 42/146 (29%) of patients could recall an incidence of trauma prior to the onset of CN.
Conclusion: A diagnosis of CN should be considered in patients with DM who present with peripheral neuropathy coupled with foot swelling, deformity, ulceration, or difficulty ambulating. This literature review has identified that nearly half of patients with CN are misdiagnosed, and many continue to ambulate and do not receive necessary total contact casting until they are correctly diagnosed later on. Subsequently, awareness of CN and the frequency of misdiagnoses associated with it is critical to preventing treatment delay. Further research is necessary to better clarify why CN is so frequently misdiagnosed and the amount of harm that can result from misdiagnoses.
DOI: 10.1177/2473011421S00428
Industry Payments to Foot and Ankle Surgeons and Their Effect on Total Ankle Arthroplasty Outcomes
Kiya Shazadeh Safavi, BS; Aryan Rezvani; Nicholas Healy, MD; Daniel Jupiter, PhD; Vinod K. Panchbhavi, MD; Cory Janney, MD
Introduction/Purpose: The Centers for Medicare & Medicaid Services (CMS) Open Payments public (OPP) database provides a means for increased transparency of physicians' financial relationships with industry. Total ankle arthroplasty is a procedure with long term clinical implications and variable outcomes published in the existing literature. We compared physician-reported conflict-of-interest (COI) disclosures in Foot and Ankle International (FAI) with CMS database information to evaluate for discrepancies.
Methods: Articles published in FAI reporting clinical outcomes of total ankle arthroplasty from 2015 and 2019 were reviewed. Payment information in the CMS database was cross-referenced with disclosure statements and International Committee of Medical Journal Editors (ICMJE) forms associated with the manuscript. Statistical analysis was performed to determine if industry payments were appropriately disclosed or influenced outcomes.
Results: We reviewed 173 articles pertaining to ankle arthroplasty with 27 meeting inclusion criteria. Of 120 total authors with 98 unique authors, 114 (95%) disclosed appropriately in disclosure statements. Twenty-two papers (82%) had appropriate declarations for the entire manuscript. For the 27 senior authorships, only two discrepancies between manuscript disclosure and the OPP database were noted, showing 13 total disclosures in the OPP database vs 11 disclosed in the manuscript. We found there was no relationship between industry payment and the outcome of the manuscript (P =.725).
Conclusion: The majority of author disclosure statements accurately reflected the OPP data. Additionally, payments were not significantly associated with positive outcomes reported for the specific implant. Overall, authors publishing on ankle arthroplasty in FAI are disclosing appropriately per our review.
DOI: 10.1177/2473011421S00429
Predisposing Factors for 30-Day Complications Following Leg Amputation
Kiya Shazadeh Safavi, BS; Joseph Villarreal; Doha Hussien, BA, BS; Vinod K. Panchbhavi, MD, FACS; Daniel Jupiter, PhD
Category: Trauma; Ankle; Diabetes; Other
Keywords: Clinical Outcomes; Complications; Surgical Site Infection
Introduction/Purpose: While amputation rates and amputation-related morbidity and mortality have been established for select populations, the impact of general demographic factors on postoperative surgical complications remains little studied. This study aims to analyze the influence of numerous demographic variables on specific surgical complications.
Methods: We extracted data from the American College of Surgeons' National Surgical Quality Improvement Program database from 2012 to 2017 and searched for leg amputations using CPT codes 27881, 27882, 27884, and 27886, identifying 4,162 patients. The association of 29 demographic variables with 4 complications (surgical infection, additional service, deep vein thrombosis [DVT], and sepsis) was analyzed using t tests or chi-squared tests. A logistic regression allowed determination of independent risk factors for each outcome, based on results from the bivariate analyses. Variables found to have P < 0.2 on bivariate analysis were subsequently included in the multivariate analysis of the corresponding surgical complication.
Results: Preoperative open, 'contaminated,' or 'dirty/infected' wounds, longer intraoperative times, development of sepsis prior to surgery, and admission of patients directly from home or from another hospital’s emergency room were found to influence postoperative surgical infection rates. An individual’s height, weight, total length of hospital stay, ethnicity, the presence of preoperative open or infected wounds, and wounds classified as 'dirty/infected' preoperatively affected postoperative additional service incidence. Preoperative congestive heart failure and large decreases in body weight, as well as a patient’s total length of hospital stay, influenced postoperative DVT rates. A patient’s preoperative functional heath status, total length of hospital stay, amputations conducted as emergency cases, as well as preoperative acute renal failure, open or infected wounds, sepsis, 'contaminated' or 'dirty/infected' wounds, impacted postoperative sepsis rates.
Conclusion: Understanding these risk factors may allow providers to anticipate and address higher rates of complications in certain patient populations.
DOI: 10.1177/2473011421S00430
Surgical Intervention for 5th Metatarsal Fracture in the Athlete: A Systematic Review
Alan Samsonov; Julia L. Diamond; Grace Randall; Nathaniel P. Mercer; Hugo Ubillus; Eoghan T. Hurley, MB BCh BAO; John G. Kennedy, MD, FRCS(Orth)
Introduction/Purpose: To provide an overview and evaluation of the available evidence on surgical intervention for 5th metatarsal fractures in the athletic population.
Methods: PubMed, Cochrane, and Embase databases were systematically reviewed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The level and quality of evidence (LOE and QoE) were recorded and assessed. Return to sport/play (RTS/RTP), radiographic outcomes, complications, reoperations, and revisions were also evaluated.
Results: Twenty-eight studies were included in this review spanning a total of 761 patients and 765 fractures. The weighted mean age of the study population was 24 years, and the mean follow-up was 33.8 months. Surgical techniques and fracture types varied across the studies, but the majority (18) used internal fixation. Nonunion occurred in 5.8% (11/190) of patients who received a surgical treatment other than internal fixation, but only in 2.3% (11/480) of patients who received surgical treatment with internal fixation. Patients presenting with acute 5th MTP fractures returned to play significantly faster than those with delayed union 5th MTP fractures (7.6 weeks vs. 11.2 weeks) (p<.001). However, reoperation/revision rates were highest in patients who received surgery for acute 5th MTP fracture, of which 8.3% (16/192) of patients with acute fracture underwent reoperation or revision after surgical management.
Conclusion: The current systematic review showed favorable outcomes for the surgical treatment of 5th MTP fractures in the athletic population. Athletes who underwent surgical treatment for an acute 5th MTP fracture returned to play at a faster rate compared to other fracture types but were associated with a high complication rate and a higher reoperation and revision rate.
DOI: 10.1177/2473011421S00431
Location of the Ankle Osteochondral Lesion of the Talus (OLT) Corresponding to the Anatomical Axis of the Tibia (Loading Axis) Crosses the Ankle Joint
Maxwell L. Sandberg; Seyed Alireza Mirghasemi, MBBS; Zachary Troiani; Zachary M. Vaupel, MD; Paul T. Fortin, MD
Category: Ankle; Sports
Keywords: Cartilage; OLT; Joint Preserving Surgery
Introduction/Purpose: studies demonstrated that mechanical axis alignment affects the clinical outcome of the chondral repair surgery in the knee. Reduction in stress concentration around chondral defects with HTO has been found to favor cartilage repair in knee surgery. this study aimed to determine the relationship between the tibia mechanical axis alignment and OLT size and location.
Methods: 57 patients that underwent OLT repair between 2016-2020 were included. X-rays and MRIs of the ankle were used to collect data on OLT in the study group. X-ray measurements included (a)-measured as distance from where vertical line through center of tibia crosses to center the talar joint in AP view (medial, lateral), (b)- measured as distance from where vertical line through center of tibia crosses to the center talar body in lateral view (ant, post). The coverage angle, TLS, TAS, MA, TI, TTI angles were measured. MRI measurements included distance of the edge of the OLT lesion from the center of the talar surface, in three plans, and for location of the OLT lesion based on the 9-zone grid system.
Results: 37.3% of these patients had the mechanical axis of the joint cross posterolaterally, 15.6% anteromedially, 5.9% anterolaterally, and 3.9% posteromedially. 33.3% had the mechanical axis cross posteriorly along the midline of the lateral axis. Using the 9-zone grid to localize lesion location, lesions were most often seen in location 6 (37.3%), location 7 (21.6%), location 9 (21.6%), and location 4 (19.6%). Of note, 36.8% of patients with a posterolateral axis had lesions at location 6 and 26.3% at location 9. For patients with poster joint axis along the midline of the lateral axis, 47.1% had lesions at location 6 and 23.5% at location 7. There is a correlation between Lesion Surface Area and axis location in the AP view (Correlation coefficient: 0.301, P Value: 0.023). we found a significant difference for coverage angle (P<0.001), TLS (P<0.001), and TTI (P<0.001) for different groups.
Conclusion: The significant correlation shows that the farther medial the location of the axis crosses the joint, the larger the surface area of the lesion. there is no significant difference between lesion length or area and location.
DOI: 10.1177/2473011421S00432
Symptomatic Hallux Valgus Deformities and 1st Tarsometatarsal Joint Morphology
Robert D. Santrock, MD; Paul Dayton, MS,DPM; Jody McAleer, DPM, FACFAS; Dane K. Wukich, MD; Daniel J. Hatch, FACFAS; Daniel C. Farber, MD; Abdi Raissi, MD; Deidre Kile
Category: Bunion; Midfoot/Forefoot
Keywords: Hallux Valgus; Bunion; TMT
Introduction/Purpose: The pathogenesis of the hallux valgus deformity is still poorly understood. Consistent observations of the 1st tarsometatarsal (TMT) joint as the CORA of hallux valgus raises questions about pathology associated with that joint. Mason and Tanaka studied the 1st TMT joint in cadaveric specimens in 2012, observing three morphological subtypes to the 1st cuneiform articular surface. They noted that specimens with hallux valgus had either a unifacet (37%) or bifacet (63%) appearance, where normal feet had a trifacet appearance. This observation suggests that these bony differences may be responsible for 'instability' that generates the metatarsal deviation into varus, and thus the development of hallux valgus. If true, surgical corrections for hallux valgus deformity should address this TMT joint pathology.
Methods: This study was designed to correlate the morphological differences of the TMT joint with symptomatic hallux valgus patients who are seeking surgery. The hypothesis was that the hallux valgus patients would show a majority unifacet and bifacet morphology and have an inclination towards unifacet in younger patients and patients with a larger deformity. The cohort of patients who are in the registered longitudinal study Align3D had their TMT joints harvested in a standard fashion as part of their surgical treatment. These specimens were analyzed for the number of facets by the surgeon at the time of their surgical procedure. This cohort therefore only includes symptomatic hallux valgus patients and eliminates hallux valgus associated with metatarsus adductus. Standard weight-bearing x-rays taken pre-operatively were analyzed for severity of deformities. Functional and Patient Reported Outcome measures were obtained pre-operatively and post-operatively.
Results: In this study we observed 143 specimens. Unifacet was observed in 116 specimens (81.1%), bifacet was observed in 26 specimens (18.2%), and trifacet was observed in 1 specimen. Neither X-Ray findings, age, nor Functional Scores suggested a trend in severity in relation to morphological type. Mason & Tanaka’s cadaveric study was limited in some respects because of the hardening effect of formaldehyde preservations. Their study represented an elderly population, mean age 86 years, whereas this study represented a much younger population, mean age 40.6, in which patients were able to participate in both X-Ray and clinical scoring. To the best of our knowledge, this is the first time that morphology of the TMT joint has been studied in symptomatic hallux valgus patients who underwent surgery.
Conclusion: Symptomatic hallux valgus deformities are associated with a higher likelihood of having a unifacet morphology than previously reported in cadavers (81.1% vs 37%). This morphology may predispose patients to decreased stability resulting in more symptomatic deformity. The number of facets does not seem to correlate with severity of deformity on X-Ray evaluation, nor does it correlate with age. However, the younger age group in our study as compared to Mason and Tanaks’s study suggests that morphological differences may even be congenital, leading to later development of deformity.
DOI: 10.1177/2473011421S00433
Unsolicited Patient Complaints in Orthopaedic Surgery: An Analysis Utilizing a Large National Database
Shumaila Sarfani, MD
Category: Other
Keywords: Practice Models; Health Care; Practice Models
Introduction/Purpose: Unsolicited patient complaints (UPCs) about surgeons have been shown to correlate with surgical complications and malpractice claims in several specialties. Analysis of UPCs in orthopaedics is limited and using large national databases of UPCs may prove informative to orthopaedic providers and administrators. Our purpose was to 1) Evaluate the differences in the number and distribution of UPCs between orthopaedic surgeons as compared to other surgeons, and non- surgeons. 2) Describe the distribution of UPCs among orthopaedic sub-specialties. 3) Assess for clinical characteristics that may be associated with UPCs.
Methods: Patient complaint reports recorded at 36 medical centers between January 1st, 2015 through December 31st, 2018 were coded using a previously validated coding algorithm, PARS® (Patient Advocacy Reporting System®). We (1) evaluated the distribution of UPCs across orthopaedic surgeons, (2) compared orthopaedic surgeons’ UPC distribution with those of other surgeons and non-surgeons, and (3) analyzed differences in complaint types across orthopaedic sub-specialties.
Results: A total of 33,174 physicians had four consecutive years of data across the 36 nation-wide participating medical centers and met other inclusion criteria, including 1,148 orthopaedic surgeons, 6,747 other surgeons, and 25,279 non-surgeons. Orthopaedic surgeons experienced more UPCs per physician than non-orthopaedic surgeons and non-surgeons (5 vs. 2 vs. 1 respectively, p<0.05); the top 20% of orthopaedic surgeons with UPCs accounted for half of all complaints about orthopaedic surgeons received by the organizations in the study. The sub-specialties that had significantly more UPCs compared to general orthopaedic surgeons were Foot and Ankle (OR 2.6 [1.4-4.6], p=.002), followed by Adult Reconstruction (OR 2.2 [1.3-3.8], p=.002), Spine [OR 2.2 (1.3-3.8), p=.005), and Trauma (OR 2.2 [1.2-4.0], p =.01). Surgeons in the midwest were less likely to get complaints that surgeons in the northeast and sex was not a predicting factor.
Conclusion: Orthopaedic surgeons receive comparatively more UPCs than other surgical and non-surgical specialties. Among orthopaedic surgeons, the subspecialties of Foot and Ankle, Adult, Reconstruction, Spine, and Trauma received the most UPCs. As increased UPCs have been linked to higher risk of malpractice claims, individual orthopaedic surgeons with high numbers of UPCs may benefit from being made aware of their elevated risk status in ways that invite reflection on underlying causes.
DOI: 10.1177/2473011421S00434
Open Ankle Fractures in the Elderly: Predisposing Factors and the Associated Mortality
Haggai Schermann, MD, MPH; Takahisa Ogawa, MD, MPH; Bart Lubberts, MD, PhD; Gregory R. Waryasz, MD; Philip Kaiser, MD; Christopher W. DiGiovanni, MD; Daniel Guss, MD, MBA
Category: Ankle; Trauma
Keywords: Ankle Fracture; Trauma; Diabetes
Introduction/Purpose: Previous studies raised awareness of high mortality associated with open ankle fractures in elderly patients. Mortality among this patient population has been reported about 23-27% during the first year postoperatively. The purpose of this study was 1) to investigate the association between patient factors and occurrence of open ankle fractures and 2) to quantify the risk of mortality associated with open ankle fractures.
Methods: This is a retrospective cohort study of 1,045 patients 65 years and older, with ankle fractures, who were operated between 2010 and 2020. Background medical data included patient age, gender, language, race, fracture type and comorbidities. Case-control approach and logistic regression analysis were used to identify risk factors for open fractures. Propensity score matching and survival analysis were used to measure the hazard of mortality with ankle fractures.
Results: There were 128 (12.2%) patients with open ankle fractures in this cohort. Patients with open ankle fractures higher odds of belonging to the age group of 70 to 79 years (OR=1.7, p=0.03) and 80 to 89 years (OR=1.8, p=0.04), having a diagnosis of hypertension (OR=2, p=0.006) and chronic kidney disease (OR=2.9, p=0.005), and smoking (OR=1.7, p=0.049). Open ankle fractures were associated with higher risk of mortality (HR=1.7, p=0.03). Other variables related to mortality in these patients were ischemic heart disease (HR=1.9, p=0.009), chronic kidney disease (HR=1.99, p=0.02), peripheral vascular disease (HR=1.8, p=0.03) and diabetes (HR=2.1, p=0.006).
Conclusion: This study identifies older patients with comorbidities as having higher risk of open, compared to closed ankle fracture. Open ankle fractures are associated with higher mortality in this population, possibly indicating the need for control of comorbidities, reduction of fall risk and barrier protection as means of primary prevention.
DOI: 10.1177/2473011421S00435
Initial Experience with a Bioresorbable Polymer Anchor
Adam P. Schiff, MD; Jayanth Kumar; Robert R. Burnham; Kamran S. Hamid, MD, MPH; Michael S. Pinzur, MD
Introduction/Purpose: Anchors are frequently used in reconstructive orthopedic surgery to achieve fixation of soft tissue to bone. Anchors vary with respect to material composition, configuration, and methods of fixation at the site of attachment. The fixation component of anchoring devices has generally evolved from metal-fabricated implants to various types of bioresorbable anchors. The SonicAnchorTM (Stryker, Kalamazoo, MI USA) polymer implant provides a unique form of anchor fixation using SonicFusionTM technology to achieve interdigitation within cancellous bone while being radiolucent and providing a small footprint.
Methods: During a four-year period, 116 patients underwent a reconstructive orthopedic foot and ankle surgical procedure with the use of at least one bioresorbable polymer anchor (SonicAnchor implant). There were 59 males and 57 females, with an average age of 42 years (range: 12-83 years).
Results: A total of 233 bioresorbable anchor (SonicAnchor) implants were used in 116 patients. Of the 116 patients, 108 (93.1%) achieved successful clinical healing of their surgery at their most recent follow-up. The average follow-up duration was 309 days (range: 14-1,429 days). Eight (6.9%) patients were lost to follow-up prior to clinical healing. Two (1.7%) patients underwent reoperation. Also, 65 (56%) patients had at least six months of follow-up and 36 (31%) had at least one year of follow-up.
Conclusion: This preliminary clinical trial of patients undergoing soft tissue repair or reconstruction with a bioresorbable polymer appears to perform comparably to other commercially available devices. The lack of adverse events, mechanical failures, or infections further supports the safety of this device.
DOI: 10.1177/2473011421S00436
The Incidence of Deltoid Ligament Interposition in Bimalleolar Equivalent Ankle Fractures
Adam P. Schiff, MD; Jayanth Kumar; Robert R. Burnham; Kamran S. Hamid, MD, MPH; Michael S. Pinzur, MD
Introduction/Purpose: When performing surgical fixation of bimalleolar equivalent ankle fractures, there has been considerable debate regarding fixation of the deltoid ligament. Many surgeons would agree that deltoid ligament repair should be undertaken if there is radiographic evidence of medial interposition of the deep deltoid. The incidence of deltoid ligament interposition has not been addressed in current literature. This study aims to assess the incidence of deltoid interposition in bimalleolar equivalent ankle fractures to provide further guidance on the importance of acute deltoid ligament repair.
Methods: Over a five year time frame, 49 bimalleolar equivalent ankle fractures were repaired in 30 males and 19 females with a mean age, 37 (15-73) years. There was no exclusion criteria and patients were consecutively enrolled if they sustained a bimalleolar equivalent ankle fracture.
Results: During this time frame, 49 patients who sustained a bimalleolar equivalent ankle fracture underwent surgical fixation with routine repair of the deltoid ligament. 18 patients (36.73%) had deltoid interposed within the medial gutter. 13 patients (26.53%) had an osteochondral defect.
Conclusion: The incidence of deltoid interposition seen with medial exploration within this cohort was 37%. While the benefits of deltoid ligament repair are still controversial, persistent medial gutter soft tissue interposition could lead to symptoms of impingement or even result in persistent medial widening. This study supports increased scrutiny to the relationship of the medial gutter and deltoid ligament in acute bimalleolar equivalent ankle fractures.
DOI: 10.1177/2473011421S00437
The Potential of Topical Antibiotic Powder to Decrease Infection Rates in Total Ankle Arthroplasty
Lew C. Schon, MD; Bonnie Y. Chien, MD; Naudereh B. Noori, MD; Jonathan Day; Zijun Zhang
Introduction/Purpose: Periprosthetic infection is a devastating complication in total ankle arthroplasty (TAA). Measures that can reduce or eliminate infection occurrence are warranted for further investigation, particularly if they also minimize added costs, operative time or potential adverse effects. There remains insufficient evidence to show definitive benefits or risks associated with use of local antibiotics such as vancomycin for infection prevention. The purpose of this study was to determine the effects of topical vancomycin powder application in TAA and whether it may decrease infection rate in the subacute postoperative period. To our knowledge, this is the first comparative study in a general population undergoing TAA.
Methods: A retrospective study was conducted based on a consecutive series of patients who underwent TAA performed by a single senior surgeon. The control group without vancomycin powder was matched to the study group that received application over the implants prior to closure, which was based on when the surgeon transitioned to usage in all patients. Various demographic data for the patients was collected. Only patients with a minimal follow up of 80 days were included in order to capture the perioperative period of infection. Infection rate was based on a definition of deep infection necessitating inpatient hospitalization for IV antibiotics and/or surgical intervention. The associations of various demographic factors and vancomycin application with infection rate were calculated with chi square and odds ratio. Significance level was set to 0.05.
Results: A total of 252 patients (n=103 without, and 149 with vancomycin powder) were included in the study. The overall infection rate was 3.2%, which was not correlated with a history of diabetes, BMI, additional concurrent surgery, or age, but was associated with current positive smoking status (p=0.03). The infection rates between the groups that received or did not receive vancomycin powder were not statistically significantly different (2.7% vs 3.9%, respectively, p=0.59). The odds ratio (OR) of infection with vancomycin powder was not statistically significant either, at OR=0.68 (95% CI 0.17-2.81). However, the vancomycin group did have a significantly higher number of patients with previous wound issues (12 vs. 2; p=0.04) and infection (7 vs. 0; p=0.04) as well as concomitant surgeries (81 vs. 41; p=.02).
Conclusion: The consequences of periprosthetic TAA infection are substantial, and the risks should be mitigated. Although this study did not detect a statistically significant difference in infection rates between patients who received or did not receive vancomycin powder, there was a trend towards risk reduction by about 30%. In addition, current smoking was found to be significantly associated with higher rates of infection and smoking cessation can serve as another point of intervention. As the complexity of patient factors and indications for performing total ankle arthroplasty expand, vancomycin powder offers a relatively cost-effective, safe, and convenient option to potentially reduce infection.
DOI: 10.1177/2473011421S00438
Comparing Traditional Lapidus to Newer Triplane Methods for Correction of Hallux Valgus
Kyle M. Schweser, MD; Anthony Bitar, BS; Jacob W. Cebulko; Kyle Fiala, DPM; Benjamin Summerhays, DPM
Category: Bunion; Midfoot/Forefoot
Keywords: Hallux Valgus; Lapidus; TMT
Introduction/Purpose: Correction of hallux valgus is a common procedure for foot and ankle specialists. Advances in the understanding of this deformity has shifted surgical correction back to the first tarsometatarsal joint. Traditional Lapidus methods had a low recurrence rate and 10% nonunion rate. Recent developments in the correction of hallux valgus have centered on triplane correction utilizing proprietary systems. These systems are effective at obtaining, and maintaining, correction. However, they are expensive and there is a paucity of unbiased literature comparing it to traditional methods. This study aims to evaluate radiographic outcomes and complications of patients undergoing traditional Lapidus fixation to triplane corrective procedures. Our hypothesis is that overall correction will be obtained and maintained at a similar rate, with no difference in overall complications.
Methods: After IRB approval, a total of 275 patients over the age of 18 were identified who underwent a total of 294 procedures for first tarsometatarsal joint fusion for hallux valgus correction between February 2010 to August 2020. A retrospective chart review was then performed dividing patients into two groups: traditional Lapidus fixation and triplane correction methods. A total of 191 patients underwent traditional Lapidus, and 103 underwent triplane correction. Charts were evaluated for complications that required a return to the operating room, specifically nonunion, loss of correction, infection, and hardware removal. AP foot radiographs were then reviewed from the patient’s preoperative visit, immediate postoperative, and final follow up. On each film, the first intermetatarsal angle (IMA) was then measured by two independent observers. Each IMA was recorded and overall surgical correction, final correction angle, and maintenance of correction were calculated.
Results: Comparing triplane correction to traditional Lapidus cohorts, there was no difference in age (50.6 vs 48.9 years, p=0.39), initial deformity (14.66 vs 15.61 degrees, p=0.05), or x-ray follow up (229 vs 393 days, p=0.23). When comparing IMA correction, there was no difference in initial amount of correction (11.2 vs 11.4 degrees, p=0.58) or final correction angle (5.22 vs 5.66 degrees, p=0.05). Comparing complications, there was no difference in secondary surgery rates (9/103, 8.7% vs 11/191, 5.76%, p=0.34), especially nonunions/loss of correction (4.85% vs 2.62%, p=0.32). Comparing number of cases that experienced an increased IMA of more than 5 degrees from post-op to final, there was no difference (10/103, 9.71% vs 12/191, 6.29%, p=0.35). Finally, there was no difference in infection (p=0.13) or implant removal (p=0.43).
Conclusion: When comparing radiographic correction of IMA, maintenance of correction, and secondary surgery rates, there appears to be no difference between triplane correction methods and traditional Lapidus procedures. Recent evidence in the literature supports correction of hallux valgus through the TMT joint, with a subsequent increase in proprietary reduction and fusion methods. These proprietary methods are expensive, and according to this study, offer no improvement over traditional, less expensive methods in terms of IMA correction and need for secondary surgery. Further study is needed to assess patient reported outcomes for each and potential radiographic findings that may suggest risk of recurrence.
DOI: 10.1177/2473011421S00439
Radiographic Evaluation of Isolated Continuous Compression Staples for Midfoot and Chopart Arthrodesis
Kyle M. Schweser, MD; Kevin Horner; Kyle Fiala, DPM; Benjamin Summerhays, DPM
Introduction/Purpose: The use of continuous compression implants (nitinol staples) in orthopaedic surgery has increased secondary to advances in metal alloy engineering. Biomechanical studies provide useful data supporting the theoretical use of nitinol staples in the foot and ankle; however, clinical data is limited. There are several advantages of nitinol staples, including a lower profile when compared to traditional fixation methods. They are easy to apply and take up a smaller footprint than most plating techniques, thus decreasing surgical time and dissection. Additionally, continuous compression across the fusion site is maintained, as opposed to lag screw fixation. The purpose of this study was to determine the overall effectiveness, clinically and radiographically, of continuous compression implants (nitinol staples) to achieve stable arthrodesis in the midfoot and Chopart joints.
Methods: A retrospective chart review was performed on 18 patients (37 joints) who underwent arthrodesis of the midfoot or Chopart joints utilizing isolated continuous compression implants between January 2017-December 2019. The primary outcome variable was radiographic evidence of arthrodesis on x-ray. X-rays were independently reviewed by three board-certified foot and ankle surgeons. All investigators were blinded towards the x-rays, and x-rays were randomized in terms of timing from surgery. Each investigator reviewed digital radiographs independently and recorded their radiographic finding responses. Joints were deemed fused if greater than 50% of the joint contained bridging bone radiographically. A partial fusion was defined as some bridging bone, but less than 50% of the joint involved, and nonunion was defined as no arthrodesis seen radiographically, broken hardware, or loss of reduction. Smokers and diabetics represented 22% and 11% of the patient population, respectively.
Results: Radiographic union was seen in 88.8% of TMT joints (16/18) and 83.3% of midfoot joints overall (20/24). Nonunion rates were 11.2% (2/18) and 16.6% (4/24) respectively. Diabetes was associated for 50% (3/6) of nonunions. Mean time-to-fusion for TMT joints was 60 days. In Chopart joint fusions, nonunion rate was 46% (6/13), 2/6 (33%) were smokers. Overall, diabetes and smoking was associated with 40% (4/10) of all nonunion cases. TMT joint fusions had a significantly lower proportion of nonunion rates than hindfoot fusions (p=0.043). Radiographic Interobserver reliability was moderately strong between reviewers. Clinically, Chopart joint fusion patients had a significantly longer time course to weight bearing (p = 0.028). 8% (4/50) had broken hardware, all in nonunions, 75% (3/4) occurring in Chopart joints.
Conclusion: Isolated nitinol staples are a viable option for midfoot arthrodesis, especially TMT joints, and offer multiple advantages when compared to traditional fixation methods. Staples are lower profile, eliminating hardware irritation and potential secondary surgeries, are technically less demanding, and time of application is decreased when compared to other methods. They offer the benefit of continuous compression of the fusion site, as well, and are rigid enough to maintain reduction. However, Chopart joints may require a more rigid fixation than CCI staples can provide, given the higher nonunion rate, and caution should be exercised in diabetics and smokers.
DOI: 10.1177/2473011421S00440
Accessory Cuboid Facet Associated with Calcaneonavicular Coalitions
Daniel J. Scott, MD, MBA; Anthony Riccio; Yassine Kanaan; Jacob R. Zide, MD
Category: Hindfoot; Other
Keywords: Tarsal Coalitions; Bone Morphology; CT
Introduction/Purpose: Though resection and soft tissue interposition is the mainstay of surgical treatment for symptomatic calcaneonavicular coalitions (CNCs) that fail conservative treatment, some consternation exists as to balancing adequacy of resection with violation of adjacent talonavicular and calcaneocuboid (CC) articulations. As better understanding of nearby articular anatomy might be helpful in determining extent of resection, this study aims to identify differences in the anatomy of the CC articulation between feet with and without CNCs.
Methods: A retrospective radiographic analysis of patients with symptomatic CNCs presenting to a single tertiary care pediatric hospital from 2010-2019 was performed. Patients without computed tomographic (CT) or magnetic resonance imaging (MRI) were excluded. Using either CT or MRI and standardized anatomic landmarks, the length and morphology of the calcaneal and cuboid articular surfaces were documented at the CC joint. When bilateral imaging was available in patients with a unilateral coalition, measurements were also made on the uninvolved side to provide a cohort of normal controls for comparison.
Results: 81 CNCs in 55 patients were identified along with18 normal feet. Mean age was 11.7 years at the time of advanced imaging. In the coalition group, an accessory cuboid facet was identified articulating with the calcaneal portion of the coalition in 61/81 (75.3%) feet. The mean total length of the cuboid articular surface measured 28.6 mm (range, 22.4-34.9 mm). The average length of the accessory facet was 10.6 mm (range, 6.0-15.5 mm) while the length of the primary cuboid articulation with the calcaneus was 15.9 mm (range, 6.4-23.2 mm). Thus, the accessory facet comprised 37.2% of the cuboid articular surface in these patients. Patients without CNCs had a significantly larger primary cuboid articulation with the calcaneus of 21.6 mm (p<0.0001). An accessory cuboid facet was identified in only a single foot in the normal cohort.
Conclusion: An accessory cuboid facet is present in over 75% of patients with CNCs and comprised nearly 40% of the proximal cuboid articular length. Moreover, significant differences in the shape of the cuboid portion of the CC joint were present in feet with and without CNCs. This information may be useful when planning the extent of CNC surgical resection as including the coalition side of the accessory articulation may have value in restoring hindfoot motion.
DOI: 10.1177/2473011421S00441
Lesser Tarsal Metatarsal Joint Fusion Using Nitinol Staples, Bone Marrow Aspirate Concentrate and a Calcaneal Bone Dowel: A Retrospective Comparative Analysis
Jared Scott; Jay Thompson; Mark Johnson, DO; Michael Anderson, BS; Bryan J. Hawkins, MD
Category: Midfoot/Forefoot; Lesser Toes
Keywords: Arthrodesis; Bone Block Graft; BMAC
Introduction/Purpose: Estimates suggest nonunion rates following lesser tarsometatarsal (TMT) fusion are up to 11.4%. Various techniques have been employed to improve fusion rates; however, none have shown significant improvement compared to other techniques. Autologous bone dowels, bone marrow aspirate concentrate (BMAC) and continuous compression devices (CCDs), such as nitinol staples, have each shown promising fusion rates in orthopedic literature. There is limited data that suggests using these techniques in conjunction with one another has been successfully employed in the fusion of lesser TMT joints. The aim of this study was to describe our technique using autologous calcaneal bone graft, CCDs and BMAC for lesser TMT fusion and to investigate whether this method improves fusion rates and decreases time to fusion in comparison to traditional constructs.
Methods: All patients undergoing arthrodesis of the lesser (2nd/3rd) TMT joints from January 2015 to January 2020 were identified. Exclusion criteria included inadequate clinical or radiographic follow-up, those with only 1st TMT joint arthrodesis, and those less than 18 years old. Chart review allowed patient demographics, risk factors and surgical approach to be identified. Twenty patients (28 lesser TMT joints) treated with arthrodesis by the senior surgeon met inclusion criteria. These patients were then divided into two groups: 1) novel treatment (Nitinol staple, BMAC and calcaneal dowel) and 2) traditional treatment (compression plate and screw construct). We then assessed for radiographic union, time to union and complications.
Results: All lesser TMT joints in the novel treatment arm went on to successful clinical and radiographic fusion. The radiographic union rate of the traditional treatment arm was 92% (P=.08). Overall time to fusion was 56 and 82 days for the novel and traditional constructs respectively (P <.05). All patients, regardless of construct, had returned to full weight bearing and maintained hardware at most recent follow-up (minimum 6 months).
Conclusion: Continuous compression devices such as the nitinol staple and use of biologic adjuvants appear to decrease nonunion rates and significantly shorten overall time to fusion in lesser TMT joints. Further investigation towards identifying patient specific factors for nonunion is warranted.
DOI: 10.1177/2473011421S00442
Lateral Dorsal Cutaneous Nerve and Anastomotic Branch to the Intermediate Dorsal Cutaneous Nerve: A Review of Cadaveric Data and Comparison with 3 Tesla MRI
Vrajesh J. Shah; Brendon Mitchell; Claudio B. Ghetti; Brady K. Huang; William Kent; Ian M. Foran, MD
Category: Other; Hindfoot
Keywords: Sinus Tarsi Approach; Subtalar Fusions; Calcaneal Fractures
Introduction/Purpose: The lateral dorsal cutaneous nerve (LDCN) and anastomotic branch to the intermediate dorsal cutaneous nerve (AICN) can be injured during foot and ankle surgery. Cadaveric specimen studies are limited by small sample size.1-11 We sought to use high-field 3-tesla (3T) magnetic resonance imaging (MRI) to examine a significantly larger cohort and obtain a more representative sample of the course of the LDCN and AICN. A more generalizable understanding of the course and position of these structures will aid surgeons intraoperatively in avoiding iatrogenic injury when performing the sinus tarsi approach, as well as during percutaneous intramedullary fixation of the 5th metatarsal.
Methods: High-field 3T MRI studies performed between January 2015 to January 2020 were reviewed. Three blinded reviewers at a single academic center measured the coronal distances of LDCN and AICN from the fifth metatarsal styloid (5MS). Intraclass correlation coefficients (ICC) were calculated to assess reviewer reliability. Foot and ankle MRIs with major structural abnormalities, such as tumor or the presence of hardware, were excluded.
Results: A total of 125 foot and ankle 3T MRIs were identified. Intraclass correlation coefficient was excellent at 0.87 for LDCN to 5MS and 0.88 for AICN to 5MS. The mean distance of the LDCN to the 5MS was 0.8 cm (range 0.3-1.4 cm, CI 0.8-0.8 cm) and that from the AICN to the 5MS was 2.1 cm (range 1.6-3.2 cm, CI 2.0-2.2 cm. Height had no significant correlation with the nerves' distance from bony landmarks with r values of 0.14 and 0.29 for the LDCN and AICN, respectively. Similarly, we did not find BMI to significantly correlate, with r values of 0.10 and 0.30 for the LDCN and AICN, respectively.
Conclusion: Our study demonstrated the LDCN and AICN can be found on average 0.8 cm and 2.1 cm, respectively, above the 5MS with no clear association to patient height or BMI. Literature studying the range of distances the LDCN is found from the 5MS is scarce, but one study noted the range to be 0.7-1.2 cm, which is significantly smaller than our range of 0.3-1.4 cm.3 To our knowledge, our study is first to note the range of distances the AICN can be found from the 5MS, which is 1.6-3.2 cm.
DOI: 10.1177/2473011421S00443
Risk of Injury to the LDCN and IACN During Surgical Approaches to the Foot and Ankle: an Anatomical Study using 3-Tesla Magnetic Resonance Imaging
Vrajesh J. Shah; Brendon Mitchell; Claudio B. Ghetti; Brady K. Huang; William Kent; Ian M. Foran, MD
Category: Ankle; Other
Keywords: Calcaneal Fractures; Subtalar Joint Arthritis; Sinus Tarsi Approach
Introduction/Purpose: The dorsomedial branch of the lateral dorsal cutaneous nerve (dmLDCN) and anastomotic branch to the intermediate dorsal cutaneous nerve (AICN) are at risk during foot and ankle surgery. Prior studies of the distal sural nerve on cadaveric specimens are limited by small sample size.1-7 We sought to use high-field 3-tesla (3T) magnetic resonance imaging (MRI) to examine a significantly larger cohort and obtain a more representative sample of the course of the dmLDCN and AICN. A more generalizable understanding of the course and position of these structures will aid surgeons intraoperatively in avoiding iatrogenic injury when performing the dorsomedial approach to the fifth metatarsal, as well as the sinus tarsi and extended sinus tarsi approaches for calcaneal fractures and subtalar/calcaneocuboid fusions.
Methods: High-field 3T MRI studies performed between January 2015 to January 2020 were reviewed. Three blinded reviewers at a single academic center measured the coronal distances of dmLDCN and AICN from the fifth metatarsal styloid (5MS). Intraclass correlation coefficients (ICC) were calculated to assess reviewer reliability. We analyzed the upper and lower quartile ranges to evaluate the risk of iatrogenic nerve injury with standard surgical approaches.
Results: A total of 125 foot and ankle 3T MRIs were measured. Intraclass correlation coefficient was excellent at 0.87 for dmLDCN to 5MS and 0.88 for AICN to 5MS. 1st and 4th quartile range for the dmLDCN to the 5MS was 0.5-0.7 cm and 0.9-1.4 cm, respectively. 1st and 4th quartile range for the AICN to the 5MS was 1.6-1.9 cm and 2.3-3.2 cm respectively. The AICN was identified in 47.2% of the images.
Conclusion: The dmLDCN, AICN, and SN are vulnerable to iatrogenic injury during surgical approaches to the fifth metatarsal and calcaneus. Our 1st quartile range for the dmLDCN to the 5MS of 0.5-0.7 cm suggests that nearly 25% of our values measured by 3T MRI were lower than the reported range of 0.7-1.2 cm by Fansa, suggesting iatrogenic injury to the dmLDCN with the 'high and inside approach' to the fifth metatarsal may be higher than previously thought. The 4th quartile range of the AICN’s distance from the 5MS of 2.3-3.2cm places it at risk with the sinus tarsi approach.
DOI: 10.1177/2473011421S00444
Defining Normal Values for Distal Tibiofibular Syndesmotic Space with and without External Rotation Stress: A Prospective Study with Volunteer Controls
Alan G. Shamrock, MD; Jonathan Day; Kieran Dowley; Nacime S. Mansur, MD; Kevin N. Dibbern, PhD; Cesar de Cesar Netto, MD, PhD; Martin J. O'Malley, MD
Introduction/Purpose: The diagnosis and treatment of distal tibiofibular syndesmosis (DTFS) injury can be challenging, especially in cases of subtle instability that may be masked on two-dimensional conventional radiographs. Weightbearing computed tomography (WBCT) has recently emerged as a useful diagnostic tool allowing direct assessment of distal tibiofibular widening. Needle-Arthroscopic Ankle Lateral Ligament Repair Using a Knotless Suture AnchorArea measurements of the distal tibiofibular incisura assessed one centimeter proximal to the ankle joint have been proposed as an accurate diagnostic tool to differentiate stable and unstable DTFS, however the literature lacks information regarding normal DTFS area measurements in asymptomatic ankles. The purpose of the current study was to examine and report normal threshold values for DTFS area measurements in a cohort of healthy volunteers, assessing the ankles in natural weightbearing position and under external rotation stress.
Methods: In this prospective study, we enrolled twenty-five healthy volunteers without a history of DTFS injury or high ankle sprain, previous foot and ankle surgery, or current ankle pain. Study participants underwent bilateral standing non-stress and external rotation stress WBCT scans. On non-stress WBCT scans, subjects stood with feet shoulder width apart in a natural, upright position with body weight evenly distributed. For external rotation stress images, patients were instructed to position their lower extremity in maximal internal rotation while the foot was held in a fixed plantigrade position. The DTFS area (mm2) was semi-automatically quantified on axial-plane WBCT images one centimeter proximal to the apex of the talar dome using dedicated software (Figure 1). Syndesmosis area values were compared between non-stressed and stressed ankles, as well as left and right ankles. Statistical analysis was performed utilizing independent t-tests/Wilcoxon analysis with statistical significance defined as p<0.05.
Results: The study cohort consisted of 50 ankles in 25 patients (12 males, 48%) with a mean age of 28.7+9.3 years. In the unstressed ankle, the mean pooled DTFS area was determined to be 99.1+2.8 mm2. The mean syndesmosis area of unstressed left ankles in the cohort was 96.5+4.0 mm2, while unstressed right ankles had a mean area of 101.6 mm2 (p=0.378). With external rotation stress, the DTFS area of left ankles (mean difference 1.2 mm2; CI: -9.8-11.8; p=0.765), right ankles (mean difference -3.1 mm2; CI: -16.1-6.6; p=0.453), and all ankles (mean difference -1.2 mm2; CI: -12.4-9.3; p=0.775) remained similar.
Conclusion: This is the first study to assess standing WBCT DTFS area measurements in a cohort of volunteer controls, with and without external rotation stress. We found a mean DTFS value of 99+-18.8 mm2. We also observed that in normal ankles with expected intact ligaments, external rotation stress did not result in significant widening of the DTFS space. Our hope is that the results of this study can be utilized in the literature as normal threshold values for DTFS area measurements, fostering additional investigations of patients with suspected and confirmed DTFS instability.
DOI: 10.1177/2473011421S00445
Utilization of Arthroscopy During Ankle Fracture Fixation among Early Career Surgeons: An Evaluation of the American Board of Orthopedic Surgery Part II Database
Alan G. Shamrock, MD; Christopher N. Carender, MD; Annunziato Amendola, MD; Natalie Glass, PhD; Kyle R. Duchman, MD
Category: Ankle; Arthroscopy; Trauma
Keywords: Ankle Arthroscopy; Ankle Fracture; ORIF
Introduction/Purpose: Rotational ankle fractures are common injuries associated with high rates of intra-articular injury. Traditional ankle fracture open reduction and internal fixation (ORIF) techniques provide limited capacity for evaluation of intra- articular pathology. Ankle arthroscopy represents a minimally invasive technique to directly visualize the articular cartilage and syndesmosis while aiding with reduction and allowing joint debridement, loose body removal, and treatment of chondral injuries. The purpose of this study was to evaluate temporal trends in concomitant ankle arthroscopy during ankle fracture ORIF surgery amongst early-career orthopaedic surgeons while examining the influence of subspecialty fellowship training on utilization.
Methods: The American Board of Orthopedic Surgery (ABOS) Part II database was queried to identify all candidates performing at least one ankle fracture ORIF (Current Procedural Terminology [CPT] codes 27766, 27769. 27784, 27792, 27814, 27822, 27823, 27829, 27846, 27848) from examination years 2010 to 2019. All ORIF cases were examined to identify those that carried a concomitant CPT code for ankle arthroscopy (CPT codes 29891, 29892, 29894, 29895, 29897, 29898, 29899). Concomitant ankle arthroscopy cases were categorized by candidates self-reported fellowship training status and examination year. Descriptive statistics were performed to report relevant data and linear regression analyses were utilized to assess temporal trends in concomitant ankle arthroscopy with ORIF for ankle fractures. Statistical significance was defined as p<0.05.
Results: There were 36,113 cases of ankle fracture ORIF performed of which 388 cases (1.1%) were performed with concomitant ankle arthroscopy. Ankle fracture ORIF was most frequently performed by trauma fellowship trained Part II candidates (n=8,888; 24.6%), followed by sports medicine (n=7,493; 20.8%) and foot and ankle (n=6,563; 18.2%). Arthroscopy was most frequently utilized by foot and ankle fellowship trained surgeon (293/ 6,270 cases; 4.5%) followed by sports medicine (29/7,464 cases; 0.4%) and trauma (4/8,884 cases; 0.1%). With respect to total arthroscopic cases, 75.5% were performed by foot and ankle fellowship trained surgeons while only 1.0% was performed by trauma trained candidates. Ankle arthroscopy utilization significantly increased from 3.65 cases per 1,000 ankle fractures in 2010 to 13.91 cases per 1,000 ankle fractures in 2019 (p=0.010). Specifically, foot and ankle fellowship trained surgeons demonstrated a significant increase in arthroscopy utilization during ankle fracture ORIF over time (p<0.001; OR: 1.101; CI: 1.054-1.151).
Conclusion: Ankle arthroscopy utilization during ankle fracture ORIF has increased ten-fold over the past decade. Foot and ankle fellowship trained surgeons contribute most significantly to this trend.
DOI: 10.1177/2473011421S00446
Influence of Medical Marijuana on Mesenchymal Stromal Cell Osteogenesis: An in Vitro Study
Jiangyinzi Shang; MaCalus V. Hogan, MD, MBA, FAAOS, FAOA; Jarrett D. Cain, MSc, DPM; Hang Lin; Peter G. Alexander; Alan Y. Yan, MD
Category: Basic Sciences/Biologics; Basic Sciences/Biologics; Sports; Other
Keywords: Biologics; Biologics; Biologics
Introduction/Purpose: Recently, purposes of medicinal marijuana including analgesia and reduction in inflammation. The active component activates the CB1 and CB2 receptors, thus mimicking the action of endogenous cannabinoids. CB1 and CB2 are important regulators of bone metabollism. In particular, endocannabinoid signaling has shown to regulate proliferation and differentiation of MSCs and the activities of osteoblasts and osteoclasts. Cannabinoids may be prescribed to patients suffering bone fractures involving prolonged immobilization and discomfort. Thus, there is an important need to understand more completely the role of cannanbinoid signaling in fracture healing. In this study, we examine the influence of a synthetic cannabinoid agonist, Win-55,212-2 (Win) on adult, human MSC-derived osteoblast activity. Cell viability and osteogenic phenotype were assessed by MTS assay, RT-PCR, and alizarin red staining.
Methods: With an IRB approved protocol, MSCs were isolated from healthy human bone marrow and expanded to the passage five for experimentation. Cells were then plated at 5,200 cells/cm2 (6-well plate) and osteogenically stimulated for 21 days before treatment with increasing concentrations of Win (0.01, 0.1, or 1 µM) for an additional 48 hours. The MTS assay was employed to determine the half-maximal (50%) inhibitory concentration (IC50) at different time points. The cell phenotype was assessed by real-time PCR and alizarin red staining.
Results: We first used the MTS assay (for metabolism and proliferation) to test 7 doses of Win-55, from 0.001µM up to 5 µM and determined that the human osteoblast IC50 of Win-55 over 1-7 days of exposure was ~ 1.5 µM (Figure 1), a dose slightly lower than concentrations found to affect chondrocytes in a previous study. At 1µM Win-55, RT-PCR revealed that the expression of inflammatory cytokines IL-1beta and TNF-alpha was significantly reduced, while that of IL-6 and COX2 was unchanged. The expression of most osteogenic markers was unchanged by Win, but we did observe significant increases in BMP2, RUNX2 and OPN (Figure 2). Alizarin Red staining revealed increased calcium deposition and mineralization in the presence of 1µM Win, corroborating the RT-PCR results (Figure 3).
Conclusion: Win-55,212-2 may be beneficial to osteogenesis. 1 µM Win enhanced the osteoblastic phenotype over control, untreated MSC-derived osteoblasts, reduced inflammatory mediators and increased calcium deposition and mineralization. This suggests that cannabidiol treatment might lead to improvements in fracture healing and provide a novel therapeutic option for the bone regeneration. Future studies are aimed at characterizing the CB-1 and CB-2 signaling associated with the changes observed here and the effects of Win on MSC-derived osteoblasts in the context of inflammation.
DOI: 10.1177/2473011421S00447
Comparing Bilateral Feet Computed Tomography Scans Can Improve Surgical Decision Making for Subtle Lisfranc Injury
Introduction/Purpose: Subtle Lisfranc injuries (SLIs) are challenging to diagnose. Although weightbearing (WB) radiographs have been suggested to identify SLIs, approximately 20% are missed on initial radiographic assessment. Computed tomography (CT) has been suggested as an alternative, but has not provided any diagnostic guideline. Therefore we compared measurement techniques on radiographs and bilateral foot CT scans for the efficiency of diagnosis and making surgical decisions for SLI.
Methods: We retrospectively investigated patients diagnosed with SLIs between January 2014 and January 2020. Distances between both medial cuneiform and second metatarsal base (C1M2), and the first and second metatarsal bases (M1M2), were measured on bilateral WB radiographs. Bilateral foot CT scans were taken, and the distances between C1M2 were checked on the axial and three points of the coronal plane (top, middle, and base) (Figure 1). The surgical indication was > 1 mm of diastasis on CT scan. Clinical outcomes were evaluated using the American Orthopaedic Foot & Ankle Society (AOFAS) score at final follow-up. Intraobserver and interobserver agreements were assessed.
Results: Thirty patients with SLIs were reviewed. Twenty-four patients underwent surgical fixation (Group A) and six patients were treated conservatively (Group B). The side-to-side difference (STSD) of C1M2 and M1M2 distances greater than 1 mm showed 91.7% and 54.2% sensitivity, and 66.7% and 16.7% specificity, respectively. Investigating STSDs of all points on CT scans were informative to discriminate both groups (P <= 0.038). Clinical outcomes showed no significant difference between the groups (P = 0.631). Intraclass and interclass correlation coefficient values showed good to very good reliability, except for STSD of WB M1M2 distance and the coronal top plane.
Conclusion: Investigating bilateral foot CT scans was significantly efficient and reliable for the diagnosis and treatment plan for SLI. On radiographs, STSD of WB C1M2 distance was more sensitive than STSD of WB M1M2 distance.
DOI: 10.1177/2473011421S00448
Comparison of Newly Designed Three Spike Insole and Total Contact Insole in Refractory Plantar Fasciitis: A Randomized, Double-Blinded, Non-Inferiority Study
Dong Woo Shim, MD
Category: Ankle; Hindfoot
Keywords: Plantar Fasciitis; Nonoperative; Pain
Introduction/Purpose: Plantar fasciitis is one of the common foot complaints that is chronic and can induce dysfunction. Total contact insole (TCI) is simple but effective in treating plantar fasciitis. Nevertheless of the effect, the cost and the long duration for production have been the major flaws. Therefore, we developed newly designed three-spike insole (TSI) that can be commercially productive and compared the clinical outcomes with TCI.
Methods: Patients with plantar fasciitis refractory to conservative treatment for more than 6 weeks were candidates. We produced insoles with hardness of 58 +- 5 Shore-A. Twenty-eight patients were randomly allocated to use either TSI or TCI evenly (Figure 1). The following assessment tools were used: visual analog scale (VAS), American Orthopaedic Foot & Ankle Society score, Foot and Ankle Outcome Score, Karlsson-Peterson (KP) score, Short Form-36 for quality of life, and Foot Function Index. Non-inferiority was declared if VAS was within the statistical variability of minimal important difference. A blinded assessor evaluated the groups at baseline and after 6, 12, and 24 weeks.
Results: The groups were homogenous for majority of variables at baseline. Overall patient-reported satisfaction showed improvement from mean 5.2 (range, 1 - 12) weeks of wearing and all clinical outcome scores showed significant improvements in both groups over time on the basis of Friedman test (p <.05). TSI showed non-inferiority to TCI at each time point. Post hoc analysis revealed that many scales showed significant superiority of TSI at 3 month (p <.0125) and KP score at 6 month (p <.001).
Conclusion: We reaffirmed that semi-rigid insole is effective in refractory plantar fasciitis and showed TSI restores pedal function more rapidly than TCI. TSI can be not only effective in deriving better clinical outcomes but also be manufactured for popularization to lower the price and producing time of orthosis.
DOI: 10.1177/2473011421S00449
Needle-Arthroscopic Ankle Lateral Ligament Repair Using a Knotless Suture Anchor
Introduction/Purpose: Arthroscopic techniques have been increasingly used to repair the anterior talofibular ligament (ATFL) for lateral ankle instability, however there are still concerns on complications, such as nerve injury, iatrogenic cartilage damage and wound scar. Additionally, standard suture anchors can cause prominent knots. Recently, a novel needle-arthroscopic system (NanoScopeTM) has been introduced, with a 1.9-mm diameter arthroscope and semirigid frame, which can reduce conventional arthroscopic-related complications by minimizing the skin incisions and provide excellent visualization without ankle distraction due to its small and semirigid features. The purpose of this surgical technical note is to describe a new, very minimally invasive surgical technique for the ATFL repair using this needle-arthroscopy with a knotless suture anchor, which has the potential to reduce both conventional arthroscopic-related and knot-related complications.
Methods: We have developed a novel surgical treatment of the ATFL repair for lateral ankle instability in a cadaveric model. The arthroscopic system (NanoScopeTM, Arthrex, Naples, FL) is used during the procedures. The handpiece tube is 9.5-cm long, semi-rigid and has a 1.9-mm outer diameter. The scope’s direction of view is 0°, with a 120° field of view. The patient is placed in a supine position and no distraction is applied to the ankle joint. Standard anteromedial and anterolateral portals are first used. An accessory anterolateral (AAL) portal is then created around 1.5 cm anterior to the tip of the fibula, of which the portal position is determined under the visualization through the anterolateral portal.
Results: Almost all of the talar and tibial surfaces are reachable without distraction, due to its small and semirigid features. There is no difficulty problem obtaining proper visualization of the ATFL and the surrounding structures during the whole procedures, due to a wide 120°-field of view. The major steps of the procedure are (1) suture anchor insertion into the distal fibula through the AAL portal using a Knotless SutureTak Anchor (Arthrex), (2) penetration of suture string into the ATFL remnant using a Micro SutureLassoTM (Arthrex), (3) capture of the ATFL remnant using a suture-relay technique, (4) reattachment of the ATFL remnant by pulling out the passing wire without knot-tying, in the dorsiflexed ankle position (Figure). All skin-incisions are tiny and require only paper skin closures. This method requires neither blunt dissection of subcutaneous tissue to pass the suture nor knot-tying to reattach the ATFL.
Conclusion: Our technique is a simple, feasible, and very minimally invasive anatomic repair of the ATFL for lateral ankle instability using a 1.9-mm diameter needle-arthroscopy with a knotless suture anchor. However, the long-term clinical results need to be evaluated in future studies.
DOI: 10.1177/2473011421S00450
Posterior Hindfoot Endoscopy Using 1.9-mm Diameter Needle Arthroscopy: A Cadaveric Study
Introduction/Purpose: Posterior hindfoot endoscopy is a safe and effective treatment for posterior ankle impingement syndrome (PAIS) and flexor hallucis longus (FHL) tendon disorders. As frequent coexistence of PAIS and FHL tenosynovitis has been reported, it is important to investigate FHL tendon pathology concomitantly when treating PAIS. However, the visualization of FHL tendon distal to the retinaculum is limited when using conventional rigid arthroscopy. Additionally, wound-healing problems following hindfoot endoscopy have been still reported. Recently, a novel 1.9-mm diameter needle-arthroscopic system has been introduced. Its small and semirigid features can help reduce the risk of wound complications and can make it easier to perform FHL tendoscopy. The purpose of this study was to assess whether 1.9-mm diameter needle-arthroscopy was useful for hindfoot endoscopy in a cadaveric model.
Methods: A 1.9-mm diameter arthroscopic system (NanoScopeTM, Arthrex) was used to perform a hindfoot endoscopy in 6 human donor ankles (3 pairs). The arthroscope tube is 9.5-cm long and semi-rigid, and has a 1.9-mm outer diameter. The scope’s direction of view is 0°, with a 120° field of view. Posteromedial and posterolateral portals were established. Visualization and operative reach with tailored arthroscopic instruments were recorded, including posterolateral talar process, posterior talofibular ligament, intermalleolar ligament, subtalar joint, ankle joint, and flexor hallucis longus (FHL) tendon. Finally, a conventional 4.0-mm diameter arthroscope with a 30° angle was used to compare the visualization of FHL tendon.
Results: All significant structures were successfully visualized and reached in all specimens. In ankle joint, all of the tibial surface was visualized, but visualization of talar surface was limited. Due to its wide 120° field of view, there was no difficulty obtaining sufficient visualization in any structures. As this needle-arthroscopic system has the semirigid frame, FHL tendoscopy was easily performed via the posterolateral portal. In all specimens, the FHL tendon was visualized from the level of ankle joint to the Knot of Henry (Zone 1 and 2), and the flexor digitorum longus tendon crossing obliquely over the FHL tendon was observed (Figure). The conventional arthroscope could not be inserted into the tunnel underneath the sustentaculum tali in any specimens.
Conclusion: Posterior hindfoot endoscopy using a 1.9-mm diameter needle-arthroscopy provides effective visualization and surgical reach of all significant structures for the treatment of PAIS. Its small and semirigid features also make the FHL tendoscopy less invasive and more accessible than conventional rigid arthroscope.
DOI: 10.1177/2473011421S00451
Quantification and Comparison of Talar Exposure Utilizing A Posteromedial Approach and Medial Malleolar Osteotomy
Ademola I. Shofoluwe, MD
Category: Ankle; Hindfoot; Trauma
Keywords: Talus; Trauma; Osteotomies
Introduction/Purpose: Fractures of the talus contain a variety of morphologies including the head, neck, body, dome, lateral process, posterior process, and medial/lateral tubercles. Specifically, the posterior medial approach is useful for surgical fixation of posterior process fractures. The use of the medial malleolar osteotomy is beneficial in more extensive medial and distal exposure for neck or neck/body fractures. The purpose of this study was to quantify the area of osseous exposure afforded by a posteromedial approach to the talus and medial malleolar osteotomy. We believe this can be potentially useful for preoperative planning. To the authors' knowledge, a quantitative comparison of the talar access afforded by these two distinct approaches has yet to be described in the literature.
Methods: Five fresh frozen cadaveric lower extremities were dissected using a posteromedial approach and medial malleolar osteotomy respectively. Following exposure, the talar surfaces directedly visualized and demarcated along its boarders using a 2.0 mm drill bit orthogonal to the talar surface. The surface visualized was labeled and captured using a calibrated digital image. The digital images were then analyzed using ImageJ software (National Institutes of Health, Bethesda, MD) to calculate the surface area of the exposure.
Results: The average square area of talus exposed using the posteromedial approach was 9.70 (SD = 2.20, range 7.20 - 12.46) cm2. The average quantity of talar exposure expressed as a percentage was 9% (SD = 1.58, range 7.03 - 10.40). The average square area of talus exposed using a medial malleolar osteotomy was 14.32 (SD 2.00, range 11.26 - 16.66) cm2. The average quantity of talar exposure expressed as a percentage was 12.94% (SD = 1.79, range 9.97 - 14.73). The posteromedial approach provided superior visualization of the posterior talus, while the medial malleolar osteotomy offered greater access to the medial body.
Conclusion: The posteromedial approach and medial malleolar osteotomy allow for significant exposure of the talus, yielding 9.70 cm2 and 14.32 cm2, respectively. Given the differing portions of the talus exposed, surgeons may prefer to utilize the posteromedial approach for surgical fixation of posterior process fractures and elect to use a medial malleolar osteotomy in cases requiring more extensive medial and distal exposure for neck or neck/body fractures.
DOI: 10.1177/2473011421S00452
Efficacy of Fluoroscopically Guided Corticosteroid Injections for Foot and Ankle Pain
Tyler Slone; Michael Ciesa; Ania Bartholomew; Nicholas A Cheney, DO; Brian C. Clark
Introduction/Purpose: Arthritis of the foot and ankle can severely hamper quality of life resulting in decreased mobility and functionality. Conservative treatment can involve corticosteroid injections into affected joint spaces. Fluoroscopic guided injections provide confirmation that the injection was successfully applied within the appropriate joint space. Due to this, they can be of diagnostic value and result in more accurate injection placement. Current literature focuses on ultrasound guided injections and does not fully address the efficacy of fluoroscopic injections. Objective: Assess and determine overall efficacy of fluoroscopically guided corticosteroid injections including the degree and period of relief provided.
Methods: We retrospectively reviewed patient charts from 2016 through 2020 of patients that received fluoroscopically guided corticosteroid injections in foot or ankle joints. 224 injections were reviewed, gathering responses to percent relief, days of relief, pre-/post-injection VAS pain score and efficacy of repeat injections. Additionally, Kellgren-Lawrence arthritis scale vs pain relief were analyzed.
Results: Analysis limited by incomplete patient response. 24/83 (28.9%) injections provided less than 2 weeks of relief while 59/83 (71.1%) injections averaged 109.49 +- 72.03 days of pain relief. Of 127 responses, post-injection relief at first follow up had an average VAS reduction of 2.87 +- 3.17 with 70.38 +- 30.8 % improvement. 40 subjects with repeat injections had 109.41 +- 64.96 days of relief per injection. No significant correlation was found between joint injected or degree of arthritis and percent improvement.
Conclusion: Fluoroscopic guided injections are an effective conservative option providing prolonged but varying relief of 3-4 months irrespective of the specific joint or degree of arthritis. Repeat injections show similar efficacy. In contrast to ultrasound guided injections, fluoroscopy provides additional diagnostic and therapeutic value. This can be beneficial if the injections fail and the patient must progress to surgery. Future prospective studies could directly compare different injections modalities and further analyze efficacy for specific diagnoses.
DOI: 10.1177/2473011421S00453
Talocalcaneal Interosseous Ligament Provides Greatest Talar Stability in the Sagittal Plane
Michelle Smith; Emma Knapp, BS; Hani A. Awad, PhD; Irvin Oh, MD
Category: Hindfoot; Ankle
Keywords: Talus; Ankle; Biomechanics
Introduction/Purpose: Talar ANV, trauma, and implant failure or collapse after TAR are major challenges in foot and ankle surgery. Custom total talar implants are a promising option for such conditions and have shown promising results. However, there are no biomechanical studies examining the kinematics of total talus implant. We aimed to investigate the critical stabilizers of the native talus and the biomechanics of a total talar replacement. We hypothesize that the stability an implant is less affected by medial and lateral ligaments, with partial stability provided by the tibiotalar mortise, and the most instability occurs on the talocalcaneal joint due to absence of plantar restraint. Total talar implant will be most unstable in the sagittal plane, especially in heel-raise position.
Methods: Eight cadaveric samples underwent biomechanical testing in a midstance and seated heel-raise models in an E10000 Instron testing system. An OptiTrack system was used to record the 3D positions of the tibia, talus, calcaneus, navicular and first metatarsus throughout testing. The Achilles tendon was loaded in tension, while the tibia was cyclically loaded. The lateral ligaments, deep deltoid ligaments, talonavicular joint capsule, and the talocalcaneal interosseous ligament (TCIL) were sequentially released and underwent cycles in midstance and heel-raise positions after each release. The talus was removed and replaced to simulate total talar implant. Lastly, TA, EHL, and EDL were sutured into place to provide static soft tissue coverage of the talus, and final kinematics were measured. Data was analyzed to determine the joint motion and joint angles. Each ligament release was compared to one another using a one-way ANOVA, and compared to the initial condition using a one-sample t-test.
Results: Eight cadaveric foot and ankle models were examined (four left feet and four right feet). Under maximum force in a simulated seated plantarflexion position, gradual increase in talonavicular sagittal angle compared to initial condition was noted with sequential soft tissue releases. The talar dorsiflexion angle showed no significant change after lateral ligament, deltoid ligament, and talonavicular joint capsular releases. However, a significant increase in the talar dorsiflexion angle (4.38+/-4.04o ) was noted after the interosseous ligament release compared to initial condition (p= 0.02). Similarly, the displacement of the talus relative to the navicular was significantly increased after the talonavicular joint capsule release (1.47+/-1.33 mm, p = 0.03) and the interosseous ligament release (5.28+/-3.82 mm, p = 0.01).
Conclusion: In this study, we utilized native talus as a surrogate for a custom total talar implant to investigate the peritalar kinematics of the total talus implant. We found that the TCIL provides the most talar stability in the native ankle joint. Without the TCIL, the talus is most unstable in the sagittal plane, especially during the simulated heel-raise position. Significant medial and lateral stability of the tibiotalar joint maybe provided by the mortise of the ankle joint. Taken together, recreation of the TCIL or plantar stabilization of the implant should be considered to improve stability of a total talar implant.
DOI: 10.1177/2473011421S00454
State-Wide COVID-19 Lockdowns Did Not Adversely Affect the Management of Acute Ankle Fractures
Richard M. Smith; Tonya L. Dixon, MD, MPH; Nihar Shah, MD
Introduction/Purpose: The novel coronavirus (COVID-19) pandemic has presented a unique challenge to orthopaedic trauma and operative fracture management throughout the United States. Various public health and safety measures imposed during the lockdown lead to cancelation or rescheduling of non-emergent or non-urgent surgery cases. In order to provide appropriate standard of care, certain operative cases were deemed urgent and managed on an inpatient basis. This change in practice had an impact on the management of acute ankle fractures which has previously reported excellent results and cost-savings with outpatient operative management. The goal of this study is to determine the impact of the COVID-19 lockdown and barriers to care in treating isolated operative ankle fractures in the inpatient setting.
Methods: The current IRB approved study is a retrospective review of adult patients presenting to University of Cincinnati (UC) with isolated, operative ankle fractures. The study period consisted of patients who presented during the months of January 1st - July 1st 2020 to coincide with pre-, intra and post- COVID lockdown in Southwestern Ohio. Of note, the official mandated lockdown within the state of Ohio was March 23rd - May 1st with phased business re-openings after May 1st. Similarly, hospital operations including operative capacity was restricted until a return to full capacity on June 29, 2020. A total of 464 patient records were reviewed (159, 176, 129 ankle fractures for the respective years 2018-2020). A review of the data from years 2018, 2019 were analyzed for statistical comparison. Polytraumatized patients, open fractures and those with bilateral injuries were excluded.
Results: The final cohort included 190 ankles (52, 71, 67, for 2018, 2019, 2020 respectively). This comprised of 71 males (38%), 119 females (62%). The average age of patients were 48+-19, 51+-18, 48+-20, respectively. There were no significant differences in BMI, smoking and diabetic status. There was a total of eight isolated ankle fractures during the immediate lockdown period of 2020, all managed with inpatient surgery. This was compared to the previous year 2019 (7/16 treated with inpatient management), versus 2018 (4/5 inpatient). Overall, among allcomers, 2020 had the lowest amount of acute fractures treated as outpatient, elective cases (34%) versus 45% -2019, 58%- 2018; however, this was not statistically significant. The length of stay for inpatients, time until surgical management, time to physical therapy clearance, postoperative follow up with index surgeon or midlevel providers were not significantly different among the 2020 cohort during and immediately after the state-wide lockdown.
Conclusion: Little has been published about the effect of the coronavirus lockdown on acute fracture management. In this study of acute ankle fractures, strategic practice changes to predominantly inpatient management did not adversely affect patient care. However, there are disadvantages to inpatient versus outpatient management such as: (1) resource allocation (such as hospital beds during a pandemic) and (2) associated costs to both patients and hospital. Future efforts will be made to elucidate the cost analysis within our hospital system (not available at the time of this submission).
DOI: 10.1177/2473011421S00455
Minimally Invasive Management of a Rare Giant Cell Tumor of Talus: A Case Report and Literature Review
Sandip S. Sonawane
Category: Ankle; Hindfoot; Other
Keywords: Talus; Autograft; Minimally Invasive
Introduction/Purpose: Giant cell tumor (GCT) of small bones of hand and feet is rare. A benign but locally aggressive neoplasm with a tendency for local recurrence with undifferentiated mesenchymal stromal cells and the presence of abundant, multinucleated giant cells. It occurs in a slightly younger age group with usually an expansile and eccentric epiphyseo-metaphyseal region lytic lesion. A 22 yrs. old patient, presenting as lytic expansile lesion of talus, suspected Giant cell tumor (GCT) of talus preoperatively and intraoperatively and proven subsequently, is presented along with review of literature. This patient is the young and nearly 24th case reported in the literature for GCT of talus.
Methods: Author reviewed the literature for the GCT of talus from 1964 to till 2021. The author reported a case of left ankle joint pain and swelling for 6 months in a 22 yrs. old male, which turns out to be aneurysmal bone cyst of talus on radiographs, Computed tomography and aspiration cytology. Campanacci grade II lesion was planned for the curettage and autologous bone grafting.
Results: Retrospectively, the intraoperative biopsy confirmed the lesion as giant cell tumor with aneurysmal bone cyst. After 4 years the lesion showed the near complete resolution on radiographs and CT scan. However, because of the historical recurrence and metastasis reports of GCT, author is continuously monitoring patient’s ankle with yearly follow up. Author reviwed the literarue for the GCT of talus from 1964 to till 2021. Author found total of 23 reported cases for GCT of talus in literature, out of which 2 cases showed recurrence and distant metastasis to chest which is 8.69 percent of total cases.
Conclusion: Author concludes that the Campanacci grade I and II can be managed with mini-open lesional curettage and autologous bone grafting while grade III and IV needed osteotomy, en-bloc excisions and tibio-calcaneal fusion or below knee amputation in recurrent or aggressive lesions. As author found 8.69 percent cases of distant pulmonary metastasis out of total reported cases, he recommends yearly follow up of the lesions and look for distant metastasis in suspected cases.
DOI: 10.1177/2473011421S00456
Percutaneous Correction Surgery of Hammer Toes with Biodegradable Pins
Pablo Sotelano, MD; Daniel S. Villena, MD; Ana C. Parise, MD; Leonardo A. Conti, MBA, PhD; Nelly M. Carrasco, MD; Jonathan M. Verbner, MD; Maria Gala Santini Araujo, MD
Introduction/Purpose: The standard treatment for deformities in lesser toes is proximal interphalangeal arthrodesis with Kirschner wires. It is relatively inexpensive but complications have been described such as infection, recurrences and misalignment. New devices were developed, among them biodegradable pins avoid the need for withdrawal and exposure to the outside. The objective of this study was to describe the clinical and radiological results one year after surgery in a group of patients with a diagnosis of rigid hammer toes, who underwent percutaneous surgical correction with a biodegradable pin.
Methods: Methods: We present a retrospective study in a consecutive series of cases with a diagnosis of hammer toe operated between January 2016 and December 2018. Patients older than 18 years of age who underwent a percutaneous proximal interphalangeal arthrodesis, with a biodegradable pin, were included. The patients were asked through a survey to rate the results obtained with the intervention (excellent, very good, good, fair and bad). loss of contact with the ground was evaluated with podobarography. The patients were evaluated with weightbearing X rays to assess interphalangeal alignment and consolidation. We used the AOFAS scale to assess clinical results, preoperatively and one year after surgery. Postoperative complications, infection, wound dehiscence, rupture of osteosynthesis material, loss of correction were also evaluated.
Results: 117 patients were identified, 23 (16%) underwent bilateral surgery (140 feet), with a total of 220 lesser toes who underwent proximal interphalangeal arthrodesis stabilized with percutaneously biodegradable pin. 50% had a minimum follow-up of 1 year. The pre-surgical AOFAS of 52 improved to 95 points in the postoperative period. In 96 (43.63%) fingers, an F1 base osteotomy was performed to correct the alignment in the coronal plane. We observed pseudo osteoarthritis in 5% of the toes but with good alignment. We observed 6% of floating fingers, the pin was removed in 5 fingers; without loss of correction. In 1.36% cases it migrated early, causing a recurrence of the lesion. Patient satisfaction was excellent or very good in 79 %.
Conclusion: According to our serie results, we consider that percutaneous technique with biodegradable pins manages to maintain adequate alignment and a consolidation rate both in radiological and clinical results with good patient satisfaction. No infection case was reported. We found a low rate of biodegradable pin removal. For its part, the biodegradable plug allows osteotomies to be performed with the implant already in place, it does not require routine removal of the implant, reducing the need for a second intervention.
DOI: 10.1177/2473011421S00457
Efficacy of 3T MRI vs Diagnostic Arthroscopy for the Diagnosis of Osteochondral Lesions of the Talus in Patients Undergoing Brostrom Repair for Lateral Ankle Instability
Chris M. Stauch, BS; Zachary Koroneos; Anna Ptasinski; Brandon Martinazzi, BS; Shawn M. Bifano, MD; Michael C. Aynardi, MD
Category: Ankle; Arthroscopy
Keywords: Osteochondral Lesions of the Talus; Broström; Ankle Arthroscopy
Introduction/Purpose: Osteochondral lesions of the talus (OLT) are commonly seen in patients with lateral ankle instability. If left undiagnosed, OLTs can lead to significant ankle pain and progressive osteoarthritis. While arthroscopy has long been the gold standard for the diagnosis of OLTs, MRI is a useful imaging modality for pre-operative evaluation and surgical planning in patients undergoing surgery for lateral ankle instability. The purpose of this study was to evaluate the diagnostic accuracy of 3T MRI for the diagnoses of OLTs in patients undergoing a Broström Gould procedure for lateral ankle instability.
Methods: Following institutional review board approval, a database was obtained for all patients from 2/11/2015 to 1/21/2019 who underwent a Broström Gould procedure for lateral ankle instability in addition to diagnostic arthroscopy of the tibiotalar joint. Additionally, patients required a pre-operative 3T MRI for inclusion in the study. Patients who underwent the Broström Gould procedure but did not have a diagnostic arthroscopy or did not have a pre-operative MRI were excluded from the study. The average time from MRI to surgery was 3.5 months. Patient charts were then reviewed to determine the proportion of MRIs that correctly identified the presence or absence of OLTs compared to diagnostic arthroscopy.
Results: A total of 80 patients were included for analysis with an average age of 38.1 +- 14.3 years. 46 (57.5%) patients were female and 34 (42.5%) were male. A total of 39 patients (48.8%) were identified to have an OLT on arthroscopy. Of these 39 patients, 28 patients (71.8%) were correctly identified by the pre-operative 3T MRI as having an OLT and 11 patients (28.2%) had MRIs that failed to identify an OLT. 41 patients had an arthroscopy that was negative for OLTs. Of these 41 patients, MRI correctly diagnosed 40 patients (97.6%) as not having an OLT and misdiagnosed 1 patient as a false positive (2.4%).
Conclusion: In patients undergoing Broström Gould procedures with diagnostic arthroscopy for osteochondral lesions of the talus, 3T MRI demonstrates a sensitivity of 71.8% and a specificity of 97.8%. Thus, pre-operative MRI can be a useful imaging modality to assess for OLTs prior to surgery and should prompt surgeons to perform an arthroscopy with subsequent treatment of the OLT. However, a negative MRI does not rule out the possibility of an OLT being present due to a relatively high false- negative rate.
DOI: 10.1177/2473011421S00458
Can Bedside Needle Arthroscopy of the Ankle be an Accurate Option in the Office Setting for Intra- Articular Delivery of Injectable Agents?
Tobias Stornebrink, MD; Sjoerd A. Stufkens, MD, PhD; Nathaniel P. Mercer; John G. Kennedy, MD, FRCS(Orth); Gino Kerkhoffs, MD
Introduction/Purpose: To evaluate accuracy and patient experience of inspection-injections of the ankle with in-office needle arthroscopy in a relevant clinical setting - including patients with end-stage ankle pathology and/or a history of prior surgery.
Methods: This was a prospective study that included adult patients who were scheduled for an injection with hyaluronic acid to the tibiotalar joint. In our center, these injections are used as a last resort prior to extensive surgery. The primary outcome was injection accuracy, which was defined as injecting through the arthroscopic cannula with intra-articular positioning confirmed by a clear needle arthroscopic view of the joint space. Secondary outcome measures included a patient reported numeric rating scale (NRS, 0-10) of pain during the procedure and willingness of patients to return for the same procedure. NRS of ankle pain at rest and during walking was collected during the intervention and at two-week follow-up. Complications were monitored from inclusion up to a two-week control visit.
Results: We performed 24 inspection-injections (11 (46%) males, mean age 47.8 +- 14.5 years). The indication was end-stage osteoarthritis in 21 (88%) cases - eight (33%) Kellgren-Lawrence grade IV, 10 (42%) Kellgren-Lawrence grade III - and an osteochondral defect in three (13%) cases. Fourteen (58%) patients had had prior ankle surgery - 11 (46%) patients had had multiple prior surgeries. Accuracy was confirmed in 22 (88%) cases. The three unsuccessful injections all occurred in patients with Kellgren-Lawrence grade IV osteoarthritis. Median NRS of pain during the procedure was 1 (IQR 0 - 2). Willingness to return was 100%. Median NRS of pain in rest decreased from 4 (IQR 2 - 5) at intervention to 3 (IQR 1 - 5) at follow-up (p < 0.01). The median NRS of pain during walking decreased from 8 (IQR 6 - 8) to 7 (IQR 4 - 8) (p < 0.01). There were no complications.
Conclusion: In-office needle arthroscopy of the ankle under local anesthesia is a procedure that is well tolerated by patients. It is able to provide intra-articular delivery of injectable agents with high accuracy. Accuracy can be expected to approach 100% if patients with total ventral joint obliteration and a history of extensive prior ankle surgery are excluded.
DOI: 10.1177/2473011421S00459
Safe and Effective Anterior Ankle Arthroscopy with A 2-mm Diameter Operative System
Tobias Stornebrink, MD; Nienke Altink; Daniel Appelt, PhD; Coen A. Wijdicks; Sjoerd A. Stufkens, MD, PhD; Gino Kerkhoffs, MD
Keywords: Ankle Arthroscopy; Surgical Instrumentation; Structural Anatomy and Biomechanics
Introduction/Purpose: The purpose of this study was to assess whether all significant structures in the ankle could be visualized and surgically reached during 2-mm diameter operative arthroscopy, without inflicting iatrogenic damage.
Methods: A novel, 2-mm diameter arthroscopic system was used to perform a protocolled arthroscopic procedure in 10 fresh- frozen, human donor ankles. Standard anteromedial and anterolateral portals were utilized. Visualization and reach with tailored arthroscopic instruments of a protocolled list of articular structures were recorded and documented. A line was etched on the most posterior border of the talar and tibial cartilage that was safely reachable. The specimens were dissected and distances between portal tracts and neurovascular structures were measured. The articular surfaces of talus and tibia were photographed and inspected for iatrogenic damage. The reachable area on the articular surface was calculated and analysed.
Results: All significant structures were successfully visualized and reached in all specimens. The anteromedial portal was not in contact with neurovascular structures in any specimen. The anterolateral portal collided with a branch of the superficial peroneal nerve in one case, but did not cause macroscopically apparent harm. On average, 96% and 85% of the talar and tibial surfaces was reachable respectively, without causing iatrogenic damage.
Conclusion: 2-mm diameter operative arthroscopy provides safe and effective visualization and surgical reach of the anterior ankle joint. It may hold the potential to make ankle arthroscopy less invasive and more accessible.
DOI: 10.1177/2473011421S00460
Safe and Effective Tendoscopy around the Ankle with A 2-mm Diameter Operative System
Tobias Stornebrink, MD; Sjoerd A. Stufkens, MD, PhD; Daniel Appelt, PhD; Coen A. Wijdicks; Gino Kerkhoffs, MD
Introduction/Purpose: To assess whether 2-mm-diameter operative tendoscopy of the tibialis posterior, peroneal, and Achilles tendons was safe and effective in a cadaveric model.
Methods: A 2-mm-diameter arthroscopic system was used to perform a tendoscopic procedure in 10 nonpaired, freshfrozen, human ankles. Standard tendoscopic portals were utilized. Visual examination and operative reach with tailored tendoscopic instruments within the tendon sheaths were recorded and documented. Adhesiolysis and vincula resections were performed. After dissection, distances between portal tracts and neurovascular structures were measured and the tendons were inspected for signs of iatrogenic damage.
Results: The entire tendon sheath and tendon of the tibialis posterior, peroneus brevis, and Achilles tendons were visualized and reached with tailored operative instruments. The proximal part of the peroneus longus tendon was visible and reachable from proximally up to the cuboid bone distally. Adhesiolysis and vincula resections were successfully performed in all specimens. The mean distances between portal tracts and local neurovascular structures ranged between 9.4 and 19.2 mm and there were no cases of contact. None of the tendons showed signs of iatrogenic damage.
Conclusion: Two-millimeter-diameter operative tendoscopy provided safe and effective visualization and operative reach of the tibialis posterior, peroneal, and Achilles tendons.
DOI: 10.1177/2473011421S00461
The Influence of Metatarsus Adductus Angle on Fifth Metatarsal Jones Fractures
Carson D. Strickland, MD; David J. Ruta, MD; Benjamin J. Grear, MD; David R. Richardson, MD; G. Andrew Murphy, MD
Category: Trauma; Midfoot/Forefoot
Keywords: Jones Fracture; Metatarsus Adductus; Fractures
Introduction/Purpose: Previous studies have reported increasing metatarsus adductus angle (MAA) to be associated with delayed union and refracture following intramedullary screw fixation of fifth metatarsal Jones fractures. The purpose of this study was to determine the influence of MAA on postoperative course following intramedullary screw fixation of Jones fractures. We also sought to identify associations between elevated MAA and both fracture and patient characteristics.
Methods: We performed a retrospective review of all Jones fractures treated with primary intramedullary screw fixation by 4 foot and ankle fellowship-trained orthopaedic surgeons at a single institution from 1995 through 2015. Exclusion criteria included concomitant foot/ankle procedures and revision surgery. Charts were reviewed for patient and injury characteristics, implant, and postoperative course. Radiographs were examined for fracture classification, radiographic union, and MAA. MAA calculations were performed on standard weight-bearing digital radiographs using the traditional method, with the 5th metarso-cuboid joint as a reference. Based on severity of MAA, comparative and correlation analyses were performed. Primary outcomes were the number of surgical failures (defined as delayed union, nonunion, or refracture) and time to radiographic union, weight bearing, and pain resolution. Data was analysed using independent T test, one-way ANOVA, chi-square, and correlation analyses with significance defined as p<0.05.
Results: 59 feet in 58 patients were identified with a mean age of 30 years and average follow-up of 9.6 months. The pooled union rate was 96.6%. The mean MAA was 20.9 (SD 6.7). Eleven feet had MAA<15, 18 mild (MAA 15-20), 12 moderate (MAA 20- 25), 18 severe (MAA>25), and 1 unknown. 11 patients had failures (18.6%), which consisted of 7 delayed unions (11.9%), 2 delayed unions (3.4%), and 3 refractures (5.1%). Compared to the uncomplicated unions, there was no significant difference in mean MAA (24.3 vs. 20.1, p=0.16). Three of the 4 non-union or refracture patients had MAA>25. MAA was correlated with time to weight bearing (r=0.365, p=0.005), weight (r=0.503, p<0.001), BMI (r=0.280, p=0.03), and approached significance with age (r=0.230, p=0.082). No significant correlation was found with time to radiographic union.
Conclusion: To our knowledge, this is the largest series investigating MAA in fifth metatarsal Jones fracture patients treated with intramedullary screw fixation. Our mean MAA is consistent with previous reports. We found an association between increased MAA and postoperative recovery time, given increased time to initiate weight bearing. We did not find significant associations with prolonged radiographic healing, age, nor failure. The prolonged time to weight bearing may reflect surgeon preference in patients with higher MAA. These results suggest that reported associations with MAA may not be as strong as previously thought.
DOI: 10.1177/2473011421S00462
Risk Factors for Aseptic Revision of Surgically-Treated Ankle Fractures
Kristen L. Stupay, MD; Steven Staffa, MS; Michael McTague; Michael J. Weaver; Christopher P. Miller, MD; John Y. Kwon, MD
Category: Trauma; Ankle
Keywords: Ankle Fracture; ORIF; Syndesmosis
Introduction/Purpose: Early revision rates within 12 months after ankle fracture open reduction internal fixation (ORIF) are fairly low, however remain relevant given the sheer volume of ankle fractures which occur each year. Understanding these rates is complex because reoperation due to technical or mechanical complications - such as malunion, inadequate reduction or fixation failure - are typically reported alongside returns to the operating room for soft-tissue related problems like wound dehiscence or infection. There is limited data identifying risk factors specifically for revision of ankle fracture fixation in the absence of soft-tissue complications. Understanding variables which predispose to aseptic technical and mechanical failure without this confounder may provide insight and improve patient care.
Methods: The purpose was to identify risk factors for aseptic revision of ankle fracture within ORIF 1 year of primary operation. A retrospective cohort study was performed at two large academic medical centers. Research Patient Data Registry (RPDR) data available from 2002-2019 was used to identify patients who underwent aseptic revision of ankle fracture ORIF within 12mo of their primary ORIF. Patients were excluded if <18yo at primary surgery, or if indications for return to the operating room included surgical management of a dehisced wound or deep infection. A control group was selected by identifying sequential patients who underwent ankle fracture ORIF which did not require revision within 12mo. Primary and revision surgeon characteristics, patient demographics, comorbidities, fracture characteristics, surgical techniques and post-operative events were recorded and compared in univariate analysis. Variables which achieved significance in univariate comparisons were included as candidates for multivariable analysis.
Results: 33 patients were identified for the Revision group. 100 patients were identified for the Control group (Power = 80% for detecting moderate differences). Groups did not differ in age or gender. Final multivariable logistic regression modeling, adjusting for all other variables within the multivariable analysis, demonstrated the following factors to be independently associated with an increased risk of revision surgery: Documented falls in the early post-operative period (aOR: 298; 95% CI: 15.4, 5759; P<0.001), Movement-altering disorders (aOR=81.7; 95% CI: 4.12, 1620; P=0.004), a non-anatomic mortise (MCS > SCS) on immediate post- operative imaging (aOR=28.4; 95% CI: 5.53, 267; P<0.001), more severe initial fracture displacement (ARCS Type C) (aOR vs Type A =25.8; 95% CI: 2.81, 237; P=0.004), Substance abuse (aOR=15.7; 95% CI: 2.66, 92.8; P=0.002), and polytrauma (aOR=12.3; 95% CI: 2.02, 74.8; P=0.006).
Conclusion: Six factors were found to be predictive of the need for aseptic revision: Documented falls in the early post- operative period (aOR: 298), movement-altering disorders (aOR=81.7), a non-anatomic mortise (MCS > SCS) on immediate post- operative imaging (aOR=28.4), more severe initial fracture displacement (ARCS Type C) (aOR=25.8), substance abuse (aOR=15.7) and polytrauma (aOR=12.3). Identifying these factors may allow surgeons to better counsel their patients and discuss risk during the informed consent process. These may also serve as future targets for intervention aimed at improving patient safety and outcomes follow ankle fracture ORIF.
DOI: 10.1177/2473011421S00463
Depressive Disorders Lead to Increased Complications after Pilon Fracture Surgery
Syed Tahmid; Matthew S. Broggi; Jerad Allen, MD; Roberto Hernandez-Irizarry
Introduction/Purpose: Given the increased survival of the polytrauma patient, the incidence of tibial pilon fractures has increased. Preoperative depression has been linked with worse morbidity and mortality following lower extremity surgery, however its effect on outcomes following tibial pilon fractures has not been studied. This studies purpose was to investigate the relationship between preoperative depression and potential complications following tibial pilon fracture surgery.
Methods: This retrospective study utilized the Truven Marketscan claims database to identify patients who underwent outpatient tibial pilon fracture surgery from January 2009 to December 2018 based on Common Procedure Terminology (CPT) codes. The two cohorts entailed patients with and without preoperative depression based on International Classification of Diseases (ICD codes. The associated between preoperative depression and common postoperative complications following tibial pilon fracture was analyzed using chi square testing and multivariate analysis.
Results: In total, 4,795 patients were identified for analysis. In those patients with preoperative depression, the complications associated with the greatest increased odds were infection (OR 1.59), wound complication (OR 1.31), ED visit pain (OR 1.29), hardware complications (OR 1.22), and DVT/PE (OR 1.14).
Conclusion: Increased complications and use of healthcare resources have been associated following tibial pilon fracture surgery in persons with a preoperative diagnosis of depression. Acknowledgement of patient’s preoperative depression can allow surgeons to tweak treatment protocols before and after surgery. Additional studies should be conducted to investigate the degree of modifiability of depression as a risk factor.
DOI: 10.1177/2473011421S00464
Preoperative Depression is Associated with Increased Complications Following Ankle Fracture Surgery
Syed Tahmid; Matthew S. Broggi; John Hurt, BS; Rishin J. Kadakia, MD; Jason T. Bariteau, MD; Michelle M. Coleman, MD, PhD
Introduction/Purpose: Ankle fractures are a common injury treated by orthopaedic surgeons with a rising incidence. Preoperative depression is a known risk factor for postoperative complications in joint replacement surgery, however its effects on outcomes following ankle fracture surgery is unknown. The purpose of this study was to investigate the relationship between preoperative depression and outcomes following ankle fracture surgery.
Methods: In this retrospective study, the Truven MarketScan claims database was used to identify patients who underwent outpatient ankle fracture surgery from January 2009 to December 2018 using Common Procedure Terminology (CPT) codes. Patient characteristics, and medical comorbidities were collected. Patients with and without a diagnosis of preoperative depression were identified based on International Classification of Diseases (ICD) codes. Chi-squared and multivariate analyses were performed to investigate the association between preoperative depression and common postoperative complications following ankle fracture surgery.
Results: In total, 107,897 patients were identified for analysis, 13,981 of whom were diagnosed with depression (13%). Preoperative depression was associated with the increased odds for postoperative infection (OR 1.33, CI 1.20-1.46), wound complications (OR 1.13, CI 1.00-1.28), pain-related postoperative emergency department visits (OR 1.58, CI 1.30-19.1), 30-day and 90-day readmissions (OR 1.08, CI 1.03-1.21 and OR 1.13, CI 1.07-1.18), sepsis (OR 1.39, CI 1.12-1.72) and postoperative development of complex regional pain syndrome (OR 1.46, CI 1.18-1.81).
Conclusion: Preoperative depression in patients undergoing ankle fracture surgery is common and associated with increased complications following surgery. An understanding of patients' preoperative depression diagnosis can allow providers to modify perioperative and postoperative protocols for these higher risk patients. Further studies are warranted to investigate the degree to which depression is a modifiable risk factor.
DOI: 10.1177/2473011421S00465
Elite Athletes Successfully Return to the Preinjury Level of Sport Following Ankle Syndesmosis Injuries: Systematic Review and Meta-Analysis
Eric W. Tan, MD; Ioanna K. Bolia; Jacob Bogdanov; Kyle Schoell; Frank A. Petrigliano; Alexander E. Weber
Category: Sports; Ankle
Keywords: Ankle Sprain; Syndesmosis; Sports
Introduction/Purpose: No meta-analysis has been conducted to examine the clinical outcomes following operative and nonoperative management of high ankle sprain injuries in elite athletes. the purpose of this systematic review was (1) To report the rate and time to return to sport (RTS) following high ankle syndesmotic injury in elite athletes (2) To examine the rate and time of RTS as well as the postoperative complications in elite athletes who underwent surgical treatment of high ankle syndesmotic injury with screw versus suture button fixation.
Methods: Three electronic databases were searched for eligible articles. Two reviewers independently screened the titles, abstract and full-text articles using pre-specified criteria. Eligible articles were those that reported the rate of return to sport following operative and nonoperative treatment of ankle syndesmotic injuries in elite athletes (collegiate or professional level). Data collected were type of sport, type of treatment received (operative versus nonoperative), surgical technique (screw versus suture button fixation), rate and time to return to the preinjury level of competition, and complications. A random-effects model was used for meta-analysis.
Results: The estimated overall rate of RTS was 99% (95% CI 95.5-99.9). The mean time to RTS was 38 +- 18 (range: 14-137) days. Of the 440 athletes, 269 (269/440,61%) were treated nonoperatively (nonoperative group); the rate of RTS was 99.6% and the athletes returned at a mean time of 29+-14 (range: 13-45) days. A total of 171 athletes (171/440,39%) underwent surgical treatment (operative group); All (171/171,100%) athletes returned at a mean time of 50.3+-13 (range:41-137) days. Almost all athletes who underwent surgery had suture button fixation (164/171 athletes,96%) and the mean time to RTS was 7 weeks with 9.1% complication rate.
Conclusion: Elite athletes with ankle syndesmosis injury return to sport at an extremely high rates, following operative or nonoperative treatment. Suture button fixation remains the gold standard technique in elite athletes with syndesmotic injury requiring surgical treatment. Return to the preinjury level of competition should be expected at 4 weeks and 7 weeks in high-level athletes who undergo nonoperative and operative management, respectively.
DOI: 10.1177/2473011421S00466
Fifth Metatarsal Injuries in NCAA Division I Athletes: Management and Return to Play
Eric W. Tan, MD; Ioanna K. Bolia; Alexander E. Weber; Alexander B. Peterson; Hyunwoo P. Kang; Russel Romano; James Tibone; David B. Thordarson, MD; Seth C. Gamradt
Category: Midfoot/Forefoot; Sports; Trauma
Keywords: Fifth Metatarsal Fractures; Athlete; Return to Play
Introduction/Purpose: Optimal management of metadiaphyseal fifth metatarsal fractures (Jones fractures) in athletes remains controversial. In high-level athletes, surgical treatment with intramedullary screw fixation is commonly recommended to minimize the risk of nonunion and to allow for faster return to sport. The purpose of this study was to report the rate and time to return to sport in collegiate athletes who sustained an isolated fracture to the fifth metatarsal bone.
Methods: From 2003 to 2020, we retrospectively reviewed the clinical notes and imaging studies of all athletes participating in NCAA Division I sports at a single college and who sustained a fracture of the fifth metatarsal bone. Athletes with a diagnosis of 5th metatarsal bone fracture were included. Athletes were excluded if they had a fracture in any of the other metatarsal bones (1st-4th). Data collected were: demographic information (age, gender), type of sport, date of injury and/or surgery, diagnosis of Jones fracture, type of treatment received (operative with intramedullary screw fixation versus non operative with the application of boot or cast of the lower extremity and non- weightbearing activity), rate of return to sport, and time to return to sport. The rate and time to return to sport were reported as percentage and mean-standard deviation, respectively. The level of statistical significance was set at <0.05.
Results: From 2003 to 2020, we retrospectively reviewed the clinical notes and imaging studies of all athletes participating in NCAA Division I sports at a single college and who sustained a fracture of the fifth metatarsal bone. Athletes with a diagnosis of 5th metatarsal bone fracture were included. Athletes were excluded if they had a fracture in any of the other metatarsal bones (1st-4th). Data collected were: demographic information (age, gender), type of sport, date of injury and/or surgery, diagnosis of Jones fracture, type of treatment received (operative with intramedullary screw fixation versus non operative with the application of boot or cast of the lower extremity and non- weightbearing activity), rate of return to sport, and time to return to sport. The rate and time to return to sport were reported as percentage and mean-standard deviation, respectively. The level of statistical significance was set at <0.05.
Conclusion: Jones fractures of the 5th metatarsal bone are a relatively rare injury in collegiate athletes at our institution occurring mostly in male football and basketball players at a rate of about one fracture per year for 21 intercollegiate teams. These fractures are treated with a high level of success with intramedullary screw fixation. Given that postoperative recovery may last for approximately 3 months, return to play following surgical fixation of a Jones fracture is highly dependent on the timing of injury; an athlete who sustains the injury in-season is unlikely to return to play that same season.
DOI: 10.1177/2473011421S00467
Effect of Weight Bearing Variations & Heel Height on Forefoot Width for Orthopaedic Imaging
Introduction/Purpose: The biomechanics of a foot when weight bearing change significantly due to the changes in the function through the gait cycle. Variations in heel height are known to influence load distribution in weightbearing, thus affecting change in forefoot widths. Weight bearing in radiographs are commonly used to identify these changes, which may have clinical relevance. However, there are limited studies that accurately quantify the extent of these differences in the forefoot to be analysed effectively. Hence, there is a need to investigate different weight bearing conditions and its influence on forefoot width changes required for accurate analysis of imaging. This study’s aim is to evaluate the significance and degree of foot splaying with different modes of weight-bearing and heel height to achieve optimum increase in forefoot width.
Methods: 32 volunteers with no clinical issues with their feet were selected for this study. Weight bearing photographs of their feet were reviewed by 2 foot and ankle surgeons (under blinded conditions) to ensure they were normal morphologically. The forefoot width is measured using sliding callipers between the medial margin of the first metatarsal head and lateral margin of the fifth metatarsal head when non weight bearing - NWB, partial weight bearing - PWB (dual leg stance) and full weight bearing - FWB (single leg stance). Single leg stance measurement is also taken at increasing heel heights of 2cm (FWB1), 4cm (FWB2) and 6cm (FWB3) using polyurethrane blocks. Each individual foot non weight-bearing width will act as its own control for the changes in the differing positions measured.
Results: Statistical analysis of data demonstrated the results with the use of student t-test analysis via SPSS which showed statistically significant differences in forefoot width in both genders(p<0.05). There is an increasing trend of forefoot width as weightbearing conditions increase up to 2cm of elevated heel height. However, forefoot width decreases as heel height increases beyond 2cm in both genders. Female subjects have a higher trend of percentage of increase in mean forefoot width compared to males in all weightbearing conditions except for full weightbearing with 6cm heel height elevation.
Conclusion: In conclusion, there is a linear trend of increase in forefoot width with increase from non-weightbearing up to 2cm heel height inclination. Full weightbearing with 2cm heel height inclination produces the widest foot splaying in this study. Larger future studies will need to be conducted to validate these findings.
DOI: 10.1177/2473011421S00468
Pes Planus Does Not Negatively Affect Clinical Outcomes after Hallux Valgus Surgery
Adriel You Wei Tay, MBBS, MRCS (Edin); Graham Goh, MBBS, MRCSEd; Yogen Thever; Nicholas Yeo, MBBS, MRCS, MMed(Ortho), FRCS(Edin), FAMS; Kevin Koo, FRCS(Orth)(Edin)
Category: Bunion; Hindfoot; Midfoot/Forefoot; Other
Introduction/Purpose: Pes planus is associated with hallux valgus development. Increased forefoot abduction and pressure through the hallux during the heel-rise phase of the gait in a pes planus foot is believed to contribute to hallux valgus formation. These abnormal forces through the hallux may result in poorer healing and more residual pain after surgical correction. We investigated if patients with increasing severity of pes planus presented with more severe hallux valgus deformity and whether these patients had more residual pain and poorer function following hallux valgus surgery.
Methods: We evaluated 191 consecutive cases of hallux valgus surgery with Scarf osteotomy as the primary procedure. American Orthopaedic Foot & Ankle Society (AOFAS) hallux metatarsophalangeal-interphalangeal scale, visual analog scale (VAS), Short Form-36 physical component summary (SF-36 PCS), mental component summary (SF-36 MCS) and a satisfaction questionnaire were assessed at baseline, 6 months and 24 months postoperatively. Pes planus angles measured were the talonavicular coverage angle (TNCA), lateral talus-first metatarsal angle (Meary’s angle) and lateral talocalcaneal angle (LTCA). The cohort was stratified into controls (0°-4.0°), mild (4.1°-14.9°), moderate (15.0°-30.0°) and severe (>30.0°) pes planus groups according to Meary’s angle. Clinical outcomes were compared among the groups. Multiple regression was used to determine association between pes planus angles and outcomes.
Results: There were 78 controls, 95 mild, 18 moderate and no severe cases of pes planus. Meary’s angle was independently associated with preoperative HVA (beta 0.408, 95% CI 0.104-0.712, P =.009). Patients with mild and moderate pes planus had significantly greater preoperative HVA (P <.001) compared to controls. Pes planus angles were not associated with pre- or postoperative VAS, AOFAS score, SF-36 PCS or SF-36 MCS. Among controls, mild and moderate pes planus groups, there were no significant differences in pre- or postoperative clinical scores (Table 1), and satisfaction was 84.6, 80.0% and 77.8%, respectively (P =.667).
Conclusion: Patients with increasing severity of pes planus presented with greater severity of hallux valgus deformity. However, patients with pes planus had similar pre- and postoperative clinical outcomes and satisfaction after hallux valgus surgery in comparison to patients with neutral foot arches.
DOI: 10.1177/2473011421S00469
Peritalar Kinematics Restored with Combined Subtalar Fusion and Medial Ligament Reconstruction in a Simulated Advance Progressive Collapsing Flatfoot Deformity Model
Nahom Tecle; Irvin Oh, MD; Emma Gira; Hani A. Awad, PhD
Introduction/Purpose: Progressive collapsing flatfoot deformity (PCFD) leads to a disruption of the medial peritalar ligaments with progressive loss of the medial arch and further valgus alignment of the subtalar and tibiotalar joints. This ultimately leads to peritalar instability with subtalar and tibiotalar osteoarthritis. Conventional joint sparing reconstruction methods alone may not correct the valgus heel alignment. Some have suggested subtalar fusion (SF) with or without combined medializing calcaneal osteotomy (MCO) as an option. Although SF provides a more effective correction of hindfoot alignment, a resultant increase in valgus moment arm with a larger strain on the medial ankle ligament has been reported. The study aim is to investigate the efficacy of a combined MCO with SF and medial tibionavicular ligament (TNL) reconstruction on restoring peritalar stability.
Methods: Ten fresh-frozen cadaveric foot specimens were employed to create a severe PCFD model. Reflective markers were placed on the tibia, talus, navicular, calcaneus, and first metatarsal. A multiple-camera motion capture system (OptiTrack, Prime13) was utilized to document peritalar joint kinematics. Severe AAFD model was created by sectioning the medial capsuloligamentous complex followed by cyclic axial loading. Sequential surgical procedures were performed, including MCO, SF, MCO + SF, and MCO + SF + medial tibionavicular ligament (TNL) reconstruction. Subtalar joint coronal angle, tibiotalar coronal angle, forefoot abduction axial angle, and talo-first metatarsus (Meary’s) lateral angle were calculated for each sequential procedure and compared to the severe flatfoot model. The kinematic changes were calculated between groups utilizing a custom MatLab code and statistical significance was determined using a one-way ANOVA and a Tukey’s multiple comparison test.
Results: The subtalar joint valgus angle of the severe PCFD model (mean 8.1°) was significantly reduced by the MCO+SF+TNL reconstruction (mean 3.2°, p = 0.019). The tibiotalar joint valgus angle of the severe flatfoot model (mean 4.4°) was significantly reduced by the MCO (mean 1.0°, p = 0.04), but increased after combined MCO with SF (mean 2.5°, p = 0.01). The increased valgus tibiotalar angle of the MCO+SF was reduced by adding TNL reconstruction (mean 0.75°, p = 0.027). Forefoot abduction angle was found to be significantly reduced in all reconstruction methods compared to the severe flatfoot model. Meary’s angle was also significantly improved after the MCO+SF and MCO+SF+TNL reconstruction (P= 0.015 and 0.006, respectively).
Conclusion: Although addition of SF to MCO improved forefoot abduction and Meary’s angles of advanced PCFD model, it resulted in increased tibiotalar valgus angle. The subsequent increase in medial ligament strain may be reduced by adding TNL reconstruction which can support medial stability while improve kinematics in all planes. Addition of TNL may be considered when performing SF for correction of PCFD, especially when a residual valgus heel alignment remains.
DOI: 10.1177/2473011421S00470
Quantitative Evaluation of Ankle Instability Using a Capacitance-Type Strain Sensor
Introduction/Purpose: Manual evaluation is an important method for assessing ankle instability, but it is not quantitative. Capacitance-type sensors can be used to measure the distance on the basis of the capacitance value. We applied the sensor to the noninvasive device for measuring ankle instability and showed its utility.
Methods: First, five ankles embalmed by Thiel’s method were used in an experiment using a cadaver. The capacitance-type sensor was fixed alongside the anterior talofibular ligament (ATFL) of a specially made brace, and the anterior drawer test was performed. The test had been performed for the intact ankle, with the ATFL transected, and with both the ATFL and calcaneofibular ligament (CFL) transected. The anterior drawer distance was calculated by the sensor. Intra and interinvestigator reliability were also analyzed. Next, as a clinical study, a brace with a sensor was fitted to 22 ankles of 20 patients with a history of ankle sprain. An anterior drawer test at a load of 150 N was conducted using a Telos stress device. The anterior drawer distances measured by the sensor and based on X-ray images were then compared.
Results: The mean anterior drawer distance for the intact cadavers was 3.7 +- 1.0 mm, 6.1 +- 1.6 mm with the ATFL transected (P < 0.001), and 7.9 +- 1.8 mm with the ATFL and CFL transected (P < 0.001). The intrainvestigator intraclass correlation coefficients (ICC) were 0.862-0.939, and the interinvestigator ICC was 0.815. In the experiments on patients, the mean anterior drawer distance measured by the sensor was 2.9 +- 0.9 mm and 2.7 +- 0.9 mm from the X-ray images. The correlation coefficient between the sensor and the X-ray images was 0.843.
Conclusion: We carried out a quantitative evaluation of anterior drawer laxity using a capacitance-type sensor and found it had high reproducibility. It was also very strongly correlated with stress radiography measurements in patients with ankle instability. Capacitance-type sensors can be used for the safe, simple, and accurate evaluation of ankle instability.
DOI: 10.1177/2473011421S00471
Surgical Takedown Approaches to Insertional Achilles Tendinopathy: A Systematic Review
John M. Thompson; Antonio M. Malloy McCoy; Kevin N. Nguyen; Dominick Casciato, DPM; Eric So, DPM; Mark A. Prissel, DPM; Jaime A. Ahluwalia; Tyler Tewilliager
Introduction/Purpose: Various techniques of surgical detachment for treatment of insertional Achilles tendinopathy have been described, including lateral release, medial release, central tendon splitting (CTS), and complete detachment.
Methods: A systematic review of electronic databases was performed, encompassing 17 studies involving 703 patients and 746 feet, to compare outcomes associated with surgical takedown techniques.
Results: Observed results include wound complication rates (CTS 2.8%; Lateral 0%; Medial 0.4%; Complete 1.3%), post-operative rupture rates (CTS 0.7%; Lateral 0.8%; Medial 0.7%; Complete 2.6%), rate of revision (CTS 0.4%; Lateral 0.9%; Medial 4.2%; Complete 2.6%), rate of infection (CTS 1.1%; Lateral 1.7%; Medial 3.7%; Complete 6.5%). Lateral takedown group was found to have a statistically significant lower rate of complications compared to the complete takedown group (p=0.0029).
Conclusion: In light of these results, it is recommended that patient characteristics such as case specific tendon pathology and calcaneal morphology take precedent in determining the surgical approach to Achilles takedown.
DOI: 10.1177/2473011421S00472
Lateral Extensile Approach to the Calcaneus is Safe after Sinus Tarsi Incision: A Report of Two Cases
Thiran Udawatta; Lawrence H. Goodnough; Stephen K. Benirschke, MD
Introduction/Purpose: While the optimal surgical approach for operative treatment of calcaneus fractures is controversial. Regardless of index approach, post-injury sequelae such as malunion may require subsequent extensile exposures for reconstruction. In the tenuous soft tissues overlying the Whether a lateral extensile approach is safe following a previous sinus tarsi exposure has yet to be demonstrated.
Methods: In this case report, two individuals underwent an initial sinus tarsi approach for reduction and fixation of calcaneus fractures, but went on to malunion or subtalar arthritis. A ’sham' surgery consisting of skin incision and initial flap elevation was performed to evaluate the efficacy of a lateral extensile approach to the calcaneus after previous sinus tarsi incision.
Results: In each instance, the patients experienced uneventful skin incision healing, and subsequently had successful reconstruction with distraction subtalar arthrodesis via lateral extensile exposures.
Conclusion: The lateral extensile approach to the calcaneus may be safely performed following sinus tarsi exposure.
DOI: 10.1177/2473011421S00473
Accuracy of CT Derived Patient Specific Instrumentation for Total Ankle Arthroplasty: The Impact of the Severity of Preoperative Varus Ankle Deformity
Benjamin D. Umbel, DO; Devon Myers, DO; Taylor Hockman; B. Dale Sharpe, Jr., DO; Gregory C. Berlet, MD
Category: Ankle; Ankle Arthritis
Keywords: Ankle Arthroplasty; Total Ankle Arthroplasty; End-Stage Ankle Arthritis
Introduction/Purpose: Significant preoperative varus tibiotalar deformity was once believed to be a contraindication to performing total ankle arthroplasty (TAA). While correction of ankle deformity has been shown to be possible, the ability to restore neutral alignment in more severe ankle arthritis is still a concern. Preoperative CT derived navigation is gaining popularity for its ability to accurately restore neutral alignment in TAA, in addition to decreasing operative and fluoroscopic times. The primary goal of this study was to evaluate whether accuracy and reproducibility of final implant positioning using patient specific guides were influenced as varus deformity became more severe in patients undergoing TAA.
Methods: A retrospective review of 32 patients with varus end-stage ankle arthritis who underwent TAA utilizing total ankle implants with CT derived patient-specific guides was conducted. Preoperative computed tomography (CT) scans were obtained to assess coronal plane deformity, mechanical and anatomic alignment, and build patient-specific guides that referenced bony anatomy. Preoperative weightbearing radiographs were used to measure the tibiotalar and talar tilt angles to assess coronal plane deformity severity and congruency, respectively. Patients were subcategorized into varying degrees of deformity based on their tibiotalar angles (<0-5° neutral, 6-10° mild, 11-15° moderate, and >15° severe). The first postoperative weightbearing radiograph following surgery was used to measure coronal plane alignment of the tibial implant relative to the target axis determined by the preoperative CT template.
Results: The average preoperative varus deformity, as determined by the tibiotalar angle, was 6.06° (range: 0.66- 16.3°) for the entire cohort. Average preoperative varus deformity was 2.63° for the 'neutral' group, 7.64° for the mild group, 11.5° for the moderate group and 16.3° for the severe group. Postoperative weightbearing alignments for 96.9% (30/31) of patients demonstrated neutral implant alignment (< 5°). Relative to the CT derived target axis, the average tibial implant coronal deviation for all patients was 1.54° (range: 0.17-5.7°). The average postoperative coronal alignment relative to the target axis was 1.61° for the neutral group, 1.78° for the mild group, 0.94° for the moderate group, and 1.41° for the severe group. There was no statistically significant difference in final implant alignment relative to the target axis between deformity subgroups (p= 0.256).
Conclusion: The results of our study further support that neutral postoperative TAA alignment can repeatably be obtained using preoperative CT derived patient specific instrumentation (PSI). Furthermore, the accuracy and reproducibility of achieving neutral postoperative radiographic alignment with PSI does not appear to be impacted by worsening varus ankle deformity. All but one patient (96.9%) achieved neutral postoperative alignment relative to the predicted target axis, with the only outlier being from the mild deformity subgroup. Future studies are warranted assessing the effect that even greater coronal plane deformity (>20 °) has on the accuracy of TAA implantation using PSI.
DOI: 10.1177/2473011421S00474
Early Results of A Nitinol Dynamic Compression Nail for Subtalar Joint Arthrodesis vs Two-Screw Fixation Construct
Benjamin D. Umbel, DO; Antonio M. Malloy McCoy; Mitchell Thompson; Devon Consul, DPM; Gregory C. Berlet, MD; Terrence M. Philbin, DO
Introduction/Purpose: Subtalar joint arthrodesis (STJA) for deformity correction and management of arthritis is a common surgery. STJA is a reliable operation with high patient satisfaction scores. Securing the talus to the calcaneus, so as to optimize the physiologic environment for osseous healing, has been achieved with multiple fixation techniques including one, two, and three screw constructs, plates, and staples. The goal of our study is to introduce a nitinol nail system with dynamic compression as a novel fixation method for STJA and compare union rates with a standard 2 screw fixation construct. The secondary goal was to assess union rates for this subtalar fusion nail when performed below a previous ipsilateral ankle arthrodesis (AA), with comparison to results from previously published studies.
Methods: From May 2019 through July 2020, 15 consecutive patients treated with a novel nitinol nail for STJA were compared to 27 patients undergoing STJA using a two-screw fixation method. The nail group was subcategorized into cases with (6 patients) or without (9 patients) ipsilateral AA. Concomitant talonavicular joint arthrodesis was also performed in patients from each group when indicated. Arthrodesis sites were augmented with autologous bone graft with or without bone graft substitute in all patients. Standard postoperative protocols were used. Primary outcomes included subtalar joint union rates determined by radiographic and clinical assessment. Perioperative complications were compared between groups. Patient specific risk factors were studied to assess any potential negative effects on STJA union rates.
Results: Overall, the union rates between the nitinol nail group and screw group did not demonstrate any significant difference (87% vs 88.9%). The nail group with ipsilateral AA demonstrated a 67% union rate (4/6) whereas the nail group without previous AA achieved a 100% union rate (9/9). All patients in our study who underwent STJA with associated TNJA went on to union. Union rates were similar in both groups despite the average age of patients in the nail cohort (61.3 years) being greater than the screw cohort (55.4 years). The average age of patients in the nail group with previous AA was 71 years. No significant relationship was seen between smoking, diabetes or alcohol consumption and union rates.
Conclusion: Our data supports the nitinol dynamic compression nail to have superior union rates to the two-screw fixation group when patients with previous AA were excluded (100% vs 88). Our data also indicate that the nitinol nail may provide at least equivalent or better union rates when performed under previous AA when compared to results from prior studies, despite the patients in our group having a much higher average age at the time of surgery. The early results of this nitinol nail for STJA are encouraging and appear to offer an alternative fixation construct with excellent union rates and minimal complications.
DOI: 10.1177/2473011421S00475
Early Results of a Novel Intramedullary Fixation Device for Proximal Fifth Metatarsal Fractures
Benjamin D. Umbel, DO; B. Dale Sharpe, Jr., DO; Taylor Hockman; Terrence M. Philbin, DO
Category: Midfoot/Forefoot; Sports; Trauma
Keywords: Trauma; Intramedullary Nail; Base of Fifth Metatarsal Fractures
Introduction/Purpose: Proximal fifth metatarsal fractures are commonly treated surgically due to their poor healing capacity. While intramedullary screws may be the most popular operative treatment choice, newer fixation methods continue to develop that offer fracture compression in addition to maintenance of length, alignment and rotation. We present a case-series utilizing a novel intramedullary fixation device for proximal fifth metatarsal fractures. To our knowledge, no other study in the literature has assessed the safety and efficacy of this novel fixation method
Methods: A retrospective analysis was performed for 16 patients with proximal fifth metatarsal fractures who underwent fixation with the same novel intramedullary device. Patient charts were reviewed for fracture union, plantar fracture gapping, time to weightbearing, refracture, perioperative complications, and secondary surgeries.
Results: Sixteen patients with an average age of 43.3 years old underwent fixation with this novel device from 2015 to 2020. Mean follow-up was 32.4 weeks. Fifteen of the 16 patients achieved radiographic union at a mean of 8.9 weeks. One patient suffered a non-union. Mean time to full weight-bearing in, and out of, a walking boot was 6.4 and 9.8 weeks, respectively, for healed fractures. Mean plantar fracture gap improved from 1.22 mm to 0.88 mm following surgery. There were zero infections, refractures or hardware complications. Three patients suffered iatrogenic distal diaphyseal fracture during implant insertion, however postoperative progression to weightbearing was not altered in these patients relative to the remainder of the cohort.
Conclusion: To our knowledge, this is the first report of early results for this novel intramedullary device. Excellent union rates, acceptable time to weight bearing, and a low complication profile can be achieved. Additionally, plantar fracture gapping, which has been shown to delay time to union, was improved using this novel implant. Based on our early findings, we propose a viable treatment option that is safe and effective for proximal fifth metatarsal fracture stabilization.
DOI: 10.1177/2473011421S00476
Lateral Patient Positioning for Pilon and Trimalleolar Ankle Fractures
Benjamin D. Umbel, DO; Anthony J. Melaragno; Devon Myers, DO; Taylor Hockman; Christopher Reynolds; Benjamin C. Taylor, MD
Introduction/Purpose: Preoperative planning for pilon and trimalleolar ankle fractures can be difficult. Due to fracture complexity, staged open reduction and internal fixation (ORIF) is performed, resulting in two surgeries. For other situations, definitive fixation occurs with one surgery. However, patients require both prone and supine positioning in order to address all fracture components. Repositioning, re-prepping and re-draping adds to operating room (OR) time and time under anesthesia, increasing the risk for anesthesia related complications. Additionally, repositioning the patient can potentially increase fluoroscopy time and radiation exposure to the patient. Lateral patient positioning obviates many of these concerns. Our study goal was to assess the safety and effectiveness of lateral positioning for pilon and trimalleolar ankle fracture ORIF compared with patients placed in standard positioning (i.e supine/prone).
Methods: This was a retrospective cohort analysis of 41 patients who underwent operative fixation of a pilon or trimalleolar ankle fracture at a single institution level 1 trauma center. This study compared outcome data for those undergoing the procedure in lateral positioning (n=31) vs. standard (prone/supine) positioning (n=10). Exclusion criteria included pregnant women, prisoners, patients with less than 6 weeks of follow-up, previous or bilateral pilon or ankle fracture surgery or patients treated with limited internal fixation and external fixation. Variables collected included patient demographics, time to union, time to weightbearing, complications and any repeat surgeries. Additionally, chart review was performed analyzing OR time, fluoroscopy time and radiation dose to patient.
Results: The patients fixed in the lateral position underwent significantly less time in the OR and subsequent time under anesthesia (p= 0.02). The average OR time in the lateral positioning group was 160 minutes (min) (range: 65-234 min). The average OR time in the standard positioning group was 193 minutes (range: 143- 263 min). Fluoroscopy time was less in the lateral group compared with the standard group (1.47 vs 2.09 min), though this was not statistically significant. Mean patient radiation dose was less in the lateral position group, but without statistical significance (3.22 vs 3.66 mGy). Compared with the standard positioning group, the lateral group demonstrated a significantly shorter time to weightbearing both in (avg 7.8 weeks) and out (avg 11.8 weeks) of the walking boot (p= 0.01). There were no significant differences in complications or time to fracture union.
Conclusion: Our results demonstrated that patients treated in the lateral position progressed in their weightbearing faster without increased risk of complications or delayed union, compared with the standard positioning group. Additionally, perhaps the most intriguing conclusion from our study was that OR time, and therefore time under anesthesia was significantly improved with lateral positioning. Fluoroscopic time and radiation dose exposure were also found to be less on average in the lateral positioning group. Our study suggests that lateral positioning for ORIF of pilon or trimalleolar fractures may not only improve patient safety but also reliably lead to acceptable patient outcomes.
DOI: 10.1177/2473011421S00477
Return to Run Rates Following Hallux Valgus Correction: A Retrospective Comparison of Metatarsal Shaft Osteotomies vs the Modified Lapidus Procedure
Alicia M. Unangst, DO; Paul M. Ryan, MD
Category: Bunion; Other
Keywords: Bunion; Lapidus Procedure; Return to Play
Introduction/Purpose: Hallux valgus affects 23 -36% in general populations. The purpose of this study was to evaluate return to run following either a modified Lapidus procedure or a metatarsal osteotomy. We hypothesized that there would be no difference in the ability to return to running.
Methods: A Retrospective review of a consecutive series of patients at a single institution with surgical correction was performed. 51 patients were identified. 35 were treated with a metatarsal shaft osteotomy and 16 with a modified Lapidus.
Results: No difference was found between the cohorts in terms of age, sex, or pre- operative hallux valgus angle (HVA). 27/35 (77%) with metatarsal shaft osteotomy were able to return to running versus 13/16 (81%) with modified Lapidus. There was no significant difference in the ability to return to running between cohorts (p=1.00).
Conclusion: Our study showed no statistical difference for the modified Lapidus versus metatarsal osteotomies relative to return to running.
DOI: 10.1177/2473011421S00478
Comparison of a Simple Anatomic Landmark-Based Achilles Tendon Measurement with Ultrasound and MRI Measurements
Daniel Urness, BS; Austin R. Thompson, BS; Emelia Sodders; Erik Ensrud; James E. Meeker, MD
Introduction/Purpose: Achilles tendon ruptures (ATRs) occurred with an incidence of 2.5 per 100,000 person-years in 2016. This rate has been increasing over the last decade and it has been postulated that this is due to the increasing activity level of an aging population. With a high and increasing incidence of this significant injury, further investigation must be done to optimize the treatment of ATRs. The degree of tendon lengthening has been correlated with clinical outcomes, with greater elongation being associated with worse outcomes. MRI and ultrasound (US) techniques have been validated in Achilles tendon measurements. We sought to develop a reliable, reproducible, and accurate measurement technique utilizing the manual palpation of anatomic landmarks that will be cost effective as well as convenient to perform, particularly intraoperatively.
Methods: Both lower legs of 10 healthy subjects without history of Achilles tendon injury were examined. For US and anatomic landmark-based (ALB) measurements, subjects' ankles were held at 90o with the lateral aspect of the lower leg resting on the exam table. The length from the medial head of the gastrocnemius to the bottom of the non-compressed heal pad was measured by three raters using the US and ALB techniques. Two of those raters repeated the measurements one week later. MRI studies were obtained with ankles held at 90o. Using imaging software, the above measurements were made in sagittal and coronal series. A repeated measures mixed model method was utilized to model the measurement type and the length of the Achilles tendon. The length of the Achilles tendon measured by each measurement type was estimated with least square means. All pairwise comparisons were considered.
Results: The Achilles tendon length was similar on the left [23.4 cm (95% CL: 22.3 cm, 24.5 cm)] and right [23.5 cm (95% CL: 22.4 cm, 24.6 cm)] legs. The average Achilles tendon length measured with the ALB technique was 23.2 cm (95% CL: 21.9 cm, 24.6 cm). The average Achilles tendon length measured with the US technique was 22.4 cm (95% CL: 21.0, 23.8). The average Achilles tendon length measured on the sagittal view of MRI was 24.1 cm (95% CL: 22.7, 25.4). The average Achilles tendon length measured on the coronal view of MRI was 24.2 cm (95% CL: 22.8, 25.5). Pairwise comparisons of the measurement types were not significantly different from 0.
Conclusion: The ALB measurements were not statistically different from MRI or US. With orthopaedic surgeons in need of simple, noninvasive, and cost-effective methods to assess tendon length, the authors propose this ALB technique or US as valid ways to monitor that variable both during and after repair. These results set the stage for further evaluation of this measurement technique in the operating room in subjects undergoing ATR repair.
DOI: 10.1177/2473011421S00479
For Surgical Treatment of Hallux Limitus Cheilectomy and Recession of the Collateral Ligaments of the Metatarso-Phalangeal Joint Improves Dorsiflexion 30% More Than Cheilectomy Alone
Introduction/Purpose: The goal of surgery for hallux limitus is to relieve pain, correct the dorsal joint impingement and improve ROM, especially MTP joint dorsiflexion. Obtaining increased dorsiflexion can be achieved by bone resection (cheilectomy), ostetomy of the proximal phalanx (Moberg), and soft tissue releases (plantar plate release, capsulotomy, ligament recession). In stiff joints of the hand collateral ligament recession is commonly done to improve motion. The purpose of this study was to evaluate the effect of MTPj collateral ligament recession (in addition to cheilectomy) in improving the range of motion achieved during surgery.
Methods: Twenty consecutive patients undergoing surgical treatment for hallux limitus were studied. A dorsal approach was used and the extensor tendons protected. The dorsal capsule was opened and a cheilectomy was done removing about 25% of the dorsal metatarsal head. The joint was manually distracted and the gap measured with a spacer. Dorsiflexion of the MTP joint was measured. (Historically our goal was to obtain at least 75 degrees of dorsiflexion-more motion achieved by resecting more bone). Recession of the medial and lateral collateral ligaments was then done. Prominent medial or lateral condylar processes were smoothed with a rasp. Dorsiflexion of the MTP joint was again measured. No release of the plantar structures was done. The capsule and skin were closed in standard manner and final motion measured before applying a foot dressing.
Results: The average introperative MTP joint dorsiflexion ROM obtained by chelectomy alone was 65 degrees (range 45 to 90). This motion was measured related to the plantar surface of the foot. The ROM after cheilectomy and collateral ligament recession was 85 degrees or more in all patients. Collateral ligament recession permitted the joint to be distracted (increased 'joint space') and facilitated the conversion of the MTP joint from a gliding to a hinge joint (the mechanical goal of cheilectomy). Also noted was that less bone needed to be resected from the metatarsal head to obtain the desired correction. After resection of any osteophytes from the dorsal proximal phalanx - this surface needed to rest about 5 mm dorsal to the residual surface (after cheilectomy) of the metatarsal head for optimum recovery of motion. This technique now used in all patients (> 150) with same intraoperative findings.
Conclusion: For surgical treatment of hallux limitus cheilectomy plus collateral ligament recession resulted in greater intra- operative dorsiflexion of the MTP joint than cheilectomy alone. Less bone resection from the dorsal metatarsal head was also needed to obtain 85+ degrees of intraoperative correction. Intraoperative ROM is the baseline correction and is related to the surgical techniques used. Maintaining ROM after surgery is very dependent on the patient and the intensity of their rehabilitation commitment-so the last clinical follow up ROM did vary from 30 to 90+ degrees.
DOI: 10.1177/2473011421S00480
Underutilization of Patient Reported Outcomes Data in the Recent Foot and Ankle Literature
Introduction/Purpose: The importance of collecting outcomes information was promoted by Ernest Codman in the early 1900’s. He stated the importance of 'Following every patient treated long enough to determine whether or not the treatment has been successful, then inquire-if so or if not- WHY?', ' He stressed the importance of evaluating outcomes for each patient as an individual and not from groups of patients. Since that time numerous outcomes measures have been validated and are in current use. The purpose of this study was to review all publications in Foot and Ankle International from 2019-2020 which included outcomes data. Then to determine if these principles (use of individual versus group data and WHY treatment was successful or not) were followed.
Methods: All articles published in Foot and Ankle International during 2019-2020 were reviewed. Articles which included patient outcomes data were selected for further review. This review then included assessment of outcomes measure(s) used, organization of outcomes data, utilization of this data by the study, analysis of individual versus group data, and any assessment of WHY the outcomes scores had improved or not.
Results: Eighty-five publications were selected. Eleven different outcomes measurement tools were used. All were reportedy validated tools except for the AOFAS scoring system. Every study reported outcomes data as group means (some with standard deviations, some with range of scores). These studies then compared group means (of different treatment groups or preop vs post op). No specific individual patient outcomes data was provided. There was no specific assessment of WHY scores improved or not. There was also no analysis of individual questions from these outcomes tools (e.g. can you put on your own shoes?--if patient answered 'no' there was no further explanation of why this response was selected). When the range of scores were provided it was common to have scores on the low end of the scale before and after treatment with overall conclusion of improvement based on group means but no assessment of why individual patients improved or not.
Conclusion: Outcomes measures are generally considered to be part of the ’standard of care'. They may be considered important by third party payers, used in evaluation treatment options, and are usually necessary for publication. However trhis data is being underutilized. It is commonly reported as group means +/- range or standard deviations with provides little information about the individuals in a group or groups. Even with methodologies to minimize Type I or II errors evaluation of group means can obscure significant progress, lack of progress, or decline by individual patients. Methods to more effectively utilize outcomes measures are needed.
DOI: 10.1177/2473011421S00481
Does Surgical Placement of Syndesmosis Screws Affect Breakage Rate? A Retrospective Comparative Study
Josh W. Vander Maten, MS; Matt McCraken, MS; Logan Roebke, BS; Jiayong Liu
Introduction/Purpose: Fixation of syndesmosis disruption with metal screws remains a frequent and efficacious treatment modality. Screw breakage remains a complication seen in many patients following metal fixation. Overtime physiologic rotation or the tibia and fibula can lead to bone erosion and pain in patients with screw breakage. The purpose of this study is to compare patients with syndesmosis screw breakage and patients with intact screws based surgically controlled variables.
Methods: A retrospective analysis of patients who underwent syndesmotic screw fixation from 2008 - 2020 was performed. Ninety-seven patients were found to have syndesmosis screw breakage, of which 88 met inclusion criteria. A control group of patients without syndesmosis screw breakage was selected at random and analyzed until 88 patients met inclusion criteria. The number of screws used, width, length, fracture type and number of cortices were all collected. Further analysis included radiographic measurement syndesmosis screw angle and height of placement above the tibial plafond. A regression analysis was performed to compare to the two groups, including a separate analysis comparing unbroken screws within syndesmosis screw breakage cohort versus their broken screws, as this provided an absolute control group. A stratified analysis of screw placement and angle was also performed based on standard deviation.
Results: The average screw width in the breakage group was 3.67 (SD =.38) and 4.06 (SD =0.04) in the intact group (P =<.001). Average screw angle was 94.82 (SD = 12.75) in the breakage group and 94.67 (SD 12.31) in the intact group (based on 90 degrees relative to tibial plafond). Screw placement of the tibial plafond was 20.39 (SD =10.389) in the breakage group and 16. 75 (SD = 9.28) in the intact group. 70.3% of broken screws were placed > 20mm above the tibial plafond, compared to 64.0% in the control group. Most screws were placed at angle > 82 degrees relative to the tibial plafond; 76% (n =92) of broken screws and 81.2% (n=211) of intact screws). Decreased screw width (P =<.001) and screw placement > 20mm above the tibial plafond (P =<.001) were all associated with an increased risk of screw breakage.
Conclusion: Metal screw fixation remains an efficacious treatment method of syndesmotic disruption. Despite extensive research the cause of syndesmosis screw breakage and the necessity of screw removal remains without consensus. The is study aims to analyze surgical variables in attempt to find correlation with screw breakage. An increased BMI was seen to predispose to screw breakage. Placement of the syndesmosis screw <20 mm above the tibial plafond and increased screw width provide protection against syndesmosis breakage. No significant differences were found between groups based on screw angle, number of cortices, screw length, or number of screws used.
DOI: 10.1177/2473011421S00482
Does Syndesmosis Screw Breakage Affect Patient Outcomes? A Retrospective Comparative Study
Josh W. Vander Maten, MS; Matt McCraken, MS; Jiayong Liu; Logan Roebke, BS
Category: Ankle
Keywords: Ankle; Screws; Outcomes Measures
Introduction/Purpose: Metal screw fixation remains a common and effective way to repair syndesmotic injuries. They are inexpensive, familiar, and provide superior torsional resistance to sagittal translation compared to other fixation modalities. Symptomatic screw breakage is one of the most common complications of metal screw fixation. Routine removal remains unsupported by literature. Consequently, many patients retain broken screws and are at risk for pain; particularly when the breakage occurs within the tibia or the fibula. The purpose of this study is to analyze outcomes of patients with intact syndesmosis screws and those with syndesmosis screw breakage.
Methods: A total of 176 patients (260 screws) with syndesmotic disruption treated with syndesmosis screw fixation were included in the study. Half of the patients had broken syndesmosis screws while the other half had intact syndesmosis screws. Basic patient demographic data was collected including BMI, age, and gender. Further collection of patient comorbidities was compiled using two comorbidity indices (Charlson, Elixhauser). Outcome analysis included revision rate, removal secondary to pain, complication rate, range of motion deficits, and patient pain scores. In patients who had their screws removed, further analysis was conducted to compare strength, range of motion deficits, complication rates, pain scores and revision rates between the intact and breakage group.
Results: BMI averages of 33.64 (SD=8.77) and 30.64 (SD=6.76) were seen in breakage and intact group, respectively. A complication rate of 24.0% was seen the breakage group versus 36.1% in the control group. Revision rates of 12.4% and 20.10% were seen in the breakage and control group, respectively. Range of motion deficits were seen in 50.2% in the intact group and 39.7% in the breakage group (P = 0.2253). Removal secondary to pain occurred in 60.30% (n = 73) in the broken group compared to 24.5% (n = 34) in the control group. Decreased complication rate (P =.002), increased BMI (P = <.001), and increased risk of removal secondary to pain (P = <.001) were all associated with screw breakage. Following screw removal, no difference was seen in range of motion, pain scores (P =.003) and complications rates (P = 0.147) were higher in the intact group.
Conclusion: Metal screw fixation remains a popular treatment of syndesmotic disruption. Many patients retain broken screws and intact screws which can be associated with future complications. Patients with syndesmosis screw breakage are a high comorbid population. Syndesmosis screw breakage is associated with decreased complication rates, increased BMI, and increased risk of eventual removal secondary to pain. Range of motion deficits were seen more commonly when in patients with intact syndesmosis screws. Additionally, revisions rates were higher in the intact group compared to the breakage group. Following screw removal, the intact group had a non-statistically significant increase in complication rate and range.
DOI: 10.1177/2473011421S00483
Location Matters in Syndesmosis Screw Breakage: Interosseous Breakage and Breakage Location Within the Tibia Affect Rates of Removal Secondary to Pain
Josh W. Vander Maten, MS; Jiayong Liu; Matt McCraken, MS; Logan Roebke, BS
Category: Ankle; Ankle; Trauma
Keywords: Syndesmosis; Pain; Screws
Introduction/Purpose: Broken or loose syndesmotic screws are typically reported to be clinically asymptomatic, however, screw breakage can lead to significant pain depending on location. Syndesmosis screws that span the incisura are particularly at an increased risk for painful outcomes. In patients with intraosseous screw breakage, normal physiologic translation where the distal convex of the fibula fits into the concave tibial incisure can lead to painful bony erosion overtime. The purpose of this investigation is to assess variables that my predict location of syndesmosis screw breakage and to also assess the effect of screw breakage location on eventual removal secondary to pain.
Methods: A retrospective analysis of 1,056 patients who underwent syndesmosis fixation revealed 88 patients (121 screws) who experienced pst-operative syndesmosis screw breakage and met predetermined inclusion criteria. Patient demographic data, BMI, comorbidities, pain scores, complication rate, and revision rate were all collected. Screw length, width, number, placement height above the tibial plafond, angle, location of breakage, breakage distance location on the screw and implant removal secondary to pain were also collected. A series of binomial logistic regressions were performed to ascertain the effects of the collected variables on the likelihood of breakage location and removal secondary to pain. Regression analysis included intraosseous versus clear space breakage, tibia versus fibula breakage, and removal secondary to pain in each breakage location group (tibia, fibula, clear space).
Results: Of the 121 broken screws, 91 (75.2%) broke within an intraosseous (IO) location (68 patients, 77.3%). Twenty-eight screws (23%.1) (18 patients, 20.5%) broke exclusively within the clear space (CS). Sixty screws (52 patients, 59.9%), had IO breakage within the tibia, while 29 screws (24 patients 27.7%) had breakage within the fibula. Two screws (2 patients, 2.27%) occurred within an intraosseous location and the clear space. Intraosseous screw breakage was associated with higher risk removal secondary to pain (P=.020). Multiple screw usage associated with an increased risk for CS breakage (P =.012). IO and CS screw angle and placement had no effect on screw breakage location (P =.629, P =.570). Screw breakage closer to the CS (P=.001), increased number of screws used (P=.003), and higher patient pain scores (P =.003) were associated increased risk of removal due to pain within the IO tibia breakage group.
Conclusion: Syndesmotic screw breakage location plays a more important role than previously reported. When compared to clear space, intraosseous breakage is associated with increased rates of removal due to pain. Breakage location within the tibia occurring closer to the clear space is associated with higher rates of removal secondary to pain and higher patient report pain scores. Usage of multiple screws was found to be the only significant predictor of clear space vs intraosseous breakage; all other variables were found to be non-contributary, including no appreciated significance of screw placement in relation to the tibial plafond or screw angle.
DOI: 10.1177/2473011421S00484
Valgus Drift after Total Ankle Arthroplasty
David Vier, MD; Rasikh N. Hamid; Susan M. Odum, PhD; Carroll P. Jones, III, MD; Bruce E. Cohen, MD; Todd A. Irwin, MD;
W. Hodges Davis, MD
Introduction/Purpose: Total ankle arthroplasty (TAA) is a common treatment for ankle arthritis, but many challenges exist when attempting to correct and balance coronal plane deformity. Varus ankle arthritis tends to be stiffer and often leads to a more stable TAA, but valgus ankle arthritis tends to have more laxity especially in the setting of a progressive collapsing foot deformity. Failure to achieve appropriate deformity correction and soft tissue balance can result in recurrence of the deformity with valgus drift. The purpose of this study was to evaluate the longitudinal coronal plane alignment as well as outcomes in patients treated with TAA with resultant valgus drift.
Methods: 98 patients who underwent TAA for valgus ankle arthritis were identified through a prospectively collected database. All patients had a minimum of 2 year follow-up. The tibiotalar angle was measured on preoperative radiographs to include patients with valgus ankle arthritis five degrees or greater. Radiographic alignment in the postoperative period was compared to the alignment at final follow-up. Complications, failures, revisions, and reoperations were recorded. Patients were categorized by severity of preoperative valgus deformity into 3 groups: 5-10 degrees, 11-20 degrees, and greater than 20 degrees. Valgus drift was defined as greater than 5 degrees of valgus shift at final follow-up when compared to the postoperative alignment. Median follow- up was 49.2 (37.2-68.3 inner quartile) months.
Results: Patients with greater than 20 degrees of preoperative valgus deformity had an initial postoperative alignment of 2 degrees of valgus and ended with an average of 5.5 degrees of valgus at final follow-up. The groups of patients with 5-10 degrees as well as 11-20 degrees of valgus were corrected to neutral (0 degrees) in the initial post-op period and ended with a final postoperative valgus alignment of 2.5 degrees and 2 degrees, respectively. Overall, 16 patients (18%) had greater than 5 degrees of valgus drift after their surgery, of which 2 failed and were revised (13%) and 5 had reoperations (31%).
Conclusion: All groups of preoperative valgus deformity severity had some valgus shift overall at final follow-up. The most severe preoperative valgus deformities were least likely to be corrected to neutral with the index procedure and also on average drifted back to over 5 degrees of valgus. Patients with valgus drift after TAA can still have a good result but should be monitored closely. Overall, they did not have a high failure rate. This study emphasizes the necessity of correcting both the ankle and foot deformity when performing TAA for valgus ankle arthritis in order to maintain deformity correction.
DOI: 10.1177/2473011421S00485
An Oblique Trans-Syndesmotic Screw to Augment Fixation of Distal Fibula Fractures: A Technique Guide
Eric D. Villarreal, MD; Carson D. Strickland, MD; David R. Richardson, MD
Introduction/Purpose: A subset of patients with low, transverse fractures of the lateral malleolus are at increased risk of malreduction and late loss of reduction. In patients with poor bone quality and transverse or short oblique fractures at or distal to the tibiotalar joint, distal fixation is often inadequate with a single interfragmentary lag screw. Furthermore, these fractures are susceptible to malreduction by pre-contoured locking plates. To address this, a technique was developed to augment fixation of the distal fragment and decrease the likelihood of loss of reduction. The senior author’s technique for this procedure, as well as indications for the technique and a few representative cases, are provided.
Methods: This technique involves placement of an oblique tricortical or quadricortical screw from the distal fibula into the tibia in an distal-lateral to proximal-medial direction. The screw is placed either outside of or through the distal-most hole of a one-third tubular plate placed in a neutralization position. The screw trajectory is similar to that of a typical syndesmosis screw in the sagittal plane but is aimed proximally rather than parallel to the tibial plafond. The screw enters the tibia at Chaput’s tubercle, just lateral to the joint. The indications for this technique are transverse and short oblique Danis-Weber B distal fibular fractures in which there is inadequate purchase between the plate and the distal fragment. While the purpose of this screw is not to stabilize the syndesmosis, it can be used with other augmentation techniques, such as trans-syndesmotic screws, in high-risk patients with osteoporosis and/or neuropathy.
Results: This technique has been used for many years by the senior author. There have been no implant failures (e.g. broken screws) or major complications associated with this technique. Three representative cases demonstrate appropriate indications and outcomes for this technique. These include patients with significant neuropathy or osteoporosis who present with a particularly troublesome fracture pattern (transverse fibular fracture at or below the level of the tibiotalar joint). This screw, along with any other syndesmotic screws, is removed at 3-4 months according to the senior author’s protocol.
Conclusion: A distal oblique trans-syndesmotic screw can be used to supplement current fibular fracture fixation constructs. It is easy to place under fluoroscopic guidance and generally is removed after fracture union, similar to standard syndesmosis screws. The use of this screw helps prevent the malreduction that can potentially occur when treating transverse or short-oblique Weber B distal fibular fractures with a locking plate. In our series of patients at a large urban tertiary referral center, this technique has produced good outcomes with no reportable complications.
DOI: 10.1177/2473011421S00486
Defining Return to Sport: A Systematic Review
Bryan G. Vopat, MD; Joshua Doege, MS; Jack M. Ayres; Matthew Mackay, MD; Armin Tarakemeh, BA; Symone M. Brown, BS; Mary K. Mulcahey, MD
Category: Sports
Keywords: Return to Play; Sports; Outcomes Measures
Introduction/Purpose: Return to sport (RTS) commonly serves as a measure for assessment of clinical outcomes in orthopaedic sports medicine surgery. Unfortunately, while RTS is commonly utilized in research for this purpose, currently, there is no widely accepted or standardized definition for when an athlete has officially returned to his or her sport. The purpose of this study was to conduct a systematic review to evaluate and report the differences in specific definitions of return to sport (RTS) utilized in the orthopaedic surgery literature.
Methods: A systematic review was performed using PubMed, Embase and Cochrane databases per PRISMA guidelines. Search terms consisted of variations of 'RTS' combined with variations of 'orthopedic surgery' and 'define' to capture as many relevant articles as possible. The definition of return to sport was recorded and analyzed.
Results: 718 articles were identified in the initial search, 29 of which met eligibility criteria, providing a clear definition of RTS. Of the 29 studies included, 20 (69.0%) defined RTS as an athlete competing in a game or other competitive play, and these definitions are further broken down in Table 1. Three (10.3%) defined this as the athlete competing in a game or other competitive play, but with an explicitly stated competition-level modifier of the athlete returning to their pre-injury level of competition. Two articles (6.9%) included returning to training or practice and the remaining four articles (13.8%) used terminology other than the standard RTS.
Conclusion: There is variability in the definition of RTS used in the literature. Most studies refer to the athlete competing in a game or other competitive play. Other variants include returning to practice/training and explicitly defined competition levels and objectives. Future studies should aim to standardize the definition of RTS to facilitate more precise assessment of outcome following sports medicine surgery. Using terminology that describes components of the recovery and rehabilitation process, such as 'return to participation' and 'return to performance' in addition to RTS will allow us to better understand the athlete’s recovery and associated level of competition or performance.
DOI: 10.1177/2473011421S00487
Traumatic Peroneal Nerve Injuries: A Systematic Review
Bryan G. Vopat, MD; Matthew Mackay, MD; Jack M. Ayres; Ian Harmon, BS; Armin Tarakemeh, BA; Jacob Brubacher, MD
Category: Trauma
Keywords: Trauma; Fibula Fractures; Tendon Transfer
Introduction/Purpose: The common peroneal nerve (CPN) is the most commonly injured peripheral nerve of the lower extremity in trauma patients. Traumatic CPN injuries have historically been associated with relatively poor outcomes and patient satisfaction, though recent outcome data appear promising. Given the variety of underlying injury modalities, treatment options, and prognostic variables, this study sought to evaluate and summarize current literature on traumatic CPN injuries and provide recommendations for treatment and future research.
Methods: A systematic review was performed using PubMed, Embase and Cochrane databases per PRISMA guidelines. Search terms consisted of variations of 'peroneal nerve' and 'fibular nerve' combined with 'injury,' or 'laceration,' or 'entrapment,' or 'repair,' or 'neurolysis.' Information regarding treatment modality, outcomes and patient demographics were recorded and analyzed.
Results: 2,301 articles were identified in the initial search, 42 met eligibility criteria (Figure 1). Factors associated with better clinical outcomes included shorter pre-operative interval, shorter graft length when an interposed graft was used, nerve continuity and younger patient age. Sex or gender did not affect outcomes in any studies in this review. Motor grades of M3 or greater on the MRC scale are typically considered successful outcomes. In studies we analyzed, this was achieved in 81.2% of patients who underwent neurolysis, 78.8% of patients who underwent end to end suture, 49.8% of patients who underwent nerve grafting, 62.9% of patients who underwent nerve transfer, 86.0% of patients who underwent posterior tibial tendon transfer (PTTT) and 73.9% of patients who underwent surgery with concurrent PTTT.
Conclusion: Included studies were heterogenous, complicating our ability to further analyze the data. It is not possible to uniformly advocate for the best treatment option given diverse injury modalities, presentations and prognostic factors. Many studies do not report outcomes with respect to specific injury modality. Future studies should clearly report outcomes based on injury modality and surgical treatment option. This would allow for greater analysis on the most appropriate treatment option for a given mechanism of injury. Newer surgical techniques, such as addition of growth factors to nerve repairs and concurrent tendon transfer are promising and should be further explored.
DOI: 10.1177/2473011421S00488
Importance of Midfoot Ligaments in a Hallux Valgus Cadaveric Model
Emilio Wagner, MD; Pablo Wagner, MD; Florencia Pacheco, MD; Mario López; Felipe H. Palma, PT; Rodrigo Guzman- Venegas, MSc
Category: Bunion
Keywords: Bunion; Ligament; Hallux Valgus
Introduction/Purpose: Hallux valgus (HV) is of uncertain origin. Even though a huge amount of treatment options are available, no clear cause for this deformity exist. To be able to further understand this frequent pathology, a cadaveric model should be developed. A cadaveric model was developed trying to obtain similar deformities to the ones observed in Hallux valgus (first ray varus and pronation). The objective of this research is to recreate some characteristics of a HV deformity, through sequential ligaments sectioning.
Methods: 8 fresh frozen lower leg specimens were used. Markers were attached to the medial and middle foot ray bones, including talus. A constant tibial axial load of 25 kg was used. Cyclic tibial rotation (to simulate gait phases) and 5 kg pull on the extensor and flexor hallucis tendons (EHL and FHL) were applied to the specimen. Limited and sequential medial and middle column ligamentous sectioning were performed, including the, dorsal and interosseous naviculo-cuneiform, intercuneiform, metatarso-cuneiform and intermetatarsal ligaments. After each ligament damage, bony alignment was measured including frontal (bone divergence) and axial plane (bone rotation).
Results: After intercuneiform, Lisfranc and naviculo-cuneiform ligaments sectioning, a significant angular increase was found in the naviculo-cuneiform, intercuneiform and naviculo-metatarsal angles (p=0.001). Specifically, for bone rotation, the biggest change was found for the intercuneiform and naviculo-cuneiform angles. Regarding bone divergence, the biggest increase was found in the talo-metatarsal angle. No additional angular change was found after adding metatarso-cuneiform ligament damage. No change in the sagittal alignment was found.
Conclusion: This model was able to recreate some parameters of the hallux valgus deformity. No flatfoot deformity was produced. Surprisingly, no significant angular change was produced after metatarso-cuneiform ligament damage. Most significant changes were found after intercuneiform and naviculocuneiform damage. Our findings suggest that midfoot instability has to be present to recreate a hallux valgus deformity.
DOI: 10.1177/2473011421S00489
Short Term Results of Treatment of Osteomyelitis in the Diabetic Foot with a Synthetic Bone Graft Sustitute
Introduction/Purpose: The aim of the study was to evaluate short term results of osteomyelits of the diabetic foot treated with cerament
Methods: 16 diabetics with a mean age of 61.6 years underwent surgical therapy of infection of the foot using Cerament and a 6- week resistance-based antibiotic therapy. The surgical procedures included bony debridement, temporary vacuum therapy, arthrodesis or resection arthroplasty. Postoperative treatment included clinical investigation and MRI control of the affected foot. The foot ulcerations were classified preoperatively. Pathological assessments of osteomyelitis were made. The recurrence rates of osteomyelitis and ulcerations, the number of surgical procedures, and the complication rates were determined.
Results: A foot ulcer was found preoperatively in 56.3% of the patients. 10 patients (62.5%) were diagnosed with chronic osteomyelitis, 6 with florid osteomyelitis. The number of necessary surgical procedures was 2 in 8 patients (50%), 4 in 4 patients (25%), 3 in 3 patients (18.8%) and 1 in 1 patient (6.3%). After a median followup of 8.6 months, no recurrence of osteomyelitis could be detected in 13 patients (81.3%). With regard to foot ulcerations, the ulcer healed completely in 15 patients (93.8%). One patient had ulcer recurrence. The complication rate was 18.8% (3 patients). The statistical analysis also showed that the patient’s age had no significant influence on the recurrence rate of osteomyelitis and ulceration.Furthermore, there were significant differences between patients with chronic and florid osteomyelitis. Patients with chronic osteomyelitis were more likely to have osteomyelitis recurrences, while patients with a proven florid infection were more likely to have ulcer recurrences.
Conclusion: The osteomyelitis treatment of the diabetic foot shows good results in terms of the recurrence rates of osteomyelitis and foot ulceration. With regard to the differentiated consideration of the results in chronic and florid osteomyelitis, additional investigations are necessary.
DOI: 10.1177/2473011421S00490
The Infected Diabetic Foot: A Microbiological Analysis
Introduction/Purpose: Diabetic foot infections show increasing prevalence. Their therapy is time consuming and expensive. Standardized antibiotic treatments do not exist. Suboptimal antibiotic therapy increases the morbidity of the patient. The aim of the study was to evaluate the dominating bacterial colonization in the diabetic foot. Furthermore we evaluated the changes of the colonization during surgical and antibiotic treatment and the efficiency of the therapy.
Methods: The study included 100 patients with a diabetic foot syndrome and a pedal ulcer. Ulcers were classified according to Wagner Classification. HbA1c, CRP and patients BMI were documented. All patients underwent an angiologic investigation with arterial doppler ultrasonography and TcpO2 measurement. An MRI of the affected foot was performed to rule out osteomyelitis. All patients underwent surgical and antibiotic treatment. Surgery included debridement, abscess drainage, VAK therapy, bony resection, minor amputation, resection arthroplasty, Helal osteotomies. Osteomyelitis was pathologically verified. Microbiological results of superficial and deep smears, which were taken during the surgical therapy were analyzed. The antibiotic treatment was adapted to the bacterial resistance.
Results: The duration of antibiotic treatment varied from 1 to 136 days (Mean:19.6 days, SD:17.3 ). The mean number of surgical interventions was 2.6. The dominating initial antibiotic treatment was Clindamycin/ Cefuroxim (48%) followed by Clindamycin (11%),Cefuroxim (7%), Clindamycin/ Ciprofloxacin (6%), Tazobactam (3%). The dominating bacteria were gram +. The difference of the percentage distribution compared to the gram- bacteria was statistically significant. The only significant percentage change of the antibiotic treatment was seen after the first surgical intervention, when the initial antibiotic treatment was significantly more effective against gram - bacteria. A change of the antibiotic treatment was seen with 1. Clindamycin / Ciprofloxacin in 66%, 2. Tazobactam in 67%, 3.Clindamycin in 36% and Clindamycin/ Cefuroxim in 35%.
Conclusion: The dominating bacteria of the infected diabetic feet were gram +. The initial i.v. antibiotic treatment with Clindamycin/ Cefuroxim was effective in 66%. An optimization of the initial antibiotic treatment with greater focus on the gram + bacteria seems to be necessary.
DOI: 10.1177/2473011421S00491
Anterior Ankle Skin Surface Pressures in Lower Extremity Splints: Minimizing Insult after Injury
David M. Walton, MD; Nicholas Farrar, MD; Kameron A. Shams, MD; Kristopher Mell; James R. Holmes, MD; Paul G. Talusan, MD
Category: Ankle; Trauma; Other
Keywords: Dressing; Complications; Ankle
Introduction/Purpose: Though ubiquitously utilized in orthopaedic trauma, lower extremity splints are not without their associated iatrogenic risk of morbidity. In fact, improper splinting not only necessitates replacement, but splint-related soft tissue complications are the second most common iatrogenic cause for referral to plastic surgery. Improper splinting techniques include inadequate molding of plaster/fiberglass splints, inadequate padding over bony prominences, excessive compressive forces from elastic bandages applied too aggressively, and/or pressure areas created by applying padding and casting material in varying joint positions. While clinicians commonly pad bony prominences to minimize skin pressure, the effect of joint position on skin pressure and, more specifically, changing joint position, is understudied. The purpose of this study is to evaluate anterior ankle skin pressure secondary to joint position change during splinting.
Methods: Following ethics approval by our institutional review board, various constructs of lower extremity, short-leg splints were applied to two healthy subjects (2 limbs total in this preliminary data set) with an underlying pressure transducer (Tekscan I- Scan system (Tekscan Inc, South Boston, MA, USA) on the skin surface centered on the anterior ankle on the tibialis anterior tendon. All subjects underwent anterior ankle surface pressure assessment when padding was applied in maximum plantar flexion and neutral position for conventional short leg splints application. Percent change from initial contact pressure centered on the tibialis anterior with either Webril (Covidien/Medtronic, Dublin, Ireland), or Specialist Cotton Blend Cast Padding (BSN Medical, Charlotte, NC, USA) were calculated. Neutral position of the foot/ankle will be confirmed with goniometer.
Results: There were 2 limbs total that were analyzed for the presentation of pilot data for this study. The percent change in anterior ankle contact pressure when padding was applied in maximum plantarflexion (PF) and then placed in neutral was increased at least two-fold without the addition of plaster and subsequently with the addition of plaster in lower extremity short leg splints (Figure 1).
Conclusion: In this pilot data, we report significant increases in anterior ankle contact pressures when splint padding is applied in plantar-flexion and re-positioned into neutral during splint application which may precipitate iatrogenic pressure ulcers in patients sustaining foot/ankle trauma. This data, though preliminary, underscores the importance in proper splinting techniques for all clinicians that manage lower extremity trauma (eg, orthopaedic surgery, emergency medicine, urgent care, etc).
DOI: 10.1177/2473011421S00492
Disuse Osteopenia Development with Non Weight-Bearing in Lower Extremity Trauma: CT Hounsfield-Unit-Based Analysis
David M. Walton, MD; Nicholas Farrar, MD; Jack Eichman, BS; Francisco J. Fuster; Aaron Perdue; Mark Hake; Jaimo Ahn, MD PhD
Category: Trauma; Other
Keywords: Non-Weight Bearing Restrictions; Complications; General Principles / Context
Introduction/Purpose: Disuse osteopenia develops in individuals with decrease lower limb use especially after injury necessitating non-weightbearing, hospitalization or both. However, the nature of this change is not well characterized and, therefore, cannot be appropriately addressed. Conventional CT produces a reliable evaluation of bone quality as Hounsfield Units (HU) and offers the opportunity to longitudinally study bone density in activity-altered patients. The purpose of this study is to estimate the degree of osteopenia in non-weightbearing hospitalized patients and to identify patient-related factors associated with this loss.
Methods: Initial screening criteria included patients who presented to the emergency department between January 1, 2010 to August 1, 2020; baseline lower extremity orthopaedic trauma evaluated by CT. Further criteria included CT imaging capturing the ipsilateral hip at the time of admission; a second CT scan, for any indication (eg, small bowel obstruction, diverticulitis, etc) that include that same hip; strict non-weightbearing in between scans. Exclusion criteria included change in weightbearing status and CT imaging changes that would not allow eBMD analysis (eg, intervention). Estimated BMD (eBMD) was measured at baseline and and at the secondary time point via HU approximation 12mm inferior to superior aspect of femoral neck on axial CT. The change in eBMD was calculated as a proxy for disuse osteopenia and the relationship between relative bone loss (as a nominal rate of osteopenia, eBMD loss/time) and patient-specific factors was explored.
Results: Of 200,000 patients who received CT evaluation including their hip during the targeted timeframe, seventeen patients met our inclusion and exclusion criteria. There was an average of 7.3 days (median = 6 days; mode = 4 days; interquartile range: 4 - 8.5 days) between CT scans. The average rate of disuse osteopenia in the cohort was a net average decrease of 7.5 +- 5.8 HU/day. To place in a standardized clinical context, this change is estimated to correlate linearly with respect to change in DEXA BMD T-Score and may be clinically relevant when HU approach values <100. Associated patient factors that may further precipitate osteopenia whilst non-weightbearing are smoking, female gender, and diabetes.
Conclusion: We report novel, preliminary data estimating the rate of disuse osteopenia in admitted, non-weightbearing orthopaedic trauma patients. This data underscores an important consideration all physicians should make when non- weightbearing status is being considered or required after injury or admission.
DOI: 10.1177/2473011421S00493
Patient-Reported Outcomes after Long-Term Follow-Up of Lisfranc Injuries Treated with Open Reduction Internal Fixation
David M. Walton, MD; Derek J. Semaan; Ronit Shah, BS; Christopher Robbins, PhD; James R. Holmes, MD; Paul G. Talusan, MD
Category: Midfoot/Forefoot; Trauma
Keywords: Lisfranc Injuries; PROMIS; Trauma
Introduction/Purpose: Lisfranc injuries are thought to contribute to debilitating outcomes in polytrauma patients. Due to the relative rarity of Lisfranc injuries, consistent long-term follow-up is a challenge and clinical outcomes are difficult to assess in this patient population. As a result, there exists a need for further investigation into patient-related clinical outcomes after Lisfranc injury. The purpose of this study was to collect long-term clinical outcome data following Lisfranc injuries using PROMIS Physical Function (PROMIS-PF) and Visual Analogue Scale-Foot and Ankle (VAS-FA).
Methods: A chart review was performed to identify all patients who had surgical treatment of an acute Lisfranc injury at our institution from 2005 to 2014. Of forty-five patients identified, we were able to recruit nineteen for a follow-up clinic visit consisting of a physical exam, administration of questionnaires addressing pain and medication usage, radiographs, and completion of outcome surveys including PROMIS-Physical Function and Visual Analogue Scale-Foot and Ankle.
Results: There were 14 female and 5 male patients enrolled in the study with a mean time of 6.25 years from the time of injury. Within this cohort, the mean PROMIS-PF score was 52.4+-8.2 and the mean VAS-Foot and Ankle Score was 76.6+-22.3. The risk factors of age, gender, BMI, smoking status, depression, and time from injury showed no statistically significant association with PROMIS-PF or VAS-FA scores using p<0.05 (Table 1).
Conclusion: We report satisfactory long-term patient-reported outcomes using PROMIS-PF and VAS-FA independent of several risk factors. However, the small sample size and observational nature of our study contributed to the lack of significance in the data and limit our ability to further infer which patients would be expected to do worse postoperatively.
DOI: 10.1177/2473011421S00494
Identifying Risk Factors for Nonunion of the Modified Lapidus Procedure for the Correction of Hallux Valgus
Benjamin Wang; Kshitij Manchanda, MD; Trapper Lalli, MD; George T. Liu, DPM; Michael D. VanPelt, DPM; Katherine M. Raspovic, DPM; Dane K. Wukich, MD; Matthew J. Johnson, DPM
Introduction/Purpose: There is a paucity of literature attempting to characterize risk factors for nonunion of the modified Lapidus procedure for correction of hallux valgus. The purpose of this study was to evaluate several patient factors to determine which may contribute to increased odds of nonunion.
Methods: Patients who underwent modified Lapidus procedure between 2009 to 2018 were retrospectively reviewed. Patient age, sex, body mass index (BMI), history of previous bunionectomy, history of tobacco use, fixation method, presence of diabetes mellitus (DM), and presence of hypothyroidism were recorded along with changes in radiographic parameters. A multiple logistic regression analysis was implemented to estimate the odds of nonunion.
Results: Of the 222 patients who met inclusion criteria, nonunion with modified Lapidus procedure was observed in 20 patients (9.01%). Odds of nonunion with modified Lapidus procedure were greater for patients as BMI increased (OR=1.101, 95% CI: 1.029 to 1.177), tobacco users (OR=3.511, 95% CI: 1.182 to 10.425), had a change in intermetatarsal angle (IMA) (OR=1.313, 95% CI: 1.099 to 1.569), a change in Meary’s angle (OR=1.133, 95% CI: 1.024 to 1.255), and a change in calcaneal pitch (OR=1.192, 95% CI: 0.997 to 1.426), but lower for patients who had a change in hallux valgus angle (OR=0.912, 95% CI: 0.846 to 0.983). Compared with the union group, patients with nonunion had lesser mean degrees correction of IMA (4.25° vs. 7.02°) and greater mean degrees correction of Meary’s angle (1.62° vs. 0.46°) and calcaneal pitch (1.09° vs. 0.38°). No increased odds of nonunion were found between fixation methods.
Conclusion: Predicted odds of nonunion with modified Lapidus procedure increased in patients with high BMI, smokers, and increased change in intermetatarsal angle, calcaneal pitch, and Meary’s angle pre and postoperatively.
DOI: 10.1177/2473011421S00495
Comparison of Revolving Scarf Osteotomy and Double Metatarsal Osteotomy for Treating Severe Hallux Valgus with an Increased Distal Metatarsal Articular Angle
Xinwen Wang; Liang Xiaojun, MD
Category: Midfoot/Forefoot
Keywords: Hallux Valgus; 1st MTP Joint; Valgus
Introduction/Purpose: The aim of this study was to introduce a new surgical procedure defined as revolving scarf osteotomy (RSO) and compare the clinical and radiological results of RSO and double metatarsal osteotomy (DMO) performed for treating severe hallux valgus (HV) with an increased distal metatarsal articular angle (DMAA).
Methods: First metatarsal osteotomies were performed in 56 patients (62 feet) with severe HV with an increased DMAA in Honghui Hospital from January 2015 to December 2017. RSO was performed in 32 feet and DMO was performed in 30 feet. Clinical assessments were performed using the American Orthopaedic Foot & Ankle Society (AOFAS) score and visual analog scale (VAS) score. Radiographic evaluations of the hallux valgus angle (HVA), intermetatarsal angle (IMA), DMAA, and first metatarsal length (FML) were compared preoperatively and postoperatively in the two groups, and the rates of complications were also compared.
Results: The mean AOFAS score, VAS score, HVA, IMA, and DMAA showed significant improvements in both groups after surgery, but with no significant differences between the two groups. The postoperative FML was significantly larger in the RSO group than in the DMO group (p<0.001). One of the 30 feet (3.3%) in the DMO group exhibited transfer metatarsalgia at 12 months postoperatively, while another foot (3.3%) in same group had avascular necrosis of the metatarsal head. One of the 30 feet (3.1%) in the RSO group had hallux varus.
Conclusion: No differences in the clinical and radiographic results were observed between the two groups with severe HV and an increased DMAA. However, RSO may reduce postoperative complications compared to DMO. A long-term, randomized, controlled prospective study with a larger sample would provide higher-level evidence for confirming the clinical efficacy and safety of RSO.
DOI: 10.1177/2473011421S00496
Staged Hindfoot Fusion for Osteomyelitis of the Distal Tibia and Talus
Peter R. Wasky, MD; Nihar S. Shah, MD; Augusto Roca; Richard T. Laughlin, MD
Introduction/Purpose: Management of hindfoot osteomyelitis involves eradication of infection, deformity correction, and bony stabilization in the setting of bone loss and poor bone quality. In this case series of 12 patients, we present a two-stage technique; debridement, deformity correction, joint surface preparation, and intramedullary reaming with placement of antibiotic rod and ring external fixation followed by a second stage of external fixator removal and exchange of antibiotic rod for definitive hindfoot rod. The purpose of this poster is to highlight techniques that can improve the success of obtaining stable fixation, remission of infection, and ultimately fusion. Techniques highlighted are ring fixator placement, preparation of the antibiotic rod, intramedullary canal preparation, rod exchange, and use of blocking screws to enhance compression and axial loading of the fusion.
Methods: Twelve patients were treated with this two-stage protocol. The most common indication was post-traumatic osteomyelitis followed by neuropathic (Charcot) joint. All were treated in a staged manner with an initial debridement of nonviable tissue including osteomyelitic bone. The tibiotalar and talocalcaneal joints were resected and prepared for fusion at the initial debridement. Provisional stabilization and compression were obtained through the use of a ring external fixator. An intramedullary antibiotic impregnated cement coated rod was introduced through the calcaneus, talus, and the intramedullary space of the tibia. The patients were kept in the fixator until the skin was healed and all incisions were dry. At this point, the fixator was removed, and the antibiotic rod was exchanged for the definitive hindfoot fusion rod.
Results: Cultures were positive for Staphylococcal or Streptococcal species in 58% of cases, fungal in 8%, and Gram negative organisms in 33%. On average patients spent 93 days in the fixator while wounds were healing, and they were receiving systemic antibiotics. One patient died while in the frame. There have been no amputations in the series. Of the patients that have completed the protocol, all have gone on to either bony fusion or stable fibrous union. All are able to walk unaided. And thus far, all are free of active infection. Secondary procedures are described.
Conclusion: This technique of staged fusion for hindfoot osteomyelitis offers the following advantages. the first stage involves thorough debridement and deformity correction. Oftentimes there is extensive scarring and the soft tissue envelope is not conducive to internal fixation. This technique allows the soft tissues to heal before placing the definitive internal fixation. It also allows for graduated compression at the fusion site with the ring fixator. The antibiotic rod not only delivers high concentration of local antibiotics, but it prevents deformity recurrence during the compression phase. The definitive rod provides support of pathologic bone and maintains deformity correction.
DOI: 10.1177/2473011421S00497
Comparison of 3D Surface Rendering CT to Plain Lateral Radiographs for Quantification and Characterisation of Posterior Malleolar Fracture Fragment Size and Morphology
Lizzy Weigelt; Lyndon W. Mason; Laura-Ann Lambert; Gavin Heyes
Introduction/Purpose: The aim of this study was to compare the size of the posterior malleolar fracture (PMF) fragment on plain lateral radiographs compared to three-dimensional (3D) surface rendering CT imaging, and to compare both modalities in the characterisation of PMF morphology.
Methods: Measurements of 180 lateral radiographs of PMF’s were compared to their respective 3D surface rendering CT reconstructions, by two independent observers reviewing percentage articular involvement of the PMF fragment. Morphology of the PMF was categorised initially by the CT scan as classified by Mason and Molloy and was compared to this classification using radiographs.
Results: When calculating the percentage joint surface involved by the PMF fragment, inter-observer variability was greater than 0.8 for radiographic and CT measurement. Significant differences in size of PMF on radiograph compared to CT were found for type 1 and type 2A fractures (p<0001 type 1, p=.071 type 2A). Radiographs consistently over-estimated the PMF fragment size, although in type 2B fracture patterns there was an equivalent number that were under-estimated due to the underappreciation of the posteromedial fragment. Comparison of fracture fragment morphology found that type 2A and 2B fractures (rotational Pilon’s) had poor agreement between radiographs and CT (34.15%).
Conclusion: This study shows that the use of a lateral radiograph in a PMF to estimate fracture size and morphology is poor. Additional CT imaging is imperative to allow for appropriate treatment planning in the management of PMF.
DOI: 10.1177/2473011421S00498
Identification and Fixation of Intermetatarsal Coronal Plane Instability Following Modified Lapidus Procedure
Alex Wetzig; Guillermo R. Pechero; David C. Berken, MD; Pierce Ebaugh, DO; William C. McGarvey, MD
Category: Bunion; Midfoot/Forefoot
Keywords: Bunion; Hallux Valgus; Instability
Introduction/Purpose: There are many described techniques to approach surgical correction of bunion deformity and prevention of recurrence is still a topic of interest. Coronal plane instability evidenced by intermetarsal angle (IMA) widening with weight bearing is a cause for concern with respect to recurrence. The identification of patients who are at risk for recurrence intraoperatively is challenging and currently there are few described tests that guide physician treatment. The aim of this study was to demonstrate an intraoperative intermetarsal coronal plane ’squeeze stress test' utilized by the senior surgeon along with the clinical and radiographic outcomes of patients who underwent fixation for their identified instability following the modified Lapidus procedure for hallux valgus correction.
Methods: All patients included in this study presented with clinical and radiographic documentation of hallux valgus that was treated by a first tarsometatarsal arthrodesis with additional middle column fixation following widening on intraoperative fluoroscopy ’squeeze stress test' (Figure 1) by a single senior surgeon from 2015-2020. Fixation of the middle column was achieved via endobutton (5), screw (23), or endobutton plus screw (5). Clinical descriptions were reviewed for the presence of symptomatic recurrence and for the need of revision surgery. A single observer measured the HVA and the IMA angle of the preoperative and final post-operative weight-bearing radiographs, respectively. A total of 33 patients were included with an average age of 58.5 (range, 40-80) years of age and a mean follow-up of 8.3(range, 1.5-30) months. Mean BMI was 29 (range, 19- 54). Statistical analysis of this data set utilized the chi-square test and two sample t-test.
Results: Pre-operatively, the patients with identified coronal plane instability had a mean HVA and IMA of 33 (range, 16-74) and 14 (range, 7-23) degrees, respectively. At final follow-up, these patients maintained a mean HVA of 9.8 (range, 0-32) and IMA of 4.5 (range, 0-15). No patients sustained clinical recurrence. Two patients underwent elective removal of hardware. One patient sustained a deep infection that required removal of hardware and formal debridement, this subsequently resolved.
Conclusion: Coronal plane instability remains one of the unsolved facets of effectively treating symptomatic hallux valgus. Vigilance is the first step in prevention of recurrence in these patients and the ’squeeze stress test' is a simple, quick option for their identification. Our case series demonstrates satisfactory outcomes in terms of clinical recurrence for these patients utilizing this new evaluation technique. We believe further investigation of the squeeze stress test as an instability identifier is warranted in all types of bunion correction procedures.
DOI: 10.1177/2473011421S00499
Achilles Tendon Rupture Repairs: Clinical Outcomes of a Novel Technique
Caroline Williams, BA; John Z. Zhao, MD; John Y. Kwon, MD; Christopher P. Miller, MD
Introduction/Purpose: Acute Achilles tendon rupture repair has undergone several changes in the past decade, aiming to minimize complications while maximizing clinical outcomes. Less invasive approaches have been associated with comparable results and decreased infection risk compared with traditional open techniques. Patient positioning during surgery also influences outcomes; prone positioning is associated with increased operative times as well as risk of neuropraxia and ophthalmologic injuries as compared to supine positioning. The Medial Mini-Open Supine (MMOS) Achilles Repair technique combines the benefits of supine positioning and mini-open techniques. This study compares 1-year clinical outcomes, operative times, and complication rates of patients undergoing repair with this novel technique to those treated with an open or mini-open approach with prone positioning.
Methods: Patients undergoing operative acute Achilles rupture repair at our institution after February 2015 were included in this study. Patients were grouped by technique used: 1) open repair with prone positioning, 2) mini-open repair with prone positioning, or 3) the medial mini-open repair with supine positioning. Patients were followed for a minimum of 1 year postoperatively. Primary outcome measures include Patient-Reported Outcomes Measurement Information System (PROMIS) scores (Physical Function, Pain Interference and Depression), Foot and Ankle Ability Measure (FAAM) assessments (ADLs and Sport) and Visual Analog Scale (VAS) pain scores. Secondary outcome measures include intraoperative times and complication rates. Statistical analysis to assess for significant differences between the groups was conducted using the Kruskal-Wallis test, Nemenyi test, ANOVA with posthoc Tukey test and chi-square test as was appropriate.
Results: A total of 56 patients (Group 1: n=18, Group 2: n=14, Group 3: n=24) were included in this study. Average 1-year PROMIS Physical Function scores were 59.57 (+-12.9), 64.29 (+-13.96) and 63.03 (+-11.69) for Groups 1, 2 and 3 respectively. Average Pain Interference scores were 46.05 (+-17.65), 42.12 (+-8.75) and 42.48 (+-7.11). Depression score averages were 40.79 (+-7.61), 36.87 (+-9.35) and 39.81 (+-9.48) for Groups 1, 2 and 3, respectively. Differences between groups were not significant (p >0.05). Group 3 had statistically significant differences in total OR time compared to both Groups 1 and 2. The median difference was 33 min between Groups 1 and 3, and 35 min between Groups 2 and 3 (p<0.01) The majority of time savings arose from pre- incision setup and post-closure times. Differences in complication rates (5.5% (n=1), 14.3% (n=2), and 12.5% (n=3), for Groups 1, 2 and 3 respectively) were not statistically significant (p=0.73).
Conclusion: The Medial Mini-Open Supine Achilles Repair technique shows promise as a viable option for acute Achilles tendon rupture repair; ease of patient positioning preoperatively translates to decreased set up, operative, and sedation time, directly benefiting patients. Patient-reported outcomes at 1-year follow-up demonstrate comparable results with both open and mini-open prone techniques, without an increase in complication rates.
DOI: 10.1177/2473011421S00500
Defining an Anatomic and Radiographic Safe Zone for Posterior Malleolar Ankle Hardware Fixation
Caroline Williams, BA; Kaveh Momenzadeh, MD; Max Michalski, MD; John Y. Kwon, MD; Christopher P. Miller, MD
Category: Ankle; Trauma
Keywords: Operative Approach; Posterior Malleolus Fracture; Injuries to the Syndesmosis
Introduction/Purpose: There is a lack of consensus regarding optimal management of Posterior Malleolar Fractures (PMFs). Indirect reduction and fixation with posterior-anterior (PA) screw shows promise of avoiding the risks associated with direct reduction or indirect anterior to posterior (AP) approaches. Some authors have raised concerns about potential risk to nearby structures with PA technique, including hardware prominence into the syndesmosis. This study highlights the use of a posteromedial vertical syndesmotic line as a fluoroscopic landmark, helping surgeons avoid intra-syndesmotic placement.
Methods: Indirect PA screw placement was completed on ten cadaveric specimens, followed by fluoroscopy in mortise and lateral views. Dissection was performed to assess screw placement relative to the posteromedial border of the syndesmosis. The posterior border of the syndesmosis was marked with a radiopaque wire. Repeat imaging was completed to validate the fluoroscopic posteromedial vertical syndesmotic line is representative of the posteromedial border of the tibial incisura.
Results: On dissection, 9 of 10 cadavers had accurate screw placement with no penetration into the syndesmosis (Figure 1, bottom left & bottom right). Corresponding imaging showed the screw head to be medial to the marker on mortise view. For the specimen with penetration into the syndesmosis, imaging confirmed that the screw head was lateral to the marker on mortise views (Figure 1, top center & top right). The radiopaque marker correlated with the posteromedial vertical syndesmotic line for all specimens when comparing anatomic to radiographic findings. A radiographic safe zone is defined for the PA screw 12 mm medial to the vertical syndesmotic line to ensure no iatrogenic injury to the FHL tendon.
Conclusion: This study demonstrated that the posterior incisura tibialis fluoroscopic landmark is unambiguous in localizing the posterior syndesmotic border (Figure 1, top left) and that screws medial to this line are safely out of the syndesmosis, while screws placed lateral are either in or at risk of intra-syndesmotic placement. A safe zone is defined for screw placement.
DOI: 10.1177/2473011421S00501
Prospective Observational Study of an Integrated Therapeutic Initiative for Extremities (POSITIVE): Implementation of an Integrated Orthotic and Rehabilitation Program in the Civilian Setting
Andrew Wohler, MD; Rachel Seymour; Christine Churchill; Tamar Roomian; Michael A. Jenks; Jeffrey D. Fawcett; Mark L. Elgart; Tarey Strickland; Joseph R. Hsu, MD; EMIT Collaborative
Category: Trauma; Other
Keywords: Ankle; Pain; Return to Play
Introduction/Purpose: The Return to Run (RTR) pathway currently utilized in the military have been demonstrated to facilitate return to duty, recreation and physical activity and decrease pain in high functioning patients who have sustained high energy lower extremity trauma. A recent study also demonstrated that the processes and outcomes are translatable across military settings, however, to date there is no evidence on implementation of this pathway in the civilian setting. We sought to evaluate the feasibility of implementation of a similar, Return to Performance (RTP), pathway at a high volume, level I civilian trauma center. RTP combines a custom Variable Cadence Ankle-Foot Orthosis (VCAFO) with an 8-week exercise program designed to improve performance and reduce pain.
Methods: A prospective observational study was conducted to enroll all patients eligible for the VCAFO. Patients were followed from initial referral through one year. A large, national prosthetic and orthotic company was utilized for brace manufacture and fitting. Physical therapy services were provided in the outpatient setting.
Results: The RTP pathway has been fully operational for five years. There was an initial two year run in period for initial training of therapists and prosthetists and logistic implementation at our institution. 58 patients participated in the full RTP pathway, and 21 received RTP via remote rehabilitation delivered through a manual. An additional 6 patients met with the lead PT for at least 1 visit. All expenses for prostheses as well as therapy sessions have been covered by insurance. 32 prosthetists have been trained locally in the fabrication of the brace with an additional 70 trained at the brace manufacturers most recent national meeting. 13 physical therapists have been trained to perform functional rehabilitation through the RTP pathway.
Conclusion: Implementation of the Return to Performance pathway can be translated and scaled to the civilian setting. The study has successfully replicated the brace fabrication necessary for optimal outcome in the RTR pathway, although there are remaining questions about scaling of physical therapy. This provides evidence that the process can be de-centralized and the benefits of dynamic bracing in high functioning patients following lower extremity trauma can be translated to the civilian population.
DOI: 10.1177/2473011421S00502
Results of an Interim Analysis of a Prospective Multicenter Study Assessing Radiographic and Patient Outcomes Following Triplanar Tarsometatarsal Arthrodesis with Early Weightbearing
Dane K. Wukich, MD; Robert D. Santrock, MD; Daniel C. Farber, MD; Abdi Raissi, MD; Avneesh Chhabra; Daniel J. Hatch, FACFAS; Jennifer Koay; Paul Dayton, MS,DPM; Robert P. Taylor; Jody McAleer, DPM, FACFAS; Deidre Kile
Introduction/Purpose: The majority of hallux valgus corrections are performed via a two dimensional approach with 1st metatarsal osteotomy and translation in the transverse plane. This approach has demonstrated high long-term recurrence rates. Recent research demonstrates that 87% of hallux valgus deformities are three-dimensional with abnormal frontal-plane rotation of the metatarsal, which cannot be completely addressed with a two dimensional metatarsal osteotomy alone. While correction at the 1st tarsometatarsal (TMT) joint may provide the optimal surgical approach for 3D anatomic restoration at the apex of the deformity, 1st TMT fusion entails an extended period of non-weightbearing. This study evaluated the clinical, radiographic, and patient-reported outcomes in patients undergoing instrumented triplanar 1st TMT arthrodesis (TMTA) with a biplanar plating system and protected near-immediate weightbearing.
Methods: This is a prospective multicenter study that will continue for 60 months post-operatively. Patients between 14-58 years old with symptomatic hallux valgus (intermetatarsal and hallux valgus angles between 10.0-22.0° and 16.0-40.0°, respectively) and no prior hallux valgus surgery on the operative foot are eligible for this study. Patients are treated with an instrumented TMTA procedure using a biplanar plating system with protected near-immediate weightbearing. Several outcomes (radiographic, range of motion (ROM), return to weightbearing and activities, pain measured by visual analog scale (VAS), Manchester-Oxford Foot Questionnaire (MOxFQ), and Patient Reported Outcomes Measurement Information System (PROMIS)) are evaluated post- operatively. Two independent fellowship trained musculoskeletal radiologists reviewed all radiographic data. These interim results are limited to patients completing at least 6 months of follow-up.
Results: At time of analysis, 121 patients had undergone TMTA with at least 6 months of follow-up. Mean age was 40.6 (range:15- 58) years, and 91% of patients were female. Mean (SD) days to protected weightbearing in CAM boot, return to work, and return to full work were 8.2 (6.8), 24.0 (29.5), and 51.2 (44.0), respectively. Significant improvements (p<0.05) from baseline in HVA, IMA, and TSP (Table 1), VAS score, MOxFQ and PROMIS domains were observed as early as 6 weeks post-procedure. At 12 months, mean (95% CI) change in VAS score was -4.0 (-4.5, -3.6); Walking/Standing, Pain, and Social Interaction (MOxFQ domains) change was -38.6 (-43.6, -33.5), -41.0 (-45.8, -36.2), and -40.5 (-45.3, -35.7), respectively; and physical function (PROMIS) change was 8.7 (6.6, 10.8).
Conclusion: These interim findings support that TMTA with biplanar plating is successful in correcting the 3D hallux valgus deformity with early return to weightbearing while demonstrating favorable clinical and patient-reported outcomes. Patients exhibited meaningful pain reduction after surgery and were able to return to full, unrestricted work and activities in less than two months, on average. Statistically significant improvements in patients' health-related quality of life were observed at 6 and 12 months, post-operatively. Patients will continue to be followed for up to 60 months with additional evaluations for complications, 24-month recurrence, and patient satisfaction.
DOI: 10.1177/2473011421S00503
Influence of Medical Marijuana on Interleukin-1Β Treated Cartilage: An in Vitro Study
Alan Y. Yan, MD; Jiangyinzi Shang; MaCalus V. Hogan, MD, MBA, FAAOS, FAOA; Jarrett D. Cain, MSc, DPM; Peter G. Alexander; Hang Lin
Category: Basic Sciences/Biologics
Keywords: Cartilage; Cartilage; Cartilage
Introduction/Purpose: Medical marijuana is reported to have potent analgesic, immunomodulatory and anti-inflammatory properties. Some recent studies have shown that cannabinoids may attenuate joint damage in animal models of arthritis. However, the underlying mechanism has not been completely elucidated. Interleukin-1β (IL-1β), a proinflammatory cytokine that can result in the degradation of cartilage, is known to be associated with the pathogenesis of osteoarthritis. We hypothesize that cannabinoids can mitigate the detrimental effect of IL-1β on cartilage, thus slowing the progression of osteoarthritis. We exposed human chondrocyte-derived engineered cartilage pellet cultures to IL-1 β for 48 hours or not and then treated the samples with a synthetic cannabinoid agonist, Win-55,212-2(Win). The tissue phenotypes were thereafter assessed by real time polymerase chain reaction (RT-PCR), histology and western blotting.
Methods: Medical marijuana is reported to have potent analgesic, immunomodulatory and anti-inflammatory properties. Some recent studies have shown that cannabinoids may attenuate joint damage in animal models of arthritis. However, the underlying mechanism has not been completely elucidated. Interleukin-1β (IL-1β), a proinflammatory cytokine that can result in the degradation of cartilage, is known to be associated with the pathogenesis of osteoarthritis. We hypothesize that cannabinoids can mitigate the detrimental effect of IL-1β on cartilage, thus slowing the progression of osteoarthritis. We exposed human chondrocyte-derived engineered cartilage pellet cultures to IL-1 β for 48 hours or not and then treated the samples with a synthetic cannabinoid agonist, Win-55,212-2(Win). The tissue phenotypes were thereafter assessed by real time polymerase chain reaction (RT-PCR), histology and western blotting.
Results: RT-PCR revealed persistent increase in the expression of inflammatory mediators IL-1beta, TNF-alpha and COL2 in IL1beta+ cultures over IL1beta- controls at all levels of WIN exposure. In contrast there was clear decrease in IL-6 expression at high WIN doses coincident with a downward trend the other mediators. WIN was unable to rescue IL-1beta-induced reductions in COL2 and ACN, while inducing ALP, a marker of osteogenesis and cartilage hypertrophy. Safranin O/Fast Green histology revealed progressive loss in GAG deposition with increasing doses of WIN (Figure 2). Western blots confirmed reductions in COL2 and COMP protein, persistent COX2 production, and increasing translation of the osteogenic transcription factor RUNX2 and p-SMAD1/5/8 (Figure 3).
Conclusion: At doses below 1µM, Win does not impact IL-1beta-induced chondrocyte inflammation. while inhibiting chondrogenesis and stimulating osteogenesis through RUNX2 as compared to IL-1β controls. In proper context, BMP2 stimulates osteogenesis through SMAD1/5/8 and the induction of RUNX2. We did observe an apparent anti-inflammatory role of WIN at 1µM, but this dose did not rescue a loss in cartilage pellet GAG loss. Our data suggests that cannabinoids are anti-inflammatory, but are unable to rescue cartilage degeneration by IL-1β and promote an osteogenic phenotype. However, the data are not conclusive with regarding the beneficial or detrimental to arthritic bones and cartilage
DOI: 10.1177/2473011421S00504
Comparison Between Mini-Invasive Distal and Proximal Chevron Osteotomies in the Correction of Hallux Valgus Deformity
Ding C. Yang, MD, DPM, PhD
Category: Bunion
Keywords: Osteotomies; Metatarsals; Bunion
Introduction/Purpose: The potential advantages of minimal incision surgery for hallux aboducto valgus (HAV) correction are to reduce surgical exposure, diminish soft-tissue stripping, and lessen blood supply impairment. The purpose of this study was to assess the safety and efficacy of minimally invasive techniques. Currently, there are insufficient studies to recommend one minimally invasive technique over another.
Methods: From 2018 to 2020, 141 cases with hallux abducto valgus were treated with minimal incision osteotomy using Kirschner wire fixation. 120 patients had distal chevron osteotomies and 21 patients had proximal first metatarsal osteotomies. The patient age range was between 29 yo and 96 yo, with 118 female and 23 male patients. 48 patients were 65 yo and over, and 93 patients were less than 65yo. The preoperative and postoperative hallux abducto valgus angles (HVA), intermetatarsal angles (IMA), American Orthopaedic Foot & Ankle Society (AOFAS) scores were measured and evaluated.
Results: The average AOFAS scores improved from a preoperative median of 41.4 points to a postoperative median of 88.6 points. The mean HVA and IMA angles significantly decreased after the operation. There were no complications of nonunion or delayed union, avascular necrosis, infection, or hallux varus. The technique has been largely accepted by the patients due to the short procedure time, the reduced postoperative pain, and the fast functional recovery. For the hallux aboducto valgus deformity with HVA over 35 and IMA over 16 degrees, the procedure with proximal chevron osteotomy achieved better corrections.
Conclusion: Both proximal and distal chevron osteotomy techniques showed comparable results. The distal percutaneous osteotomy was effective for the treatment of mild to moderate hallux abducto valgus deformity, and the proximal percutaneous osteotomy was effective for the treatment of severe hallux abducto valgus deformity. This study indicated that the minimal incision osteotomy was a simple and reliable technique for treating hallux abducto valgus with minimal complications. Through minimally invasive approaches, the hallux abducto valgus corrections performed in this study resulted in minimal soft tissue injury, less postoperative pain, and good cosmetic results.
DOI: 10.1177/2473011421S00505
Contact Pressures Change According to Displacement Shape in Isolated Medial Malleolar Fracture: Cadaver Study
Eui Dong Yeo, MD; Young Koo Lee, MD, PhD; Jungtaek Im
Category: Trauma; Basic Sciences/Biologics
Keywords: Ankle; Ankle Fracture; Biomechanics of the Foot and Ankle
Introduction/Purpose: Ankle fractures, representing 9% of all fractures, are among the most common types of fractures worldwide. 1 of 5 ankle fractures is an isolated medial malleolar fracture (IMMF). IMMF were treated surgically, but recently it was concluded that all IMMF(<=2mm) should be treated conservatively. The indication for surgery or conservative treatment of IMMF remains unclear. The purpose of the present study is to check the change of pressure in the ankle joint according to the shape and the displacement in the medial malleolus fractures.
Methods: Twenty pairs of fresh-frozen cadaveric lower legs, disarticulated at the knee, will be used. Specimen pairs were assigned at random into 1 of 2 groups. This study measures the pressure change in the ankle joint according to Muller type C and D. The specimen was mounted in the materials testing machine with the plantar aspect of the foot in contact with the foot-plate. Load was applied with the ankle in the neutral position. Contact area and contact pressure were quantitated with low-grade pressure-sensitive film (Prescale film; Fuji Photo Film, Tokyo, Japan). The color densities were converted to measurements of pressure. After osteotomy the medial malleolus in Muller type C and D, displace each 2mm and fix it with diameter 4.0mm and length 45 mm cortical bone screws. Pressure measurement is done in the same way as above.
Results: The median value and wilconxon singed rank test was used for the results. The median value of normal ankle contact area was 3.15cm2 [2.61.;3.51], the mean pressure was 2.18 Mpa(Megapascal) [2.00.;2.43], and the median value of contact area after transverse osteotomy was 2.89cm2 [2.41.;3.24], mean pressure was 2.37Mpa [2.14.;2.75], and the median value of contact area after oblique osteotomy was 2.72cm2 [2.50.;3.16], mean pressure was 2.50Mpa [2.33.;2.74]. P value of the mean area and mean pressure change after transverse and oblique was <0.05.
Conclusion: At 2mm transverse and oblique displacement, ankle contact area and pressure decreased significantly.
DOI: 10.1177/2473011421S00506
Correlation of Patient Wearable Outcomes to Self-Reported Patient Outcome Measures
C. Jordan Yergensen; Kristin L. Kress; Otho R. Plummer, PhD; David E. Jaffe, MD
Category: Other; Sports
Keywords: PRO; Achilles Tendon; Ankle Sprain
Introduction/Purpose: Patient reported outcome measures (PROMs), especially computerized adaptive testing (CAT), are the gold standard for outcome reporting in the field of orthopaedic surgery. Wearable technology (fitbit, apple watch, etc) and other health monitoring capabilities available on smart phones applications (i.e. apple health) are rapidly evolving and being considered as alternative methods of measuring outcomes in orthopaedics. This patient wearable outcome (PWO) method has yet to be directly compared to PROMs, nor evaluated as a viable option for outcome measurement in orthopaedics. The purpose of this study is to directly compare PWOs to PROMs and determine the advantages and disadvantages of using the health monitoring capabilities of smart phones as outcome measuring tools in orthopaedics.
Methods: This study is designed as a nonrandomized prospective cohort focused on a small subset of subjects within the field of orthopaedics. Subjects were recruited from an orthopaedic foot and ankle clinic with diagnoses of ankle sprain, plantar fasciitis, and achilles tendonitis. These conditions were chosen as these would generally represent nonoperative conditions at presentation. Subjects under 16 years of age and surgical candidates were ineligible. Standard PROM surveys, all of which have been previously validated by the AOFAS for outcome measurement were administered at enrollment and then electronically delivered at 3 and 7 weeks. Surveys utilized were the Foot and Ankle Ability Measure (FAAM), Visual Analog Scale (VAS), and PROMIS physical function, mobility and pain interference scores. An application (ActiveTrack) is installed on the subjects' smartphones to pull all past and future health data including step counts, distance traveled, etc. Statistical analysis was then performed to correlate PWO’s with PROMs.
Results: 28 subjects consented and enrolled in the study. This has provided strong encouragement for the goals of the study. 21 patients were observed at 3 weeks with a Pearson correlation of step count of 0.6975 (95% CI: 0.3804-0.8679). 7 subjects were observed at 7 weeks with a Pearson correlation of step count of 0.8387 (95% CI: 0.2325-0.9756). We found that step counts and FAAM scores generally increased after treatment, and that the correlation between the changes was positive. The strongest signal was obtained from the FAAM ADL subscale.
Conclusion: This study shows that there is a correlation between a patient’s self-reported function (PROMs) and their activity (PWOs). PWO data may represent a more accurate measurement of a patient’s activity and therefore may be a great tool in assessing functionality before and after an intervention (be it surgical or nonoperative treatments). Further analysis of the data obtained from this prospective study over time may help establish a new standard of care for measuring patients' response to orthopaedic treatment.
DOI: 10.1177/2473011421S00507
Posterior Tibial Transfer to the Lateral Cuneiform in a Young, Active Patient with Foot Drop: A Case Report
Robert G. Yoder; Nicholas Lipari; Adam T. Groth, MD
Introduction/Purpose: We report the case of a 23-year-old male who underwent a posterior tibial tendon (PTT) transfer after suffering foot drop secondary to a traumatic knee dislocation five years earlier. The common peroneal nerve is a commonly injured peripheral nerve due to its anatomic location. Peroneal nerve palsy leads to the inability to clear the foot during the swing phase of gait due to paralysis of the tibialis anterior- the strongest dorsiflexor of the foot. In the event that nerve function does not spontaneously return, tendon transfer surgeries are an established definitive treatment. Despite this, the optimal method of tendon transfer has not yet been determined. Thus, pre-operative assessment and planning remains crucial in determining which method is to be used.
Conclusion: Surgeons must decide which tendon to transfer, which route to utilize, and where to insert in effort to maximize biomechanical outcomes. Careful consideration must be made to ensure maximum strength and optimal forefoot balance to allow patients undergoing tendon transfer to become brace free. Our patient underwent a PTT transfer via the interosseous route to the lateral cuneiform- a common option for those with traumatic peroneal nerve injury. By three months post-operation, our patient achieved adequate dorsiflexion to clear swing phase. By one year post-operation and beyond, our patient has participated in physical activity brace free without any complications.
DOI: 10.1177/2473011421S00508
Obesity is an Independent Risk Factor for Achilles Tendon Rupture: A Nationwide Longitudinal Cohort Study in South Korea
Yeo Kwon Yoon, MD; Jae Han Park, MD; Seung Hwan Han, MD, PhD; Jin Woo Lee, MD, PhD; Kwang Hwan Park, MD, PhD
Introduction/Purpose: Obesity is an increasing comorbidity that can negatively affect the clinical outcomes of various disease in orthopaedics. However, there was no study to evaluate an association between Achilles tendon rupture and obesity in a nationwide study. We aimed to investigate the incidence of Achilles tendon rupture through a nationwide longitudinal cohort in Korea and evaluate the influences of demographic data including body mass index (BMI).
Methods: Between 2002 and 2015, sociodemographic factors including gender, age, BMI, income, comorbidities, and sport activity level were retrieved from National Health Insurance Service-National Sample Cohort (NHIS-NSC). NHIS-NSC database was searched for individuals treated with ATR. We excluded individuals who were less than 20 years-old.
Results: 736 (0.116%) of total 636,921 individuals in NHIS-NSC database underwent Achilles tendon repair (ATR). Multivariable logistic regression analysis revealed that obesity (BMI>= 25kg/m2) was significantly associated with ATR (odds ratio, 1.99; 95% confidence interval, 1.68 to 2.36). Other significant factors were age, male, total cholesterol, moderate sport activity, and income. After propensity score matching of all factors, obesity was significantly associated with ATR with odds ratio 1.95 (95% confidence interval, 1.60 to 2.39).
Conclusion: Obesity is an independent predictive factor for the occurrence of Achilles tendon rupture followed by ATR.
DOI: 10.1177/2473011421S00509
A Patient Cohort Comparison of Radiographic Correction and Early Complications Between Percutaneous and Open Lapidus Procedures for Hallux Valgus
Alastair S. Younger, MB ChB, ChM, FRCSC; Diogo Cardoso; Kevin J. Wing, MD, FRCSC; Andrea N. Veljkovic, MD, MPH, FRCSC; Murray J. Penner, MD, FRCSC
Introduction/Purpose: Hallux valgus can be corrected by a variety of procedures. The Lapidus procedure corrects the first ray position in three planes using a first tarsometatarsal fusion (TMTF) and distal release and realignment. In a single surgeon practice the procedure was performed open until 2017, when burrs became available to perform the procedure percutaneously. This study compares the early radiographic results and complications of the percutaneous procedure with the open procedure.
Methods: 47 patients undergoing the percutaneous procedure were compared with 44 patients undergoing the open procedure prior to July 2017. Radiographic measures preoperatively were compared to the postoperative measures for intermetataral angle (IMA), Hallux valgus angle (HVA), foot width (FW), distal metatarsal articular angle (DMMA), sesamoid station, metatarsus adductus angle (MAA), first metatarsal to second metatarsal length, and elevation of the first metatarsal. Early 30 day complications were recorded, as well as repeat surgeries. Demographics: There were 81 female and 10 male patients; The average age was MIS 58+/- 13, open 62+/-13. BMI was 28.4 vs 25.1. 1% of patients had diabetes, and 15% were smokers. Statistical analysis was performed using ANOVA. Because of multiple comparisons p<0.005. Error is quoted as 95% standard deviation. Grouped statistics were compared with a chi square test.
Results: There is less correction in the MIS group in HV angle. The IM angle reduced from 15.8o+/-4.6 o to 6.3 o +/- 3.3 o compared to 17.7 o to 4.8 o +/- 3.6 o for the open group (p<0.05 and p>0.005). The change was 9.5 o compared to 12.9 o. HVA in the MIS group went from 34.6 o +/- 9.1 o to 14.5 o +/- 7.9 o (20.1 o change) compared to the open group where HVA went from 40.7 o +/- 10.5 o down to 11.6 o +/- 6.1 o (29.1 o change) (p<0.001). The wound complication rate trended higher in the open group (4 versus 0) out of 51 in each group (p>0.05). The nonunion rate was higher in the open group (0 MIS vs 4). The revision rate for deformity correction was the same in both groups (2 versus 2).
Conclusion: In this single surgeon series between the two cohorts the MIS group showed a trend towards less correction than the open group. In particular the correction of the Hallux valgus angle was less. At the current time the distal release and realignment may not be as effective as in the open surgery, so more Aitken osteotomies may be required.However there was a trend for less wound complications and less non unions in the MIS group. The comparison included the initial experience with MIS as so the correction may not be as good as the technique evolves.
DOI: 10.1177/2473011421S00510
Prospective Three-Year Outcomes Comparing Cemented and Cementless Fixation in the Trabecular Metal Total Ankle Arthroplasty
Alastair S. Younger, MB ChB, ChM, FRCSC; J. Kent Ellington, MD, MS; Steven M. Raikin, MD; Eric Giza, MD; Donald R. Bohay, MD, FACS; Federico Giuseppe Usuelli, MD; Theodor Patsalis; Lars H. Frauchiger, MD; Selene G. Parekh, MD, MBA; Fabian Krause, MD
Category: Ankle; Ankle Arthritis
Keywords: Total Ankle Arthroplasty; Fusion; Outcomes Measures
Introduction/Purpose: In total ankle arthroplasty (TAA), the implant can be inserted with or without cement. The United States Food and Drug Administration (FDA) requires cement fixation on most TAAs, whereas cementless TAA can be performed in other countries. The laterally placed trabecular metal ankle replacement is inserted using a jig and a fibular osteotomy. The tibia and talus are reamed to match the curved contour of the replacement. Two rails on the tibial and talar component are used to transfix the cementless component onto bone. FDA licensing requires a bead of cement applied on the fixation rails to assist in early component fixation. The purpose of this study was to compare early and three-year results of TAA with and without rail cement performed in six countries.
Methods: One hundred and twenty-one patients were prospectively enrolled (from 2014 to 2016) across 11 centers in six countries. Patients were assigned cement or no cement based on the surgeon’s practice. EQ5D, AOS, and AOFAS scores were obtained preoperatively, six weeks and six months postoperatively, and yearly thereafter. Secondary endpoints were revision of metal components for infection or loosening. Statistical significance was tested by the Wilcoxon Signed Rank Test and set at p=0.05.Sixty ankles had cement; 61 ankles were press fit. Cement augmentation patients were heavier and older. Cement cases had longer surgical times (173 minutes, 95% CI 162.8 to 183.2, versus 150 minutes, 95% CI 139.9 to 158.4). The sites using cement fixation varied. Of 121 cases, 117 were followed at one year, 96 at two years, and 84 at three years. Three patients underwent revision and five withdrew (one died, two lost to follow-up, and two requested discontinuation).
Results: The EQ5D scores demonstrated better outcomes for the press fit component without cement at six weeks (p<0.001), six months (p=0.001), one year (p=0.005), and two years (p=0.02), but not at three years (p=0.132). The AOS Disability scale demonstrated better outcomes for the press fit component at six weeks (p=0.008), six months (p=0.022), one year (p=0.020) and two years (p=0.024). The AOS Pain scale demonstrated better outcomes for the press fit component at six months (p=0.05). The AOFAS score demonstrated better outcomes for the press fit component at six weeks (p<0.001), but no significant differences thereafter. Survivorship for joint replacement (revision of metal components) was 97.4% for the full cohort. Three metal components were revised in three ankles in the cementless group (chi square not significant).
Conclusion: Patient-reported outcome measures favored cementless, press fit fixation through two years postoperatively, with outcomes equalizing between the groups at three years postoperatively. Given the better early outcomes with the press fit design, there does not seem to be a need to augment fixation with cement in this total ankle implant design. There were two metal component revisions and one revision associated with loosening in the cementless group. The significant demographic differences between the groups indicate that a randomized clinical trial is needed to comprehensively define differences in early outcomes and to evaluate long-term results.
DOI: 10.1177/2473011421S00511
The Impact of Forefoot Alignment and Arthritic Change on Conversion to Fusion after Synthetic Cartilage Implant Placement for Hallux Rigidus
Alastair S. Younger, MB ChB, ChM, FRCSC; Judith F. Baumhauer, MD, MS, MPH; Christopher W. DiGiovanni, MD; Timothy R. Daniels, MD, FRCSC; Mark A. Glazebrook, MD, MSc, PhD; David Fitch
Category: Midfoot/Forefoot
Keywords: Hallux Rigidus; 1st MTP Joint; Structural Anatomy and Biomechanics
Introduction/Purpose: There are several treatments for hallux rigidus, including the use of a synthetic cartilage implant (SCI). Level I studies have shown success with these implants, but some patients do require conversion to arthrodesis for ongoing symptoms. The purpose of this radiographic review was to examine if baseline bone alignment, dimensions, and arthritis status are were different for patients who required conversion to arthrodesis compared to a control group with successful outcome.
Methods: A radiographic review was conducted using data for from 15 hallux rigidus subjects implanted with an SCI enrolled in a during a previously concluded Level 1 clinical trial. Ten (10) Success subjects were identified as subjects those without conversion and with the lowest VAS pain levels indicating the most favorable outcome formed a success (control) group. Five (5) Conversion (study) subjects were identified as those with a conversion requiring revision to fusion and the with highest VAS scores indicating the least favorable outcome. Preoperative Weight-bearing AP and lateral radiographs from baseline visits were reviewed. Using previously validated Quantitative Motion Analysis software, two radiologists made the following measurements: first interphalangeal angle; first/second intermetatarsal angle; hallux valgus intraphalangeal angle; metatarsus adductus angle; metatarsal declination angle; first to second metatarsal length; functional ratio; and first metatarsal cortical thickness. Preoperative assessments of arthritis grade, metatarsalus primus elevatuselevation, sesamoid arthritis, and sesamoid station were also performed.
Results: First metatarsal length was approximately 3% larger longer in the Conversion group compared to the Success group (85.2% vs. 82.5%). This was driven by the Conversion group having longer median normalized first metatarsal length (88.5% vs. 86.6%) and shorter median normalized second metatarsal lengths (104.0% vs. 106.3%). First metatarsal The second exception was cortical thickness was greater in the conversion group. This measurement was defined as the combined width of the medial and lateral cortices measured at the midline of the first metatarsal normalized to the full midline diameter of the first metatarsal. The median cortical thickness was almost 7% larger in the Conversion group compared to the Success group (40.1% vs. 33.2%). Nine Success subjects and 2 Conversion subjects had Grade 3 arthritis, while all other subjects had Grade 2. Three (60%) Conversion subjects and two (20%) Success subjects had evidence of metatarsus primus elevatus.
Conclusion: Baseline joint alignment did not correlate with the need for conversion to arthrodesis. Conversion subjects had larger functional ratios longer first rays and greater cortical thickness. Published literature suggests smaller functional ratios result in increased second ray loading. It is possible the opposite is occurring in Conversion subjects, with longer first and shorter second metatarsal lengths resulting in increased loading of the SCI implant. The result indicates that shortening the first ray may be required to achieve a successful outcome with SCI. Success patients had a lower incidence of metatarsus primus elevatus.
DOI: 10.1177/2473011421S00512
Outcomes and Cost Analysis of Virtual Fracture Clinic Management of 5th Metatarsal Base Fractures
Nusrat Zahan; Amit Patel, FRCS(Orth); Kate Atkinson, MBBS MRCS; Shilpa Jha, MBBS MRCS; Nima Heidari; Lee Parker, FRCS(Tr&Orth); Alexandros Vris; Francesc Malagelada Romans; Luckshmana A. Jeyaseelan
Category: Midfoot/Forefoot; Trauma
Keywords: 5th Metatarsal Fractures; Jones Fracture; Cost Effectiveness Analysis
Introduction/Purpose: Overwhelming demand for trauma services with increasing emergency department (ED) attendances, has increased pressure on fracture clinics in many units, with this demand exceeding capacity. Virtual fracture clinics (VFCs) have been shown to be safe and cost-effective in many specialties. Optimal treatment of 5th metatarsal base fractures remains controversial. Complications of base of 5th metatarsal fractures include delayed union and painful mal/non-union. Surgical fixation has been shown to enable faster return to sport, with lower faster union times and lower non-union rates than conservative management. The aims of this study were to assess whether the management of 5th metatarsal base fractures using a VFC model is safe, cost-effective and accceptable to the patients, whilst avoiding undesirable outcomes.
Methods: All patients presenting to the VFC at our major trauma centre, with a 5th metatarsal base fracture between January 2019 and December 2019 were included in the study. One hundred and thirty six patients were identified. All patients had a standardised VFC treatment protocol including full weight bearing in a walker boot, rehabilitation planning to wean out of the boot and advice to contact the unit for follow-up if ongoing pain after 4 months. Minimum follow-up was one year. Patient records were retrospectively reviewed for baseline demographic data, including co-morbidities and smoking history. Overall complication rates, including mal and non-union as well as operative intervention rates were noted. Patients from the cohort who required face to face appointments were identified and the cause for return was identified. A cost analysis was also performed to evaluate the financial implications of the service.
Results: Mean age was 41,6 years (18-92). Average time from ED attendance to VFC review was 2 days (1 - 5). Fractures were classified according to the Torg Classification with 106 (78%) Type 1 fractures, 15 (11%) Type 2 fractures and 15 (11%) Type 3 fractures. At VFC, 135/136 (99.2%) were discharged with the appropriate 5th metatarsal base fracture protocol. Twelve patients (8.8%) arranged further follow-up after initial discharge. The most common reason for return was ongoing pain (6/8 - 75.0%). This subgroup of the patients required an average of 3 (1-6) further appointments. There was 1 non-union during the study period. Based on 2 face to face visits on a traditional pathway, 248 clinic visits were saved with an approximate cost saving of nearly £40,000 ($55,500).
Conclusion: Our study supports the management of 5th metatarsal base fractures in the VFC setting. We have shown that the VFC model, with well a defined protocol is both safe and cost effective. Fifth metatarsal base fractures have good outcomes with conservative management, removing the traditional need to have in-person clinic visits to confirm the diagnosis, management and prognosis.
DOI: 10.1177/2473011421S00513
Assessing the Accuracy, Quality, and Readability of Online Patient Resources on Tarsal Coalition
Hui Zhang, MD; Brian Foster; Jove Graham, PhD; Mark Seeley
Category: Other; Hindfoot
Keywords: Health Literacy; Patient Education; Patient Comprehension
Introduction/Purpose: The internet is an inexpensive and convenient source for health information. However, without regulation, the quality and accuracy of the information is unknown. Tarsal coalition is a common cause of pediatric foot pain and disability. We hypothesized that the online patient information on tarsal coalition is of low accuracy, low quality, and of poor readability. Additionally, we hypothesized that sources found on the first search page were of higher quality, greater accuracy, and more readable.
Methods: A cross-sectional review of the internet was performed using the term 'tarsal coalition' on the 3 most popular search engines. Unique sites were categorized based on authorship and search result order. Websites were evaluated using a novel content score based on the AAOS OrthoInfo site on tarsal coalition (max score: 20), JAMA Benchmark and DISCERN scores for quality, and Flesch-Kincaid Grade Level (FKGL) and Flesch Reading Ease (FRE) for readability.
Results: A total of 47 unique websites were evaluated. They ranged from professional organization/society websites to websites for individual practices and professional blogs. The average content score was 13.1 (range: 4-20). The average DISCRN score was 34.2 (range: 19-57.5). We did find a positive correlation between the content score and DISCERN scores of the included resources (p=0.04). The average 11.4 (range 8.5-15.5). Only 2 of the websites (4%) were written at or below an 8th grade reading level, which has been documented as the average reading level of the general population in the United States. Websites that were authored by physicians had greater DISCRN and readability scores compared to academic and private practice websites (DISCERN 40.4 vs 32.3 (p=0.001) and 31.7 (p=0.01), respectively, FKGL 13.0 vs 10.4 (p=0.002) and 11.1 (p=0.03), respectively, FRE 31.5 vs 48.7 (p=0.0001) and 45.2 (p=0.025), respectively).
Conclusion: Online patient resources on tarsal coalition are of low quality, inaccurate, and too complex for the average reader. Physician authored websites may serve as better resources compared to academic or private practice sites. Physicians should caution patients using the internet for information on tarsal coalition.
DOI: 10.1177/2473011421S00514
The Lateral Drawer Test: A Novel Clinical Test to Assess Mortise Instability in Weber B Fibula Fractures
John Z. Zhao, MD; Caroline Williams, BA; Kimberly K. Broughton, MD; Christopher P. Miller, MD; John Y. Kwon, MD
Category: Trauma; Ankle
Keywords: Ankle Fracture Evaluation; Ankle Fracture; Weber B Ankle Fractures
Introduction/Purpose: Assessment of mortise stability is paramount in determining appropriate management of ankle fractures. While instability is readily apparent in bimalleolar or trimalleolar ankle fractures, determination of instability in the apparent isolated Weber B fibula fracture often requires further investigations such as stress radiography. While several authors have previously demonstrated poor predictive value of physical examination findings such as tenderness, ecchymosis and swelling with instability, no previous investigation has examined the ability of a translational test to determine deltoid ligament injury. The goal of this study is to test the validity of a novel clinical test, the lateral drawer test, in determining mortise instability in a cohort of patients with Weber B fibula fractures.
Methods: Patients presenting with isolated fibula fractures were prospectively identified by an orthopaedic nurse practitioner or resident. Three views of the ankle as well as gravity stress views (GSV) were obtained. Prior to examining radiographs, two foot & ankle fellowship-trained orthopaedic surgeons (JYK, CPM) performed and graded the lateral drawer test. (Grade 0: no instability/symmetric to contralateral ankle, Grade I: translation < 5mm, Grade II: translation >= 5mm) While the surgeons were made aware of the presence of a Weber B fibula fracture, radiographs were not visualized prior to conducting the drawer test. Medial clear space (MCS) was measured. VAS pain scores were obtained before and after testing. The results of the lateral drawer test results were compared with radiographic measurements of MCS.
Results: The study enrolled 57 consecutive patients with Weber B ankle fractures. Twenty-nine (51%) patients demonstrated radiographic instability with widening of the medial clear space >= 5 mm on GSV. When correlated with MCS measurement, the lateral drawer test demonstrated a sensitivity of 83.3%, specificity of 96%, positive predictive value (PPV) of 96% and negative predictive value (NPV) of 84% for determining instability. There was a strong correlation between the lateral drawer test grade and amount of MCS widening (⍴=0.82, p<0.001). Patients tolerated the lateral drawer test well with an average increase of 0.8 points on the VAS pain scale after testing.
Conclusion: The lateral drawer test demonstrates high sensitivity, specificity, PPV and NPV for detecting instability in patients presenting with Weber B fibula fractures. While further validation is required in a larger cohort of patients, the lateral drawer test may offer an adjunct tool via physical examination to predict mortise stability.
DOI: 10.1177/2473011421S00515
Obesity Increases Risk for Surgical Site Infections and Wound Dehiscence after Pediatric Foot Surgery: A Retrospective Cohort Review using the NSQIP-Pediatric Database
Jacob R. Zide, MD; Farzam Farahani, BS; Joel Rodriguez, BS; Dane K. Wukich, MD; Anthony Riccio
Category: Other
Keywords: Complications; Surgical Site Infection; Obesity
Introduction/Purpose: Both the incidence of childhood obesity and the number of obese children undergoing surgical procedures are increasing in pediatrics. As such, pediatric orthopaedic surgeons will likely encounter obese patients more frequently in their practice and a better understanding of the unique risks associated with obesity is valuable to maximize patient safety. The purpose of this study is, therefore, to retrospectively evaluate the relationship between obesity and post-operative outcomes in pediatric orthopaedic surgery patients across multiple institutions using a large national database.
Methods: Pediatric patients who had undergone foot surgery were retrospectively identified by cross-referencing reconstructive foot-specific CPT codes with ICD-9/ICD-10 diagnosis codes using the American College of Surgeons 2012-2017 Pediatric National Surgical Quality Improvement (ACS-NSQIP-Pediatric) database. Patients were stratified into normal weight and obese cohorts based upon Center for Disease Control BMI-to-age growth charts. Patient demographics, comorbidities, intra-operative, and post- operative factors were compared between these two cohorts via univariate analysis with false discovery rate adjustment. Multivariable logistic regression models were then generated to assess for obesity as an independent predictor of post-operative complications.
Results: Of the 3,924 patients identified, 1,063 (27.1%) were obese. Obese patients were more often male (64.7% vs 58.7%; p=0.001) and taller (56.3in vs 51.3in; p<0.001) than normal weight patients. There were no differences in pre-operative comorbidities between the two cohorts. Obese patients had a higher overall post-operative complication rate compared to normal weight patients (3.01% vs 1.32%; p=0.001). There was a significantly higher rate of wound dehiscence in obese patients (1.41% vs 0.59%; p=0.039) as well as a higher surgical site infection (SSI) rate that trended towards, but did not reach, statistical significance (1.32% vs. 0.59%; p=0.061). No differences were noted in unplanned readmissions (1.03% vs 0.9%; p=0.968) or unplanned reoperations (1.03% vs. 0.45%; p=0.175) within 30 days of surgery between the two groups. In multivariate analysis, obesity was found to be an independent predictor of both wound dehiscence (adjusted OR=2.16; 95%CI=1.05-4.50; p=0.037) and SSI (adjusted OR=3.03; 95%CI=1.39-6.61; p=0.005).
Conclusion: Obese children undergoing foot surgery had higher overall complication rates than normal weight patients. Obese children undergoing foot surgery may be at higher risk for wound complications and surgical site infections than those of normal weight. This information may be useful in assessing and discussing surgical risks with patients and their families.
DOI: 10.1177/2473011421S00516
EXOGEN Mitigates Risk of Fifth Metatarsal Fracture Nonunion: Results of a Novel Real-World Clinical Study
Robert Zura; Robert B. Anderson, MD; Sonya S. Ahmed, MD; David Hak; Tracy Watson; Christina Mack; Debra E. Irwin; Greg Maislin, MS, MA; Kim P. Kelly; John T. Jones; Tawana Wester; Alessandra Pavesio; Kevin Ong
Introduction/Purpose: Fifth metatarsal fractures are the most commonly fractured metatarsal in adults and are associated with high rates of nonunion. This study compared the 9-month incidence of nonunion in fifth metatarsal fracture patients using EXOGEN (Bioventus LLC), low-intensity pulsed ultrasound, versus a control cohort of patients receiving standard of care.
Methods: Adults (21-80 years) prescribed EXOGEN for any acute or delayed fifth metatarsal fracture and initiated treatment within 91 days of the fracture were enrolled via prescription record abstraction and direct-to-patient outreach. Open, closed, surgically repaired and conservatively managed fractures were eligible. Jones' fractures consisted of 31.2% of the overall EXOGEN population. EXOGEN treatment compliance was assessed using patient self-report and the device’s software. A control cohort of patients with the same eligible fractures were extracted from the MarketScanTM national insurance database (IBM Watson Health). Propensity score (PS) modeling accounting for demographics, comorbidities, concomitant medication, and type of fracture/fracture treatment was used to address potential selection bias via three methods: subclassification, 1:1 matching on individual covariates, and PS weighting. Effectiveness was compared for 1,943 EXOGEN and 10,259 controls. Study endpoint was based on presence or absence of an ICD-10-CM nonunion diagnosis code in the medical billing records for both groups.
Results: Matched MarketScan controls had a clinically and statistically significant increase in risk of nonunion compared to patients who used EXOGEN for at least 90 total once-daily treatments (McNemar’s OR = 1.67; p=0.048). Results improved with more treatments; the nonunion risk was 2.44 times (p=0.0239) and 5.00 times (p=0.008) for the control patients than EXOGEN patients with at least 120 and 140 total treatments, respectively. The nonunion rate was reduced by over half in Jones’ fracture patients treated with at least 90 total once-daily EXOGEN treatments (n=269; 3.3%) as compared to those not reaching this minimum threshold (n=337, 6.8%); such results approached statistical significance (p=0.057). Analyses of the treatment effect by nonunion risk factors showed EXOGEN attenuated the effect of many of these factors on nonunion rates. Early treatment was found beneficial; treatment delay was associated with increased nonunion risk of ~20% for every 15 days of latency 45 days post- fracture.
Conclusion: In this large external comparator study, EXOGEN was found to be effective in mitigating the risk of nonunion in fifth metatarsal fracture patients when used for a minimum of 90 total treatments, even in the presence of many nonunion risk factors. Treatment should be initiated as soon as possible following fracture (at least by 45 days post-fracture) to further reduce the risk of nonunion.