
Abstract
Background:
There remains a paucity of data regarding long-term patient-reported outcomes following Lisfranc injuries. We sought to collect long-term clinical outcome data following Lisfranc injuries using PROMIS Physical Function (PROMIS-PF) and visual analog scale–foot and ankle (VAS-FA).
Methods:
A chart review was performed to identify all patients who had surgical treatment of an acute Lisfranc injury at our institution from 2005 to 2014. Of the 45 patients identified, we were able to recruit 19 for a follow-up clinic visit consisting of physical examination, administration of questionnaires addressing pain and medication usage, radiographs, and completion of outcome surveys including PROMIS-Physical Function and visual analog scale–foot and ankle.
Results:
There were 14 female and 5 male patients enrolled in the study with a mean time of 6.25 years from the time of injury. Within this cohort, the mean PROMIS-PF score was 52.4±8.2 and the mean VAS–foot and ankle score was 76.6±22.3.
Conclusion:
We report satisfactory long-term patient-reported outcomes using PROMIS-PF and VAS-FA.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Accounting for nearly 0.2% of fractures, Lisfranc injuries are a rare but noteworthy cause of midfoot pathology. 2 Fifty-eight percent of these injuries occur in polytrauma patients, further complicating the evaluation. 15 Moreover, it has been found that 20% of Lisfranc injuries are misdiagnosed or completely missed at first presentation. 5,15 As a consequence, significant morbidity and disability can occur because of Lisfranc injuries.
The mechanism of injury often involves an axial load on the foot or sudden plantarflexion combined with a rotational force, often as a result of fall from height or motor vehicle accident. 6 Lisfranc injuries can be described as bony, ligamentous, or both. Numerous classification systems have been developed to describe the disruption of the joint complex. 7,15 However, it must be noted that these classification systems are useful in describing the radiographic morphology of the injury but have not been shown to correlate with outcomes. 12,15
Numerous measurement systems exist that attempt to quantify subjective clinical outcomes into a numerical score that can be measured and compared. Pertaining to the foot, these outcome scores include but are not limited to the American Orthopaedic Foot & Ankle Society (AOFAS), Foot Function Index, Foot and Ankle Outcome Score, Foot and Ankle Ability Measure, visual analog scale–foot and ankle (VAS-FA), and Lublin Foot Functional Score. 12,16,18,22,24 Owing to the relative rarity of Lisfranc injuries in addition to challenges faced in data collection for traumatic orthopedic injuries, there is a paucity of outcomes literature on Lisfranc injuries.
The Patient-Reported Outcomes Measurement Information System (PROMIS) was developed by the National Institutes of Health as a means of standardizing patient-reported outcomes related to social, mental, and physical health. This consists of a computerized adaptive testing (CAT) system that converts raw data into a standardized score with a mean of 50 and a standard deviation (SD) of 10. This score has been validated in numerous and varying patient cohorts. 4,10
Though the treatment of Lisfranc injuries is variable and includes but is not limited to closed reduction and percutaneous pinning, open reduction and internal fixation (ORIF), and primary arthrodesis (PA), 1,12,16,24 the purpose of this study was to present long-term PROMIS-PF and VAS-FA scores in patients with Lisfranc injuries after ORIF. We hypothesized that following surgically treated Lisfranc injury, long-term patient-reported outcomes will represent a significant decrease in physical function as well as increased pain.
Methodology
A retrospective chart review was performed of all skeletally mature patients who were consecutively treated surgically for a Lisfranc injury at our institution between 2005 and 2014. Patients were excluded if they were <18 or >65 years of age or had an open fracture, concurrent fracture or dislocation of the contralateral extremity, injuries treated with absorbable screws, previous ipsilateral foot trauma or surgery, peripheral vascular disease, peripheral neuropathy, and/or rheumatoid arthritis. Patients with contralateral-sided lower extremity injuries were excluded to best compare postoperative outcomes as rehabilitation processes vary significantly among those with bilateral injuries. The study was approved by our institution’s Internal Review Board (IRB no. HUM00097838). Funding was provided by an internal grant.
After identifying 45 patients who met our inclusion criteria and had a minimum of 6 months of follow-up, we attempted to recruit these patients via standardized letters and phone calls. Electronic medical records were used to identify interval between injury and surgery, and interval between injury and most recent follow-up. Of the 45 patients, we were able to recruit 19 for an interval follow-up clinic visit. These visits consisted of clinical examination, questionnaires regarding pain and medication usage, 3-view weightbearing radiographs of the affected foot, and completion of outcome surveys, VAS-FA scores, and PROMIS-PF. VAS-FA scores were then subcategorized into scores depicting function (VAS-Function), pain (VAS-Pain), and other (VAS-Other).
Descriptive and inferential statistics were analyzed using SPSS, version 22.0 (IBM, Armonk, NY). The demographic and clinical characteristics were described by using raw counts, measures of central tendency (mean and standard deviation, proportions, and measures of data dispersion (eg, 95% confidence intervals where appropriate in the regressions). We evaluated the data for normality (ie, z scores, histograms, skewness, and kurtosis).
Results
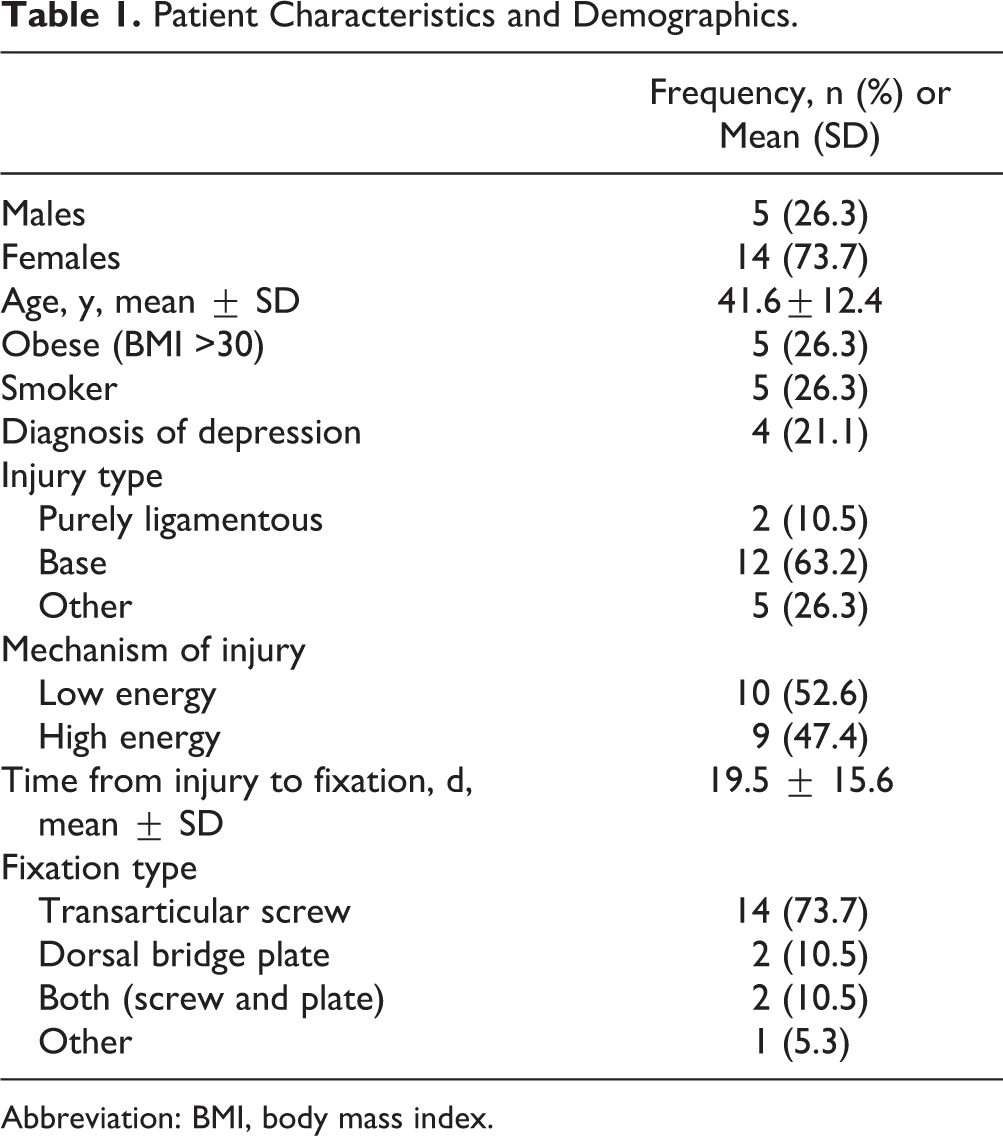
There were 14 female and 5 male patients who were enrolled in the study with an average age of 41.6±12.4 years (range 23-60 years) at the time of injury. The mean time to follow-up was 6.25 years (range 3.1-10 years). No patients had previous foot trauma or surgery in their lower extremity. Two patients sustained purely ligamentous injuries, 12 patients sustained metatarsal base fractures, and 5 patients sustained a combination of injuries (“other” category). Ten patients had a low-energy mechanism whereas 9 had a high-energy mechanism of injury—either motor vehicle accident or fall from significant height >6 ft (Table 1). Five (26%) patients were noted to have minimal subluxation (<2 mm) on initial radiographs. Six different board-certified orthopedic surgeons from a single institution operated on the patient group. Time from injury to surgery averaged 19.1±15.6 days with a range of 6-77 days. In the cohort of 19 patients, 14 underwent transarticular screw fixation, 2 underwent dorsal bridge plating, 2 underwent both transarticular screw fixation with dorsal bridge plating, and 1 underwent a combination of fixation using both dorsal plating and the use of 2 transarticular screws. Anatomic reduction was achieved in all but 4 of the patients (15/19, or 79%). Fifteen patients had an additional procedure for removal of hardware between 19 and 152 days after their index surgery; as shown in one patient in Figure 1C and D. There were several complications within the study group (Table 2). Two patients developed a deep vein thrombosis after the index procedure. During follow-up, 2 patients had examination and radiographic changes indicative of arthritis, with one having metatarsalgia and the other encountering screw loosening.
Patient Characteristics and Demographics.
Abbreviation: BMI, body mass index.

Standing injury, short-term and long-term postoperative radiographs of patient with Lisfranc injury in study. Standing (anterior-posterior) radiographs illustrating (A) day of injury; (B) 2 months status post open reduction internal fixation; (C) 8 months postoperation status post removal of hardware; (D) approximately 10-year follow-up.
Complications.

The mean PROMIS-PF score was 52.4±8.18, the mean VAS-Foot and Ankle score was 76.6±22.3, the mean VAS-Function score was 79.7±22.1, the mean VAS-Pain score was 79.5±26.0, and the mean VAS-Other score was 70.9±22.8 (Table 3). Similar results were obtained for VAS-FA with P < .05.
Patient-Reported Outcomes.

Abbreviations: PROMIS-PF, Patient-Reported Outcomes Measurement Information System Physical Function; VAS, visual analog scale.
Discussion
We sought to expand on the literature of Lisfranc injury outcomes, specifically using PROMIS-PF and VAS-FA scores. Particular to lower extremity injuries, PROMIS scores have proven to have greater reliability, validity, and dimensionality compared with 36-Item Short Form Health Survey—a generic outcomes instrument. 10 Further, the VAS-FA was created as a means of assessing purely subjective outcomes specific to foot and ankle patients. 17 After analyzing 19 patients who sustained such injuries, we found that the mean PROMIS-PF score was 52.4 ± 8.18, suggesting that our patient cohort did no worse than the general population. However, the mean VAS-FA score in our cohort was 76.6±22.3, signifying a possible element of impairment from the injury but not quite at the level found by Stüber et al, albeit not in a directly comparable patient cohort. 21 To our knowledge, this is the first reporting of patient PROMIS-PF and VAS-FA scores during long-term follow-up of Lisfranc injuries.
Treatment of Lisfranc injuries can range from observation and nonoperative management, closed reduction and percutaneous pinning, ORIF, and PA in select circumstances. 1,12,16,24 There have been many studies analyzing differences in outcomes pertaining to management of these injuries. It has been found that worse outcomes are associated with more severe injuries. 13 The type of fixation, in particular, has also been a topic of great interest. One group looking at active-duty military population found that not only did ORIF not result in earlier return to duty over PA, but timing of surgery did not result in a difference in outcomes either. 8 Moreover, a large systematic review with 193 patients found no difference between ORIF and PA. 19 Furthermore, Henning et al 9 found no difference in patient satisfaction after long-term follow-up. Finally, Qiao et al 16 found no statistical difference in American Orthopaedic Foot & Ankle Society, 36-Item Short Form Health Survey, and VAS scores when comparing ORIF and arthrodesis.
Although the modes of treatment are numerous, the most important factor in predicting long-term outcomes has been shown to be the adequacy of reduction. 16,23 A large retrospective study found that nonanatomic reduction was a significant risk factor for developing posttraumatic osteoarthritis. 11 Despite this, another study found that anatomic reduction still resulted in poor American Orthopaedic Foot & Ankle Society midfoot scores. 23 Furthermore, early treatment has been shown to provide better outcomes than delayed treatment. 22
Complications post injury include midfoot arthritis, chronic pain, and pes planus, of which arthritis is the most common. 2 The development of osteoarthritis does not always require treatment, even when symptomatic; one study found that of 33 patients with symptomatic arthritis, only 4 patients had a secondary procedure. 3 Moreover, the treatment of arthritis and related pain remains controversial, whether it be ORIF or arthrodesis. 3,20 The matter is further complicated as the extent of radiologic arthritis does not correlate with patient clinical scores. 14
There were several limitations with our study. As with any retrospective study at a single institution, there is a possibility for selection bias. Moreover, those who agreed to return for follow-up examination may misrepresent the entire sample; however, this limitation is commonplace in studies of this type. The method of fixation was surgeon and situation dependent. There were also confounders, namely, those patients who did not have adequate follow-up. The time from injury to follow-up introduces the possibility of recall bias. Moreover, the small cohort size of 19 patients may have resulted in the limited power of results. Other issues were avoided with the use of a validated outcome scores (PROMIS and VAS-FA). Owing to the lack of literature, we were not able to compare our PROMIS-PF and VAS-FA scores to other studies. In the future, we hope to increase the patient cohort analyzed and thus widen the applicability of these results.
Conclusions
We report satisfactory long-term patient-reported outcomes using PROMIS-PF and VAS-FA in this relatively small cohort.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114211039496 – Supplemental material for Long-term Follow-up of Lisfranc Injuries Treated With Open Reduction Internal Fixation Patient-Reported Outcomes
Supplemental material, sj-pdf-1-fao-10.1177_24730114211039496 for Long-term Follow-up of Lisfranc Injuries Treated With Open Reduction Internal Fixation Patient-Reported Outcomes by Kempland C. Walley, Derek J. Semaan, Ronit Shah, Christopher Robbins, David M. Walton, James R. Holmes and Paul G. Talusan in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
The study was approved by our institution’s Internal Review Board (IRB# HUM00097838).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.