
Abstract
Background:
The proximal opening wedge osteotomy (POWO) of the first metatarsal (TMT-1) is commonly performed in the operative treatment of hallux valgus. Limited work has been dedicated to study POWO’s effect on the TMT-1 joint, however. The purpose of this study is to evaluate the changes in TMT-1 joint contact stress following POWO of the first metatarsal.
Methods:
Five fresh-frozen cadaveric below-knee specimens (mean age: 73 years) with hallux valgus deformities (mean hallux valgus angle [HVA]: 37.4 ± 8.5 degrees) were studied. The specimens were loaded to 400 N on an MTS servohydraulic load frame. Joint contact characteristics at TMT-1 joint were measured with a Tekscan pressure sensor (Model 6900, 1100 psi; Tekscan Inc, Boston, MA) with various opening wedge sizes of 3, 5, and 7 mm both without and with a distal soft tissue release (DSTR). The contact force, area, and peak contact stress were compared among groups using analysis of variance and post hoc multiple comparisons over the untreated (Dunnett test, P < .05).
Results:
The mean contact force was 47.7 ± 33.5 N for untreated specimens. This increased sequentially with opening wedge size and reached statistical significance for 7-mm opening wedge (129.7 ± 62.3 N, P = .01) and 7-mm wedge + DSTR (134.8 ± 60.5 N, P = .008). The mean peak contact stress was 2.8 ± 1.3 MPa for the untreated specimens and increased incrementally with wedge size to 5.7 ± 3.0 MPa for 7-mm wedge only (P = .03) and 5.6 ± 2.5 MPa for 7-mm wedge + DSTR (P = .05). The contact area increased with corrections, but none reached significance.
Conclusion:
With increasing opening wedge size, loading of the TMT-1 joint increases. Joint stresses higher than 4.7 MPa have been shown to be chondrotoxic, potentially predisposing patients to arthritic joint changes following POWO.
Level of Evidence:
XXXXXX
Introduction
Hallux valgus is the most common forefoot deformity present in the adult population. 10 Described as lateral deviation of the great toe and medial deviation of the first metatarsal, progressive subluxation of the first metatarsophalangeal (MTP) joint is a hallmark of this condition. 10 When conservative treatment fails, more than 100 operative procedures have been described as treatment options. 5 Proximal metatarsal osteotomies (PMOs) represent a number of different procedures in the proximal metatarsal. Proximal opening wedge osteotomy (POWO) is a shaft osteotomy used in the operative treatment of moderate to severe hallux valgus deformities. 14,16,17 Initial concerns regarding osteotomy stability, dorsal malunion, and subsequent transfer metatarsalgia have subsided with the advent of specifically designed, low-profile, locked plates. 18 Previous studies have reported on the outcomes of POWOs, demonstrating reliable correction of hallux valgus deformity with good to excellent outcomes. 2,11,12,14,16 Associated complications of the procedure include recurrence as well as hardware irritation and nonunion. 17
Limited research has been dedicated to the effect of this procedure on the first tarsometatarsal (TMT-1) joint in terms of contact pressure, stability, and accelerated advancement of arthritis. Instability at the TMT-1 joint has been implicated in the pathogenesis of hallux valgus, and in late stages, obvious arthrosis of the TMT-1 joint can be seen. Coughlin et al 4 demonstrated that sagittal plane instability could be corrected to normal levels with operative correction of hallux valgus with a proximal crescentic osteotomy and distal soft tissue release (DSTR) procedure. Interestingly, despite this reported improvement in TMT-1 stability following POWO, the authors have recognized in their clinical practice that some patients go on to develop arthritic changes to the TMT-1 joint after POWO procedures (Figure 1).

(A) Preoperative and (B) postoperative (7 months) images of a patient who underwent a proximal metatarsal osteotomy utilizing a 4 mm wedge plate. The postoperative image shows medial metatarsal subluxation, incongruity of the joint, and loss of joint space medially.
To our knowledge, there have been no published studies investigating changes in TMT-1 contact pressures following POWO of the fist metatarsal. The primary purpose of this study is to evaluate the changes in TMT-1 joint pressure in the diseased and corrected state following proximal metatarsal osteotomy. The secondary purpose of the study is to evaluate the effect of a DSTR as it relates to radiographic correction and TMT-1 joint pressure. We hypothesize that TMT-1 joint pressure increases with growing opening wedge osteotomy size, and that this change is reduced with the addition of a DSTR.
Materials and Methods
Five fresh-frozen cadaveric below-knee specimens with moderate and severe hallux valgus deformities were obtained from 4 donors (mean age: 73.0 years, range: 58-78 years). There were 3 left and 2 right specimens. Three feet were from male donors and 2 from 1 female donor. The lower leg of these specimens was transected approximately 20 cm proximal to the ankle. The specimens were thawed at room temperature overnight prior to testing. Following similar protocol as a previous study, the passive range of motion of the first MTP joint in dorsiflexion and plantar flexion was measured with a goniometer. 6
About 1-inch segment of the proximal end of the tibia and fibula was exposed; a loading cylinder was mounted against the proximal surface of the tibia and, with a threaded rod, was inserted into the canal of the tibia. The specimen was then mounted onto a servo-hydraulic load frame (Landmark 370; MTS Systems, Eden Prairies, MN) with the tibia at 90 degrees to the neutrally positioned foot. Axial compression up to 400 N (simulating double-leg stance, assuming average North American body mass of 82 kg based on data from the Centers for Disease Control and Prevention) was applied through the tibial (Figure 2).

Experimental setup with pressure sensor in place prior to load applications.
Joint contact properties at the TMT-1 joint was measured with a pressure sensor (model 6900, 1100 psi; Tekscan Inc). The sensor has a resolution of 121 sensing elements over the area of 13 by 13 mm, and has previously been used to study contact mechanics of small joints of the foot, 7,19,20 and the radiocapitellar joint of the elbow. 1 Before being used in the tests in the present study, the sensor was calibrated in-house against the MTS loadcell. A conversion equation was fitted by using polynomial regression. To place the sensor in the joint, the superficial soft tissues were first exposed around the medial midfoot to allow visualization of the TMT-1 joint. A dorsal-medial capsulotomy was performed to allow for insertion of the pressure sensor while the joint space was manually distracted. This sensor was consistently seated in the same orientation inside the TMT-1 joint. The sensor data were collected at 100 Hz for 1 second while the load held at the peak value. The mean of the 100 samples was used in the analysis. The contact area and pressure distribution were obtained from the sensor software; from these results and calibration formula, the joint contact force and peak contact pressure were derived.
A standard proximal metatarsal osteotomy was performed 1 cm distal to the TMT joint. 16 The lateral bony cortex was preserved, acting as a hinge through the osteotomy. Various-sized metal wedges (3, 5, and 7 mm) with locking plates and screws were inserted in the osteotomy for correction of the varus positioning of the first metatarsal. The fixation and wedge sizes are clinically relevant and widely used. Following these initial series of tests, a complete DSTR was performed, including tenotomy of the abductor tendon, release of the transverse tarsal ligament, and lateral MTP joint capsulotomy. The specimens were then retested in the manner described above.
In total, 7 configurations were repeatedly tested in each specimen in the following sequence: Untreated specimen (Untreated) Specimen with POWO and 3-mm wedge with intact distal soft tissues (3 mm) Specimen with POWO and 5-mm wedge with intact distal soft tissues (5 mm) Specimen with POWO and 7-mm wedge with intact distal soft tissues (7 mm) Specimen with POWO and 7-mm wedge with DSTR (7 mm_DSTR) Specimen with POWO and 5-mm wedge with DSTR (5 mm_DSTR) Specimen with POWO and 3-mm wedge with DSTR (3 mm_DSTR)
For each testing condition, a single dorsoplantar weightbearing radiograph with a 15-degree tilt was obtained using a portable radiograph unit and a flat panel digital detection system (resolution: 2048 × 2048). A custom-built stand was made to hold the foot/ankle specimen and axially load it to 400 N via slotted weights. The intermetatarsal angle (IMA) and hallux valgus angle (HVA) were measured, and the congruency of the TMT-1 joint was assessed (Figure 3). All radiographic measurements were performed using the NIH ImageJ software. Additionally, the percentage length increases of the first metatarsal with each correction was assessed on the weightbearing radiographs to determine its potential effect on the joint pressure. This was represented as the length ratio between the first and second metatarsal at each condition.

Radiograph showing intermetatarsal angle and hallux valgus angle.
The joint contact metrics, including the contact force, contact area, and peak contact pressure at the TMT-1 joint under 400 N, along with radiographic measurements (IMA, HVA, first metatarsal length increase) were compared among the groups. One-way analysis of variance was used to determine if there was a significant difference between configurations. Post hoc multiple comparisons using Dunnett tests were used to identify the specific correction group(s) over the untreated. To compare the effect of DSTR, 2-tailed ratio paired t tests of the corrections with and without DSTR were performed. The level of significance was set at .05.
Results
On average, the passive range of motion of the TMT-1 joint of the 5 specimens was 30.8 ± 16.7 degrees (range: 8-46 degrees) in dorsiflexion and 17.0 ± 8.3 degree (range: 5-25 degrees) in plantar flexion.
Joint Contact Force and Area
The mean (SD) contact force at TMT-1 joint for the untreated group was 47.7 ± 33.5 N. All 6 correction procedures increased the contact force incrementally with wedge size, with small release after DSTR (Figure 4). The increases were around 30% with the two 3-mm groups but elevated sharply for the 5- and 7-mm groups. These increases over the untreated reached the level of statistical significance with the 7-mm group (mean: 129.7 ± 62.3 N, P = .01) and the 7 mm_DSTR group (mean: 134.87 ± 60.5 N, P = .008).
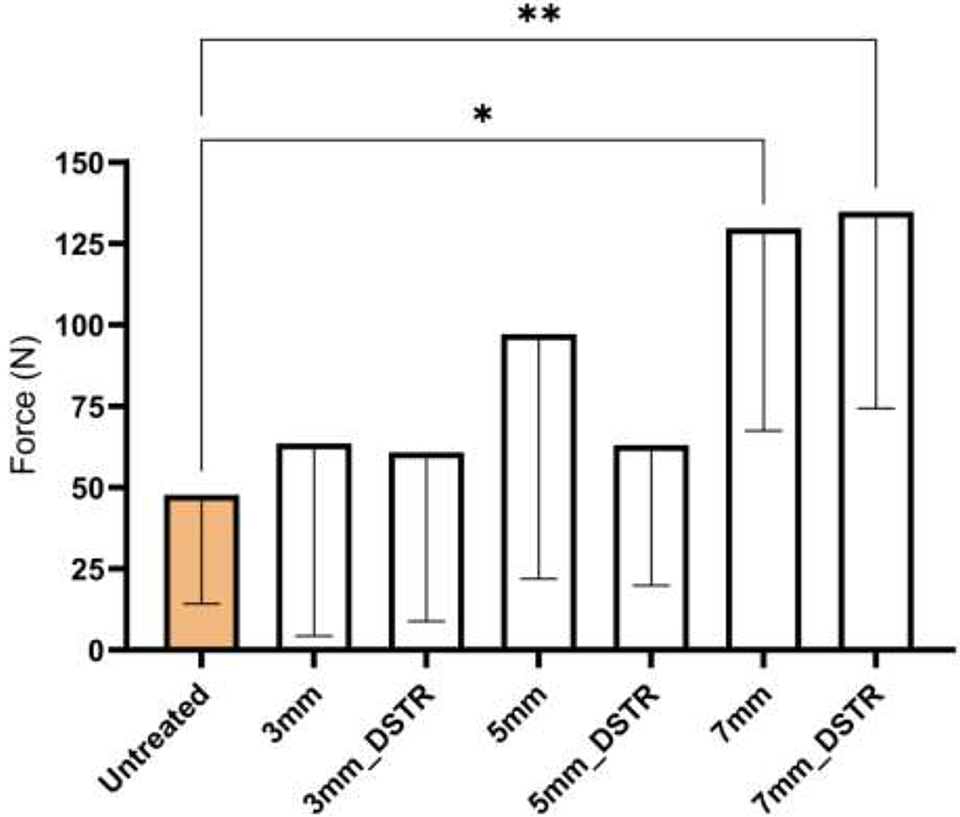
Mean (SD) of first metatarsal joint contact force. Asterisks indicate a significant difference over the untreated.
The mean (SD) contact area of the TMT-1 joint was 32.3 ± 17.4 mm2 for the untreated group. Like the joint contact force, the contact area also increased after all corrections. In the 3- and 5-mm wedge groups, the mean contact area increases were not significant, ranging from 35.8 ± 19.5 to 60.7 ± 32.9 mm2. The contact area peaked in the 7 mm_DSTR group (68.5 ± 21.0 mm2) and was statistically significant over the untreated (P = .04). The addition of DSTR had no effect on the contact area and nonsignificant 7% mean reduction in contact force.
Peak Contact Pressure
The peak contact pressure of the TMT-1 joint followed a similar incremental increasing trend as the contact force (Figure 5

Mean (SD) of first metatarsal joint peak contact pressure. Asterisks indicate a significant difference over the untreated.
Radiographic Measurements
For the untreated specimens, the mean HVA was 37.4 ± 8.5 degrees (range: 24-47 degrees), and the mean of IMA was 15.2 ± 2.7 degrees (range: 11-18 degrees). Both angles decreased with operative corrections (Figure 6). The decreases in HVA and IMA were inversely proportional to the wedge size. The differences in HV angle of the operative groups over the untreated group reach statistical significance in the 5-mm group (P = .01) and the 7 mm_DSTR group (P = .003). The differences in IMA of the operative groups over the untreated reached statistical significance for the 7-mm group (P = .002).

Mean (SD) intermetatarsal angles (IMA)and hallux valgus angles (HVA). Asterisks indicate a significant difference over the untreated.
Small increases of the first metatarsal length were found after correction procedures over the untreated stage. The mean of the percentage increase over untreated ranged from 1.9% to 7.1% (Table 1). The differences between these corrections were not statistically significant, but a trend of linear increase was detected as the wedge size increased (P = .003).
Percentage Increase in First Metatarsal Length With Corrections Over Untreated.

Abbreviation: DSTR, distal soft tissue release
Discussion
Findings from the present study also show that the TMT-1 contact area increased with POWO size and reached maximum contact values at 7 mm (69 mm2). This finding indicates that a plateau in joint congruity is perhaps reached at a 5-mm wedge size. This relationship could have a subsequent effect on peak pressure within the joint. For instance, with 3- and 5-mm wedge sizes, we found moderate and non–statistically significant increases in peak stress compared with intact measurements. Although the force transmitted across the joint sequentially increased at these wedge sizes, the contact area increased as well, resulting in a modest effect on peak pressure. With a 7-mm wedge size, however, this increase in force was not distributed across an accompanying increased contact area, resulting in a >2-fold increase in peak pressure (5.7 ± 3.0 MPa, P = .03, and 5.6 ± 2.5 MPa + DSTR, P = .05) over intact measurements (2.8 ± 1.3 MPa).
Biomechanical studies of TMT joints in normal feet have identified the TMT-2 and TMT-3 joints as the primary weightbearing surfaces in the midfoot, with the TMT-1 bearing approximately 8% of the axial load applied to the foot in neutral position. 9 In this study, we found the TMT-1 joint of hallux valgus feet carry a slightly higher force, at 10% of applied load. More importantly, with sequential increases in opening wedge osteotomy size, the TMT-1 joint is subjected to a substantially increased loading environment. For instance, with a 7-mm opening wedge, mean contact forces reached nearly 30% of the applied load, or 3 times the level of untreated measurements (129.7 ± 6.3 N vs 47.7 ± 33.5 N, P = .01). The authors believe this increased joint loading environment following POWO could pose substantial implications on the long-term health of the TMT-1 joint.
POWO is a well-accepted option to correct moderate to severe hallux valgus. The advent of opening-wedge locked plates has improved this procedure, providing reliable deformity correction and encouraging patient outcomes. 2,11,12,14,16 However, limited attention has been dedicated to POWO’s effect on the adjacent TMT-1 joint. At our institution, we have seen multiple cases of TMT-1 joint arthrosis following POWO, necessitating subsequent intervention and, in some cases, fusion. It is unclear whether these arthritic findings are related to the underlying hallux valgus, some components of the procedure, or both.
Mechanical overload has been widely recognized as one major factor for the failure of articular cartilage. Sadeghi et al 13 in their analysis of articular cartilage damage in response to repetitive loading, described a critical peak contact stress of 4.7 MPa above which all articular cartilage samples in their study either cracked or fissured. This value fits between the measurements of 5- and 7-mm opening wedge in our study, suggesting the potential for cartilage damage of the TMT-1 joint following POWO with wedge size larger than 5 mm. The development of arthrosis of the TMT-1 joint following POWO of the first metatarsal has not been described in the prior literature. To our knowledge, this work is the first to demonstrate increased loading properties in the TMT-1 joint following POWO, which would likely predispose the joint to premature arthritic change.
A definitive explanation for the increased loading environment in the TMT-1 joint following POWO is at this time unclear; however, a potential etiology could be through lengthening of the first metatarsal. Kia et al, 7 in a study of similar design to our work, investigated joint forces of the first metatarsophalangeal (MTP) joint following POWO. They utilized opening wedges of varying sizes with the goal of obtaining an IMA of <9 degrees. Although they did not note a significant increase in joint reactive forces in the first MTP joint following POWO, they did report a median increase of first metatarsal length of 3.3% (2.9%-3.3%). 7 Saragas et al 14 also reported an average 2.3-mm increase in first metatarsal length following POWO in 46 patients (64 feet) utilizing primarily 2.0- and 2.5-mm opening wedges. Kugan et al, 8 in a saw bone model of POWO, reported increases in length of the first metatarsal of 2.6, 4.6, and 5.0 mm with 3, 5, and 7 mm opening wedge plates, respectively. Our results indicated sequential increases in first metatarsal length with opening wedge size, reaching an increase as high as 6.4% over untreated measurements (Table 1). A similar phenomenon has been well documented in the CCJ following operative correction of posterior tibial tendon deficiency, often referred to as “flatfoot” deformity. Joint pressures in the CCJ are increased in the diseased state, likely as a result of forefoot abduction. As this deformity is corrected with sequential lengthening of the lateral column through an Evan osteotomy, the joint pressure initially normalizes. Xia et al 20 demonstrated, however, that beyond a lateral column lengthening of 8 mm, the pressure in the CCJ increased dramatically. Cooper et al 3 reported similar results, with an 8-fold increase in compressive forces at the CCJ following an Evans osteotomy of 10 mm. We theorize that a similar mechanism may exist in the TMT-1 joint. Increased length of the first metatarsal could lead to overstuffing of the medial column of the midfoot, thereby generating increased stress through the proximal TMT-1 joint. Further study would need to be completed to investigate this theory.
A DSTR is commonly performed in conjunction with a POWO for correction of the hallux valgus. This procedure entails release of the transverse metatarsal ligament, tenotomy of the abductor tendon, and lateral capsulotomy. It has been theorized that increased tension on these soft tissues contribute to the deforming forces that result in hallux valgus, and that their release can contribute to correction. 15 We theorized that the soft tissues tension of these structures could contribute to higher forces at the TMT-1 joint following osteotomy, and that a subsequent DSTR would lead to a reduction in TMT-1 joint forces. Our data did not support this hypothesis, however. At all wedge sizes, the addition of a DSTR did not result in a significant decrease in mean contact forces or peak contact stress.
Our article has several weaknesses. First, this study uses a cadaveric model with relatively small sample size and did not apply normal forces across the joints seen in gait from muscle activation or progression of the center of force under the plantar aspect of the foot in stance phase. Second, we did not see a robust correction of HVA and IMA across specimens, though the procedures performed did correct the deformity. This could potentially be explained by the variability of our cadaveric samples, which differed both in the severity of their hallux valgus and pre-existing first MTP joint arthrosis. Third, we did not randomize the wedge size applications. Given our inconsistent HVA/IMA correction across specimens and low sample size, we were unable to determine the optimal degree of correction in order to limit increased loading through the TMT-1 joint. This has important clinical implications for the surgeon, who will need to weigh the degree of optimal correction of HVA/IMA against the increased loading properties across the TMT-1 joint with increasing opening wedge size. Additionally, our lab had limited ability to measure MTP-1 and TMT-1 range of motion with modern 3-dimensional techniques, and relied on manual goniometric analysis. The balance between HV correction and TMT-1 forces is a direction for future research.
Conclusion
The results from this study demonstrate that with sequentially increasing opening wedge size, loading through the TMT-1 joint increases. This may have implications for the long-term health of the TMT-1 joint following POWO using larger wedge sizes.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211026934 - First Tarsometatarsal Joint Loading After Sequential Correction of Hallux Valgus Using a Proximal Opening Wedge Metatarsal Osteotomy and Distal Soft Tissue Procedure
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211026934 for First Tarsometatarsal Joint Loading After Sequential Correction of Hallux Valgus Using a Proximal Opening Wedge Metatarsal Osteotomy and Distal Soft Tissue Procedure by Jonathan Kraus, Michael J. Ziegele, Mei Wang and Brian Law in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Ethics Approval
Ethical approval was not sought for this study because it was a cadaveric biomechanical study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.