
Abstract
Background:
Accurate identification of primary pathogens in foot infections remains challenging due to the diverse microbiome. Conventional culture may show false-positive or false-negative growth, leading to ineffective postoperative antibiotic treatment. Next-generation sequencing (NGS) has been explored as an alternative to standard culture in orthopedic infections. NGS is highly sensitive and can detect an entire bacterial genome along with genes conferring antibiotic resistance in a given sample. We investigated the potential use of NGS for accurate identification and quantification of microbes in infected diabetic foot ulcer (DFU). We hypothesize that NGS will aid identification of dominant pathogen and provide a more complete profile of microorganisms in infected DFUs compared to the standard culture method.
Methods:
Data were prospectively collected from 30 infected DFU patients who underwent operative treatment by a fellowship-trained orthopedic foot and ankle surgeon from October 2018 to September 2019. The average age of the patient was 60.4 years. Operative procedures performed were irrigation and debridement (12), toe or ray amputation (13), calcanectomies (4), and below-the-knee amputation (1). Infected bone specimens were obtained intraoperatively and processed for standard culture and NGS. Concordance between the standard culture and NGS was assessed.
Results:
In 29 of 30 patients, pathogens were identified by both NGS and culture, with a concordance rate of 70%. In standard culture, Staphylococcus aureus (58.6%) was the most common pathogen, followed by coagulase-negative Staphylococcus (24.1%), Corynebacterium striatum (17.2%), and Enterococcus faecalis (17.2%). In NGS, Finegoldia magna (44.8%) was the most common microorganism followed by S. aureus (41.4%), and Anaerococcus vaginalis (24.1%). On average, NGS revealed 5.1 (range, 1-11) pathogens in a given sample, whereas culture revealed 2.6 (range, 1-6) pathogens.
Conclusion:
NGS is an emerging molecular diagnostic method of microbial identification in orthopedic infection. It frequently provides different profiles of microorganisms along with antibiotic-resistant gene information compared to conventional culture in polymicrobial foot infection. Clinical use of NGS for management of foot and ankle infections warrants further investigation.
Level of Evidence:
Level II, diagnostic study.
Introduction
Deep musculoskeletal infections (MSKIs), such as infected diabetic foot ulcers (DFUs) and prosthetic joint infections (PJIs), are serious orthopedic conditions that are steadily increasing in frequency. 1,6,7,10,12 -18,20,21 DFUs are one of the most prevalent complications of diabetes mellitus, and are experienced by 19% to 34% of the diabetic population, with more than half leading to infection. 1,7,10,21 Two-thirds of lower extremity amputations are associated with infected DFU. 1,10,21 The diverse microbiome in DFUs and biofilm formation in infected bone create a complicated environment and prove challenging when trying to identify pathogens in DFUs. 7,10,22 The conventional diagnostic method of microbial culture is subject to spatial sampling error, contamination associated with instruments or the mishandling of specimen. As a result, it can lead to false-positive or false-negative growth, and ultimately may not provide a full representation of the DFU’s microbiome. 7,10 These inaccurate or negative cultures may lead to ineffective antibiotic treatment and recurrent infection. 13,16 Previous studies have demonstrated a high rate (46.2%) of recurrent infection within 3 months after debridement and antibiotic treatment of infected DFUs. 13 Because recurrent DFU infections often lead to unplanned hospital readmission and reoperation in patients with comorbidities, including neuropathy and hyperglycemia, it is critical to accurately identify the dominant pathogen for postoperative antibiotic therapy.
Molecular diagnostics have gained clinical attention for improved identification of the main pathogen and addressing false negative cultures in MSKIs. 2,7,8,12,13,16 -18,20 Genetic techniques including sequencing 16 S ribosomal RNA (rRNA), which is ubiquitous in prokaryotes, have been successful in determining greater counts of organisms present in DFU samples. 7,10,12,22 Next-generation sequencing (NGS) is a high-throughput, parallel sequencing diagnostic method in which billions of DNA fragments can be simultaneously sequenced. 5,6 Two broad methodologic approaches to implement NGS in MSKIs are currently used: (1) 16 S amplicon–targeted NGS and (2) shotgun metagenomic sequencing. 6,12,16 -18,20 16 S rRNA sequencing targets the hypervariable region of the 16rRNA gene, whereas shotgun metagenomics sequences all the genomic DNA from a given sample. By sequencing a specific region, the 16 S amplicon–targeted method encompasses more bacteria and fungi with a low risk of false positives, thus demonstrating utility for dominant pathogen detection in PJI. 6,10,12,16,17 To determine bacterial genome using NGS, the genome is split into multiple fragments that produce sequences ranging from hundreds to tens of thousands of bases in length. The constructed genome is then compared to a reference database to identify the organism. It is highly sensitive and is able to sequence and quantify an entire bacterial genome in a given sample. 5,6,16 Its application in pathogen identification in PJI after hip, knee, or shoulder arthroplasty has been explored. 12,16 -18,20 In one PJI study, standard cultures were positive in 60.7% whereas NGS was positive in 89.3% of PJI patients. 16 NGS was also able to identify potential pathogens in 81.8% of culture-negative infections, allowing species-specific targeted antibiotic therapy. 16
Given the challenges associated with accurately identifying dominant pathogens in polymicrobial infected foot ulcers with high recurrent infection rates, we sought to investigate the applicability of NGS for this cohort. One infected DFU study demonstrated that shorter duration (<6 weeks’) of DFUs led to NGS results with a less complex microbiome than chronic and longer durations of DFU. 11 This can be more advantageous in identifying antimicrobial therapy than standard culture. We hypothesize that NGS will provide a more accurate means of diagnosing and profiling microorganisms in infected foot ulcers compared to the standard culture method.
Methods
Patients were recruited from a fellowship-trained orthopedic foot and ankle surgeon’s practice from October 2018 to September 2019. Recruitment criteria included type 1 or 2 diabetes mellitus, older than 18 years, and presentation of an infected DFU that necessitated operative intervention (irrigation and debridement or amputations). Preoperative clinical symptoms and signs of infection (swelling, erythema, local tenderness or pain, warmth and purulent discharge, sinus tract and probe-to-bone tests) were documented. 9 Demographic data were collected, in addition to the duration of ulcer, comorbidities, and antibiotic status. Preoperative laboratory data, including glycated hemoglobin, white blood cell count, erythrocyte sedimentation rate, and C-reactive protein level were also obtained. The infected DFUs were measured and graded. 14 Patients with severe ischemia (ankle brachial index less than 0.45), a venous stasis ulcer, immunodeficiency, malnutrition (albumin less than 3.0 g/dL), presented as pregnant, or unconscious were excluded from the study.
Operative Procedures and Specimen Collection
Whenever possible, infected DFUs were managed by irrigation and debridement of the wound followed by daily wet-to-dry dressing change with normal saline. In patients with extensive soft tissue and bone necrosis with or without bacteremia, amputation of the infected part was necessary. Biomechanical derangement such as equinus or isolated gastrocnemius contracture was addressed by preforming concomitant Achilles tendon lengthening or gastrocnemius recession as indicated. Two pea-sized grossly infected bone samples at the base of the DFU were collected intraoperatively during wound debridement or amputation procedures. Samples were then placed into 2 separate sterile vials: one vial was transferred to the institutional microbiology lab for standard culture (aerobic, anaerobic, and fungal); the other was promptly stored in a –80°C freezer until it was shipped overnight at an ambient temperature to MicroGen (Lubbock, TX) for NGS analysis.
Next-Generation Sequencing
After the specimen arrived at the laboratory, the DNA was extracted and a quantitative polymerase chain reaction (qPCR) was performed to determine the bacterial burden and antibiotic resistance genes using specific primers. The initial qPCR report was sent to the PI within 24-48 hours from receipt of the specimen. The NGS assay followed. The DNA was amplified via PCR using forward and reverse primers flanking the regions of interest. For the detection of bacteria and fungi, the 2 areas of interest are highly conserved regions of the rRNA gene in bacteria (16 S and fungi [internal transcribed spacer]). Following the amplification process, the amplified DNA was organized based on amplified strength. Sample DNA was then loaded onto beads for emulsion PCR, which generated high sample levels of DNA for NGS. The sample was sequenced onto the Ion Torrent Personal Genome Machine system sequencing platform (ThermoFisher Scientific, Waltham, MA). After the denoting process (the removal of short sequences), the generated sequence reads were compared to a curated National Institutes of Health (NIH) Gen Bank database using USearch7 with agreement of at least 90% between sequence reads and the database. 21 The combined PCR and NGS reports were sent to the senior author within 4 days from the receipt of the specimen (Figure 1). The report list identified species based on the number of DNA copies and antibiotic-resistant genes present that were detected using qPCR.
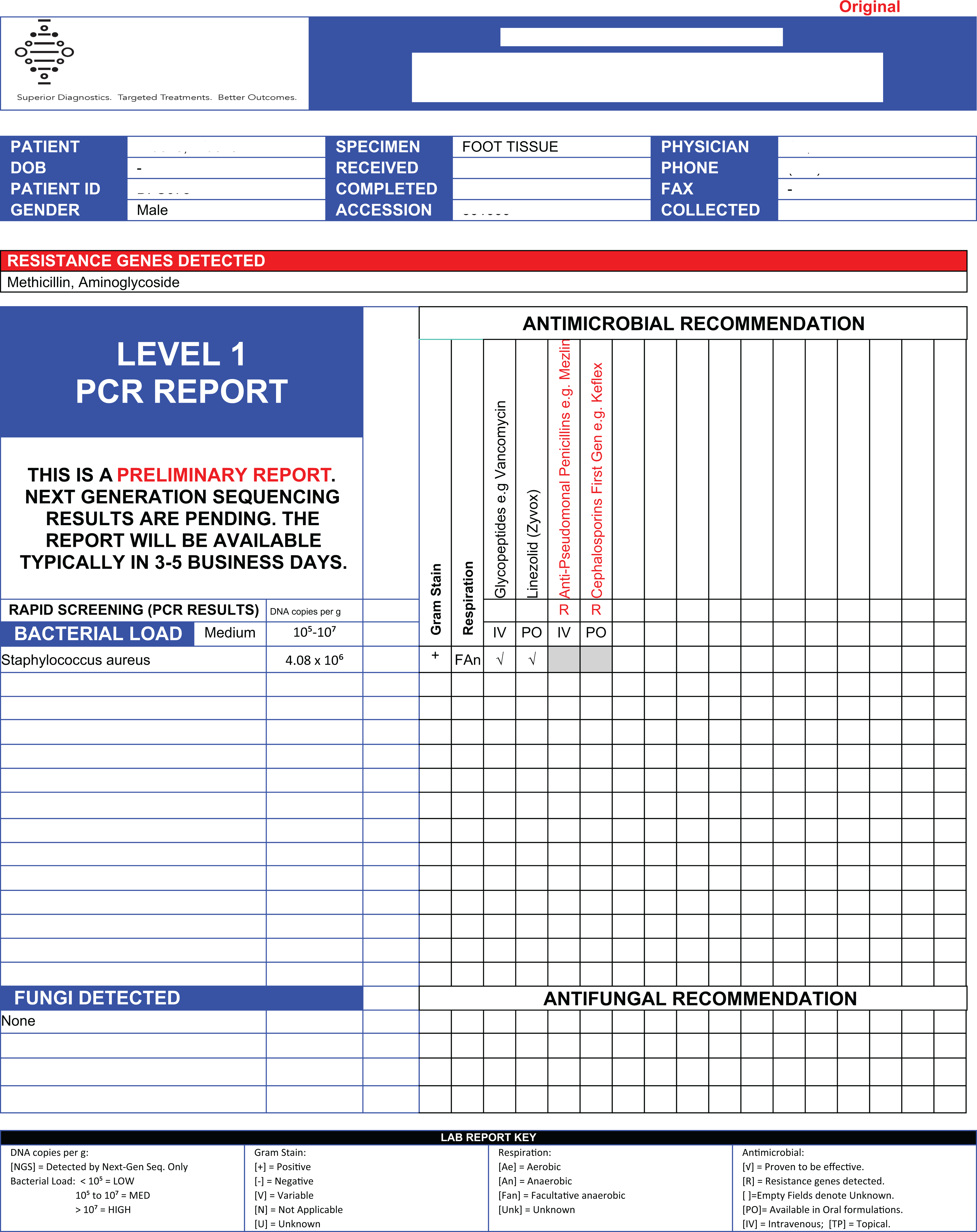
An example of a next-generation sequencing (NGS) preliminary report of an infected bone specimen. S. aureus was the dominant pathogen. Various antibiotic resistant genes (anti-pseudomonal penicillins, first generation cephalosporins) were reported along with suggestions for antibiotics (IV Vancomycin or oral Linezolid).
Antimicrobial Therapy
For most patients, administration of intravenous antibiotics was withheld until intraoperative specimens were obtained. Once obtained, an intravenous (IV) broad-spectrum antibiotic such as piperacillin/tazobactam (Zosyn) was administered until the standard culture result was available or antibiotic regimen was changed by a consulting infectious disease (ID) specialist. For patients with a history of methicillin-resistant Staphylococcus aureus (MRSA) infection, vancomycin was initiated instead. Pathologic evaluation of the resection margins was performed for all patients who underwent an amputation or bony resection (ie, calcanectomy) procedure. If clean margins were obtained, patients were placed on oral antibiotics for an additional 2 weeks after surgery. If the resection margins were contaminated, targeted long-term (6-week) IV or oral antibiotics were instituted as recommended by the consulting ID specialist. As NGS has not been licensed for clinical use in our state, we did not share the NGS information with ID specialists. They only considered standard culture results when tailoring antimicrobial therapy.
Assessment of Wound Healing Status
During the postoperative period, various biomechanical offloading strategies such as total contact cast, pneumatic boot, Plastazote insoles, or soft cushioned postoperative shoe were utilized to offload the operated foot as deemed appropriate by the treating surgeon. The end point of the study for each subject was at the 12-week postoperative intervention or at the time of reoperation as a sequelae of treatment failure, whichever occurred first. Patients were divided into 2 groups: healed (H) vs nonhealed (NH) based on (1) the size of the wound and (2) the absence or presence of 12 secondary signs and symptoms (pain, erythema, edema, heat, purulent exudate, serous exudate with concurrent inflammation, delayed healing, dislocation of granulation tissue, friable granulation tissue, pocketing at the base of the wound, foul odor, and wound breakdown) to clinically diagnose persistent infection. 3,4 NH wounds were defined as unimproved or increased size and depth of the wound with persisting 12 signs and symptoms of infection. 3,4
Statistical Data Analysis
Samples were grouped based on whether they generated positive culture results. All cases that identified at least 1 species were considered culture-positive. Because NGS is highly sensitive, detection of multiple species was common. Concordance was defined as NGS identifying the predominant organisms in culture. Concordance between standard culture and NGS was assessed. Complete concordance was defined as NGS detecting all organisms identified on the culture. Partial concordance was defined as partial overlap of organisms identified by NGS and culture. If NGS and standard culture identified completely different bacteria without any overlap, it was considered discordant. Concordance rates were estimated using Fisher exact binomial confidence intervals. Fisher exact test was used to compare culture type (mono-, polymicrobial) vs concordance (complete, partial, discordant). It was also used to analyze wound healing status (H, NH) vs duration (acute, subacute, chronic), culture type (mono-, polymicrobial), and concordance (complete, partial, discordant). Analysis was performed using SAS, version 9.4.
Results
Thirty patients who underwent operative intervention for infected DFUs were enrolled in this study. The average age was 60.4 years (range, 33-82) . The mean erythrocyte sedimentation rate, C-reactive protein level, and white blood cell count were 60 ± 38 mm/h (normal: 0-30), 107 ± 89 (normal: 1-10 mg/L), and 11 ± 3.5/µL (normal: 4.2-9.1), respectively. Demographic characteristics are summarized in Table 1. Operative procedures performed were irrigation and debridement (12), toe or ray amputations (13), calcanectomies (4), and a below-the-knee amputation (1). There were 9 acute (<3-week), 4 subacute (3- to 6-week), and 17 chronic (>6-week) DFUs. In 1 patient, intraoperatively obtained bone sample failed to identify any microorganism in both culture and NGS. The patient was treated with 2 weeks of oral Augmentin to cover any potential residual skin or soft tissue infection, and successfully healed the wound. The rest (n = 29) showed positive culture and NGS findings.
Patients Demographic Characteristics and Operative Procedure Performed (N = 30).

Correlation of NGS With Standard Culture
We analyzed the concordance between cultures and NGS in all infected DFU patients. We noted complete concordance (including the 1 true negative culture) in 14 cases (46.7%), partial concordance in 8 cases (26.7%), and discordance in 8 (26.7%) cases. S. aureus (17 of 29, 58.6%) and coagulase-negative Staphylococcus (7 of 29, 24.1%) were the most cultured bacterial species, followed by Corynebacterium striatum (5 of 29, 17.2%) and Enterococcus faecalis (5 of 29, 17.2%). For NGS, the most identified organisms were Finegoldia magna (13 of 29, 44.8%) followed by S. aureus (12 of 29, 41.4%), and Anaerococcus vaginalis (7 of 29, 24.1%) (Table 2). Overall, NGS detected a greater polymicrobial presence in each sample than standard culture. On average, NGS revealed 5.1 (1-11) pathogens whereas standard culture revealed 2.6 (1-6) pathogens in a given sample. The NGS report also included bacterial loads with quantified DNA copies per gram (low: <105, medium: 105 to 107, high: >107) and percentages of each organism present (Figure 1).
Microorganisms Identified in Infected Bone Samples With 2 Diagnostic Techniques.

Mono- vs Polymicrobial Infection
Among the 29 standard positive cultures, 10 (34.4%) were monomicrobial and 19 (65.6%) were polymicrobial. NGS identified polymicrobials in 25 (86.2%) cases. The majority of monomicrobial cultures identified S. aureus (8 of 10, 80%), followed by Streptococcus agalactiae (1 of 10, 10%) and F. magna (1 of 10, 10%). A high concordance rate (9 of 10, 90%) was noted between the standard culture and NGS in monomicrobial DFU infection group, and complete concordance was seen at a significantly higher rate in monomicrobial compared to polymicrobial infections (P = .0002). The majority of discordant cases were identified as polymicrobial infections by culture (8 of 9, 88.9%) and NGS (9 of 9, 100%).
Wound Healing Status
There were 16 (53.3%) patients who had completely healed ulcers or operative wounds by their 12-week follow-up, whereas 14 (46.7%) patients failed to heal. Three of 14 patients underwent subsequent surgeries (2 irrigation and debridement and 1 proximal amputation), whereas 11 patients continued local wound care. Multivariate analysis did not show notable differences between H vs NH groups in correlation with the duration of the DFU (acute, subacute, chronic), number of organisms identified by culture or NGS (mono-, polymicrobial), or the degree of concordance between the standard culture vs NGS (complete, partial, discordant).
Antibiotic-Resistant Gene
In 6 patients (20.7%), 7 different antibiotic resistant genes were identified by NGS. They included aminoglycosides (3), aminopenicillins (3), penicillins (1), antipseudomonal penicillins (3), cephalosporins (3), and extended-spectrum penicillins with beta-lactamase inhibitors (1). However, NGS did not identify MRSA, which was identified by standard culture in 1 patient. NGS reports presented the above information along with recommendations for antibiotic treatment.
Discussion
Overall, NGS identified larger numbers of microorganisms present in infected DFU samples. Whether this represented the true pathogen, bystander, or contaminant is not clear. NGS identified polymicrobials in 25 (86.2%) cases, whereas standard culture identified polymicrobials in 19 (65.6%) patients. NGS and culture showed a general (complete and partial) concordance rate of 70%. In 1 case, NGS identified a 99% presence of S. aureus (methicillin sensitive) whereas standard culture identified Staphylococcus epidermidis, which most likely was a contaminant. In such cases, clinicians can choose to target the main pathogen suggested by NGS rather than relying on standard culture alone. Furthermore, NGS can detect antibiotic-resistant genes and suggest potential antibiotic therapy as soon as 48 hours from the receipt of specimen, which allows for an earlier initiation of targeted antibiotic therapy. This emerging molecular diagnostic test has been suggested to have the ability to drastically improve the field of clinical microbiology by offering a single, all-inclusive diagnostic test. 5,6 As NGS is already available for clinical use in some states in the US and may be used in our microbiology lab in the future, we wanted to investigate its application in management of foot infections.
In this study, most infected patients had positive culture samples, with 1 or 2 predominant organisms identified. The most common organisms grown in culture included S. aureus, coagulase-negative Staphylococcus, C. striatum, and F. magna. When culture results were compared to their respective NGS results, NGS detected a greater variety of organisms at differing concentrations. This may suggest that the agar used for culture growth favored some organisms over others, while NGS was able to objectively sequence and quantify a whole genome from a given sample. Alternatively, it is likely the 16 S rRNA PCR step favored amplification of some organisms over others, ultimately causing significant differences in relative abundance of amplicons. We found NGS to be especially helpful in verifying and confirming the presence of predominant organisms determined through standard culture. For instance, in one DFU sample, standard culture grew Pseudomonas aeruginosa, Proteus, E. faecalis, and S. epidermidis, whereas NGS only identified a medium bacterial load of P. aeruginosa. In such cases, clinicians can conclude that the dominant pathogen is P. aeruginosa and tailor postoperative antibiotics as indicated.
Promising results have been suggested in using NGS for the diagnosis of PJI, especially when identifying pathogens in false negative cultures. 6,15,16 Moreover, in a prospective investigation of 86 synovial fluid samples obtained from patients undergoing hip or knee joint aspiration, a high degree (96.1%) of NGS concordance with standard culture was reported. 17 Whereas the above authors reported an excellent concordance rate between standard culture and NGS, Namdari et al 12 reported a fair concordance between culture and NGS in their comparative study of shoulder PJIs.
Combining complete and partial concordance results between NGS and culture gives our study a 70% concordance rate. We noted a high (90%) rate of concordance between culture and NGS in monomicrobial DFU infections, which were predominately S. aureus. Therefore, NGS may be useful in suggesting potential pathogens in polymicrobial culture with the presence or absence of antibiotic-resistant genes to suggest targeted antibiotic therapy. In 8 discordant DFU specimens, none of the polymicrobial microorganisms identified by culture and NGS matched. This finding may suggest that the standard culture contained contaminants or failed to grow the true pathogen. The discordance may also suggest possible contamination before or during NGS analysis. Thoendel et al 19 has suggested potential sources for contaminant DNA in molecular diagnostics, including mishandling of specimen during collection or in the laboratory by usage of contaminated lab equipment, disposables, and reagents. It can also indicate limitations associated with the current NGS technique. Because of its molecular-based identification method, it is unable to differentiate pathogens from dormant or dead microorganisms.
Johani et al 7 previously reported that NGS was able to detect pathogens in 6 of 20 (30%) of culture-negative infected bone sample obtained from diabetic foot osteomyelitis. The authors also conducted scanning electron microscopy (SEM) of the infected bone samples and identified biofilms in 15 of 18 (80%) bone specimens. They suggested that standard culture does not accurately detect multiple organisms protected in biofilm of DFUs, which can explain frequent failure of treatment. Given that all but 1 showed positive standard culture, the clinical utility of NGS for detection of pathogens in negative cultures was not observed in our study. Although a higher treatment failure was reported in polymicrobial DFUs, our study did not show a remarkable difference in healing status. 3,4 We believe this may be due to the complicated nature of DFU patients, whose operative treatments and unpredictable healing processes depend on various biological, mechanical, and behavioral factors.
There were a number of limitations in this study. First, this study was limited by the small sample size. Second, patients were referred to the surgeon’s office at various stages of infection. Some (26 of 30) participants were on oral antibiotics prior to recruitment and some required preoperative IV antibiotics because of systemic signs of infection. Preoperative antibiotics most likely confounded the culture or NGS results. This may explain the negative culture and NGS results in 1 patient. Because of the small sample size, we were not able to perform a comparative analysis of patients who were (26 of 30) vs those who were not (4 of 30) on antibiotics before recruitment to investigate the effects of preoperative antibiotics on the concordance of culture vs NGS. Third, subjects’ wound healing process may have been affected by other various medial comorbidities and biomechanical derangements. To mitigate this effect, we excluded patients with vascular insufficiency and evidence of immune deficiency or malnutrition. Whenever possible, we addressed biomechanical derangement of the foot through operative or conservative means. However, it is very challenging to control for various medical and biomechanical factors that could have affected the wound healing process. Fourth, limitations of NGS include high cost compared to standard culture, high sensitivity that may challenge interpretation of the result, and limited detection of organisms owing to selected primers dependent on applications of 16 S rRNA. Instead of the targeted 16 S amplicon method, the whole genome sequencing method of NGS has also been explored: metagenomic shotgun sequencing is another method that uses NGS techniques to detect organisms by using all the nucleic acids present rather than manipulating the highly conserved 16 S rRNA region. 6,18 Although it possesses similar limitations to NGS, including contaminants, costs, and difficulty in differentiating pathogens from commensals, metagenomic shotgun sequencing is able to detect elusive pathogens that standard culture cannot. Furthermore, there was 1 patient whose NGS result failed to detect what the culture identified as MRSA; it is unclear if the NGS was unable to detect the mecA gene in the samples or if the mismatch was caused by a sampling error. Given the small sample size and limitations, our study was unable to demonstrate that NGS changes our management or improves care for infected DFU patients. A larger-scale comparative study is warranted to investigate the accuracy and clinical benefit of NGS. Despite the above limitations, this study demonstrates that NGS provides a more complete representation of the microbiome of a DFU than a standard culture would. NGS may be a promising diagnostic tool in identifying pathogen and profiling microbiome in foot and ankle infections, such as infected DFU, ankle PJI, and fracture-related infections. Because the use of NGS in clinical laboratories has become increasingly widespread across the United States, its application in management of foot and ankle infections warrants further investigation.
Conclusion
NGS is an emerging molecular diagnostic tool in microbial identification in orthopedic infection. Our study demonstrated that NGS frequently provides different profiles of microorganisms along with antibiotic-resistant gene information compared with conventional culture in polymicrobial foot infection. Clinical utilization of NGS for management of foot and ankle infections warrants further investigation.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211026933 - Next-Generation Sequencing for Pathogen Identification in Infected Foot Ulcers
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211026933 for Next-Generation Sequencing for Pathogen Identification in Infected Foot Ulcers by Yoonjung Choi, Eimi Oda, Olivia Waldman, Thomas Sajda, Christopher Beck and Irvin Oh in Foot & Ankle Orthopaedics
Footnotes
Acknowledgment
We thank Dr Edward Schwarz and Dr Javad Parvizi for advising on the molecular diagnostic aspect of this study and Ms Samantha Hoffman for assistance with patient recruitment, data collection, and documentation.
Ethics Approval
The current study was approved by the University of Rochester Medical Center’s Research Subjects Review Board (RSRB#00057719). The principal investigator (PI) identified candidate patients. Enrollment, consenting, and sampling were performed by PI or clinical coordinators. All personnel involved in the sample collection were Institutional Review Board (IRB)-approved with current Collaborative Institutional Training Initiative (CITI) certification. Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute of Health (NIH)/National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) grant number R21AR07457 awarded to Irvin Oh, MD.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.