
Abstract
Background:
Osteochondral lesion of the talus (OLT) is commonly found as a concomitant pathologic lesion in a large proportion of patients with chronic lateral ankle instability (CLAI). This study investigated which characteristics in a patient with CLAI increase the risk for OLT.
Methods:
Three hundred sixty-four patients who underwent a modified Broström operation for their CLAI were reviewed retrospectively. The characteristics of each patient and variables associated with OLTs were investigated. Statistical analyses were performed to determine the effect of each potential predictor on the incidence of OLT, and to evaluate the associations between the patient characteristics and variables associated with OLTs.
Results:
Patients with OLTs were more frequently female (female vs male: 63.1% vs 43.9%, P = .003). In addition, the lesion sizes were larger in female patients (female vs male: 113.9 ± 24.9 mm2 vs 100.7 ± 18.0 mm2, P = .002), and medial lesions were more common in female patients (female vs male; 93.3% vs 81.8%, P = .036). The lesion sizes were larger in patients with a wider talar tilt angle (P < .001), and patients with a medial OLT showed a wider talar tilt angle (12.0 ± 2.0 degrees vs 10.3 ± 2.2 degrees, P = .002).
Conclusion:
In this CLAI patient cohort, we found female patients to be at greater risk for OLTs than male patients. Furthermore, CLAI female patients with concomitant OLT had on average a larger lesion size, more frequent OLT medial position, and were associated with wider talar tilt angles, suggesting that females had more intrinsic ankle instability than males.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Ankle sprains are one of the most common injuries that individuals experience during sports or daily activities, and the great part of cases involve the lateral ligamentous complex. 14,16,35,53 Most ankle sprains can be managed successfully with conservative treatment, including bracing and subsequent physical therapy focused on peroneus muscle-strengthening exercises and proprioceptive-based rehabilitation. 1,12 However, when these conservative managements fail, ankle sprains may lead to chronic lateral ankle instability (CLAI) requiring operative intervention. 10,21 Although several studies have reported encouraging outcomes of operative procedures for CLAI, 26,27,38 persistent pain is often experienced by patients even after successful reconstruction of the lateral ankle ligaments. 13,33,39,41,48 This persistent pain may be caused by a concomitant pathology of the ankle affected with CLAI. A review of the literature demonstrated that a large proportion of patients with CLAI have concomitant pathologic lesions such as osteochondral lesions of the talus (OLTs), synovitis, loose bodies, adhesions, or osteophytes. 5,11,25,28,48,50 Therefore, when conducting lateral ligament reconstruction, it is important to diagnose and treat the concomitant pathologic lesions as they may lead to persistent pain after surgery if not addressed.
OLT is commonly accompanied by CLAI, with some studies reporting that OLT is present in 16% to 54% of patients with the condition. 25,28,32,46,50 Controversy exists whether OLT accompanied by CLAI should be treated operatively at the same time, 55 although a few studies have reported favorable outcomes associated with simultaneous treatment of the 2 conditions. 22,36,49,55 However, these studies focused on outcomes of simultaneous treatment of OLT and CLAI; studies investigating predictors of concomitant OLT in patients with CLAI have rarely been published. An understanding of factors associated with concomitant OLT in patients with CLAI will help patients have more realistic expectations regarding the simultaneous treatment of OLT and CLAI. Furthermore, identifying and managing patients at risk for OLT may prevent persistent pain following lateral ligament reconstruction and can reduce the need for secondary procedures addressing the OLT. Accordingly, the purpose of this study was to describe the characteristics that would increase the risk for OLT in a patient with CLAI.
Methods
Patient Selection and Study Design
This study was reviewed and approved by the institutional review board of our hospital, and written informed consent was obtained from all participants. All methods were performed in accordance with the relevant guidelines and regulations. From August 2008 to April 2019, 416 patients with a diagnosis of CLAI underwent lateral ankle ligament reconstruction. All patients had a history of recurrent ankle sprain or subjective symptoms of ankle instability, including giving way, unstable ankle, or localized weakness. A diagnosis of CLAI was confirmed based on each patient’s history and symptoms, physical examination, stress radiography (side-to-side difference of ≥10 degrees in the talar tilt angle under inversion stress compared with the contralateral side or ≥4-mm anterior displacement of the talus during the anterior drawer test), 9 and/or magnetic resonance imaging (MRI) findings. Physical examinations, including anterior drawer test and talar tilt test, were conducted as described previously. 44 MRI findings were used to evaluate the lateral ligament complex and any associated injuries or pathologies of the affected ankle joint prior to surgery. Surgery was performed on patients who had repetitive ankle sprain injury or instability with pain despite a minimum of 3 months of nonoperative management. Nonoperative treatment options included ankle bracing and taping to decrease the occurrence of ankle sprains, and a structured physical therapy program focused on peroneus-strengthening exercises and proprioceptive-based rehabilitation of the ankle.
We retrospectively reviewed the 416 patients and applied strict criteria for entry into the study. Only patients who had undergone reconstruction of the lateral ligament using a modified Broström technique for CLAI were included in the study. Patients who had previous operative treatments, rheumatoid arthritis, arthritic changes, or structural deformity of the ankle joint were excluded. Of the 416 patients, 52 patients were excluded; 34 patients did not meet the inclusion criteria, and 18 patients refused to undergo MRI. Accordingly, the 364 patients were finally enrolled in this study, and divided into 2 groups: 141 patients with OLTs (OLT group) and 223 patients without OLTs (Non-OLT group) based on MRI evaluation (Figure 1).
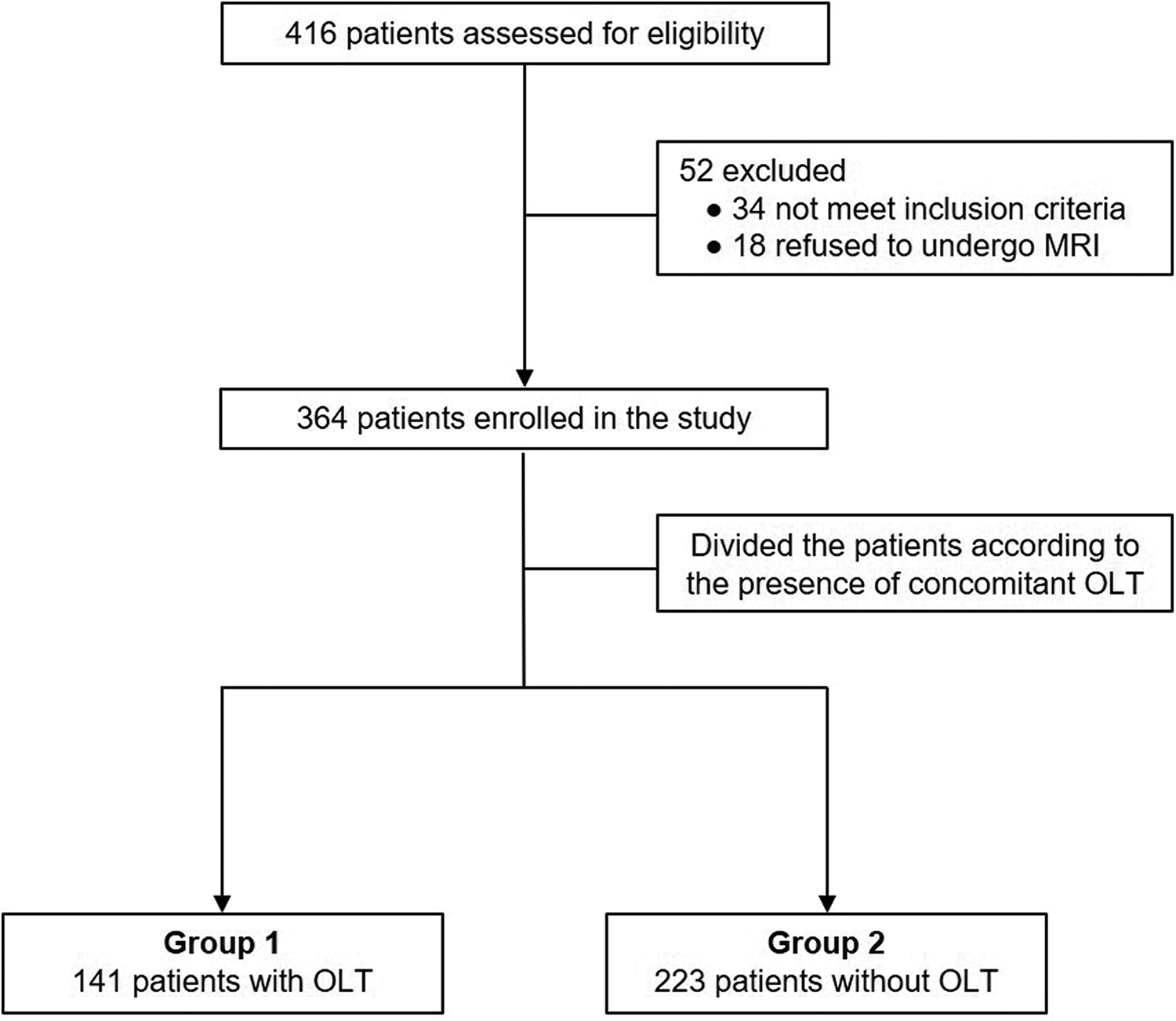
Flow diagram of patient involvement in the study. MRI, magnetic resonance imaging; OLT, osteochondral lesion of the talus.
Variables Analysis
Variables that can be potential predictors of OLT, including age, sex, body mass index, side of involvement, duration of symptoms, smoking, diabetes mellitus, hypertension, level of sports activity, and work level, were investigated (Table 1). The levels of sports activity and work were recorded as high or low, and heavy or light, respectively. A high level of sports activity was defined as exercising dynamic sports that involve running (eg, jogging, basketball, football, volleyball, tennis), and a low level of sports activity was defined as exercising sports that have a low risk of ankle sprain (eg, yoga, swimming, weight training) or rarely joining sports. A heavy work level was defined as manual labor requiring standing or walking, and a light work level was defined as sedentary work.
Patient Demographic Data.a

a Data are expressed as mean ± SD (range) unless otherwise indicated.
b Physical examinations were conducted as described by Sizer et al. 44
c Values are expressed as differences compared with the contralateral side.
To investigate the variables associated with OLTs in the OLT group, the size, location, and type of lesion were identified from preoperative MRI scans. All MRI findings were evaluated by an independent observer who was a musculoskeletal-trained radiologist not involved in the care of the patients and blinded to the study. To measure the lesions, we used a method previously described by Kim et al 31 : the lesion size was calculated using the ellipse formula after measuring the width and length of the OLT on preoperative MRI; the location of the lesion was categorized as medial or lateral; and the type of lesion was categorized as chondral (cartilage only) or osteochondral (cartilage and bone), as described previously. 7 The size, location, and type of lesion determined by preoperative MRI scans were reconfirmed through arthroscopic examination.
Operative Procedures
For the OLT group, standard arthroscopic procedures were performed. After routine arthroscopic examination, the lesion was evaluated along the surrounding cartilage and underlying bone, and all unstable and damaged cartilage in the lesion was accurately debrided, including the calcified layer down to the subchondral bone plate. 30 A microfracture awl (Linvatec, Largo, FL) was then used to make multiple holes in the defect, 3-4 mm apart, in areas where the subchondral bone was intact, as described by Steadman et al. 45 For areas with subchondral bone loss, abrasion arthroplasty was performed by removing loose chondral or osteochondral fragments with a ring-shaped or curved curette and by trimming damaged cartilage with a power shaver until a stable, smooth articular surface was created. 30 Associated lesions such as a subchondral cyst, anterior spur in the distal tibia, loose body, soft tissue impingement, or tibial chondral lesion were identified and treated at the same time.
After each arthroscopic procedure was completed, the patient was turned to the lateral position to perform lateral ligament reconstruction. A slightly curved longitudinal incision was made 2-3 cm above the distal tip of the fibula, centered over the lateral malleolus and curving toward the sinus tarsi. 34 The location of the inferior extensor retinaculum was identified and mobilized for attachment to the distal fibula. 34 An oblique capsular incision was then made along the anterior border of the fibula, from just distal to the anterior inferior tibiofibular ligament to the calcaneofibular ligament, leaving a small 3- to 4-mm cuff of tissue on the fibula for reattachment. 34 The incompetent anterior talofibular ligament was identified by a thickening of the capsule, whereas the calcaneofibular ligament was found in the distal portion of the wound under the tip of the fibula, running deep to the peroneal tendon. 29 After raising a periosteal flap from the tip of the lateral malleolus, the anterior talofibular ligament and/or calcaneofibular ligament were sutured to the anteroinferior aspect of the fibula using the modified Broström technique, as described by Kim et al. 29 Then, double augmentation with the inferior extensor retinaculum and a periosteal flap was carried out.
After surgery, we recommended immobilization with a short leg walking cast and partial weight bearing for 4 weeks. Patients began active and passive ankle range-of-motion exercises 4 weeks after surgery, and sports or other high-impact activities were limited for at least 3 months.
Statistical Analysis
All continuous variables are reported as mean ± standard deviation, and the categorical variables are reported as n (%). A univariate analysis using the Student t test and chi-square test was conducted in order to compare the continuous and categorical variables, respectively, between patients with and without OLTs. We then used univariate logistic regression analysis to determine the effect of each potential predictor on the odds of patients having OLTs. Stepwise multivariate stepwise logistic regression was then performed to evaluate the potential associations between the patient characteristics and OLT variables in patients with OLTs. For the logistic regression models, we report odds ratios, correlation coefficients (CCs), and 95% confidence intervals (CIs) relative to a chosen reference group. The Pearson correlation test was used to analyze the correlation of patient sex with OLT variables and the results of stress radiography in group 1. Statistical analyses were performed using SPSS, version 13.0 (IBM Corp, Armonk, NY), and a P value <.05 was considered to indicate statistical significance.
Results
Patient Characteristics
The study population included 187 women and 177 men, with a mean age of 35.7 years (range, 22-54 years) at the time of operation. The average preoperative body mass index was 26.6 (range, 19.6-32.1), and the mean duration of symptoms was 24.9 weeks (range, 12-38 weeks) (Table 1). Other demographic data (smoking, diabetes mellitus, hypertension, level of sports activity, and work level), results of physical examination and stress radiography, and concomitant pathologies of the affected ankle are also summarized in Table 1. Preoperatively, 97 patients (26.6%) stated that they enjoyed a high level of sports activity and 97 (26.6%) claimed to have a heavy work level. On preoperative physical examination, 296 (81.3%) patients showed positive findings on talar tilt test, and 318 (87.4%) patients showed positive findings on anterior drawer test. The combined pathologies of the affected ankle were identified on preoperative MRI. Among all patients, synovitis (54.1%, n = 197) was the most frequently identified concomitant pathology, followed by OLT (38.7%, n = 141), syndesmosis widening or scar formation (22.2%, n = 81), bony spur or osteophyte formation (19.8%, n = 72), peroneal tendon tear or tendinopathy (15.1%, n = 55), soft tissue impingement on gutter (12.9%, n = 47), and loose body (4.1%, n = 16), in that order.
The results of univariate analysis comparing patients with and without OLTs at the time of lateral ligament reconstruction are presented in Table 2. Patient sex and duration of symptoms were significant predictors of OLTs. Patients with OLTs were more frequently female (63.1% vs 43.9%, P = .003), and the mean duration of symptoms was significantly longer in the OLT group than in the Non-OLT group (27.0 weeks vs 26.4 weeks, P = .002). However, no significant differences were found for age, body mass index, side of involvement, smoking, diabetes mellitus, hypertension, level of sports activity, and work level (P > .05. for all) between the groups.
Comparison of Patient Characteristics Between the Groups.a

Abbreviation: OLT, osteochondral lesion of the talus.
a Data are expressed as mean ± standard deviation or n (%).
b Values are expressed as differences compared with the contralateral side.
Associations Between Patient Characteristics and OLT Variables
In the OLT group, the mean OLT size was 107.7 ± 24.9 mm2 (range, 65.1-176.3 mm2). When comparing the location of the lesion, medial lesions (87.9%, n = 124) were more common than lateral lesions (12.1%, n = 17). For type of lesion, chondral types (65.2%, n = 92) were more common than osteochondral types (34.8%, n = 49). The associations between patient characteristics and OLT variables in the OLT group are shown in Table 3. The bivariate correlation showed a statistically significant association between the lesion size and sex (CC = 0.265, P = .002), between the lesion size and symptom duration (CC = 0.179, P = .033), between the lesion size and level of sports activity (CC = 0.276, P = .001), and between the lesion size and work level (CC = 0.208, P = .013). The mean lesion size was significantly larger in female patients (113.9 ± 28.4 mm2) than in male patients (100.7 ± 18.0 mm2) (P = .002). The mean lesion size was also significantly larger in patients who enjoyed a high level of sports activity (P = .001) and engaged in heavy work level (P = .013). There was also a significant association between the lesion location and sex (CC = –0.176, P = .036); medial lesions were more common in female patients (93.3%, n = 70) than in male patients (81.8%, n = 54). However, there were no significant associations of the type of lesion with all patient characteristics.
Associations Between Patient Characteristics and Lesion Size of OLTs in the OLT Group.a

Abbreviations: CC, correlation coefficient; OLT, osteochondral lesion of the talus.
a Data are calculated using the stepwise multivariate logistic regression analysis.
Associations Between Stress Radiography Results and OLT Variables
On stress radiography, the mean difference of talar tilt angle compared with the contralateral side was significantly wider in the OLT group (mean, 11.8 ± 2.2 degrees) than in the Non-OLT group (mean, 11.2 ± 2.0 degrees) (P = .008). However, there was no significant difference in the mean difference of anterior displacement of the talus compared with the contralateral side (mean, 4.2 ± 1.6 mm in the OLT group, and 4.1 ± 1.1 mm in the Non-OLT group, respectively) (P = .381) (Table 2). Correlations between results of stress radiography and OLT variables in the OLT group are shown in Figure 2 and Table 4. In multivariate analysis, as illustrated in the scatter plots, significant correlation between lesion size and difference of talar tilt angle compared with the contralateral side was found (P < .001) (Figure 2A). The lesion sizes were larger in patients with a wider talar tilt angle. However, there was no significant correlation between lesion size and difference of anterior displacement of the talus compared with the contralateral side (P = .808) (Figure 2B). Patients with a medial OLT showed a wider talar tilt angle (12.0 ± 2.0 degrees vs 10.3 ± 2.2 degrees, P = .002) (Table 4). They also showed substantially longer anterior displacement of the talus (4.2 ± 1.2 mm vs 3.8 ± 1.2 mm), but this difference did not reach statistical significance (P = .143). The results of stress radiography (mean differences of talar tilt angle and anterior displacement of the talus compared with the contralateral side) were not different according to the type of OLT (P > .05, both).

(A) Correlation between the size of the osteochondral lesion of the talus (OLT) and difference of talar tilt angle compared with the contralateral side. (B) Correlation between size of OLT and difference of anterior displacement of the talus compared with the contralateral side.
Results of Stress Radiography According to the Location and Type of Lesions in the OLT Group.a

Abbreviation: OLT, osteochondral lesion of the talus.
a Data are expressed as mean ± standard deviation.
b Values are expressed as differences compared with the contralateral side.
Discussion
Several theories concerning the underlying cause of OLTs, including traumatic events, vascular, endocrine, or metabolic irregularities, degenerative joint disease, and genetic causes, have been suggested. 2,8,37,42,51 OLT is a common injury found in patients with chronic disabling pain after an ankle sprain, 25,32,49 and traumatic insult is widely accepted as the cause of OLTs. 2,15,37,51 Ankle sprains can cause a small fracture and subsequent impaired vascularity, leading to the formation of an osteochondral defect. 8 In addition, microtrauma caused by repetitive articular cartilage surface loading or excessive stress can lead to cellular degeneration or death by the disruption of collagen fibril ultrastructure and thickening of subchondral bone. 18 To date, although many studies have reported concomitant OLTs in patients with CLAI, 5,9,22,25,28,32,36,46,48,50 little is understood about which characteristics in a patient with CLAI increase the risk for OLTs. To our knowledge, this is the first study to investigate patient characteristics as predictors of concomitant OLTs in patients with CLAI by using different statistical analyses.
Various concomitant pathologic lesions have been reported in patients with CLAI. For example, Komenda and Ferkel 32 performed arthroscopy on 54 patients (55 ankles) with CLAI, and found concomitant pathologies such as synovitis (69.1%), loose bodies (21.8%), and OLTs (16.2%). In a study of 64 patients who underwent a modified Broström operation for CLAI, Choi et al 9 reported that concomitant pathologies included soft tissue impingement (81.5%), ossicles at the lateral malleolus (38.5%), syndesmosis widening (29.2%), OLTs (23.1%), and osteophyte formation (10.8%). Takao et al 50 reported, in their study of 72 patients with CLAI, that 29 patients (40.3%) had OLTs, 13 patients (18%) had symptomatic os subfibulare, 3 patients (4.2%) had anterior impingement exostosis, and 3 patients (4.2%) had impingement due to abnormally fibrous bands. Hintermann et al 25 performed arthroscopic examination of 148 patients with symptomatic CLAI and found synovitis (32%), deltoid injuries (40%), syndesmosis injuries (9%), and cartilage lesions on the talus (53%) as concomitant pathologies. Approximately similar results were found in the present study. As concomitant intra-articular pathologies, synovitis (54.1%), OLT (38.7%), syndesmosis widening or scar formation (22.2%), bony spur or osteophyte formation (19.8%), soft tissue impingement on gutter (12.9%), and loose body (4.1%) were found. In addition, in a recent study by Burrus et al 4 of 136 patients with CLAI, 67 patients (51.5%) had peroneal tendon tear or tendinopathy as concomitant extra-articular pathologies, whereas a relatively smaller number of patients (15.1%, n = 55) had peroneal tendon tear or tendinopathy in this study.
The most important finding of the present study is that patient sex and duration of symptoms are significant predictors of OLTs in patients with CLAI. That is to say, in a patient with CLAI, the risk for OLTs would be increased for women who have a longer duration of symptoms. Although the exact reason for this finding is unclear, we speculate that a natural tendency toward increased ligamentous laxity in women compared with men may be the potential cause for this finding. Female sex is widely accepted as a predictor of primary anterior cruciate ligament injury, which has a multifactorial pathogenesis. 24,40,47 Likewise, hormone-related alterations in laxity and deficits in proprioception and muscle training cannot supplement the lateral ligament complex, thus it can be stated that subsequent repetitive ankle sprains occur more frequently in female patients. As well, Frey et al 19 compared the incidence of lateral ankle instability in 957 high school volleyball players and found a significantly increased incidence of inversion ankle sprains in female athletes, providing further evidence for increased ankle ligamentous laxity in females. Therefore, possible increased ligamentous laxity in female patients and the resultant increased ankle instability, coupled with a period of prolonged instability (ie, longer duration of symptoms), may contribute to accelerate the development of OLTs.
Chronic ankle instability is generally caused by inadequate and inappropriate healing after ligamentous injury and develops when the injured ligaments do not regain the mechanical integrity necessary to shield the ankle from physiologic stress. 54 The structural insufficiency of an injured ligament may induce mechanical ankle instability that implies loss of normal anatomic constraint to lateral ankle stability. Mechanical instability is usually detected on stress radiography, including the talar tilt test and anterior drawer test. The talar tilt angle is considered to be a parameter of dysfunction of the calcaneofibular ligament, and the anterior drawer displacement of the talus is thought to be related to injury of the anterior talofibular ligament. Biomechanically, the anterior talofibular ligament functions as a collateral ligament in a planter-flexed ankle joint, whereas the calcaneofibular ligament functions as a collateral ligament in a neutral or dorsiflexed ankle joint. 3 The anterior talofibular ligament is frequently injured because the majority of ankle sprains occur during inversion of the plantar-flexed ankle joint, 22,52 and further, it is the weakest ligament of the lateral ligamentous complex, followed by the calcaneofibular ligament. 43 The calcaneofibular ligament works synchronically with the anterior talofibular ligament and, therefore, is rarely injured in isolation. 20 In this study, only the talar tilt angle—not the anterior displacement of the talus—was found to be predictive of a higher incidence of OLTs in patients with CLAI (Table 2). Concerning this result, we believe that OLTs may develop in patients with severe ankle instability that involves not only the anterior talofibular ligament but also calcaneofibular ligament insufficiency. Sugimoto et al 46 also reported that a larger talar tilt angle was a risk factor for the development of OLTs in patients with CLAI. Therefore, we consider the severity of ankle instability described as the degree of talar tilt angle to be factors accelerating the development of OLTs.
In this study, we investigated the associations between patient characteristics and OLT variables and found that the lesion size was significantly larger in female patients, patients who enjoyed high level of sports activity, and patients who engaged in a heavy work level (Table 3). We assumed that episodes of repetitive ankle injury might occur more frequently in female patients because of their increased ligamentous laxity and that the subsequently developed OLTs would be aggravated, resulting in larger lesion sizes. Our assumption is supported by the findings of a previous study by Sugimoto et al, 46 wherein arthroscopic examination revealed that a much greater proportion of female CLAI patients experienced advanced chondral damage. In addition, participation in a high level of sports activity and a heavy work level in patients with CLAI would understandably contribute to the larger lesion size of OLTs.
In this study, significant association between the lesion location and sex was found (Table 3). Medial lesions were more common in female patients than in male patients. Taga et al 48 evaluated the prevalence of chondral lesions in ankles with recurrent lateral instability, and found that chondral lesions typically were located in the medial half of the joint. Recent studies have also reported a high prevalence of focal chondral lesions in the medial region of patients with chronically unstable ankles. 25,36 We considered female patients with CLAI to be at greater risk for repetitive and severe inversion ankle injuries than male patients; thus, OLTs would be more likely to develop in the medial side of the ankle joint following traumatic injury.
This study investigated the associations between the results of stress radiography and OLT variables. As a result, in patients with wider talar tilt angle, the lesions were located mainly in the medial side of the ankle joint and were larger in size (Table 4 and Figure 2). Moreover, female patients with concomitant OLT and CLAI had wider talar tilt angles than male patients (Table 5). Accordingly, there were positive correlations of female sex with lesion size, lesion location, and talar tilt angle (Table 6) in patients with concomitant OLT and CLAI. From this point of view, we considered that female sex is a principal predictor of OLT in patients with CLAI.
Comparison of Patient Characteristics According to the Sex in Both Groups.a

Abbreviation: OLT, osteochondral lesion of the talus.
a Data are expressed as mean ± SD or n (%).
b Values are expressed as differences compared with the contralateral side.
Correlations of Patient Sex With OLT Variables and Results of Stress Radiography in the OLT Group.a

Abbreviations: CC, correlation coefficient; OLT, osteochondral lesion of the talus.
a Data are calculated using the Pearson correlation test.
b Values are expressed as differences compared with the contralateral side.
The present study has some limitations. First, the data were collected retrospectively, and only patients who underwent reconstruction of the lateral ligament for CLAI were included in the study. A comparative study evaluating the predictors of OLT in patients with CLAI who received operative or conservative treatment is required for more accurate identification of the predictors of OLT in patients with CLAI. Second, the number of enrollees was relatively small for a cohort study evaluating predictors of OLT in patients with CLAI. However, given that no similar studies of this size have been published, we believe that these data are valuable to know the predictors of OLT for patients with CLAI requiring reconstruction of the lateral ligament. Furthermore, this study is ongoing and can be strengthened over time as the number of patients in the matched group increases. Lastly, the present study focused on patients with mechanical instability who underwent reconstruction of the lateral ligament. However, chronic instability can be caused by mechanical ankle instability as well as functional ankle instability. 6 Functional ankle instability is defined subjectively as a “giving-way sensation” 17 that is not associated with any physical laxity of the ankle joints, 23 and it is caused by specific insufficiencies in proprioception, neuromuscular control, postural control, or muscle strength. To ensure more precise evaluations of predictors for OLT in patients with CLAI, further studies involving patients with mechanical ankle instability as well as functional ankle instability will be necessary.
Conclusion
As the incidence of ankle instability continues to rise, it is important for surgeons to recognize concomitant OLTs that can influence treatment outcomes. In our study, we found that female patients with CLAI tended to be at greater risk for having an associated OLT than male patients. Furthermore, female patients with concomitant OLTs and CLAI had larger lesion sizes, medially located OLTs, and wider talar tilt angle, which suggest severe ankle instability.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211013344 - Demographic Predictors of Concomitant Osteochondral Lesion of the Talus in Patients With Chronic Lateral Ankle Instability
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211013344 for Demographic Predictors of Concomitant Osteochondral Lesion of the Talus in Patients With Chronic Lateral Ankle Instability by Yong Sang Kim, Tae Yong Kim and Yong Gon Koh in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Institutional review board and ethics approval was obtained by the regional health authority.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.