
Abstract
Background:
This investigation’s purpose was to perform a systematic review of the literature examining the biomechanics of the ligaments comprising the distal tibiofibular syndesmosis with specific attention to their resistance to translational and rotational forces. Although current syndesmosis repair techniques can achieve an anatomic reduction, they may not reapproximate native ankle biomechanics, resulting in loss of reduction, joint overconstraint, or lack of external rotation resistance. Armed with a contemporary understanding of individual ligament biomechanics, future operative strategies can target key stabilizing structure(s), translating to a repair better equipped to resist anatomic displacing forces.
Study design:
Systematic review.
Methods:
A systematic review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines using a PRISMA checklist. Biomechanical studies testing cadaveric lower limb specimens in the intact and injured state measuring the distal tibiofibular syndesmosis resistance to translational and rotational forces were included in this review. Only studies that included numerical data were included in this review; studies that only reported figures and graphs were excluded.
Results:
Twelve studies met the inclusion and exclusion criteria. Two studies determined the mechanical properties of syndesmotic ligaments, finding superior strength and stiffness of the interosseous ligament (IOL), as compared to the anterior (AITFL) or posteroinferior tibiofibular ligament (PITFL). Four studies examined native ankle biomechanics establishing physiologic range of motion of the fibula relative to the tibia. Fibular range of motion was found to be up to 2.53 mm of posterior translation (Markolf et al), 1.00 mm lateral translation (Xenos et al), 3.6 degrees of external rotation (Burssens et al), and 1.4 degrees of internal rotation (Clanton et al). Four studies evaluated syndesmotic biomechanics under physiological loading and found that the AITFL, IOL, and PITFL provide the majority of resistance to external rotation, diastasis, and internal rotation, respectively. Two studies investigated the biomechanics of clinically and intraoperatively used tests for syndesmotic injuries and found increased sensitivity of sagittal plane posterior fibular translation, as opposed to coronal plane lateral fibular translation for unstable injuries.
Conclusions:
Study findings suggest that although the IOL is the strongest syndesmotic ligament, the AITFL has a dominant role stabilizing the distal tibiofibular syndesmosis to external rotation force. Because of these characteristics, operative repair of the AITFL along its native vector may provide a more biomechanically advantageous construct and should be investigated clinically. Additionally, evaluation of clinical stress tests revealed that the external rotation stress test is the most sensitive test to recognize an AITFL tear, and that a 3-ligament disruption is needed to cause diastasis greater than 2 mm.
Keywords
Introduction
Injuries to the distal tibiofibular syndesmosis can occur in isolation with deltoid ligament injuries or with ankle fractures, particularly posterior malleolar and/or proximal fibula fractures. These injuries are commonly caused by high-energy mechanisms, usually in external rotation or hyperdorsiflexion. 22 These injuries have been seen, as well, in high-level athletes with long associated recovery times. 22 The structures that make up the syndesmosis work in concert to maintain stability of the talus within the ankle mortise. Thus, the anatomy and biomechanics of the individual ligaments as well as the syndesmosis as a whole must be considered to optimize fixation methods and patient outcomes.
The tibiofibular syndesmosis is composed of 3 main stabilizing structures: the anteroinferior tibiofibular ligament (AITFL), posteroinferior tibiofibular ligament (PITFL), and the interosseous ligament (IOL). The AITFL originates on the anterior tibial tubercle, approximately 5 mm above the tibiotalar articular surface. 12 Williams et al 26 describe the tibial footprint 9.3 mm superior and medial to the anterolateral corner of the tibial plafond. Its fibers extend obliquely in a laterodistal direction, at a 30-degree angle to the horizontal. 26 The fibers insert on the anterior margin of the lateral malleolus, 30.5 mm superior to the inferior tip of the lateral malleolus. 26 Bartonícek et al 1 found that the AITFL has 3 distinct anatomic components: superior, middle, and inferior. The PITFL is the largest supporting ligament of the tibiofibular syndesmosis and is divided into superficial and deep components; these components are sometimes described as the upper and lower components of the ligament. 13 The superficial component originates on the posterior edge of the lateral malleolus, and runs proximally and medially to insert in the posterior tibial tubercle. The deep component is also known as the transverse ligament of the syndesmosis. It is cone shaped, originating in the proximal area of the posterior malleolar fossa and inserting in the posterior edge of the tibia. 12 The IOL of the tibiofibular syndesmosis is a dense mass of short fibers spanning from the distal tibia to the distal fibula, 4 to 5 cm above the tibiotalar joint. 12 The presence of the IOL is variable; in some individuals, the ligament is prominent whereas in others it is not present at all and blends into the interosseous membrane. 13 Cadaveric images depicting the AITFL, PITFL, and IOL can be found in Figure 1.
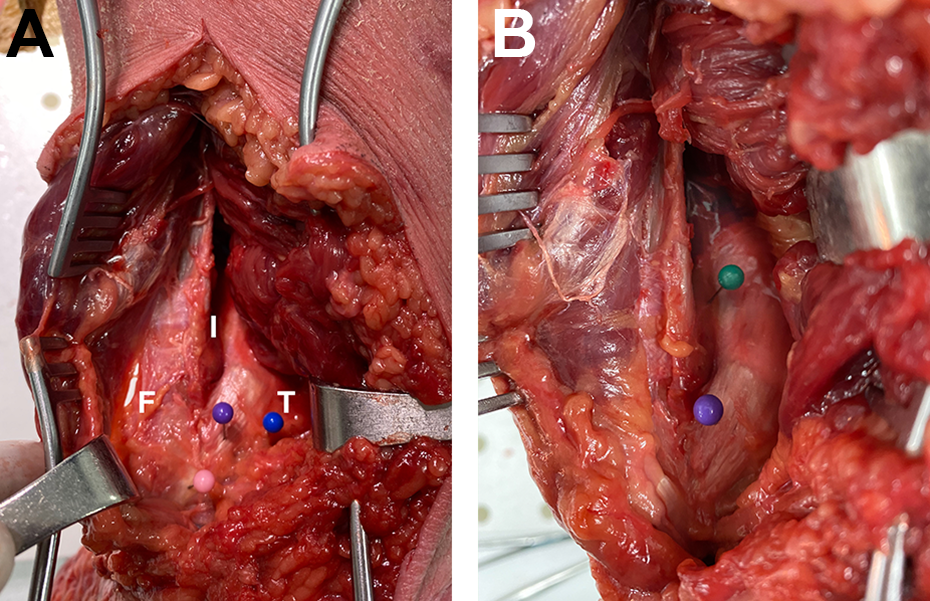
(A) Anterior view of a dissected cadaveric left ankle depicting the anteroinferior tibiofibular ligament (purple) with its most distal tibial (blue) and fibular (pink). F, fibula; T, tibia; I, interosseous ligament. (B) Posterolateral view of a dissected cadaveric left ankle in the substance of the posteroinferior tibiofibular ligament (purple) and interosseous membrane (green).
Operative repair of an unstable syndesmosis strikes a careful balance between maximizing joint stability and minimizing risks of complications, such as loss of reduction, tibiotalar joint overconstraint, or hardware failure. Traditional screw fixation of the syndesmosis has good clinical outcomes and is useful for short-term constraint of the joint to allow for healing. However, screw fixation is associated with several drawbacks such as overconstraint of the joint in the long term and frequent hardware failure requiring reoperation for removal. 11 Suture button fixation is becoming a more popular method of stabilization of the syndesmosis as an alternative to traditional 3.5-mm tricortical or quadricortical screw fixation. Benefits of suture button fixation include long-term dynamic stabilization. However, traditional suture button fixation is associated with instability to external rotational stress and reduction loss. 11
It is vital to consider the biomechanics of individual syndesmotic ligaments when considering targets for repair. 14 The primary purpose of this article is to provide a systematic review of the literature examining the biomechanics of the distal tibiofibular syndesmosis, with a focus on resistance to translation and rotation by individual ligaments as well as the joint complex as a whole. This study seeks to provide the most comprehensive biomechanical understanding of the structure of the syndesmosis and identify an avenue for repair that may provide a more biomechanically advantageous construct.
Methods
Literature Review
The following databases were searched for existing systematic review of distal tibiofibular syndesmosis biomechanics: The Database of Abstracts of Reviews of Effects, the Cochrane Database of Systematic Reviews, and the International Prospective Register of Systematic Reviews (PROSPERO). No studies reviewing the biomechanics of the distal tibiofibular syndesmosis have been published in the last 10 years.
Search Strategy
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines using a PRISMA checklist, shown in Figure 2. The following databases were searched from inception to October 2020 for relevant studies: Cochrane CENTRAL, PubMed (MEDLINE), Ovid (MEDLINE), and Scopus. The authors independently conducted the search on October 9, 2020. The search strategies combined text words and relevant indexing using appropriate Boolean operators to capture the articles discussing the biomechanics of the distal tibiofibular syndesmosis. The literature search used the following terms (including synonyms and other closely related words): distal and tibio* and syndesmo*. The searches were not limited by study design or date of publication, but only to references published in the English language. The full PubMed search strategy is shown in Appendix A.

Preferred Reporting Systems for Systematic Reviews and Meta Analyses (PRISMA) Diagram.
The inclusion criteria consisted of articles with cadaveric lower limb models tested biomechanically in the intact and sequentially injured state. Exclusion criteria included the following: meta-analyses, systematic reviews, review articles, case reports, and studies with human subjects. Studies that examined ligaments outside of the distal tibiofibular syndesmosis and studies that examined syndesmosis repair methods were also excluded to maintain the focus on ligamentous biomechanics of the syndesmosis itself.
Data Abstraction and Analysis
After search of the databases, a total of 873 articles were identified. The search process is shown in Figure 1. After title and abstract assessment, 18 full-text articles were selected for further review. A total of 6 articles were excluded after further review. Five articles were excluded due to reporting charts and figures without including numerical data. 7,16,17,21,24 One article by Beumer et al 2 was excluded for not defining loads applied to the studied specimens. Notably, another study by Beumer et al 3 did not define applied loads, but it was included because syndesmotic stress tests done in a clinical setting would not measure loads. To ensure that all available studies were identified, the reference lists of included articles were assessed for additional relevant studies.
Outcome Measures
The main outcome of interest in our review was individual ligament contribution to syndesmotic biomechanical stability, which was measured through changes in fibular translation in the coronal and sagittal planes as well as fibular rotation in response to external rotational forces. Secondary outcome measures recorded include the biomechanical properties of syndesmotic ligaments as well as indirect measurements of ligament biomechanics such as forces and torques required to induce motion in the syndesmosis. These outcome measures provide a comprehensive overview of the biomechanical properties of the uninjured ankle, and can serve as a target for biomechanical properties of repaired injured ankles.
Results
Twelve studies met the given inclusion criteria. The Quality Assessment for Cadaveric Studies (QUACS) tool was used for assessment of included studies, with a mean QUACS score of 82.3% and a standard deviation of 13.2%. Complete results of QUACS scoring can be found in Table 4, and criteria for QUACS scoring can be found in Appendix A. Two of the 12 included studies examined individual syndesmotic ligament stiffness and strength, and reported superior strength and stiffness of the IOL compared with the AITFL and PITFL. 4,14 Six of the 12 included studies examined the biomechanics of the syndesmosis under compression and external rotational loading, and recorded fibular translation in the coronal and sagittal planes, and rotation of the fibula and foot. 6,8,15,19,25,27 Details of loading parameters for each study are included in Table 1. The largest measurements of fibular range of motion recorded in these studies were 2.53 mm of posterior translation (Markolf et al 19 ), 1.00 mm lateral translation (Xenos et al 27 ), 3.6 degrees of external rotation (Burssens et al 6 ), and 1.4 degrees of internal rotation (Clanton et al 8 ). Clanton et al 8 demonstrated that fibular external rotation increases significantly with sectioning of the AITFL and that fibular internal rotation increases significantly with sectioning of the PITFL. Multiple studies demonstrated increases in fibular translation and rotation with sectioning of the AITFL. 6,25,27 The results of these biomechanical investigations are shown below in Table 1 and depicted in Figures 3 and 4.
Results of Biomechanical Testing.

Abbreviations: AITFL, anteroinferior tibiofibular ligament; IOL, interosseous ligament; PITFL, posteroinferior tibiofibular ligament.
* The standard deviation was not reported.

Bar chart depicting (A) mean ligament strength (N) and (B) mean ligament stiffness (N/m). AITFL, anteroinferior tibiofibular ligament; IOL, interosseous ligament; PITFL, posteroinferior tibiofibular ligament.

External rotation of the fibula under loading after sequential sectioning of syndesmotic ligaments. AITFL, anteroinferior tibiofibular ligament; DL, anterior deltoid ligament; dPITFL, deep posteroinferior tibiofibular ligament; sPITFL, superficial posteroinferior tibiofibular ligament.
Three included studies evaluated individual syndesmotic ligament contributions to stabilizing translational and rotational loads by recording the force required to create diastasis and percentage reduction in forces and torques on sectioning of syndesmotic ligaments. 9,15,23 The results of these investigations are shown below in Table 2. Clanton et al 8 reported that sectioning of the AITFL resulted in the largest percentage decrease in torque required to cause external rotation displacement, whereas sectioning of the PITFL resulted in the largest percentage decrease in internal rotational torque to cause a similar internal rotation displacement. Ogilvie-Harris et al 23 demonstrated similar findings, where sectioning of the AITFL and deep portion of the PITFL were each associated with the largest percent decreases in force required to create 2 mm of diastasis, with a relatively smaller contribution by the IOL.
Individual Ligament Contributions to Resistance in Translation and Rotation.

Abbreviations: AITFL, anteroinferior tibiofibular ligament; CI, confidence interval; ER, external rotation; IOL, interosseous ligament; IR, internal rotation; NA, not available; PITFL, posteroinferior tibiofibular ligament.
Two included studies examined the biomechanics of commonly used stress tests for clinical and intraoperative assessment of syndesmotic injuries. 3,18 Both studies reported diastasis measured at the anterior syndesmosis during testing of the intact syndesmosis and after sequential sectioning of syndesmotic ligaments. The results of these studies are shown below in Table 3. Notably, Beumer et al demonstrated that there is a large change in external rotation displacement after sectioning of the AITFL with minimal changes in external rotation appreciated after subsequent successive ligament sectioning.
Biomechanical Evaluation of Clinical and Intraoperative Stress Tests.

Abbreviations: ADL, anterior deltoid ligament; AITFL, anteroinferior tibiofibular ligament; CI, confidence interval; IOL, interosseous ligament; PITFL, posteroinferior tibiofibular ligament.
Complete Results of QUACS Scoring by Criteria.

Abbreviation: QUACS, Quality Assessment for Cadaveric Studies.
Discussion
The syndesmosis is essential in providing stability of the ankle joint. Each individual component of the syndesmosis is unique and contributes to the overall function of the ligamentous complex. In the search for an anatomic syndesmosis repair technique that allows for long-term dynamic stabilization of the joint, it is essential to consider individual ligament biomechanical contributions to the overall stability of the ankle mortise. The purpose of this systematic review was to determine the biomechanical profile of the individual components comprising the distal tibiofibular syndesmosis.
Four of the 12 studies evaluated the normal range of excursion of the syndesmosis and the variation therein with loading and ankle position. 6,8,15,19 Although the IOL was the strongest and stiffest of the ligaments, the AITFL was found to be the largest contributor to resistance of external rotation forces, and the PITFL was the largest contributor to resistance to the internal rotation force. Not only do these findings provide a baseline for clinical and radiographic assessment for injury to the syndesmosis, but they provide a framework for which repairs and reconstructions can be designed to restore proper anatomic biomechanics to the syndesmosis following injury.
Findings by Hoefnagels 14 and Beumer et al 4 demonstrate the superior mechanical stiffness and strength of the IOL as compared to the AITFL and PITFL. 14 However, specimens in both studies were loaded in pure tension along the longitudinal axis of each ligament, unlike physiological loading patterns which are more likely to be eccentric. 4,14 Results of sequential sectioning studies performed by Clanton et al, 8 Ogilvie-Harris et al, 23 and D’Hooghe et al 9 demonstrate significant variability in results based on the order in which ligaments were sectioned. 15 The considerable variability in individual ligament contributions to resistance identify a need for further standardized evaluation. Some variability can be explained by sequential cutting in the anteroposterior direction performed by D’Hooghe et al, 9 whereas Ogilvie-Harris et al 23 sectioned ligaments in random sequence avoiding bias incurred by synergistic resistance by combinations of ligaments. These findings suggests that sectioning of successive ligaments may confound the true contribution by individual ligaments and that randomizing specimens to sectioning of individual ligaments may be required to determine each ligaments’ contribution to stabilizing the syndesmosis. Regardless of sectioning order, Clanton et al 8 demonstrated that the AITFL plays a dominant role in stabilizing external rotational forces, with the PITFL complex predominantly stabilizing internal rotation. Ogilvie-Harris et al 23 similarly demonstrated that both the AITFL and PITFL play significant roles in stabilizing against diastasis of the syndesmosis. The results obtained from sequential sectioning studies suggest that the AITFL and PITFL play more significant stabilizing roles than results of studies by Hoefnagels et al 14 and Beumer et al 4 indicate, and that eccentric loads mimicking physiological loading patterns are better suited for assessment of syndesmotic stability and should be standard in future biomechanical studies.
Beyond the scope of biomechanical testing, the findings of Massri-Pugin et al 20 suggest that further research is required into diagnostic testing for injuries to the syndesmosis. Currently used radiologic markers for syndesmotic injury include medial clear space widening and tibiofibular clear space widening, both assessing translation in the coronal plane. 27 Arthroscopic findings by Massri-Pugin et al 20 demonstrate that coronal plane translation varies from the anterior to posterior syndesmosis. This variation is difficult to assess with standard anteroposterior, lateral, and mortise views of the ankle; thus, radiologic measurement of coronal translation may be inadequate to accurately diagnose syndesmotic injury. In contrast, 4 included studies demonstrated significant increases in posterior translation of the fibula in response to external rotational forces with syndesmotic injury. 6,8,15,19 An excluded study by Patel et al 24 also validates posterior translation as a marker for syndesmosis injury in response to inversional loading. These findings suggest that posterior translation of the fibula during a stress examination must be considered alongside coronal plane diastasis and fibular rotation when evaluating for syndesmotic injury.
Syndesmosis repair using suture button constructs in the plane of the IOL has steadily gained popularity in recent years. Yet, this fixation method is associated with instability to external rotation as compared to screw fixation and native ankle physiology. 10,18 Screw fixation has been used for syndesmotic instability for decades, but it is associated with several drawbacks, including overconstraint of the joint and incidence of hardware failure requiring reoperation. Newer fixation methods using suture button constructs in anatomic configurations may be better suited to restoring native biomechanics with long-term dynamic stabilization of the syndesmosis. Findings from this systematic review summarize the cumulative biomechanical data available that defines the syndesmosis to our knowledge. Based on data presented above, the optimal restraint to syndesmosis displacement may be best accomplished with fixation along the planes of the AITFL and IOL when stability to external rotation is required, and repair in the planes of the superficial PITFL and IOL when stability in internal rotation is required. As there are only very small displacements in all planes that occur in a normal tibiofibular joint during weightbearing, stabilizing the planes of the AITFL, IOL, and PITFL may provide the best biomechanical construct. 5 However, further biomechanical testing comparing anatomic vs partial or nonanatomic fixation strategies would be required to substantiate this.
Limitations
This review included all human cadaver studies examining biomechanics of the distal tibiofibular syndesmosis, resulting in a small number of total studies included. Additionally, some articles may not have been identified with the given search strategy or exclusion criteria. The included cadaveric biomechanical studies exhibited considerable variation in experimental design and biomechanical testing methodology in addition to variations in baseline demographics of the specimens themselves. However, most studies applied similar loading parameters (axial, rotational, and combined loading) and reported similar outcome measures as seen in Tables 1 to 3 above. Although the magnitude of measured syndesmotic translation and rotation varied between studies, a consistent trend was seen in that each syndesmotic ligament is the primary constraint for different loading patterns as described above. Finally, the included studies exhibited variation in methods used to determine displacement after ligament transection. This variation identifies a potential topic for further study, as accurate diagnosis of syndesmotic injury patterns is yet to be optimized and these difficult injuries are frequently missed or misdiagnosed.
Conclusion
Treatment of distal tibiofibular syndesmosis injuries has developed in the last decade, sparking a controversy in determining optimal treatment modalities. Current fixation techniques focus on repair in the plane of the IOL. However, biomechanical evidence presented in this review suggest that the AITFL and, to a lesser extent, the PITFL play stabilizing roles alongside the IOL and present targets for anatomic repairs. Findings from this systematic review can be used to guide the development of novel approaches to syndesmosis repair with the aim to provide the most biomechanically advantageous repair.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211012701 - Biomechanics of the Distal Tibiofibular Syndesmosis: A Systematic Review of Cadaveric Studies
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211012701 for Biomechanics of the Distal Tibiofibular Syndesmosis: A Systematic Review of Cadaveric Studies by Pranav Khambete, Ethan Harlow, Jason Ina and Shana Miskovsky in Foot & Ankle Orthopaedics
Footnotes
Acknowledgments
The authors express sincere gratitude to Amber Catherine Stout, medical librarian at University Hospitals Cleveland Medical Center, for her assistance in conducting the systematic review.
Ethics Approval
Ethical approval was not sought for the present study because living human subjects were not involved and no protected health information was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix A
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.