
Abstract
Background:
Fractures of the talus are a rare but challenging injury. This study sought to quantify the area of osseous exposure afforded by a posteromedial approach to the talus and medial malleolar osteotomy.
Methods:
Five fresh-frozen cadaveric lower extremities were dissected using a posteromedial approach and medial malleolar osteotomy respectively. Following exposure, the talar surfaces directedly visualized were marked and captured using a calibrated digital image. The digital images were then analyzed using ImageJ software (National Institutes of Health) to calculate the surface area of the exposure.
Results:
The average square area of talus exposed using the posteromedial approach was 9.70 cm2 (SD = 2.20, range 7.20-12.46). The average quantity of talar exposure expressed as a percentage was 9% (SD = 1.58, range 7.03-10.40). The average square area of talus exposed using a medial malleolar osteotomy was 14.32 cm2 (SD = 2.00, range 11.26-16.66). The average quantity of talar exposure expressed as a percentage was 12.94% (SD = 1.79, range 9.97-14.73). The posteromedial approach provided superior visualization of the posterior talus, whereas the medial malleolar osteotomy offered greater access to the medial body.
Conclusion:
The posteromedial approach and medial malleolar osteotomy allow for significant exposure of the talus, yielding 9.70 and 14.32 cm2, respectively. Given the differing portions of the talus exposed, surgeons may prefer to use the posteromedial approach for operative fixation of posterior process fractures and elect to use a medial malleolar osteotomy in cases requiring more extensive medial and distal exposure for neck or neck/body fractures.
Level of Evidence:
Level IV.
Introduction
Talus fractures, which account for less than 2.5% of all fractures, present a unique challenge to the treating orthopedic surgeon. 3,5,9,13,17 In addition to the rarity of these injuries, gaining access to the talus is often difficult as the talus maintains articulations with the distal tibia, distal fibula, medial malleolus, navicular, and calcaneus. The talus also resides in proximity to peroneal tendons laterally and retromalleolar contents medially, further limiting operative exposure. Furthermore, soft tissue dissection to the talus can be challenging, as preservation of the talar blood supply is paramount in healing.
Fractures of the talus contain a variety of morphologies, including the head, neck, body, dome, lateral process, posterior process, and medial/lateral tubercles. 3 The careful selection of an appropriate operative approach yielding clear access to the desired area is critical in preoperative planning process for these injuries. Classically described operative approaches to the talus include the anteromedial, anterolateral, medial malleolar osteotomy, and posteromedial approach. 4,5,7,11,14,15,16,18 Specifically, the posterior medial approach is useful for operative fixation of posterior process fractures. The use of the medial malleolar osteotomy is beneficial in more extensive medial and distal exposure for neck or neck/body fractures. The purpose of this study was to quantify the area of osseous exposure afforded by a posteromedial approach to the talus and medial malleolar osteotomy. We believe this can be potentially useful for preoperative planning. To the authors’ knowledge, a quantitative comparison of the talar access afforded by these 2 distinct approaches has yet to be described in the literature.
Materials and Methods
Ten fresh-frozen cadaveric lower extremities, from midshaft femur to toe, were obtained, and all specimens were free of trauma or other deformity. The 10 cadaveric legs were not matched pairs. All procedures were performed by chief residents under the supervision of a fellowship-trained orthopedic trauma surgeon. Five posteromedial approaches and 5 medial malleolar osteotomies were performed, as detailed below.
Posteromedial Approach
The posteromedial approach was performed as described by Shi et al. 9 With the cadaveric limb positioned in the prone position, a skin incision was planned midway between the medial boarder of the Achilles tendon and the posterior aspect of the medial malleolus. The skin incision originated distally at the level of the calcaneal tuberosity and extended proximally for 10 cm. The skin was incised and careful dissection was preformed down the fascia overlying the FHL and tibial neurovascular bundle. Next, the fascia distally was released and the FHL and neurovascular bundle were mobilized and carefully retracted anteriorly exposing the distal tibia and posterior capsule. A capsulotomy was preformed and the tibiotalar and subtalar joints were identified.
Medial Malleolar Osteotomy
The medial malleolar osteotomy was performed as described by Ziran et al. 17 With the cadaveric limb externally rotated in the supine position, a skin incision was planned, using the standard medial approach, and carried distal and posterior around the medial malleolus with extension caudally in line with the navicular. The skin was incised, and careful dissection was performed. The anterior tibialis tendon was identified, demarking the anterior margin of the capsular incision, as was the deltoid ligament and retromalleolar contents. Without complete release of the flexor retinaculum or tendon sheath, the posterior tibial tendon was identified and protected as an osteotome was used to create an oblique osteotomy. The osteotomy was directly visualized through the anterior arthrotomy and completed at the level of the medial shoulder of the joint. The medial malleolus was then hinged inferiorly on the deltoid ligament, providing access to the talus.
Following each dissection, the area of the talus visible while dorsiflexing the foot allowing for maximal visualization from the perspective of the operating surgeon was demarcated along its borders using a 2.0-mm drill bit orthogonal to the talar surface visualized (Figure 1C). Each talus was then removed, denuded of soft tissue, and the marked area was carefully painted. A calibrated digital image of the talus and a ruler was taken in 6 planes (anterior, superior, posterior, medial, lateral, and inferior). These digital images were analyzed using ImageJ (National Institutes of Health, Bethesda, MD). 10 Once calibrated to a known distance, the computer program calculated the surface area based on the number of pixels in a selected field. The surface area of the exposed area, as well as the total surface area of the talus, were then calculated. Then, the average area of each exposure was calculated and the area was compared using a Student t test.
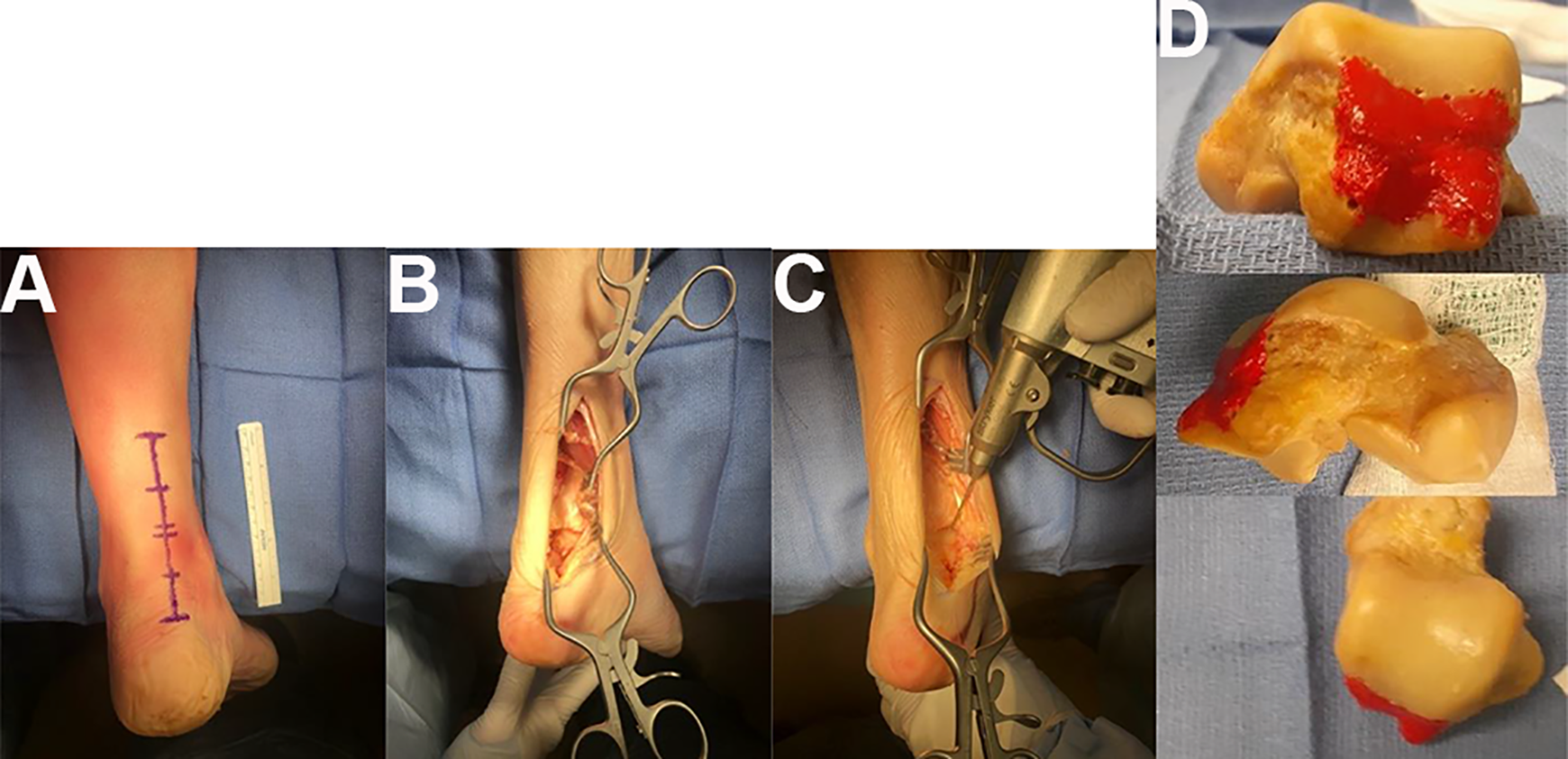
(A) Planned skin incision for posteromedial approach. (B) Exposure of the posterior tibiotalar joint following capsulotomy. (C) Marking the exposed area of the talus with a 2.0-mm drill bit. (D) Painted area of the talus highlighting the visualization obtained from the approach in vivo.
Results
The average age of the cadaveric specimens was 70.4 years (range 62-77). Five right and 5 left limbs were used in the study. All limbs were from Caucasian cadavers and the average BMI was 23.22 (range 17.93-28.19). The cadavers were not matched paired feet. There were 6 surface area planes of talus evaluated (anterior, posterior, medial, lateral, superior, and inferior). We calculated the area of talus exposed on each plane by dividing the total surface area of the specific plane by the area quantitatively visualized by the demarcation by ImageJ software. The average square area of talus exposed using the posteromedial approach was 9.70 cm2 (SD = 2.20, range 7.20-12.46). The average quantity of talar exposure expressed as a percentage was 9% (SD = 1.58, range 7.03-10.40) (Table 1). The average square area of talus exposed using a medial malleolar osteotomy was 14.32 cm2 (SD = 2.00, range 11.26-16.66). The average quantity of talar exposure expressed as a percentage was 13% (SD = 1.79, range 9.97-14.73). The area exposed by medial malleolar osteotomy was statistically significantly larger (P = .008) than that of the posteromedial approach (Table 2).
Individual and Total Surface Area Calculations for Posteromedial Approach.

Abbreviations: MM, medial malleolus osteotomy; PM, posteromedial approach; SA, surface area.
Individual and Total Surface Area Calculations for Medial Malleolar Osteotomy.

Abbreviation: SA, surface area.
Discussion
Fractures of the talus are an uncommon and challenging injury 3,5,9,17 ; proper treatment includes accurate reduction and stable fixation to minimize both the significant complications and functional deficits associated with these injuries. 3,5,13,17 There are multiple operative approaches in the armamentarium of the orthopedic surgeon that are useful in caring for these injuries, each with limitations in the exposure provided.
Swords et al 11 described 10 cases of patients with posteromedial talus fractures who underwent operative fixation using the posteromedial approach. All patients had acceptable outcomes and no arthrodesis procedures were necessary. 1 Giuffrida et al 4 identified 6 posteromedial talar facet fractures and described poor outcomes if not appropriately treated. Complication rates for posterior medial talus fractures are unacceptably high if not properly addressed, and this can result in subtalar instability, functional impairment, and development of arthritis. 1,6,8 This further supports that posteromedial talus fractures necessitate the appropriate approach for fixation.
Osteochondral lesions of the medial talar dome, intra-articular fractures of the talar body, and fractures of the talar neck may potentially require a medial malleolar osteotomy for surgical exposure. 2 Thordarson and Kaku 12 described the results of 14 patients who underwent step-cut medial malleolar osteotomies for intra-articular pathology or osteochondritis dissecans lesions. Each patient had excellent exposure of the medial and distal talus and healed the osteotomy site uneventfully.
The purpose of this study was to quantify the area of osseous exposure afforded by a posteromedial approach to the talus and medial malleolar osteotomy. Knowing the average surface area exposure and location of this visualization on the talus is beneficial to the treating surgeon in selecting the proper approach for a specific pathology. In our study, the posteromedial approach provided superior visualization of the posterior talus (Figure 1), whereas the medial malleolar osteotomy offered greater access to the talar neck and medial body (Figure 2). In considering the example of a pure posterior process fracture, the posteromedial approach offers robust exposure of the desire area at 5.01 cm2 (SD = 1.06, range 3.95-6.72), whereas the medial malleolar osteotomy was the less effective approach because it offered less visualization at 2.07 cm2 (SD = 1.26, range 0.69-3.91). Limitations to our study include a relatively small and a homogenous group of cadaveric specimens. Also, the potential inaccuracies that may arise when using 2-dimensional digital images to describe 3-dimensional anatomy was a limitation. Another limitation to this study is that in a clinical setting, the use of a distractor is often used, as this aids in further visualization of the talus.

(A) Planned skin incision for medial malleolar osteotomy. (B) Exposure of talus following reflection of medial malleolus. (C) Painted area of talus highlighting the visualization obtained from the approach in vivo.
In conclusion, the posteromedial approach and medial malleolar osteotomy allow for significant exposure of the talus. Given the differing portions of the talus exposed, surgeons may prefer to use the posteromedial approach for operative fixation of posterior body, posterior process, and medial and/or lateral tubercle fractures. The use of a medial malleolar osteotomy is traditionally used to extend the area visible in the medial approach for neck or neck/body fractures. Our study may potentially add in operative decision making, offering a quantitative assessment of the amount of visible talus, and the appropriate approach can be determined based off preoperative planning and review of pertinent patient injury imaging.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211012691 - Quantification and Comparison of Talar Exposure Utilizing a Posteromedial Approach and Medial Malleolar Osteotomy
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211012691 for Quantification and Comparison of Talar Exposure Utilizing a Posteromedial Approach and Medial Malleolar Osteotomy by Jeffrey Donahue, Ademola Shofoluwe, Kurt Krautmann, Emilio Grau-Cruz, Stephen Becher and Jennifer Bruggers in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethics approval for this study was not sought for because the paper does not meet the definition of human subjects research according to our Graduate Medical Education research committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Internal funding from Department of Orthopedic Surgery at WellStar Atlanta Medical Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.