
Abstract
Background:
The purpose of this article is to document the normal arthroscopic appearance of the posterior ankle capsular and ligamentous structures, and variations in their anatomical relationships.
Methods:
102 ankle arthroscopy videotapes were evaluated retrospectively for the configuration of the posterior capsuloligamentous structures. Based on these observations, the variations in the appearance and position of the posterior tibiofibular ligament (PTFL) and transverse (tibiofibular) ligament (TTFL) were documented. In addition, differences in the appearance of the flexor hallucis longus (FHL) were also noted.
Results:
All patients had evidence of both a PTFL and TTFL, which formed a labrum or meniscus-like addition to the posterior distal tibia. No patients demonstrated disruption of the PTFL; 3 had tears of the TTFL. We noted 4 distinct patterns of the PTFL and the TTFL. Thirty-four patients (33%) had a gap of ≥2 mm between the 2 ligamentous structures. Thirty-three (32.4%) had a gap <2 mm between the PTFL and TTFL. Twenty-six (25.5%) had a confluence of the 2 ligaments without a gap. Nine (9%) demonstrated a sizable gap between the 2 ligaments, and the TTFL appeared as a “cord-like” structure.
Conclusion:
To our knowledge, this is the first article to describe the variations in the arthroscopic normal posterior capsuloligamentous structures and FHL of the ankle.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
The advent of ankle arthroscopy has given us a better understanding of the intra-articular structures of the ankle and common anatomic variations. However, most reports still fail to detail the posterior capsuloligamentous anatomy. Throughout our ankle arthroscopic experience, we have noted distinct variations in these capsuloligamentous structures, which we believe are important normal variations. Although the posterior arthroscopic anatomy has been described, few studies have reported on the variability of the appearance and relationships of these ligaments to each other. Two of the most prominent structures seen in the posterior aspect of the ankle on arthroscopy include the posterior tibiofibular ligament (PTFL) and transverse tibiofibular ligament (TTFL). Together, these 2 structures have been demonstrated to provide up to 42% of syndesmotic stability in cadaveric models. 19
The purpose of this study is to document the normal arthroscopic appearance of the posterior capsular structures, the PTFL and TTFL as well as variations in their anatomical relationships including the “tibial slip” and the flexor hallucis longus (FHL). Our hypothesis was that there is variability in the normal posterior capsular, ligamentous, and tendinous structures. Understanding the normal anatomy arthroscopically assists the surgeon to identify the posterior pathologic anatomy and correlate it to the patient’s symptomatology.
Nomenclature
There is confusion about the appropriate terminology for some of the posterior ligaments of the ankle. These should be named according to the International Anatomical Terminology (IAT). In 1998, the Federative Committee on Anatomic Terminology indicated that the term inferior should be dropped for both the anterior tibiofibular and posterior tibiofibular ligaments. 4,5 In addition, the previously named inferior transverse ligament should be omitted and the ligament should be called the transverse ligament or deep component of the posterior tibiofibular ligament.
Chen noted the ligament structure between the posterior talofibular and transverse ligaments and termed it the “tibial slip.” 2 Other authors prefer the term “intermalleolar ligament” instead of the tibial slip, and this will be discussed in further detail later in this article. 10
Methods
Operative Procedure
Ankle arthroscopy was performed on all patients in the supine position with the hip flexed 45 degrees, using a thigh support and noninvasive distraction, as previously described in detail. 7 Both 2.7-mm 30- and 70-degree and 1.9-mm 30-degree short video arthroscopes were used as needed. In all patients, the anteromedial, anterolateral, and posterolateral portals were used. 11 A 21-point diagnostic arthroscopic examination and therapeutic arthroscopy were performed according to the diagnosis. 7 All cases were digitally stored for archiving and research purposes.
Arthroscopic Findings
Over a 3-year span, 222 consecutive ankle arthroscopies were performed and video recorded at our institution. These videos were reviewed independently by 3 separate examiners, paying particular attention to the posterior capsuloligamentous structures, including the PTFL, TTFL, tibial slip, and FHL tendon. Videos that did not give adequate visualization to assess these structures, along with all ankles with significant degenerative changes requiring ankle arthrodesis, were excluded from the study (Figure 1). The remaining 102 ankle arthroscopies were evaluated for the configuration of the posterior capsuloligamentous structures and measurements were taken to document the gap between the PTFL and the TTFL. Overall, there were only 7 patients where one examiner’s observations differed from the other 2 examiners. All of these patients’ videos were then reviewed again by all 3 examiners and agreement was reached on the capsuloligamentous configuration. In each case, there was a slight difference in the measurement between the 2 ligaments that caused the discrepancy.

Overview of the review process and exclusion criteria.
The posterior capsuloligamentous structures were viewed from both the anteromedial and anterolateral arthroscopic portals with a 30-degree 2.7-mm arthroscope. The PTFL and TTFL were evaluated on the basis of their size, configuration, number of discrete bands, and their relationship to each other. The flexor hallucis tendon and recess were evaluated according to how well the tendon could be visualized. The tendon was assigned into one of 4 categories based on the overlying anatomy about the FHL tendon. The categories consisting of (1) the FHL tendon could not be discerned from the other capsular structures, (2) a faint discernable recess for the tendon could be visualized, (3) the FHL tendon was located in a discrete recess, and (4) the tendon itself could be visualized through a very thin layer of synovium. Finally, the presence or lack of a “tibial slip” (intermalleolar ligament) and “vertical band” in the posterior cul-de-sac was also noted at the time of review.
Results
There were 48 men and 54 women with a variety of indications for ankle arthroscopy. Of the 102 arthroscopies, 122 major diagnoses were assigned (Table 1). Thirty-six (29.5%) had osteochondral lesions of the talus requiring debridement and drilling and 24 (19.7%) had loose bodies requiring removal. Other diagnoses included anterolateral soft tissue impingement in 16 (13.1%), synovitis in 12 (9.8%), instability in 9 (7.4%), distal tibial osteophyte in 9 (7.4%), peroneal tendon subluxation in 5 (4.1%), acute fracture in 4 (3.3%), chondromalacia in 3 (2.5%), painful os trigonum in 2 (1.6%), and posterior tibial tendinitis in 2 (1.6%). We found no correlation between the type of ankle pathology seen and the posterior capsuloligamentous structure variations.
Associated Major Diagnoses With 102 Ankle Arthroscopies.a
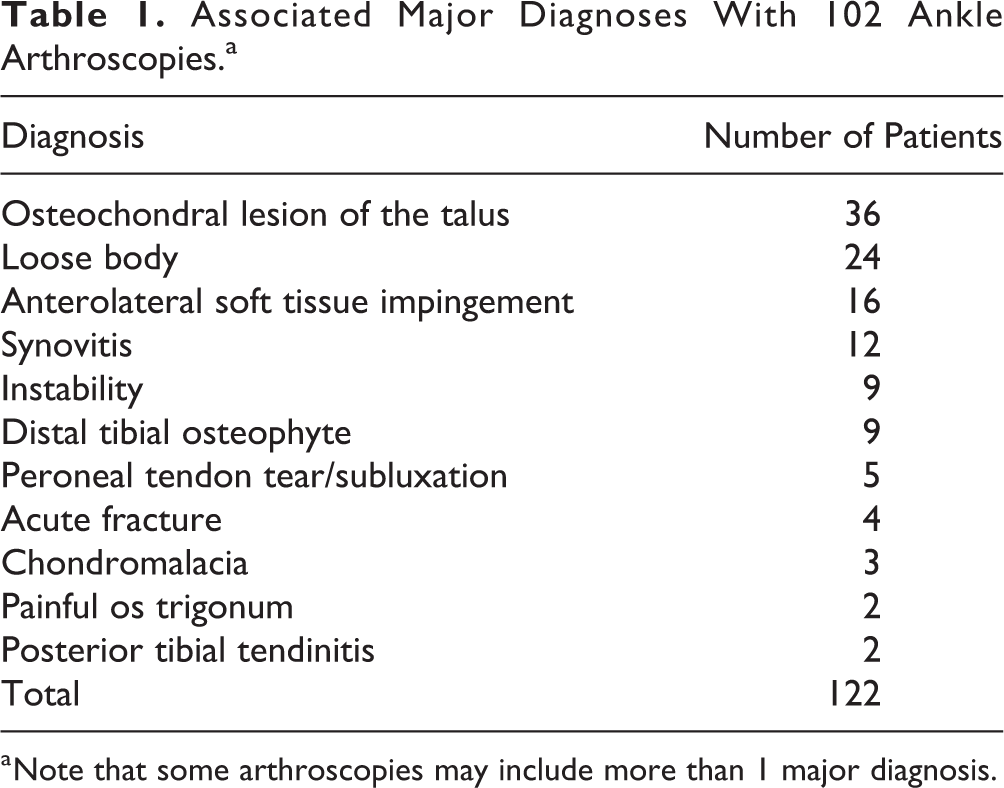
a Note that some arthroscopies may include more than 1 major diagnosis.
All patients in the study had evidence of both a PTFL and a TTFL, which formed a labrum or meniscus-like addition to the posterior distal tibia (Figure 2A and B). No patients demonstrated disruption of the PTFL, whereas 3 patients had longitudinal tears of the TTFL. The relationship between these 2 ligaments was variable but could be divided into 4 major types. In the type I configuration, there was a confluence of the 2 ligaments without a discernable gap. The ligaments were a single entity attaching to both the posterolateral corner of the distal tibia and forming a labrum-like structure along the posterior articular margin (Figure 3). A type II configuration consisted of 2 separate ligaments, with only a small gap (<2 mm) between the 2 limbs (Figure 4). The type III ligamentous configuration was formed by 2 discrete ligaments with separate origins and insertions with greater than or equal to a 2-mm space between them (Figure 5A and B). The type IV configuration also consisted of 2 discrete ligaments, where the TTFL appeared as a “cord-like” structure (Figure 6A and B).

The posterior ankle ligaments in a right ankle. (A) Drawing showing the location of the posterior talofibular ligament (PTFL), transverse tibiofibular ligament (TTFL), and tibial slip (posterior intermalleolar ligament) in a right ankle. (Reprinted with permission from Ferkel RD. Foot and Ankle Arthroscopy, 2nd edition. Philadelphia: Wolters Kluwer, 2017.) (B) Anatomical dissection. 1, Fibula; 2, tip of the fibula; 3, peroneal groove of the fibula; 4, tibia; 5, posterior tubercle of the tibia; 6, superficial component of the posterior tibiofibular ligament; 7, deep component of the posterior tibiofibular ligament or transverse ligament; 8, interosseous membrane; 9, posterior talofibular ligament; 10, lateral talar process; 11, tunnel for flexor hallucis longus tendon; 12, flexor hallucis longus retinaculum; 13, calcaneofibular ligament; 14, subtalar joint; 15, flexor digitorum longus tendon (cut); 16, tibialis posterior tendon (cut); 17, posterior intermalleolar ligament; A, tibial insertion (tibial slip in arthroscopic view); B, talar insertion lateral talar process; c, tibial malleolar insertion through the septum between the flexor digitorum longus and posterior tibial tendons; D, talar insertion (medial talar process) through the joint capsule. (Reprinted with permission from Ferkel RD: Foot and Ankle Arthroscopy, 2nd edition. Philadelphia: Wolters Kluwer, 2017.)

Type I configuration (artist depiction) with confluence of PTFL (red) and TTFL (green) without a discernible gap in a right ankle. PTFL, posterior talofibular ligament; TTFL, transverse tibiofibular ligament.
Type II configuration (artist’s depiction) with the PTFL (red) and TTFL (green) separated by <2 mm gap between them in a right ankle. PTFL, posterior talofibular ligament; TTFL, transverse tibiofibular ligament.

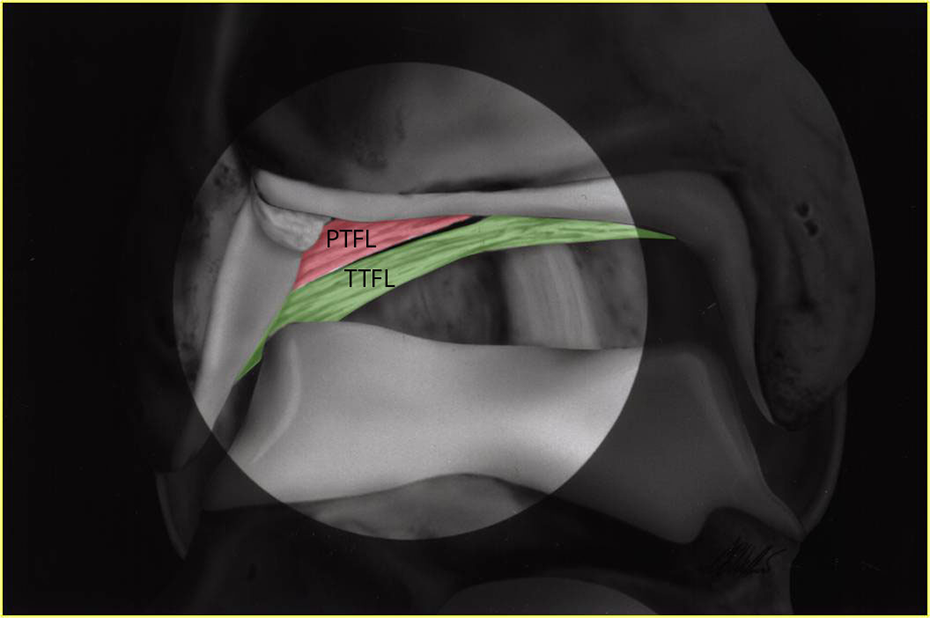
Type III configuration with the PTFL and TTFL separated by a ≥2-mm gap between them in a right ankle. (A) Artist’s depiction with PTFL in red and TTFL in green. (B) Arthroscopic view. PTFL, posterior talofibular ligament; TTFL, transverse tibiofibular ligament.

Type IV configuration with the PTFL and TTFL separated by ≥2-mm gap and TTFL having a “cord-like” structure in a right ankle. (A) Artist’s depiction with PTFL in red and TTFL in green. (B) Arthroscopic view. PTFL, posterior talofibular ligament; TTFL, transverse tibiofibular ligament.
The most common configurations noted were type III in 34 (33.3%) patients, and type II in 33 (32.4%) patients (Table 2). Twenty-six patients (25.5%) had a type I configuration whereas only 9 patients (8.8%) demonstrated a type IV or “cord-like” TTFL. Variability was noted within each group. Ten patients were noted to have a bifid (or double limbed) TTFL and 1 patient even had a trifid ligament. These variations were consistently found in type II (7 patients) and type III (4 patients) configurations. The “tibial slip” (intermalleolar ligament) was observed in 50% of the arthroscopies reviewed (Figure 2). Finally, the presence of a “vertical band” was also appreciated in 30% of the arthroscopies reviewed. This entity consisted of a band of tissue overlying the inferior lateral aspect of the TTFL. The band was variable in its configuration, ranging from a confluence of the capsule to a stout ligamentous band. Neither the “tibial slip” (intermalleolar ligament) or “vertical band” were associated with increased frequency of a specific diagnosis.
Distribution of PTFL and TTFL Subtypes.

Abbreviations: PTFL, posterior talofibular ligament; TTFL, transverse tibiofibular ligament.
The FHL and recess were also evaluated on the degree or ability to localize the tendon within the posterior capsule. In the great majority, 60 patients (58.8%), the FHL tendon was not discernible, usually secondary to synovial proliferation in that area. There was a faint outline of the tendon in 20 patients (19.6%), an easily visualized recess in 12 patients (11.8%), and a discrete tendon structure noted in 10 patients (9.8%) although there was no association of the appearance and a specific diagnosis (Figure 7).

Arthroscopic view of the flexor hallucis longus (FHL) tendon seen through the posterior capsule.
Discussion
Sarrafian and Kelikian 23 described the posterior tibiofibular ligament as being composed of 2 components, superficial and deep. The superficial component originates from the posterolateral distal fibula and extends upward and medial to insert on the posterolateral tibial tubercle. The deep component, coined the transverse tibiofibular ligament by Sarrafian and Kelikian, lies deep and inferior to the posterior tibiofibular ligament. It originates from the posterior fibular tubercle and the upper segment of the digital fossa, and inserts on the posterior aspect of the tibial tubercle surface, reaching the medial border of the medial malleolus. The TTFL projects below the posterior tibial margin, constituting a true posterior labrum and deepening the tibial articular surface. The TTFL fills the posterior aspect of the medial surface of the lateral malleolus and comes in contact with the articular cartilage of the posterolateral talus (Figure 2).
Inferior to the PTFL, the posterior talofibular (PTAF) ligament arises from the depression at the medial and posterior aspect of the lateral malleolus and runs almost horizontally to its insertion onto the trigonal process on the posterior surface of the talus. During dorsiflexion, the posterior talofibular ligament moves distally to expose a synovial-lined cul-de-sac. The floor of this recess often demonstrates a thin band known as the “tibial slip” or intermalleolar ligament. 2,27 The “tibial slip,” first described by Chen, 2 extends from the superior border of the posterior talofibular ligament and runs medially and upward. It inserts on the posterior tibial margin blending with the fibers of the transverse (tibiofibular) ligament and its insertion may reach the posterior surface of the medial malleolus. Paturet 21 called this structure the “posterior intermalleolar ligament.” Golano et al 9,12 prefer the term posterior intermalleolar ligament (IML) instead of the tibial slip and reported that this ligament was found to be a constant structure (100%) with varying size and shape, and well evident during arthroscopy because of its oblique course. Different authors have noted a high variability of presence of the intermalleolar ligament in different anatomical studies, ranging from 0% to 100%. 17 Lee et al 16 identified it in about 20% of MRI examinations. The function and significance of the tibial slip (posterior intermalleolar ligament) is unknown. The tibial slip (posterior intermalleolar ligament) tenses during dorsiflexion and relaxes during plantar flexion. Forced dorsiflexion of the ankle may be the mechanism that leads to an injury or a tear of the tibial slip (posterior intermalleolar ligament). In contrast, plantar flexion takes tension off the tibial slip (posterior intermalleolar ligament), which may make it more prone to becoming entrapped between the tibia and the talus, leading to a posterior soft tissue impingement. 26 Tears of this structure have also been described, especially in professional dancers, basketball players, and other athletes, and are usually treated by excision. 1,3,14
In some of the arthroscopic and radiologic literature, the posterior ligaments are named differently than anatomic texts. Most agree that PTFL is easily visualized but some controversy exists regarding the TTFL, the tibial slip, and the posterior intermalleolar ligament. From an anatomic point of view, the TTFL should be considered the deep component of the PTFL. However most arthroscopic literature consider the TTFL a distinct structure that could be easily visualized in all the ankle arthroscopies. Many authors have confirmed these anatomical findings, whereas Ferkel and colleagues 6,7 noted the same structures arthroscopically in area 17 of the arthroscopic examination. 2,13,15,18,25 They describe the posterior tibiofibular ligament and the transverse (tibiofibular) ligament forming a firm, thick covering or labrum over the posterior tibial lip. Guhl and Patel 13 described the TTFL as a structure that occasionally appears doubled, contradictory to anatomic textbooks in which the TTFL is never reported as a bifid structure. Morgan 18 and Harty and Rives 15 described the anatomy of the TTFL as an extra-articular structure covered with synovium. However, approximately 70% of older patients will have absence or fraying of this lining. 15 They also noted how this ligament forms a labrum-like structure, deepening the posterior lip of the distal tibia helping to prevent posterior talar displacement. This entity has been implicated in pathologic hindfoot impingement syndrome due to hypertrophy. 1,2,14
More confusion arises regarding the tibial slip or the posterior intermalleolar ligament. Guhl and Patel 13 believe that the tibial slip is a variation of the PTFL. Ferkel and Harty consider the presence of this ligament inconsistent and sometimes extrasynovial. 7,15 Morgan considers the tibial slip a thin condensation of the posterior capsule. 18 Based on arthroscopic literature review, it appears that the TTFL is considered distinct from the PTFL and the presence of the tibial slip or the posterior intermalleolar ligament is a variable finding. We found it 50% of the time in our video review.
Another structure, which has not been noted on anatomic or arthroscopic reviews of the ankle, was identified consistently during this review of the ankle arthroscopies. This structure varied in its configuration, ranging from a confluence of the capsule to a separate stout ligamentous band. We have termed this entity the “vertical band” because it is seen overlying the lateral aspect of the transverse tibiofibular ligament running in a vertical orientation (Figure 8). The significance of this structure is unknown at this time; however, it should be considered a normal variant.

Vertical band. This structure overlies the lateral aspect of the transverse (tibiofibular) ligament, running in a vertical direction.
The clinical significance of our findings regarding the 4 distinct ligament patterns in the posterior ankle is unknown. Little information is available regarding the function and biomechanics of these ligaments. Currently, there is some debate as to the exact nature of the posterior ligamentous configurations. In our experience, there are many more variations in the structure of the posterior ligaments of the ankle when compared to the anterior ligaments. These normal variations have not yet been fully described but are important in understanding normal and pathologic findings at ankle arthroscopy. The lack of information regarding these posterior structures makes it difficult to assess the posterior structures of the ankle. In the future, a prospective study needs to be done on a large number of patients to more accurately correlate the posterior capsuloligamentous and FHL configurations to the type of ankle pathology, and to see if certain configurations are more likely to have a specific pathologic diagnosis.
Another interesting finding noted in rare cases was the TTFL appearing as a bifid or even 3-limbed structure. Boynton and Guhl 1 and Morgan 18 also noted that the TTFL can vary in size and may even be a double structure. Although uncommon in this study, this finding was much more prevalent in the type II and III configurations.
These ligamentous variations are important to recognize and understand in order to identify pathologic findings, especially in patients with posterior ankle impingement. Boynton and Guhl,
1
Chen,
2
Conner and Ferkel,
3
and Morgan
18
each described how the TTFL may hypertrophy and cause impingement between the posterior tibia and the posterior talofibular ligament. Debriding or occasionally excising the hypertrophied ligament usually relieves the symptoms. In this study, a ruptured TTFL was noted in 2 patients and an avulsion of the TTFL from the posterior articular surface, similar to a Bankart lesion, was seen in 1 patient (Figure 9). In the past, excision of the torn portion of this ligament has been our treatment of choice although formal outcome testing has not been performed. We reviewed a series of 2352 ankle arthroscopies and found 40 patients with a tear of the TTFL, for an incidence of 1.7% (personal communication). Longitudinal tear of the transverse (tibiofibular) ligament. View is from the anteromedial portal looking posterior in a right ankle.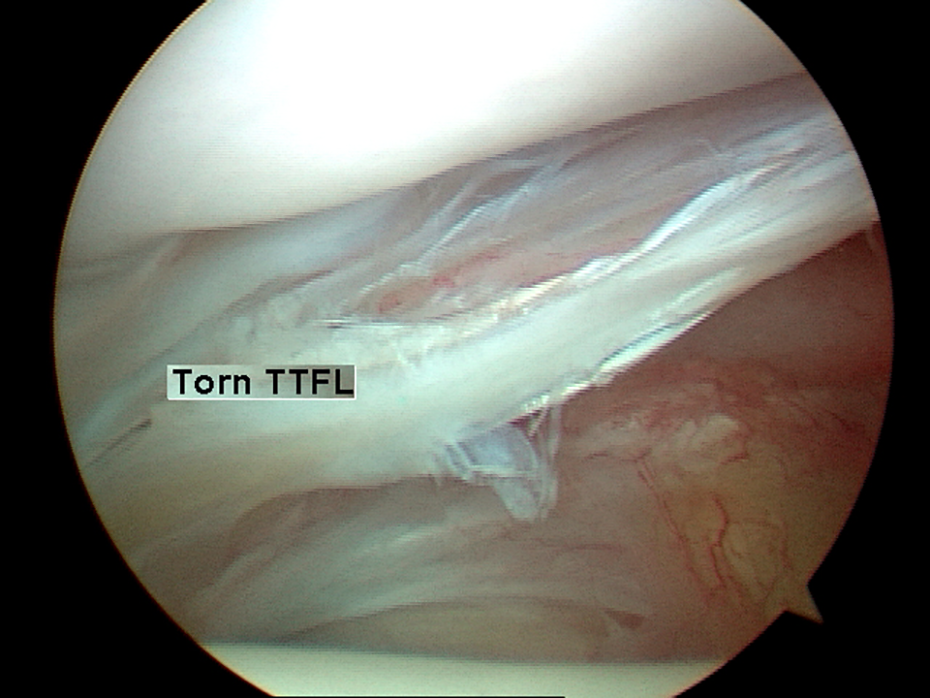
The course of the flexor hallucis longus tendon is described in detail in most anatomic texts. 27 The muscle belly hugs the posterior aspect of the tibia until it forms a tendon approximately 1 to 2 cm proximal to the ankle joint. This tendon passes under the flexor retinaculum and enters the proximal tendon sheath 1 cm above the ankle. The tendon then courses within the fibro-osseous tunnel created by the medial and lateral tubercles of the posterior talus to the level of the sustentaculum tali. The tendon and its sheath are in close contact to the posterior ankle capsule. In fact, Saraffian states that 13% of ankles have a communication between the flexor hallucis longus tendon sheath and the posterior capsule. 24 The FHL tendon then accompanies the flexor digitorum longus and posterior tibialis tendons across the posterior ankle.
In ankle arthroscopy, the flexor hallucis longus tendon is important to identify, especially when creating the posterolateral and posteromedial portals to avoid injury to the neurovascular structures. We have found that identifying the FHL can often be difficult secondary to anatomical variations in capsular thickness or synovial proliferation. In this study, the flexor hallucis longus could not be clearly identified arthroscopically in nearly 60% of the cases. Because of the obvious difficulty in identifying the tendon, extreme care should be used with only blunt instrumentation penetrating the capsule in order to protect the tendon. We routinely place the posterolateral portal in the space between the TTFL and the flexor hallucis longus tendon. It is critical to stay lateral to the FHL tendon to avoid damage to the neurovascular bundle.
Strengths of this study include the highly standardized methodology for identifying and documenting arthroscopic ankle findings. This systematic approach allowed for reliable retrospective video review and data collection. Furthermore, this cohort of more than 100 patients is a substantial sample size for a detailed analysis of this nature.
Limitations
Limitations of this study include its retrospective design. The cohort, although reasonably sized, excluded more than 50 percent of the ankle videos, and it is possible that the results would be different with a larger study group. Additionally, the sample population was drawn from a series of ankles with varying pathologic findings that could have affected the representation of each posterior ligament or FHL type. However, this bias would be present in any arthroscopic study of normal anatomy as arthroscopic examination of a large number of ankles would be ethically challenging. In addition, because there were no ankles with isolated tears of the TTFL, the clinical significance and long-term results of treating these tears is unknown. Moreover, MRI correlation with the arthroscopic findings was not possible, but previous authors have described these findings in detail. 8,20,22
Conclusion
In this study, the arthroscopic appearances and frequency of the posterior ankle structures have been described. To our knowledge, this is the first paper to define the arthroscopic variations of the posterior capsuloligamentous and tendinous structures in the ankle. This is important since understanding the normal posterior anatomy helps the arthroscopic surgeon identify pathology processes that may contribute to the patient’s signs and symptomatology Further studies are needed to understand the biomechanics and function of the posterior ligaments and their correlation to pathologic conditions of the ankle.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211000624 - Arthroscopic Posterior Ankle Ligament Anatomy
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211000624 for Arthroscopic Posterior Ankle Ligament Anatomy by Richard D. Ferkel, Cory Kwong, Randall Farac, Mark Pinto, Nader Fahimi, Scott Rahhal and Jay Marumoto in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was waived by Southern California Orthopedic Research & Education because the research is considered exempt from the Common Rule and all de-identification processes were followed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.