
Abstract
Background:
The high prevalence of ankle sprains in the population produces a significant number of patients with lateral instability. Persistence of this condition may lead to the progressive involvement of medial structures, causing a multidirectional rotational instability.
Methods:
This is a retrospective study with patients diagnosed with multidirectional instability who underwent ankle arthroscopy with medial (arthroscopic tensioning) and lateral repair (arthroscopic Bröstrom) between January 2018 and January 2020. All patients were evaluated for pain and function according to the visual analog scale (VAS) score and the American Orthopaedic Foot & Ankle Society (AOFAS) Hindfoot Score at a mean of 14.8 months (5-27 months) in follow-up. A total of 30 ankles (29 patients) were included in the study.
Results:
The AOFAS score increase from a 49.7 (CI 5.8) to a 91.9 (CI 2.4) mean (P = .001) and was followed by significant improvement in the mean VAS score (6.8, CI 0.37-0.95, CI 0.31). The majority of patients had associated procedures (53.3%), and a low complication rate was found (16.6%).
Conclusion:
Combined medial and lateral arthroscopic repair might be an effective and safe alternative in the treatment of multidirectional instability. Inclusion of the deltoid ligament complex and the low invasiveness of the arthroscopic technique may improve the clinical outcomes of these patients.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Chronic lateral ankle instability (CLAI) is a common condition due to the high incidence of ankle sprains in the population. It can develop in up to 40% of patients experiencing a lateral ligament injury. 26,35 The continuous stress applied by this instability may affect the medial ankle, particularly the deltoid complex and its superficial layer. 19,32,36 This ligament stretching is believed to occur because of 3 possible reasons: continuous talus anterior displacement, direct injuries from talar/medial malleolus collision, and new sprains that may have an eversion moment. 8,14,36
The combination of CLAI with this medial involvement has been termed by authors as multidirectional ankle instability (MAI). 7,25 This condition produces complete anterior laxity and, despite the absence of epidemiologic data, has been associated with a worse prognosis in nonoperative and operative treatment of ankle sprains. 10,26 Clinical and arthroscopic diagnosis remains challenging, as validation of maneuvers and operative findings continue to be scarce. Anteromedial drawer and valgus stress on physical examination, medial laxity, and a “open book” deltoid detachment on arthroscopy are currently used for diagnostic corroboration. 22,36
Meanwhile, deltoid repair techniques have been described, initially using an open approach and ligament imbrication similar to medial repairs during ankle fractures repair. 5,7,24,42 Lately, encouraged by the reliable results of the lateral arthroscopic repair, studies demonstrated the feasibility and good outcomes of the deltoid arthroscopic ligamentoplasty. 20,27,33,36 The objective of this study was to report results of patients diagnosed with multidirectional instability treated with lateral and medial arthroscopic repair, considering pain and function as outcomes.
Methods
This study received approval from the university research committee. It complied with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act (HIPAA). All participants signed a written informed consent.
The research protocol was registered at a public accessible database with the number NCT04459910 (https://clinicaltrials.gov/) in accordance with the Declaration of Helsinki and the International Committee of Medical Journals Editors (ICMJE) good practices.
Design
In this retrospective case series, patients who underwent arthroscopic ligament repair of the medial and the lateral complexes were assessed. The research was undertaken at the Universidade Federal de Sao Paulo Escola Paulista de Medicina.
Participants
Male and female patients from 15 to 65 years old, with complaints of ankle giving away for the last 6 months, and clinical findings of lateral and medial instability were included. Individuals needed to undergo a minimum of 6 months of nonoperative treatment to qualify for surgery.
Existence of previous surgery, autoimmune diseases, neuropathy, inflammatory disease, isolated medial instability, progressive collapsing foot deformity, previous ankle infiltration, radiographic findings of ankle arthritis, cavovarus deformity, coagulopathies, a body mass index higher than 35, and site infection were exclusion criteria. Associated injuries, such as osteochondral lesions, syndesmosis instability, tendon ruptures, and fractures also excluded subjects from this research.
From March 2018 until January 2020, a total of 29 patients (30 ankles) were operated with MAI diagnosis. The mean participant age was 38.0 (SD 12.1), 48% were male (14/29), and women comprised 52% (15/29). Follow-up average was 14.8 (SD 6.9) (Appendix).
Lateral ankle instability was defined as the existence of giving-away symptoms associated with both maneuvers, anterolateral drawer and varus stress. 26,40 Medial instability in this multidirectional scenario was established by the presence of at least 1 of the clinical or arthroscopic findings below: anteromedial drawer or ankle valgus stress in the preoperative clinical assessment; an open book lesion at the medial malleolus, the ability to insert a 5-mm probe in the medial corner of the ankle, or the ability to insert a 5-mm probe at the medial clear space (between the medial surface of the talar body and the articular surface of the medial malleolus) in the arthroscopic evaluation. 36
Physical examination for multidirectional instability was performed with the patient sitting with both limbs hanging, physician seated in front. Anteromedial drawer was executed by holding the lateral distal leg with one hand while the other embraced the medial calcaneus and talar region (index finger at the posterior tuberosity, thumb at the talar neck), producing an anterior movement combined with external rotation. Stress valgus was performed with one hand stabilizing the lateral distal leg while the other embraced only the calcaneus (thenar area at the calcaneus medial region, hypothenar area at the calcaneus lateral region), producing a valgus/eversion moment to the hindfoot. Any subjective asymmetry among ankles (millimeters for the drawer, degrees for the stress) determined the respective maneuver as positive.
For the arthroscopic diagnosis, an “open-book” lesion at the medial malleolus, as described by Vega et al, 36 was considered an indication of multidirectional instability. This finding corresponds to the proximal detachment of the superficial deltoid ligament (tibionavicular band) and explains the rotational component of this instability. 11 Besides, introduction of a 5-mm probe through the medial ankle corner or across the medial tibiotalar space were also considered signs of medial involvement in a multidirectional instability. 18 These assessments were performed by inserting the probe from the anteromedial portal whereas the visualization was carried from the anterolateral portal.
Interventions
Previous nonoperative treatment consisted of at least 6 months of regular physical therapy focusing on global stretching, calf/intrinsics muscle strengthening, and balance training. Surgery was indicated if baseline symptoms persisted and was carried out by 4 fellowship-trained orthopedic foot and ankle surgeons, 2 with more than 20 years and 2 with less than 10 years of experience in the area.
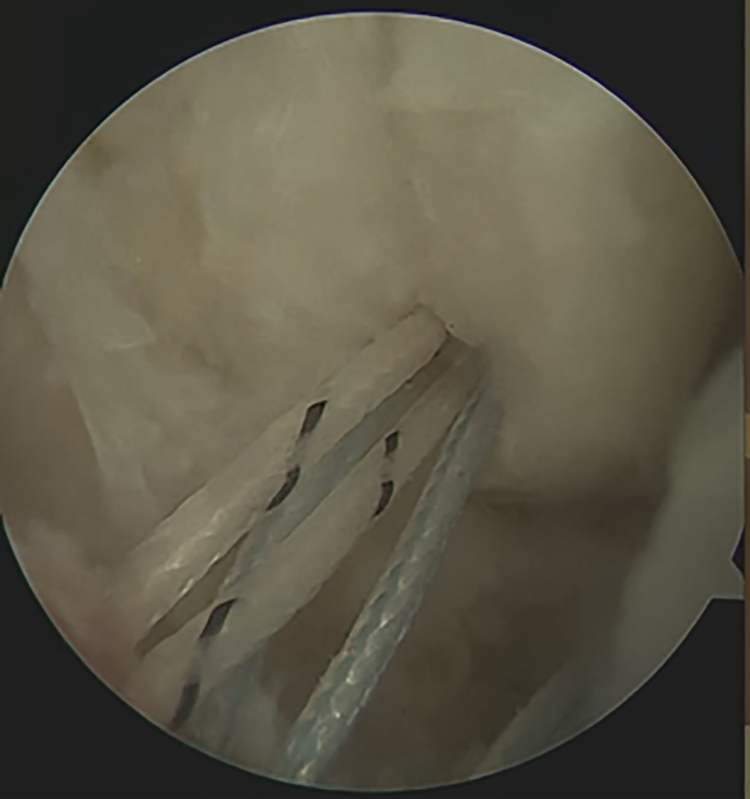
After anesthesia and operative site preparation, traditional anterolateral (AL) and anteromedial (AM) arthroscopic portals were performed. A 4.5-mm (70-degree) scope was used to clean the joint and assess possible associated injuries. Necessary adjuvant procedures were executed before the ligament repair (Appendix). AL and AM impacts were resected when needed. Lateral and medial instability were confirmed arthroscopically, and ligament repairs performed starting laterally. A traditional arthroscopic Bröstrom was performed, using an anchor and suture passers as previously described. 2,27 Sutures were passed but not tightened (Figure 1).
A medial anchor was inserted at the medial malleolus, in the quadrant described by Vega et al 36 (Figure 2). Sutures were passed respecting the safe zone illustrated by Acevedo et al. 1 The ankle was positioned in neutral (no posterior drawer) and the lateral sutures tightened with arthroscopic knots. Finally, the medial repair was finalized by tightening the deltoid sutures with the ankle still in neutral position (Figure 3).
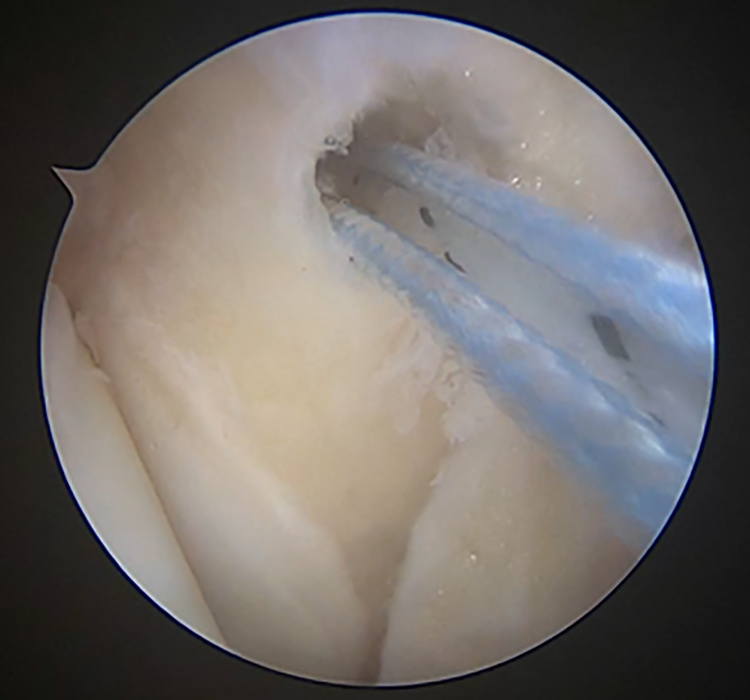
Medial anchor insertion at the medial malleolus quadrant as described by Vega et al. 36

Sutures are passed using an inside-out technique for both ligament complexes. A “Spider Web” configuration is obtained and arthroscopic knots implemented.
Portals were closed and a dressing applied. Patients were put in a walker boot and remained nonweightbearing for 1 week. By the end of this first week, patients were evaluated, and progressive weightbearing began. The boot was worn until the fourth week, when it was replaced by a rigid ankle brace. This orthosis was used until the sixth week and then progressively removed (used for sports until the fifth month).
Physical therapy was started at the second postoperative week (no inversion, eversion, or rotation until the sixth week) and patients were allowed to return to practice (or baseline activities) in a light manner after 3 months. Full return to competitive activity was allowed by the fifth postoperative month (Figure 4).

Weightbearing anteroposterior ankle radiograph from a patient submitted to the described technique and 12 months of follow-up.
Outcomes
Patients were assessed primarily for function through the American Orthopaedic Foot & Ankle Society (AOFAS) Hindfoot Score. Secondary outcomes included pain using the visual analog scale (VAS) and complications. Assessments occurred preoperatively (by 1 week before intervention) and at the 5-month postoperative follow-up. 9,21,30
Complications were recorded as dehiscence, neural damage, infection, and rerupture. Dehiscence was defined as inability to heal the skin by the fourth postoperative week. Peripheral nerve damage was defined as hypoesthesia or paresthesia not resolved by the end of the sixth month after the surgery. Infection was defined as clinical signs of infection or pus drainage of the wound requiring the use of antibiotics. Rerupture was classified as an ankle sprain during the follow-up.
Statistics
After collecting the information, we characterized the variable normality of the qualitative variables through the Kolmogorov-Smirnov test. For relationship between qualitative variables analysis, the Two Proportion Equality Test and the Spearman Correlation were used. Comparison among times of the study was performed with the Wilcoxon test.
Results
AOFAS values showed a mean of 91.9 (2.9 CI) points at the last assessment with a statistically significant difference (P = .001) from baseline (49.7, CI 5.8) (Figure 5). VAS progression (mean 6.8, CI 0.37-0.95, CI 0.31) was also found significant (P < .001). These results were not influenced by other variables, such as adjuvant procedures, complications, and laterality (Figure 6).

American Orthopaedic Foot & Ankle Society (AOFAS) Ankle scores preoperatively and postoperatively in all subjects and in specific subgroups. All P < .005.
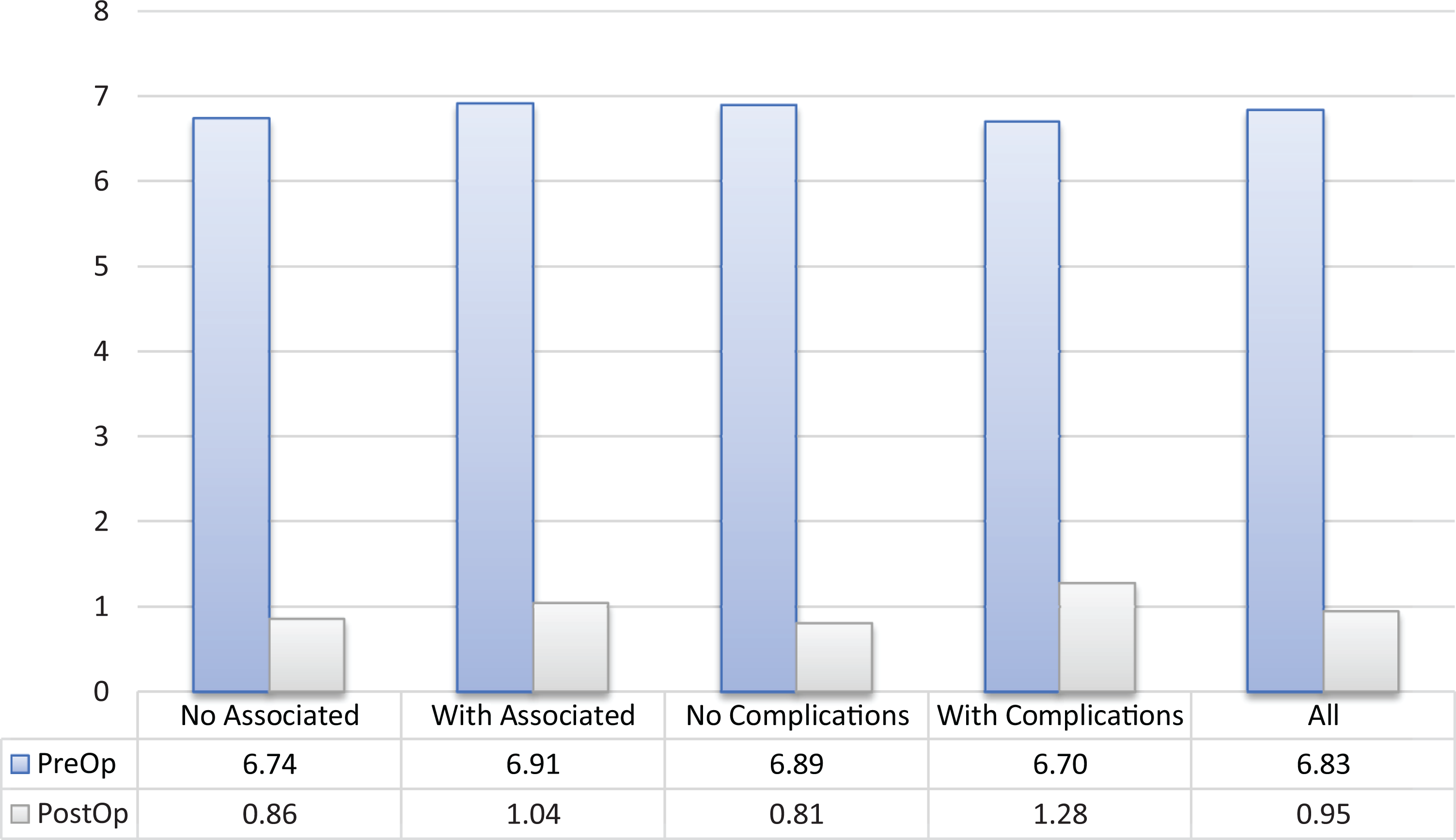
Visual analog scale (VAS) scores preoperatively and postoperatively in all subjects and in specific subgroups. All P < .005.
Complications occurred in 16% of the patients, the majority found to be minor and self-limited. One peri-implant fracture at the medial anchor insertion, 1 transient paresthesia of the sural nerve, 1 superficial infection, and 1 scar retraction were noted. An established superficial peroneal nerve paresthesia accounted for the only major complication in this series.
Adjuvant procedures corresponded mostly to microfracture for osteochondral lesion of the talus (20%), peroneal tendoscopy (10%), lateral internal bracing (10%), and syndesmosis fixation (6%) (Appendix).
Discussion
This study showed good functional results for arthroscopic lateral and medial ligament repair in patients diagnosed with multidirectional ankle instability. MAI has been discussed over the last years as a possible cause for failures in patients having lateral ankle instability. 26,29 Moreover, it also may be related to some types of impingement, tendinopathies, and different degenerative processes. 31,37,39 Medial ligament failure in addition to lateral laxity produces a distinct instability of the ankle joint, a concept that has still to be tested.
A few theories exist to explain the etiology and the pathogenesis of this condition, because the majority of cases do not have a history of eversion or external rotation trauma. Recurrent strain to the superficial deltoid during multiple inversion sprains could be the cause for the medial impairment in this syndrome. 8 Biomechanically, the tibionavicular deltoid limits talar anterior translation and external rotation. 16,23 Continuous deltoid impingement between talus and medial malleolus might also weaken the ligament. 14 Ultimately, the possibility of an associated eversion or external rotation component to a sprain may also explain the injury to the deltoid. 36
Medial ligament insufficiency in a multidirectional scenario was first described by Vega et al, 36 who determined the absence of deltoid attachment at the medial malleolus corner as a sign of this impairment. Our study incorporated other clinical findings of medial involvement as a predictor, as the anteromedial drawer and the valgus stress test. Early or late signs of foot flattening were considered medial ankle instability, a different condition in the opinion of many authors, and, therefore, not included in our series. 6,15,28 Besides, other arthroscopic findings, such as the drive-through test in the medial clear space and in the anteromedial gutter, were also considered medial ligament deficiency. 18
Plication of the medial ligament structures, specifically the superficial deltoid ligament, was proposed as a solution to multidirectional instability. 20,36 By inserting an anchor in a predetermined quadrant of the medial malleolus and passing the sutures through a safe zone, Acevedo et al 1 had sustained clinical results. The present study supported this idea by demonstrating good functional results and a low complication rate.
Pain levels at final evaluation, measured by the VAS, were found similar to the work of Feng et al 12,13 (1.12 ± 0.13), which assessed this outcome in patients who underwent a Brostrom arthroscopic repair at medium-term follow-up. Findings of the current study support ankle arthroscopic ligament repairs, specifically when combining lateral and medial complexes, as a secure option in terms of reestablishing a painful joint. Microinstability theories rely on the presence of pain as an indirect sign of its true existence, which may favor the argument that a multidirectional repair could actually treat this disease. 37
In terms of function, AOFAS postoperative scores reached good and excellent levels in the majority of patients, with a mean of 92.6. This is also comparable to the studies of Vega et al 38 (mean 97, range 85-100) and Woo et al 41 (94.2 ± 10.0) that used this score to assess patients after a lateral arthroscopic repair. The findings of Vega et al 36 (100, range 77-100) and Acevedo et al 1 (90%), more suitable for the discussion of the deltoid arthroscopic repair, are also consistent with the present results, endorsing the potential for functional gain with this procedure.
A low rate of direct complications (5 of 30, 16%) was also found in the present study, most of it minor and self-limited (5 of 6, 83%). Guelfi et al 17 and Takao et al 34 also have shown very low complication rates in reconstructive arthroscopic procedures of the lateral ligaments. 4 This perception of safeness was also demonstrated by Acevedo et al 1 and Vega et al 36 in their medial repair series. A lack of major complications was noted in those studies, although loss in range of motion was not considered a complication criteria.
A peri-implant fracture of the medial malleolus was observed in our study, probably because this anchor was inserted below Vega’s quadrant, producing stress at the bone apex. It occurred in the 26th postoperative week and healed by decreasing the patient activity level. Other indirect complications, such as sural paresthesia, screw prominence, and Tight-Rope protuberance were related to adjuvant procedures.
All patients had an absence of sprains or instability symptoms during the follow-up. Clinical postoperative assessment found negative anterolateral and anteromedial drawer tests, and negative varus and valgus stress, in addition to no signs of syndesmosis instability. They were also able to return to normal daily and sports activities as desired.
The main limitations of this study are its retrospective design, the absence of a control group, and the short-term follow-up. Lack of a more objective outcome measure for this condition would have been helpful now that instability-specific questionnaires are available. A nonvalidated score (AOFAS) was used instead. Moreover, no sample size calculation or postoperative power analysis was performed, weakening study validity, especially when associated procedures are pondered. Study’s strenghts include its actuality, the number of patients, and the medium-term evaluation period. The inclusion of patients with other clinical and arthroscopic signs of medial instability in a multidirectional scenario, previous protocol publication and the description of complications are also positive aspects of this research.
In conclusion, multidirectional instability still has a long debate ahead and many aspects to be tested. Its importance and treatment necessity are increasingly gaining attention as the notion that not every ankle behaves the same. Results of this study, grounded in its good results and low complication rate, may establish a strong base for potential case-control studies and clinical trials in a near future.
Supplemental Material
Supplemental Material, sj-docx-1-fao-10.1177_2473011420986150 - Medial and Lateral Combined Ligament Arthroscopic Repair for Multidirectional Ankle Instability
Supplemental Material, sj-docx-1-fao-10.1177_2473011420986150 for Medial and Lateral Combined Ligament Arthroscopic Repair for Multidirectional Ankle Instability by Nacime Salomão Barbachan Mansur, André Vitor Kerber Cavalcante Lemos, Daniel Soares Baumfeld, Tiago Soares Baumfeld, Marcelo Pires do Prado, Fernando Cepolina Raduan and Caio Augusto Souza Nery in Foot & Ankle Orthopaedics
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420986150 - Medial and Lateral Combined Ligament Arthroscopic Repair for Multidirectional Ankle Instability
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420986150 for Medial and Lateral Combined Ligament Arthroscopic Repair for Multidirectional Ankle Instability by Nacime Salomão Barbachan Mansur, André Vitor Kerber Cavalcante Lemos, Daniel Soares Baumfeld, Tiago Soares Baumfeld, Marcelo Pires do Prado, Fernando Cepolina Raduan and Caio Augusto Souza Nery in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
University Ethics Committee approved this research under the number 32854720.8.0000.5505 in accordance with the Declaration of Helsinki. Protocol registration was executed at the Clinical Trials database under the protocol number NCT04459910.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD
Supplemental Material
A supplemental video for this article is available online.
Appendix
Raw patient data. AOFAS: American Orthopaedic Foot and Ankle Society – Ankle Score.

| AGE | SIDE | AOFAS PREOP | VAS PREOP | FOLLOW-UP | AOFAS POSTOP | VAS POSTOP | COMPLICATIONS | ADJUVANT PROCEDURES |
|---|---|---|---|---|---|---|---|---|
| 49 | L | 18 | 7.8 | 22 months | 90 | 1.5 | no | microfractures OLT (AL) + syndesmosis fixation |
| 36 | R | 64 | 6.2 | 18 months | 90 | 0.5 | peri implant medial fracture | microfractures OLT (AM) |
| – | L | 64 | 6.2 | 18 months | 90 | 0.5 | no | microfractures OLT (AM) |
| 17 | R | 56 | 6.7 | 24 months | 85 | 1 | no | no |
| 45 | R | 45 | 8.2 | 8 months | 87 | 2.1 | no | microfractures OLT (AM) |
| 24 | R | 67 | 4.8 | 6 months | 82 | 3 | no | no |
| 34 | R | 69 | 5.2 | 6 months | 100 | 1 | no | no |
| 42 | R | 57 | 5.7 | 6 months | 82 | 2 | loss of 10 in ROM | no |
| 65 | R | 57 | 7.2 | 10 months | 90 | 1 | no | microfractures OLT (AM) |
| 28 | R | 55 | 5 | 5 months | 82 | 3 | no | peroneal tenoscopy |
| 21 | R | 25 | 8 | 24 months | 100 | 0 | no | no |
| 48 | R | 55 | 5.2 | 6 months | 100 | 1 | temporary scar retraction of the lateral portal | no |
| 30 | R | 45 | 7 | 12 months | 90 | 1 | no | no |
| 20 | R | 55 | 6.7 | 8 months | 87 | 0 | no | no |
| 44 | R | 31 | 8 | 27 months | 100 | 0 | no | no |
| 47 | R | 53 | 7 | 26 months | 100 | 0 | no | arthroscopic internal brace (lateral) |
| 51 | R | 53 | 7 | 25 months | 100 | 0 | no | no |
| 26 | R | 17 | 8 | 24 months | 86 | 2 | pain at dweyer screws insertion (hwr) | dweyer calcaneus osteotomy |
| 62 | R | 49 | 7 | 17 months | 100 | 0 | no | no |
| 55 | R | 49 | 7 | 16 months | 88 | 1 | SPN established paresthesia | no |
| 29 | L | 53 | 7 | 16 months | 87 | 1 | no | arthroscopic internal brace (lateral) |
| 42 | R | 31 | 8 | 16 months | 100 | 0 | no | no |
| 35 | L | 53 | 7 | 15 months | 100 | 0 | no | peroneal tenoscopy |
| 23 | R | 22 | 8 | 10 months | 87 | 1 | no | microfractures OLT (AL) |
| 38 | R | 27 | 8 | 7 months | 90 | 1 | no | arthroscopic internal brace (lateral) |
| 49 | L | 61 | 7 | 18 months | 97 | 1 | tight-rope removal due prominence | syndesmosis flexible fixation |
| 34 | L | 67 | 5 | 12 months | 97 | 0 | no | distal fibula fragment resection |
| 39 | R | 62 | 7 | 18 months | 91 | 1 | no | peroneal tenoscopy |
| 37 | R | 53 | 8 | 12 months | 83 | 2 | superficial infection (treated with atb) | no |
| 34 | R | 79 | 6 | 12 months | 97 | 1 | temporary sural paresthesia | dweyer calcaneus osteotomy |
Abbreviations: VAS, visual analogic scale; R, right; L, left; OLT, osteochondral lesion of the talus; AL, anterolateral; AM, anteromedial; HWR, hardware removal; ATB, antibiotics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.