
Abstract
Background:
Adult acquired flatfoot (AAFD) is commonly treated by foot and ankle surgeons. Despite how commonly this disease presents, its incidence and economic impact have yet to be defined. We hypothesized that the operative incidence of AAFD and its economic burden would increase over the time period 1996 to 2014.
Methods:
The South Carolina database was queried for data from acute care and ambulatory surgery centers. Bivariate descriptive statistics were used to analyze the data. Operative incidence was calculated and demographics and medical comorbidities of patients who progressed to operative intervention were analyzed. Costs associated with operative care episodes were calculated to determine the economic burden.
Results:
A total of 1299 patients underwent AAFD corrective surgery between 1996 and 2014. Patients who underwent surgery for AAFD were most likely to be white, female, and in their fourth, fifth, and sixth decade of life. Operative incidence for AAFD rose from 0.26 per 100 000 covered lives in 1996 to 3.04 in 2014. The total health care costs associated with patients who underwent surgery for AAFD increased from $57 395.33 in 1996 to $6 859 723.60 in 2014.
Conclusions:
This data demonstrate that patients most commonly undergoing operative intervention for AAFD were white, female, and in their fourth, fifth, or sixth decade of life. There has been a significant increase in operative incidence, which may help direct attention to further exploration of outcome data in these patient populations, associated treatment costs, and preventative treatment options.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Adult acquired flatfoot deformity (AAFD) is one of the most common conditions seen by foot and ankle surgeons. At present, there are no large-scale epidemiologic studies; however, the reported rates of AAFD are greater than 3% in women aged ≥40 years and greater than 10% of all adults aged ≥65 years. 4
Dysfunction of the tibialis posterior tendon (ie, PTTD) is thought to be a common etiology predisposing to the subsequent development of AAFD. Discussion of “flatfoot” in the literature dates back to the late 19th century and continues to this day with publications about our understanding of the disease and novel operative interventions published almost monthly. 8
Surgeons understand more about AAFD and improvements in patient outcomes both via operative and nonoperative interventions. However, despite this, the disease progression along with incidence, optimal operative timing, and economic impact of disease has yet to be well defined. These variables are key for orthopedic surgeons to understand to allow continued improvement in caring for patients with this complex problem.
We sought to determine the incidence of operative intervention for AAFD through a state database query. Additionally, we aimed to evaluate the number of and type(s) of surgeries performed, establish patient demographics, analyze comorbidities, determine admission type, and determine the economic impact for patients with a diagnosis of AAFD who underwent corrective surgery. Our hypothesis was that the operative incidence of AAFD would increase over time secondary to an aging population, improvement in imaging technologies, operative treatment, increased recognition of the disease, and surgeons trained to treat this condition. We also performed a cost analysis to assess the economic burden AAFD has on our community.
Methods
Data Source
After local institutional review board approval, billing data were obtained from the South Carolina Fiscal Affairs and Revenue database (SC database) from 1996 to 2014. The SC database compiles billing data annually from approximately 185 acute care and ambulatory surgery centers in the state of South Carolina. Discharges contain a unique patient identifier that allows tracking of patient readmissions. Along with demographic information, the SC database includes multiple diagnoses and procedures per patient visit. We obtained the following demographic and descriptive information: length of stay, day of the week admission, month of admission, day of the week discharge, month of discharge, admission source, admission type, time from admission to discharge, patient age at admission in years, patient gender, patient race/ethnicity, county of patient’s residence, admitting diagnosis, admission indicator for all diagnoses, diagnosis codes, procedure codes, procedure day, major diagnostic categories, E-codes (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM]), external cause of morbidity codes (International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM]), patient discharge statues, Diagnosis-Related Group (DRG), All Patients Refined Diagnosis-Related Group (APR-DRG) score, APR-DRG description, primary expected payer classification, charges by summary revenue codes, total charges, days in special units, physician specialty code, health care professional classification. Despite the availability of these demographics, many of these were beyond the scope of this article. Hospital characteristics included trauma level and bed size based on licensed beds. The SC database utilized the ICD-9-CM to code diagnoses and procedures.
Inclusion and Exclusion Criteria
All patients included in the final analysis had an ICD-9-CM diagnoses of flatfoot (734). All included patients were also identified as having undergone corrective surgery for flatfoot deformity. This was determined by identifying patients with an ICD-9-CM diagnosis of flatfoot who also had at least 1 ICD-9-CM procedure code indicative of a corrective procedure for flatfoot deformity. Patients who did not have an ICD-9-CM procedure code indicative of a flatfoot corrective procedure were excluded from the study as well as all patients aged ≥15 years because of the potential that they were still skeletally immature.
Statistical Analysis
Bivariate descriptive statistics were used to analyze the data. The operative incidence was calculated by assessing the number of operative procedures performed per year for AAFD compared with the number of lives covered by the SC database per year. Demographics and medical comorbidities of patients who progressed to operative treatment for AAFD were analyzed. The cost associated with the operative care episode was calculated to determine the economic burden of the disease. Given the retrospective nature of the study, we used a regression analysis with multiple dependent variables to look for trends that could be analyzed in a larger cohort or prospective fashion.
Results
In total, 1299 patients underwent 1650 AAFD corrective surgeries between 1996 and 2014. The operative incidence of AAFD per 100 000 increased from 0.26 in 1996 to 3.04 in 2014 (Figure 1). The highest operative incidence was seen in 2010 at 4.03. Raw procedure counts for AAFD increased during this time period as well, from 10 procedures performed in 1996 to 147 in 2014. During their index surgery, 1034 patients underwent 1 procedure, 219 patients underwent 2 procedures, 41 patients underwent 3 procedures, 4 patients underwent 10 procedures, and 3 patients underwent 5 procedures to correct their flatfoot. AAFD procedures were defined as patients who had at least 1 associated ICD-9 code that was indicative of a procedure or surgery performed for AAFD. Individual patient identifiers were not available, and therefore bilateral flatfoot surgeries were not able to be separately analyzed.

The operative incidence per 100 000 of adult acquired flatfoot deformity (AAFD) from 1996 to 2014.
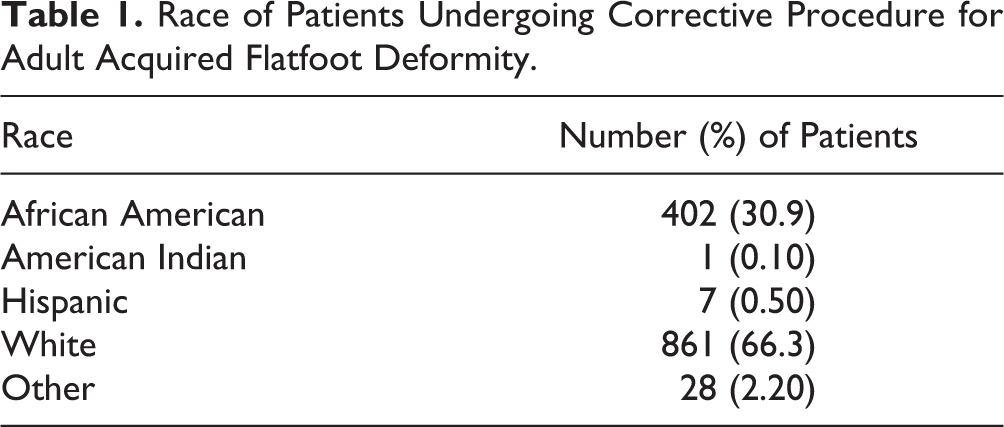
Patients who underwent surgery for AAFD were more likely to be white, female, and in their fourth, fifth, or sixth decade of life. Women accounted for 71.1% of the patient population (Figure 2). Whites made up the majority of patients, accounting for 66.3%, followed by African Americans at 30.9% (Table 1). Hypertension, tibialis tendinitis, diabetes, and obesity were common among our patients as noted in the top 10 most frequently associated diagnoses and comorbidities of our patient population (Table 2).

Percentage of patients per 5-year age group by sex. Percentage male and percentage female each total 100% individually.
Race of Patients Undergoing Corrective Procedure for Adult Acquired Flatfoot Deformity.
Top 10 Associated Diagnoses and Comorbidities.

Patients who had more than 1 associated ICD-9 code indicating an AAFD corrective surgery were most likely to have had a combination of soft tissue procedures, osteotomies, and fusion procedures, followed by soft tissue procedures alone and then fusion procedures in isolation. The most commonly performed procedure was a tendon transfer or transplantation (likely of the flexor digitorum longus or a similar transfer). The second most commonly performed procedure was a tendon recession. This was followed by wedge osteotomy, likely to be a calcaneal, Evans or Cotton osteotomy. Arthrodesis and fusion procedures were also common among our patient population (Table 3). Common procedure terminology was not included in this database, making it difficult to determine the exact type of tendon transfer/transplantation, and type of osteotomy that was performed.
Most Commonly Performed Corrective Procedures for Adult Acquired Flatfoot Deformity.

The total economic burden of patients who underwent corrective surgery for AAFD from 1996 to 2014 in South Carolina was estimated to be $48 465 337.00. The average total cost per procedure was $29 373.00. The total health care costs associated with patients who underwent surgery for AAFD rose from $57 395.33 in 1996 to $6 859 723.60 in 2014 (Figure 3). The majority of procedures were elective in nature, with the primary payer being commercial insurance (Table 4).

Total health care costs of patients undergoing corrective procedures for adult acquired flatfoot deformity (AAFD) from 1996 to 2014.
Number of Patients Making Up Each Primary Payer Group and Admission Type.

Discussion
The purpose of this study was to begin to understand the true incidence, operative management and cost burden of AAFD deformity in our community. With this initial data, it is clear that not only is there a population who undergoes operative intervention for this procedure more often than others but also that the operative management of AAFD is increasing overall with an increased cost burden to our health care system.
AAFD is a debilitating problem and can lead to time off work, loss of quality of life years, and disability. Despite recognition of patients with painful flatfoot and discussions in the literature since the late 19th century, there remains little knowledge of the incidence of this disease. Previous studies have found that the population most at risk for AAFD is elderly women, specifically over the age of 40. 2,3,9 PTTD and subsequent AAFD is 3 times more common among women, and presents on average at 40 years of age. 2 The largest of these studies was a self-reported telephone survey conducted in England. This study surveyed 1000 women aged ≥40 years. Included in the final analysis were 582 patients of whom only 9 had AAFD. This study found the prevalence of PTTD to be 3.3% among women aged ≥40 years. 4 However, this study was limited by the self-reported nature of the problem and its 58% attrition rate.
The treatment for AAFD includes both nonoperative and operative intervention. Nonoperative intervention includes rest, anti-inflammatory medication, orthotics, bracing, custom bracing, and physical therapy. Operative intervention includes a combination of soft tissue procedures, bony procedures, and fusions. 1,5 -7,10 Unfortunately, the rate of progression of this disease and the number of patients who fail conservative treatment and may require operative intervention is not well known. However, our paper was aimed to help the reader have a better understanding of who these patients may be and understand current trends in operative management. Our data support that during the past 18 years, more patients have been undergoing operative treatment for AAFD. The reason why is multifactorial, but most likely because of increased recognition of the disease and disease process, improvement in operative treatment options, and the aging population.
We were able to show both that the operative incidence of AAFD is increasing within our community and the most commonly affected patients are white, female, and in their fourth, fifth, or sixth decade of life. During the last decade, 929 female and 378 male patients underwent corrective surgery for AAFD. Fewer men underwent surgery in general, and they tended to undergo corrective surgery later than women, in the fifth and sixth decades of life. Among females, 60% were age 40 years or older when undergoing surgery, thus confirming trends seen in previous studies. 2,4,9
When undergoing operative intervention, our data suggest that most patients undergo only 1 or 2 procedures. This was an unexpected and interesting finding as most published data would suggest a minimum of 2 procedures (flexor digitorum longus transfer and calcaneal osteotomy) should be done for treatment of most stages of AAFD. This raises the questions of the spread of common treatment guidelines, new innovations for operative management, and spread of education in our communities. These studies are often done at large tertiary referral centers by fellowship-trained foot and ankle surgeons. Therefore, this knowledge may be limited to more isolated communities than we once thought. As a foot and ankle society, these data show that many in the community may not be doing what current literature supports, and further studies need to look at large community cohorts to analyze procedures that are done. This may direct further educational efforts to optimize both treatment strategies and patient outcomes.
Our cost analysis shows that the economic burden of operative management of AAFD has increased over time. Further studies need to be done to look at the direct cost of quality of life years and lost time from work in the management of AAFD both from an operative and nonoperative standpoint. Additionally, these data are important because it provides us insight into those most likely to undergo operative intervention. More studies will now need to focus on these patients to see how well they do with nonoperative intervention and the cost associated with this. These data will be important to help us better direct treatment options and possible timing of operative intervention, which could improve outcomes and minimize the overall cost for our patients and health care system.
As with any database analysis, this study has limitations. In order to determine the most accurate operative incidence rates and patient populations, the medical condition of interest must have a specific ICD-9-CM diagnosis code, and as many potential confounders as possible must be accounted for. Nuances in coding and errors in data input, collection, or interpretation can lead to inaccurate results, which likely resulted in the majority of our patients having only 1 associated ICD-9 code indicative of an AAFD corrective procedure. In our study, we used the ICD-9-CM diagnosis code 734 (flatfoot), which is specific to AAFD, yet still prone to errors in coding and diagnosis. In our study, the most common procedure performed on patients who were included in our final analysis was a tendon transfer/transplantation. Because of coding terminology, it is impossible to determine exactly what tendon was transferred; therefore, results may be confounded by bias in assuming these procedures were performed to correct for AAFD. It is also impossible to ascertain whether an adult with a diagnosis of AAFD had a congenital flatfoot deformity that was not diagnosed until adulthood. Because of the nature of the database and medical coding, we concluded that patients with a diagnosis of flatfoot as well as multiple procedure codes indicative of corrective procedures for flatfoot were likely to have undergone a procedure to correct AAFD. Specific to our study, it must be noted that the decision to proceed with surgery is multifactorial. There are numerous patient factors and physician considerations prior to recommending or proceeding with operative intervention. Given the nature of this database study, we cannot speculate on these factors. There is no information on the extent of the patient’s preoperative flatfoot deformity, level of rigidity, or radiographic findings that are important for the diagnosis and management of this disease. The impact of surgeon awareness of AAFD and its treatment options, which have evolved during the studied time period, is unable to be analyzed with a database study. Additionally, we do not know the number of patients who did not desire to proceed with surgery to whom it was recommended or the number of patients who were not deemed candidates for operative intervention but had painful AAFD.
In conclusion, our study provides a foundation for the operative incidence of AAFD and we hope helps surgeons have a better understanding of which patients may require operative intervention. This information demonstrates that the cost of treatment of AAFD in our society is increasing and, therefore, improved understanding of the burden to the patient and to society may warrant the need for increased scientific investigation of the etiology, pathophysiology, and prevention of this disease. To improve our patient outcomes and minimize future cost, we hope these data will help investigators secure funding for well-planned, longitudinal, scientific studies that seek to answer these clinically relevant questions about the development, progression, treatment, and costs of AAFD so we can optimize the treatment of this disease process.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420985864 - 18-Year Operative Incidence and Cost Analysis of the Treatment of Adult Acquired Flatfoot Deformity
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420985864 for 18-Year Operative Incidence and Cost Analysis of the Treatment of Adult Acquired Flatfoot Deformity by J. Benjamin Jackson, Tyler M. Goodwin and Tyler A. Gonzalez in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was waived by the Prisma Health - Midlands Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.