
Abstract
Background:
The intermetatarsal joint between the fourth and fifth metatarsals (4-5 IM) is important in defining fifth metatarsal fractures. The purpose of the current study was to quantify this joint in order to determine the mean cartilage area, the percentage of the articulation that is cartilage, and to give the clinician data to help understand the joint anatomy as it relates to fifth metatarsal fracture classification.
Methods:
Twenty cadaver 4-5 IM joints were dissected. Digital images were taken and the articular cartilage was quantified by calibrated digital imaging software.
Results:
For the lateral fourth proximal intermetatarsal articulation, the mean area of articulation was 188 ± 49 mm2, with 49% of the area composed of articular cartilage. The shape of the articular cartilage had 3 variations: triangular, oval, and square. A triangular variant was the most common (80%, 16 of 20 specimens). For the medial fifth proximal intermetatarsal articulation, the mean area of articulation was 143 ± 30 mm2, with 48% of the joint surface being composed of articular cartilage. The shape of the articular surface was oval or triangular. An oval variant was the most common (75%, 15 of 20 specimens).
Conclusion:
This study supports the notion that the 4-5 IM joint is not completely articular and has both fibrous and cartilaginous components.
Clinical Relevance:
The clinical significance of this study is that it quantifies the articular surface area and shape. This information may be useful in understanding fifth metatarsal fracture extension into the articular surface and to inform implant design and also help guide surgeons intraoperatively in order to minimize articular damage.
Introduction
The proximal fourth and fifth intermetatarsal (4-5 IM) joint is commonly involved in fractures of the base of the fifth metatarsal as well as other conditions such as lateral midfoot arthritis. 1,20,21 There is little published on the anatomy and characterization of the 4-5 IM joint, including the size and orientation of the articular cartilage. The published literature on fifth metatarsal fractures emphasizes extension into the 4-5 IM joint as an important variable but does not describe if this represents extension into an articular surface. 9,12,18 An understanding of the articular anatomy may provide insight into the variation of published outcomes from these types of fractures. 10,17
The purpose of the current study was to quantify the articular surface of the 4-5 IM joint in order to determine the mean cartilage area, the shape and dimensions of the joint, the percentage of the articulation that is cartilage, and to give a surgeon data to use in understanding this anatomic location.
Methods
Twenty paired, below-knee specimens were obtained and dissected. All specimens had an intact foot and ankle. Specimens with evidence of previous foot or ankle surgery or with significant pathologic abnormalities that were identified during dissection were excluded. The mean age of the donors was 77 years (range: 56-91 years). Dissections were carried out at room temperature and under supervision of a fellowship-trained orthopedic foot and ankle surgeon.
The cartilaginous and fibrous aspects of the proximal fourth and fifth metatarsals were carefully identified and quantified by calibrated digital imaging software. This was done by taking digital images of the joint surface, calibrating the image size and measuring the cartilage surface using an image processing software as described by others (ImageJ 1.47, http://rsbweb.nih.gov/ij/, accessed September 8, 2020). 2,6,7 This facilitated an accurate measurement of area of an irregular surface. Statistical analysis was performed with R (R version 2.11.1, http://cran.r-project.org/, accessed March 25, 2020).
Results
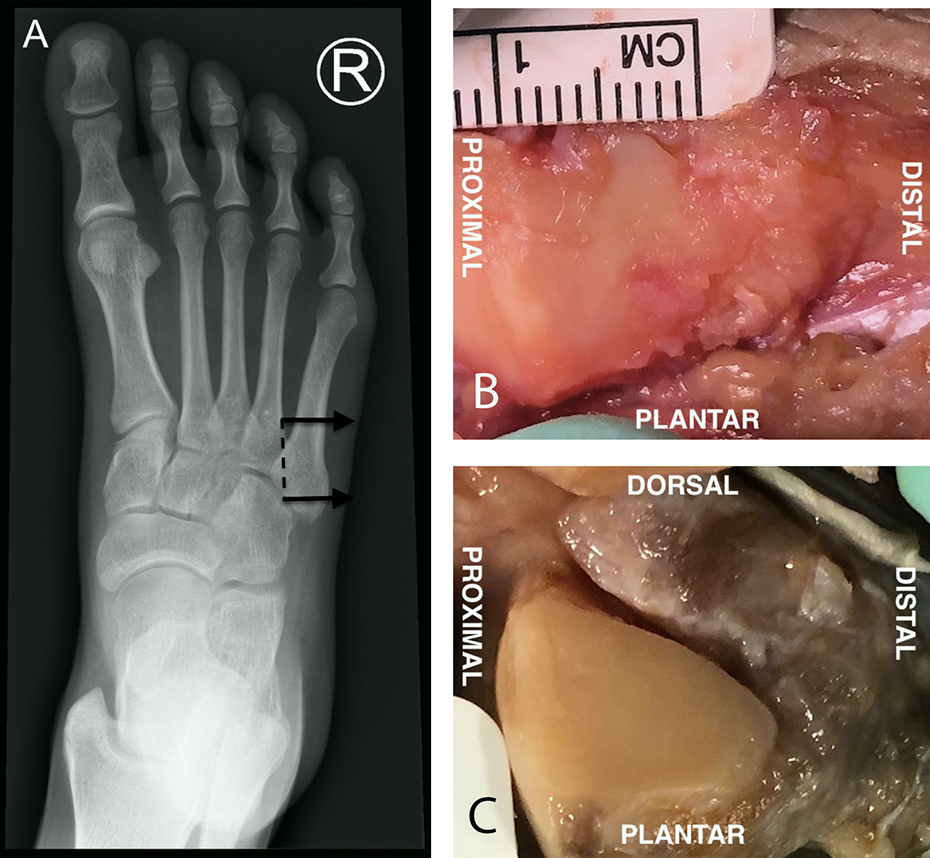
For the lateral fourth metatarsal proximal intermetatarsal articulation, the mean area of articulation was 188 ± 49 mm2, with 49% of the area composed of articular cartilage. The shape of the articular cartilage had 3 variations, which are demonstrated in Figure 1: triangular, oval, and square, with the triangular variant being the most common (80%, 16 of 20 specimens). The square-shaped variation was seen in 15% of specimens (3 of 20) and the oval variation was seen in 5% of specimens (1 of 20). The triangular variant had a vertical proximal base and a plantar-distal directed apex. Dorsal to the articular cartilage was the location of the fibrous aspect of the articulation. The square variant had articular cartilage located more centrally and was surrounded by a thin rim of fibrous tissue that was more prominent distal to the articulation. The oval variant also had more central articular cartilage and was surrounded by a thin rim of fibrous tissue that became more prominent distally. In the triangular and oval variants, the articular cartilage tapered off from proximal to distal, leading to more of the joint being fibrous distally. All articular surfaces were noted to be nearly flat.

(A) The lateral fourth proximal intermetatarsal articulation. The arrow denotes the direction of the viewing plane, and the dotted line represents the viewing plane. (B) The square variant in the lateral fourth proximal intermetatarsal articulation with articular cartilage located more centrally and surrounded by a thin rim of fibrous tissue that is more prominent distal to the articulation. (C) The triangular variant with a vertical proximal base and plantar-distal directed apex. Dorsal to the articular cartilage lies the fibrous aspect of the articulation. (D) The oval variant in the lateral fourth proximal intermetatarsal articulation with its articular cartilage centrally located and surrounded by a rim of fibrous tissue
For the medial fifth metatarsal proximal intermetatarsal articulation, the mean area or articulation was 143 ± 30 mm2, with 48% of the joint surface being composed of articular cartilage. The shape of the articular surface was oval and triangular, with the oval variant being the most common (75%, 15 of 20 specimens). These variants are demonstrated in Figure 2. The oval variant also had a more central articular cartilage and was surrounded by a thin rim of fibrous tissue that became more prominent distally. The triangular variant was similar to the one seen for the lateral fourth proximal intermetatarsal articulation in that it had a vertical proximal base and a plantar-distal directed apex. Dorsal to the articular cartilage was the location of the fibrous aspect of the articulation. In both variants, the articular cartilage tapered off from proximal to distal, leading to more of the joint being fibrous distally. All articular surfaces were essentially flat to visual inspection.
(A) Medial fifth proximal intermetatarsal articulation. The arrow denotes the direction of the viewing plane and the dotted line represents the viewing plane. (B) The oval variant in the medial fifth proximal intermetatarsal articulation with its articular cartilage more centrally located and surrounded by a rim of fibrous tissue. (C) The triangular variant with a vertical proximal base and plantar-distal directed apex. Dorsal to the articular cartilage lies the fibrous aspect of the articulation.
Based on the measurements above, the lateral fourth proximal metatarsal joint had a substantially larger articular surface area than the medial fifth metatarsal joint (92 ± 25 mm2 vs 69 ± 18 mm2; P < .001).
The proximal to distal length of the 4-5 IM joint articular surface was also measured. The lateral fourth proximal intermetatarsal articular surface measured 9.7 ± 1.6 mm in the proximal to distal direction from the ridge between the fourth tarsometatarsal joint and intermetatarsal joint. The medial fifth proximal intermetatarsal articular surface measured 9.5 ± 1.2 mm in length in the proximal to distal direction from the ridge between the fifth tarsometatarsal joint and the intermetatarsal joint. The difference between the 2 joints was not statistically significant (P = .6573).
Discussion
This study was undertaken to examine the 4-5 IM joint, which is poorly described in the literature. To our knowledge, this is the first study to quantify the cartilage area between these bones. This study fills an information gap in the literature surrounding fifth metatarsal fractures that consider extension into this region as a defining feature.
Jones fractures, first described in 1902 by Sir Robert Jones, have subsequently been classified as fractures that extend into the 4-5 IM joint. 9 These fractures have subsequently been thought to be problematic because of vascular considerations but without published clarification as to why extensions of the fracture into the joint itself is important mechanically and anatomically. 22,24 The features of the joint, as described in the current study, provide a framework for this injury to be considered an articular fracture. Additionally, fixation options that include plate and screw fixation often are placed from a lateral approach whereby screw tip penetration may be a risk to the articular surface as well. This study supports the notion that a Jones fracture likely has a cartilage injury unless it penetrates the articulation very distally where the joint becomes more fibrous in nature. It also supports the notion that screws should not penetrate the 4-5 IM space as they can cause iatrogenic cartilage damage.
Another clinical consideration of the current findings is that the articular surface of the medial aspect of the fifth metatarsal at the 4-5 IM joint was noted to be flat as opposed to concave or convex. This may be important clinically during open reduction and internal fixation of a fracture in this area. Little is published on the rotation of the proximal tuberosity fragment in relation to the shaft. Recently, biomechanical studies have demonstrated that larger-diameter screws have better fatigue properties and thus may be biomechanically superior for percutaneous fifth metatarsal fixation. 8,15 Larger screws, however, have increased insertion torque and may rotate the proximal fracture fragment. 11 The current study finds that if larger screws cause rotation of the proximal fragment, this may lead to a malunion of the joint surface. The clinical implications of this are an area of future proposed research.
The bony anatomy of the fifth metatarsal is well described, and numerous studies are available to help avoid pitfalls of proximal fifth metatarsal fracture fixation. Ebraheim et al demonstrated that the fifth metatarsal is bowed laterally on the anteroposterior (AP) radiographic view and gave insight into the geometry of the medullary canal. 5 A cadaver study of the fifth metatarsal estimated the average canal width to be 4.1± 0.9 mm in the AP dimension view and 5.3 ± 1.1 mm in the lateral dimension view at the apex of this curvature. 20 A separate computed tomography analysis measured the average fifth metatarsal length in the AP view at about 71.4 ± 6.1 mm and in the lateral view at about 70.4 ± 6.0 mm. The authors also measured the distance from the apex of the curvature to base of the fifth metatarsal to be 42.6 ± 5.8 mm in the AP view and 40.4 ± 6.4 mm in the lateral view. 3 These studies are immensely helpful in providing information regarding optimal screw length and diameter when considering operative fixation of proximal fifth metatarsal fractures.
However, details of the 4-5 IM joint in the literature are limited. Sarafian notes in his textbook on the functional anatomy of the foot and ankle that “the lateral surface [of the fourth metatarsal] gives support to a triangular articular surface (base dorsal, apex plantar), occupying the posterosuperior segment of the surface and articulating with the fifth metatarsal.” 19 He also notes that on the fifth metatarsal, “the medial surface bears an oval or triangular surface articulating with the base of the fourth metatarsal.” 19 The current study supports the findings described by Sarafian that the lateral fourth proximal intermetatarsal joint articular surface has a triangular shape. This was seen in 80% of our specimens. However, all the triangular variants demonstrated a vertical proximal base and plantar-distal directed apex with more fibrous tissue resting above the cartilage as one assessed the joint more distally. About 15% of our specimens had a square-shaped articular surface and only 5% had an oval one. We were also able to redemonstrate that the medial surface of the medial fifth proximal intermetatarsal joint shape was both triangular (seen in 25% of our specimens) and oval (seen in 75% of our specimens). The significance of this geometric characterization is in the fact that the articular cartilage tapers off in most specimens and becomes more fibrous distally.
Singh described the facet on the lateral side of the proximal fourth metatarsal as being a “concave and somewhat triangular facet. It is always present and varies only slightly in size and shape.” Regarding the facet on the fifth metatarsal, he describes it as “constant in size and shape.” 23 Contrary to Singh, we found that the articular surfaces in both the fourth and fifth metatarsals were mostly flat and not rounded. This observation is noteworthy when considering that rotational malreduction of a flat joint causes more articular step off than that of a rounded joint.
Meta-diaphyseal fractures of the fifth metatarsal (also known as the Jones fractures or zone 2 fractures) involve extension of the fracture into the metaphyseal-diaphyseal junction of the fifth metatarsal. 18 We measured the length in the medial fifth metatarsal proximal intermetatarsal articular surface and found that it is a mean of 9.5 ± 1.2 mm in length starting from the ridge between the fifth tarsometatarsal joint and intermetatarsal joint. Knowledge of the length of the articular surface is relevant to recognizing radiographically when a proximal fifth metatarsal fracture extends intraarticularly, and correlating these results clinically may be an area of future research. It is also relevant in the fixation of proximal fifth metatarsal fractures if one elects to use a bicortical screw fixation method as this aids in planning the screw trajectory to avoid intra-articular placement of the screw. 10,13,17
Additionally, there are biomechanical implications to the findings of this study. It is thought that the enhanced mobility of the lateral column of the foot plays a role in accommodating uneven surfaces during gait. 14 Ouzounian et al studied the kinematics of various metatarsals and found that the fourth and fifth tarsometatarsal joints have the most motion in the sagittal and rotational plane. 4,16 Knowledge of the articular surface area and configuration of 4-5 IM joints may aid in a more accurate biomechanical model and may be an area of future research. An examination of the articular surface area of the 4-5 IM joint demonstrated that the joint has both fibrous and articular components. It is also noted that the lateral fourth proximal metatarsal joint was substantially larger in the articular surface area than the medial fifth metatarsal joint (92.29 ± 24.68 mm2 vs 68.7 ± 17.5 mm2; P < .001). This difference in the articular surface area supports the biomechanical notion that the smaller articular surface of the fifth metatarsal glides over the more stationary, and larger articular surface of fourth metatarsal.
The current study has several limitations. First, this was a cadaver study with a relatively small sample size. Second, the articular surface was not perfectly flat and was projected onto a flat digital image. The accuracy of this image-based measurement technique has not been quantified and is an area of possible future research.
Conclusion
This study supports the notion that the 4-5 IM joint is not completely articular and has both fibrous and articular components. The clinical significance of this study is that it quantifies the articular surface area and shape. This information may be useful in understanding fifth metatarsal fracture extension into the articular surface and inform implant design and instrumentation placement in order to minimize articular damage.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420975709 - Anatomy of the Intermetatarsal Facets of the Fourth and Fifth Metatarsals
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420975709 for Anatomy of the Intermetatarsal Facets of the Fourth and Fifth Metatarsals by Mossub Qatu, George Borrelli, Christopher Traynor, Joseph Weistroffer and James Jastifer in Foot & Ankle Orthopaedics
Footnotes
Ethics Statement
Ethical approval for this study was waived by Western Michigan University School of Medicine Institutional Review Board because no protected health information was to be accessed in this cadaveric study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.