
Abstract
Background:
There is a potential role for tranexamic acid (TXA) use in foot and ankle procedures; however, the benefits of this intervention have not been fully elucidated. The purpose of this study was to explore the safety, outcomes, and medical complication profile of the use of intravenous TXA in patients undergoing foot and ankle surgery.
Methods:
A prospective study with retrospective review of 241 patients undergoing elective and traumatic foot and ankle procedures was performed. One gram of intravenous (IV) TXA was administered prior to incision. Patients were followed and evaluated for medical comorbidities, intraoperative blood loss, wound complication, superficial and deep infections, hematoma formation, medical complications, 30-day hospital readmission rate, and return visits to the emergency department or urgent care setting prior to first postoperative visit. Descriptive statistics were used for subgroup analysis. Mean postoperative follow-up was 4.5 months.
Results:
Estimated blood loss in all cases was less than 20 mL. There was 1 case of superficial cellulitis (1/241, 0.4%), 1 deep infection after Achilles tendon repair (1/241, 0.4%), 4 cases of delayed wound healing (4/241, 1.6%), 1 instance of deep vein thrombosis (1/241, 0.4%), and 2 cases of postoperative pulmonary embolism (2/241, 0.8%). There were no instances of postoperative hematoma formation. There were no additional recorded thromboembolic events. There were no adverse drug reactions. There were no 30-day hospital readmissions or return visits to the emergency department or urgent care setting before the first postoperative visit. In a subgroup analysis, there was no significant difference in wound complications or infections between nondiabetics and diabetics (P > .05) and traumatic and nontraumatic cases (P > .05).
Conclusions:
The use of IV TXA in foot and ankle surgeries was associated with low risk of wound complications, infections, hematoma formation, thromboembolic events, and overall complication rates with minimal side effect profile. Perioperative tranexamic acid use may prove to be beneficial in foot and ankle surgery patients but especially in higher-risk patients such as those with diabetes, trauma, and those that are immunocompromised.
Level of Evidence:
Level IV, case series.
Introduction
Tranexamic acid is an anti-fibrinolytic agent that competitively inhibits a lysine-binding site of plasminogen. This inhibits the conversion of plasminogen to the active fibrinolytic enzyme, plasmin, thus stabilizing blood clots 16 and reducing bleeding. TXA has become a commonly used agent to reduce blood loss in trauma, cardiac, and orthopedic procedures and has been shown in numerous randomized controlled trials to reduce total blood loss, wound complications, postoperative infections, blood transfusion rates, and minimize postoperative pain. 10,14,17,19,26,30,32 Additionally, large-scale database studies have demonstrated a favorable side effect profile with TXA use and found no significant increased complication risk even when TXA was administered to patients with relative contraindications. 2,13,15,27
TXA is widely used throughout multiple subspecialties of orthopedic surgery to minimize total blood loss, postoperative pain, infection rates, hematoma formation, and delayed wound healing. 10,14,17,19,26,30,32 Despite a low incidence of all-cause mortality, complications, and the use of tourniquets, the risk of postoperative bleeding after foot and ankle procedures is associated with an increased risk of infection, hematoma formation, and overall wound complications. 1,5,12,22 Given these risks, the use of TXA during the intraoperative period could play a valuable role in foot and ankle surgery. Additionally, the average cost of 1 g of IV TXA is US$25. Nevertheless, there is a paucity of literature addressing the use of TXA in all foot and ankle procedures.
What is known and understood about TXA use in other orthopedic subspecialties has not yet been validated in foot and ankle surgery. Therefore, the purpose of this study was to explore the safety, outcomes, and medical complication profile of the use of intravenous TXA in patients undergoing outpatient foot and ankle procedures. It was our hypothesis that the use of TXA in foot and ankle procedures would be associated with a decreased incidence of postoperative wound complications and infections with a low risk of thromboembolic events and adverse medication-related outcomes.
Methods
A prospective study with retrospective review was performed on 241 consecutive patients undergoing foot and ankle procedures between December 2019 to August 2020 who were treated with perioperative TXA. Inclusion criteria included patients who were greater than 18 years of age and having a traumatic, infectious, or elective foot and ankle procedure. Exclusion criteria included those who could not have TXA due to medical contraindications, including seizure history, severe renal disease (creatinine clearance <30 mL/min), bleeding disorders/coagulopathy, pregnancy, massive bleeding in the upper urinary tract (risk of ureter obstruction due to thrombosis), or acute thromboembolic disease (deep vein thrombosis [DVT], pulmonary embolism, myocardial infarction, cerebrovascular accident). Mean postoperative follow-up was 4.5 months (range: 6 weeks-9 months).
Operative Details
Foot and ankle procedures of the forefoot, midfoot, and hindfoot included for analysis are described in Table 1. One gram of IV TXA was administered approximately 10 minutes before incision. An ankle or thigh tourniquet was used in all patients at 250 to 300 mm Hg. After surgery during the nonweightbearing period, all patients were on Aspirin 325 mg daily for DVT prophylaxis. All preoperative blood thinners were continued in the immediate postoperative period based on patients medication profile.
Frequency of Medical Comorbidities for Operative Patients.

Data Collection and Analysis
After institutional review board approval was granted, a consecutive list of all foot and ankle procedures was tracked by the primary surgeons. Patients were followed and evaluated for baseline demographics, blood loss, wound complication, postoperative infection rates, hematoma formation, medical complications, 30-day hospital readmissions, and return visits to the emergency department or urgent care setting before the first postoperative visit. Descriptive statistics were used to do subgroup analysis.
Results
Intraoperative estimated blood loss in all cases was less than 20 mL. A tourniquet was used in 233/241 (97%) cases. One patient, who was diabetic with hemoglobin A1c > 7, had superficial cellulitis at their 2-week follow-up, which resolved with 2 weeks of oral antibiotics. There was 1 deep operative site infection in a patient following primary Achilles tendon repair, which required return to the emergency room at 3 weeks postoperatively in addition to irrigation and debridement, which healed with 6 weeks of IV antibiotics and no further intervention. There were 4 cases of delayed wound healing, which followed pilon fracture open reduction internal fixation, ankle fusion after open talus fracture, revision lateral ligament reconstruction with allograft reconstruction, and Kidner procedure. All of these cases were superficial wounds involving approximately less than 10% of the length of the incision, which healed uneventfully within 6 weeks with local wound care. There were no other wound healing complications or instances of hematoma formation. There was 1 recorded DVT at 4 weeks following surgery, which occurred in the soleal vein, and 2 pulmonary emboli, 1 occurring at 5 weeks following surgery. There were no myocardial infarction or cerebrovascular accident events. There were no adverse drug reactions. There were no 30-day hospital readmissions or return visits to the emergency department or urgent care before the first postoperative visit.
In a subgroup analysis, we did not find a significant difference in wound complications or infections between nondiabetics and diabetics and traumatic and nontraumatic cases with the numbers available; however we did not perform a power analysis so it is unclear the statistical strength of these findings.
Discussion
TXA has been shown in numerous randomized controlled trials to be a safe and effective blood-saving technique for minimizing blood loss, wound complications, transfusion rates, and even improved postoperative pain after orthopedic surgery. 10,14,19,30,32 In total joint arthroplasty, the advent of TXA has resulted in significant reductions in intraoperative blood loss, blood transfusion rate, and hospital length of stay without increased risk of thromboembolic events when used in oral, topical, or intravenous form. 21,32 Additionally, Yazdi et al 33 asserted that patients undergoing primary total joint arthroplasty who received TXA are at significantly lower odds of developing periprosthetic joint infection.
Similarly, the use of TXA in orthopedic arthroscopic procedures has yielded favorable results. 18,23 The use of IV TXA during anterior cruciate ligament reconstruction resulted in 90 mL reduction in postoperative drain output, improved visual analog scale pain scores, and lower postoperative hemarthrosis grades compared with placebo. 18 Furthermore, the use of IV TXA in shoulder arthroscopy for rotator cuff repair has resulted in reduced postoperative pain levels and analgesic use in addition to improvements in surgeons’ subjective visual clarity scores. 23 Additionally, Yang et al 31 demonstrated that the use of IV TXA in spinal surgery resulted in significant reductions of blood loss and fewer blood transfusions without risk of DVT or thromboembolic events compared to control.
Despite having a more established presence in other orthopedic subspecialties, complete understanding of the role of TXA in foot and ankle surgery has not yet been elucidated. In a retrospective review of 50 patients undergoing TAR, 25 patients who received intraoperative IV TXA had a significantly lower drain output (71.6 mL vs 200.2, P < .0001) and change in pre- to postoperative hemoglobin level (0.4 vs 1.5 g/dL, P = .01) compared to the 25 patients who did not receive intraoperative TXA. 25 Additionally, there was a lower wound complication rate (8% vs 20%, P = .114) in patients treated with TXA vs nontreated patients; however, this was not statistically significant. 25 In a randomized controlled trial comparing outcomes after TXA vs non-TXA treatment for 90 consecutive calcaneal fractures, the TXA-treated cohort had a significantly reduced incidence of wound complications (7.3% vs 23.8%, P = .036) without a significant difference in thromboembolic events or adverse drug reactions between the 2 groups.
Our study is the first to examine the potential role of preoperative TXA in all foot and ankle procedures, with results indicating minimal postoperative wound complications, infections, hematoma formation, and a safe medical side effect profile throughout a mean postoperative follow-up of 4.5 months.
One of the main concerns of using TXA is the risk of thromboembolic event. The rate of DVT in the present study was 0.4%, which is consistent with previous literature of DVT rate in foot and ankle procedures. 9,34 In addition, in the present study, the rate of pulmonary embolisms was 0.8%, and there were no recorded myocardial infarction, cerebrovascular accident, or other thromboembolic events throughout the follow-up. Thus, the present study supports the existing literature highlighting the favorable side effect profile of TXA. 2,13,15,27 Overall, 239 of the 241 procedures were performed as outpatient surgery, whereas the remaining 2 patients underwent irrigation and debridement for diabetic lower extremity infections but were previously admitted in the inpatient setting because of diabetic complications. Total ankle replacement and diabetic infections were performed on an outpatient basis per the primary surgeons protocols (Table 2). Of this cohort, there were no 30-day hospital readmissions or return visits to the emergency department or urgent care setting prior to their first postoperative visit at 2 weeks. All diabetic cases had close follow-up with Infectious Disease physicians for antibiotic management and IV antibiotics as needed.
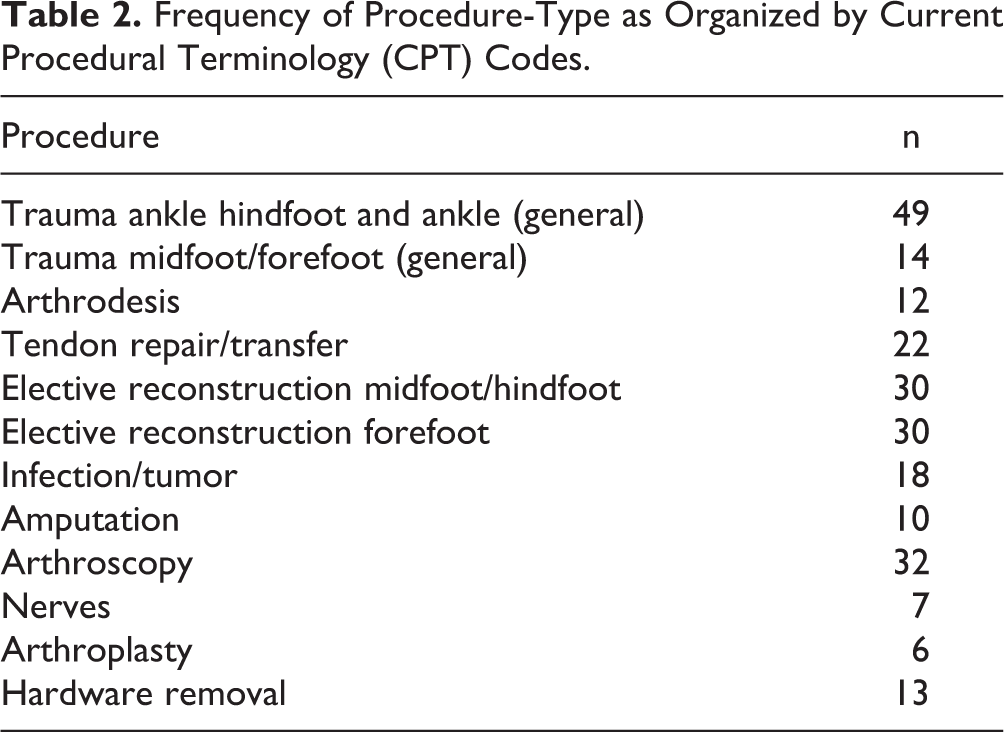
Frequency of Procedure-Type as Organized by Current Procedural Terminology (CPT) Codes.
The low rate of infection with TXA use in the present study is significantly lower than what is reported in the previous foot and ankle literature, which is up to 5% in various types of ankle procedures and as high as 20% in Achilles tendon repairs. 6 -8,24 Although there was 1 deep infection in an Achilles repair surgery requiring irrigation and debridement (0.4%, 1/241) and 1 case of uncomplicated cellulitis (0.4%, 1/241), the infectious complication rate of 0.8% (2/241) in the present study is substantially lower than that represented in prior foot and ankle literature. The rate of delayed wound healing in the present study was 1.6% (4/241); however, all of these wounds were less than 10% the length of the incisions, none of them required reoperation, and all healed within 6 weeks with local wound care. Additionally, we found no statistically significant difference between groups who are at higher risk for wound complications, including those with diabetes and traumatic injuries compared with those undergoing elective foot and ankle procedures. This finding suggests that TXA could prove especially valuable for those patients at higher risk for wound complications and infection undergoing foot and ankle surgery. Nevertheless, more research is needed to further elucidate these findings.
In our study, we used IV administration of TXA. Previous studies in total joint arthroplasty have shown no significant differences between oral, intra-articular, and IV administration of the drug in terms of transfusion rates, blood loss, drain output, and thromboembolic complications. 3,11,20,28,29 Combined administration of IV and topical TXA was associated with lower total blood loss, drainage volume, and maximum hemoglobin drop in primary knee arthroplasty. Interestingly, total blood loss was less in patients without a tourniquet. 35 Additionally, the low cost of a single dose of IV TXA makes for the cost-benefit ratio to be favorable. Complications from orthopedic surgery are burdensome financially. Avilucea et al showed for complications after ankle fractures the total cost increases more than $20 000 per case. 4 Based on our initial data, we showed a lower infection rate in our trauma cases compared with historical controls. We understand the limitation that there is no control in the present study; however, these data provide valuable insight for additional studies as the cost benefit in these cases may prove to be favorable especially with a cost of $25 per 1 g of IV TXA. Although our study shows promising outcomes with IV administration of TXA, further studies are necessary in order to provide recommendations on the safest and most efficacious regimen of administration during foot and ankle procedures.
Limitations
The findings of this study must be viewed with respect to its limitations. First, this was a prospective study with a retrospective review of outcomes. The inherent biases associated with retrospective study designs are substantial; however, because we evaluated consecutively treated patients undergoing all foot and ankle procedures, we feel that the retrospective nature of the present study does not discredit the findings. Second, the lack of control group in the present study could serve to minimize the potential conclusions and causality of outcomes related to TXA use demonstrated in this study. Therefore, it is difficult to definitively determine if administration of TXA played a role in our study outcomes. However, the main purpose of this study was to demonstrate the safety profile of TXA use in all foot and ankle surgery while highlighting an equivalent to lower complication rates compared to historical controls in previous studies, which we were able to demonstrate. Additionally, we were able to show a very low and similar thromboembolic event rate compared with historical controls of these events in foot and ankle surgery, thus minimizing one of the most common fears of utilizing IV TXA. Third, the presence of nonblinded observers during postoperative wound assessment facilitates researcher bias and is another significant limitation in the present study. Fourth, the average length of follow-up of the present study was 4.5 months. However, outcomes such as postoperative wound complications, infection, hematoma formation, thromboembolic event, hospital readmissions, and other complications most frequently occur within this period of time; therefore, we did not feel that longer follow-up periods were necessary in order to assess the value, safety, and efficacy of the use of TXA in these patients. Additionally, we did not perform a true cost-benefit analysis as we were lacking a control group. We understand the limitations of using historical controls vs a control group in this study; however, our initial data suggest that infections and wound complication rates may be lowered with the use of TXA in foot and ankle surgery. These data are similar to reported outcomes in other orthopedic specialties including total joints, spine, and sports medicine. Therefore, we believe that given the very low cost of IV TXA combined with the low risk profile and high potential upside, the cost-benefit at this time appears very favorable in foot and ankle surgery. However, more research needs to be done in this area to determine the true cost-benefit. Lastly, we did not perform a power analysis and thus any statistical measurements of equivalency are inconclusive.
Conclusions
In conclusion, the use of preoperative bolus IV TXA in foot and ankle surgeries was associated with low risk of wound complications, infections, hematoma formation, thromboembolic events, and overall complication rates with minimal side effect profile. This may prove to be beneficial in foot and ankle surgery patients but especially in higher-risk patients such as those with diabetes, trauma, and those that are immunocompromised. A future comparative study on TXA use in all foot and ankle procedures is warranted to determine the true effect of TXA on blood-related and wound healing outcomes.
Supplemental Material
Supplemental Material, FAO975419-ICMJE - Tranexamic Acid Use in Foot and Ankle Surgery
Supplemental Material, FAO975419-ICMJE for Tranexamic Acid Use in Foot and Ankle Surgery by William L. Johns, Kempland C. Walley, Raees Seedat, Benjamin Jackson, Karim Boukhemis and Tyler Gonzalez in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from PRISMA Health Institutional Review Board (Pro00098968).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.