
Abstract
Background:
Stabilization methods for distal tibiofibular syndesmotic injuries present risk of malreduction. We compared reduction accuracy and biomechanical properties of a new syndesmotic reduction and stabilization technique using 2 suture buttons placed through a sagittal tunnel in the fibula and across the tibia just proximal to the incisura with those of the conventional method.
Methods:
Syndesmotic injury was created in 18 fresh-frozen cadaveric lower leg specimens. Nine ankles were repaired with the conventional method and 9 with the new technique. Reduction for the conventional method was performed using thumb pressure under direct visualization and for the new method by tightening both suture buttons passed through the fibular and tibial tunnels. Computed tomography was used to assess reduction accuracy. Torsional resistance, fibular rotation, and fibular translation were evaluated during biomechanical testing.
Results:
The new technique showed less lateral translation of the fibula on CT measurements after reduction (0.06 ± 0.06 mm) than the conventional method (0.26 ± 0.31 mm), P = .02. The new technique produced less fibular rotation during internal rotation after 0 cycles (new –2.4 ± 1.4 degrees; conventional –5.0 ± 1.2 degrees, P = .001), 100 cycles (new –2.1 ± 1.9 degrees; conventional –4.6 ± 1.4 degrees, P = .01), and 500 cycles (new –2.2 ± 1.6 degrees; conventional –5.3 ± 2.5 degrees, P = .01) and during external rotation after 100 cycles (new 3.9 ± 3.3 degrees; conventional 5.9 ± 3.5 degrees, P = .02) and 500 cycles (new 3.3 ± 3.2 degrees; conventional 6.3 ± 2.6 degrees, P = .03). Fixation failed in 3 specimens.
Conclusion:
The new syndesmotic reduction and fixation technique resulted in more accurate reduction of the fibula in the tibial incisura in the coronal plane and better rotational stability compared with the conventional method.
Clinical Relevance:
This new technique of syndesmosis reduction and stabilization may be a reliable alternative to current methods.
Introduction
Ankle fractures are associated with syndesmotic injury in 10% to 43% of cases. 3,17 Disruption of the ankle mortise can alter tibiotalar joint mechanics and contact pressures. These alterations can predispose the ankle to post-traumatic arthritis. 14 Several reduction and stabilization methods have been described for syndesmotic disruptions, including screw fixation, the use of suture buttons, and anatomic repair of the anterior-inferior tibiofibular ligament (AITFL) and posterior-inferior tibiofibular ligament (PITFL).
Current syndesmotic stabilization methods have many pitfalls. Many, if not most, syndesmotic injuries are malreduced with operative treatment. 4 Positioning of clamps away from the natural axis of the syndesmosis is associated with malreduction. 13 Strategies to improve reduction include open reduction and use of intraoperative 3-dimensional fluoroscopy and computed tomography.
Suture button fixation has less torsional strength, 3 produces similar functional outcomes, and poses less risk of malreduction compared with syndesmotic screw fixation. 11 Single– or double–suture button constructs have rotational stability similar to that of screw fixation but do not restore preinjury rotational stability nor syndesmotic anatomic relationships. 2 Similar results have been reported after screw fixation, PITFL repair, or PITFL and deltoid ligament repair. 17
An ideal syndesmotic reduction and stabilization strategy should replicate the orientation and stabilizing forces of the syndesmotic ligaments. Our goal was to evaluate a new technique for reduction and stabilization of the distal tibiofibular syndesmosis. This technique changes the orientation of the suture buttons to replicate the AITFL and PITFL to improve stability and minimize risk of malreduction. We hypothesized that the new technique would restore the anatomic position of the distal tibiofibular syndesmosis and provide greater rotational stability and less risk of malreduction compared with the conventional double–suture button syndesmosis stabilization method.
Materials and Methods
Specimen Preparation and Imaging
Institutional review board processes were completed to use human cadaveric specimens for biomechanical testing. We used 18 fresh-frozen cadaveric lower leg specimens, which were disarticulated through the knee to the toes, without previous injuries or surgeries, and with intact proximal tibiofibular articulations.
Each specimen was imaged with fine-cut computed tomography (CT) with 1-mm slices at the ankle joint to evaluate the alignment of the distal tibiofibular syndesmosis before simulated injury and after repair. Previously validated measurements of the syndesmosis were obtained 10 mm proximal to the tibial plafond to determine the quality of syndesmotic reduction after repair (Table 1, Figure 1). 1,12,13
Changes in Distal Tibiofibular Syndesmosis Measurements From Preinjury to After Reduction, by Stabilization Method.a

a Each value represents the difference between the measurement taken on the same specimen before injury and after reduction and internal fixation.
b Measure A = distance between the most anterior point of the incisura and the nearest most anterior point of the fibula. Measure B = distance between the most posterior point of the incisura and the nearest most posterior point of the fibula. Measure = distance between a line perpendicular to the center of the syndesmosis and the anterior fibula edge. Measure E = distance between a line perpendicular to the center of the syndesmosis and the posterior fibula edge. Angle 1 = rotation of the fibula relative to a line parallel to the anterior and posterior edges of the incisura. Angle 2 = rotation at the level of the talar dome, between 2 lines along the talar sides of the 2 malleoli.
c Median (interquartile range) was used to compare the nonnormally distributed data, Mean and SD was also reported for ease of comparison.
d Negative values represent external rotation.

Axial computed tomography scans of a normal syndesmosis 10 mm proximal to the tibial plafond, used to measure rotation and medial-lateral translation (a, b, c), anterior posterior translation (d, e, f), and rotation (angles 1 and 2). Measure “a” represents the distance between the most anterior point of the incisura and the nearest most anterior point of the fibula. Measure “b” represents the distance between the most posterior point of the incisura and the nearest most posterior point of the fibula. Measure “c” represents the distance between the tibia and fibula in the middle of the incisura. Measure “d” represents the distance between a line perpendicular to the center of the syndesmosis and the anterior fibula edge. Measure “e” represents the distance between a line perpendicular to the center of the syndesmosis and the posterior fibula edge. Angle 1 measures rotation of the fibula relative to a line parallel to the anterior and posterior edges of the incisura. Angle 2 measures rotation at the level of the talar dome, between 2 lines along the talar sides of the 2 malleoli.
Soft-tissue dissection was performed to expose the deltoid ligament, syndesmotic ligaments, anterior and posterior tibiotalar joint capsule, and interosseous membrane. The simulated syndesmotic disruption was created by sectioning the AITFL, interosseous tibiofibular ligament, PITFL, and interosseous membrane up to 6 cm proximal to the tibial plafond to destabilize the syndesmosis. Sectioning was performed with a scalpel. The superficial and deep deltoid ligaments were sectioned at their medial malleolar origin to simulate a Lauge-Hansen supination, external rotation type IV injury. 9 The ankle joint capsule was left intact. The fibula was also left intact to simulate anatomic reduction of the fibula with plate fixation. 4
Operative Techniques
Specimens were separated into 2 groups that were destabilized as described and then repaired with the conventional method (n = 9) or the new technique (n = 9).
Conventional Method
The conventional method used a construct with 2 divergent suture buttons (TightRope; Arthrex Inc, Naples, FL) placed through the fibula and tibia parallel to the joint line. Syndesmotic reduction was performed under direct visualization. The fibula was held in position with thumb pressure until temporary stabilization was achieved with a single Kirschner wire. Double–suture button constructs were placed. Proximal and distal tunnels were made on the lateral cortex of the fibula. Each hole was drilled parallel to the joint line and divergent to the transmalleolar axis.
New Technique
The new stabilization technique used 2 suture buttons (TightRope) placed through the fibula and routed anterior and posterior to the fibula into the tibia tunnels at the level of the physeal scar along the same plane of the native AITFL and PITFL. A sagittal fibular tunnel was created in line with the most proximal point of the anterior and posterior ridges of the fibular incisura (Figure 2). Two tibial tunnels were created anterior and posterior to the fibula, in line with the fibular tunnel, at the proximal attachments of the AITFL and PITFL, respectively. The tunnels were drilled with a trajectory parallel to the joint line, exiting at the anterior and posterior thirds of the medial tibia distal metaphysis. With the syndesmosis left unreduced, a suture button was passed from posterior to anterior through the fibular tunnel and from lateral to medial through the anterior tibia tunnel, a second suture button was passed through the fibular tunnel in the opposite direction (anterior to posterior) and through the posterior tibia tunnel. The medial tibial periosteum was cleared to allow suture buttons to lie directly against cortical bone. Finally, we manually tightened both suture button constructs simultaneously to reduce the syndesmosis and center the fibula in the incisura (Figure 2).

(A) Illustration of a new syndesmotic fixation technique. At the level of the physeal scar, 2 suture buttons are passed through the fibula and the respective tibial tunnels. The syndesmosis is reduced when the implants are tightened. (B) Illustration of a conventional method of syndesmotic fixation. Parallel suture buttons are placed 1.5 cm proximal to the joint line divergent to the mechanical axis of the ankle. 1, tibialis anterior tendon; 2, extensor hallucis longus tendon; 3, extensor digitorum longus tendon; 4, peroneus tertius; 5, posterior tibialis tendon; 6, flexor digitorum longus tendon; 7, flexor hallucis longus tendon; 8, peroneus brevis muscle; 9, peroneus longus tendon; 10, Achilles tendon; 11, tibia; 12, fibula; 13, suture button implant; 14, talus; and 15, tibial neurovascular structures.
Biomechanical Testing
Specimens subjected to syndesmotic repair using the new technique or conventional method underwent biomechanical testing to obtain torque, rotational and translational measurements.
Specimens were mounted to a servohydraulic testing machine (MTS 858 Mini Bionix; MTS Systems Corp, Eden Prairie, MN) via a custom mounting jig. The foot was positioned in neutral plantarflexion and neutral rotation with respect to the tibia. Specimens were attached proximally with two 5-mm pins placed anterior to posterior through the tibia. Two 5-mm transverse pins were placed medial to lateral in the calcaneus distally to stabilize the heel on the testing machine platform. Two screws inserted through the anterior talar neck fixed the talus to the calcaneus to avoid confounding results by subtalar motion. Optotrak Certus sensors (NDI, Ontario, Canada) with an accuracy of up to 0.1 mm and resolution of 0.01 mm were attached to the tibia and fibula 8 cm proximal to the joint line to measure alignment.
Specimens were loaded axially to 750 Nm throughout testing. Specimens were cyclically loaded ±5 Nm at 0.5 Hz of internal and external rotation for 500 cycles. Testing was paused at 0, 100, and 500 cycles to assess torsional resistance, fibular rotation, and fibular translation within a physiologic range of motion. At these time points, the foot was first internally rotated to 10 degrees and then externally rotated to 15 degrees. Peak torque (in newton-meters) during these movements was measured with the servohydraulic testing machine. Fibular rotation (in degrees) and fibular translation (in mm) in relation to the tibia was measured with the Optotrak Certus.
Statistical Methods
All analyses were performed using SPSS, version 25, software (IBM Corp). P values <.05 were considered significant. For both quality of reduction and biomechanical analyses, we tested continuous variables for normality using skewness and kurtosis statistics. If either statistic was higher than an absolute value of 2.0, then the assumption was violated. Levene’s test for equality of variances was performed to check for the statistical assumption of homogeneity of variance. When both statistical assumptions were met, independent samples t tests were used to compare the groups.
Means and SDs are reported for the t-test analyses. When either statistical assumption was violated for an outcome, nonparametric Mann-Whitney U tests were used for between-subject comparisons. Medians and interquartile ranges are reported for the nonparametric analyses. Fisher exact tests were used to compare both groups on measure “c”. Frequencies and percentages are reported for the categorical analyses.
Results
Instrumentation Failure
During the initial 100 cycles, failure of instrumentation occurred in 3 constructs. One failure occurred in the conventional method group and 2 occurred in the new technique group. The 3 failures were associated with fractures through the fibular tunnel in 2 specimens and subsidence of the suture button construct in one during the 100-cycle biomechanical testing phase. The remaining ankles underwent measurements after 100 and 500 cycles without failure.
Reduction Accuracy
When comparing preoperative vs postoperative measurements, measure C differed less with the new technique (mean, 0.06 ± 0.06 mm) than with the conventional method (mean 0.26 ± 0.31 mm) (U = 17, P = 0.02). No significant differences between groups were found in any other comparison (Table 1).
Biomechanical Testing
We found significant differences between the conventional method and new technique for fibular internal rotation at 0 cycles (conventional –5.0 ± 1.2 degrees, new –2.4 ± 1.4 degrees, t(16) = –4.2, P = 0.001), 100 cycles (conventional –4.6 ± 1.4 degrees, new –2.1 ± 1.9 degrees, t(13) = –2.9, P = 0.01), and 500 cycles (conventional –5.3 ± 2.5 degrees; new –2.2 ± 1.6 degrees t(13) = –2.9, P = 0.01). For each of the t-test comparisons that demonstrated statistical significance, the new technique group had significantly smaller changes in alignment (Table 2). Using Mann-Whitney U tests, we found significant differences between the groups for external rotation after 100 cycles (conventional 5.9 ± 3.5 degrees; new 3.9 ± 3.3 degrees, U = 8.0, P = 0.02) and 500 cycles (conventional 6.3 ± 2.6 degrees; new 3.3 ± 3.2 degrees, U = 9.0, P = 0.03). In each instance, the new technique group demonstrated significantly less change in alignment than the conventional group. No other between-group comparisons were significantly different.
Biomechanical Propertiesa of Distal Tibiofibular Syndesmosis Repair, by Stabilization Method.
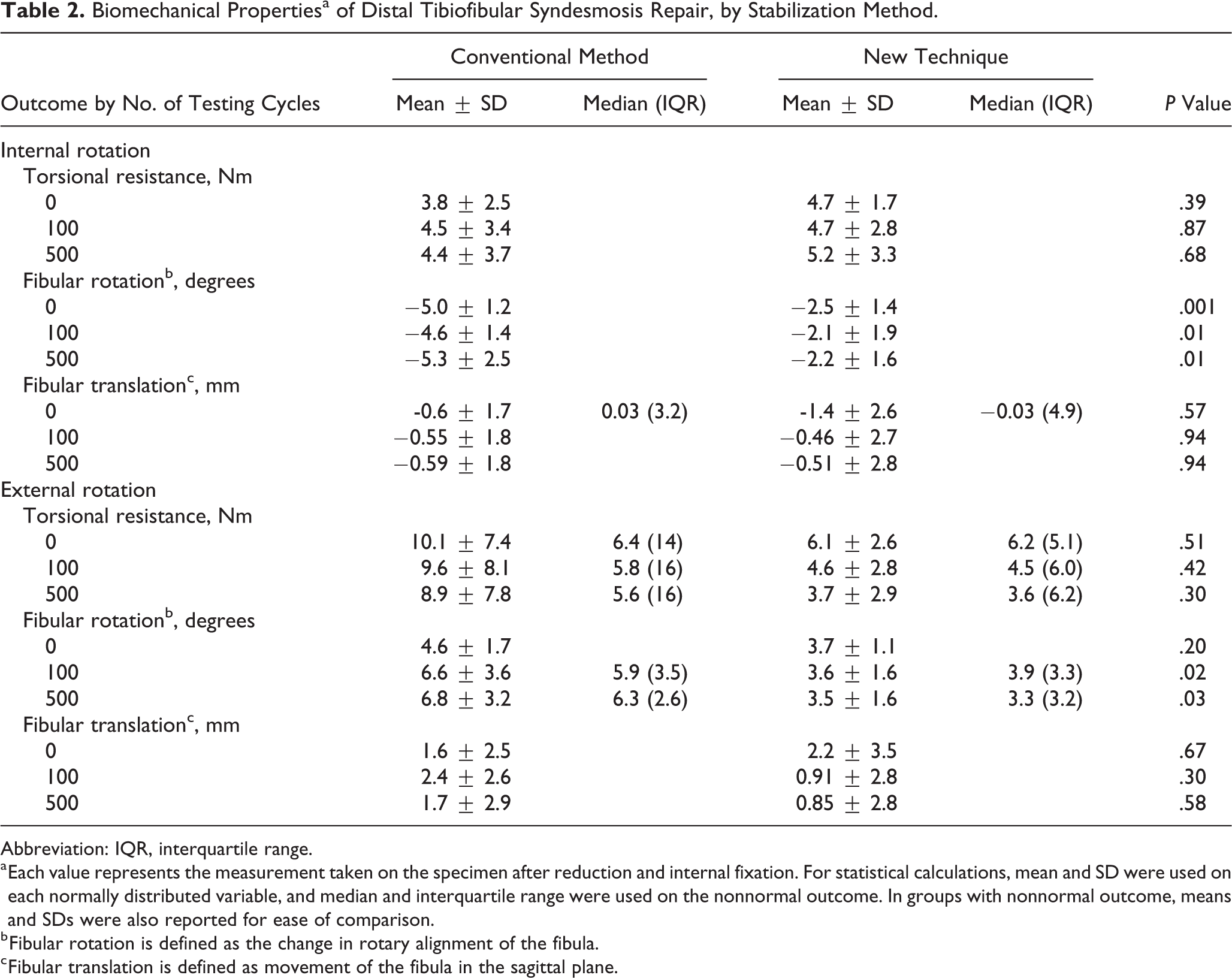
Abbreviation: IQR, interquartile range.
a Each value represents the measurement taken on the specimen after reduction and internal fixation. For statistical calculations, mean and SD were used on each normally distributed variable, and median and interquartile range were used on the nonnormal outcome. In groups with nonnormal outcome, means and SDs were also reported for ease of comparison.
b Fibular rotation is defined as the change in rotary alignment of the fibula.
c Fibular translation is defined as movement of the fibula in the sagittal plane.
Discussion
We present a new technique for syndesmosis reduction and fixation using 2 suture buttons placed anterior and posterior in the fibula, in line with the native AITFL and PITFL axes. This technique achieved more accurate reduction in the coronal plane and better rotational stability compared with the conventional method. The key feature and benefit of this technique is that it avoids performing reduction maneuvers prior to fixation.
Rigid syndesmotic fixation has been associated with higher risks of malreduction and the need for reoperation compared with fixation with suture button devices. 16 The use of suture buttons has become increasingly common to address syndesmotic disruptions because the buttons allow physiologic motion. 7 Clanton et al 2 compared stability of the syndesmosis after screw fixation, 1 suture button fixation, and 2 suture button fixation and found that none of the 3 methods restored stability similar to the preinjury state. Although flexible fixation restores syndesmotic coronal stability, excessive rotational and anterior-to-posterior translation is noted compared with screw fixation and the uninjured ankle.
Ligament reconstruction has also been explored as an alternative to flexible syndesmosis fixation. Teramoto et al 18 showed superior biomechanical stability of the syndesmosis when a suture button was placed in line with the native AITFL compared with divergent suture buttons. Notably, this construct was not an attempt to re-create the PITFL. Schottel et al 17 showed improved rotational stability after PITFL and deltoid ligament repair compared to transsyndesmotic screw fixation, but increased residual external rotation was present in all the constructs. Recent work by Goetz et al 5 found that flexible suture button fixation failed to restore axial and sagittal stability of the ankle and talus, whereas augmentation with AITFL and deep deltoid ligament repair restored rotational and translational stability to near normal levels. Our new technique showed improved fibular stability in the axial plane when the ankle was internally or externally rotated under load, resembling results after augmented repairs targeting the AITFL and deltoid ligament. 5 We believe that placement of the suture buttons anterior and posterior to the fibula provides greater rotational stability that it more closely matches the native AITFL and PITFL.
Malreduction of the syndesmosis is associated with poor outcomes. 15 Malreduction has been associated with clamp malposition, overcompression, and screw placement. 10,13 A cadaver study comparing 3 reduction techniques showed that direct visualization and thumb pressure resulted in greater contact area and joint force compared with the clamp and suture-button reduction techniques. 8 Compared with reduction of the distal tibiofibular syndesmosis under direct visualization and stabilization with 2 suture buttons through the transmalleolar axis, our technique reduced the syndesmosis to near anatomic coronal alignment. An average of only 0.06 mm of lateral translation was noted on postoperative CT scan measurements compared with preoperative values. In comparison, reduction with the conventional method resulted in 0.26 mm of fibular lateral translation compared with preoperatively. Although an average improvement of 0.20 mm in the coronal plane appears negligible, we find that any improvement in anatomical alignment is critical, if we take into account that syndesmotic diastasis resulting in 1 mm of lateral talar translation can decrease tibiotalar contact areas by 42%, change peak contact pressures, and predispose to development of tibiotalar joint arthritis. 6,14,19 An interesting finding is that postreduction images showed that the new method resulted in less fibular external rotation compared to the conventional method, but this finding did not reach statistical significance.
The new technique we describe may allow surgeons to better restore anatomical distal tibiofibular syndesmosis alignment without performing reduction maneuvers prior to fixation. In the setting of a fibula fracture, securing the suture buttons through the plate with the novel technique could be an alternative to avoid failures associated with fibular tunnel fractures. This technique could be also used in the setting of ligamentous disruptions without posterior malleolar fracture, in which direct repair of the PITFL by anatomic reduction and internal fixation of the posterior malleolus is impossible. The new double–suture button technique may provide more accurate coronal alignment and greater rotational stability compared with existing methods, with biomechanical advantages similar to those of direct syndesmotic ligamentous repair.
Our study has several strengths. It describes a new fixation technique for syndesmosis injuries. The technique was tested biomechanically using a cadaveric model, and reduction quality and construct strength were compared with those of a conventional suture button method. Weaknesses of our study include the small number of specimens in both groups. Bone quality was not tested and could differ among specimens. Additionally, we were unable to quantify how forcefully the syndesmosis was tightened with either stabilization method. Three implants sustained mechanical failure during biomechanical testing by fracture of the fibula through the suture button tunnel. Failures were likely related to poor bone quality and stress through the weakened fibula. To avoid this problem, we recommend securing the suture buttons to the fibular plate in the setting of a fracture. We did not perform biomechanical testing before and after fixation, so we are unable to compare these measures. As a cadaver study, generalizability to living patients is unknown. Our method approximates the anatomy of the native ligaments but does not recreate them. The suture buttons have little compliance, perhaps rendering the joint overly stiff with this method compared with the conventional double–suture button method.
Conclusions
The new method we describe for syndesmosis stabilization used 2 suture buttons to dynamically reduce the distal tibiofibular joint without direct reduction. The method reapproximated the native anatomy by orienting the suture buttons parallel to the native AITFL and PITFL. This technique resulted in more accurate postreduction coronal alignment compared with reduction with direct visualization and thumb pressure followed by internal fixation with a divergent double–suture button construct. In biomechanical testing, the new technique produced greater internal and external rotational stability under loading compared with the conventional method. Translation and ability to resist rotation were unchanged. For all other measures, the new method achieved reduction similar to the conventional method. This new technique of syndesmosis reduction and stabilization represents an alternative to current methods with improved reduction accomplished without direct manipulation of the fibula into the incisura but rather by orienting suture buttons to the anatomic landmarks of the torn anterior and posterior inferior tibiofibular ligaments.
Supplemental Material
Supplemental Material, FAO969140-ICMJE - Biomechanical Evaluation of a New Suture Button Technique for Reduction and Stabilization of the Distal Tibiofibular Syndesmosis
Supplemental Material, FAO969140-ICMJE for Biomechanical Evaluation of a New Suture Button Technique for Reduction and Stabilization of the Distal Tibiofibular Syndesmosis by Andres Eduardo O’Daly, R. Timothy Kreulen, Sorawut Thamyongkit, Alfred Pisano, Kitchai Luksameearunothai, Erik A. Hasenboehler, Melvin D. Helgeson and Babar Shafiq in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Institutional review board processes were completed to use human cadaveric specimens for biomechanical testing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Babar Shafiq, MD, reports grants and non-financial support from Arthrex, Inc, during the conduct of the study. ICMJE forms for all authors are available online.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and/or publication of this article: cadaver specimens and implants were donated by Arthrex through grant number ST946.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.