
Abstract
Background:
Patient-Reported Outcomes Measurement Information System (PROMIS) is a newly developed patient-reported outcome that has been validated for the general foot and ankle population and has been applied to a variety of specific foot and ankle procedures. However, there is little data regarding clinical outcomes of patients at a more intermediate subgroup level. Thus, our study utilized PROMIS to provide normative data on pathologic conditions of the foot and ankle and assess postoperative outcomes based on anatomical location.
Methods:
Preoperative and 1-year postoperative PROMIS Physical Function (PF) and Pain Interference (PI) surveys were prospectively collected from a cohort of patients undergoing a foot and ankle procedure at a tertiary medical center. The cohort was split into forefoot (n = 136), midfoot (n = 44), hindfoot (n = 109), and Achilles (n = 62) procedure groups. Paired-t tests were used to compare preoperative versus postoperative outcomes within operative groups, while a 1-way analysis of variance (ANOVA) was used to detect differences in PROMIS scores between anatomic subgroups.
Results:
Paired t tests indicated that all 4 operative groups had significantly improved PROMIS PF and PI scores preoperatively versus 1 year postoperatively (all P < .001). One-way ANOVA demonstrated that there were no differences in postoperative PROMIS PF and PI scores between anatomic subgroups. A majority of patients achieved the minimal clinically important difference level of improvement in PROMIS PF and PI scores following surgery.
Conclusions:
All 4 operative groups had improvement in physical function and pain outcomes. Additionally, there were no differences in physical function and pain outcomes between operative groups.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Foot and ankle disorders encompass a wide variety of pathologies that may result in increased pain and decreased physical function, ultimately leading to decreased quality of life and even disability. 11,13,21,27 Patients who do not respond to conservative therapies may require operative treatment. When evaluating the need for surgery preoperatively, it is important to utilize patient reported outcome, in addition to clinical and radiographic outcomes, to track postoperative improvement.
Patient-reported outcomes (PROs) have become an increasingly important aspect of patient care and are commonly used to assess operative outcomes within foot and ankle surgery. 15 -18 Examples of PROs include the Visual Analog Scale Foot and Ankle (VAS-FA), 22 the Lower Extremity Function Scale, 2 the American Orthopaedic Foot & Ankle Society (AOFAS) scale, 19 the Foot Function Index, 4 the Foot and Ankle Ability Measure, 20 and the Self-Reported Foot and Ankle Score. 7 However, many of these PROs are neither well validated nor reliable, making it difficult to compare clinical outcomes among different clinical research studies. 5
In recent years, the development of the Patient-Reported Outcomes Measurement Information System (PROMIS) by the National Institutes of Health has ameliorated several limitations of previous PROs, including standardization and generalizability. Through the use of computerized adaptive testing (CAT), PROMIS allows for a more objective assessment of clinical outcomes in patients as well as more standardization to facilitate better comparisons between patients, providers, and research studies. 5,6,23 PROMIS has been validated within orthopedic surgery 9 and was recently validated within foot and ankle surgery. 1,14,15
Anderson et al, 1 Ho et al, 14 and Hung et al 15 looked at all foot and ankle procedures to validate PROMIS for Foot & Ankle surgery. Since the validation of PROMIS at a high level within the field, numerous studies have applied it to specific foot and ankle procedures. 3,8,10,12,28 Although it is certainly useful to look at PROMIS outcomes at both a high level and a granular, procedure-specific level, it is important to evaluate PROMIS outcomes at an intermediary level, investigating possible differences between foot and ankle procedure subgroups. This study aimed to elucidate PROMIS outcomes for patients who underwent forefoot, midfoot, hindfoot, and Achilles procedures. The overall cohort was subsegmented into these anatomical subgroups to closely match the AOFAS clinical rating system, which divides pathologies into ankle-hindfoot, midfoot, hallux, and lesser toes. We also believe that it is important to subsegment the foot and ankle population into these anatomical subgroups because indications and treatment algorithms for procedures within each subgroup are more likely to be more similar than between subgroups. Consequently, we believe that subsegmenting foot and ankle procedures at this level can be useful in clinical decision making.
Currently, there is little normative patient-reported outcomes data regarding pathologies of the foot and ankle, stratified by anatomical location. The few studies that do report normative data do not provide postoperative outcomes. 24,26 Overall, the goal of this study was to contribute to the limited clinical outcomes data in the foot and ankle patient population as well as be the first study to compare PROMIS scores preoperatively and postoperatively between the main anatomical subgroups of the foot and ankle patient population.
Methods
After obtaining approval from the Northwestern Institutional Review board (STU00084014/00082417/00084030), we retrospectively reviewed a cohort of all patients who had undergone foot and ankle procedures at a tertiary academic center between August 2013 and November 2018 that had completed preoperative PROMIS Physical Function (PF) and Pain Interference (PI) CATs. The PF scale measures a patient’s self-reported capability to perform physical activities, with a higher PF score indicating higher physical function. The PI scale measures the impact of pain on daily life, with higher PI scores indicating higher pain levels. Ultimately, the PROMIS PF and PI scores were compared to a reference general population (mean score of 50 with a standard deviation of 10). 1
A total of 941 patients were initially included in the study, all of whom had completed at least 1 assessment of the preoperative PF and PI CATs. All eligible patients for this study were older than 18 years and had a minimum of 1-year postoperative follow-up for both PROMIS CATs. Patients with incomplete PROs were excluded. A total of 351 patients met these criteria and were therefore included in the final analysis. This main cohort was further split into 4 anatomical subgroups based on procedure type—forefoot (n = 136), midfoot (n = 44), hindfoot (n = 109), and Achilles (n = 62) (Figure 1). The most common procedures in the forefoot group included metatarsophalangeal fusion, hallux valgus correction, and hammertoe correction. The most common midfoot procedures included single-joint arthrodesis, multiple-joint arthrodesis, and Lisfranc fracture open reduction internal fixation. The most common hindfoot procedures included hindfoot/ankle arthrodesis, ligament reconstruction, and adult-acquired flatfoot reconstruction. The most common Achilles procedures included acute Achilles rupture repair, insertional Achilles reconstruction without graft, and insertional Achilles reconstruction with tendon transfer. Patients were also stratified by gender (male or female) and age (<45, 45-64, and ≥65 years) for analysis.

Patients included in analysis.
Of the 351 patients included in the study, 148 (42.2%) were male, 173 (49.3%) were female, and 30 (8.5%) did not specify. In addition, 261 (74.4%) were white, 40 (11.4%) were African American, 9 (2.6%) were Asian, 10 (2.8%) were of another race, and 31 (8.8%) preferred not to specify. The mean age of the cohort was 46.9 ± 14.6 years. The mean time to follow-up for the cohort was 22.1 ± 9.8 months (Table 1).
Demographics.

Statistical Analysis
The mean preoperative and postoperative PROMIS PF and PI scores were calculated for the forefoot, midfoot, hindfoot, and Achilles groups. Two-tailed t tests were conducted to determine whether postoperative PROMIS scores were statistically significantly improved from preoperative PROMIS scores. The change in scores postoperatively were also calculated for each subgroup. One-way analysis of variance (ANOVA) was used to determine whether changes in PROMIS scores were statistically significantly different between anatomic and age subgroups. A Tukey post hoc test was used to demonstrate the specific differences detected by the 1-way ANOVA. Mann-Whitney U tests were also conducted to detect differences between genders. An alpha level of 0.05 was used for all analyses.
To determine if the change in each respective PROMIS scale was clinically significant between baseline and postoperatively, we used the minimal clinically important difference (MCID) for PROMIS PF and PI. 14 MCID is the minimum clinical improvement required to determine operative success from the perspective of the patient. The MCID was defined as 0.5 SD of each preoperative PROMIS domain. Based on this method, MCID thresholds were calculated as an increase of 4.1 or greater in PROMIS PF for forefoot cohort, increase of 5.4 or greater for midfoot, increase of 3.9 or greater for hindfoot, and increase of 7.8 or greater for Achilles. Similarly, MCID thresholds for the PROMIS PI domain was calculated as a decrease in 3.6 or greater for forefoot, a decrease of 4.2 or greater in midfoot, a decrease of 3.4 or greater in hindfoot, and a decrease of 5.5 or greater in Achilles.
All statistical analysis was performed using SPSS software (version 25, IBM Corp, Armonk, NY).
Results
PROMIS Outcomes
All of the anatomical subgroups had significant preoperative to postoperative improvement in PROMIS PF scores (Table 2): 6.6 (95% confidence interval [CI] 4.3-7.9, P < .001) in the forefoot cohort, 9.0 (95% CI 5.3-12.7, P < .001) in the midfoot cohort, 4.8 (95% CI 2.9-6.7, P < .001) in the hindfoot cohort, and 11 (95% CI 6.4-15.6, P < .001) in the Achilles cohort. For the PROMIS PI domain, all anatomic subgroups also had significant preoperative to postoperative improvements (Table 3): –8.0 (95% CI −9.7 to – 6.3, P < .001) in the forefoot cohort, –9.1 (95% CI −11.7 to – 6.4, P < .001) in the midfoot cohort, –8.4 (95% CI −10.4 to – 6.3, P < .001) in the hindfoot cohort, and –14.2 (95% CI −17.1 to – 11.4, P < .001) in the Achilles cohort. One-way ANOVA found that there were no differences in postoperative PROMIS PF and PI scores between the cohorts. Furthermore, 1-way ANOVA of PROMIS PF and PI were both adequately powered.
PROMIS Physical Function (PF).

Abbreviations: PROMIS, patient-reported outcomes measurement information system.
Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Interference (PI).
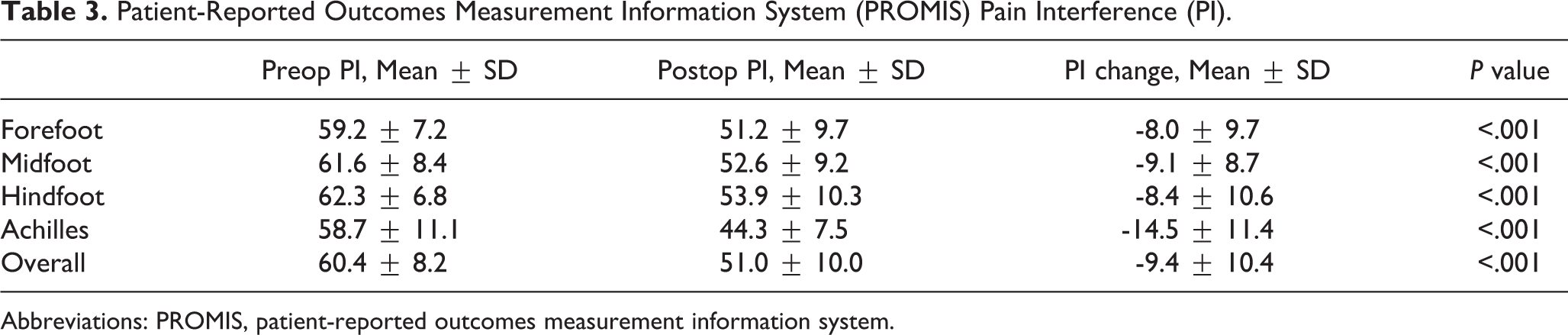
Abbreviations: PROMIS, patient-reported outcomes measurement information system.
Additional analysis of subgroups by gender (Table 4) found no significant differences in mean change in PROMIS PF and PI scores following foot and ankle surgery. Analysis of subgroups by age (Table 5) found no significant differences in PROMIS PF and PI scores following surgery with the exception of the <45-year forefoot cohort demonstrating a significantly larger increase in PF scores compared to the 45-64-year and ≥65-year forefoot cohort (mean change in PF = 11.0 in forefoot patients aged <45 years vs 5.1 and 0.8 in forefoot patients aged 45-64 and ≥65 years, respectively; P = .01, P < .001, respectively) Additionally, in the Achilles cohort, patients in the <45-year age group had a significantly larger decrease in PI scores compared to patients in the 45-64-year age group (–17.7 vs –7.3, P = .002).
Mean Change in PROMIS Scores ± SD Following Surgery by Gender.

Abbreviations: PROMIS, patient-reported outcomes measurement information system.
Mean Change in PROMIS Scores ± SD Following Surgery by Age Group.

aA Tukey post-hoc test was used to demonstrate the specific differences detected by the one-way ANOVA.
Abbreviations: PROMIS, patient-reported outcomes measurement information system.
Minimal Clinically Important Difference
A post hoc analysis was completed to predict the percentage of patients that met MCID for both PROMIS PF and PI (Table 6). Fifty-four percent in the forefoot cohort, 61% in the midfoot cohort, 56% in the hindfoot cohort, and 47% in the Achilles cohort postoperative PROMIS PF had successful operative outcomes using the MCID metric. Using the same method to look at PROMIS PI scores, 71% in the forefoot cohort, 74% in the midfoot cohort, 71% in the hindfoot cohort, and 75% in the Achilles cohort had successful postoperative outcomes.
Proportion of Patients Who Achieved MCID Improvement.

Abbreviations: MCID, minimal clinically important difference; PF, physical function; PI, pain interference.
Discussion
Foot and ankle pathologies can lead to significant disability and often require surgery following failure of more conservative medical treatment. 11,13,21,27 Legacy PROs such as the VAS-FA, AOFAS scale, and Foot Function Index are often used to measure outcomes following foot and ankle surgery. However, these PROs are often not well validated or reliable for the general foot and ankle patient population. The more recently developed PROMIS has addressed some of the issues with the legacy PROs, as it is validated, highly reliable, and can be applied to a more generalized foot and ankle patient population. 5,6,9 Currently, there exists literature to demonstrate clinical outcomes following a few specific foot and ankle procedures, 3,8,10,12,28 but there is little data about foot and ankle procedures at a more general level grouped by anatomy. The few studies that provide normative data 24,26 for the foot and ankle patient population do not look specifically at outcomes following foot and ankle surgery. Our study aimed to be the first to use PROMIS to provide normative data on pathologies of the foot and ankle and compare clinical outcomes following forefoot, midfoot, hindfoot, and Achilles surgeries.
Patient-reported outcomes are becoming increasingly important aspects of patient care within foot and ankle surgery. PROMIS has been shown to be a well-validated, highly reliable PRO that measures operative improvement within foot and ankle surgery. 1,14,15 In addition to being validated at a high level, PROMIS has also been used at a procedure-specific level to measure patient-reported operative improvement. Although procedure-specific data are certainly important, this article compared major anatomic subgroups of patients (forefoot, midfoot, hindfoot, and Achilles) to provide a general sense of operative improvement stratified by operative outcomes. There is a lack of studies that stratify foot and ankle patients by anatomic location. The commonly used AOFAS scale measures patient- and clinician-reported outcomes based on 4 subscales—ankle-hindfoot, midfoot, MTP-IP for the hallux, and MTP-IP for the lesser toes. Despite this anatomic subsegmentation, SooHoo et al 25 showed that the AOFAS scale has been shown to have poor construct validity compared with well-validated PROs like 36-Item Short Form Health Survey and PROMIS.
In our study, each anatomical subgroup of patients (forefoot, midfoot, hindfoot, and Achilles) made statistically significant improvements (P < .001) in PROMIS PF and PI scores postoperatively (Table 2 and 3), indicating that all cohorts do well postoperatively. One-way ANOVA found no statistically significant differences in outcomes between any of the cohorts, despite the study having adequate power to discern a difference. Stuber et al compared pain and function, as measured by VAS-FA scores, in patients with foot and ankle pathologies to normative control. 26 They found that VAS-FA scores for patients with forefoot, midfoot, and hindfoot pathologies differ from normative controls; however, VAS-FA scores did not differ between different pathology groups, which was consistent with the results from our study.
Regardless, it is useful to look at certain trends within each anatomical subgroup. In general, forefoot patients (PF: 49.7, PI: 51.2) returned closer to the population mean PROMIS PF and PI score of 50 postoperatively compared to the midfoot (PF: 47.2, PI:52.6) and hindfoot (PF 44.4, PI: 53.9) patients. Of note, the Achilles subgroup had the best postoperative PROMIS scores (PF: 57.3, PI: 44.3) and made the largest postoperative improvements but had the widest distribution of scores, indicating a large range of clinical outcomes. We theorize that the midfoot and hindfoot subgroups have limitation of motion postoperatively that compromises function that may account for the increased deviation from normal population. Further stratifying the anatomical subgroups by gender revealed no differences in clinical outcomes. Stratifying by age revealed that younger patients (aged <45 years) in the forefoot cohort tended to have larger improvements in functional outcomes but the same improvement in pain levels compared to the middle-age patients (aged 45-64 years) and elderly patients (aged ≥65 years). In the Achilles cohort, younger patients (aged <45 years) tended to have larger improvements in pain but the same improvement in functional outcomes compared with middle-age patients (aged 45-64 years).
Statistical improvements in PROMIS scores do not necessarily translate to better clinical outcomes. MCIDs were used to detect clinically meaningful changes in PROMIS scores. Overall, a majority of patients achieved MCID in all 4 anatomical subgroups in both the PROMIS PF and PI domains (Table 6). The exception is the Achilles PROMIS PF domain where only 47% of patients achieved MCID. Specifically, the percentage of patients who achieved PROMIS PF MCID is 54%, 61%, 56%, and 47% in the forefoot, midfoot, hindfoot, and Achilles groups, respectively. The percentage of patients who achieved PROMIS PI MCID is 71%, 74%, 71%, and 75% in the forefoot, midfoot, hindfoot, and Achilles groups, respectively. Thus, a significant proportion of patients who undergo foot and ankle surgery achieve clinically appreciable improvements in physical functioning and pain. By comparison, Ho et al 14 found that 34% of patients met MCID for PROMIS PF and 33% of patients met MCID for PROMIS PI, determined by the same methodology.
Strengths of this study include its novel contribution to clinical outcomes in foot and ankle surgery stratified by anatomical location rather specific type of pathology, which may not be generalizable. In addition, this study uses a well-validated and standardized PRO (PROMIS PF and PI) for measurement of clinical outcomes and demonstration of statistical and clinical improvement in patients. The study also had 1-year follow-up and a large enough cohort to conduct an adequately powered study.
There are some limitations to our study. Because we cannot force all foot and ankle patients from our institution to participate in our study and fill out PROMIS surveys, our population may be subject to selection bias. However, we have taken all patients that presented for operative intervention over a period of time, and the loss of follow-up is a limitation in all studies. Our focus on the anatomic location vs the specific procedure we feel limits the adverse effect of selection bias as we have focused on the overall anatomic subgroups and had sufficient patients in each group. Additionally, our study was carried out at a single tertiary academic center located in a major US metropolitan area, so the results may not be generalizable to areas with significantly different demographics such as different countries or rural areas. However, we have a significant proportion of primary cases at our tertiary care center and therefore we do feel this is a good representation of the standard preoperative population of foot and ankle orthopedic surgeons who treat both primary and revision pathology. Lastly, the study could have included additional variables for further stratification (ie, ethnicity and comorbidities). Future studies that analyze these trends may be able to help patients predict their outcomes based on their individual characteristics.
We feel this is a good initial step in understanding that forefoot surgery does not significantly offer inferior outcomes compared with other anatomic aspects of foot and ankle surgery. Additionally, our data help to improve our ability as a community to improve the preoperative expectation following foot and ankle surgery.
Conclusion
In conclusion, our entire foot and ankle cohort had significantly improved PROMIS scores postoperatively compared to preoperatively. A majority of patients also had clinically significant improvements in physical function and pain. However, approximately one-fourth of patients may not attain the level of pain improvement that they are expected to achieve. Furthermore, our results show that there are no differences in clinical outcomes between the forefoot, midfoot, hindfoot, and Achilles subgroups.
Supplemental Material
Supplemental Material, FAO959059-ICMJE - Comparison of Patient-Reported Outcomes for Major Pathologies of the Forefoot, Midfoot, Hindfoot, and Achilles Using PROMIS
Supplemental Material, FAO959059-ICMJE for Comparison of Patient-Reported Outcomes for Major Pathologies of the Forefoot, Midfoot, Hindfoot, and Achilles Using PROMIS by Daniel A. Hu, Rusheel Nayak, Elijah O. Ogunkoya, Milap S. Patel and Anish R. Kadakia in Foot & Ankle Orthopaedics
Footnotes
Editor’s Note
The authors are to be congratulated for a novel way of looking at all foot and ankle procedures and assessing them by different anatomic areas. I would agree that many forefoot patients seem not to improve as much as some of our other patients, which this study found not to be the case. It is unclear how well trauma patients in the study, that is, Lisfranc ORIF and Achilles repair patients, could accurately assess their preoperative condition compared to chronic degenerative conditions such as midfoot/hindfoot/ankle arthritis and flatfoot patients. Further studies could help elucidate that question.
Ethics Approval
Ethical approval for this study was obtained from Northwestern Institutional Review board (STU00084014/00082417/00084030).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.