
Abstract
Background:
Calcaneofibular impingement is characterized by lateral hindfoot pain and is commonly resulting from calcaneal fracture malunion or severe flatfoot deformity. Lateral calcaneal wall decompression has been used successfully to relieve pain in patients who have calcaneofibular impingement. However, in cases of severe impingement and hindfoot valgus, lateral wall excision may leave only a small remnant of calcaneal bone for weightbearing and can lead to chronic heel pain. We describe a surgical technique using a medial displacement calcaneal osteotomy (MDCO) combined with a lateral wall exostectomy and report on the outcomes from our series of patients.
Methods:
Retrospective study of a single surgeon’s patients was done from 2010 to 2020 who underwent medial slide calcaneal osteotomy and lateral wall exostectomy for calcaneofibular impingement. Descriptive statistics were used to summarize patient characteristics. Our study included 9 patients, 6 females and 3 males, with a mean age of 59 years (range: 19-77) and a mean follow-up of 62 weeks (range: 6-184).
Results:
Five had an Achilles split approach, 2 had an oblique lateral approach, and 1 had an extensile lateral approach. Patients achieved radiographic relief of impingement and improvement in pain. Minor skin and soft tissue complications occurred in 3 patients, all of which were associated with laterally based incisions, and all resolved after a 10-day course of oral antibiotics. No major complications, emergency department visits, or readmissions occurred.
Conclusions:
MDCO and lateral wall exostectomy was a safe and effective treatment for severe calcaneofibular impingement.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Introduction
Calcaneofibular impingement is characterized by lateral hindfoot pain and can result as a sequela of calcaneal fracture malunion, severe flatfoot deformity, congenital deformity, and inflammatory arthropathy with lateral subluxation of the calcaneus. Calcaneus fractures frequently result in lateral wall blowout and heel widening, which predisposes patients to calcaneofibular impingement. This causes peroneal tendon irritation or dislocation as well as symptomatic bony impingement. 1,5,8 -10 In flatfoot deformity, there is progressive hindfoot valgus that can be further exacerbated by lateral subluxation of the subtalar joint leading to painful impingement of the calcaneus and fibula. 6,11 Malicky et al 7 analyzed simulated weightbearing computed tomography imaging in 19 adults with symptomatic flatfoot deformity and found that calcaneofibular impingement was present in 66% of patients.
Following an appropriate trial of nonoperative management, lateral calcaneal wall decompression has been used successfully to relieve pain and improve function in patients with calcaneofibular impingement. 2,4 Braly et al 2 evaluated lateral decompression without subtalar arthrodesis as a treatment alternative for malunited calcaneal fractures with subtalar involvement. They reported satisfactory results in 9 of the 11 patients at an average follow-up of 28 months. Additionally, Clare et al 3 reported long-term improvement in pain, function, and restoration of a plantigrade foot in 40 patients with malunited calcaneal fractures managed with a surgical protocol including lateral wall exostectomy for all malunions. However, in the case of severe calcaneofibular impingement and hindfoot valgus, simply excising the calcaneal bone adjacent to the fibula would result in significant bone removal from the calcaneus to achieve adequate decompression. Leaving only a small remnant of the calcaneus to be available for weightbearing can lead to heel pain while also not addressing the deformity.
Therefore, the senior author has developed a surgical technique to achieve adequate decompression of osseous calcaneofibular impingement, without narrowing the posterior inferior calcaneus, while doing so in a safe and reproducible manner. An oblique, midcalcaneal osteotomy is performed via a posterior incision, where the calcaneus is translated medially and the excess superolateral calcaneal bone is removed from beneath the fibula. Our evidence suggests that there have been excellent clinical outcomes with no surgical failures or major complications using this technique and protocol. The current study is the first to describe outcomes using this surgical technique for management of symptomatic, severe calcaneofibular impingement. Therefore, we aimed to (1) discuss the surgical technique and postoperative protocol used, (2) evaluate radiographic and clinical outcomes, and (3) describe any postoperative complications for patients undergoing oblique calcaneal osteotomy for calcaneofibular impingement.
Methods
This is a retrospective case series and technique guide of patients undergoing medial slide calcaneal osteotomy and lateral decompression for severe calcaneofibular impingement by the senior author between 2010 and 2020. Inclusion criteria included patients who had calcaneofibular impingement, as evidenced by radiographic impingement with symptomatic lateral hindfoot pain and who underwent medial slide calcaneal osteotomy. Patients below the age of 18 years were excluded on the basis of skeletal immaturity.
Following Institutional Review Board approval, patients were queried using our institution’s Duke Enterprise Data Unified Content Explorer (DEDUCE) query tool to identify patients using the Current Procedural Terminology (CPT) code 28300, defined as a calcaneal osteotomy, yielding 211 patients. Operative reports were then analyzed to identify patients who underwent the procedure of interest, and review of electronic medical records and imaging studies allowed for identification of patients with symptomatic, severe calcaneofibular impingement. Nine patients met the inclusion and exclusion criteria and comprised our final study case series. Collection of demographics, radiographic and clinical outcomes, and any complications were also recorded via retrospective review of electronic records. Minor and major complications, as defined by the relative clinical impact on patient health and surgical outcome, and emergency department visits and readmissions were monitored within 90 days from the index procedure as a measure of quality and safety of the procedure.
Nine patients were identified to meet the inclusion and exclusion criteria for our case series. Mean patient age was 59 years (range: 19-77), with 6 females and 3 males. Mean follow-up from the surgery of interest was 62 weeks (range: 6-184).
Data were collected and stored using Microsoft Excel (Seattle, WA) within a Protected Analytics Computing Environment (PACE), a highly protected virtual network space that served as a marketplace where approved users can work with identifiable protected health information. Descriptive statistics were used to quantify our population’s demographics and outcomes. Contraindications were lateral heel pain caused by contact between the lateral malleolus and the side of the shoe or alternate causes of lateral heel pain (ie, calcaneocuboid arthrosis, sural neuritis, and plantar fasciitis).
Technique
Patient is placed under either general anesthesia or intravenous sedation with supplemental regional nerve blockade.
The patient is positioned prone on a radiolucent operating room table, with the forefeet extending just beyond the end of the table.
Either a pneumatic thigh tourniquet or calf tourniquet is used.
A longitudinal incision is made over the mid-axis of the calcaneus straight through the Achilles tendon.
The tendon is dissected off the lateral calcaneus but its distal portion attached to the distal calcaneus and medial side is left undisturbed.
A key elevator is then used to free tissue up medially just inferior to the planned osteotomy site.
A guide wire is inserted from proximal to distal, beginning about 1 cm posteriorly from the subtalar joint at an approximately 45-degree angle to the longitudinal axis of the calcaneus.
A fluoroscopic image is obtained to show the correct angle and placement.
The larger blade of the small oscillating saw is used to cut along the guidewire posteriorly to perform the osteotomy. The guidewire is removed. Now the calcaneal tuberosity is translated as far as possible medially, usually approximately 1.5 cm.
A 7.5-mm screw guidewire is inserted to hold this position and another guidewire is now added and their position checked on fluoroscopy (Figures 1 and 2).
Then 2 fully threaded 7.5-mm headless cannulated screws, usually 40 to 55 mm, are inserted across the osteotomy site. The position and length of the screws are verified on fluoroscopy (Figure 3).
Optional: If there is extensive subtalar arthritis, the subtalar joint may be exposed through this incision, debrided with a combination of rongeurs and curettes, bone grafted, and the fully threaded screws inserted across the subtalar joint.
Through the same posterior-based incision and dissection, a ½-inch osteotome is placed along the lateral side of the calcaneus. The superior lateral portion of the calcaneus articulating with the lateral talus is cut and subsequently removed with a long thin rongeur, pituitary rongeur, or a Kocher clamp. Fluoroscopy demonstrates relief of bony impingement (Figure 4). This leaves a portion of the subtalar joint on the talus and the calcaneal cuboid joint on the cuboid exposed.
The posterior aspect of the cut on the calcaneus is rongeured or rasped smooth.
The Achilles tendon is then closed with 2-0 Vicryl, the subcutaneous tissue with 3-0 Vicryl and the skin with 3-0 nylon.
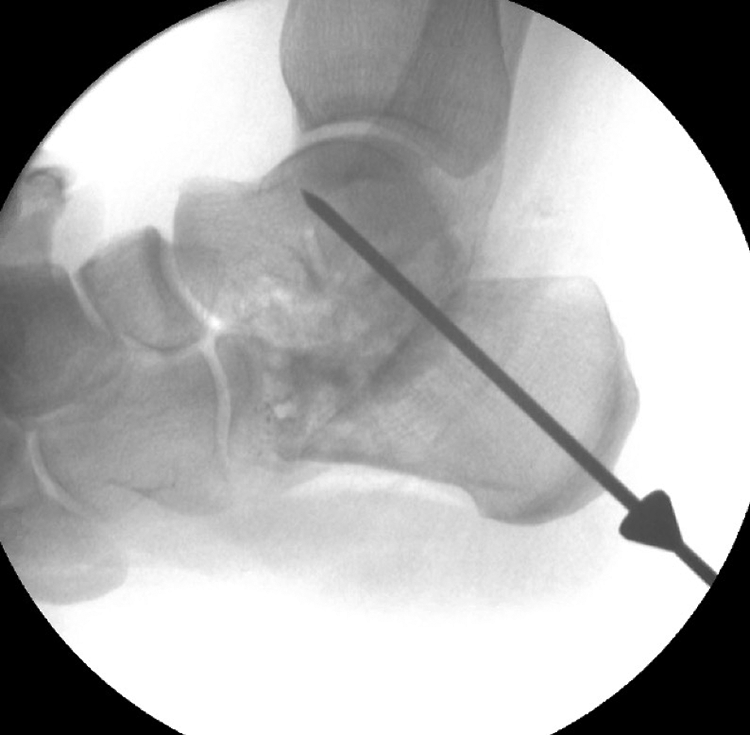
Intraoperative lateral fluoroscopic image of the hindfoot demonstrating appropriate guidewire positioning for a 7.5-mm screw to achieve fixation across both the calcaneal osteotomy and subtalar joint in a combined medializing calcaneal osteotomy and subtalar arthrodesis.
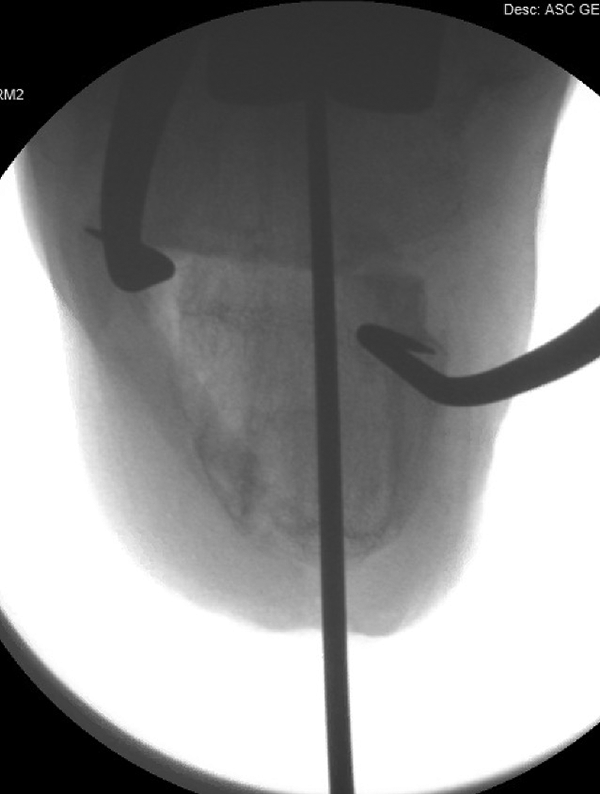
Intraoperative fluoroscopic Harris heel view demonstrating guidewire placement after obtaining approximately 10 mm of medial shift with the calcaneal osteotomy.

Intraoperative fluoroscopic lateral hindfoot view demonstrating two 7.5-mm screw fixation across the calcaneus osteotomy and subtalar joint in a combined medializing calcaneal osteotomy and subtalar arthrodesis.

Intraoperative fluoroscopic Harris heel view demonstrating final image of two 7.5-mm screw fixation across the medialized osteotomy site in addition to a lateral wall exostectomy.
Pearls
Use lateral calcaneus exostectomy bone as bone graft if performing subtalar arthrodesis
In order to slide the calcaneal tuberosity as far medially as possible, it is necessary to use key elevator to free tissue up medially just inferior to the osteotomy site.
Postoperative Protocol
0-3 weeks: A well-padded cast is applied with the foot in a neutral position. The patient is strictly nonweightbearing with an emphasis on elevation.
3-6 weeks: Sutures are removed at 3 weeks, and a well-padded nonweightbearing cast is reapplied.
6-9 weeks: Radiographs are obtained at the 6-week postoperative visit. If appropriate healing is appreciated, the patient is placed in a weightbearing controlled ankle motion boot for 3 weeks.
9+ weeks: Normal shoe wear with resumption of activities as tolerated.
Results
Patient Case
Patient B is a 68-year-old woman who underwent a subtalar fusion in 2008 for severe subtalar arthrosis, with subsequent hardware removal a year later. The patient then presented in 2016 with a complaint of lateral ankle pain, 5 of 10 in severity, with imaging consistent with subtalar nonunion as well as subfibular impingement (Figure 5). On April 21, 2016, the patient underwent revision subtalar arthrodesis, combined with a medial slide calcaneal osteotomy and superolateral calcaneal exostectomy. The calcaneal bone decompressed from underneath the fibula was combined with bone growth material and placed within the subtalar nonunion site (Figure 6). At 3-week follow-up, patient had mild serous drainage from the incision and a 10-day course of oral antibiotics was prescribed. Incision appeared improved by 6-week follow-up and the patient was transitioned to a controlled ankle motion boot, then to a normal shoe, per protocol. Patient had no complaints until at final follow-up, 68 weeks postoperatively, when the patient developed a mild burning lateral ankle pain consistent with sural neuritis. Please see Table 1 for summary of patient data from our case series.

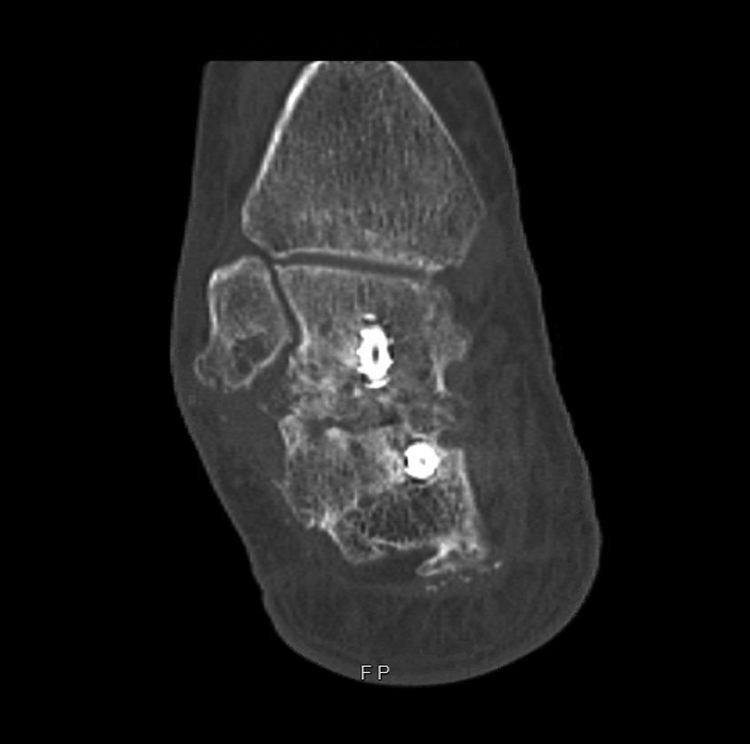
Patient B, preoperative coronal computed tomography image demonstrating calcaneal valgus and sclerosis of the distal fibula and adjacent calcaneus consistent with calcaneofibular impingement.
Patient B, postoperative coronal computed tomography image demonstrating relief of calcaneofibular impingement and improved hindfoot alignment.
Demographics, surgical characteristics, and outcomes for 9 patients included in our study population.

Abbreviations: MDCO, medial displacement calcaneal osteotomy; ORIF, open reduction internal fixation.
a All minor complications managed successfully with a 10-day course of oral antibiotics.
Complications
Minor skin and soft tissue complications occurred in 3 of 9 patients, with 1 patient developing superficial erythema concerning for cellulitis, 1 patient with mild drainage from the incision, and 1 patient with a small superficial dehiscence of the incision. All minor wound complications were noted at 3-week follow-up on removal of the cast and resolved after a 10-day oral course of antibiotics. None of these wound healing complications were associated with the posterior Achilles split approach. Additionally, 1 patient developed mild burning pain about the lateral foot consistent with sural neuritis. There were no major complications, Achilles tendon ruptures, or surgical failures at final follow-up. There were no emergency department visits or readmissions postoperatively within 90 days from surgery.
Discussion
Calcaneofibular impingement can be a source of significant lateral heel pain due to pathologic valgus or lateral displacement of the calcaneus, commonly resulting from flatfoot deformity and calcaneus fracture malunion. After exhausting nonoperative management modalities, surgical intervention has been shown to be effective in relieving pain secondary to calcaneofibular impingement. In our series of 9 patients managed with medial slide calcaneal osteotomy and superolateral calcaneal wall exostectomy, we experienced excellent clinical and radiographic outcomes with no major complications or surgical failures, thus demonstrating safety and relative efficacy of this novel treatment approach.
In patients with calcaneofibular impingement secondary to flatfoot deformity, correcting the heel valgus is the primary goal, typically achieved via either a medializing calcaneal osteotomy, subtalar arthrodesis, or combination of the two. However, without specific attention paid to removing the subfibular, superolateral calcaneal bone, the pain generator in this clinical entity may not be fully addressed. Additionally, an isolated lateral calcaneal wall decompression is relatively contraindicated in patients with heel valgus. In our series, the 3 patients with a history of flatfoot deformity had undergone prior triple arthrodesis with subsequent development or noncorrection of heel valgus, resulting in symptomatic calcaneofibular impingement. Our technique of using the medializing calcaneal osteotomy combined with a superolateral calcaneal exostectomy directly addresses the extra-articular osseous abutment and valgus deformity via a single incision approach with access to the subtalar joint if required for subtalar arthrodesis. Most importantly it does not narrow the heel. Using this technique appears particularly well suited as a surgical option for patients with flatfoot deformity who fail triple arthrodesis due to subsequent heel valgus and calcaneofibular impingement.
Lateral calcaneal wall decompression has been used successfully to relieve pain and improve function in patients with calcaneofibular impingement secondary to calcaneus fracture malunion. 2,4 Braly et al 2 evaluated lateral decompression without subtalar arthrodesis as a treatment alternative for malunited calcaneal fractures. Using an isolated lateral calcaneal exostectomy as an alternative to late subtalar arthrodesis for type II malunions (both calcaneal malunion and subtalar involvement), they reported satisfactory results in 9 of the 11 patients at an average follow-up of 28 months. Additionally, Clare et al 3 reported long-term improvement in pain, function, and restoration of a plantigrade foot in 40 patients with malunited calcaneal fractures managed with a surgical protocol including lateral wall exostectomy via an extensile lateral approach for all malunions. However, in the case of severe calcaneofibular impingement and hindfoot valgus, simply excising the calcaneal bone adjacent to the fibula may result in significant bone removal from the calcaneus to achieve adequate decompression, leaving only a small remnant of the calcaneus to be available for weightbearing, while also not addressing the valgus deformity. However, this study raises concerns regarding wound healing complications with the extensile lateral approach, with reported delayed wound healing occurring in 14.3% to 31.2% of patients in the setting of reconstruction for calcaneus malunion, 3 highlighting the need for a less morbid surgical approach.
Although this is the first study to report on the described technique, these findings and technique must be understood in light of their limitations: small number of patients included in our study, the heterogeneity of coexisting foot and ankle pathology in our population, and the lack of standardized patient-reported outcomes collected. However, regardless of these limitations, this technique was shown to be a novel, safe, and effective means for surgically managing calcaneofibular impingement in a variety of clinical situations.
Supplemental Material
Supplemental Material, FAO953793-ICMJE - Surgical Technique for Management of Severe Calcaneofibular Impingement: Case Series
Supplemental Material, FAO953793-ICMJE for Surgical Technique for Management of Severe Calcaneofibular Impingement: Case Series by Jay M. Levin and James K. DeOrio in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the Duke Health IRB, PRO00104234.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.