
Abstract
Background:
Patients undergoing fixation for foot and ankle fractures may experience poor outcomes despite achieving apparent anatomic reduction. Adjunct arthroscopy to identify missed concomitant injuries and subtle displacements has been proposed as a vehicle to enhance functional results for these patients. The purpose of this review is to provide an overview of the literature regarding arthroscopically assisted open reduction and internal fixation (AAORIF) methods for commonly encountered foot and ankle injuries including pilon, ankle, and calcaneus fractures published to date.
Methods:
A systematic review of the literature was performed using the PubMed database to access all studies reporting on arthroscopically assisted internal fixation methods for pilon, ankle, and calcaneus fractures. Relevant publications were analyzed for details on their respective study designs, the operative technique used, clinical outcomes, outcome instruments used, and reported complications.
Results:
A total of 32 studies were included in this review. Two studies on pilon fractures, a randomized controlled trial (RCT) and case series with a total of 243 patients, met inclusion criteria. Postoperative articular reductions, bone union, and Mazur scores were found to be significantly better for those using adjunct arthroscopy when compared to those with no arthroscopy use. Patient-reported outcomes were overall reported as excellent for most patients, with no difference in patient-reported outcomes reported in the RCT. For ankle fractures, a total of 17 studies comprising of 2 systematic reviews, 1 meta-analysis, 2 RCTs, 5 retrospective comparative studies, 6 case series, and 1 case-control study met inclusion criteria for this review. Results were mixed, though the overall consensus was that arthroscopy use may help to better visualize concomitant intra-articular injuries and is generally considered safe with at least comparable outcomes to conventional methods. For the calcaneus, 13 studies met the criteria. Two studies were review papers, 8 were case series, and 3 were retrospective comparative studies. A total of 308 patients with 316 fractures formed the basis of analysis. In general, the studies found comparable functional outcomes between with or without arthroscopy use, but found that anatomical reductions were significantly improved with the use of arthroscopy.
Conclusions:
Arthroscopy shows promise as a valuable adjunct tool for internal fixation of foot and ankle fractures, though definitive conclusions as to its clinical significance have yet to be drawn because of limited evidence. Potential advantages related to the direct visualization of the fracture site and minimally invasive nature of arthroscopy were suggested throughout studies examined in this review. The presence of intra-articular pathology may lead to unexpectedly poor outcomes seen in some patients who undergo surgical fixation of ankle fractures with an otherwise anatomic reduction on postoperative radiographs; the ability to diagnose and address these lesions with arthroscopy, therefore, has the potential to improve patient outcomes. To date, however, available literature has not shown that significant improvements in anatomical reductions and treatment of these intra-articular injuries provide any improvement in outcomes over standard fixation methods. Few prospective randomized controlled studies have been performed comparing these 2 operative techniques, rendering any suggestion that AAORIF improves clinical outcomes over traditional open fixation difficult to justify. Further research is indicated for what may be a potentially promising surgical adjunct prior to advocating for its routine use in patients.
Keywords
Introduction
The advent of arthroscopy has greatly improved orthopedic care over the past half century. Improved instrumentation and operative techniques have allowed many conditions to be treated less invasively, avoiding traditional open approaches and their associated morbidity. More recently, arthroscopy has been utilized for fracture care with an increase in published reports demonstrating its application in the treatment of common foot and ankle fractures. 17
Fractures of the foot and ankle can be challenging to manage given their often articular or periarticular nature. Despite achieving acceptable alignment via direct visualization or conventional intraoperative imaging modalities, studies have shown that patients undergoing traditional management may still experience unfavorable mid- and long-term outcomes. 16,24 Although multifactorial, it has been suggested that poor outcomes can be attributed to concomitant cartilaginous, ligamentous, and soft tissue injuries as well as subtle articular malreduction. 16,24 Recent literature has proposed that arthroscopic assistance may help improve visualization and enhance accurate articular reductions, which could ultimately improve patient outcomes. 33
To date, a comprehensive review of arthroscopically assisted internal fixation techniques, including arthroscopically assisted open reduction and internal fixation (AAORIF), arthroscopically assisted percutaneous reduction and fixation (APRF) and arthroscopically guided minimally invasive screw fixation techniques (ARMIS), for foot and ankle fractures does not exist in the literature. Although this is attributable to a relative paucity of studies, an increasing number of works including randomized control trials (RCTs), case series, technical tips, and case reports have reported on these techniques and their benefits. Although several authors have suggested a variety of factors influencing outcomes, including sex, age, comorbid conditions (ie, smoking, diabetes), fracture severity, and concomitant injury, the majority of current studies emphasize that anatomic articular reduction is the primary modifiable factor that may influence outcomes. 19,24 Although intraoperative direct visualization and radiographic assessment during open procedures have been the standard modalities for confirming anatomic reduction, the advent of arthroscopy has enabled direct visualization of structures that are typically more challenging to assess through imaging, such as the joints of the foot and ankle. In light of this, there is increasing support in the literature for arthroscopically assisted fracture fixation.
The purpose of the current investigation was to provide surgeons with an overview of the currently published literature regarding arthroscopically assisted internal fixation methods for commonly encountered foot and ankle injuries including pilon, ankle, and calcaneus fractures.
Methods
A systematic electronic literature search was performed to identify articles that reported the use of arthroscopy in the management of foot and ankle fractures. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were implemented. The PubMed database was searched using various combinations of the following key phrases: (ankle, distal tibia, pilon, calcane*, foot) and [fracture* AND (arthroscop* OR endoscop*)]. Duplicates between search results were identified and removed. Abstracts were reviewed to eliminate studies not relevant to the goals of this review. Following the initial screening process, full texts of each article were reviewed to finalize the list of included studies. The reference lists of the full texts were also screened to identify additional relevant articles.
Inclusion criteria included studies that reported on patients with acute foot and ankle fractures (specifically pilon, ankle, and calcaneus fractures) treated with arthroscopically assisted internal fixation methods. Meta-analyses, reviews, case series, randomized controlled trials, and comparative series that compared arthroscopically assisted internal fixation methods to other interventions were included. Articles not written in English were translated using Google Translate by the reviewers when possible. Exclusion criteria included publications on fractures treated without arthroscopy, arthroscopic surgeries performed for subsequent conditions following primary open reduction and internal fixation (ORIF), case reports, letters to editors, and technical notes. Studies reporting on the treatment of acute or chronic osteochondral lesions in the absence of concomitant fracture ORIF were excluded (Figure 1).
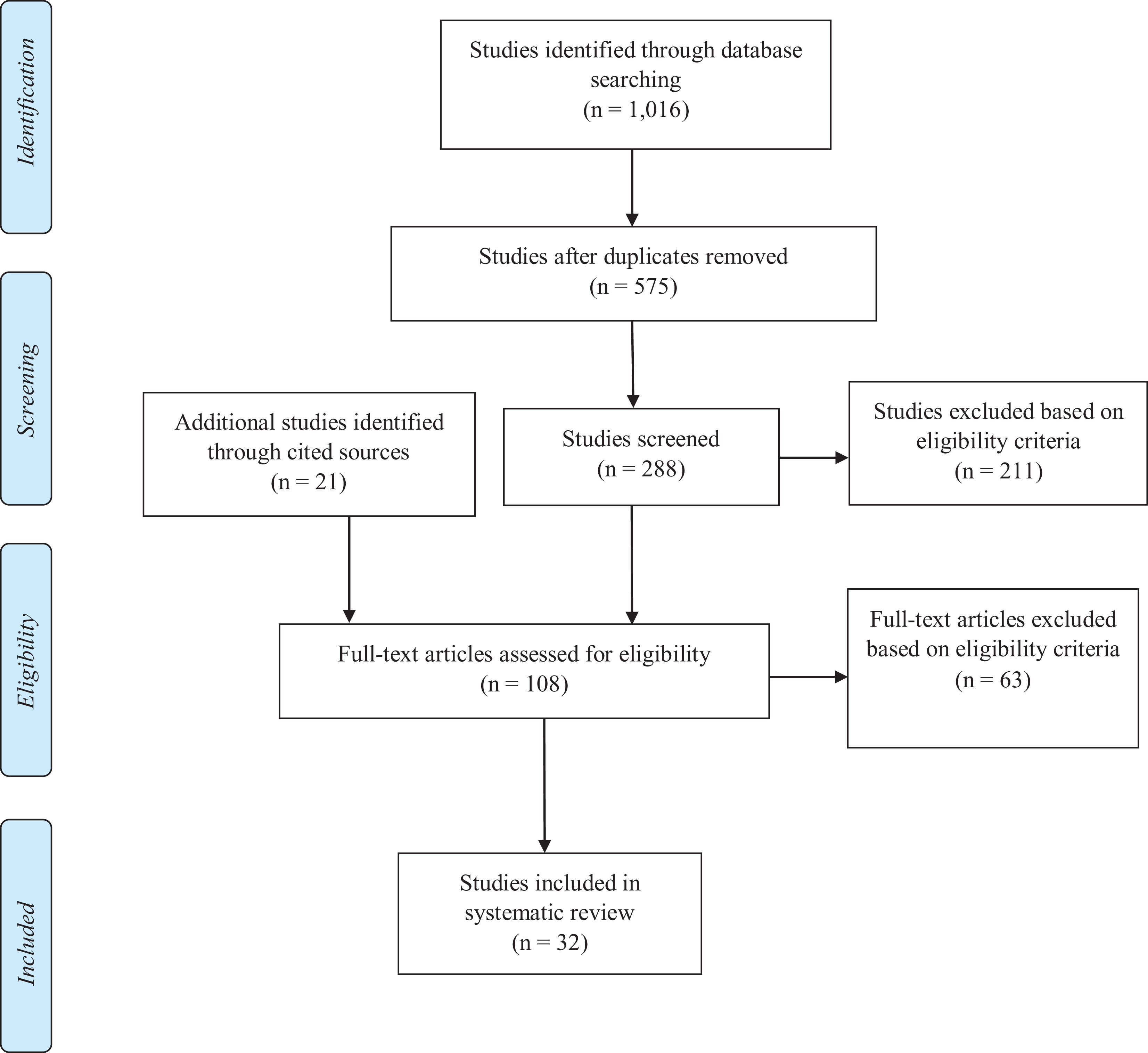
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for AAORIF Systematic Review. Process from: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097.
The full texts of all relevant studies were obtained and reviewed by 2 independent reviewers according to the above inclusion and exclusion criteria. Data extraction was performed by 2 independent reviewers using a standardized data sheet. The following information was extracted from included studies: study type, sample size, mean age, sex, fracture classification and location, operative technique used, follow-up length, clinical outcomes, outcome instruments used, and complications. Reviewers also extracted author’s opinion as to the source of any potential complications, differentiating between those directly attributable vs not attributable to arthroscopic intervention.
Results
Pilon Fractures
Review of current literature identified 2 studies, 1 nonblinded randomized controlled trial (RCT) and 1 case series, that met criteria for this review. 25,26 The total number of patients from these studies was 243. There were 166 men and 77 women with ages ranging from 19 to 68 years old. The RCT utilized the Ruedi-Allgower system (all patients with type III pilon fractures), whereas the case series used the AO/OTA classification (AO 43-C1 pilon fracture). 25,26 In the RCT study, patients were split evenly into 2 groups with no difference in age, sex, mechanism, side, and type of fracture (P > .05 for all); 115 patients (group A) underwent external fixation combined with limited internal fixation (EFLIF), whereas the other 115 patients (group B) underwent AAORIF. 25 The patients in the case series underwent arthroscopy-assisted reduction with limited internal fixation combined with external fixation (Table 1). 26 Described indications for arthroscopic use were visualization of articular reduction, and concomitant procedures mentioned in the studies included debridement. Mean follow-up time among studies was 12 months. 25,26
Overview of Included Pilon Fracture Studies Excluding Meta-analyses and Systematic Reviews.

Abbreviations: APRF, arthroscopically assisted percutaneous reduction and fixation; EFLIF,; RCT, randomized controlled trial.
Study results
Both studies used the Mazur Ankle Grading Scale. Liu et al showed that compared with the EFLIF group, the AAORIF group achieved superior articular reductions (65.2% vs 48.7% graded anatomical), bone union (97.4% vs 87.8% normal union), and Mazur scores (69.6% vs 53.0% excellent outcome; P < .05 for all data). Patient satisfaction, hardware failure, and infection were not significantly different between the groups. Although the AAORIF group demonstrated lower rates of posttraumatic arthrosis compared with the EFLIF group at final follow-up, short-term follow-up is inadequate to fully assess the development of arthrosis. 25 For the case series on arthroscopy-assisted reduction with limited internal fixation combined with external fixation, Luo et al used postoperative radiographs to assess outcomes, using reduction quality, internal fixation position, and fracture union as variables to grade outcomes. With limited details in reporting, 9 cases were scored overall as excellent, 2 as good, and 2 as poor; the satisfaction rate was 85%. Two patients’ outcomes were graded as poor; both developed mild traumatic arthritis and reported mild pain with ambulation 1 year postoperation. 26
Complications
No serious complications directly attributable to arthroscopy were reported in either of these studies. Although the RCT reported complications (postoperative infections and traumatic arthritis) in some patients, the prevalence of infection was similar between the 2 groups (AAORIF 11.3%, EFLIF 13.9%) and the rate of grade 4 traumatic arthritis, defined as severe narrowing of joint space, large osteophytes, marked sclerosis, and definite bone deformity per the Lawrence system, was noted to be lower in the AAORIF (2.6%) when compared to the EFLIF (5.2%) group. The relatively equal and lower rates for each complication, respectively, support the conclusion that the complications were unlikely attributable to AAORIF. 25 No complications were reported with the case series.
Ankle Fractures
For ankle fractures, we identified a total of 17 studies. 2 -4,5 -8,10 -13,16,27,29,35 -38 Among these, 2 were systematic reviews, 1 meta-analysis, 2 RCTs, 5 retrospective comparative studies, 4 retrospective series, 2 prospective series, and 1 case-control study. The studies reported a total of 952 patients. There were 46.7% male and 53.3% female participants with mean age 41.9 years (range: 18-85). The mean follow-up time was 31.1 months (range: 4-76). Six studies used the Lauge-Hansen classification system, 3 used the Danis-Weber classification system, 2 used the AO/OTA classification system, 1 used the Herscovici classification system, and 3 reported the location of the fractures without classification. Of these, the most common fracture types were Danis-Weber and AO/OTA type B corresponding to Lauge-Hansen supination-external rotation injury (Table 2).
Overview of Included Ankle Fracture Studies Excluding Meta-analyses and Systematic Reviews.

Abbreviations: AAORIF, arthroscopically-assisted open reduction and internal fixation; AOFAS, American Orthopaedic Foot & Ankle Society; ARMIS, arthroscopic reduction and minimally invasive surgery; MODEMS, Musculoskeletal Outcomes Data Evaluation and Management Scale; NR, not reported; OM, Olerud and Molander; ORIF, open reduction and internal fixation; PROMIS PF, Patient-Reported Outcome Measurement Information System Physical Function; RCT, randomized controlled trial; SF-36, 36-Item Short-Form Health Survey; VAS, visual analog scale.
Although several studies noted their rationale for using and studying arthroscopic use for unstable ankle fractures for evaluation of suspected syndesmotic disruption, there does not seem to be a consensus on specific indications for use among the included studies. 7,8,16 At one institution, the primary indication for arthroscopic assisted surgery in medial malleolus fractures was identification of impaction. 35 On the other hand, Fuchs et al performed AAORIF on all ankle fractures with an intact medial malleolus because arthroscopy allowed direct evaluation of the articular surface. 13 Although indications are evolving, several studies have suggested arthroscopy as a tool for identifying subtle syndesmotic instability and/or examining for articular impaction not evident on plain radiographs.
Almost all investigations identified concomitant procedures (79%) related to arthroscopy use, including microfracture, synovectomy, osteochondral lesion debridement, loose body removal, talar dome drilling and evacuation of hemarthroses. Although concomitant procedures may potentially confound the effects of arthroscopy during a statistical analysis, it is important to recognize that arthroscopy itself was generally a concomitant procedure to the primary ORIF in nearly all reports. Of note, the meta-analysis and 2 systematic reviews included a total of 12 AAORIF studies (excluding duplicate studies). Only 4 of the 12 studies were comparative studies between AAORIF and ORIF. 13,36 -38 There was a general consensus among the 3 studies that larger and more comprehensive comparative studies are needed to definitively elucidate the effects on clinical outcomes of AAORIF vs ORIF. In their meta-analysis of the 4 comparative studies, Ahmed et al concluded that AAORIF may add minimal additional risk and lead to higher postoperative functional scores as compared to conventional ORIF. 2 Gonzalez et al included 3 comparative studies and 1 case series on AAORIF in their review. They concluded that further research on indications for arthroscopic use and the clinical value of the tool are warranted to justify its addition for acute ankle fracture management. 16 Chen et al reviewed 8 observational studies and 2 comparative studies and reported that arthroscopy was used in most of these studies to identify concomitant intra-articular injuries such as chondral lesions, deltoid ligament injuries, and syndesmotic injuries. They concluded that AAORIF is a safe and effective treatment for acute ankle fractures although clear clinical benefits of AAORIF were inconclusive. 6
Study Results
Seven studies used the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score postoperatively, reporting an AOFAS mean score of 93.2 (range 85.4-96.9). 3,7,8,10 -12,36 Five studies reported the visual analog scale (VAS) score, with a mean score of 0.7 (range 0-1.03). 8,10 -13 Takao et al (n = 72) in their randomized control trial reported a significant AOFAS score difference between the AAORIF group and the ORIF group (91 vs 87.6, respectively, P = .011) suggesting that AAORIF may be associated with superior outcomes compared to ORIF. 36 This is supported by a recent comparative study by Chiang et al (n = 105) that found that the early postoperative (within 3 days) VAS score was significantly lower in the arthroscopic group compared to the ORIF group (1.96 vs 2.83 respectively, P = .027). 8 On final follow-up (>3 years), VAS and AOFAS scores tended to be better in the arthroscopy group, though the difference was not statistically significant. 8 Similarly, Turhan et al (n = 47) reported significantly different Olerud and Molander score between the AAORIF and ORIF groups (92.3 vs 86.3, respectively, P = .015) at a mean follow-up of 26 months. 38
Two other comparative studies (n = 112) reported that outcomes for AAORIF were similar to that of ORIF in the Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function (PF)/Pain Interference (PI) scores, 36-Item Short Form Health Survey (SF-36), Olerud and Molander, or the Musculoskeletal Outcomes Data Evaluation and Management Scale (MODEMS) lower extremity score. 13,37 In one study, arthroscopy was used intraoperatively to confirm anatomic articular reduction after ORIF. Initial malreduction was identified in 32 of 96 patients (33.3%), necessitating revision reduction and fixation. 5 Although the efficacy of arthroscopy use during fixation may at the very least be comparable to traditional methods, the ability to directly visualize and confirm reduction is a potential value.
Complications
Overall, no serious complications were directly attributed to arthroscopy use. Minor complications reported for the cohort of patients who underwent AAORIF (but not necessarily attributable to the use of arthroscopy) included hardware irritation (3), superficial infection (3), and transient superficial peroneal nerve irritation (3). 8,13 Of the 3 superficial wound infections, 2 patients underwent subsequent irrigation and debridement. 8,13
Operative times were slightly longer for AAORIF as compared to conventional ORIF. Five studies reported a mean AAORIF duration of 66 minutes (range, 36.3-105.22), and 3 studies reported a mean ORIF duration of 62.2 minutes (range, 34-93.59). 6,10,11,13,38 One study compared operative times for AAORIF combined with microfracture to AAORIF with debridement only, and found an average of 6.6-minute increase in the group with combined microfracture. 10
Calcaneus Fractures
There was a total of 13 studies included regarding utilization of arthroscopically assisted internal fixation techniques of calcaneal fractures. 9,14,15,25,28 -32,34,39 -41 Eleven studies reported on AAORIF techniques in combination with a percutaneous approach, 1 study described implementation of the sinus tarsi approach (STA), 1 detailed use of the extensile lateral approach, and 1 study reported on both the percutaneous and extensile lateral approach techniques combined with arthroscopically assisted fixation. Two studies were review papers, 7 were retrospective case series, 3 were retrospective comparative studies, and 1 was a prospective case series. A total of 308 patients with 316 fractures formed the basis of analysis. There were 247 (80.2%) male and 61 (19.8%) female participants with a mean age of 44.5 (range, 37.8-52.3) years old. The mean follow-up time was 21.7 (range, 13.63-79.2) months. All of the studies used the Sanders classification system, with Sanders type II fractures making up the majority of cases (73%), followed by type III (26%) and type IV (1%). Four studies subcategorized Sanders type II fractures: 47% IIA, 25% IIB, and 27% IIC. 9,29 -31 Of those that also used the Essex-Lopresti classification system (4/10 studies), 45.6% were classified as tongue-type, and 54.4% as joint-depression type (Table 3). 9,29,34,41
Overview of Included Calcaneus Fracture Studies Excluding Meta-analyses and Systematic Reviews.
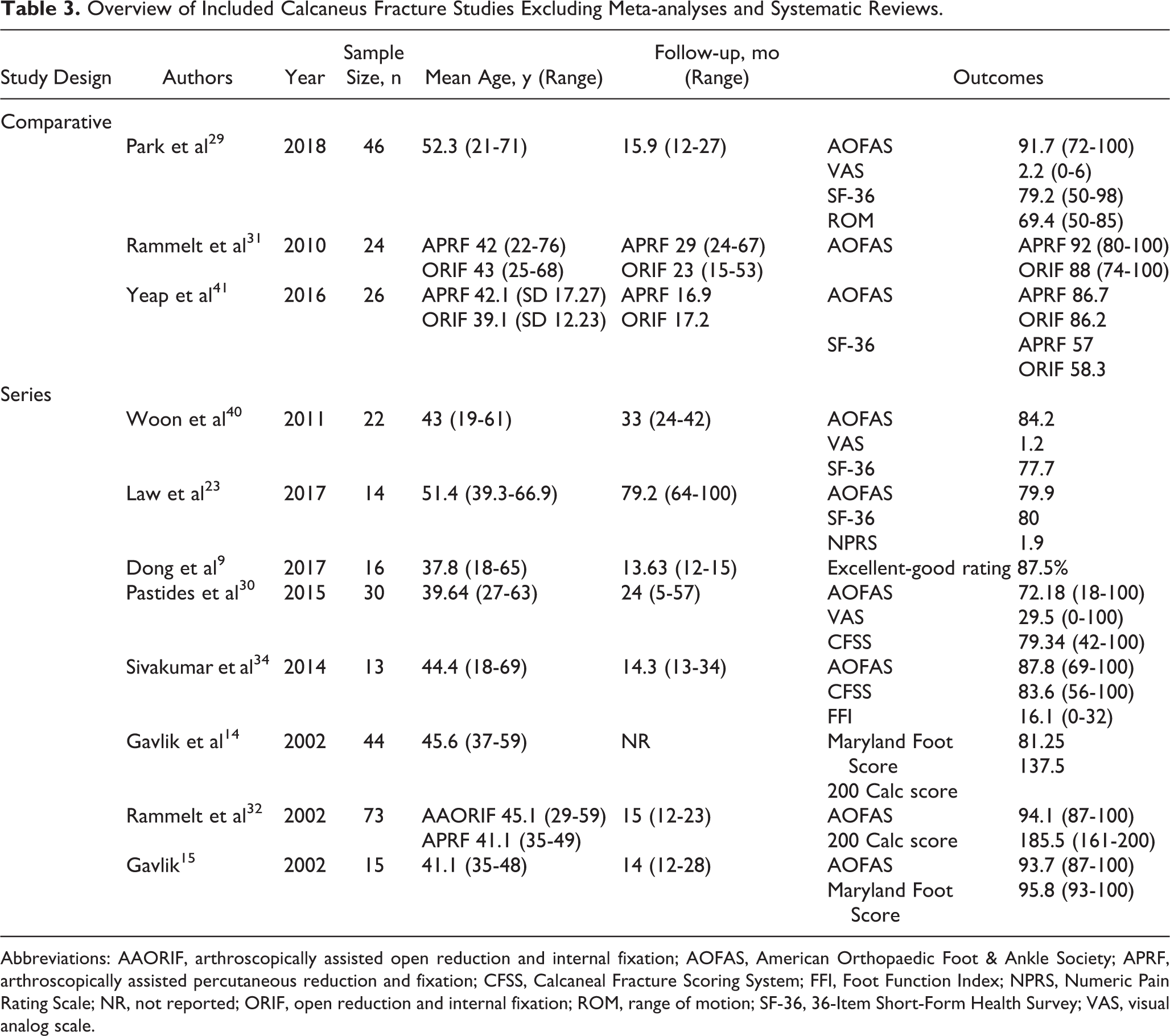
Abbreviations: AAORIF, arthroscopically assisted open reduction and internal fixation; AOFAS, American Orthopaedic Foot & Ankle Society; APRF, arthroscopically assisted percutaneous reduction and fixation; CFSS, Calcaneal Fracture Scoring System; FFI, Foot Function Index; NPRS, Numeric Pain Rating Scale; NR, not reported; ORIF, open reduction and internal fixation; ROM, range of motion; SF-36, 36-Item Short-Form Health Survey; VAS, visual analog scale.
The proposed indications for arthroscopy use in these studies included visualization of potential concurrent pathology within the joint space and to confirm proper reduction and alignment of the posterior facet. 29 Studies that confirmed additional injury via arthroscopy reported subsequently performing arthroscopic hematoma evacuation, loose body removal, and debridement of fibrous tissue within the joint. 39
Of note, 2 reviews highlighted the role of arthroscopy in treating moderate calcaneal fractures (Sanders II-III). In their recent review from 2019, Park concluded that arthroscopy can be a safe and effective adjunct in either percutaneous or open repair and should be used in conjunction with fluoroscopy to best determine articular joint congruity. 28
Wallin et al reviewed a total of 11 studies, comparing percutaneous fixation without arthroscopy (5 studies), APRF (arthroscopically assisted percutaneous reduction and fixation) (4 studies), and percutaneous fixation with bone substitute utilization (2 studies). 39 Although direct comparison among the 3 categories was difficult because of the heterogeneity of reported outcomes measures, the authors concluded that APRF appears to be safe and effective for Sanders type II, III, and IV fractures. However, it should be noted that 3 of 4 APRF studies only included Sanders II injuries, and 1 of 4 included Sanders I, II, and III. Therefore, no definitive conclusions can be drawn especially for type IV fractures.
Study Results
All studies used patient-based clinical outcome measures. Of the studies, 9 of 10 reported the AOFAS ankle-hindfoot score, 4 reported the SF-36, 3 reported the VAS score, and 2 reported the Calcaneal Fracture Scoring System scores. 9,14,15,23,29 -32,34,40,41 The mean AOFAS score for APRF was 87.95 (range, 72.18-100) for follow-up periods of over 1 year. One study reported an AOFAS score for AAORIF using the sinus tarsi approach of 91.7 at >1-year follow-up. 29 SF-36 scores ranged from 57 to 80 with a mean of 75.8 between 1 and 3 years of follow-up, with one study reporting a score of 92.7 at long-term follow-up between 5 and 8 years. 29 The mean VAS scores for APRF was 2.25 at the 2-year follow-up, and 2.2 for the arthroscopic STA at >1-year follow-up. 20,22,29
In studies comparing AAORIF to conventional ORIF using fluoroscopy, no significant differences were noted for the patient-reported functional outcome measures utilized. 29,41 On the contrary, a recent study by Park et al found that arthroscopy used for the STA significantly improved articular reduction as compared to fluoroscopy alone (95.7% vs 73.9% respectively, P = .040), though clinical outcomes at 1 year were comparable between the 2 groups. 29 Contrary to findings from the ankle studies, the mean operative times for the arthroscopic procedures tended to be shorter at 82.6 to 112.9 minutes compared to ORIF at 86.1 to 118.3 minutes, though these values were not significantly different (P = .50). 29,41 Further, Yeap et al and Rammelt et al showed statistically significant differences in time off from work between the 2 groups, with mean ranges of 11-11.6 weeks in the AAORIF group (n = 48) vs 16-24.8 weeks in the ORIF group (n = 30) (P < .001 and P < .001, respectively). 31,41 Yeap et al also reported a reduced mean postoperative length of stay in the AAORIF group of 3.8 days compared to 7.3 days for the ORIF group (P = .037). 41 The shorter operative times, time off from work, and postoperative length of stay show promise for clinical importance in the use of arthroscopy in treatment of calcaneal fractures.
Complications
No serious complications specifically attributable to arthroscopy were reported although 3 reports of portal site infection were noted. There were 7 minor complications per 316 fractures (2.2%). The total number of hardware removal due to prominence was 11 cases per 316 fractures (3.5%). 9,14,15,23,28 -32,34,39 -41 Transient sural nerve neuropraxia was reported in 1 study at an incidence of 13% (3/23). 29 Another study reported 3 superficial arthroscopic port site infections (3/33) that resolved with antibiotics. 30 One transient seroma (1/22) that resolved after 6 weeks was noted by Woon et al. 40
Discussion
To our knowledge, this is the first systematic review of literature on arthroscopy-assisted internal fixation methods encompassing the breadth of fractures to the ankle and hindfoot. Through this systematic review, we found that arthroscopy has potential benefits in fracture reduction of ankle and hindfoot fractures, though as of this writing remains an adjunct tool of unproven clinical significance. In the studies included in this review, no serious complications associated with arthroscopic use, such as permanent nerve damage, were reported. Although arthroscopy use may improve clinical results, further evidence is required in the form of higher-level investigations to determine its true efficacy. Definitive summation of the effect of arthroscopically assisted internal fixation techniques for pilon, ankle, and calcaneus fractures are limited given the paucity of literature.
It is frequently suggested in the literature that direct visualization and removal of joint debris may lead to improved clinical and functional outcomes. 33 Adams et al demonstrated that the intra-articular inflammatory burden after ankle fractures changed significantly over 10 days, suggesting that early evacuation of synovial fluid and hematoma may improve clinical outcomes by reducing cytokine burden. 1 Although evacuation may also be accomplished with thorough irrigation during ORIF, the use of arthroscopy may further reduce the inflammatory burden by means of smaller incisions and less iatrogenic soft tissue trauma. A major concern regarding the use of arthroscopy and irrigation in the foot and ankle is compartment syndrome. However, compartment syndrome developing after AAORIF has only been reported twice in the literature to date, and was not reported in any of the studies in this review. 18,21 Appropriate caution in the postoperative period should be used, as the paucity of published reports in the literature may represent either underreporting or lack of recognition.
Aktas et al suggested that chondral lesions should be routinely checked with arthroscopy, as concomitant injuries do not correlate with fracture severity and may portend poorer outcomes if not addressed. 3 Duramaz et al in their recent study showed that microfracture yielded better outcomes compared with debridement, which was one of the first studies to delineate which arthroscopic adjunct procedures may improve outcomes. 10 As evidence on the safety and efficacy of arthroscopy continues to grow, further studies on the value of arthroscopic use, associated risks, and the additional procedures involved are needed, especially considering severe soft tissue edema and swelling often noted in an acutely fractured ankle.
Although conclusive evidence is lacking, many potential advantages to arthroscopic use have been suggested through this systematic review. Direct visualization of the fracture site and surrounding structures may be performed without large incisions or arthrotomies. All studies examining pilon fractures suggested that the use of arthroscopy in their cases limited soft tissue injury and allowed for more accurate reduction and fixation of pilon fractures under direct visualization. However, patient assignment was not randomized, which may have resulted in selection bias. Minimally invasive approaches tend to preserve blood supplies and thus may lead to faster healing times compared to traditional extensile approaches. Reductions may be more accurately assessed compared to fluoroscopy alone. However, only ankle and calcaneal fracture studies directly compared arthroscopy-assisted reduction and fixation outcomes to ORIF and further investigations are required.
Limitations in the present study, as well as in the included studies, must also be addressed. The paucity of comparative studies on arthroscopically assisted internal fixation of fractures of the foot and ankle limited the conclusions that could be drawn from this present review. In particular, literature on the fractures of the distal tibia was sparse. Furthermore, it must be noted that this review was not fully comprehensive of all foot and ankle fractures; talus, midfoot, and forefoot fractures were not included because of a dearth of literature on arthroscopy use in fracture fixation in these anatomical areas. Further research exploring the utility of arthroscopy in fixation of all foot and ankle fractures, particularly those of the talus, midfoot, and forefoot, is needed in order to determine if comparable or superior outcomes are achievable when compared to traditional open approaches.
As new techniques and technologies arise, learning curves, and in turn potentially longer operative times, exist when performing these procedures. Although AAORIF of foot and ankle fractures has been described for roughly 30 years, newer techniques such as Park et al’s modified arthroscopic open reduction internal fixation sinus tarsi approach (AORIF-STA) procedure for calcaneal fractures or Liu et al’s arthroscopy-assisted minimally invasive approach to pilon fractures, continue to emerge. 25,29 Interestingly, Park et al found that the mean operative time for the AORIF-STA group was shorter than for the ORIF group, though not statistically significant. 29 This may reflect more efficient achievement of anatomic reduction compared with the open group, which may require obtaining multiple fluoroscopic views for assessing the quality of reduction. They noted that for the arthroscopy group, the first half of the cases took on average 20 minutes longer than the last half of the caseload. This highlights the possible learning curve associated with performing this technique. Further studies are required to control for surgeon experience on operative times and long-term outcomes for these procedures.
Conclusion
Arthroscopy may serve as a useful tool for accurate diagnosis and appropriate treatment of foot and ankle fractures. The current evidence regarding implementation of arthroscopy as an adjuvant tool for internal fixation of pilon, ankle, and calcaneal fractures appears to thus far indicate comparable outcomes as compared to traditional methods. Given the preponderance of larger, Level III to V studies, higher-quality comparative investigations are needed before concluding on the benefits and recommendations for arthroscopy utilization.
Supplemental Material
Supplemental Material, FAO950214-ICMJE - Arthroscopically Assisted Internal Fixation of Foot and Ankle Fractures: A Systematic Review
Supplemental Material, FAO950214-ICMJE for Arthroscopically Assisted Internal Fixation of Foot and Ankle Fractures: A Systematic Review by Caroline E. Williams, Peter Joo, Irvin Oh, Christopher Miller and John Y. Kwon in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because it is a systematic review paper thus not requiring IRB approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.