
Abstract
Background:
Although complications following hammertoe correction surgery are rare, older patients with comorbid conditions are often considered poorer operative candidates compared with younger, healthier patients because of a suspected increased risk of adverse outcomes. The aim of this study was to determine if the presence of multiple comorbidities was associated with increased complications or unsuccessful patient-reported outcomes following operative hammertoe correction in geriatric patients.
Methods:
Prospectively collected data was reviewed on 78 patients aged 60 years or older who underwent operative correction of hammertoe deformity. Patient demographics, comorbidities, and postoperative complications were recorded. Patient-reported outcomes were assessed using preoperative and postoperative visual analog scale for pain and Short Form Health Survey Physical and Mental Component Summary with 1 year of follow-up. Patients were divided into 2 groups based on number of comorbidities (0 or 1 vs > 2) and then compared. The average age of patients was 69.4 years and the prevalence of comorbidities in the study population was as follows: 11.5% smokers, 25.6% on blood thinners, 15.4% with rheumatoid arthritis, 7.7% with diabetes mellitus, 2.6% with peripheral arterial disease, 6.4% with chronic obstructive pulmonary disease, 11.5% with coronary artery disease, and 23.1% with osteoporosis.
Results:
Fifty-three patients (67.9%) had 0 or 1 comorbidity and 25 (32.1%) had 2 or more comorbidities. Compared to the 0 or 1 comorbidity group, the presence of multiple comorbidities was associated with an adjusted odds ratio (OR) for superficial wound infection of 4.18 (P = .045) and deformity recurrence requiring surgery OR of 23.15 (P = .032). Patient-reported outcomes were similar between comorbidity groups.
Conclusions:
This study further informs foot and ankle specialists to maintain increased surveillance for postoperative complications and unsuccessful outcomes in patients with multiple comorbidities. Although geriatric patients still report significant improvements in both pain and function, patients with underlying medical conditions should be counseled about their increased risks when pursuing operative hammertoe correction.
Level of Evidence:
Level III, retrospective comparative series.
Introduction
Recent years have seen an increase in the geriatric population, and orthopedics, in particular, must be prepared to mitigate the inevitable decline in both function and mobility that occurs with aging. Epidemiologic studies have shown that one-third of the population suffers from hammertoe deformity, 10 making hammertoe corrective surgery the most common foot and ankle procedure performed in geriatric patients between 2000 and 2011. 5 Many recent studies have assessed hammertoe deformity correction and the means of fixation that minimizes complications. 1,2,8,15,16,27,29,30,32 However, little in the literature describes which patients are more inclined to have complications and poor outcomes. Although complications following hammertoe correction surgery are rare, older patients with comorbid conditions are often considered more frail and therefore at an increased risk for adverse outcomes. 11,33,37,38 The aim of this study was to determine if the presence of multiple comorbidities was associated with increased complications or unsuccessful patient-reported outcomes following operative hammertoe correction in geriatric patients.
Methods
A multicenter, prospective study was conducted on patients who underwent operative correction of hammertoe deformity at Emory Healthcare and Baylor University Medical Center between January 1, 2015, and September 1, 2018. Informed consent was received from all participants. Patient demographics, including age, gender, and number of toes affected were noted. Patients younger than 60 years were excluded from the study. 11 Patients were surveyed regarding their past medical history, and the following comorbidities were recorded: smoking history, blood thinner use (including aspirin, warfarin, and antiplatelet agents), rheumatoid arthritis, diabetes mellitus, peripheral arterial disease, chronic obstructive pulmonary disease, coronary artery disease, and osteoporosis. A preoperative visual analog scale to assess pain (VAS) and Short Form-36 Health Survey (SF-36) Physical and Mental Component Summary (PCS and MCS, respectively) to assess function were recorded for all patients.
A total of 116 patients who underwent hammertoe correction surgery were enrolled in the study. Of them, 78 patients met inclusion criteria based on age ≥60 years. Baseline characteristics and comorbidity prevalences are presented in Table 1. The average age was 69.4 years with predominantly female patients. The mean number of toes operated on per patient was 2.5. Overall, 53 patients (67.9%) had 0 or 1 comorbidity and 25 (32.1%) had 2 or more comorbidities.
Baseline Characteristics (N=78).

Two foot and ankle fellowship-trained orthopedic surgeons performed operative correction of hammertoe deformity on patients who previously failed conservative treatment. Proximal interphalangeal (PIP) arthroplasty and flexor tenotomy were conducted on all patients. In cases of persistent extension of the metatarsophalangeal joint, extensor lengthening was employed. The joint position was then reassessed and, if deformity was still present, a capsulotomy was performed. In severe deformities not corrected by the aforementioned procedures, a Weil osteotomy was performed. This was also done in all occurrences of plantar plate tears, or ligamentous reconstruction with flexor transfer (ie, transfer of the long flexor tendon to the extensor hood on the side of the continued deformity). All PIP joints were stabilized with smooth 0.045- or 0.035-in. wires, and 1 or 2 twist-off or 2.0-mm screws were used in all Weil osteotomies. Following surgery, all patients were cleared for full weightbearing on their heel in a postoperative shoe or boot. Sutures were removed after 2 weeks. At 5-6 weeks, the Kirschner wires were removed, and patients were counseled to proceed to full weightbearing when comfortable. Patients were then transitioned to normal shoes as tolerated.
Patients were instructed to follow up at regular intervals (2 weeks, 6 weeks, 3 months, 6 months, or 1 year), where they were assessed for postsurgical complications, including wound infections requiring antibiotics, deep vein thrombosis, recurrence of the deformity, and revision surgery. All patients followed up at 1-year postoperatively and, at this time, were also readministered the VAS, PCS, and MCS to assess for patient-reported outcomes.
Patient-reported metrics were first assessed by comparing preoperative results with postoperative results to demonstrate the efficacy of the procedure. Patients were then divided into 2 groups based on number of comorbidities (0 -1 vs ≥2) and compared as the accumulation of comorbid conditions is thought to decrease a patient’s physiologic reserve and thereby be a marker of frailty. 37
Statistical Analysis
Categorical variables were reported as “counts (%)” and were analyzed using Pearson chi-square or Fisher exact test. All continuous variables were analyzed with Levene test to assess for equality of variances and then 2-sample t tests for independent means or paired t tests when appropriate. The change over time of patient-reported outcome scores was calculated by subtracting preoperative scores from postoperative scores. Continuous variables will be reported as “mean ± standard deviation.” Binomial logistic regression was then used to assess the risk of each complication using the 0 or 1 comorbidity group as a reference and controlling for the presence of other complications. Adjusted odds ratios (ORs) are reported with 95% confidence intervals (CIs). All tests of hypotheses were 2-sided, with an alpha of 0.05. Analyses were performed with IBM SPSS Statistics, version 25 (IBM, Armonk, NY).
Results
Patient-Reported Outcomes
Patient-reported outcome metrics were examined. The overall mean preoperative VAS was 4.0 ± 2.8, and the mean postoperative score was significantly lower at 1.5 ± 2.2 (P < .001). This difference is displayed in Figure 1. The overall mean preoperative PCS was 56.2 ± 23.1. This was significantly lower than the overall mean postoperative PCS of 65.6 ± 23.3 (P = .013). There was no significant difference found between the preoperative MCS and postoperative MCS (79.9 ± 17.0 vs 84.6 ± 14.2, respectively; P = .068). The SF-36 results for all studied patients are shown in Figure 2.
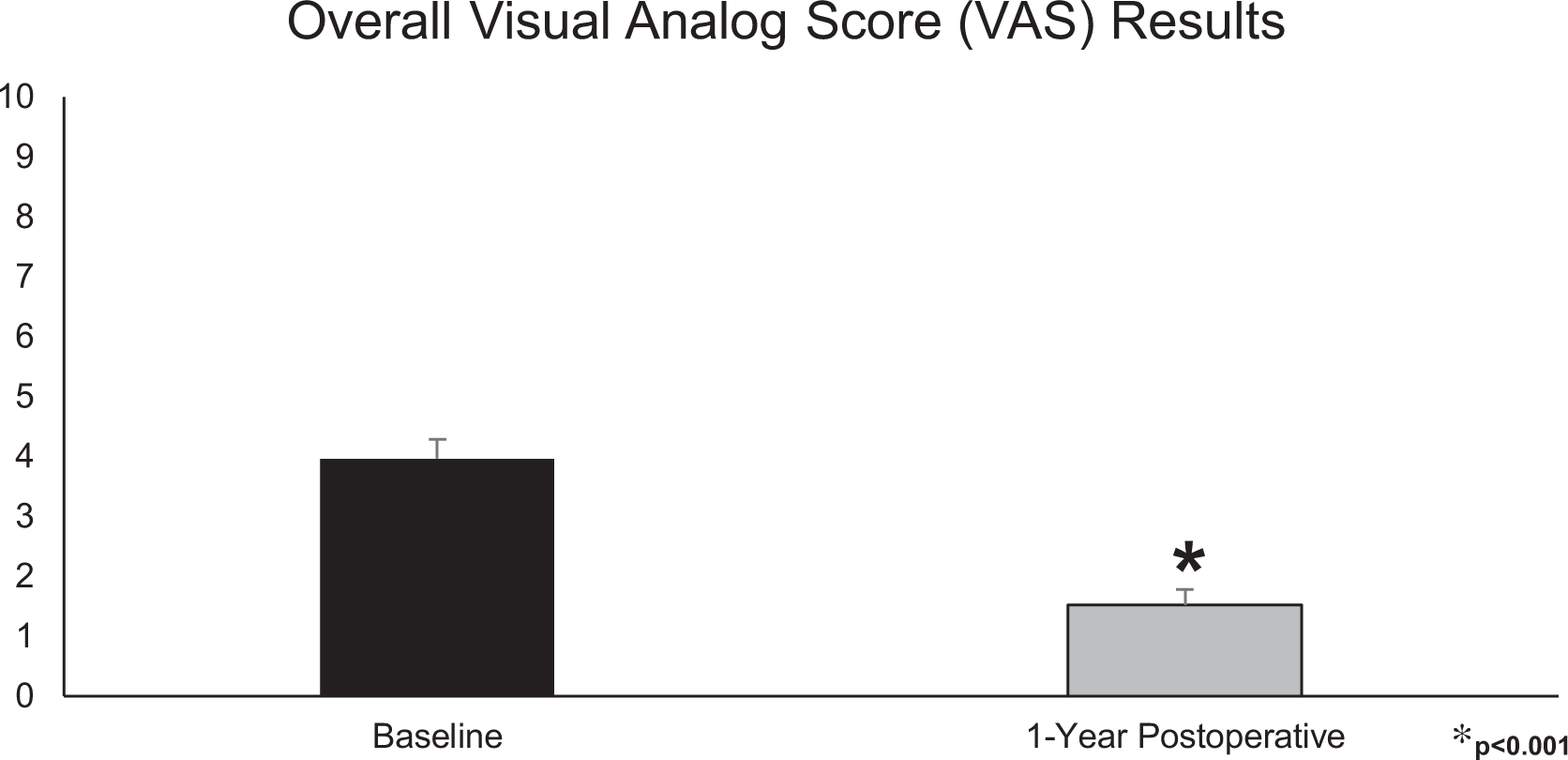
The impact of operative hammertoe correction on patient-reported pain among all patients

The impact of operative hammertoe correction on patient-reported physical and mental function among all patients
Enrolled patients were then stratified into groups based on the number of comorbidities they presented with at the time of surgery. The included comorbidities are displayed in Table 1. A total of 53 patients had 0 or 1 comorbidity, and 25 patients had greater than 2 comorbidities. Patient-reported outcomes were then compared between comorbidity groups as shown in Table 2. Patients with multiple comorbidities reported similar VAS, MCS, and PCS scores compared to those with 0 or 1 comorbidity at the preoperative and postoperative time points as well as changes over time.
Comparison of Patient-Reported Outcomes Between Comorbidity Groups.

Abbreviations: MCS, Mental Component Summary; PCS, Physical Component Summary; VAS, visual analog scale.
a Presented as average (SD).
Postoperative Complications
Postoperative complications were then compared between comorbidity groups and displayed in Table 3. Patients with 2 or more comorbidities experienced significantly higher rates of superficial wound infection (P = .034) and pathology recurrence requiring operative revision (P = .018) relative to those with 0 or 1 comorbidity. No other differences were observed in postoperative compilation rates between groups.
Comparison of Complications Between Comorbidity Groups.a

a Values are presented as n (% of comorbidity group) and odds ratio (95% confidence interval); significant values highlighted in bold.
b Univariate analysis.
c Adjusted odds of complications for patients with >2 comorbidities with ≤1 comorbidity used as reference.
Adjusted odds ratios for postoperative complications were calculated for patients with greater than 2 comorbidities in reference to patients with 0 or 1 comorbidity (Table 3). These patients were found to have a significantly increased odds of developing superficial wound infection (OR 4.18, P = .045) or a recurrence requiring operative intervention (OR 23.15, P = .032).
Discussion
This study sought to determine whether older patients with multiple comorbidities are at an increased risk for poor outcomes following hammertoe correction surgery. This study had 3 main findings: (1) in general, older patients reported significant improvements in pain and physical function following hammertoe correction surgery; (2) older patients with multiple medical conditions were not associated with poor patient-reported postoperative outcomes compared to those with 1 or no comorbidities; and (3) the presence of multiple comorbidities was associated with increased risk for superficial wound infections and deformity recurrence requiring reoperation. This is the largest study to date examining the relationship between comorbidities and outcomes for operative hammertoe correction in a geriatric population. 8,26,27,36
The current study demonstrated that hammertoe correction surgery results in an overall improvement in patient-reported pain levels (VAS 4.0 ± 2.8 decreased to 1.5 ± 2.2, P < .001) and physical function (PCS 56.2 ± 23.1 increased to 65.6 ± 23.3, P = .013) among an older patient population. There was also an improvement in mental function, though not statistically significant, even with our relatively large sample size. We previously reported similar findings when investigating hammertoe surgery outcomes. 25 In our 2018 study, we compared older and younger patients, and reported significant improvements in VAS, MCS, and PCS among the ≥65 years group from preoperative to 1-year postoperative. Rates of comorbidities were not found to differ between the 2 age groups. This study is much larger and further supports that operative correction effectively treats hammertoe deformity in geriatric patients.
Patients with multiple comorbidities were not found to be associated with worse patient-reported outcomes compared to those with 1 or 0 comorbidities. Although this finding may be due to the fact that our study is underpowered, previous studies have demonstrated that patients with preexisting comorbidities perceive operative outcomes differently. 3,28 In their 2016 publication, Backhouse et al 3 analyzed how patients with rheumatoid arthritis viewed their experience after undergoing foot surgery and noted that a multitude of factors contribute to how patients interpret the success of their operations. Patients were found to be particularly stoic and not dwelling on negative impacts of their chronic condition. 3 A possible explanation for similar measures of pain and function between comorbidity burden groups is that patients with multiple comorbidities have previously developed coping strategies, thereby affecting their self-perception of disability.
The presence of 2 or more comorbidities was demonstrated to be associated with higher rates of both superficial wound infections as well as deformity recurrence necessitating reoperation. Past comparisons have analyzed the impact of specific comorbidities on the development of superficial infections following various forefoot surgeries, though none have examined their impact on solely hammertoe correction. In their 2015 study, Bettin et al 6 studied patients who underwent 24 different types of forefoot operations and noted smokers to have a 9.1% risk of infection after surgery. Ample evidence exists showing diabetes to be related to the development of infections in elderly orthopedic patients. 4,9,18
Past studies have also shown other specific comorbidities to be associated with postoperative complications. Chronic obstructive pulmonary disease has been linked with an increased risk of complications and operative failure following orthopedic procedures. 4,7,12,19,20 Past research has shown both cardiovascular disease 34 and osteoporosis 21,23,24,31 to negatively impact bone healing, thereby providing a possible explanation for our finding of increased deformity recurrence rates requiring surgery among patients with multiple comorbid conditions.
Overall frailty, as defined by multiple comorbidities, has been linked to postoperative complications among other kinds of orthopedic surgeries. 33,38 To our knowledge, no study has previously assessed the relationship between a summative comorbidity burden or frailty and outcomes following hammertoe surgery. Nevertheless, our finding that the presence of multiple comorbidities is associated with increased rates of superficial wound development and recurrence requiring surgery agrees with the aforementioned studies.
Our study has many strengths, including a high response rate to the questionnaires, with at least 1 year of data collected on 71 of 78 patients (91.0% response rate). Validated questionnaires were used to determine the subjective assessment of pain and function (the VAS and SF-36 surveys) and obtained both preoperative and postoperative responses. 22 As a case series, it also had inherent limitations. The presence of comorbid medical conditions was based on patient interviews and not confirmed by laboratory or imaging studies. In cases of missed follow-up appointments, patients were called to conduct questionnaires over the phone, presenting the possibility for recall bias. However, studies have shown that patients can reliably recall functional status up to 2 years or more after orthopedic surgery. 13,17,35 The SF-36 PCS is standardized to the US population to have a mean of 50 and a standard deviation of 10. 14 Our study’s baseline PCS show our patient population to be higher functioning and more variable, which may make the findings from this group less generalizable. Another limitation lies with the determination of superficial infections: we did not culture wounds nor measure serum markers. This, therefore, adds an observer bias to these measurements. A post hoc power analysis resulted in a finding that our study was underpowered. Lastly, our study was conducted by 2 different attending surgeons at 2 separate institutions. Although this may increase the generalizability of our study, it also adds variability in how operative candidates were selected, which techniques were utilized, the treatment of patients postoperatively, and the interpretation of subjective outcomes.
Conclusions
This study found that geriatric patients benefited from operative correction of hammertoe deformity. However, patients with underlying comorbid conditions were found to be at increased risk for worse outcomes, as we expected. When assessing geriatric patients with comorbidities for operative hammertoe correction, foot and ankle specialists should consider not only the benefits in pain and function but also the increased risk for postoperative complications.
Supplemental Material
Supplemental Material, FAO946726-ICMJE - Comorbidities Associated With Poor Outcomes Following Operative Hammertoe Correction in a Geriatric Population
Supplemental Material, FAO946726-ICMJE for Comorbidities Associated With Poor Outcomes Following Operative Hammertoe Correction in a Geriatric Population by Samuel D. Maidman, Amalie E. Nash, Wesley J. Manz, Corey C. Spencer, Amanda Fantry, Shay Tenenbaum, James Brodsky and Jason T. Bariteau in Foot & Ankle Orthopaedics
Footnotes
Acknowledgments
The authors would like to thank Danielle Mignemi, MS, ATC, LAT, OTC, for all her support with data collection and management.
Ethics Approval
Ethical approval for this study was obtained from Emory University Institutional Review Board (ID: STUDY00000652).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.