
Abstract
Background:
Some recent studies have reported the role of the posterior malleolus as an attachment of the posterior-inferior tibiofibular ligament (PITFL) and suggested that even a small fragment should be fixed. However, there are few anatomic studies of the tibial plafond attachment of the PITFL.
Methods:
Seven Thiel-embalmed ankles were obtained. The margin of the distal tibial joint surface and the attachments of the superficial fiber of the PITFL (sPITFL) and the deep fiber (dPITFL) were identified. In the frontal view, the percentages of the attachments of the sPITFL and dPITFL of the mediolateral dimension of the posterior tibial plafond were measured. In the lateral view, the line that started from the proximal margin of the attachment of the sPITFL and parallel to the tibial axis was drawn, and the distance between that line and the posterior edge of the joint surface was measured (AP distance of the sPITFL). Then, the percentage of the AP distance of the sPITFL of the joint surface in the anteroposterior dimension of the tibial plafond was measured.
Results:
In the frontal view, the mediolateral distance of the attachment of the sPITFL was 5.0 mm, and that of the dPITFL was 19.5 mm. The percentage of the attachment of the sPITFL on the tibial plafond was 20.6%, and that of the dPITFL was 78.2%. In the lateral view, the average AP distance of the sPITFL was 0.5 mm, and the percentage in the anteroposterior dimension of the tibial plafond was 1.7%.
Conclusion:
The PITFL was attached to less than 10% of the anteroposterior dimension of the tibial plafond in most ankles. Conversely, the PITFL attached widely in the mediolateral dimension.
Clinical Relevance:
This study suggests that the size of the posterior malleolar fragment in the mediolateral dimension could help estimate how much of the PITFL attaches to the fragment which may have implications for ankle stability.
Introduction
Ankle fractures are the most common lower extremity fractures treated by orthopedic surgeons. Although numerous surgeons have agreed that the posterior malleolus should be stabilized when the fragment involves greater than 25% of the ankle articular surface, 11,16 indications for reduction and fixation of posterior malleolar fractures are controversial. Recently, many reports emphasized the importance of treatment to maintain syndesmotic stability. 2,14,16 In addition, some studies reported the role of the posterior malleolus as an attachment of the posterior-inferior tibiofibular ligament (PITFL). 8,13 The PITFL is a strong syndesmotic ligament formed by 2 components: the superficial component (sPITFL) and the deep component (dPITFL). 5 In biomechanical studies, a tear of the PITFL leads to syndesmotic instability. 2,14 That is why some reports have suggested that even a small fragment of the posterior malleolus should be fixed. 3,12
In past reports, fragment size as a percentage of the anteroposterior dimension of the articular surface was often cited as an indication for fixation. 3,8,12,13 However, it is uncertain whether the evaluation of fragment size in the anteroposterior dimension is suitable for the assessment of syndesmotic instability. There are few anatomic studies; thus, the relationship between the size of the posterior malleolar fragment and the loss of the attachment of the PITFL is unclear. 4,5 The goal of this study was to investigate the positional relationship of the tibial plafond attachment of the PITFL and the articular surface.
Materials and Methods
Approval of the ethics committee of our institution was obtained. Seven Thiel-embalmed ankles from 5 donors were obtained. All specimens were female, and the average age at death was 87.7 years (range, 86-93 years). The average height was 156.2 cm (148-160 cm), weight was 63.1 kg (39.5-78.0 kg), and body mass index was 25.6 (18.0-30.5). Of these 7 ankles, 5 were left, and 2 were right. All ankles were transected at the talocrural joint, and soft tissues were dissected to expose the margin of the distal tibial articular surface and the attachments of the sPITFL and the dPITFL. First, 1.0-mm Kirschner wires were inserted parallel to the tibial axis into the anterior and posterior margins of the distal tibial articular surface. Second, another 1.0-mm Kirschner wire was inserted at right angles to the tibial axis from the proximal margin of the attachment of the sPITFL. Finally, the medial margins of the sPITFL and dPITFL were marked by skin markers (Figure 1). Then, photographs of the front and side of the posterior malleolus were taken, and evaluation was performed by Image J. 15 In the frontal view of the posterior malleolus, the percentages of the attachments of the sPITFL and dPITFL of the mediolateral dimension of the posterior tibial plafond were measured (Figure 2). In the lateral view of the posterior malleolus, the line that started from the proximal margin of the attachment of the sPITFL and parallel to the tibial axis was drawn, and the distance between that line and the posterior edge of the joint surface was measured (AP distance of the sPITFL). Then, the percentage of the AP distance of the sPITFL of the joint surface in the anteroposterior dimension of the tibial plafond was measured (Figure 3).

Marking of the margin of the sPITFL, the dPITFL, and the distal tibial articular surface. (a) Anterior edge of the articular surface. (b) Posterior edge of the articular surface. (c) Proximal margin of the attachment of the sPITFL. (d) Attachment of the sPITFL. (e) Attachment of the dPITFL. dPITFL, deep component of the posterior-inferior tibiofibular ligament; sPITFL, superficial component of the posterior-inferior tibiofibular ligament.

Method of measurement of the distal tibial articular surface and the attachment of the PITFL in the mediolateral dimension. α: tibial plafond; β: the mediolateral distance of the attachment of the sPITFL; γ: the mediolateral distance of the attachment of the dPITFL. The percentages of the attachments of the sPITFL and dPITFL are calculated by the following formula: sPITFL = β/α*100, dPITFL = γ/α*100. dPITFL, deep component of the posterior-inferior tibiofibular ligament; sPITFL, superficial component of the posterior-inferior tibiofibular ligament.
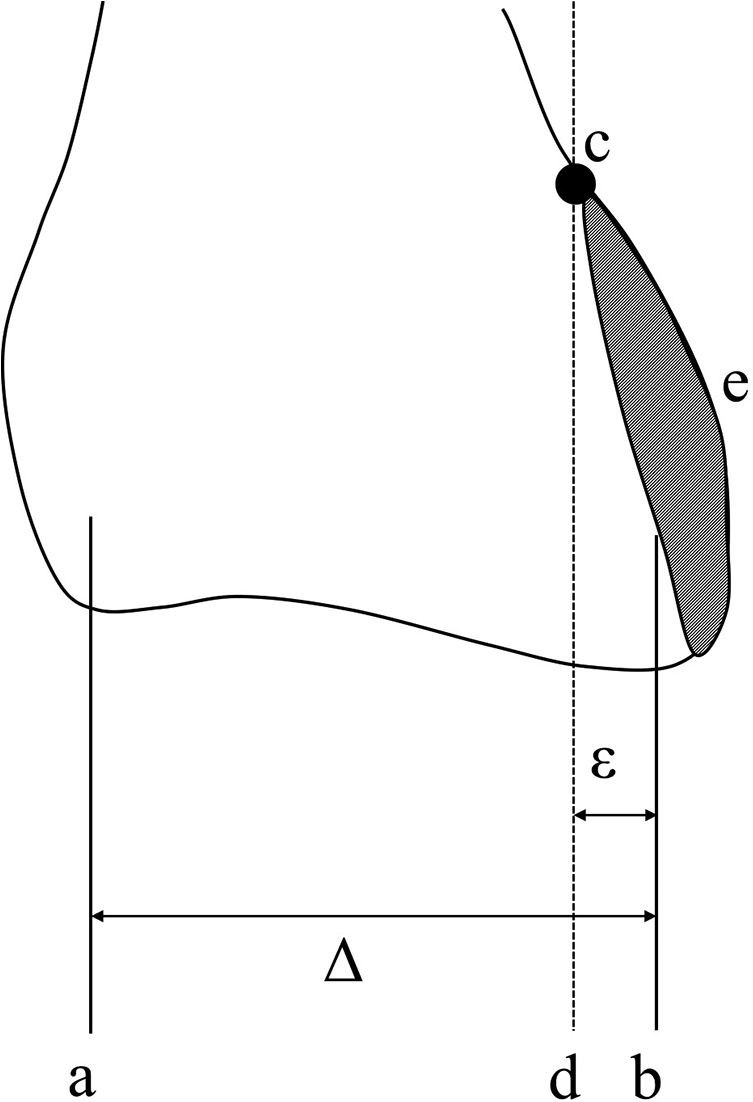
Method of measurement of the distal tibial articular surface and the attachment of the PITFL in the anteroposterior dimension. (a) The wire inserted in the anterior edge of the articular surface. (b) The wire inserted in the posterior edge of the articular surface. (c) Proximal margin of the attachment of the sPITFL. (d) The line that started from the proximal margin of the attachment of the sPITFL and parallel to the tibial axis. (e) Attachment of the sPITFL. Δ: tibial plafond; ε: the distance between the line that started from the proximal margin of the attachment of the sPITFL and parallel to the tibial axis and the posterior edge of the joint surface (AP distance of the sPITFL). The percentage of the AP distance of the sPITFL was calculated by the following formula: AP distance of the sPITFL = ε/Δ*100. dPITFL, deep component of the posterior-inferior tibiofibular ligament; sPITFL, superficial component of the posterior-inferior tibiofibular ligament.
Results
The average anteroposterior and mediolateral dimensions of the tibial plafond were 29.7 mm (28.3 to 30.8 mm) and 25.1 mm (21.8 to 28.6 mm), respectively. In the frontal view, the mediolateral distance of the attachment of the sPITFL was 5.0 mm (3.2 to 9.3 mm), and that of the dPITFL was 19.5 mm (15.4-23.3 mm). The percentage of the attachment of the sPITFL on the tibial plafond was 20.6% (12.9% to 39.4%), and that of the dPITFL was 78.2% (62.5% to 99.1%). In the lateral view, the average AP distance of the sPITFL was 0.5 mm (–2.1 to 4.6 mm), and the percentage in the anteroposterior dimension of the tibial plafond was 1.7% (–7.3% to 15.1%) (Table 1).
Measurement of the Distal Tibial Articular Surface and Posterior-Inferior Tibiofibular Ligament.

Abbreviations: dPITFL, deep component of the posterior-inferior tibiofibular ligament; sPITFL, superficial component of the posterior-inferior tibiofibular ligament.
a AP distance of the sPITFL: the distance between the line that started from proximal margin of the attachment of the sPITFL and parallel to tibial axis and posterior edge of the joint surface.
Discussion
Syndesmotic instability has been recognized widely by orthopedic surgeons, and therefore many biomechanical reports have been published. 2,14,17,18 Ogilvie-Harris et al 14 reported the contribution of each syndesmotic ligament to ankle stability. In that report, the sPITFL and dPITFL provided 8.7% and 32.7% of total ankle stability, respectively. Based on this information, Gardner et al 3 evaluated the stability of the syndesmosis with cadaveric posterior malleolar ankle fracture models. 3 The authors reported that after fixation of the posterior malleolar fragment, which was the attachment of the PITFL, syndesmotic stability was greater than with a syndesmotic screw alone. More recent studies have shown that the reduction and fixation of a posterior malleolar fragment provided syndesmotic stability and good clinical outcomes, and they suggested that even a small fragment of the posterior malleolus should be fixed. 8,12,13 However, in these previous reports, the size of the fragment that should be fixed was unclear. Although fragment size as a percentage of the anteroposterior dimension of the articular surface is often cited as an indication for fixation, the relationship between the posterior malleolar fragment and the attachment of the PITFL was uncertain. 3,8,12,13
In past anatomic reports of the tibial plafond attachment of the PITFL, the length, the width, and the size of the attachment of PITFL were varied. 1,6,7,9,10,19 This study is the first report of the tibial plafond attachment of the PITFL focused on the positional relationship with the articular surface. In the present study, in 6 of 7 ankles, the sPITFL was attached to less than 10% of the anteroposterior dimension of the tibial plafond. Moreover, in 3 ankles, the sPITFL attached posterior to the edge of the articular surface. In all ankles, the dPITFL attached just at the edge of the posterior articular surface. Based on these data, the size of the posterior malleolar fragment in the anteroposterior dimension cannot be a predictor of the remaining attachments of the sPITFL and dPITFL. On the other hand, the PITFL, especially the dPITFL, was attached widely in the mediolateral dimension. The average percentages of the sPITFL and dPITFL on the tibial plafond were 20.6% and 78.2%, respectively. Therefore, in the mediolateral dimension, the size of the posterior malleolar fragment could help estimate how much of the sPITFL and dPITFL attach to the fragment.
This study has several limitations. First, only 7 ankles of 5 specimens were investigated, and they were all from elderly women of the same racial background. Although it is difficult to obtain young specimens in our institution, further studies with a larger sample size, both sexes, and a wider range of ages and racial backgrounds could be helpful. Second, the evaluation of the attachment of the PITFL was done by macroscopic inspection. There is a possibility that there was a difference in the attachment between macroscopic and histologic evaluations. Finally, there were no data about a past history of ankle injuries or clinical symptoms, though all ankles showed no obvious findings of past injuries or operative treatment.
In conclusion, the PITFL attached to less than 10% of the anteroposterior dimension of the tibial plafond in most ankles. On the other hand, the PITFL attached widely in the mediolateral dimension. This study suggests that the size of the posterior malleolar fragment in the mediolateral dimension could help estimate how much of the sPITFL and dPITFL attach to the fragment which could have implications for syndesmotic stability.
Supplemental Material
Supplemental Material, FAO945689-ICMJE - Tibial Plafond Attachment of the Posterior-Inferior Tibiofibular Ligament: A Cadaveric Study
Supplemental Material, FAO945689-ICMJE for Tibial Plafond Attachment of the Posterior-Inferior Tibiofibular Ligament: A Cadaveric Study by Shutaro Fujimoto, Atsushi Teramoto, Ken Anzai, Yasutaka Murahashi, Yohei Okada, Tomoaki Kamiya, Kota Watanabe, Mineko Fujimiya and Toshihiko Yamashita in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the Ethics Committee of Sapporo Medical University (Approval number 28-2-56).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.