
Abstract
Background:
Active participation in patients’ own care is essential for success after Lapidus procedure. Poor health literacy, comprehension, and retention of patient instructions may be correlated with patient participation. Currently, there is no objective measure of how well patients internalize and retain instructions before and after a Lapidus procedure. We performed this study to assess how much of the information given to patients preoperatively was able to be recalled at the first postoperative visit.
Methods:
All patients between ages 18 and 88 years undergoing a Lapidus procedure for hallux valgus by the senior author between June 2016 and July 2018 were considered eligible for inclusion. Patients were excluded if they had a history of previous bunion surgery or if the procedure was part of a flatfoot reconstruction. Patients were given written and verbal instructions at the preoperative visit. Demographic and comprehension surveys were administered at their first visit approximately 2 weeks postoperatively. A total of 50 patients, of which 42 (84%) were female and 43 (86%) had a bachelor’s degree or higher, were enrolled.
Results:
Mean overall score on the comprehension survey was 6.2/8 (±1.2), mean procedure subscore was 1.8/3 (±0.64), and mean postoperative protocol subscore was 4.4/5 (±0.8). The most frequently missed question asked patients to identify the joint fused in the procedure.
Conclusion:
Although comprehension and retention of instructions given preoperatively was quite high in our well-educated cohort, our findings highlight the importance of delivering clear instructions preoperatively and reinforcing these instructions often.
Level of Evidence:
Level II, prospective cohort study.
Introduction
Successful orthopedic procedures depend not only on surgical expertise but on patients thoroughly understanding the recovery process and taking an active role in their own postoperative care. 13,18 Preoperative patient education and written instructions are crucial in facilitating this involvement. 10,13 However, in order to succeed, patients must be able to comprehend the instructions given. Unfortunately, patients frequently do not fully understand the procedures they are undergoing and are likely to forget what they are told during preoperative visits. 3,4,15 Health literacy is vital to a patient’s involvement in his or her own health and can be defined as one’s ability to obtain and understand basic health information and instructions given to make informed decisions. 1,11,12,13 Inadequate health literacy is one potential barrier to successful preoperative education, is a problem widely prevalent in orthopedic surgery patients, and may be directly linked to negative health outcomes. 1,5,8,9,11
Patient understanding of postoperative protocols and instructions is both crucial and particularly challenging in foot and ankle surgery. 12 Complex anatomy may be difficult for patients to comprehend, and postoperative restrictions (necessary to protect wounds, arthrodesis, tendon transfers, and soft tissue repairs) can be difficult to follow. This holds particularly true for the Lapidus procedure, which requires patients to protect their wounds, take medication to prevent deep vein thrombosis, remain nonweightbearing while allowing for bony healing, follow progressive weightbearing instructions, and perform range of motion exercises among other tasks required for a good recovery. Although every effort is made to educate patients on the procedure, recovery, and potential risks involved, we do not currently have an objective measure of how well patients internalize and retain this information after a Lapidus procedure. The aim of our study was to assess how much of the information given at the preoperative visit were patients able to recall at their first postoperative visit.
Methods
All study materials and activities were institutional review board–approved under a minimal-risk exemption from informed consent. All consecutive patients 18 years and older undergoing a Lapidus procedure for hallux valgus by the senior author from June 2016 to July 2018 were considered eligible for inclusion. Patients were excluded if English was not indicated as a first language in order to limit the effect of language preference on health literacy. Patients were also excluded if they had a history of previous bunion surgery as they likely would have additional understanding of the recovery based on that experience, or if the Lapidus procedure was part of a flatfoot reconstruction given the increased magnitude and different nature of that procedure.
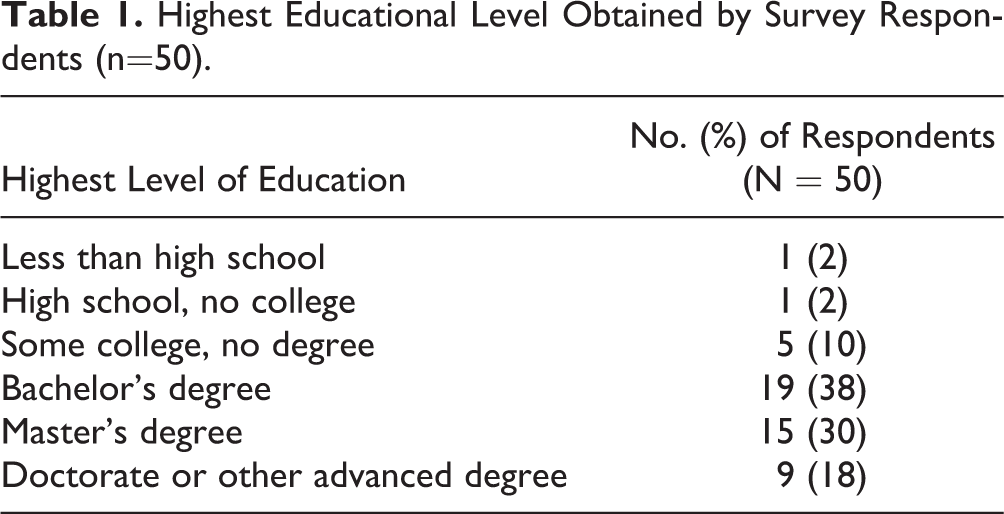
A total of 50 patients, of which 42 (84%) were female, were enrolled and completed the postoperative comprehension survey. Forty-one (82%) patients reported their race as white or white/another race whereas 9 (18%) patients reported their race as nonwhite. Four (8%) patients reported Hispanic ethnicity. Forty-three (86%) of patients had a bachelor’s degree or higher, 24 (48%) patients had a master’s degree or higher. Two (4%) patients had no college education. A detailed breakdown of demographic data is shown in Table 1.
Highest Educational Level Obtained by Survey Respondents (n=50).
All patients were seen 1-2 weeks before surgery at a routine preoperative visit, at which time they were given a standardized written postoperative instruction sheet (Figure 1). The written instructions were reviewed with the patient by the senior author and all questions were answered. The senior author routinely reviewed the surgery, including anesthesia, anatomy, the procedure to be performed, as well as the postoperative recovery, medications, and expected outcome at this visit. The written instructions summarized this information and were given to the patient to both review in the office and take home as a reference.

Handout of the postoperative instructions following the Lapidus procedure.
At the initial (2-week) postoperative visit, patients were asked to complete a demographic survey and a comprehension survey regarding information provided in the written preoperative instructions. These surveys were administered immediately before patients were seen by their surgeon. Demographic data collected included age, sex, race, education level, and history of prior orthopedic surgery. Also included were questions regarding patients’ preferences for instruction format, satisfaction with the instructions, and whether or not they had read the written instructions. The comprehension survey consisted of eight multiple-choice, single-answer questions (Figure 2). These questions were chosen to address understanding of the basic technical aspects of the planned procedure, potential complications, and interventions used to prevent them, and postoperative protocol and time course. Scores were calculated overall out of eight, consisting of a procedure subscore out of three, and a postoperative protocol subscore out of five.

Comprehension survey questions. The procedure subscore consists of 3 questions: questions 1, 2, and 4. The postoperative protocol subscore consists of 5 questions: questions 3, 5, 6, 7, and 8.
The Mann-Whitney U, or Kruskal-Wallis test when appropriate, was used to evaluate for differences in the distribution of the overall score as well as the procedure and postoperative protocol subscores based on baseline variables. Bivariate comparison with a cut-off of 55 years was performed to determine whether scores were affected by age. This cut-off was chosen based on previous studies in the literature that have examined health literacy in different age groups. 7,16,17,19 Fisher exact test, or chi-square tests when appropriate, were used to examine relationships between baseline variables and responses to individual questions. P values less than .05 were considered statistically significant.
Results
Nearly a third (30%) of patients reported a history of prior orthopedic surgery that was not a bunion correction. Most patients (92%) reported having read the postoperative protocol instructions before the initial postoperative visit. A majority (78%) of patients preferred receiving the instructions in a paper handout form whereas 16% of patients indicated that they would have preferred instructions provided via a web page. Almost all (92%) patients reported that they were overall satisfied with the instructions given to them preoperatively.
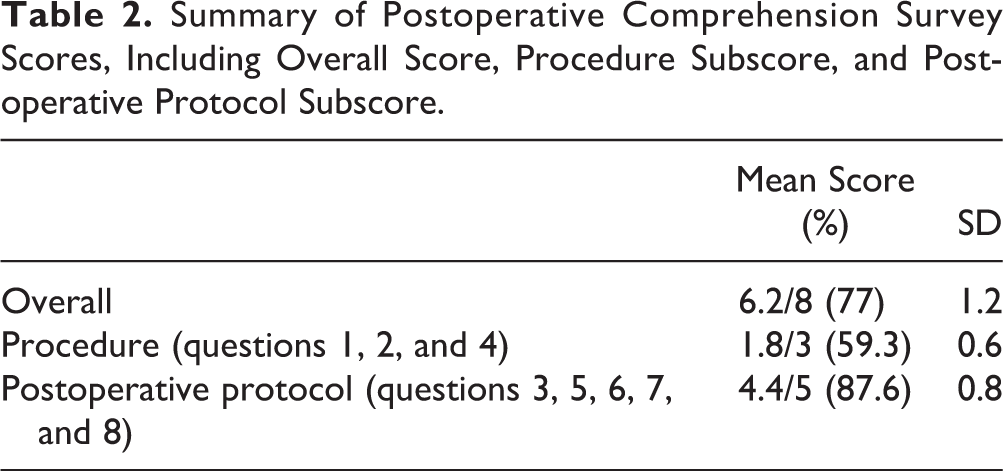
Mean overall score on the comprehension survey was 6.2 (±1.2) out of 8 points. Mean procedure subscore was 1.8 (±0.6) out of 3 points, and mean postoperative protocol subscore was 4.4 (±0.8) (Table 2). Notably, the most frequently missed question was question 1, which is included in the procedure subscore. This question asked patients to identify the joint fused in the procedure, and only 10% of patients (n=5) answered correctly. The second most frequently missed question was question 7, which asked patients to recall the amount of time needed before returning to low-impact activity, which 66% of patients (n=33) answered correctly (3 months postoperatively) (Table 3).
Summary of Postoperative Comprehension Survey Scores, Including Overall Score, Procedure Subscore, and Postoperative Protocol Subscore.
Correct Responses for Each of the Comprehension Survey Questions (N = 50).

Abbreviations: CAM, controlled-ankle motion; NWB, nonweightbearing; PT, physical therapy.
There were no significant differences in overall score or either subscore when analyzed by age group (≥55 years vs <55 years), gender, race, ethnicity, education level, instruction format preference, or satisfaction with the instructions. Overall, the differences in scores did not reach statistical significance in association with reported reading of the instructions before the initial postoperative visit.
When questions were analyzed individually, question 7 regarding time to return to low impact activity was missed by men significantly more frequently (6/8, 75%) than by women (11/42, 26.2%) (P = .008). Question 7 was also missed more frequently by patients with a bachelor’s degree or higher (17/43, 39.5%) vs patients with less than a bachelor’s degree (0/7) (P < .001); however, patients with less than a bachelor’s degree made up only 14% of the cohort.
Discussion
One of the challenges in foot and ankle surgery is that each procedure is vastly different, with varying anatomy, goals, and postoperative recovery. We therefore chose to focus on evaluating comprehension in a single condition, the Lapidus procedure, because it is commonly performed at our institution and requires a rather lengthy recovery. In this cohort we found that recall of instructions given preoperatively was overall quite high in patients who underwent a Lapidus procedure. Given the generally high level of education and mostly Caucasian cohort, our results seem to corroborate with previously published findings by both Rosenbaum et al and Noback et al, who demonstrated that patients with less than a college-level education and non-Caucasian race were associated with decreased health literacy as measured using the Literacy in Musculoskeletal Problems (LiMP) questionnaire. 8,14 A study by Crepeau and colleagues used a postoperative questionnaire to survey how much information patients recalled from preoperative informed consent. The authors reported that on average patients only recalled 59.5% of that information at the first postoperative visit following elective orthopedic surgery. 3 Although recall rates in our study were higher overall, our cohort had far fewer patients with no college education.
Interestingly, the most frequently missed questions were regarding anatomy (asking patients to name the joint fused in the procedure) and about a specific time period to return to low-impact activity. It is well accepted that the use of medical terminology can be confusing to patients, and while there is no way to definitively say whether recall that the first tarsometatarsal joint was fused relates to outcomes, it is a good example of a detail that may be easily forgotten because it is an unfamiliar term to most patients. 2 Similarly, recall of the time to resumption of low-impact activity may have been diminished because “6 weeks” may sound arbitrary to patients and “low-impact activity” is a broad category compared to a specific action such as “being nonweightbearing” or “beginning physical therapy.” This suggests that the addition of other methods of reinforcing this information, such as web-based materials and videos, may be beneficial.
Although details of the surgery, including the postoperative instruction sheet, were carefully discussed at the preoperative visit between the senior author and each patient, we chose to test comprehension of instructions at a singular time point. At the conclusion of the preoperative visit, patients were asked if they understood the details of their surgery and were encouraged to ask questions if further clarification was needed. We did not administer the survey at this time point as this was felt to test immediate recall, and instead chose to administer this survey at the first postoperative visit (2 weeks), after patients had time to participate in their postoperative management. This methodology is identical to a previous study by Kadakia et al of 146 orthopedic trauma patients undergoing fracture fixation, in which patient comprehension was assessed using a comprehension survey at the first postoperative visit (2-3 weeks following surgery). 6 The authors not only reported a similar comprehension score of 2.54 (±1.27) out of 5 possible points, but also noted similar trends in knowledge deficits in which only 47.9% of patients who knew the bone they fractured and only 18.5% knew the expected healing time. 6 The results of the current study, although assessed using a different comprehension survey with different questions, further highlights potential areas of patient comprehension that can be improved. Additionally, other variables of interest, such as the presence of family members at the visit, may be worth investigating in order to better understand how we can improve patient understanding of their operative procedures.
Our study has some limitations. First is the homogeneity of the cohort and that no power analysis was performed, which may contribute to a lack of statistical power. We strove to mitigate this effect by keeping exclusion criteria minimal and approaching all consecutive patients who had undergone a Lapidus procedure. However, the cohort reflects the practice of the senior author who participates in the majority of commercial insurances in a large metropolitan area. A further potential limitation is that the instrument used to measure comprehension/recall has not been validated, and the instrument may not be universally applicable given the variability in postoperative protocols between other surgeons. Despite this, we feel that this instrument does effectively address important details of the preoperative patient instructions, and could be easily modified to accommodate different details of the postoperative plan while retaining the same overall format. It could also be adjusted for different types of procedures with different postoperative protocols. Future directions for this study should seek to evaluate comprehension and retention in other common foot and ankle procedures, such as total ankle replacement and ankle arthrodesis, flatfoot reconstruction, and first metatarsophalangeal surgeries. Future studies to correlate measures of comprehension with metrics for operative outcomes, such as patient-reported outcomes and postoperative complications, are needed to more rigorously assess these relationships.
In conclusion, our findings demonstrate that while information and instructions given preoperatively are often well comprehended and retained, particularly among well-educated patients, patients will frequently forget isolated details about the procedure and the postoperative plan. While these may seem like trivial points that get lost in the shuffle as a patient prepares for surgery, our findings serve as a reminder of the importance of providing clear instructions in simple language during preoperative planning and counseling, and continuing to reinforce instructions at successive postoperative visits.
Supplemental Material
Supplemental Material, FAO940221-ICMJE - Health Literacy and Recall of Postoperative Instructions in Patients Undergoing the Lapidus Procedure
Supplemental Material, FAO940221-ICMJE for Health Literacy and Recall of Postoperative Instructions in Patients Undergoing the Lapidus Procedure by Jonathan H. Garfinkel, Amelia Hummel, Jonathan Day, Andrew Roney, Mackenzie Jones, Andrew Rosenbaum and Scott J. Ellis in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the Hospital for Special Surgery IRB (ID: 2015-397).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.