
Abstract
Background:
The state of Ohio implemented legislation in August of 2017 limiting the quantity of opioids a provider could prescribe. The purpose of this study was to identify if implementation of legislation affected opioid and nonopioid utilization in patients operatively treated for ankle fractures in the initial 90-day postoperative period after controlling for injury severity and preoperative narcotic usage.
Methods:
A retrospective review of 144 patients treated for isolated ankle fractures in a pre-law group (January 2017–July 2017; n = 73) and post-law group (January 2018–July 2018; n = 71) was completed using electronic medical records and a legal prescriber database. Total number of opioid prescriptions, pills, milligrams of morphine equivalents (MMEs), and nonopioid prescriptions were recorded. Multiple regression analysis was run to identify predictors of opioid prescribing after controlling for law group, demographic, preoperative narcotic use, and injury severity characteristics.
Results:
Mean MME prescribed per patient significantly decreased from 817.2 MME pre-law to 380.9 post-law (P < .01). Mean number of opioid pills prescribed per patient decreased from 99.1 in the pre-law group and 55.3 in the post law group (P < .001), respectively. Multiple linear regression analysis to predict the mean number of opioid pills prescribed was statistically significant (R
2 = 0.33; P < .001), with law group adding significantly to the prediction (P < .001). The multiple linear regression analysis to predict MME per patient was found to be statistically significant (R
2 = 0.31; P < .001), with the law group contributing significantly (P < .001
Conclusion:
The Ohio prescriber law successfully contributed to the decreased number of opioid pills and MME prescribed in the initial 90-day postoperative period after controlling for injury severity and preoperative narcotic usage. Policies on opioid prescriptions may serve as an important public health tool in the fight against the opioid epidemic.
Level of Evidence:
Level III, retrospective comparative series.
Introduction
Opioid medications are commonly prescribed in orthopedic clinics, and their use has increased over the past 3 decades. 10,12 It has become the most common cause of accidental death in the United States. 10 It also has been designated as an epidemic, and action has been taken in the interest of public safety. 9 Orthopedic surgeons are among the providers that prescribe the most narcotics. 18 In light of this, they have an opportunity to make an impact on this new health reform. 3,11
A number of states across the country have begun prescription drug monitoring programs to address narcotic abuse and misuse. The state of Ohio implemented legislation in August of 2017, limiting the quantity of opioid medications a provider could prescribe for the treatment of acute pain. Some of the changes include limiting prescriptions for 7 days during an acute pain episode and the total morphine milligram equivalents (MMEs) cannot exceed an average of 30 per day. This may impact the management of pain by orthopedic surgeons where balancing patient pain and satisfaction postoperatively in a safe and legal manner can be a challenging, yet necessary, task for providers.
Patterns of opioid prescriptions have been recently studied in the literature among various orthopedic subspecialties. 1,4,16,19 Glogovac and colleagues recently published evidence that implementation of prescriber laws can decrease the number of opioid pills and MMEs per prescription in patients with ankle fractures. 6 However, their study lacked control for various factors that may affect prescription patterns. One topic of interest has been the effect of preoperative opioid use on postoperative opioid use. Westermann et al 20 and Anthony et al 1 found that preoperative opioid use is predictive of postoperative opioid use in a dose-dependent manner for anterior cruciate ligament reconstruction and rotator cuff surgery patients. Additionally, there is some evidence in ankle fractures that injury severity or procedure type may predispose patients to persistent opioid use. 7
In light of emerging trends in the literature demonstrating that preoperative opioid use and injury severity portends an increased risk for postoperative opioid use, studies that clearly control for these variables are needed to make more definitive conclusions on the effect of opioid legislation on prescribing patterns. The purpose of this study was to evaluate whether prescription patterns of opioids in the immediate 90-day postoperative period were affected by implementation of legislation after controlling for demographics, injury severity and preoperative opioid usage. Furthermore, we investigated nonopioid prescriptions to determine whether implementation of the opioid legislation played a role in displacing opioid pain medication prescriptions to other nonopioid analgesics. We hypothesized that opioid legislation would significantly affect opioid prescriptions patterns irrespective of characteristics known to modify their consumption.
Methods
After institutional review board approval, a retrospective review was performed to identify patients who were operatively treated for isolated ankle fractures during two 6-month periods at a single institution. Patients were identified using CPT codes 27766, 27769, 27784, 27792, 27814, 27822, 27823, and 27829 (Appendix 1). Two hundred eighty patients were on the initial report and screened for possible inclusion. Patients were screened for operative treatment of isolated ankle fractures. Patients who sustained concomitant injuries or had chronic injuries (eg, osteoarthritis) were excluded. A total of 144 patients met inclusion criteria and were included in the study. Patients were divided into a pre-law group from January 2017 to July 2017 (n = 73) and a post-law group from January 2018 to July 2018 (n = 71). Classifications of injury severity included open vs closed injuries, isolated malleolar vs bimalleolar vs trimalleolar fractures, and syndesmotic involvement. The electronic medical records were reviewed for patient demographics, injury characteristics, and treatment strategies.
Preoperative narcotic use was defined as acute (first prescription for opioid use within 30 days of surgery), exposed (opioid use within a 1-year period preoperatively, but no continuous use), intermediate sustained use (continuous use of opioids <6 months preoperatively), and chronic sustained use (continuous use of opioids >6 months preoperatively). Postoperative narcotic prescriptions were reviewed using the Ohio Automated Rx Reporting System (OARRS), a legal prescriber database. Total number of prescriptions, pills, and milligrams of morphine equivalent (MME) per patient prescribed during the initial 90-day postoperative period were documented and compared between those treated before implementation of opioid legislation to those treated after. It is worth noting that the number of prescriptions was not recorded utilizing the electronic medical record. Therefore, to prevent overestimating the data, OARRS was utilized because it only reports prescriptions that were filled and not all prescriptions given by providers. For the limited number of patients living out of state, and whom had no OARRS record, the electronic medical record was utilized.
The same extraction was performed for nonopioid analgesics from the electronic medical records. Non-opioid analgesics that were included in this study were nonsteroidal anti-inflammatory drugs (eg, ibuprofen, aspirin, naproxen, ketorolac, meloxicam, celecoxib), muscle relaxants (eg, cyclobenzaprine), benzodiazepines (eg, lorazepam, clonazepam, alprazolam), gabapentinoids (eg, gabapentin, pregabalin), and acetaminophen (Appendix 2).
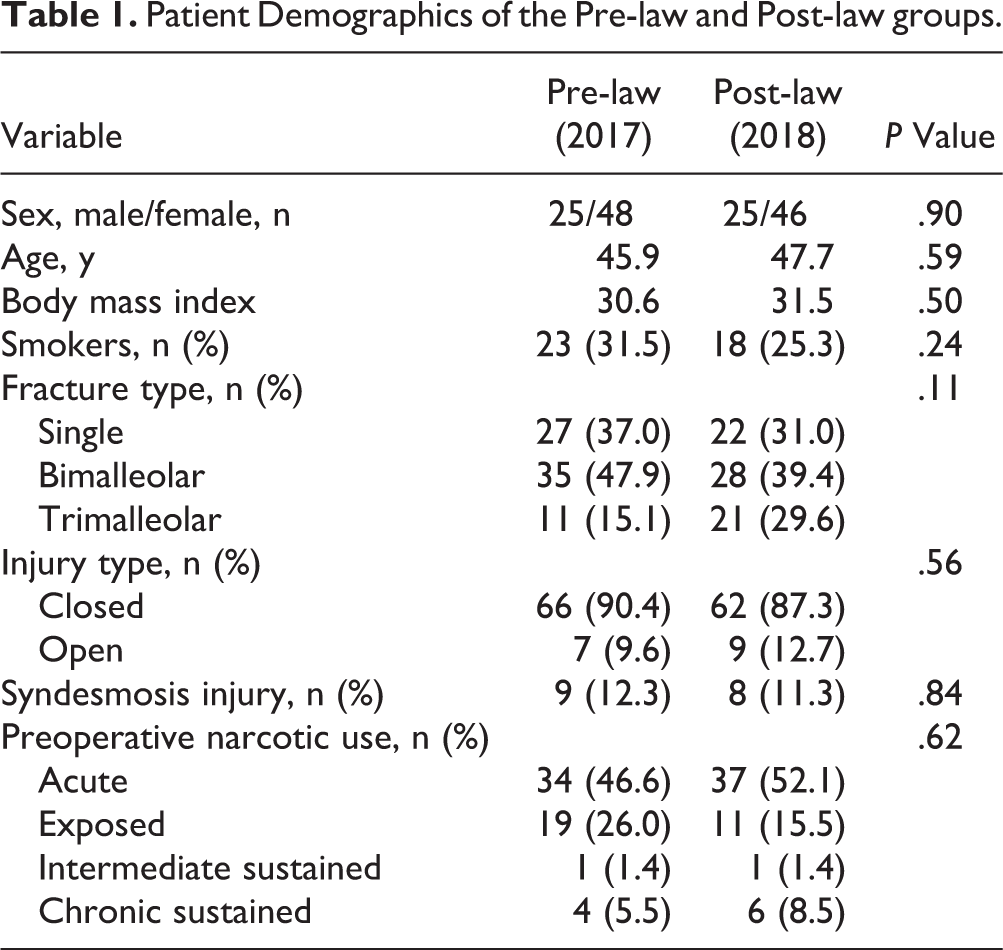
The mean patient age was 46.8 years; 45.9 years and 47.7 years in the pre-law and post-law group, respectively (P = .59). More than three-fourths (79.5%; 58/73) of patients in the pre-law group and 77.5% (55/71) in the post-law group had some preoperative narcotic use, although no statistically significant difference was found between the 2 groups (P = .62). There were no significant differences in fracture type (single, bimalleolar, and trimalleolar), injury type (closed/open), and syndesmotic injuries between the pre-law and post-law groups (Table 1). Further demographics and injury characteristics are described in Table 1.
Patient Demographics of the Pre-law and Post-law groups.
Statistical Analysis
Descriptive statistics such as mean and range calculations were utilized on all continuous variables. Continuous variables such as the number of prescriptions, number of pills, and MME were compared for those undergoing surgery before the Ohio Prescriber law went into effect to those that had surgery after using t tests. Frequencies and percentages were calculated for all categorical variables. Pearson chi-square test was used to compare proportions of categorical variables. Multiple linear regression analysis was run to identify predictors of mean number of opioid prescriptions, mean number of opioid pills, MME per patient, and number of nonopioid prescriptions in the initial 90-day period from pre and post-law groups, age, body mass index (BMI), gender, smoking history, preoperative narcotic use, and injury categories. R 2 was used to determine the percentage of variation in the dependent variable that is explained by the independent variables used in the multiple linear regression analysis. Significance was defined as a P value <.05. Statistical tests were performed using R. 13
Results
The mean number of opioid prescriptions prescribed per patient in the immediate 90-day postoperative period was 1.4 in the pre-law group and 1.2 in the post-law group (P = .43). Mean MME prescribed per patient significantly decreased from 817.2 MME pre-law to 380.9 post-law (P < .01) in the immediate 90-day postoperative period. Mean number of opioid pills prescribed per patient in the immediate 90-day postoperative period was 99.1 in the pre-law group and 55.3 in the post-law group (P < .001). Mean number of nonopioid prescriptions per patient in the immediate 90-day postoperative period decreased from 1.9 in the pre-law group to 1.6 in the post-law group (P = .28). Further opioid and nonopioid prescription data are recorded in Table 2.
Opioid and Nonopioid Prescription Data in the Pre- and Post-law Groups During the Initial 90-Day Postoperative Period.

Abbreviation: MME, milligrams of morphine equivalents.
* Values are expressed as means.
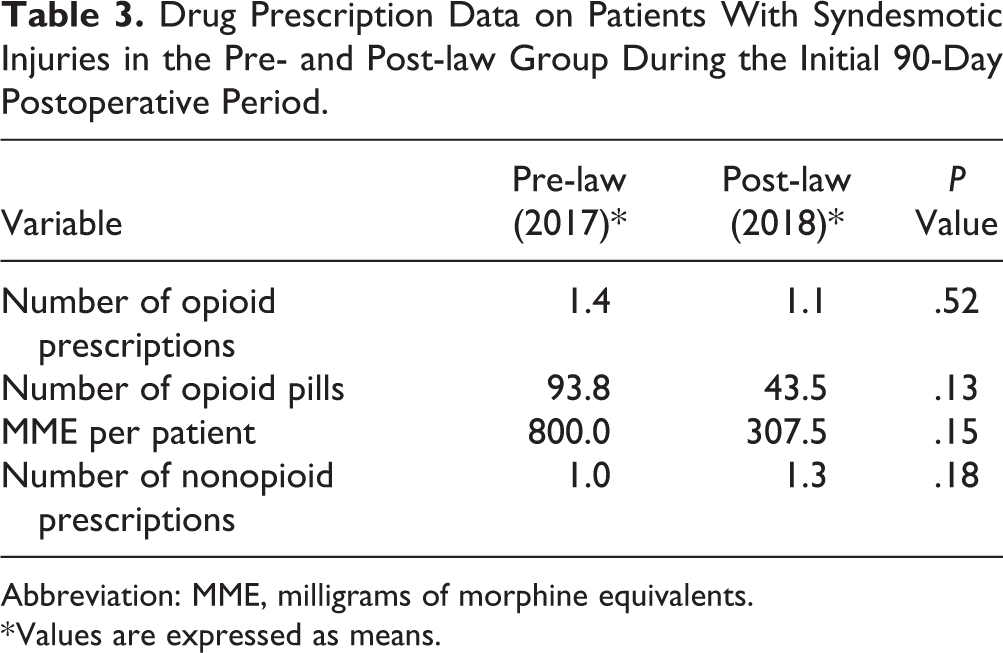
Syndesmotic injury was further classified as a subgroup, and there were no significant differences found in the initial 90-day postoperative period in opioid or nonopioid prescriptions between the pre- and post-law groups (Table 3). In comparing patients with syndesmotic injuries to patients without syndesmotic injuries during the initial 90-day postoperative period, there were no significant differences in any of the opioid prescription categories in the pre-law or post-law periods (Table 4). We found that the mean number of nonopioid prescriptions was higher in patients with nonsyndesmotic injuries compared to syndesmotic injuries in the total cohort (1.8 vs 1.2; P = .005), as well as the pre-law period (2.0 vs 1.0; P < .001).
Drug Prescription Data on Patients With Syndesmotic Injuries in the Pre- and Post-law Group During the Initial 90-Day Postoperative Period.
Abbreviation: MME, milligrams of morphine equivalents.
* Values are expressed as means.
Drug Utilization of Patients With Syndesmotic Injuries vs Nonsyndesmotic Injuries: Total Cohort and Pre-law and Post-law Groups.

Abbreviation: MME, milligrams of morphine equivalents.
* Values are expressed as means.
The multiple linear regression analysis significantly predicted the number of mean opioid prescriptions (R 2 = 0.18; P = .002) in the initial 90-day postoperative period, with only preoperative narcotic use adding significantly to the prediction (P < .001). The multiple linear regression analysis to predict the mean number of opioid pills prescribed in the initial 90-day period was statistically significant (R 2 = 0.33; P < .001), with pre and post-law group, preoperative narcotic use, and open/closed injury adding significantly to the prediction, respectively (P < .001; P < .001; P = .047). The multiple linear regression analysis to predict MME per patient in the initial 90-day period was found to be statistically significant (R 2 = 0.31; P < .001), with pre- and post-law group and preoperative narcotic use contributing significantly (P < .001). The multiple linear regression analysis to predict nonopioid prescriptions in the initial 90-day postoperative period was not significant overall (R 2 = 0.10; P = .68) and none of the individual variables analyzed were found to be significant predictors.
Discussion
Awareness and understanding of opioid prescriptions and their implications in caring for the orthopedic surgery patient has increased recently. Many factors, such as preoperative opioid usage and injury severity, can alter the amount of opioids prescribed to a postoperative patient. 1,2,7,8,20 Our study provides evidence that implementation of opioid prescription legislation remains a significant predictor of the number of opioid pills and MMEs per prescription after controlling for variables known to modify prescription patterns.
Prior studies on opioid prescription patterns following legislative changes have been performed. A study by Reid et al aimed to identify the effects Rhode Island legislation had on narcotic prescriptions for spine surgery. The study found greater than 50% reduction in pills and MME for the initial and 30-day postoperative period among all patients, regardless of preoperative tolerance, from the pre-law to post-law period. 14 Similarly, a study on 6 common orthopedic procedures demonstrated that the post-law group had decreases in initial pill quantity and MME, regardless of preoperative opioid exposure. 15 Glogovac et al found a decrease in the initial number of opioid pills and MMEs per prescription after implementation of legislation in patients with ankle fractures. 6 In line with previous studies, our study found that there was a significant decline in the mean number of opioid pills and MME in the immediate 90-day postoperative period after implementation of the Ohio opioid prescriber law.
Preoperative narcotic use has been found to predict increased opioid demand and dependence in other orthopedic specialties. 1,2,8,20 In ankle fractures, previous studies have demonstrated that patients with isolated malleolar fractures have lower levels of pain compared to other fracture types. 17 Additionally, a study by Egol et al found that syndesmotic injury is predictive of more severe injury and worse outcomes. 5 Our study found that patients with syndesmotic injuries did not necessitate a higher number of opioid prescriptions or pills compared to patients with nonsyndesmotic injuries. A strength of our study compared to previous reports on the effect of legislation on opioid prescription patterns in ankle fractures is that we were able to control for these various injury severity characteristics and preoperative narcotic use in our analysis. Our study identified that post-law group remained a significant predictor for the mean number of opioid pills and MME per patient in the initial 90-day postoperative period after controlling for these variables. This data provides further support that opioid legislation can be effective at curbing opioid consumption in patients with ankle fractures, irrespective of their injury severity or previous opioid consumption.
Implementation of the opioid prescriber law, although significantly reducing the number of opioid pills prescribed in the initial 90-day postoperative period, did not alter the utilization of nonopioid prescriptions. There was a reduction in the number of nonopioid analgesics prescribed in the initial 90-day postoperative period, albeit not statistically significant. Additionally, multiple linear regression analysis did not find post-law group to be a significant predictor of nonopioid prescriptions in the immediate 90-day period. Interestingly, we found that patients with more severe injuries (eg, syndesmotic injuries) were using a lower number of nonopioid prescriptions at the 90-day postoperative period in the pre-law subgroup compared to patients with less severe injuries (eg, nonsyndesmotic); however, syndesmotic injury was not found to be a significant predictor of opioid or nonopioid prescriptions on multiple linear regression analysis.
The data suggest that while patients are taking less narcotics during the acute phase postoperatively, the fact that the nonopioid analgesics are not increased overall in ankle fractures, may be attributed to patient education that some pain is acceptable and are thus tolerating the number of narcotics they have received without the need to also consume nonopioid analgesics. It may also be due to an underestimation of the number of nonnarcotics used because many may be purchasing over-the-counter NSAIDs which would be undetected during electronic medical record extraction, since no prescription would be ordered. As the number of narcotics prescribed beyond the acute postoperative period decreases, patients still dealing with postoperative pain who are not receiving narcotic prescriptions, may be utilizing over-the-counter analgesics for chronic pain.
This study has some limitations. The first is attributed to its retrospective design, which is inherently dependent on accurate and complete reporting. To account for this, we utilized OARRS as confirmation for accurate data. Another limitation is that certain factors such as a history of addiction and psychiatric disorders, that perhaps can influence analgesic consumption, may not have been adequately excluded. Third, some of the common over-the-counter nonsteroidal anti-inflammatory drugs can be purchased without a prescription. Our study only accounted for patients receiving these drugs from prescriptions and did not consider if the patient is taking over-the-counter medications. Fourth, patients may have sought care outside of our network postoperatively, whether due to chronic pain or dissatisfaction with their surgeon. Unfortunately, we were not able to properly assess the follow-up of these patients and the true value of the implementation of legislation on chronic opioid utilization could not be calculated. Finally, a sample size calculation was not performed and is a weakness in the study design.
In conclusion, although there is preliminary data on the effects of prescriber laws on opioid prescription patterns, to our knowledge, this is the first study to evaluate if implementation of such laws successfully reduces prescriptions in patients with ankle fractures after controlling for preoperative narcotic use and injury severity. The reduction in number of opioid pills and MME per patient, as well as both remaining significant predictors after controlling for various factors that affect acute pain, further strengthens the growing evidence that legislation can be an effective measure in managing opioid consumption in an orthopedic patient population in the initial postoperative period. Future studies evaluating the long-term effects of opioid legislation are needed to determine the true value these laws have in helping fight the opioid epidemic.
Supplemental Material
Supplemental Material, FAO939501-ICMJE - Effect of Opioid Limiting Legislation on Postoperative Opioid Utilization in Patients Treated for Ankle Fractures
Supplemental Material, FAO939501-ICMJE for Effect of Opioid Limiting Legislation on Postoperative Opioid Utilization in Patients Treated for Ankle Fractures by Connor G. Hoge, Robert N. Matar, Colin D. F. Cotton, Michael G. Rubeiz, Tonya L. Dixon and Richard T. Laughlin in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Approved by University of Cincinnati Medical Center IRB: #2018-6875.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1
Appendix 2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.