
Abstract
Background:
Lateral sliding calcaneus osteotomies are common procedures to correct hindfoot varus deformities. Shifting the calcaneal tuberosity laterally (lateralization) can lead to tarsal tunnel pressure increase and tibial nerve palsy. The purpose of this cadaveric biomechanical study was to investigate the correlation of lateralization and pressure increase underneath the flexor retinaculum.
Methods:
The pressure in the tarsal tunnel of 12 Thiel-fixated human cadaveric lower legs was measured in different foot positions and varying degrees of calcaneal lateralization.
Results:
The mean pressure increased from plantarflexion (PF) to neutral position (NP) and from NP to hindfoot dorsiflexion (DF), and with increasing amounts of lateralization of the calcaneal tuberosity. The mean baseline pressure in PF was 1.5, in NP 2.2, and in DF 6.5 mmHg and increased to 8.1 in PF, 18.4 in NP, and 33.1 mmHg with 12 mm of lateralization. The release of the flexor retinaculum significantly lowered the pressure.
Conclusion:
Increasing pressures were found in the tarsal tunnel with increasing lateralization of the tuberosity and with both dorsiflexion and plantarflexion of the ankle.
Clinical Relevance:
A pre-emptive release of the flexor retinaculum for a lateralization of the calcaneal tuberosity of more than 8 mm should be considered, especially if specific patient risk factors are present. No tibial nerve palsy should be expected with 4 mm of lateralization.
Introduction
The tarsal tunnel is located at the lower medial hindfoot and encompasses the tibialis posterior artery and veins, the tibial nerve, and the tendons of the flexor hallucis longus (FHL), flexor digitorum longus (FDL), and tibialis posterior muscles (TP). The roof of the tarsal tunnel consists of the flexor retinaculum. Proximally, there is a gradual transition from the crural fascia to the flexor retinaculum that continues distally to the fascia of the abductor hallucis muscle. 21 The neurovascular bundle lies between the FDL tendon anteriorly and the FHL tendon posteriorly, and between an intermediary intertendinous aponeurosis medially and the deep aponeurosis laterally (Figure 1). 24 The boundaries of the flexor retinaculum are defined as follows: 2 cm proximal from and distal to a line extending from the tip of the medial malleolus to the calcaneal tuberosity. 7
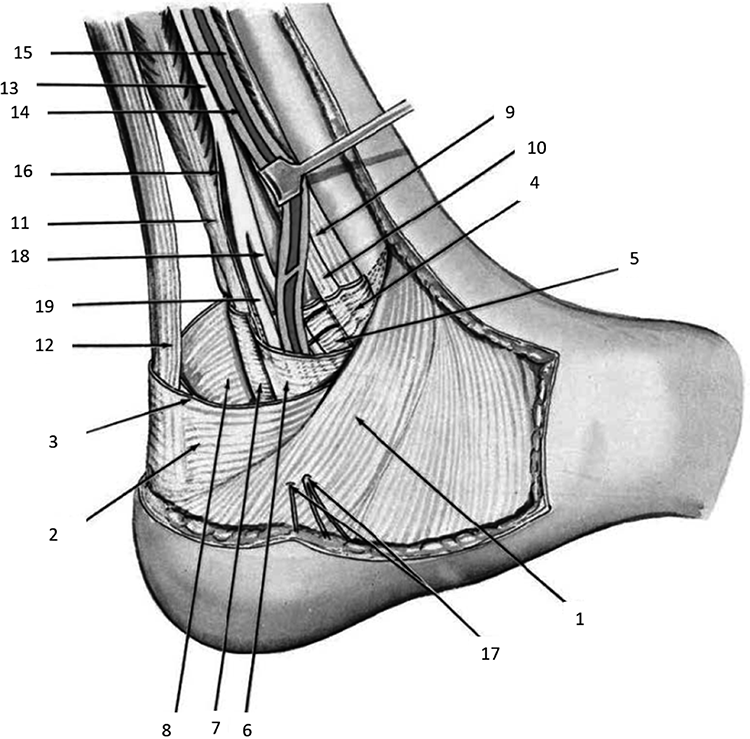
Anatomy of the tarsal tunnel. 1, Flexor retinaculum; 4, deep aponeurosis; 5, intermediary intertendinous aponeurosis forming floor of neurovascular compartment; 6, deep aponeurosis forming roof of neurovascular compartment and continuing over tunnel of flexor halluces longus tendon; 9, tibialis posterior tendon; 10, flexor digitorum longus tendon; 11, flexor hallucis longus tendon; 13, posterior tibial nerve; 14, 15, posterior tibial artery and vein. Reprinted with permission from Wolters Kluwer Health. 12
Hindfoot deformities are complex disorders and can be treated conservatively or surgically. One such surgical option is the calcaneus osteotomy. Possible variations of this include a translational single-plane osteotomy (Figure 2), a closing/open-wedge rotational osteotomy, or rotational Z-osteotomy with or without additional translation. 27 By shifting the calcaneal tuberosity laterally, the flexor retinaculum is effectively tightened (Figure 3) narrowing the space below. 6 Thus, depending on the amount of required correction, a lateralizing calcaneus osteotomy can potentially compress the tibial nerve. This constellation was first described in 1960 by Kopell, and later referred to as “tarsal tunnel syndrome” in 1962 by Keck and Lam. 13,17 This syndrome typically is associated with burning pain, paresthesia, and numbness in the area supplied by the tibial nerve. 17 Without decompression, symptoms can progress to irreversible sensory loss, muscle weakness and atrophy, as well as trophic disturbances. 1

Fluoroscopy of a left foot from (left) lateral and (right) axial after a fixed lateralized translational single plane osteotomy.
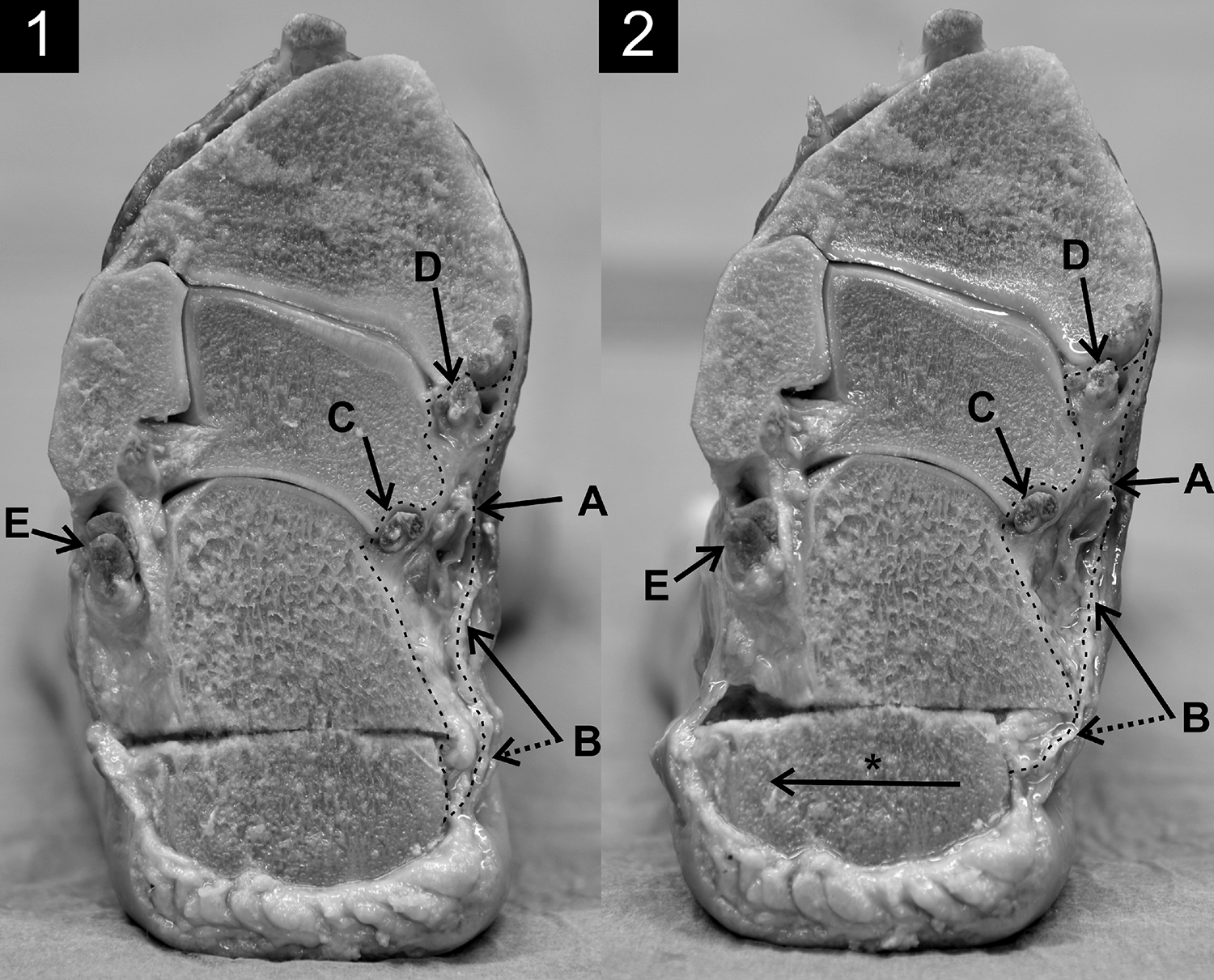
Posterior view on a cross-section of a left foot, (1) before and (2) after lateralization (*). The cut goes along the retinaculum flexorum. The lateralization of the distal calcaneus fragment directs the distal attachment of the retinaculum flexorum around the proximal calcaneus edge (dotted line of B), thereby narrowing the space in the tarsal tunnel (dotted area). A, Tibial nerve with tibialis posterior artery and vein; B, flexor retinaculum; C, tendon of flexor hallucis longus; D, tendons of tibialis posterior and flexor digitorum longus; E, tendon of peroneus longus and peroneus brevis.
In this study, we aimed to quantify the change in pressure below the flexor retinaculum in relation to the degree of calcaneal tuberosity lateralization and hypothesized that the pressure would change depending on the foot position and rise with increasing degrees of lateralization. Using this information, surgical strategies can be adopted to reduce potential compression of the tibial nerve and reduce the likelihood of developing tarsal tunnel syndrome.
Materials and Methods
Materials
Human cadaveric material used for this study was processed according to the current Federal Act on Research involving Human Beings (Human Research Act [HRA]) and in accordance with current guidelines of the Academy of Medical Sciences. The donors formally consented to use for research purposes by signing the required donation forms. Twelve Thiel-fixated human cadaveric leg specimens with a normal range of ankle motion (dorsiflexion/plantarflexion 10-0-20° or more) were used for the study. Specimens with obvious hindfoot deformities, previous fractures, or operative treatments were excluded.
For the pressure measurements, a neurosurgical “parenchymal probe 3ps” pressure sensor and “ICP Monitor HDM 29.3” (Spiegelberg GmbH & Co. KG, Hamburg, Germany) were used. With a diameter of 1.3 mm and an accuracy of 2 mmHg, the probe is comparable to other devices in clinical use.
Surgical Procedure
Pressure sensor application
To expose the tibial nerve and flexor retinaculum, the skin was incised from 1 cm posterior to the posteromedial edge of the tibia to 1 cm posterior to the tibialis posterior tendon giving an incision length of approximately 15 cm. After dissection of the superficial and deep crural fascia, the nerve was identified 5 to 10 cm proximal to the flexor retinaculum. The sensor probe was inserted alongside the nerve and carefully advanced distally, until the tip of the probe reached the desired position in the posterior part of the flexor retinaculum. The reproducible location of the probe was confirmed by external palpation and by measuring its length from the entry point to the posterior part of the flexor retinaculum.
Calcaneal osteotomy
For the calcaneus osteotomy, an oblique skin incision of about 5 cm was made on the lateral side of the hindfoot, perpendicular to the axis of the body of the calcaneus (Figure 4, left). The lateral wall of the calcaneus was exposed. The osteotomy plane was marked with Kirschner wires and checked under fluoroscopy. An incomplete translational single plane calcaneus osteotomy (Figure 2) was performed from lateral to medial with an oscillating saw, leaving the medial cortex intact. To avoid injury to the flexor retinaculum and the neurovascular bundle, the osteotomy of the medial cortex was carefully completed with an osteotome, and the tuberosity gently mobilized with a laminar spreader.

Shows the skin incisions. (Left) Lateral view of a left foot with skin incision for the calcaneal osteotomy. (Right) Medial view of a left foot with skin incision, fascia opening, and inserted pressure-measuring probe (continuous line). The tip of the probe lies under the flexor retinaculum (dotted line).
Measurements
As minor injury to the flexor retinaculum is possible using this procedure, the pressure in the tarsal tunnel was measured before and after osteotomy in order to account for this in subsequent pressure measurements. The osteotomized calcaneal tuberosity was fixed with two 1.6-mm Kirschner-wires at 0, 4, 8, and 12 mm of lateralization, to simulate a range of varying degrees of hindfoot alignment. For the measurements, the specimens were secured with the foot fixated flat on the ground and the tibia proximally fixated at various points.
The pressure measurements were taken in the following sequence: no lateralization of the calcaneal tuberosity in neutral position (NP), 20° of plantarflexion (PF), 10° of dorsiflexion (DF), and finally again in NP for validation purposes. Measurements were repeated in the same sequence with the specimens with 4, 8, and 12 mm of lateralization. All measurements were taken 3 times, and the mean pressure value was calculated. Utmost care was taken to prevent inversion or eversion of the foot.
Flexor Retinaculum Release
Following all measurements, the flexor retinaculum release was performed. The tibial nerve was exposed by opening both fascial layers. In the area of the tarsal tunnel, the transected flexor retinaculum was loosely placed but left open. The skin was closed using a mattress stitch. Again, all measurements were done in the same manner: with no lateralization and 4, 8, or 12 mm of lateralization.
Statistical Analysis
For statistical analysis, normality tests (D’Agostino-Pearson-Test), analysis of variance, and post hoc tests (Friedman-Test) were calculated with Graph Pad Prism software (Graph Pad Software, Inc, La Jolla, CA, USA). Significance level was set to P < .05. The confidence interval of Figure 5 was calculated using the Wilson/Brown test.
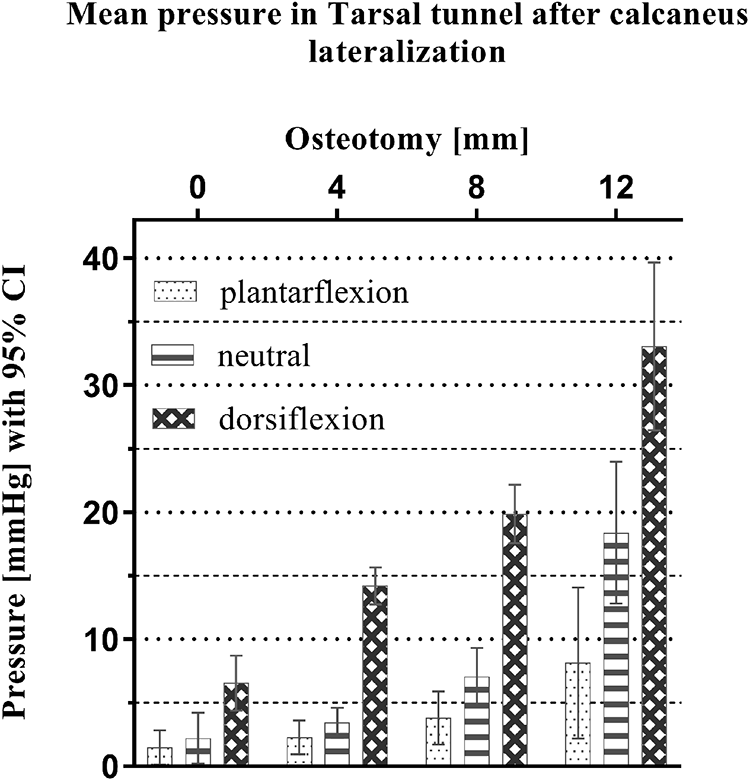
Pressure values depending on the osteotomy and the foot position.
Results
Osteotomy
There was no significant change in pressure following osteotomy (P > .877) indicating no relevant injury of the flexor retinaculum by the saw or osteotome (Table 1). The pressure in mmHg in the tarsal tunnel before the osteotomy was 1.6 in plantarflexion (PF), 3.5 in neutral position (NP), and 7.6 in dorsiflexion (DF). After the osteotomy (prior to lateralization) the pressure was 1.5 in PF, 2.2 in NP, and 6.5 mmHg in DF.
Effect of the Osteotomy to the Pressure in Tarsal Tunnel (n = 12).a

aValues are mean ± standard deviation.
Tuberosity Lateralization
With increasing lateralization of the calcaneal tuberosity, mean pressure increased, and was highest at 12 mm of lateralization (Table 2; Figure 5). Generally, the pressure measurements revealed low values for PF, higher values for NP, and the highest values for DF. With the tuberosity lateralization, the pressure (in mmHg) increased in every foot position: 2.3 in PF, 3.4 in NP, and 14.2 in DF for 4-mm lateralization; 3.8 in PF, 7.0 in NP, and 19.9 in DF for 8-mm lateralization; 8.1 in PF, 18.4 in NP, and 33.1 in DF for 12-mm lateralization. The mean pressure in NP und DF increased significantly for all degrees of lateralization (P < .05). There was, therefore, no significant difference for any lateralization from PF to NP.
Effect of Lateralization and Foot Position on Pressure in Tarsal Tunnel (n = 12).a

aValues are mean ± standard deviation.
Every change of the foot position (from PF to NP and from NP to DF) led to an increase in pressure. The mean pressure increases from NP to DF for 0- and 4-mm lateralization, as well as all position changes for 8- and 12-mm lateralization were significant (P < .05). There was, therefore, no significant difference from PF to NP in 0 and 4 mm (Table 2).
Release of Tarsal Tunnel
The release of the tibial nerve by transection of the flexor retinaculum reduced the mean pressure substantially for all foot positions (Table 3). In NP and DF positions, with all degrees of lateralization, the decrease of the mean pressure was significant (P < .05). There was, therefore, no significant pressure difference with release with the foot in PF, for all degrees of lateralization.
Pressure Change in Tarsal Tunnel After Release of Tibial Nerve (n = 12).a

aValues are mean ± standard deviation.
Discussion
The study demonstrated a substantial increase of the pressure below the flexor retinaculum with increasing degrees of lateralization of the calcaneal tuberosity, being significant in the majority of measurements. The release of the tibial nerve by transection of the flexor retinaculum reduced the pressure substantially. Interestingly, the index pressure was highest in hindfoot dorsiflexion, lower in neutral position, and lowest in plantarflexion, with and without lateralization. It follows, therefore, that ankle dorsiflexion narrows the flexor retinaculum and thereby increases the pressure in the tarsal tunnel.
The pressure increases are most likely due to the protruding anterior calcaneus fragment produced by the process of lateralization as well as the retinaculum being under tension (Figure 3). The release of the retinaculum prevents pressure increases and increases potential space for structures in the tarsal tunnel.
In the literature, the pressure in the tarsal tunnel has been studied previously, though outside the context of lateralizing calcaneus osteotomies. Barker et al reported pressures below the flexor retinaculum of 3.5 mmHg in NP of the ankle, 8.8 mmHg in DF, and 17 mmHg in PF in fresh-frozen cadavers. 3 Rosson et al measured 4 mmHg for NP, 4 mmHg for DF, and 13 mmHg for PF in 9 patients intraoperatively. 22 We assume that higher values recorded in PF than in DF may be due to the fact that the measuring probe lies more anteriorly underneath the flexor retinaculum. We assume that in PF, the retinaculum is more stretched anteriorly than posteriorly. Trepman et al analyzed 10 fresh-frozen human feet, with the tip of the probe approximately in the middle of the flexor retinaculum. A pressure of 2 mmHg was measured in NP, 32 mmHg in eversion, and 17 mmHg in inversion. 29 Barker and Rosson reported highest pressure values for PF. However, the exact position of the sensor in these studies was not documented and might have led to divergent findings if positioned at the entry or end of the tarsal tunnel. Apart from the higher pressure values in DF, our findings reflect those reported in the wider literature. 3,22,29
In the literature, statements of the incidence of tarsal tunnel syndrome after lateralizing osteotomies of the calcaneal tuberosity are sparse. To our knowledge, no study describes the relative incidence in relation to varying degrees of calcaneus lateralization. In a retrospective analysis, Van Valkenburg et al reported an incidence of 34% or 27/80 for neurologic deficit of the tibial nerve after lateralization of calcaneus using translational and Z-osteotomies through a lateral approach. Fifty-nine percent or 16/27 of these resolved spontaneously within 3 months, resulting in an incidence of 14% or 11/80 after 3 months. 30 In contrast, Jeffe et al reported no neurologic deficit in a retrospective study of 24 patients with translational lateralizing osteotomies of the calcaneal tuberosity using a medial approach. 11 Although the authors did not formally release the tarsal tunnel, the use of the medial approach potentially involves inherent injury or release of the flexor retinaculum. With only sparse data regarding the incidence of tarsal tunnel syndrome, it is difficult to make an absolute recommendation with regard to whether or not to perform a release in this context.
The pressure threshold above which symptoms occur due to tibial nerve compression is, to our knowledge, unknown. However, such a threshold for the median nerve and carpal tunnel syndrome, respectively, have been described. In the carpal tunnel, a pressure of 20 to 30 mmHg impairs epineural venous blood flow and a pressure of 30 mmHg can induce paresthesia. 19,23 The median and tibial nerves have almost the same cross-sectional area (7.97 and 8.05 mm2, respectively). 15 They also have comparable histologic structures. Extrapolating from the literature discussing the median nerve, we deduce that with rising compartment pressures, the mechanism of tibial nerve compression should be broadly similar.
Extrapolating the pressure threshold of the carpal tunnel syndrome to the pressure values of the tarsal tunnel (Table 2), a pre-emptive release of the flexor retinaculum after calcaneus lateralization of 12 mm should be considered as pressure values in DF exceed the critical threshold of 20 mmHg (33.1 mmHg) and are just below in NP (18.4 mmHg). With 8 mm of lateralization, the mean pressure value in DF was only slightly below the critical threshold of 20 mmHg (19.9 mmHg) which may therefore impair blood flow. If the planned lateralization exceeds 8 mm, or if other patient risk factors are present (as described below) with smaller degrees of planned lateralization, a pre-emptive release of the flexor retinaculum should be considered. The risk of tibial nerve palsy with lateralization of 4 mm is probably unlikely but is not impossible.
However, some factors may additionally influence the pressure in the tarsal tunnel and have to be considered when the indication for the release is taken. Individual patient risk factors, which may raise tarsal tunnel pressure, include (1) thickened and therefore more compression-prone tibial nerves as seen in Charcot-Marie-Tooth disease, 14,20 (2) chronic venous insufficiency with lipodermatosclerosis, 25 or (3) shortening of the Achilles tendon as in pes equinus. The exact influence of these specific risk factors requires further elaboration, but surgical planning in the context of any of these should probably involve a release.
The postoperatively fixed position of the foot influences the pressure in the tarsal tunnel and should be taken into account in preoperative planning. Keeping the foot postoperatively in fixed DF (ie, after tendon and soft tissue release for pes equinus) results in higher tarsal tunnel pressure and should be avoided where possible.
With a pressures of 20 mmHg and above, an impairment of the blood flow should be assumed, 23 but the patient can still be asymptomatic. Generally, it is the responsibility of each surgeon to consider a release in view of the various above-mentioned factors influencing the pressure. As an alternative to performing a flexor retinaculum release, patients can be kept under surveillance postoperatively for tibial nerve palsy symptoms. The surgeon should be aware that temporary and continuous anesthetic blocks can mask these symptoms.
Tibial nerve palsy following lateralizing calcaneal osteotomy may be prevented by release of the flexor retinaculum at the time of surgery. 1 In this study, the effect of a tarsal tunnel release was shown to substantially reduce pressure in the tarsal tunnel (Table 3). The treating surgeon should balance the risk of developing tibial nerve palsy by considering the amount of the tuberosity lateralization and potential patient-specific risk factors.
A limitation of this study is the use of Thiel-fixated cadaver tissue. Thiel-fixated tissue has many advantages 32 but has important limitations when used in biomechanical studies. 2 Several authors have explored its effect specifically on connective tissue. 4,5,8 -10,18,26,31 -33 The parameters, methods, and results of these various studies were, however, all very different. Some authors questioned its use for biomechanical investigation due to altered material properties such as lower Young’s modulus or increased flexibility. 8,9,18,26,31,33 Other authors found an increased Young’s modulus, 31 a similarly sized joint space, 32 and similar appearance of connective tissue under light microscopy 4 and identical linear material properties. 5
There are further attributes of Thiel-fixated tissues which influence their use in studies. Thiel fixation involves the use of solutions. 28 Some have a softening (boric acid) and some a hardening (formalin) effect on connective tissue. 8 Furthermore, the solubility and diffusion of the solutions into the tissue are different, 31 which is why the entry and duration of perfusion 18 as well as the ratio of cadaver weight and amount of solution are decisive for the biomechanical effect.
We did not find a study comparing pressure values in the tarsal tunnel before and after Thiel fixation, and further investigations which consider the numerous complex aspects of Thiel-fixated tissue are needed. It is possible that the measured pressure values are falsely low because of the lower Young’s modulus of the flexor retinaculum after Thiel fixation 8,18,26 where the expected pressure in the tarsal tunnel would be higher. Based on similar pressure values found in studies using fresh-frozen tissue, the positive aspects mentioned above, 4,5,31,32 and the clinical importance of tibial nerve compression, we consider the recommendation for the release of the flexor retinaculum to be appropriate.
A further limitation is that dead tissue is less elastic than living tissue. 16 However, fresh or fresh frozen tissue also have their own limitations in terms of mimicking in vivo conditions. Regardless of the tissue type used, however, the tibial nerve, following lateralization, is under a constantly increased pressure, despite differing baseline elastic properties. The consideration of a flexor retinaculum release can therefore still be recommended in the clinical setting based on our data.
Finally, we are aware that other operative treatments can prevent pressure increase in the tarsal tunnel, for example, a closing-wedge osteotomy. However, the intention of this study was to investigate the effects of the commonly used lateral sliding osteotomy on the pressure in the tarsal canal.
Conclusion
In this biomechanical cadaver study, we investigated the pressure change in the tarsal tunnel following lateralization of the calcaneus in Thiel-fixated specimens and measured the pressure in different foot positions and different degrees of lateralization. By comparing our values with those found in the literature, the possibility of developing tibial nerve palsy should be kept in mind if the lateralization exceeds 8 mm, especially in the presence of other risk factors. A prophylactic flexor retinaculum release can therefore generally be considered. Alternatively, surveillance for tibial nerve palsy symptoms is recommended postoperatively.
Supplemental Material
Supplemental Material, FAO931015-ICMJE - Effect of Lateral Sliding Calcaneus Osteotomy on Tarsal Tunnel Pressure
Supplemental Material, FAO931015-ICMJE for Effect of Lateral Sliding Calcaneus Osteotomy on Tarsal Tunnel Pressure by Sebastian Halm, Paul G. Fairhurst, Stefan Tschanz, Fluri A. M. Wieland, Valentin Djonov and Fabian Krause in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because donors had formally consented to use body parts for research purposes by signing the donation forms.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.