
Abstract
Background:
Previous Level I studies show promising results for the use of a hydrogel synthetic cartilage implant (SCI) for the treatment of hallux rigidus. A recent independent retrospective review has put those results into question, however. The purpose of this article is to report patient-reported outcomes and early complications using this implant so as to add to the paucity of data in the literature regarding this implant.
Methods:
This was a retrospective chart review of patients undergoing hydrogel synthetic cartilage implant for the treatment of hallux rigidus from July 2017 to November 2018. Data collected included patient demographics, radiographic grading, and outcomes: Veterans Rand 12 Item Health Survey (VR-12), Foot and Ankle Ability Measure (FAAM), visual analog scale (VAS), patient satisfaction, and complications. Fifty-four patients (59 feet) with an average age of 57.6 (range, 39-78) years were analyzed. The average latest follow-up was 18.9 (range, 3-31.3) months. Body mass index was 26.7 (range, 18.7-35.2). None were diabetic and 5 were smokers.
Results:
The mean outcome improvements were 6.5 points (VR-12 Physical), 17.2 points (FAAM ADL), 27.4 points (FAAM Sport), and 18.4 points (VAS) (P < .01 for each). Scores were significantly improved from preoperatively to most recent follow-up for FAAM ADL (71.0 vs 88.2 points), FAAM Sports (44.6 vs 72.0 points), and VAS (49.4 vs 31.0) (P < .01). Overall, 72.5% patients would definitely or probably have the operation again. Ten patients (18.5%) went on to have revision surgery. Of these, 7 patients were revised to an arthrodesis, and 1 metal hemiarthroplasty and 2 implants were removed because of infection.
Conclusion:
Synthetic cartilage implantation for the treatment of hallux rigidus demonstrated improved pain and outcome scores at short-term follow-up. Reoperation and conversion to fusion rates were comparable to prior studies.
Level of Evidence:
Level IV, case series.
Introduction
Hallux rigidus, or arthritis of the first metatarsophalangeal (MTP) joint, is the most common site of arthritis in the foot and ankle. 7 It is a frequent cause of pain and dysfunction in patients seen by orthopedic surgeons. The condition is radiographically characterized by loss of cartilage and thus joint space narrowing, osteophyte formation, and subchondral cyst formation. 5 On physical examination, patients often have tenderness to palpation along the dorsal aspect of the joint, decreased range of motion, and pain at the extremes of motion.
Nonoperative treatment options for hallux rigidus include activity modification, nonsteroidal anti-inflammatory drugs, orthotics, footwear modification, and intra-articular steroid injections. Should these conservative treatment options fail, operative intervention can be considered. In patients with mild hallux rigidus and pain at the extremes of range of motion due to dorsal osteophyte formation, cheilectomy has resulted in satisfaction rates of 88% to 95%. 8,9 For patients with more severe disease, numerous procedures have been attempted including interposition arthroplasty, Keller resection arthroplasty, 3 numerous joint replacement devices and arthrodesis. The materials that have been used for joint replacement of the first MTP joint include silicone, metals, and polyethylene. 11,12 Additionally, both hemiarthroplasty and bipolar arthroplasty have been attempted. Unfortunately, loosening, subsidence, and poor patient satisfaction have been reported with these devices. In one study, Raikin 10 compared metal hemiarthroplasty to MTP arthrodesis. Patients with a successful arthrodesis demonstrated better function, higher satisfaction, and less pain.
A hemiarthroplasty hydrogel synthetic cartilage implant (SCI) (Cartiva Inc, Alpharetta, GA) has demonstrated promising results in a randomized controlled trial. Baumhauer et al demonstrated noninferiority of the SCI when compared to first MTP arthrodesis with an equivalence level of <15%. Additionally, this study did not demonstrate any instances of bone lysis, subsidence, or implant fragmentation. They did, however, have a 9.2% conversion rate to arthrodesis because of continued pain. 2
A recent study by Cassinelli et al demonstrated less favorable results in a retrospective single surgeon case series. This study showed a 20% reoperation rate with 8% conversion to arthrodesis. They also had mixed patient satisfaction rates, with 42% stating they were highly satisfied or satisfied, 20% with neutral satisfaction, and 38% were either unsatisfied or very unsatisfied. Overall, the study concluded that SCI “yielded neutral patient satisfaction, mild pain, and dysfunction at early follow-up.” One major confounding variable in their study was the use of intra-articular steroid injection in the first MTP joint following implantation of the SCI. It is unclear how this may have impacted the clinical outcome but it may simply be an indication that a significant number of patients were not satisfied. 4
The goal of this study was to report patient-reported outcomes and early complications using a synthetic cartilage implant in the treatment of hallux rigidus. This was a multisurgeon study performed in the United States without confounding postoperative intra-articular injections. We hypothesized that patients would have overall improved pain relief and function as well as high patient satisfaction at short-term follow-up.
Methods
Data Collection
A retrospective chart review was performed between July 2017 and November of 2018 for 5 foot and ankle fellowship–trained orthopedic surgeons in a single private practice group. Patient characteristic data collected included age, sex, body mass index (BMI), smoking status, and presence of diabetes. Radiographic analysis to determine Coughlin and Shurnas grade 5 was performed for all patients. Intraoperative concomitant procedures were also documented. Pre- and postoperative outcome measures used were as follows: the Veterans Rand 12 Item Health Survey (VR-12), Foot and Ankle Ability Measure (FAAM), and visual analog scale (VAS). Additionally, a patient satisfaction survey was given to patients asking if they would have the SCI procedure performed again. Potential responses were definitely yes, probably yes, probably not, or definitely not. If patients were unable to return for clinical follow-up, telephone and mailed surveys were allowed. Reoperation and complications were also collected.
Fifty-nine feet in 54 patients underwent synthetic cartilage implantation during this time period. Thirty-seven females and 17 males had the procedure performed. Average age was 57.6 (range, 39-78). Average BMI was 26.7 (range, 18.7-35.2). There were 5 smokers and no patients with diabetes. Thirty-one were performed on the left side and 28 on the right. Preoperative Coughlin and Shurnas classification 5 analysis was performed, and it demonstrated that 57.6% (34/59) were grade 2 and 42.4% (25/59) were either grade 3 or 4. It was difficult to distinguish between grades 3 and 4 because physical examination findings were not documented consistently before surgery. Five patients underwent bilateral SCI implantation and 3 were performed on the same date. Twelve of 59 (20.3%) feet underwent concomitant procedures. These include third webspace neuroma excision, dorsomedial neuroma excision, tarsal tunnel release, Moberg osteotomy, talonavicular fusion, Akin osteotomy (2 patients), hammertoe correction (2 patients), first-metatarsal hardware removal, fourth-toe flexor tenotomy, and second-metatarsal shortening osteotomy. Average follow-up was 18.9 (range, 3-31.3) months.
Operative Technique
The operative technique used in this study followed the manufacturers recommendations. 2 A standard dorsal approach to the first MTP joint was performed. Once the arthrotomy was performed, osteophytes on the proximal phalanx and metatarsal head were removed. A guide pin was then placed perpendicular to the metatarsal head and in line with the longitudinal axis of the metatarsal. A cannulated drill bit was advanced over the guide pin and the drill was advanced until approximately 1 mm short of flush against the metatarsal head. The SCI was then implanted into the cavity. This left the implant approximately 1-2 mm proud of the metatarsal head articular surface. The toe was then taken through range of motion to ensure that it was able to articulate without restriction. The wound was then closed in a layered fashion. Because multiple surgeons were included in this study, variations in tourniquet type and suture used existed.
Postoperative Protocol
Patients were placed in a postoperative dressing and stiff soled shoe following surgery. All patients were allowed to bear weight as tolerated following the procedure and range of motion exercises were begun as early as they were tolerated so as to avoid stiffness. Sutures were removed and patients were instructed to gradually transition into regular footwear at 2 weeks postoperatively.
Statistical Analysis
Two-sample t tests were used to determine differences in outcome scores over time. Statistical analyses were performed using Sigma Plot 11.0 (Systat Software, Chicago, IL) with significance set at an alpha level of 0.05.
Results
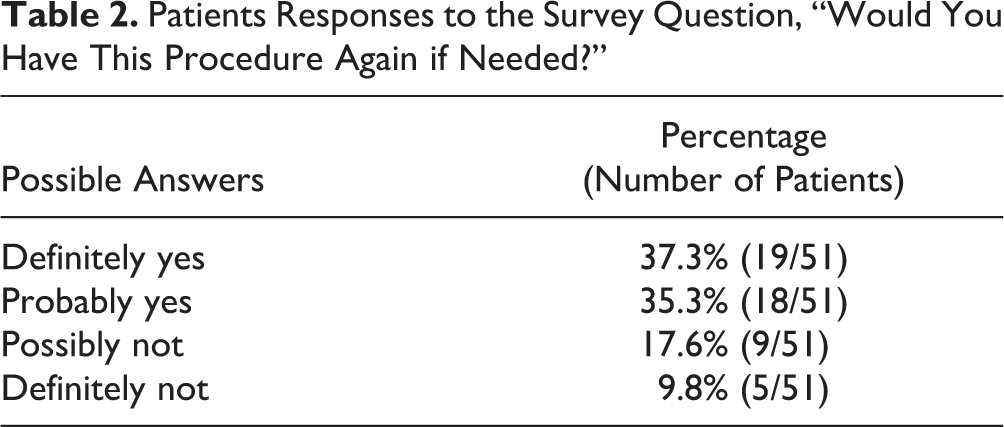
Preoperative and postoperative VR-12, FAAM, and VAS scores are shown in Table 1. Other than VR-12 Mental, all scores had a significant improvement (P < .01 for each). 84.8% of patients were overall satisfied with this procedure. Response to the question of “Would you have this procedure again?” is included in Table 2. Fifty-one of 54 patients (94.4%) responded to this question. Three patients did not answer this question. Although these patients did not supply an answer to this question, their outcome data were included. Overall, 72.5% patients would definitely or probably have had the operation again. There was a 16.9% (10/59) reoperation rate, with 7 (7) successfully converted to a first MTP arthrodesis, 1 converted to an arthroplasty (Arthrosurface, Franklin, MA), and 2 were explanted because of infection.
Preoperative and Postoperative Mean Outcome Measures With Change.

Abbreviations: ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure; VAS, visual analog scale; VR-12, Veterans Rand 12 Item Health Survey.
Patients Responses to the Survey Question, “Would You Have This Procedure Again if Needed?”
Discussion
With a recent retrospective case series 4 demonstrating conflicting results with the initial level I SCI study, 2 this article adds more cases to the current literature and provides a multisurgeon experience without a major confounding factor of postoperative intra-articular corticosteroid injections. Overall, the current study demonstrates that patients undergoing SCI implantation had improved VAS pain scores, good patient outcomes, and that the majority of patients would have the procedure performed again. Overall, 72.6% (37/51) of patients surveyed in this study would definitely or probably have the procedure performed again compared with the 27.4% (14/51) who would not. In the 20.3% of patients who had had a concomitant procedure, it is difficult to be certain that their perception of the procedure outcome was not altered by the fact that they had had more than 1 procedure performed. In looking at this subset of patients, 66.7% (8/12) would definitely or probably have had the procedure again compared with the 33.3% (4/12).
The survey data in this study only slightly differs from the study by Cassinelli et al. 4 In their retrospective cohort, they found that 66% of patients surveyed would have the procedure performed again. They also had a 20% reoperation rate, although this study had a rate of 16.9%. As mentioned previously, the Cassinelli et al study had a confounding variable of corticosteroid injections in the postoperative period. A total of 79 injections were given. They also used a splinting device (Dynasplint, Severna Park, MD) in 14% of their patients to help improve range of motion. The current study included no postoperative injections or use of splinting devices.
The initial level I study by Baumhauer et al 2 had excellent satisfaction rates, with 93% of patients stating that they would have the procedure again. They also had an 11.2% reoperation rate, with 9.2% successfully being converted to arthrodesis. The study by Baumhauer et al showed an improvement in mean VAS score from 68 to 5.0 at 2 years. Furthermore, at 2-year follow-up they demonstrated an improvement in mean FAAM sport and mean FAAM ADL of 36.9 to 79.5 and 59.4 to 90.4, respectively. When compared to this current study, their results were more favorable for VAS scoring but were similar or slightly inferior with regard to FAAM sport or FAAM ADL scores. This study showed a VAS improvement from 49.4 to 31.0, a FAAM sport score of 44.6 to 72.0, and a FAAM ADL score of 71.0 to 88.2. It is unclear why VAS pain scores differed in these 2 separate patient populations. One likely explanation could be the shorter follow-up in this study.
Further validating their study with a midterm follow-up, the same patient cohort as in the level I study was followed up at a minimum of 5 years. 6 Twenty-seven patients were available and demonstrated excellent pain relief. Only 1 patient was converted to arthrodesis, demonstrating an implant survivorship of 96% at 5 years. They also noted no instances of loosening, subsidence, or implant wear. In the current study, in patients who were converted to arthrodesis, we found numerous instances of implant subsidence and loosening intraoperatively (Figure 1). Implants were frequently removed with ease. Although the width of the implant did not decrease (Figure 2), we did notice significant wear of the implant. This was also seen by Cassinelli et al. 4 One possible explanation for implant subsidence or loosening could be due to bone loss. All patients who had an explantation performed were female, and the average age was 58.8. Unfortunately, osteopenia or osteoporosis data was unavailable for analysis. Another potential cause of loosening or subsidence could be stress placed on an implant due to a stiff first metatarsophalangeal joint. Because preoperative and postoperative range of motion was not consistently documented, this potential cause could not be evaluated.

Intraoperative image demonstrating implant subsidence with bone overgrowth.

Intraoperative image of a removed 10-mm implant with no change in width but significant discoloration and wear.
More than half (57.6%; 34/59) of the current patients were Coughlin and Shurnas 5 grade 2, and 42.4% (25/59) were either grade 3 or 4. We did not have appropriate clinic physical examination documentation to determine whether patients were grade 3 or 4. The preoperative hallux rigidus grading was different compared to the Baumhauer et al study, 2 which showed 29% grade 2, 55% grade 3, and 16% grade 4. The Cassinelli et al 4 study was also different, which showed 25% grade 2, 60% grade 3, and 13% grade 4. The grade of hallux rigidus may not matter, however, as has been previously demonstrated. 1
There were numerous limitations in this study. The first is the retrospective nature and no comparison group. Furthermore, physical examination findings were not recorded as this was inconsistently documented by the 5 foot and ankle surgeons included in the study. Physical examination data that would be valuable for analysis would include preoperative and postoperative range of motion, pain at extremes of dorsiflexion and plantarflexion, and pain at midrange arc of motion. With these data, we may have been able to determine which clinical findings were associated with better outcomes and, consequently, which might represent the best indications for SCI. Additionally, no long term radiographic analysis was performed. The fact that this study was performed by 5 fellowship-trained orthopedic foot and ankle surgeons is both a strength and a weakness. Technique differences between each surgeon could alter outcomes, but each surgeon followed the technique guide as previously described, with only slight variations in suture and tourniquet type.
Conclusion
Synthetic cartilage implantation for the treatment hallux rigidus demonstrated improved pain and outcome scores at short-term follow-up. Reoperation and conversion to fusion rates were comparable to prior studies.
Supplemental Material
Supplemental Material, FAO930691-ICMJE - Patient-Reported Outcomes and Early Complications After Synthetic Cartilage Device Implantation
Supplemental Material, FAO930691-ICMJE for Patient-Reported Outcomes and Early Complications After Synthetic Cartilage Device Implantation by William M. Engasser, J. Chris Coetzee, Patrick B. Ebeling, Bryan D. Den Hartog, Jeffrey D. Seybold, Scott M. Holthusen, Rebecca Stone McGaver, Kayla J. Seiffert and M. Russell Giveans in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from IntegReview institutional review board (approved 10.2.2019).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bryan D. Den Hartog, MD, reports personal fees from Wright Medical outside the submitted work. ICMJE forms for all authors are available online. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.