
Abstract
Background:
Hallux rigidus (HR) is a common pathology of the first metatarsophalangeal (MTP) joint causing pain and stiffness. However, severity of symptoms and radiographic findings are not always concordant. A novel flexibility device, which measures the mobility of the MTP joint through its arc of motion, has been validated. This study compares flexibility in patients before and after cheilectomy (with or without proximal phalanx osteotomy) for HR.
Methods:
This is a single-center study of adult patients with HR who were indicated for cheilectomy or cheilectomy and Moberg (dorsiflexion closing wedge) osteotomy of the proximal phalanx based on symptoms and radiographs from 2013 to 2015. Pre- and postoperatively, patients underwent testing with a validated flexibility protocol to generate flexibility curves. Parameters included early and late flexibility, laxity torque, and laxity angle. Patients completed Foot and Ankle Outcomes Scores (FAOS) pre- and postoperatively. Twelve operative patients underwent preoperative testing, with 9 completing postoperative testing (mean age, 53.0 years; 67% female; mean 2.8-year follow-up).
Results:
Patients had significant improvements in early sitting and standing flexibility, sitting and standing laxity angles, standing laxity torque, and both sitting and standing maximum dorsiflexion after surgery (all P < .05). While preoperative early flexibility, laxity angle, and maximum dorsiflexion all differed significantly between patients and controls (P < .015), postoperative early flexibility was similar to controls (P > .279). FAOS scores for pain, symptoms, sport, and quality improved significantly after surgery.
Conclusion:
Surgical treatment with cheilectomy was associated with significant improvements in nearly all flexibility parameters for sitting and standing positions. However, most postoperative flexibility parameters did not improve to the level of normal controls. Regardless, patients still experienced significant improvements in outcomes. This study demonstrated that surgical correction is associated with significant biomechanical and clinical results. The flexibility device can be used in further studies to assess outcomes after other HR procedures.
Level of Evidence:
Level II, prospective comparative study.
Hallux rigidus (HR), or degenerative joint disease of the first metatarsophalangeal (MTP) joint, is the most common form of osteoarthritis of the foot, affecting 34% of men and nearly half of women by the age of 50 years. 19 HR is classically associated with pain, stiffness, osteophytes, and loss of joint space. 3 There are more than 10 classification schemes for HR; of these, the Coughlin and Shurnas classification, which incorporates radiographic and clinical data, is one of the most frequently cited. 3,4 While classification systems may provide a framework for assessing HR, clinical-radiographic grades do not always reliably correlate with patient-reported outcomes scores. 13
Range of motion, as assessed by clinicians in the office, is a common method to evaluate HR. Classically, range of motion is assessed at extremes. However, the literature has shown that such static range-of-motion tests may not correlate well with function. 6 On the other hand, dynamic measurements that incorporate a joint’s motion in response to load may be more meaningful for discerning aberrant vs normal function. Flexibility is one such measure and describes the mobility of a joint throughout its arc of motion in response to applied load. 2 Moreover, flexibility is a measurement that is affected by anatomic hallmarks of HR, including capsular scarring and synovial hypertrophy. 2
A flexibility jig was developed at the authors’ biomechanics department, with the capacity to measure rotational flexibility and associated parameters of the first MTP joint (Figure 1). 15,17,18 This device has been validated in symptomatic patients as well as controls and was found to have excellent intra- and interrater reliability. 2 Testing is simple to perform and tolerated well by patients, as it simply requires passive motion of the great toe performed by an examiner. 2,15,17,18 In a comparison of patients with HR and asymptomatic controls, patients with HR had significantly less flexibility based on several dynamic parameters. 2

The first metatarsophalangeal joint flexibility jig.
Surgical procedures such as a cheilectomy and the Moberg (dorsiflexion closing wedge) osteotomy are effective treatments for HR in that they improve total MTP dorsiflexion and have high rates of patient satisfaction. 10,11,14 Prior studies have investigated effects of cheilectomy on MTP motion, with varying conclusions. A kinematic analysis of gait found no difference in total range of motion at the MTP after cheilectomy. 9 Conversely, other studies have found that after cheilectomy, MTP motion may improve but may never reach the level of normal controls. 1,12 Cheilectomy may also result in increased peak ankle push-off power. 16 However, most of these MTP motion studies have provided data about kinematics but have not included information about flexibility and load at the MTP joint.
This study sought to identify the impact of surgical treatment for HR on flexibility and dynamic motion parameters using the novel jig. We hypothesized that patients would have improvement in these parameters from before to after surgery, but they would not reach the same level as controls. Despite this, however, we hypothesized that patients would still have significant improvement in clinical outcomes scores.
Methods
This is a follow-up analysis to a previous study performed at a single tertiary care institution. In the first phase, 15 patients with HR were enrolled from surgeons’ offices at our institution. Inclusion criteria were (1) age older than 18 years at the time of initial enrollment and (2) Coughlin stage II or III HR (joint space narrowing and osteophytic changes with flattening of the metatarsal head) based on radiographs. 3 Patients were considered for inclusion if they were indicated for cheilectomy, with or without Moberg osteotomy, by 1 of 2 fellowship-trained foot and ankle surgeons. Patients were excluded if (1) they had prior ipsilateral foot or ankle surgery, (2) hallux valgus (defined by an intermetatarsal angle of >9°), and (3) connective tissue disorder (eg, Ehlers-Danlos) or similar pathology that would affect tissue or joint flexibility. Prior to study initiation, institutional review board approval was obtained. Patients meeting criteria were recruited and all provided informed consent.
Separately, a control group of 20 subjects were recruited through the approved Clinical Trials Registry at our institution. All subjects denied foot or ankle pathology or symptoms. In addition, all subjects had standard bilateral anteroposterior (AP) and lateral weightbearing radiographs that confirmed the absence of foot or ankle pathology.
A power analysis was not performed a priori; rather, we recruited all patients who performed initial testing to return for follow-up testing. Of the initial 15 patients with HR who participated in the study, 3 elected to undergo conservative therapy, leaving 12 patients who underwent operative treatment from 2013 to 2015. These 12 patients were all contacted at minimum 1 year postoperatively and asked to participate in a second phase of testing with the flexibility jig. Of these 12, there were 9 patients (75%) who agreed to participate in repeat testing. Demographics are shown in Table 1. The mean age was 53.0 ± 6.6 years, and the majority (6/9) were female. Mean follow-up was 2.8 ± 0.8 years (range, 1.6-3.9). All patients underwent dorsal cheilectomy; 7 of 9 also had Moberg (dorsiflexion closing wedge) osteotomy of the proximal phalanx.
Demographics of the Study Group.a

a Moberg = Moberg osteotomy (dorsiflexion closing wedge osteotomy of the proximal phalanx).
Operative data were collected from the medical chart. All procedures were performed based on surgeon discretion. The senior author generally performed cheilectomy with Moberg osteotomy for HR unless the patient declined the osteotomy or had preserved motion preoperatively. Cheilectomy was performed via an open dorsal approach, and approximately 30% of dorsal metatarsal bone was removed. Medial and lateral bony ridges of the dorsal metatarsal, as well as the osteophytic rim of the proximal phalanx, were also removed. The Moberg dorsiflexion osteotomy of the proximal phalanx was performed via a 2- to 3-mm closing wedge osteotomy and fixed with a staple. For Moberg and cheilectomy and cheilectomy alone, patients were allowed to immediately weight bear in a postoperative shoe, which was worn for 2 weeks for cheilectomy-only patients and 6 weeks for cheilectomy and osteotomy patients. Physical therapy, which included active and passive range of motion, was initiated at 2 weeks for all patients. Preoperative and postoperative Foot and Ankle Outcomes Scores (FAOS) were collected.
Flexibility testing was performed before and after surgery according to a standardized institutional protocol. The flexibility jig was specially constructed for first MTP testing purposes. All testing was performed by the same examiner who performed testing in the first phase of analysis. Before any data were recorded, each patient’s first MTP joint was cyclically loaded 10 times to provide a controlled recent strain history prior to data collection. Then, 3 trials were collected in both seated and standing positions. The average of the 3 measurements was used as an unbiased estimate of the mean for analysis. For measurements in the seated position, the patient sat in a chair with knees flexed to 90 degrees and thighs parallel to the floor. For measurements in the standing position, the patient stood with his or her foot in the jig with body weight evenly distributed across both feet. Range of motion and torque were applied via direct manipulation by the examiner, which was shown to be reliable in prior work. 2
Rater-applied torque and range-of-motion measurements were acquired at 100 samples per second using TracerDAQ Pro software (Measurement Computing Corporation). The recorded voltage signals were processed with MATLAB (MathWorks) using an analysis developed in the first phase of the study. The voltages that corresponded to the rater-applied load and patient range of motion were converted to torque (N cm) and angle (degrees) in accordance with the calibration factors.
Several parameters that described first MTP joint flexibility were computed from the testing data (Figure 2). First, applied torque (x-axis) and first MTP dorsiflexion (y-axis) were graphed forming a sigmoidal-shaped flexibility curve for each patient. Early flexibility was defined as the slope of the curve over the first 25% of the graph; late flexibility was the slope over the last 25% of the graph. The average intersection point of the early and late flexibility curves for control subjects was used to specify the torque (N cm) from which laxity (degrees) was determined. Therefore, laxity represents the amount of angular rotation of the first MTP joint observed for a standardized amount of applied torque.
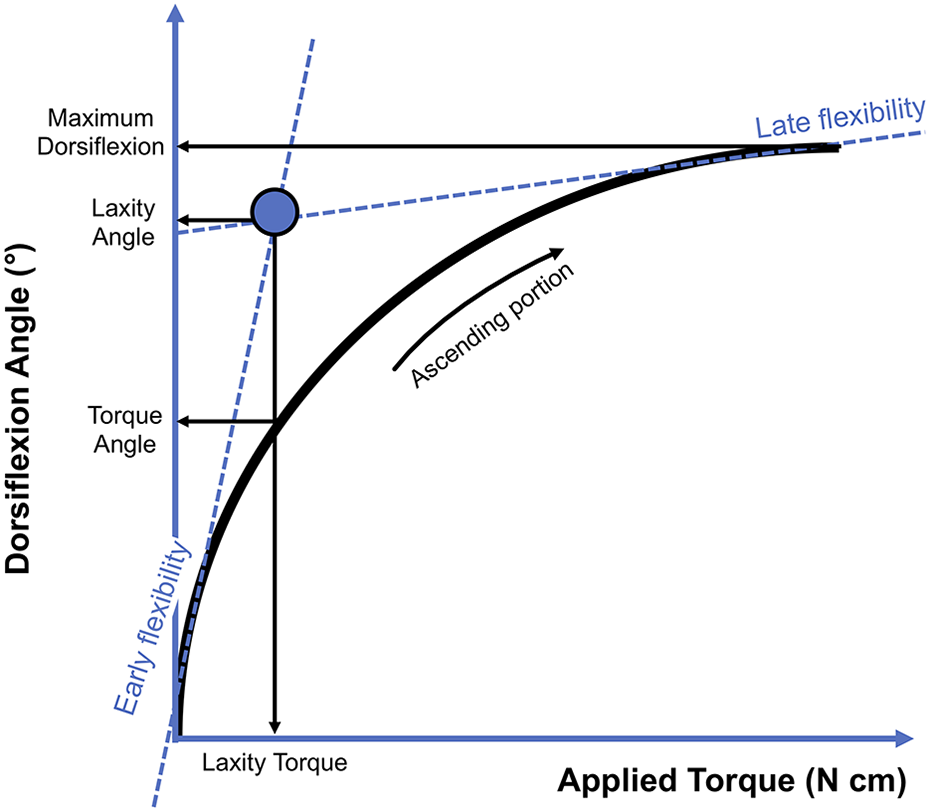
Diagram of the torque vs dorsiflexion flexibility curve. The slope lines of early flexibility and late flexibility portions of the curve intersect at a point represented by the circle. The x-axis and y-axis coordinates for this point are the laxity torque and laxity angle, respectively. The torque angle is the point on the y-axis at which the normal laxity torque value (mean of healthy controls) intersects the patient’s flexibility curve.
For statistical analysis, the preoperative and postoperative values for each flexibility parameter (early flexibility, late flexibility, and laxity) were compared using the Wilcoxon signed-rank test for paired samples. In addition, paired t tests were used to compare preoperative and postoperative values to controls. Paired t tests were also used to compare preoperative and postoperative FAOS scores. Level of significance was set at .05. Statistical analyses were performed in SPSS version 22.0 (SPSS, Inc) and Microsoft Excel 2016.
Results
Postoperative flexibility curves for the patients in seated and standing positions are shown in Figure 3 and Figure 4. Flexibility parameters are detailed in Table 2. Patients with HR had significant improvements postoperatively in nearly all parameters, including early flexibility, laxity, standing laxity torque, torque angle, and maximum dorsiflexion. However, despite these improvements, postoperative flexibility parameters of patients with HR still did not reach those of normal controls (Figures 5 and 6).

Postoperative flexibility curves for patients in the seated position.
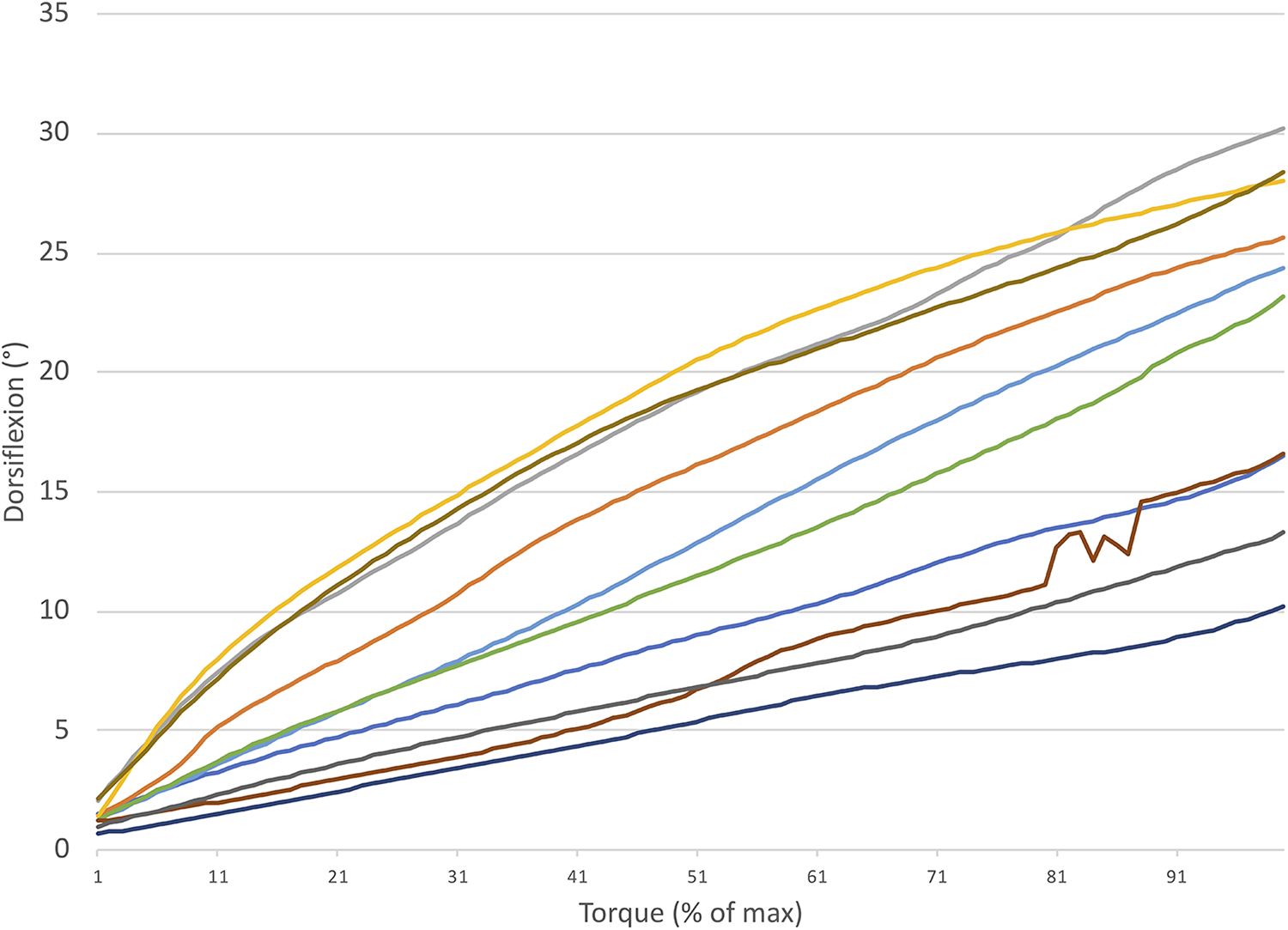
Postoperative flexibility curves for patients in the standing position.
Preoperative HR, Postoperative HR, and Control Subject Flexibility Parameters.a

a P values compare preoperative patients with hallux rigidus (HR) vs to postoperative patients with HR, preoperative patients with HR vs controls, and postoperative patients with HR to controls. Values expressed as mean ± standard deviation.
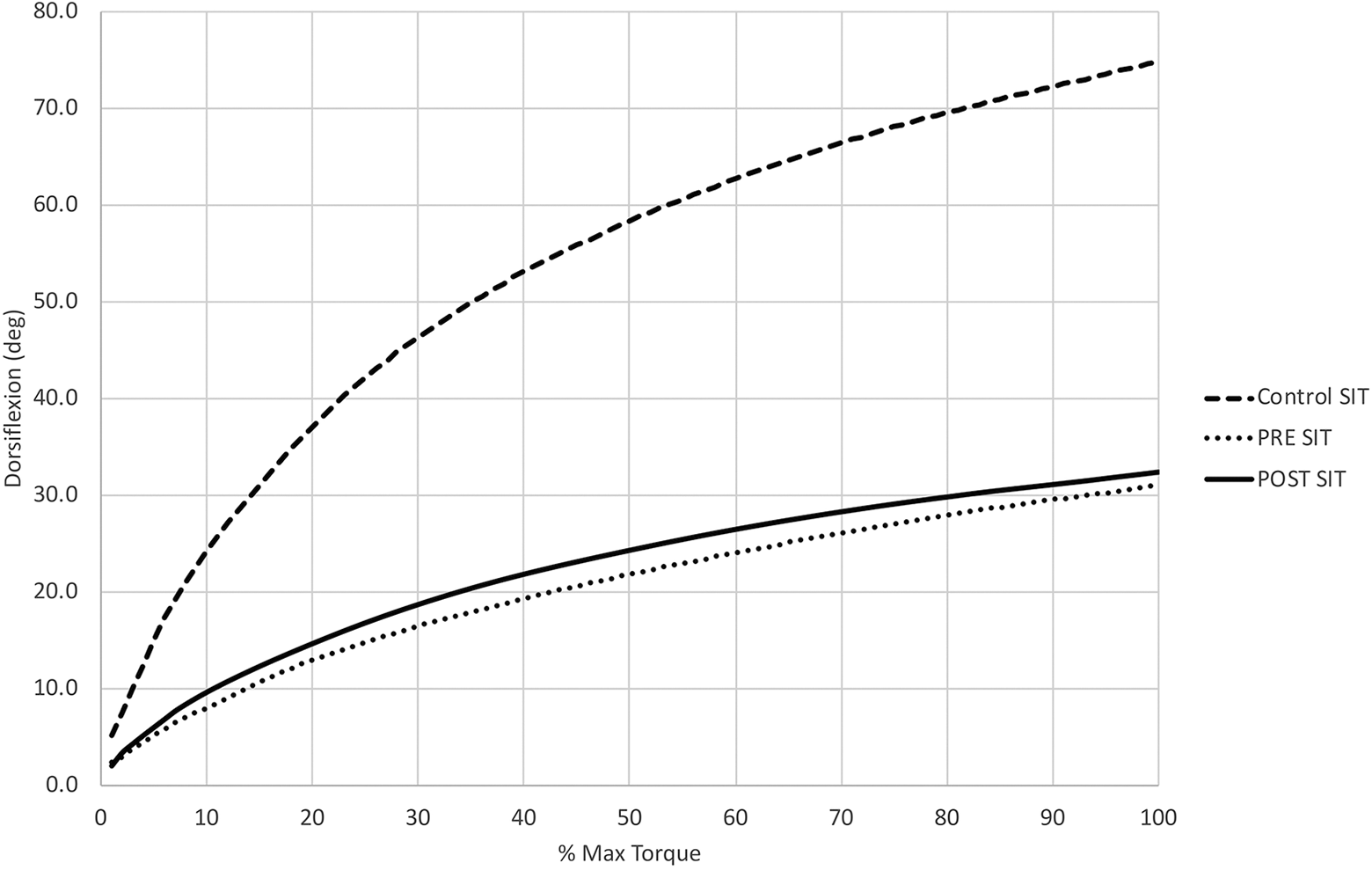
Flexibility curves in the seated position for patients with HR preoperatively (dotted line), patients with hallux rigidus (HR) postoperatively (solid line), and controls (dashed line).

Flexibility curves in the standing position for patients with hallux rigidus (HR) preoperatively (dotted line), patients with HR postoperatively (solid line), and controls (dashed line).
FAOS scores are shown in Table 3. There were significant improvements in the domains of pain, symptoms, sports, and quality of life. Only the domain for activities of daily living remained not significant.
Preoperative and postoperative scores in the FAOS domains.

Abbreviation: FAOS, Foot and Ankle Outcomes Scores.
a P < .05.
Discussion
The literature has described the multiple kinematic and motion changes in the foot after cheilectomy for hallux rigidus. 16 This study assessed flexibility, which is a unique parameter that represents the motion of the joint through an applied load at the first MTP joint in patients with HR pre- and postoperatively. Operative management, consisting of cheilectomy and commonly Moberg osteotomy (dorsiflexion closing wedge osteotomy of the proximal phalanx), produced significant improvement in flexibility parameters for both sitting and standing positions. In addition, maximum dorsiflexion improved significantly. Finally, while the majority of flexibility parameters did improve after surgery, they did not reach the same levels of controls.
This study is a follow-up to an analysis comparing first MTP flexibility in symptomatic patients with hallux rigidus to controls. 2 In the first analysis, the flexibility jig was validated, and intra- and interrater reliability for the jig were determined to be good to excellent. 2 Patients with HR had significantly lower early flexibility, laxity angle, torque angle, and maximum dorsiflexion compared to controls in both sitting and standing positions. 2 However, there was generally greater first MTP joint flexibility in the seated position compared to standing, which was more marked in patients with HR compared to controls.
Cheilectomy and dorsal closing wedge osteotomy of the proximal phalanx have been shown to increase joint motion and dorsiflexion as well as outcomes scores. 10,11,14 Operative treatment for hallux rigidus lead to improvements in flexibility curves, although not necessarily to the level of normal controls (Figures 5 and 6). Specifically, surgical treatment with cheilectomy was associated with improvement in early flexibility, laxity angle, laxity torque (standing position only), torque angle, and maximum dorsiflexion. Postoperatively, early flexibility for patients was statistically similar to that of controls. Prior work has shown that dorsal cheilectomy for hallux rigidus may reduce the osseous barrier to dorsiflexion, creating a more favorable geometry of the joint. 5 Although this procedure does not ultimately correct the underlying biomechanical imbalances of the joint, it may allow for increased dorsiflexion due to a pivoting motion, rather than the typical gliding motion of the joint. 8 This pivot may be responsible for the early flexibility.
In other instances, such as laxity angle, torque angle, and maximum dorsiflexion, while parameters improved postoperatively, they never reached values similar to controls. Laxity angle, which represents the intersection of early and late flexibility lines on the flexibility curve, can be considered a surrogate for overall joint flexibility. Laxity angle in the standing position doubled from pre- to postsurgery but was still half of normal controls. Maximum dorsiflexion followed a similar pattern. Hallux rigidus is characterized not just by bony abnormalities but also by increased tension in the soft tissues as well as abnormal stress across the articular cartilage, which are not addressed by cheilectomy or Moberg osteotomy. 5 Therefore, it is consistent that these procedures improve, but do not completely resolve, the stiffness of the first MTP in hallux rigidus.
Despite this, patients still had significant improvements in FAOS scores for pain, symptoms, sports, and quality of life. Due to the small number of patients included, the analysis was underpowered to detect statistically significant relationships between flexibility parameters and outcomes scores. However, these results are consistent with other studies of symptomatic improvement after cheilectomy and osteotomy. 14
In addition, while there were improvements from pre- to postsurgery in flexibility parameters, flexibility was usually greater in the sitting position when compared to standing. This may be attributable to tightness in the plantar fascia, which can restrict motion of the first MTP. 5 During weightbearing activities, activation of the windlass mechanism may exacerbate plantar fascia tightness and further tension the soft tissues around the MTP.
There are several limitations to this study. There was a small sample size of patients, as this was partially limited by the first phase of the study. 2 However, we hope that future studies could use this flexibility device in larger-scale studies. Such analyses could include assessment of flexibility after polyvinyl alcohol implants. In addition, while weightbearing testing in the standing position simulates a more functional position than what is typically performed in the office, it is still not a surrogate for actual gait. Future studies could analyze motion and flexibility of the first MTP during ambulation or higher-impact activity. Finally, there were too limited data to perform adequately powered correlations with clinical outcomes scores. Further, not all patients had a Moberg osteotomy, which could affect outcome. However, no study has compared these procedures directly, and both cheilectomy operations and combined cheilectomy with Moberg osteotomy procedures have been shown to have excellent results. 7,14
Future work, incorporating a greater number of patients, should attempt to quantify which flexibility parameters are associated with the greatest improvements in clinical outcome scores. This would also be useful for more novel outcomes such as computerized adaptive testing metrics like PROMIS (Patient-Reported Outcomes Measurement Information System), which were not in use at our institution at the time of patient enrollment. It would also be important to understand if there are certain thresholds for flexibility parameters that should be met to achieve a desirable amount of symptom relief. Further understanding of flexibility would therefore be valuable in honing clinical diagnosis and surgical indications, as well as evaluating postoperative results. In addition, given the rising use of synthetic implants as interpositional spacers, flexibility testing would be a useful way to evaluate MTP function across multiple treatments for hallux rigidus.
Conclusion
This study provides an important tool for the assessment of hallux rigidus. The flexibility jig was a reliable method to assess motion of the first MTP joint, especially when compared to the lower reliability of existing classification methods. 13 Moreover, the jig illustrates that the function of the first MTP joint as well as outcomes scores were related not just to conventional range of motion but to other inherent flexibility properties measured by the flexibility jig. Flexibility of the first MTP joint should be considered as we attempt to better diagnose and treat hallux rigidus.
Supplemental Material
Supplemental Material, FAO930000-ICMJE - Comparing First Metatarsophalangeal Joint Flexibility in Hallux Rigidus Patients Pre- and Postcheilectomy Using a Novel Flexibility Device
Supplemental Material, FAO930000-ICMJE for Comparing First Metatarsophalangeal Joint Flexibility in Hallux Rigidus Patients Pre- and Postcheilectomy Using a Novel Flexibility Device by Jensen K. Henry, Andrew Kraszewski, Lauren Volpert, Elizabeth Cody, Howard Hillstrom and Scott J. Ellis in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the Hospital for Special Surgery’s Institutional Review Board (#12112, #2013-047).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.