
Abstract
Background:
Severe adult-acquired flatfoot deformity (AAFD) is often associated with painful medial column collapse at the naviculocuneiform (NC) joint. However, many surgeons surgically correct the deformity without directly addressing this joint. The purpose of this study was to examine the role of first-tarsometatarsal (TMT) fusion combined with subtalar fusion in correcting deformity at the NC joint.
Methods:
We retrospectively analyzed 40 patients (41 feet) who underwent first-TMT and subtalar (ST) fusion as part of a flatfoot reconstructive procedure. We assessed 6 radiographic parameters both preoperatively and at a minimum of 6 months postoperatively, including talonavicular (TN) coverage angle, lateral talo–first metatarsal angle, lateral talocalcaneal angle, calcaneal pitch, hindfoot moment arm, and a newly defined navicular-cuneiform incongruency angle (NCIA). Patient-Reported Outcomes Measurement Information System (PROMIS) clinical outcomes were assessed preoperatively and at a minimum 1-year follow-up.
Results:
The NCIA demonstrated excellent interobserver reliability, with no significant change between pre- and postoperative measurements. All other radiographic parameters, except calcaneal pitch, demonstrated statistically significant improvement postoperatively (P < .01). Overall, patients had statistically significant improvement in all PROMIS domains (P < .01), except for depression. Worsening NC deformity was not associated with worse patient-reported outcomes.
Conclusions:
Our data suggest that when addressing painful collapse of the medial arch in patients with AAFD, fusion of the first-TMT joint in combination with other procedures leads to acceptable radiographic and clinical outcomes. There was no change in deformity at the NC joint in our patient cohort at short-term follow-up, and patients achieved significant improvement in multiple PROMIS domains. Although TMT fusion had no effect on NC deformity, residual or worsening NC deformity did not significantly affect clinical outcomes. In addition, the NCIA was found to be a reliable radiographic parameter to assess NC deformity in the presence of talonavicular and/or first-TMT fusion.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Collapse of the medial arch is a characteristic finding in adult-acquired flatfoot deformity (AAFD). AAFD is a progressive, complex disorder associated with degeneration of the posterior tibial tendon as well as other structural deficiencies. 10,11,17,25 Medial arch collapse may occur at the talonavicular (TN), naviculocuneiform (NC), or the tarsometatarsal (TMT) joints and is associated with medial column instability. 24 If left uncorrected, these deformities may become more difficult to manage and lead to poor patient outcomes. 24
Arthrodeses of the hindfoot and/or midfoot are often indicated for symptomatic, severe AAFD. 10,11,31 Rigid hindfoot valgus is typically corrected with subtalar fusion. TN fusion may be added for residual forefoot abduction or supination. While additional midfoot procedures are occasionally required to address “midfoot sag,” there is no clear consensus on the best way to manage this problem. A previous study by Aiyer and colleagues 1 suggest that Cotton osteotomy results in improvement in NC sag postoperatively. Fusion of the first-TMT joint may be performed to address elevation and instability in the first ray such as in the setting of hallux valgus or first-TMT arthritis, but may not be able to compensate for deformity at the NC joint. In addition, there is no consensus on whether correction of NC deformity is important clinically.
Although NC fusion has been shown to improve deformity at the NC joint, it is associated with delayed union and nonunion. 2,12 Nonunion rates reported in the literature range from 3% to 8.5%. 12,18 In addition, a triple arthrodesis along with NC joint fusion can lead to excessive stiffness and resulting patient discomfort. 30 Therefore, we sought to examine the role of combined TMT and hindfoot fusion in restoring medial arch collapse at the NC joint without the addition of NC fusion. In addition, we describe the efficacy of a novel radiographic parameter in assessing congruence at this joint. To date, there have been no studies examining the effect of first-TMT fusion as an adjunctive procedure for deformity correction of severe AAFD with midfoot collapse. We hypothesized that patients with AAFD and painful medial arch collapse would have radiographic improvement in NC joint deformity with first-TMT and subtalar fusions in the absence of NC fusion.
Methods
All patients at the authors’ institution who underwent a flatfoot reconstruction with first-TMT and subtalar (ST) fusions between April 2016 and November 2018 were retrospectively identified. All reconstructions were performed by one of 2 foot and ankle fellowship-trained orthopedic surgeons (S.J.E., J.T.D.). The study protocol was approved by the registry’s research steering committee. All patient demographic, radiographic, and operative information was obtained through chart review. Hospital records were reviewed to record the incidence of postoperative complications including infection, wound healing problems, nonunion, revision surgery, or removal of painful hardware.
Patient Cohort
Patients were eligible to be included in the study if they underwent a flatfoot reconstruction with combined first-TMT and ST fusion with or without additional procedures (see Operative Techniques section) by one of the senior authors (S.J.E., J.T.D.) between April 2016 and November 2018 (Figure 1). Forty-six feet in 44 patients met the inclusion criteria. Patients were excluded for history of tarsal coalition (2 patients), history of prior ipsilateral flatfoot reconstruction (3 patients), or missing preoperative or at least 6-month postoperative weightbearing radiographs (0 patients). In total, 41 feet in 40 patients met the inclusion and exclusion criteria and were included in the study.

Preoperative (A and C) and postoperative (B and D) weightbearing radiographs of flatfoot reconstruction with combined first-tarsometatarsal and subtalar fusions.
This study cohort included 20 men and 20 women with a mean age of 63.8 years (range, 35.9-82.1 years) at the time of surgery. The average body mass index was 30.7 (range, 21.6-43.1). The mean follow-up time was 18.4 months (range, 12-24.5 months).
Radiographic Evaluation
To evaluate deformity at the NC joint, we developed a novel sagittal angle measurement using the articular surfaces of the joint: the navicular-cuneiform incongruency angle (NCIA) (Figure 2). The NCIA was measured by drawing a vertical line from the dorsal to plantar aspect of both the navicular and medial cuneiform articular surfaces on a lateral weightbearing radiograph, and measuring the angle of intersection. This NCIA was arbitrarily defined as positive if the distal articular surface of the cuneiform was plantarflexed compared with the proximal articular surface of the navicular. A negative value indicates sag at the NC joint.

Navicular-cuneiform incongruency angle (NCIA) radiographic measurement on lateral weightbearing radiographs. (A and C) Preoperative NCIA demonstrating sag at the NC joint; a dorsiflexion deformity of the joint results in a negative angle that opens downwards. (B) Postoperative NCIA showing correction of sag at the NC joint in which there is no longer a negative angle. (D) Postoperative NCIA demonstrating worse deformity at the NC joint, as depicted by a greater, negative angle measurement.
Additional previously validated radiographic measurements were also measured. These measurements included on the weightbearing foot anteroposterior view, the TN coverage angle on the lateral weightbearing view, 5 the talo–first metatarsal (Meary) angle, 26 talocalcaneal angle, 26 and calcaneal pitch, 26 and on the Saltzman view, the hindfoot moment arm (HMA). 27
All parameters were digitally measured using a metric software system (IDS7, Sectra, Sweden). Deformity correction was assessed by comparing preoperative radiographs with those taken at final follow-up, a minimum of 6 months after operative treatment. Mean radiographic follow-up was 12.7 (range, 6-26) months. The status of joint fusion, defined as the presence of bridging bone across the fusion site(s), was assessed on the latest plain radiographs. 21
Clinical Outcomes Measurement
Patient-reported outcomes (PROs) were measured using PROMIS, which has been validated for foot and ankle surgery and specifically in patients with AAFD. 3,13,14,16,19 PROMIS is a computerized adaptive test used to assess functional outcomes in multiple domains. The following PROMIS domains were evaluated: Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression. Scores have a standardized mean of 50, the reference population average, with a standard deviation (T score) of 10. Higher scores indicate better physical function, greater severity of pain, better global health, and worse depression. The minimal clinically important difference (MCID) for the PROMIS physical function domain has been previously defined as a range from 7.8 to 9.8 points. 8,15
PROMIS scores were collected both preoperatively and at minimum 1 year postoperatively. Clinical outcomes were measured by the change between preoperative and minimum 1-year postoperative PROMIS domains. Out of the cohort of 40, 32 had both preoperative and minimum 1-year postoperative PROMIS scores, whereas 8 patients were either missing preoperative or postoperative PROMIS scores.
Operative Technique
Two of the senior authors, both fellowship-trained in foot and ankle surgery, performed all flatfoot reconstructions. First-TMT fusion was performed to address first-ray elevation and instability in the setting of hallux valgus, first-TMT arthritis, and/or severe midfoot collapse. Depending on the deformity, procedures performed in addition to the ST and first-TMT fusions included flexor digitorum longus transfer, medializing calcaneal osteotomy (MCO), lateral column lengthening, TN fusion, and spring ligament reconstruction (Table 1). Of the 41 feet included in our study that underwent both first-TMT and ST fusion; 15 feet underwent concomitant TN fusion.
In Addition to First-Tarsometatarsal Joint and Subtalar Joint Fusion, Patients Underwent Additional Concomitant Procedures as Part of Their Flatfoot Reconstruction.a

Abbreviations: FDL, flexor digitorum longus; LCL, lateral column lengthening; MCO, medializing calcaneal osteotomy; TN, talonavicular.
a Percentages are calculated from of a total sample size of 41 feet.
First-TMT fusions were performed through a dorsal longitudinal approach. The joint surfaces were meticulously debrided of cartilage and prepared with flat cuts. Subchondral bone was fenestrated using a small drill or Kirschner wire. Two fully threaded cortical crossing screws were used for fixation. ST fusions were performed using a sinus tarsi approach. After joint preparation as above, 2 screws were used for fixation. Concomitant MCOs were performed through a separate incision with the same screws used to fix the osteotomy and fusion. Postoperatively, patients remained nonweightbearing for 6-8 weeks before progressing to full weightbearing by 10-12 weeks.
Statistical Analysis
The NCIA was measured independently for all subjects by 2 investigators, and interobserver reliability was assessed using intraclass correlation coefficients. Correlations of 0.81 to 0.99 were considered excellent; 0.61 to 0.80, good; 0.41 to 0.60, moderate; 0.21 to 0.40, fair; and
In order to assess whether severity of sag was associated with clinical outcomes, patients with negative postoperative NCIA were stratified into mild vs severe groups based on postoperative NCIA. The cutoff between mild and severe sag was determined by calculating 1 standard deviation below the mean postoperative NCIA. Wilcoxon rank-sum test was used to compare preoperative and postoperative PROMIS outcomes between patients with mild vs severe deformity.
Wilcoxon signed-rank tests were used to compare changes in preoperative and postoperative radiographic measurements and PROMIS scores. Of the 41 feet, 15 feet underwent concomitant fusion of the TN joint. Therefore, a subgroup analysis was performed using the Wilcoxon rank-sum test to compare preoperative, mean change, and postoperative PROMIS as well as radiographic measurements between patients who did and did not undergo TN fusion. All P values were 2-sided and statistical significance was evaluated with an alpha of .05. All analyses were conducted in R (version 3.6.1).
Results
Radiographic Outcomes
At final follow-up, the rate of radiographic union with all procedures combined was 95.1% (39 cases). Preoperatively, the average NCIA was –5.4 degrees (range, –13.7 to 0, SD = 3.5) and postoperatively the average NCIA was –5.1 (range, –18.9 to 2.3, SD = 5.5, P = .513) (Table 2, Figure 3). There was no significant difference between the pre- and postoperative average NCIA. Interobserver reliability was excellent for both preoperative and postoperative NCIA measurements, with an intraclass correlation coefficient of 0.910 and 0.947, respectively. The subgroup analysis demonstrated that patients who underwent TN fusion (n = 15) had similar preoperative NCIA (–6 vs –5 degrees, P = .30) and significantly lower postoperative NCIA (ie, more sag) compared with patients who did not undergo TN fusion (–8.5 vs –3.1 degrees, P < .01) (Table 3).
Mean Preoperative, Postoperative, and Correction in Radiographic Parameters.a

Abbreviations: HMA, hindfoot moment arm; NCIA, navicular-cuneiform incongruency angle; TN, talonavicular.
a P values reflect comparisons between pre- and postoperative values.
*P < .05.

Box-and-whisker plot of preoperative and postoperative navicular-cuneiform incongruency angle (NCIA) measurements. X = mean.
Subgroup Analysis of Radiographic Correction With the Addition of Talonavicular Fusion.a
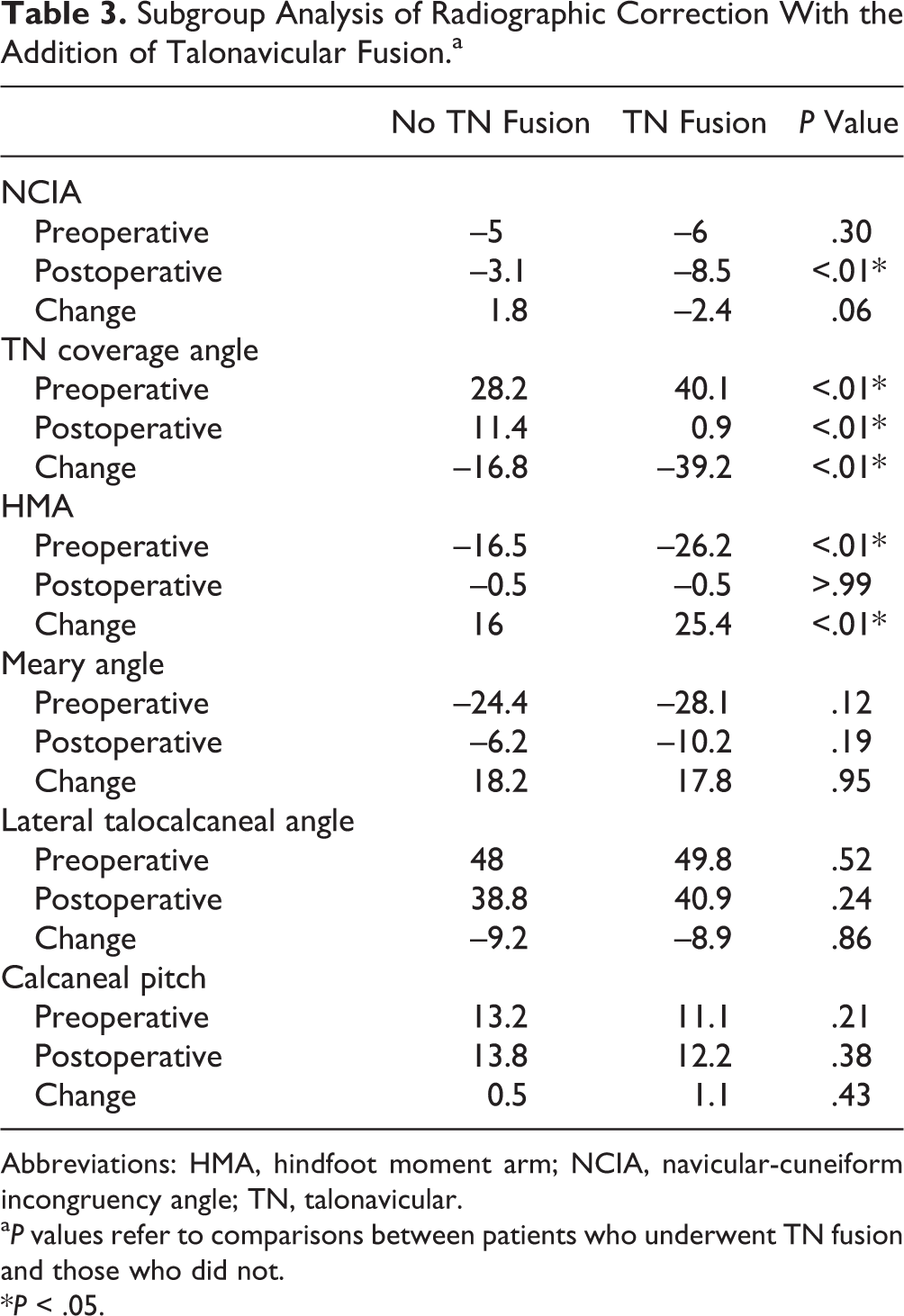
Abbreviations: HMA, hindfoot moment arm; NCIA, navicular-cuneiform incongruency angle; TN, talonavicular.
a P values refer to comparisons between patients who underwent TN fusion and those who did not.
*P < .05.
All other radiographic parameters measured after operative correction demonstrated a statistically significant improvement compared to the preoperative findings, except for calcaneal pitch (Table 2). Patients who underwent TN fusion had worse preoperative talar uncoverage and a greater mean HMA compared with patients who did not. Patients who underwent TN fusion achieved a lower final TN coverage angle (mean 0.9 vs 11.4 degrees, P < .01). There was no difference in final HMA between the 2 groups (P > .99) (Table 3).
Clinical Outcomes
Out of 41 cases (40 patients), 33 cases (80.5%) had both pre- and postoperative PROMIS scores collected with a mean follow-up time of 18.4 months (range, 12-24.5). In the entire cohort, all PROMIS domains except depression showed statistically significant improvement (P < .01) (Table 4). Patients who underwent TN fusion demonstrated no statistically significant differences in improvement in PROMIS domains when compared with patients who did not (Table 5).
Mean Preoperative, Postoperative, and Change in PROMIS Domains.a

Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
a Improvement in each domain is reflected as a positive change in physical function, global physical health, and global mental health, and a negative change in pain interference, pain intensity, and depression. P values reflect comparisons between pre- and postoperative values.
*P < .05.
PROMIS Patient-Reported Outcomes Compared Between Patients With and Without Talonavicular (TN) Fusion.a

Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
a P values refer to comparisons between patients who underwent TN fusion and those who did not.
*P < .05.
In patients with worsening sag at the NC joint, defined as a decrease in NCIA postoperatively, there was no statistically significant difference in pre- or postoperative PROs when compared to patients with improvement in NCIA (Table 6).
Navicular-Cuneiform Incongruency Angle (NCIA) Deformity Analysis.a

Abbreviations: Post, postoperative; Pre, preoperative; PROMIS, Patient-Reported Outcomes Measurement Information System.
a On the left is a comparison of pre- and postoperative PROMIS outcomes between patients with improved postoperative sag, defined as an increase in NCIA, and patients with worse postoperative sag, defined as a decrease in NCIA. On the right is a comparison of pre- and postoperative PROMIS outcomes between patients with mild postoperative sag, defined as an NCIA greater than or equal to –10 degrees, and patients with severe postoperative sag, defined as an NCIA less than –10 degrees.
To differentiate between mild and severe NC sag, an NCIA cutoff value of –10 degrees was used as this was approximately 1 standard deviation below the mean postoperative NCIA. In patients with severe postoperative sag at the NC joint, defined as an NCIA of less than –10 degrees, there was no statistically significant difference in pre- or postoperative PROs when compared to patients with less severe sag deformity (NCIA ≥ –10 degrees) (Table 6).
Complications
Both patients with evidence of radiographic nonunion were symptomatic and underwent revision fusion. One patient underwent revision TN fusion. A second patient, who initially underwent first-TMT and ST fusion, underwent revision ST fusion. A total of 9 patients underwent removal of painful hardware, including first-TMT, MCO, and ST fusion screws.
One patient developed worsening ankle arthritis postoperatively which was treated with conversion to a tibiotalocalcaneal arthrodesis. Three patients had residual hindfoot valgus treated with MCO. There were no incidences of infection or deep vein thrombosis in the immediate postoperative period.
Discussion
Numerous treatment options for the correction of AAFD have been described in the literature. 7,10,11,31 Optimal management is patient-specific and therefore requires a comprehensive clinical and radiographic assessment of the overall deformity. Joint-sacrificing procedures are typically indicated for the most severe deformities. Although subtalar and/or talonavicular fusion are frequently performed, midfoot fusions are less common. Some authors have advocated for NC fusion in cases of substantial midfoot sag, but the indications for this procedure are not well defined. 24,29 Steiner et al examined the role of combined ST and NC fusion in restoring medial arch collapse in severe flatfoot deformity. The authors demonstrated in their cohort of patients a significant correction in Meary angle, talocalcaneal angle, TN coverage, and HMA, concluding that collapse at the medial arch can be restored with these procedures with good clinical and radiographic outcomes. 29 However, the necessity of correcting deformity at the NC joint has not been established.
We report similar radiographic correction in a cohort of patients that did not undergo fusion at the NC joint. In addition, we describe a new radiographic parameter that more specifically measures sag deformity at the NC joint. Some studies have used similar angles to quantify midfoot collapse. 1,4 One of these angles is the medial arch sag angle (MASA) developed by Aiyer et al 1 which utilizes the articular surfaces of the navicular at the TN joint and the medial cuneiform at the first-TMT joint to establish an angle. The authors found that the MASA was useful in assessing restoration of midfoot collapse in the setting of an opening-wedge medial cuneiform (Cotton) osteotomy. 1 However, this angle does not isolate collapse at the NC joint specifically because it spans both the NC and TMT joints. Therefore, we developed a novel radiographic measurement utilizing the articular surfaces of the NC joint with the aim of assessing sagittal deformity at this joint. Our study demonstrates that in patients with AAFD and midfoot collapse, fusion of the first-TMT joint may be an acceptable alternative to fusion of the NC joint, as these patients achieve significant clinical and radiographic improvement without worsening collapse at the NC joint.
Although there was no statistically significant improvement or worsening of NC sag, analysis of NC sag deformity and PROMIS outcomes revealed that neither increased postoperative sag nor severity of sag at the NC joint portended worse postoperative clinical outcomes. This important finding corroborates the clinical experience of the authors, which is that patients tend to tolerate more deformity at the NC joint.
Fifteen cases involved concurrent TN fusion, and therefore a subgroup analysis was performed. Patients who underwent TN fusion were observed to have mild worsening in NCIA of a mean –2.4 degrees whereas patients who did not undergo TN fusion had an improvement of a mean 1.8 degrees (P = .06). This finding could be explained by the effect of deformity correction through fusion at the TN joint, which may lead to transfer of deformity to the NC joint. However, this finding is unlikely to be clinically significant as the degree of change is small and PROs were comparable.
In regard to complications, our overall fusion rate (95.1%) is similar to if not better than those reported in the literature. 6,20,23 Notably, at a minimum of 1 year postoperatively, none of the patients in our cohort underwent fusion for NC arthritis or worsening NC deformity. This further supports the viability of combined first-TMT and ST fusion in AAFD cases with midfoot sag.
Our study is not without limitations. A notable limitation is the potential heterogeneity of our cohort in terms of conventional staging of AAFD. Our cohort consisted of both stage II and stage III patients. Although stage II (flexible) AAFD patients are traditionally indicated for joint-sparing procedures, the senior authors believe that this is not a strict criterion to adhere to. Patients with severe deformities and those with subtalar impingement and/or subluxation are often indicated for subtalar fusion by the authors. 9 In addition, patient age and lifestyle considerations are taken into account. We believe that although our cohort may have been heterogeneous in terms of these 2 disease stages, the benefit of the interventions exists in both groups and should therefore be considered. Another limitation is the relatively short-term follow-up, and that 8 of the 40 patients included in our cohort did not have postoperative PROMIS follow-up. However, these patients did have pre- and postoperative radiographs for comparison and were therefore still included to evaluate our primary outcome. In addition, no power analysis was performed for this study. Relatively few patients are treated with subtalar fusion combined with first-TMT fusion, making this set of patients very difficult to study. Because of the attention given to NC fusion in recent literature, our aim was to add to the understanding of how or if NC joint deformity affects treatment of AAFD. Despite the limitations of our article, we believe that it contributes useful data supporting that NC joint deformity is not important to outcomes.
In conclusion, first-TMT fusion in combination with hindfoot fusion resulted in improvement of radiographic and clinical outcomes. Neither the presence nor worsening of sag deformity at the NC joint was associated with inferior patient outcomes. Although the clinical importance of correction of midfoot collapse in AAFD has not been established, currently either first-TMT fusion or NC fusion appear to lead to good outcomes, irrespective of deformity at the NC joint. Additionally, the NCIA is a new, reliable radiographic measurement for assessing deformity at the NC joint and may be useful in future research studies.
Supplemental Material
Supplemental Material, FAO927321-ICMJE - Contribution of First-Tarsometatarsal Joint Fusion to Deformity Correction in the Treatment of Adult-Acquired Flatfoot Deformity
Supplemental Material, FAO927321-ICMJE for Contribution of First-Tarsometatarsal Joint Fusion to Deformity Correction in the Treatment of Adult-Acquired Flatfoot Deformity by Jonathan Day, Matthew S. Conti, Nicholas Williams, Scott J. Ellis, Jonathan T. Deland and Elizabeth A. Cody in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from Hospital for Special Surgery Foot and Ankle Steering Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.