
Abstract
Background:
Insertional Achilles tendinopathy (IAT) is a common cause of chronic posterior heel pain. Surgical intervention reproducibly improves patients’ pain and functional status. We hypothesized that patients older than 60 years would have similar improvements in pain and function and low rates of complications after surgery for IAT when compared to a younger cohort.
Methods:
Retrospective review of adult case series in patients undergoing surgical management of IAT. Patients were stratified into those 60 years and younger and those older than 60 years. Patients with prior or concomitant surgical procedures and revisions were excluded. Visual analog scale (VAS), Short Form–36 Physical Component Summary and Mental Component Summary (SF-36 PCS/MCS) scores, wound infection, and recurrence, defined as a redevelopment of heel pain in the operative extremity within 6 months, were assessed with a minimum follow-up of 12 months. Statistical analysis was performed using linear regression mixed models and χ2 analysis. Thirty-seven patients were enrolled, with 38 operative heels. The younger cohort had an average age of 49.1 (range, 26-60) years. The older group had an average age of 66.8 (range, 61-76) years.
Results:
VAS and SF-36 PCS scores for the entire cohort significantly improved at 6 and 12 months postoperatively (P < .001). Postoperative SF-36 MCS scores for the cohort significantly improved only at 12 months (P < .001). No significant differences between the young and elderly were seen with regard to improvements in VAS and SF-36 PCS/MCS at 6 or 12 months postoperatively. Multiple linear regression models showed no significant difference between age groups and VAS score, SF-36 PCS/MCS, or change in pain scores after controlling for comorbidities. No significant difference in overall complication rates was seen between the 2 groups (4.9% vs 29.4%, P = .104). There was 1 recurrence of heel pain in the younger group and 4 recurrences of pain in the older group (23.5%) at 6 months, of which 2 resolved at 1 year. There was 1 case of a superficial wound infection requiring antibiotics in the older cohort (5.9%). No patients required surgical revision.
Conclusion:
Surgical management of IAT in an older population produced similar improvements in clinical results when compared to a younger cohort, with no significant increase in postoperative complications.
Level of Evidence:
Level III, retrospective comparative series.
Insertional Achilles tendinopathy (IAT) is a common cause of chronic posterior heel pain, commonly affecting intermittently active individuals, who are usually middle aged to elderly with an incidence between 7% and 9%. 11,12,16,21,24 IAT as first described by Clain and Baxter is defined as tendinopathy at the calcaneal tendon-bone interface and is associated with bursal wall degeneration and formation of a Haglund deformity. 3,4,28
Initial management comprises conservative therapies such as eccentric exercises, extracorporeal shockwave therapy, or injections to the retrocalcaneal bursa, with the majority of literature composed of level IV studies investigating heterogeneous groups of all ages. Patient satisfaction following conservative therapy ranges from 30% to 67%, and the current treatment standard is a trial of differing conservative therapies, with surgical intervention reserved for refractory cases. 6,14,23,27
Surgical management of IAT involves debridement and partial vs complete detachment of the Achilles tendon, as well as resection of the retrocalcaneal bursa and Haglund’s deformity, with subsequent reattachment of the tendon typically with suture anchors. Previous studies from various groups have shown significant positive improvements in patient pain and function scores postoperatively, as well as high postoperative patient satisfaction rates. 21 Review of 6 studies exploring surgical IAT repair from Wiegerinck et al 28 found that 89% of 211 operative tendons, with a weighted mean age of 54 (range, 47-57) years, had excellent or good satisfaction postoperatively. Of the 226 total procedures reviewed, 5 (<3%) developed major surgical complications, including deep wound infections or detachment of the tendon. Recently, similar positive results in surgical correction of IAT have been observed by Guzzini et al, 8 where approximately 80% of their patients reported “good” or “excellent” outcomes and returned to their desired level of preinjury sporting activity.
Aging is known to predispose individuals to an increased risk of tendon injury, as decreases in blood flow and collagen strength—along with increases in tendon stiffness—are primarily responsible for this observed phenomenon. 17,19,25 Recent data have shown the number of people within this aging population who are physically active has increased from 1998 to 2013, and that number continues to trend upward. 15 While positive outcomes in surgical correction have been well documented in groups of a heterogeneous age, there is no literature investigating the sequelae of IAT repair in the elderly.
The aim of this study was to compare the postoperative outcomes of pain, improvements in physical and mental qualities of life, and surgical complications between the young and the elderly who undergo IAT repair with bioresorbable polylactic acid (PLDLLA) suture anchors. Our primary hypothesis was that there would be no significant difference in postoperative outcomes between those 60 years and older and those younger than 60 years undergoing surgical management for IAT.
Methods
This study is an institutional review board–approved retrospective review of prospectively collected data pertaining to a consecutive case series of patients undergoing surgical management for IAT. All patients older than 18 years who underwent surgical management of IAT by the senior author (J.T.B.) were eligible for inclusion in the study. Exclusion criteria were prior surgery or injury to the affected tendon. Patients were divided into 2 groups: those who were older than 60 years and those 60 years and younger. The cohort was identified, and data were collected through review of operative records, clinical notes, and questionnaires conducted at postoperative visits.
A history of rheumatoid arthritis, diabetes mellitus, peripheral arterial disease, chronic obstructive pulmonary disease, coronary artery disease, HIV, thyroid dysfunction, or osteoporosis (diagnosed by documented bone density scan with T score <–2.5) was recorded. Postoperative complications were defined as superficial wound infections (successfully treated with a course of oral antibiotics alone), deep wound infections (requiring formal irrigation and debridement), deep vein thrombosis, recurrence of heel pain (defined as redevelopment of heel pain at 6 months), and need for revision surgery. Pre- and postoperative clinical outcomes were recorded using the visual analog scale (VAS) and Short Form–36 Physical Component Summary and Mental Component Summary (SF-36 PCS/MCS) scores. Functional capacity evaluations were not performed as these data were not routinely collected within the senior author’s practice. Preoperative scores were then compared to scores at 6 months and 1 year. Variance in postoperative outcome scores was assessed by calculation of a delta value to reflect improvement from preoperative to each postoperative follow-up date.
Demographics
Thirty-seven patients were identified, with 38 heels that met inclusion criteria for data analysis. There were 17 cases in patients older than 60 years, with a mean age of 67 (range, 61-76) years, and 21 cases in patients 60 years or younger, with a mean age of 49 (range, 26-60) years. The 2 cohorts were statistically similar in terms of sex, rates of smoking, anticoagulation use, and presence of comorbidities as listed (Table 1). Two patients, 1 in the elderly group and 1 in the younger cohort, did not undergo a calcaneal exostectomy. One patient in the younger cohort required a flexor hallucis longus (FHL) transfer. Five patients had concomitant procedures: in the elderly, 1 patient underwent an ankle arthroscopy, and 1 underwent a peroneus brevis debridement; in the younger cohort, 2 patients underwent a peroneus brevis debridement, and 1 underwent a removal of a calcaneocuboid screw that was initially placed during a revision surgery for a failed calcaneocuboid arthrodesis.
Descriptive Characteristics of Study Population by Age.a
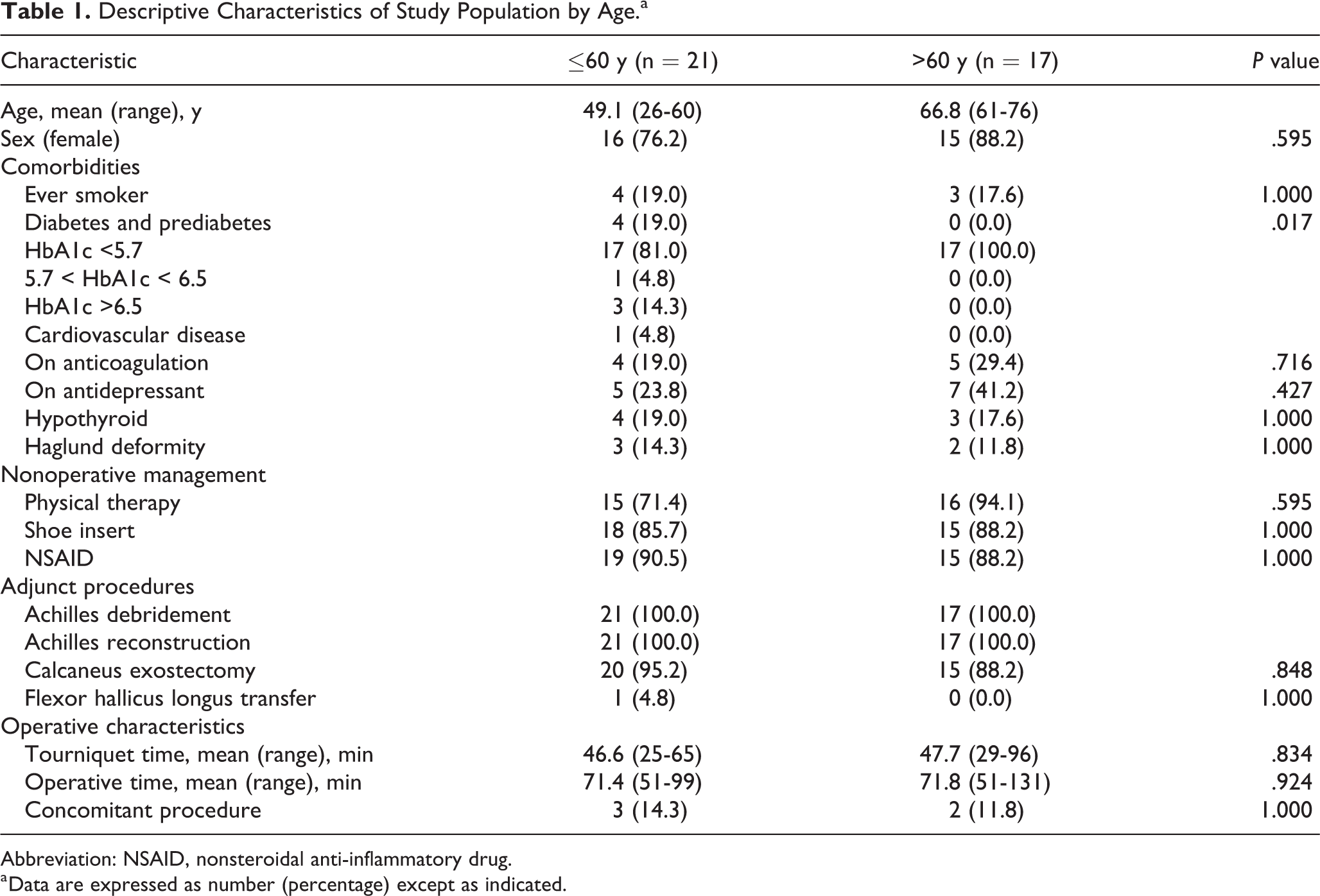
Abbreviation: NSAID, nonsteroidal anti-inflammatory drug.
a Data are expressed as number (percentage) except as indicated.
The operative technique incorporated 3 fully bioresorbable suture anchors in a technique previously described by Boden et al, 1 with a 6- to 8-cm central incision over the Achilles tendon with a central split, debridement of the retrocalcaneal bursa, and a calcaneal exostectomy, if warranted. Tendon reattachment was achieved by use of a double-row PLDLLA suture anchor fixation (SonicAnchor, Stryker). FHL transfer was performed if the debrided portion of the Achilles tendon exceeded more than 50%. Concomitant procedures were recorded and stated in the Results.
Statistical analysis was performed using Welch’s t test for independent groups and a χ2 test for independence to compare continuous and categorical variables, respectively. Differences between the 2 age groupings in VAS, SF-36 PCS, and SF-36 MCS across the time points of interest were analyzed using linear mixed models, including fixed effects for time (preoperative, 6 months, or 1 year) and age groupings (≤60 or >60 years of age), and a random effect for patient ID was included to control for repeated measures. From the linear mixed models, estimated marginal means (with 95% confidence intervals) were used to test differences in mean scores between the groups preoperatively, at 6 months, and at 1 year, as well as the change in scores from preoperative to 6 months and the change in scores from preoperative to 1 year. Statistical significance was determined using a prior a value of .05, and standard error of the means (σx¯) are presented as 95% confidence intervals.
Results
With the numbers available, there was no statistically significant difference between mean tourniquet time, total operative times, or rates of postoperative complications between the 2 groups. Overall complication rates were 4.9% (1 of 21) and 29.4% (5 of 17) for the younger and older cohorts, respectively (P = .104) (Table 2). One patient within the younger group (4.8%) developed a recurrence of heel pain at 6 months, but this was successfully treated with nonoperative modalities by 1-year follow-up. Four patients in the older group (23.5%) redeveloped heel pain at 6 months. Of these patients, 2 were treated successfully at the 1-year mark with nonoperative intervention, and 2 had persistent heel pain at 1 year. No patients required revision surgery due to recurrence of pain. There was 1 case of a superficial wound infection requiring antibiotics in the older cohort (5.9%). Data pertaining to changes in VAS and SF-36 scores at 6 months and 1 year are presented in Table 3.
Complication Rates.
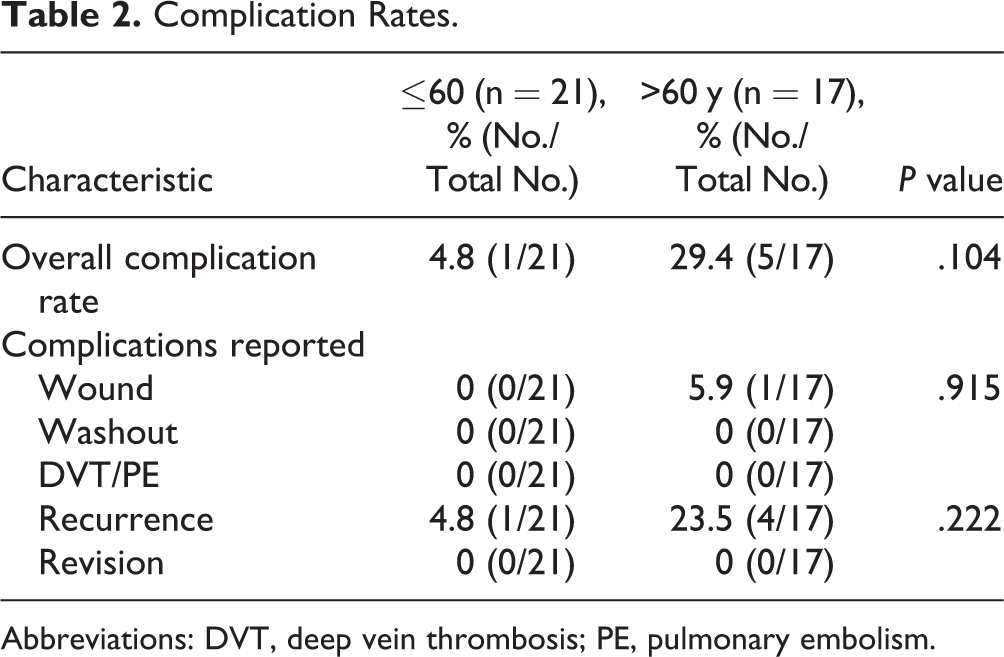
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
Mean VAS and SF-36 Scores.a

Abbreviations: SF-36, Short Form Health Survey, VAS, visual analogue scale.
aData are expressed as mean (95% CI).
b P-value for a test between time point and the preoperative score.
c P-value between the less than equal to 60 and greater than 60 age groups.
dConfidence intervals displayed as: mean value (lower bound of CI to upper bound of CI).
VAS
All patients had a recorded VAS score at the preoperative and 6-month visits. At the 1-year mark, 11 patients (29.7%) did not have a VAS available. VAS scores across both groups were significantly improved by a mean of 3.0 (σx¯: 2.15-3.82) at 6 months and by a mean of 4.5 (σx¯: 3.65-5.43) at 1 year following surgical intervention (P < .0001). Preoperatively, the average VAS in the older group was 5.4 (σx¯: 4.17-6.59) compared with 6.3 (σx¯: 5.20-7.37) in the younger group. With the numbers available, at 6 months, the mean VAS in the older group had improved to 2.7 (σx¯: 1.47-3.88) compared to 3.0 (σx¯: 1.94-4.11) in the younger group, with no significant difference seen in improvements between groups (0.56; 95% CI, –1.11 to 2.22; P = .507). At 1 year, the mean VAS in the older group was 1.3 (σx¯: 0.05-2.57) compared to 1.3 (σx¯: 0.08-2.47), with no significant difference in improvements seen between groups (0.94; 95% CI, –0.84 to 2.72; P = .298) (Figure 1).
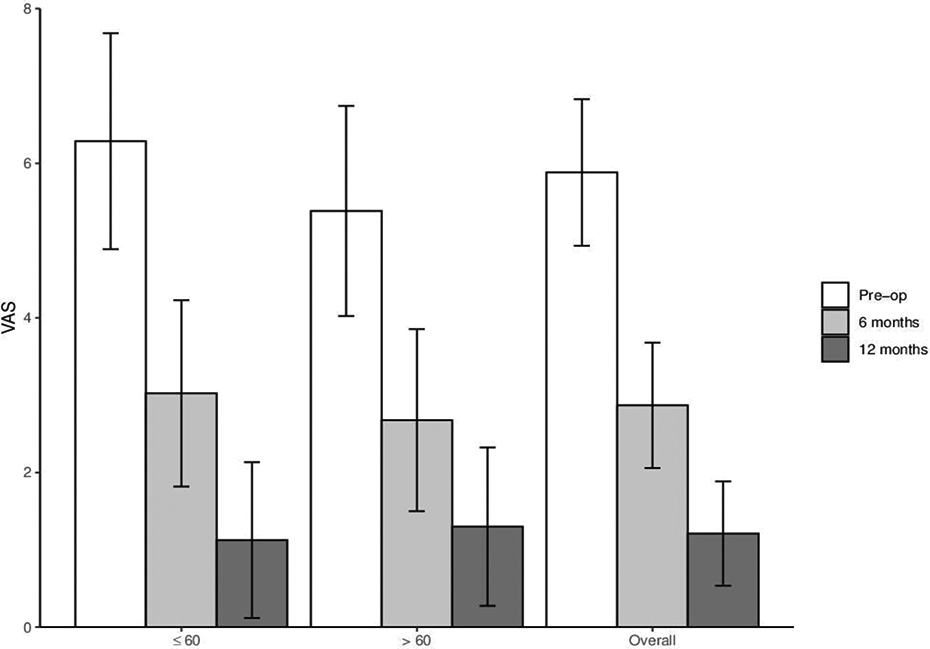
Histogram displaying mean visual analog scale (VAS) scores between the 2 groups at the preoperative, 6-month, and 1-year visit.
SF-36
Thirty-two patients had a recorded SF-36 at the preoperative visit. There were 19 scores available at 6 months and 17 available at 12 months. SF-36 PCS scores across both groups improved significantly over the course of a year following surgical intervention (Figure 2). Preoperatively, the average SF-36 PCS in the older group was 49.4 (σx¯: 39.5-59.4), compared with 49.3 (σx¯: 40.2-58.3) in the younger group. With the numbers available at 6 months, the mean SF-36 PCS in the older group had improved to 58.7 (σx¯: 48.0-69.4), compared to 71.3 (σx¯: 59.1-83.6) in the younger group, with no significant difference in improvement between groups (–12.8; 95% CI, –28.9 to 3.4; P = .118). Similarly, at 1 year, the mean SF-36 PCS in the older group was 69.8 (σx¯: 59.6-80.0), compared to 79.6 (σx¯: 69.1-90.1) in the younger group, with no significant difference in improvement seen between the 2 groups (–10.0; 95% CI, –24.3 to 4.4; P = .168).
Grouped MCS scores significantly improved at 1 year postoperatively (13.5; 95% CI, 4.9-22.1; P = .003). Preoperatively, the average SF-36 MCS in the older group was 70.0 (σx¯: 59.1-80.7), compared with 67.0 (σx¯: 57.2-76.8) in the younger group. With the numbers available at 6 months, the mean SF-36 MCS in the older group had improved to 68.4 (σx¯: 56.6-80.1), compared to 78.1 (σx¯: 64.3-92.0) in the younger group, with no significant difference in improvements seen between the 2 groups (−12.7; 95% CI, –31.9 to 6.6; P = .193). At 1 year, the mean SF-36 MCS in the older group was 79.1 (σx¯: 68.1-90.2), compared to 84.8 (σx¯: 73.1-96.4), with no significant difference in improvement seen between the 2 groups (–8.5; 95% 95% CI, –25.7 to 8.7; P = .323) (Figure 3).

Histogram displaying mean Short Form–36 Physical Component Summary (SF-36 PCS) scores between the 2 groups at the preoperative, 6-month, and 1-year visit.

Histogram displaying mean Short Form–36 Mental Component Summary (SF-36 MCS) scores between the 2 groups at the preoperative, 6-month, and 1-year visit.
Discussion
Operative intervention for IAT refractory to conservative therapy in the elderly may often be deferred due to fear of surgical-related complications and recurrence. Within our cohort, there was no statistical difference seen in complication or recurrence rates between patients older and younger than 60 years who underwent operative treatment for IAT.
Tenodesis using a double-row bioresorpable suture anchor technique with nonabsorbable sutures was the primary method of bony fixation within our cohort, with no patients requiring a revision surgery, a similar finding to other studies using suture anchor fixation with differing methods of suturing to the tendon. 5,7,18,21,22,29 Our series also shows a significant improvement in the physical and mental quality of life within our patients at 1 year, as quantified using the SF-36 form. Other studies have predominantly used the American Orthopaedic Foot & Ankle Society (AOFAS) score to quantitate surgical outcomes. 13,20,26 We opted to use the SF-36 and VAS as our main patient-reported outcome, as they are both a well-reputed and thoroughly published quality-of-life metric within the foot and ankle literature, as well as patient-reported rather than physician-reported outcomes. 2,9,10
Oshri et al 21 described their cohort of 21 cases undergoing surgical management with a lateral incision for IAT refractory to conservative therapy, with a mean age of 51 years, and found a statistical improvement in preoperative VAS scores of 7.9 ± 1.8 to 3.7 ± 3.8 at 6 months. Gillis and Lin 7 presented their series of 14 cases, with a mean age of 54 years, undergoing a central splitting debridement with a double-row bridging suture anchor repair and showed a significant improvement of preoperative VAS from 7.25 to 1.81. No preoperative SF-36 scores were obtained within their population, although there was a mean postoperative SF-36 PCS of 77.7 with a mean follow-up of 18 months. Ettinger et al 5 presented their series of 45 consecutive patients with a mean age of 52 years undergoing either single or double anchor row fixation of the Achilles tendon and found a significant improvement in pre- and postoperative SF-36 MCS from 69.5 ± 21.9 to 78.2 ± 18 and a nonsignificant increase in SF-36 PCS from 42.8 ± 23.2 to 81.8 ± 21.4 at 12 months.
Our study carries with it an inherent recall bias secondary to its retrospective design, as well as a relatively short follow-up time of 12 months. A post hoc power analysis for the change in preoperative to 1-year scores between the age groupings revealed low power (VAS, 19%; SF-36 PCS, 31%; and SF-36 MCS, 19%). However, as previous literature has noted, post hoc power analyses should be interpreted cautiously as they are directly related to the observed effect size and sample size of the study in question. 30 Furthermore, there were patient reported outcomes at 6 and 12 months that were lost to follow-up. Despite these limitations, we present a consecutive series of 38 patients undergoing surgical management of IAT by a single surgeon, limiting variation in technique, as well as their outcomes at both 6 months and 1 year.
Conclusion
Operative intervention for IAT refractory to conservative measures was a valid option for all patients, irrespective of age, with similar rates of improvement in pain and quality-of-life metrics and no difference in postoperative complications at 1 year. Further prospective higher-powered studies would be of benefit to further ascertain and quantify the benefit of operative intervention in the elderly.
Supplemental Material
Supplemental Material, FAO-20-0032-ReportedAuthorDisclosures-final - Outcomes of Operative Management of Insertional Achilles Tendinopathy in the Young vs Elderly
Supplemental Material, FAO-20-0032-ReportedAuthorDisclosures-final for Outcomes of Operative Management of Insertional Achilles Tendinopathy in the Young vs Elderly by Huai Ming Phen, Wesley J. Manz, Danielle Mignemi, Joel T. Greenshields and Jason T. Bariteau in Foot & Ankle Orthopaedics
Supplemental Material
Supplemental Material, FAO926101-ICMJE - Outcomes of Operative Management of Insertional Achilles Tendinopathy in the Young vs Elderly
Supplemental Material, FAO926101-ICMJE for Outcomes of Operative Management of Insertional Achilles Tendinopathy in the Young vs Elderly by Huai Ming Phen, Wesley J. Manz, Danielle Mignemi, Joel T. Greenshields and Jason T. Bariteau in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from Emory University Institutional Review Board. Approval number: IRB00076989 (Surgical Foot and Ankle Registry).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.