
Abstract
Background:
The Ponseti method has revolutionized the treatment of idiopathic clubfoot, but recurrence remains problematic. Dynamic supination is a common cause of recurrence, and the standard treatment is tibialis anterior tendon transfer using an external button. Although safe and effective, the placement of the button on the sole creates a pressure point, which can lead to skin ulceration. In our institution, a suture button has been used for the tibialis anterior tendon transfer and we report our results here.
Methods:
Two senior authors’ case logs were retrospectively reviewed to identify 23 patients (34 feet) for tibialis anterior tendon transfer using a suture button. Complications and additional operative procedures were assessed by reviewing operative notes, follow-up visit clinic notes, and radiographs. The mean age of the patients was 6 years 2 months (SD 40 months) and the average follow-up duration was 67.1 weeks (SD 72 weeks).
Results:
There were 5 complications (14.7%). Recurrence occurred bilaterally in 1 patient (5.9%) but did not require reoperation. Other complications included a cast-related pressure sore (2.9%) and an infection (2.9%) requiring irrigation with debridement along with hardware removal.
Conclusions:
Tibialis anterior tendon transfer using a suture button was a safe procedure with theoretical advantage of providing stronger fixation and reducing the risk of skin pressure necrosis compared to the standard external button technique. We believe a suture button could allow earlier rehabilitation and may afford stronger ankle eversion. Prospective studies are required to compare the differences in functional outcomes between the procedures.
Level of Evidence:
Level IV, case series, therapeutic study.
Introduction
Congenital talipes equinovarus, also known as congenital clubfoot, is a common congenital lower limb defect resulting in a characteristic foot deformity of hindfoot equinus and varus, and mid-/forefoot adduction and cavus. In the past, idiopathic clubfoot was predominantly managed with extensive soft tissue surgery, which produced unpredictable and often unsatisfactory results. 8,15 Over the past few decades, a less invasive regimen by Ignacio Ponseti, which involves serial gentle manipulations and casting, has gained popularity for its excellent success rates and the prevention of relapse. 7,19,22 The Ponseti method is currently considered the treatment of choice for the initial management of idiopathic clubfoot.
Despite the excellent effectiveness in the correction of deformity at its initial phase, the recurrence rate is still considerable after treatment with the Ponseti method. Multiple studies have shown the success rate at early follow-up to be very high, ranging from 92% to 100%. 5,6,21 However, the rate of relapse in long-term follow-up was reported to be as high as 62.5% in one study. 22 A study by Janicki and colleagues 17 demonstrated a significant decrease in the relapse rate when a foot abduction orthosis was used instead of an ankle-foot orthosis, from 83% to 31%. Other studies that used boots and bars orthosis to maintain the foot in abduction have shown generally lower recurrence rates, ranging from 22% to as low as 4%. 1,3,26,34 Noncompliance with the orthosis is quoted as the most contributing factor for the relapse. 1
Nonetheless, recurrence does occur and poses a challenge to orthopedic surgeons. A common cause of recurrence is dynamic supination of the foot, which results from the overactivation of the tibialis anterior muscle during ankle dorsiflexion. 31 Garceau is reported to be the first surgeon to perform tibialis anterior tendon transfer (TATT) in order to correct dynamic supination. 12 Traditionally described procedures for correcting recurrence involve the transfer of the tibialis anterior tendon to either the base of the fifth metatarsal or cuboid. 12 Multiple studies have demonstrated that TATT is effective in preventing the recurrence of clubfoot, particularly dynamic supination. 16,20,31 The most commonly used technique has been to transfer the entire tendon through a drill hole in the lateral cuneiform and to afix it against the plantar aspect of the foot using a sewing button and felt pad. 18,20,31 Although this is an effective procedure, the placement of the button on the sole increases the risk of a pressure sore (Figure 1). Agarwal and colleagues 2 found no complications/recurrences in a pilot study of 30 patients (46 feet) treated with 3 common techniques for anterior tibial tendon transfer, using the external button as an anchor. However, this was at short-term follow-up (average of 5.5 months). Although most studies on the use of the external button in TATT for recurrent club foot report degree of correction achieved with the respective TATT techniques, they do not explicitly report on wound complication and recurrence rates. 10,20,31

Infected skin necrosis due to the pressure from the external button placement.
In our institution, 2 pediatric orthopedic surgeons have used a novel technique to eliminate the external placement of the button by using a suture button. The purpose of this study is to describe this novel technique and report the complication profiles for the patients who have undergone this procedure. To our knowledge, there has been no published article that describes the operative technique for TTAT using this suture button.
Methods
After ethics approval was obtained, TATT cases were identified from the case logs of 2 local senior surgeons between the year 2011 and 2016. We included TATT as a sole procedure or done in conjunction with other foot reconstruction procedures such as Achilles tendon lengthening, posterior release, and/or corrective osteotomies. The main indication for this procedure was the same as the traditional tendon transfer technique—dynamic supination seen in recurrent idiopathic clubfoot. 13 The use of a suture button (EndoButton; Smith & Nephew Endoscopy, Andover, MA) was confirmed with both operative records and postoperative radiographs showing its placement. Upon confirmation of the procedure, patients’ follow-up visit clinic notes and radiographs were reviewed to screen for any postoperative complications. Patients with follow-up less than 12 weeks were excluded.
A total of 23 patients (34 feet) underwent the index procedure since August 2011 when we first used the suture button for the TATT procedure. The mean age of the patient at the time of operation was 6 years 2 months (28-193 months, SD 40 months), and the average follow-up was 67.1 weeks (12.1-249 weeks, SD 72 weeks).
Operative Technique
The patient is positioned supine on a standard operating table with a radiolucent extension. A medial longitudinal incision just proximal and lateral to the insertion of the tibialis anterior tendon is made (Figure 2). The identification of the insertion of the tendon was optimized using fluoroscopy as a guide in locating the base of the first metatarsal. Once identified and the skin incision made, the tibialis anterior tendon sheath is incised longitudinally and the tendon sharply dissected off its broad insertion on the base of the first metatarsal. The resected tendon should be of appropriate length, that is, able to reach the plantar aspect of lateral cuneiform with the foot both in dorsiflexion and eversion. Excess tendon should be resected to avoid redundancy that would compromise tensioning and correction of the deformity. Friden and colleagues, in a 1998 study on tendon lengths in transfer surgery, determined that if resting sarcomere length (tendon stretch at rest) was short then length would remain close to optimal at any given tension. 11 The application of a below knee cast in dorsiflexion, at the end of the procedure, also helps keep tendon stretch to a minimum during the healing process. Using a strong nonabsorbable suture, a running whip-stitch is applied to the end of exposed tendon (Figure 3). The diameter of the whip-stitched tendon is measured to help approximate the size of bone tunnel needed.

Standard skin incision for the retrieval of the tibialis anterior tendon.

Tibialis anterior tendon was retrieved and whip-stitch was placed using the Ultrabraid suture.
A dorsolateral longitudinal incision is made over the lateral cuneiform (Figure 4). The lateral cuneiform is exposed by retracting the tendons of the extensor digitorum longus medially and the tendons of the extensor digitorum brevis laterally. A blunt hemostat is used to develop a subcutaneous plane (beneath extensor retinaculum) for the transfer of the tibialis anterior tendon. Grasping the suture ends, the tibialis anterior tendon is passed underneath the extensor retinaculum of the ankle with a straight line of pull to the lateral incision (Figure 5). The lateral cuneiform is identified using fluoroscopy, and an appropriately sized bone tunnel is drilled in the lateral cuneiform from a dorsolateral to plantar-medial direction. The EndoButton (with 4 holes) is used to anchor the tendon suture. First, the 2 ends of the tendon sutures are passed through the middle holes of the suture button (Figure 6A). Each suture end is doubled back through their respective medially adjacent holes and pulled toward the tendon and left untied, allowing for appropriate tensioning of the tendon once seated in the tunnel (Figure 6B). Two strong sutures of different colors are passed through each of the peripheral holes (Figure 6C). The sutures are then passed through the lateral cuneiform tunnel to the sole of the foot using straight needles (Beath pin) (Figure 6D). The leading suture is pulled so that the suture button completely exits the plantar surface of the hole. The trailing suture is pulled to flip the suture button so that it sits flush against the plantar cortex of the lateral cuneiform. The tendon sutures pull the tibialis anterior tendon through the tunnel (Figure 7). A fluoroscopic image confirms the position of the suture button (Figure 8). The ankle is placed in maximal eversion and dorsiflexion to facilitate appropriate tensioning of the tendon. 27 Once the tendon is in a satisfactory position, a Mayo needle is used to tie the tendon sutures through the most proximal part of the tendon, thereby further maximizing the tension. The leading and trailing sutures are pulled and discarded. A well-padded below knee plaster cast is placed with the ankle in eversion and 10 degrees dorsiflexion.

(A) Dorsolateral longitudinal incision is made over the lateral cuneiform where the tibialis anterior tendon will be fixated. A needle is placed over the lateral cuneiform. (B) The fluoroscopic image confirms that the needle is placed in the lateral cuneiform.

Tibialis anterior tendon is brought through the dorsolateral incision.

Stepwise approach to EndoButton passage and placement: (A) passage of tendon sutures through 2 central holes on EndoButton; (B) each suture end looped back toward the tendon with passage through respective medial hole; (C) a lead suture (green Ethibond) is passed through one peripheral hole and trailing suture (purple Vicryl) is passed through the other peripheral hole; (D) button and sutures passed through bone tunnel using a Beath pin. Tensioning the lead suture passes the EndoButton while tensioning trailing suture flips and seats it on the plantar surface.

Direct visualization dorsally confirms that the tibialis anterior tendon is seated within lateral cuneiform bone tunnel.
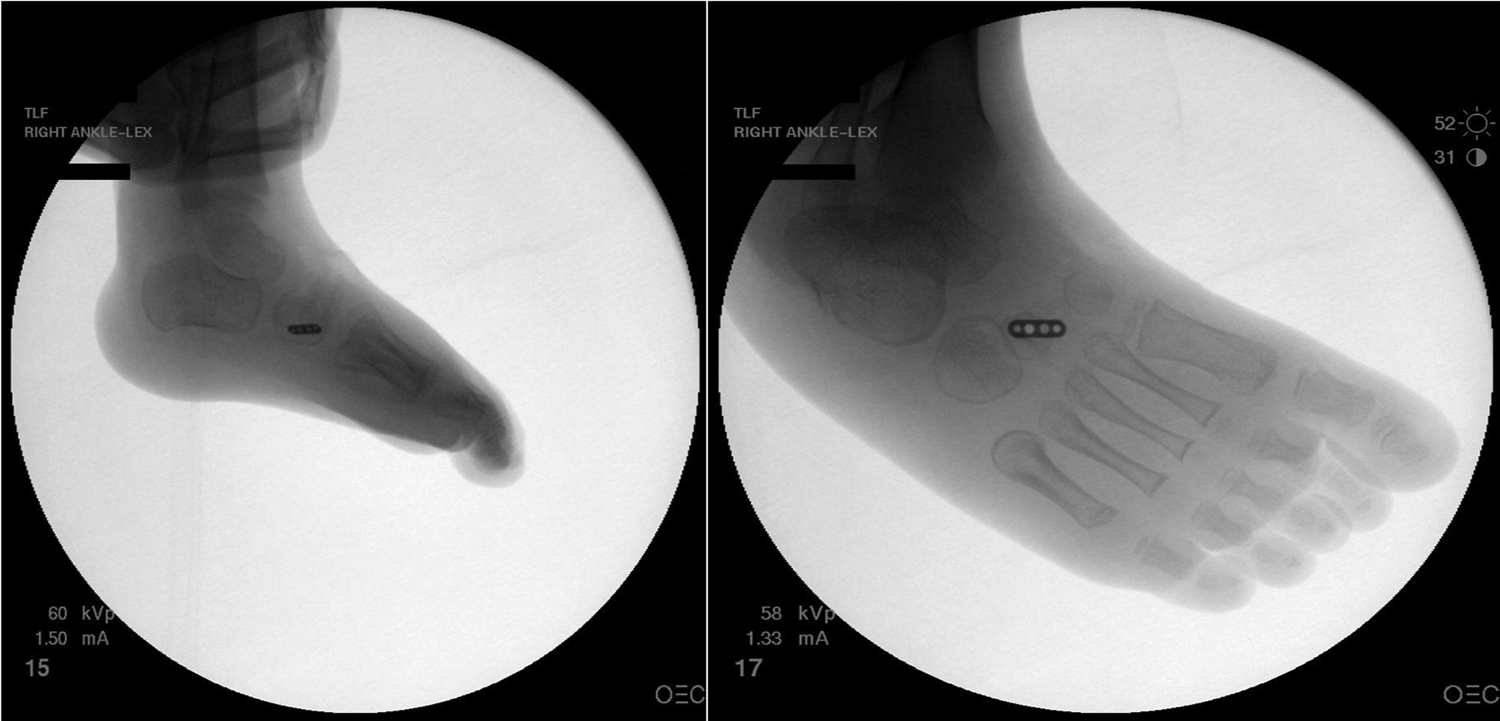
Fluoroscopic images confirming the satisfactory placement of the EndoButton.
Postoperative Care
The cast can be split to allow swelling during the immediate postoperative period or if a nerve block is used. The patient is kept nonweightbearing in a cast for 6 weeks and allowed to weight-bear as tolerated thereafter. If there is any concern about the fixation, plain radiographs of the foot confirmed the suture button position. After 6 weeks, there are no limitations placed on range of motion (active or passive).
Results
Overall, there were 5 complications (14.7%, 5/34) with varying degrees of severity. There was one instance of bilateral recurrence treated conservatively (5.9%, 2/34). There was 1 loss of fixation of the suture button (2.9%, 1/34), and there was 1 infection in the dorsum of the foot requiring irrigation and debridement and implant/suture removal (2.9%, 1/34). There was 1 minor complication (2.9%, 1/34) involving the plantar aspect of the foot, irritation caused by a pressure point from the cast. This pressure point was without ulcer or blister and resolved spontaneously without any active treatment. The patient (2 feet) who experienced recurrence of foot deformities had progressive metatarsus adductus and equinus. This complication was likely not due to the TATT, but rather a failure of procedures performed in conjunction, that is, bilateral Achilles tendon lengthening and posterior release. This was treated conservatively with boots and bars, with no signs of recurrence at 1-year follow-up. One patient experienced loss of fixation at 2 weeks because of suture button and tendon displacement through the bone tunnel to the dorsal aspect of the foot. We suspect the suture button was not adequately seated against the plantar cortex of the lateral cuneiform during the index procedure. This patient underwent successful revision surgery with a new suture button. Table 1 outlines the study population and the nature of complications encountered. Procedures were categorized as complex foot reconstruction whenever there were 2 or more bony procedures performed in 1 foot in conjunction with the TATT.
Summary of the Patients Who Underwent the TATT.

Abbreviations: B, bilateral; I&D, irrigation and debridement; L, left; R, right; TAL, Tendo Achilles Lengthening; TATT, tibialis anterior tendon transfer.
Discussion
The Ponseti method has revolutionized the treatment of clubfoot by reducing the magnitude and number of operations for clubfoot with outcomes superior to previous methods including operative release and reconstruction. 29 Yet, recurrence of the deformity remains a significant issue. The most common recurrent deformities are forefoot adduction and supination. 24 TATT is a well-described technique to address dynamic supination with good mid-term and long-term results. 9,10 However, traditional external button placement can lead to pressure necrosis and wound complications. In this study, we describe a novel technique for TATT using a suture button, which eliminates the need for external button placement. We also demonstrated the safety and effectiveness of this technique in reporting a recurrence rate of 5.9% (2/34) and postoperative infection rate of 2.9% (1/34). There was one instance of postoperative loss of fixation treated successfully with suture button revision. The technique employed in revision surgery depends on the mode of fixation failure. Failure of fixation due to a larger bone tunnel or disruption of the plantar cortex may be revised using a larger suture button. Another alternative would be to revise to the external button technique. However, we believe the most likely cause of mechanical failure that likely occurred here to be improper flipping and anchoring of the suture button against the plantar cortex of the lateral cuneiform intraoperatively. This will result in the suture button pulling out through the bone tunnel and subsequent loss of tension.
Regarding potential modes of suture button failure in the postoperative period, we predict infection to be the most common nonmechanical cause. The patient in our case series diagnosed with an infection was managed with operative irrigation and debridement along with hardware removal. We recommend that all postoperative infections be treated in this manner. Decision on revision TATT surgery may be made later after the infection has completely resolved.
Our technique was used both as an isolated procedure and in conjunction with other soft tissue and bony procedures in the foot to treat the recurrence of clubfeet. Except for 1 patient who had fixation failure, dynamic supination was successfully corrected for all feet. A recent biomechanical study by Pathy and colleagues on cadaveric feet showed that the internal button technique provided more solid fixation compared to the traditional external suture-button, in theory allowing for improved tendon-bone integration while avoiding the risk of plantar skin ulceration. 25 The suture button alleviated undue external pressure to the sole of the foot and has shown excellent outcomes for the operative repair or reconstruction of anterior cruciate ligament, posterior cruciate ligament, biceps brachii, and pectoralis major tendons. 4,14,28,32
A bioabsorbable interference screw is another commonly used TATT technique and has been shown to achieve good fixation while also alleviating the risk of skin ulceration seen with the external button technique. 33 A biomechanical analysis by Mazzocca and colleagues has shown that the tendon fixation using the suture button technique can resist greater load before failure when compared with other anatomic fixation techniques, including bone tunnel, suture anchor, and interference screw. 23 Recently, surgeons have employed the interference screw in conjunction with the suture button for TATT as a second method of fixation to further reduce the risk of failure. 30 Although this combined technique was not employed in this study, it could further improve security of the fixation.
The main limitation of the current study is in its retrospective nature and lack of prospective assessment of the patients. Follow-up clinic notes often do not provide objective measures to reliably assess the results of the operation. Most TATTs were performed as part of complex foot reconstructive procedures, which make it difficult to ascertain the true cause of any recurrence. The one recurrence we identified presented with metatarsus adductus and equinus after our surgery that also included tendo-Achilles lengthening and posterior release. A prospective study comparing this novel technique alone to the external button with objective measures of recurrence and complication rates may confirm its relative superiority. We believe that the strong and reliable fixation achieved with the suture button may allow earlier rehabilitation and may result in stronger ankle eversion.
In conclusion, this novel TATT technique using a suture button was a safe procedure that eliminated the risk of plantar pressure necrosis associated with the traditional TATT technique while theoretically providing stronger tendon fixation. Further studies are required to compare the differences in functional outcomes between the procedures.
Supplemental Material
Supplemental Material, FAO923591-ICMJE - Suture Button Technique for Tibialis Anterior Tendon Transfer for the Treatment of Residual Clubfoot
Supplemental Material, FAO923591-ICMJE for Suture Button Technique for Tibialis Anterior Tendon Transfer for the Treatment of Residual Clubfoot by Chanseok Rhee, Bernard Burgesson, Ben Orlik and Karl Logan in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.