
Abstract
Background:
Perioperative opioid consumption has received a great deal of recent attention. However, perioperative opioid utilization in the total ankle arthroplasty (TAA) population has not been well studied. We sought to identify factors associated with postoperative opioid use following TAA.
Methods:
The PearlDiver Research Program was used to query the Humana, Inc, administrative claims database from 2007 to 2017 for patients undergoing TAA. Additional variables of interest were identified using ICD-9 and ICD-10 codes. Preoperative opioid use was defined as having filled an opioid prescription in the 3 months before TAA. Prescription opioid claims data were tracked for 12 months postoperatively. Risk ratios (RRs) were calculated and multivariate analysis was performed at 3, 6, and 12 months postoperatively.
Results:
A total of 544 patients who underwent TAA were identified, with 180 (33.1%) filling an opioid prescription preoperatively. Those filling prescriptions preoperatively had a significantly greater risk for postoperative opioid use compared to those not taking opioids (RR: 4.36 [95% confidence interval (CI): 2.80-6.80] at 12 months). Anxiety or depression (RR: 2.27 [1.44-3.59]), low back pain (LBP) (RR: 2.27 [1.50-3.42]), and fibromyalgia (RR: 2.15 [1.42-3.28]) were also found to increase the risk of taking opioids at 12 months postoperatively. Multivariate analysis found preoperative opioid use to be the strongest predictor of postoperative opioid use.
Conclusions:
Nearly one-third of patients filled an opioid prescription within 3 months of TAA, and filling a prescription preoperatively was the strongest factor associated with postoperative opioid use. Fibromyalgia, depression or anxiety, and LBP were also associated with an increased likelihood of postoperative opioid use.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
In the United States, opioids are frequently prescribed following operations such as total ankle arthroplasty (TAA) and occasionally for symptomatic treatment of osteoarthritis, despite publications such as the American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for management of osteoarthritis of the knee and hip not recommending opioids as a treatment option. 1 Opioid prescribing rapidly increased in the 1990s, with some attributing the increase to a movement to assess pain as the “fifth vital sign.” 14 The United States consumes more than 80% of all opioids prescribed globally, with orthopedic surgeons accounting for 7.7% of all issued opioid prescriptions. 11,18 Along with the increased prescribing, there has been an increase in abuse. Opioid-related deaths have surpassed deaths related to suicide, motor vehicle crashes, as well as other drugs such as cocaine and heroin combined. 10 Some studies have shown worse patient-reported outcomes following routine orthopedic procedures, such as total knee arthroplasty, spine surgery, or shoulder arthroplasty, to be associated with opioids use. 9,13,20 A recent study found preoperative opioid use to be associated with increased emergency room visits, wound complications, and revision surgery following total knee arthroplasty, total hip arthroplasty, and posterior spinal fusion. 8 As a result of the multitude of negative consequences of opioid use, prescribers have begun to consider alternative strategies for pain management in the perioperative setting and decrease the number of opioids they prescribe.
A recent 2019 retrospective cohort study using data from the nationwide Premier Healthcare claims database showed decreasing trend of inpatient opioid use following TAA from 2011 through 2016. 6 Despite increasing popularity of TAA, data on perioperative opioid use following this procedure remains extremely limited. Therefore, the purpose of this study was to identify preoperative factors associated with postoperative opioid use in patients undergoing total ankle arthroplasty.
Methods
The PearlDiver Research Program (PearlDiver, Fort Wayne, IN) was used to query the Humana, Inc, administrative claims database. This data set contains patient records from 2007 through the first quarter of 2017 and encompasses more than 25 million covered lives. It includes both patients who have private insurance and those who have Medicare Advantage plans. All patient records were deidentified and were fully compliant with the Health Insurance Portability and Accountability Act. Our institutional review board reviewed the study methodology and provided an exemption from human subjects research.
Patients who underwent primary TAA were identified using Current Procedural Terminology (CPT) code 27702. Insurance claims data for opioid prescription medication were assessed during the 3 months prior to the index TAA and longitudinally at monthly intervals for 12 months postoperatively. Patients were only included if they remained in the data set for the entire study period to eliminate those who were lost to follow-up and did not have complete prescription claims records available to query. The query identified claims for all commercially available oral and transdermal prescription opioid medications, specifically including hydrocodone, oxycodone, hydromorphone, codeine, morphine, fentanyl, oxymorphone, and methadone. Opiates in combination with other analgesic medications were included, such as oxycodone with acetaminophen or ibuprofen. Products in combination with medications intended to treat cough or cold symptoms were excluded. Because tramadol does carry an AAOS Clinical Practice Guideline recommendation for treatment of some forms of osteoarthritis, 1 it was not included in this portion of the query with the pure opioid agonists. Patients were stratified based on claims data for prescription opioids in the 3 months preceding TAA into 2 groups: opioid use or no opioid use.
Additionally, patients were stratified by concurrent diagnoses of low back pain (LBP), fibromyalgia, depression or anxiety disorder, sex, smoking status, and filling a prescription for tramadol during the 3 months prior to TAA. These groups were defined as tracked variables available for query within the PearlDiver Research Program (sex) or using International Classification of Diseases (ICD)-9 and 10 codes (Appendix A). Age (≥50 or ≤49 years), drug abuse, and alcohol abuse were queried as variables of interest; however, there were too few of these patients who also underwent TAA to assess postoperative opioid use.
The number of patients who filled a prescription for an opioid medication was tracked monthly for each of the 12 months following TAA. Risk ratios (RRs) were determined for each of the patient factors at each monthly interval. Analytics software within the PearlDiver Research Program was then used to perform multivariate Poisson regression to calculate odds ratios (ORs) for filling of opioid prescriptions at 3, 6, and 12 months following TAA. Criteria for inclusion in the model was set at P <.1 and the following variables were included: preoperative opioid use, fibromyalgia, LBP, depression or anxiety, and smoking. Sex met criteria for inclusion in the multivariable model at 3 and 6 months, and preoperative tramadol use was included at 6 and 12 months.
Results
A total of 544 patients who underwent TAA were identified. Of these, 282 patients (51.8%) were female and 529 patients (97.2%) were age 50 or greater. Opioid prescriptions were filled within the 3 months prior to the operation for 180 patients (33.1%). In those with preoperative opioid use, there was significantly greater risk for opioid use in each of the 12 months following TAA compared to those who did not fill an opioid prescription in the 3 months prior to surgery, with a peak risk at 11 months (RR: 5.78 [95% confidence interval (CI): 3.68-9.07]) (Table 1). At 12 months after TAA, 30.5% of those taking opioids preoperatively continued to fill a prescription for an opioid medication, contrasted with only 6.9% of patients who did not receive opioid prescriptions in the 3 months prior to surgery (Figure 1).
Relative Risk for Filling Opioid Prescription by Month After Total Ankle Arthroplasty (TAA).a

a Data is presented as relative risk (95% confidence interval).
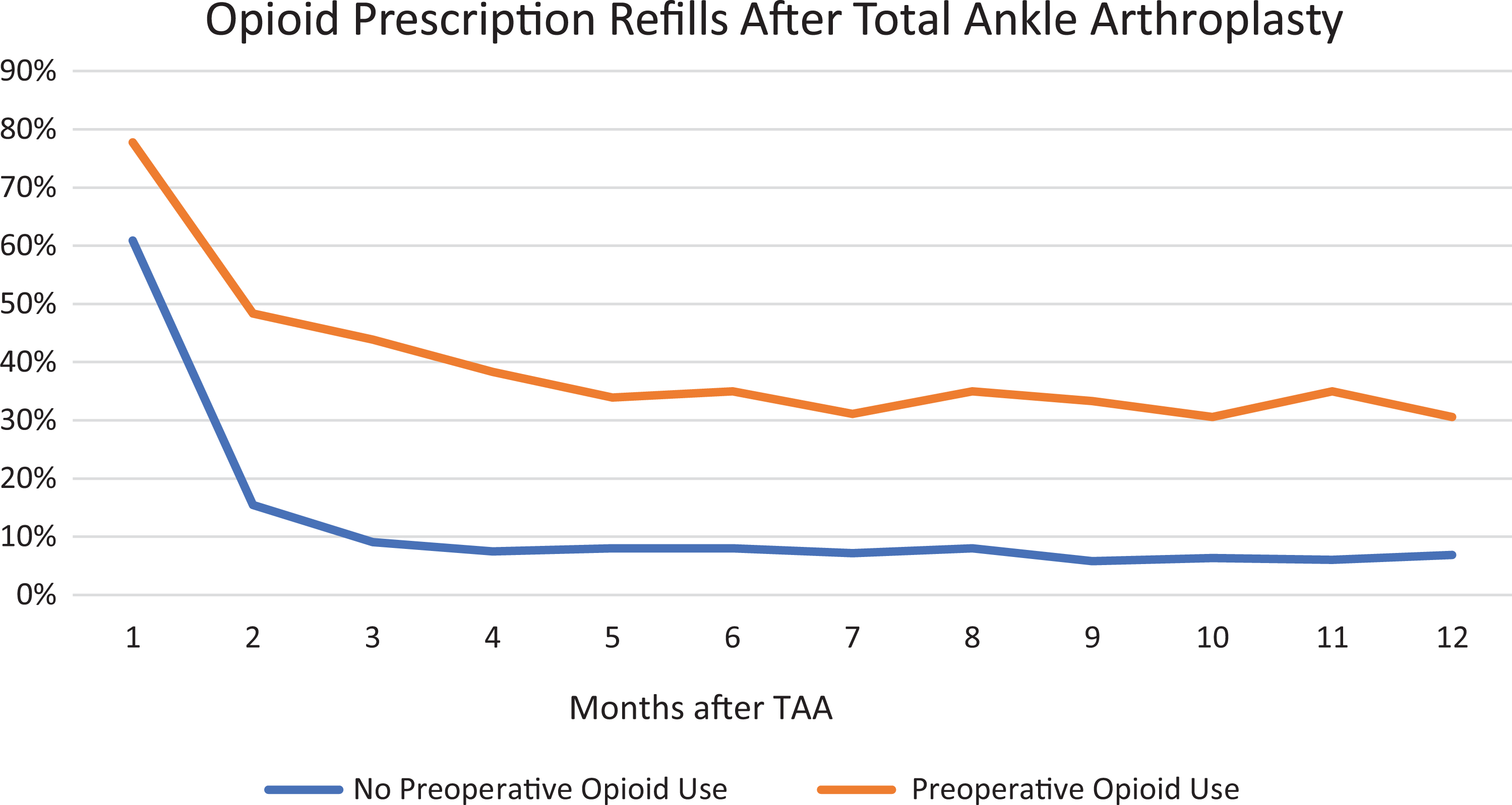
Percentage of patients with opioid prescription refills after total ankle arthroplasty.
Fibromyalgia, LBP, anxiety or depression, smoking, female sex, and preoperative tramadol use were also found to be associated with greater odds of postoperative opioid prescription fills. Those with LBP had significantly greater risk at postoperative months 2 through 12, with the highest risk occurring at 9 months (RR: 2.43, 95% CI: 1.61-3.66]). Fibromyalgia, anxiety or depression, and smoking were also associated with greater risk at months 2 through 12. RR at 12 months following TAA was 2.13 (95% CI: 1.40-3.25) for fibromyalgia, 2.17 (1.37-3.45) for anxiety or depression, and 1.75 (1.14-2.67) for smoking. Female sex was associated with greater risk at 2, 3, 4, 7, 8, and 9 months postoperatively. Preoperative use of tramadol had higher risk for opioid prescription fills at postoperative months 6, 10, and 12 following TAA. At 12 months following TAA, 27.0% of those taking tramadol preoperatively filled an opioid prescription compared with 13.1% of those who did not fill a prescription for tramadol in the 3 months prior to TAA.
In the multivariate analysis, those with preoperative opioid use were again found to have significantly higher odds for filling an opioid prescription at 3 months (OR: 5.06 [95% CI: 2.91-8.93], P < .001), 6 months (OR: 5.03 [2.69-9.50], P < .001), and 12 months (OR: 9.20 [4.89-17.4], P < .001) following TAA (Table 2). At 3 months, female sex (OR: 2.72 [1.68-4.50], P < .001) and smoking (OR: 1.95 [1.24-3.05], P = .004) were also found to be significant. Female sex (OR: 2.99 [1.78-5.16], P < .001), smoking (OR: 1.77 [1.06-2.93], P = .027), and preoperative tramadol use (OR: 1.87 [1.03-3.25], P = .031) were found to have significantly higher odds for opioid prescription fills at 6 months postoperatively. At 12 months, there were significantly greater odds for opioid prescription fills with a concurrent diagnosis of LBP (OR: 2.22 [1.21-4.20], P = .012). In the multivariate analysis, no significant difference could be detected with the diagnoses of fibromyalgia and depression or anxiety at any of the time points.
Multivariate Analysis for Postoperative Opioid Use Following Total Ankle Arthroplasty.

Abbreviations: CI, confidence interval; OR, odds ratio; TAA, total ankle arthroplasty.
a Variable did not meet inclusion criteria (P < .1) for inclusion in multivariate model.
Discussion
This study found that opioid use within the 3 months prior to TAA was most strongly associated with prolonged postoperative opioid use, increasing the risk of continued opioid prescription filling at 12 months postoperatively over 4 times. In the univariate analysis, fibromyalgia, depression or anxiety, smoking, and LBP were consistently associated with greater risk for postoperative opioid use. Female sex and preoperative tramadol use were also associated with increased postoperative use during several of the postoperative months.
Several studies have previously investigated the association between pre- and postoperative opioid use following other orthopedic procedures. 3,5,19 The current study found a rate of 33.1% in TAA patients. This is similar to previously reported values seen in total knee arthroplasty, anterior cruciate ligament reconstruction, and rotator cuff repair, which ranged from 31% to 43%. 3,5,19 In an orthopedic trauma population, Holman et al 7 found approximately 15.5% of patients had filled an opioid prescription within 3 months prior to injury, and these patients were 6 times as likely to continue opioid use beyond 12 weeks postoperatively. Previous studies have also shown LBP to be a risk factor for prolonged opioid use postoperatively, consistent with the current study. 4,15,19 Although female gender has been suggested in other studies to be a risk factor for prolonged opioid use, no consistent difference based on gender was found in the current study. 5,16 Recently, a study found increased rates of adverse events, such as wound complications, emergency department visits, and revision surgery, to be associated with preoperative opioid use. 8 However, opioid cessation may mitigate this risk, further emphasizing the need for greater understanding of factors associated with chronic opioid utilization. 8
Although several studies have examined opioid usage following foot and ankle procedures, there is a paucity of data on risk factors for prolonged opioid usage following TAA. A recent prospective cohort study by Saini et al 17 identified 4 independent factors associated with increased opioid consumption following outpatient foot and ankle procedures: regional block anesthesia, age <60 years, preoperative visual analog scale score >6, hindfoot procedures, and bony procedures. In the same study, there was a trend toward patients who self-reported anxiety consuming greater opioids; however, it did not achieve statistical significance. 17 Merrill et al 12 reported that patients undergoing ankle/hindfoot procedures consumed a significantly higher number of long-acting opioids, such as MS Contin or Oxycontin (Purdue Pharma), when compared to forefoot procedures. They found no difference in bony vs soft tissue procedures or in use of short-acting opioids. However, the study was limited in that patients were only followed until the first postoperative visit and those taking opioids preoperatively were excluded. As demonstrated by this study and other studies assessing the impact of preoperative opioid use on postoperative opioid use, those taking prescription opioids preoperatively are at significant risk for prolonged use following an operation. Other studies have found preoperative opioid use to be associated with greater hospital length of stay, poorer patient-reported outcomes, and even higher rates of reoperation. 9,20 Given the high rate of preoperative opioid use found in this study and association with prolonged postoperative opioid usage, there could be a benefit in identifying these patients preoperatively and coordinating services to help these patients wean from opioid medications. However, additional studies are needed to assess whether cessation of opioids in the preoperative opioid decreases the risk for ongoing postoperative use or opioid-related adverse drug events. The high rate of both pre- and postoperative opioid use should encourage surgeons to limit both the individual prescribing during these time periods, and also encourage other providers prescribing opioids to do the same when assessing patients with a condition treated reliably with an operative procedure.
This study is not without limitations. This is a retrospective study and, similar to other studies involving large insurance claims databases, the data reported are dependent on accurate claims data and coding. Similarly, only opioid medications processed through the insurer prior to dispensing would be captured by the query; however, this is thought to represent only a small quantity as the majority of prescription drugs are processed through insurance at ambulatory pharmacies. Additionally, the data set does not contain information regarding the exact quantity of opioid medication dispensed. Additionally, this study uses opioid prescription claims data as a surrogate for opioid consumption and we are unable to ascertain whether patients were taking the medications as prescribed, or at all. Tramadol was separated from other opiate medication, as it does carry a recommendation from the AAOS for treatment of symptomatic knee osteoarthritis and has additional pharmacologic properties compared with traditional opiate medications. 2 Although prescriptions for chronic and largely silent conditions, such as hypertension, may go unfilled and have been associated with concerns about medication compliance, opioids are prescribed in an attempt to alleviate pain and it is reasonable to assume patients are taking the prescribed medication to treat their symptoms. Additionally, it may be the practice of some surgeons to provide a prescription prior to surgery intended for postoperative use. If this occurred and the prescription was filled prior to TAA, it is possible some patients not taking opioids preoperatively were mistakenly classified as taking opioids. However, including patients not taking opioids preoperatively with those who were would likely underestimate the risks for ongoing postoperative opioid use.
Conclusion
The present study found that preoperative opioid use in those undergoing TAA was common, with more than 30% of patients found to have filled a prescription for an opiate in the 3 months prior to surgery. Preoperative opioid use was strongly associated with prolonged postoperative opioid use following TAA, even after controlling for other known risk factors in a multivariate model. In addition to preoperative opioid use, LBP, female sex, smoking, and preoperative tramadol use were found to be associated with higher risk of postoperative opioid use. Given the relatively high rate of preoperative opioid utilization and prolonged postoperative opioid use in this population, surgeons should routinely screen for preoperative opioid use, and future studies should investigate the role of preoperative opioid cessation programs in the perioperative period.
Supplemental Material
Supplemental Material, FAO897911-ICMJE - Association of Preoperative Opioid Use and Prolonged Postoperative Opioid Use Following Total Ankle Arthroplasty
Supplemental Material, FAO897911-ICMJE for Association of Preoperative Opioid Use and Prolonged Postoperative Opioid Use Following Total Ankle Arthroplasty by David E. DeMik, Chris C. Cychosz, Nicholas A. Bedard, Cameron Barton, Qiang An and Kyle R. Duchman in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.