
Abstract
The role of arthroscopy in the management of ankle and hindfoot pathology management has increased greatly in recent years with the potential for lower complication rates, faster recovery, improved access, and improved outcomes when compared to open techniques. Procedural variations exist as techniques aim to optimize lesion access, decrease operative time, and improve patient safety. Our goal is to summarize the described approaches and patient positionings common in minimally invasive arthroscopic surgery for anterior, lateral, and posterior ankle pathologies. A survey of pathology organized by arthroscopic approach and a review of recent advances in concomitant lesion management may be useful when planning arthroscopic foot and ankle surgery.
Level of Evidence:
Level V, expert opinion.
Introduction
As arthroscopic technologies and techniques evolve, the procedure is becoming increasingly recognized as an effective means of treating ankle and hindfoot pathologies. Many minimally invasive techniques have been described, 14,19,29,37 with an array of available patient positionings, portal placements, and operative approaches. Optimizing these choices is necessary for effective operative management, but decisions are complicated by overlapping terms, patient-specific anatomical variations, and a variety of surgeon preferences. This article aims to provide a functional tool for arthroscopists by describing common foot and ankle maladies from the perspective of operative approaches and patient positioning (Figure 1). Understanding the accepted techniques for access may aid planning operative teams in aligning setup with the specifics of the pathology and in concomitant lesion management.
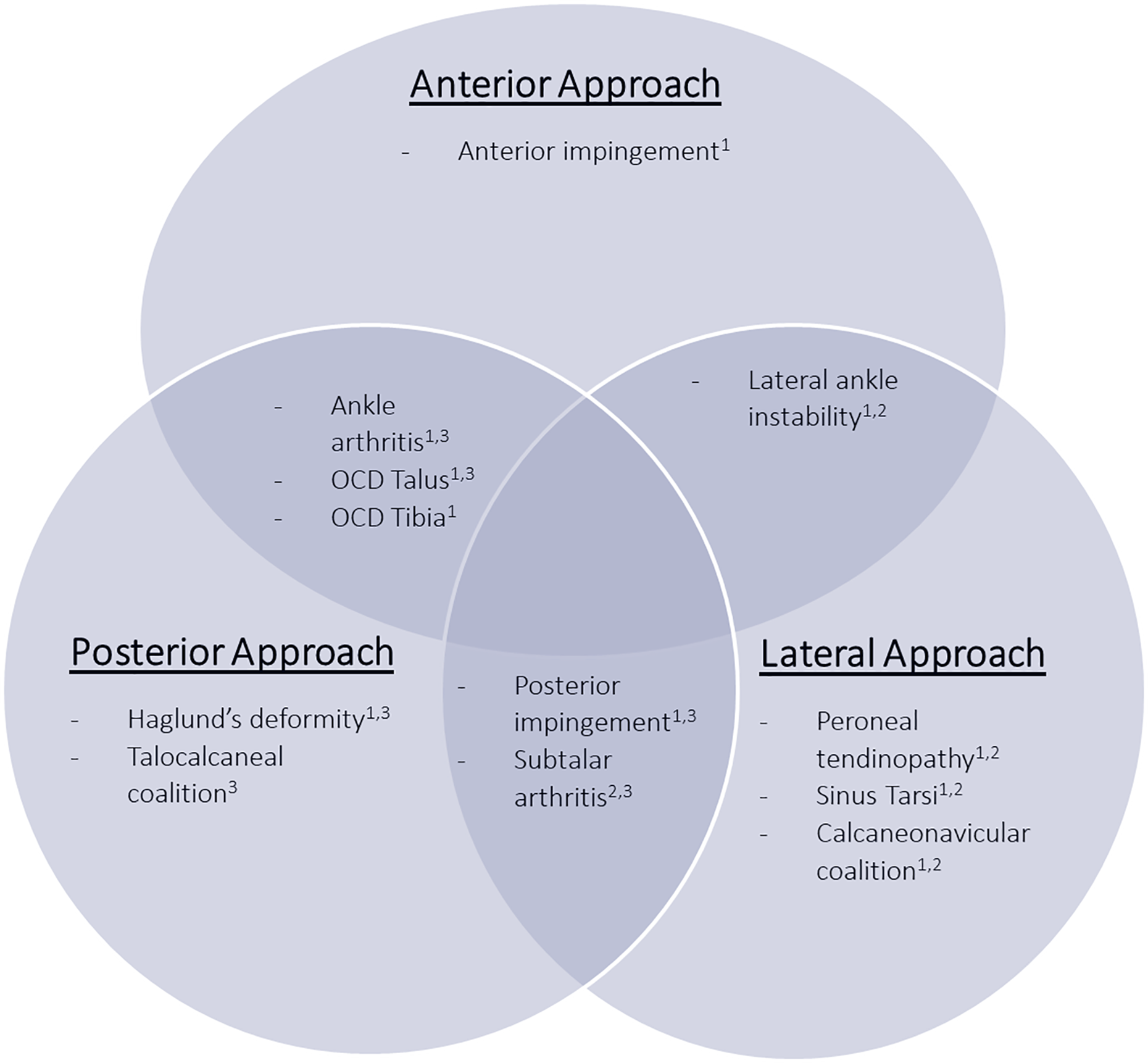
Common ankle pathologies grouped by arthroscopic approach. Superscript indicates acceptable patient positionings: 1, supine; 2, lateral decubitus; 3, prone. OCD, osteochondral defect.
Across all arthroscopic approaches described, there are a number of shared technical pearls: Distend and infiltrate the joint with either saline or an anesthetic mixed with epinephrine. The mix with epinephrine may be helpful to the less experienced surgeon to minimize iatrogenic damage. Utilize the nick and spread technique when establishing portals to avoid neurovascular injury. Incisions are made to the level of the dermis, followed by subcutaneous blunt dissection with a mosquito clamp to open the portal and establish the working space. Establish the portal with less risk of neurovascular injury first, and then create secondary portals under direct needle localization. Utilize a fluid pump and alternate portals to optimize visualization and access. Adjust instrumentation based on the extent of the pathologies noted. A 4.0-mm scope provides a larger field of view and greater flow than a 2.7-mm scope. As an example, because of the variability in pathology extent and the difficulty of accessing smaller lesions, the shaver size may be as small as 2.0 mm. Having a wide range of shavers and burrs is often helpful to adjust intraoperatively. Maintain the appropriate degree of suction. Insufficient suction may not allow for sufficient flow and cleansing of the tissues to maintain visualization, while excessive suction may result in closure of the field of view.
Approaches
Anterior Approach
Non-invasive distraction is usually recommended for evaluating the intra-articular space (Figure 2A, B). 10 In the anterior approach, the standard anteromedial portal is established first, at the level of the joint line immediately medial to the tibialis anterior tendon with care taken to avoid the saphenous nerve and greater saphenous vein (Figure 2C). Under needle localization, the anterolateral portal is created immediately lateral to the peroneus tertius tendon at the joint line. The superficial peroneal nerve must be avoided, and can often be visualized in a position of plantarflexion and inversion. When entering the joint, it is important to pass the arthroscope across the anterior aspect of the joint and not into the cartilage of the talus.

Supine patient positioning and portal designation. (A) Supine position with the affected ankle (arrow) elevated and hip bumped. (B) Waist distraction is used to improve access to the joint. (C) Anterior approach portals. TA, tibialis anterior; AL, anterolateral portal; AM, anteromedial portal; SPN, superficial peroneal nerve. (Image courtesy of Dr Kirk A. McCullough.) (D) A posterior thigh pad elevates the knee, creating a counter for the distractor.
Posterior Approach
Two options exist to optimize the working angles and may be done in combination or individually. The operative hip may be extended slightly compared to the contralateral limb to provide clearance for instrumentation. Care is taken to avoid prolonged extension of the hip, given that it has been associated with femoral nerve palsies. The operative hip is maintained in neutral flexion/extension and the knee is placed in slight flexion. The operating table may be adjusted in reverse Trendelenburg.
The standard 2-portal posterior approach for hindfoot pathologies was originally described and popularized by van Dijk. 35 The lateral malleolus (LM), medial malleolus (MM), and Achilles tendon should be established as anatomic landmarks prior to incision. Posteromedial and posterolateral portals are located just anterior to the borders of the Achilles and level with the line connecting the inferior poles of MM and the tip of LM (Figure 3). Care should be taken to avoid iatrogenic injury to the sural nerve laterally, and the neurovascular bundle medially. A 4.0-mm camera is most common alongside 3.5-4.5-mm shavers for soft tissue and 4.0-5.0-mm burrs for osseous resection. Generally, the direction of the dissection should be toward the first interdigital web space, and the posterior talar process can be felt as a landmark between the ankle and subtalar joints. 25

(A) Prone patient positioning and portal designation. (B, C) Prone positioning with the operative extremity bumped above the level of the contralateral limb. (1) Standard posterolateral and (2) posteromedial portals with instruments. AT, Achilles tendon.
Lateral Approach
The patient is placed in the lateral decubitus position with the operative side up, and the foot positioned off of the table edge to allow for gravity-assisted foot inversion and subtalar joint opening. An anterolateral portal is created 1 cm distal and 3 cm anterior to the distal fibular tip, and a middle portal just anterior to the tip of the fibula (Figure 4). Some initial shaving may be necessary to enable arthroscopic examination and to aid in the establishment of the posterolateral portal, located just anterior to the Achilles and level with the intermalleolar line.

Lateral decubitus positioning. The operative foot rests off the table to allow for gravity-assisted subtalar inversion. (1) Anterolateral portal used in anterior approach; (2) anterolateral portal used in lateral approach; (3) middle portal for lateral approach.
Alternatively, and as described by Marumoto and Ferkel, 19 the patient may be placed supine with the hip flexed at 45 degrees using a padded thigh support (Figure 2D). Standard anterolateral and posterolateral portals are used with the incorporation of accessory portals as needed. Distension is performed through the posterolateral portal, followed by establishing the anterolateral (viewing) portal for the 2.7-mm 30-degree arthroscope. Maneuvering the arthroscope to the lateral gutter allows the posterolateral (working) portal to be created under direct visualization. Care should be taken to avoid injury to the flexor hallucis longus (FHL) tendon, posterior tibial neurovascular bundle, and posterior talofibular ligament. 19
Pathologies
Anterior Pathologies
Anterior Impingement
Anterior impingement describes a syndrome of pain along the anterior aspect of the ankle joint from abnormally abutting structures. Patients often present with swelling, restricted range of motion, and exacerbation of pain with dorsiflexion. Anterior impingements are distinguished by whether involved structures are osseous and/or soft tissue and by medial-lateral localization within the ankle joint. Bony impingement generally occurs anteromedially, while soft tissue impingement is most commonly observed anterolaterally. 41 Waist distraction may be helpful in the setting of impingement, allowing for variable distraction and therefore a larger working space when distraction is released. Alternating traction is recommended so that the articular surfaces can be addressed while under distraction, and the extra-articular but intra-capsular impingement can be accessed more easily without traction, especially in a position of dorsiflexion.
Anterior approach, supine position
Excision of osseous spurs both on the talus and tibia requires a 3.5-5.0-mm burr, with resection carried out to restore normal anatomic dimensions (Figure 5A). Dynamic impingement testing and fluoroscopic imaging aid in assessing the extent of resection. 22 Impinging lesions potentially encountered and debrided with 3.5-4-mm shavers include synovitis, meniscoid lesions, an accessory distal fascicle of the anterior inferior tibiofibular ligament known as Bassett ligament, synovial shelves, or fibrous adhesions (Figure 5B,C). 5
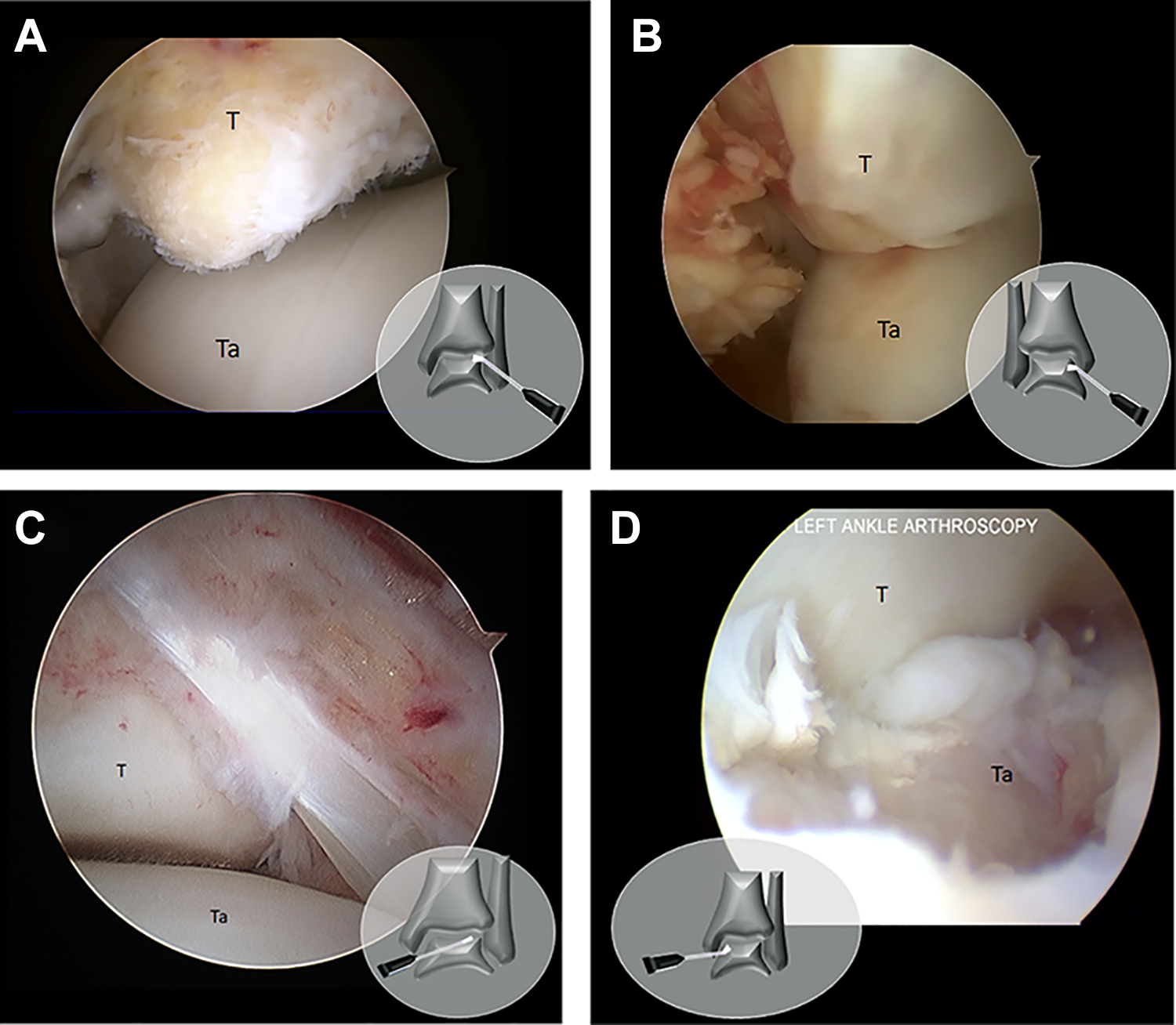
Arthroscopic visualization from anterior approach. (A) Anterior tibial spur in left ankle viewed from the anterolateral portal. (B) Synovial impingement in right ankle viewed from the anteromedial portal. (C) Bassett ligament impingement in left ankle viewed from the anteromedial portal. (D) Centromedial talar osteochondral defect in left ankle viewed from the anteromedial portal. T, tibia; Ta, talus.
Osteochondral defects of the talus
Osteochondral defects (OCDs) of the talus frequently accompany acute trauma, present in 50% ankle sprains and 73% of ankle fractures. 30 All-arthroscopic techniques include shaving, microfracture, drilling, particulated/micronized cartilage procedures, and osteochondral autologous transplantation (OAT). Biological adjuvants may also be considered.
Anterior approach, supine position
Most talar lesions can be accessed from the anterior approach with 30 degrees of plantarflexion to improve talar access (Figure 5D). 23 A 30-degree arthroscope is typical, and noninvasive metal and waist distraction may be applied to increase visualization of the articular surfaces and minimize micromotion.
Posterior approach, supine or prone position
It has been previously suggested that 55% of lesions on the posterior third of the talus are inaccessible from the anterior approach, though this remains a point of controversy. 23 Posteromedial lesions in particular are difficult to access from supine positioning, often requiring a posteromedial portal and prone positioning. Alternatively, a coaxial approach has been described with portals parallel to the bimalleolar axis and immediately anterior to medial and lateral neurovascular structures, which may improve access to the posterior joint. 1 However, in cases where both anterior and posterior lesions are present, intraoperative positioning switches are a significant inconvenience. While the option for a standard 2-portal hindfoot approach remains accepted, 34 a standard posterolateral portal with the patient in a supine position allows for access to nearly all lesions encountered. 10
Osteochondral defects of the distal tibia
While rare in prevalence and poorly described in the literature relative to talar counterparts, OCDs of the tibia may be present in 15.8% to 20.5% of patients with talar OCDs. 40 Both all-arthroscopic and arthroscopic-assisted treatments of the distal tibia have been described, analogous to those described for talar OCDs.
Anterior approach, supine position
Tibial OCDs are visualized with 30-degree or 70-degree arthroscopes. Standard anterolateral and anteromedial portals are usually sufficient if the lesion is anterior, with the addition of a posterolateral portal for posterior defects. 8,20 Noninvasive distraction is preferred.
Posterior approach, supine position
The coaxial approach described above for talar OCDs may also be employed for distal tibial OCDs, and also may supplement an anterior approach.
Ankle arthritis
Anterior approach, supine position
The patient is placed in the supine position and a posterior thigh holder is utilized for countertraction (Figure 2C). Standard anteromedial and anterolateral portals are established, and an accessory portal for outflow can be considered either with a standard posterolateral portal or a retromalleolar tendoscopic portal located 1 cm posterior to the tip of the lateral malleolus. 11,24,31 Debridement of the articular cartilage of the tibial plafond, the talar dome, the medial gutter, and the lateral gutter is completed. A motorized burr is then used to promote a vascular response from the subchondral bone. Fluoroscopic guidance and burring are used to eliminate gaps between the bone surfaces and to adjust alignment, preferentially along the tibial side to maximize talar bone stock. The ankle joint then is fixated with large cannulated compression screws.
Posterior approach, prone position
Some suggest that posterior arthroscopic ankle arthrodesis offers improved fusion rates, but further studies are required before definitive conclusions can be drawn. 21 Still, a posterior approach and prone positioning may be especially helpful when combining with subtalar arthrodesis with standard posteromedial and posterolateral portals used.
Posterior Pathologies
Subtalar arthritis
Posterior approach, prone position
Arthrodesis may be performed to address subtalar arthritis. In this procedure, the cartilage of the subtalar joint facet is removed using curettes. An option to increase the working space is to place an accessory portal through the sinus tarsi and to introduce a 4.0-mm blunt trocar to open the subtalar joint (Figure 6A). Portals are switched to ensure full visualization and bone preparation. The bone is prepared using curettes, osteotomes, shavers, and burrs to spot weld and disrupt the surfaces. Two divergent cannulated lag screws are introduced across the posterior subtalar joint for fixation. Coaptation of posterior subtalar joint surfaces may be checked arthroscopically as the screws are tightened. 7

Arthroscopic visualization from posterior approach. (A) Subtalar arthrodesis of right ankle. View from posteromedial portal with cannula in the accessory anterolateral portal and burr in the posterolateral portal. (B-D) Stieda process in left ankle viewed from the posterolateral portal and resected through the posteromedial portal. (B) Establishing working space with a blunt trocar and shaver. Stieda process (C) pre- and (D) postresection. T, tibia; Ta, talus; C, calcaneus.
Lateral approach, lateral decubitus position
The patient is placed in the lateral decubitus position with the operative side up (Figure 4). The foot is positioned off of the table edge to allow gravity-assisted foot inversion and subtalar joint lateral opening. An anterolateral portal should be established 1.5 cm anterior and 1 cm distal to the tip of the lateral malleolus, at the posterior margin of the sinus tarsi. An accessory anterolateral portal is initiated 1 cm posterior to the anterolateral portal. Some initial shaving may be necessary to enable arthroscopic examination and to aid in the establishment of the posterolateral portal, which is located 1 cm posterior and 1 cm proximal to the tip of the lateral malleolus. Fixation is achieved using a 7-mm cannulated screw with a C-guide to aid in localization. A small incision is made over the neck of the talus, followed by dilation until the bone surface is exposed. One end of the C-guide is placed directly over the bone, while the other end is placed in the middle of the heel. The position is checked with fluoroscopy and a guidewire introduced. The subtalar joint is fused in slight valgus and the ankle in maximum dorsiflexion to avoid the possibility of screw head impingement with the distal tibia. 9
Posterior impingement
Posterior ankle impingement syndrome describes an array of clinical disorders that manifest as ankle and hindfoot pain posteriorly during plantarflexion. Flexor hallucis longus (FHL) tenosynovitis and osseous defects of the posterior talar process are frequently observed. The os trigonum is an inconsistent accessory bone of the talus with a prevalence of 1.7% to 7.7%, 19 which may become symptomatic with repetitive extremes of plantarflexion. Impingement may also be caused by an elongated lateral tubercle, or Stieda process, which causes impingement between the tibia and calcaneus in plantarflexion. 39 Both FHL tenosynovitis and posterior talar process abnormalities may be accessed with either the Marumoto and Ferkel 19 lateral approach or van Dijk et al 35 posterior approach, depending on preference.
FHL tenosynovitis
Posterior approach, prone position (preferred)
Tenosynovitis is commonly observed around the flexor hallucis longus (FHL) tendon proximal to the fibro-osseous tunnel. With the patient in a prone position, a 4.0-mm 30-degree arthroscope is introduced into the standard posterolateral portal with the posteromedial portal established under direct visualization. Flexion of the great toe allows the surgeon to visualize and address soft tissue impingement, stenosis, tearing, and tenosynovitis. Debridement and resection of impinging bone is also performed if indicated. 38
Lateral approach, supine position
Although originally described in the context of posterior talar process abnormalities, the Marumoto and Ferkel 19 lateral approach may additionally be used to address FHL tenosynovitis.
Stieda process or os trigonum
Posterior approach, prone position
Impingement may be visualized during surgery by manually inducing dorsiflexion. The surgeon may proceed with debridement of the fat and scar tissue found in the posterolateral subtalar joint. As a safety landmark, the FHL may be identified superomedially before it enters the fibro-osseous tunnel (Figure 6B). The ligamentous attachments of the posterior talar process, notably the posterior talofibular ligament, FHL retinaculum, and posterior talocalcaneal ligaments, are removed. After the os trigonum or Stieda process is cleared of soft tissue, it may be excised with a grasper or resected completely with a hooded high-speed burr angled away from the FHL and neurovascular bundle (Figure 6C-D). 36 The ankle should be assessed for full range of motion to ensure absence of impingement.
Lateral approach, supine position
While not routinely adopted by the senior author, some prefer the Marumoto and Ferkel 19 lateral approach. This may be especially useful in cases where a high body mass index precludes prone positioning.
Talocalcaneal coalition
Talocalcaneal coalitions are the second most common type of hindfoot coalitions (37%), and can be addressed arthroscopically through arthrodesis or resection. 32 Based on current limited outcome studies, resection is considered in patients with less than 50% involvement of the joint who do not present with arthritic changes of the subtalar joint. 4
Posterior approach, prone position
A 4.0-mm 30-degree arthroscope is used with standard posteromedial and posterolateral portals. The FHL retinaculum is released and FHL tendon mobilized to visualize the posterior aspect of the subtalar joint. 4,15 FHL retraction opens the working space and protects the medial neurovascular bundle, incorporating a nylon tab over the tendon and resting the arthroscope over it. With the shaver directed laterally, a cartilage lip is created by shaving the subarticular bone 2 mm beyond the articular cartilage margin, followed by radiofrequency blade over the subarticular bone to prevent recurrence. 4 Alternatively, a 4.0-6.0-mm chisel or osteotome may be introduced, and an attempt made to remove the bar connecting the talus and calcaneus.
Haglund disease
Haglund disease causes pain and tenderness posteriorly secondary to a calcaneal prominence. This pathology may be addressed through endoscopic resection of the calcaneus and removal of inflamed retrocalcaneal bursa. Consideration should be given to further treatment of the Achilles, including debridement and possible repair. Most cases of Achilles insertional tendinopathy are better treated with open resection, but this depends on the extent of Achilles involvement.
Posterior approach, prone position
If the prone position is used, the feet are placed just over the edge of the operating table (Figure 3A). A 4-mm 30-degree arthroscope may be used. The lateral portal is made with standard technique at the level of the superior aspect of the calcaneus, and the arthroscope is introduced. A spinal needle is then placed just medial to the Achilles, also at the level of the superior aspect of the calcaneus. A 4-mm resector is then introduced, visualized through the arthroscope. First, the inflamed retrocalcaneal bursa is removed to improve visualization. Once the superior surface of the calcaneus is visualized, the resector may be used to remove the fibrous layer and the periosteum. A 4.0-mm hooded burr resects the Haglund deformity and any other prominence posteriorly at the Achilles insertion. Full dorsiflexion of the foot aids in addressing the impingement site before transitioning to full plantarflexion to remove the posterosuperior bone rim. Palpation from the outside of the skin may assist in identifying additional bony prominences that may bring discomfort with shoe wear. 4
Posterior approach, supine position
If supine positioning is preferred, a posterior thigh pad may be used along with a narrow bump to support the heel to allow for free movement of the camera and instrumentation from both sides of Achilles (Figure 2A).
Lateral Pathologies
Calcaneonavicular coalition
The calcaneonavicular coalition makes up 53% of all hindfoot coalitions and may be treated through arthroscopic resection. 6
Lateral approach, lateral decubitus (preferred), or supine position
After an attempt to identify and avoid the superficial peroneal nerve, a visualization portal is established dorsal to the angle of Gissane, formed by the intersection of the downward- and upward-sloping surfaces of the superior calcaneus. A 4.0-mm arthroscope is introduced, and the working portal established on the distal medial synostosis at the junction of the navicular bone, dorsal and medial to the superficial peroneal nerve. A shaver is used to debride soft tissue laterally to the anterior process of the calcaneus and the calcaneocuboid joint and medially to the talonavicular joint. The calcaneonavicular synostosis is now resected using a 4.0-mm burr, until the lateral side of the talonavicular joint may be visualized fully. Inversion and eversion mobilization may be used to confirm mobility between the navicular bone and the calcaneus and to test for impingement. 6 For the other rare coalitions such as calcaneocuboid and naviculocuneiform, the portal positioning can be identified with fluoroscopic guidance and with care to avoid crowding of the portals.
Lateral ankle instability
Anterior approach, supine position
While traditionally addressed with an open procedure, arthroscopic techniques for chronic ankle instability have recently been described. Minimally invasive lateral ligament repair and reconstruction can be performed from an anterior approach with the patient in the supine position. 28,33 A noninvasive distraction device may be used with standard anteromedial and anterolateral portals, especially if concomitant cartilage lesions are present. Additional portals are frequently required in cases of lateral ligament reconstruction, but care must always be taken to stay within the “safe zone” in the lateral region bordered by the distal fibula, the superior margin of the peroneal tendons, and the intermediate branch of the superficial peroneal nerve.
Lateral approach, lateral decubitus position
If ankle instability is to be addressed arthroscopically followed by an open lateral ankle surgery, a modified approach may be taken to avoid time spent in repeated prep and drape. The patient is placed in a lateral decubitus position on the operating table using a beanbag. The nonoperative limb is padded and flanked with arm board pads. A sheet is placed over the nonoperative limb and padding to create a working surface on which to rest the operative extremity. The hip of the operative leg is flexed 45 to 50 degrees and abducted, rotating externally until the foot is in the supine position with the knee flexed at 90 degrees. 14 The posterior thigh is now supported with a well leg holder and noninvasive distraction applied to perform standard anterior ankle arthroscopy. Removal of the well leg holder and restoration of the leg to the lateral position allows subsequent lateral open surgery. A similar transition between the anterior and lateral approaches has been recently described in the context of lateral ligament reconstruction, where gracilis tendon autograft harvesting was carried out in an anterior approach followed by rotation of the operative leg to access the lateral ligament complex from a lateral approach. 13
Sinus tarsi syndrome
Sinus tarsi syndrome presents with sinus tarsi tenderness and hindfoot instability. Theories of origin range from scarring, interosseous talocalcaneal ligament tearing, and synovitis; however, an exact etiology has not yet been uncovered. 3,17
Lateral approach, lateral decubitus (preferred), or supine position
Both lateral decubitus 7 and supine positioning 17 may be employed from a lateral approach, with lateral decubitus preferred by the senior author. The lateral approach anterolateral portals and middle portals are used (Figure 4). A posterolateral portal typical of the 2-portal hindfoot approach is rarely necessary, but remains an option for concomitant posterior pathology.
The anterolateral and middle portals can be alternated between visualization and instrumentation. Following initial synovectomy and debridement, the interosseous talocalcaneal ligament and calcaneofibular ligament should be examined for pathology (Figure 7A). The lateral gutter may be visualized through the anterolateral portal, and any abnormal or impinging tissues may be debrided. The superior portion of the sinus tarsi is then debrided before conducting dynamic impingement testing under arthroscopic visualization. 16

Arthroscopic visualization from lateral approach. (A) View from the middle portal of a frayed interosseous ligament in a right ankle sinus tarsi. Debridement of the ligament with a shaver in the anterolateral portal. (B-D) Visualization of peroneal tendinopathy from the distal portal looking proximal. (Obtained with permission from Marmotti et al. 18 ) (B) Normal and (C) tenosynovitis observed in peroneal tendons. (D) Tear in the peroneus brevis. Ta, talus; C, calcaneus.
Peroneal tendinopathy
Lateral approach, lateral decubitus (preferred), or supine position
Both supine 27 and lateral decubitus 26 positioning provide access to the peroneal sheath with the potential to address concomitant anterior lesions. A 2.7-mm 30-degree scope is typical, as it is difficult to introduce instrumentation larger than 2.9 mm into the peroneal sheath. The first portal is established 1.5 to 2 cm distal to the posterior edge of fibular apex. After distension, a longitudinal incision along the lateral aspect of the sheath grants tendon visualization and retraction with a Kelly clamp. Introduction of the arthroscope into the tendon sheath is facilitated by plantarflexion (Figure 7B-D). A second portal is then established 2-2.5 cm proximal to the posterior edge of the lateral malleolus under direct arthroscopic visualization. Additional accessory portals proximal to the fibular tip (6 cm maximum) may be used as dictated by the pathology. A shaver and radiofrequency blade debride impinging soft tissue structures, whereas a burr is used for any bony prominences. 18
Conclusion
The variety of patient positioning and approaches brings both choice and challenge to foot and ankle operative preparation. In all cases of operative planning, safe access is a primary goal. 13,15 Successful management of a single pathology can often be achieved with multiple positionings or approaches, but means of concomitant lesion management without repositioning and redraping are still being explored. 13,29 A potential reduction in operative duration without sacrificing access is highly desirable, given the well-established association between operation time and arthroscopic complications. 2,12 A summary of options available to the foot and ankle arthroscopist (Table 1) may provide greater flexibility in operative planning and introduce recent innovations in accessing common foot and ankle pathologies.
Common Ankle Pathologies With Respective Approaches/Positionings.

Supplemental Material
Supplemental Material, FAO894968-ICMJE - Operative Approaches to Ankle and Hindfoot Arthroscopy
Supplemental Material, FAO894968-ICMJE for Operative Approaches to Ankle and Hindfoot Arthroscopy by Dominic S. Carreira, Steven R. Garden and Thomas Ueland in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.