
Abstract
Background:
Ankle fractures are among the most common injuries encountered by orthopedic surgeons, with an incidence ranging from 71 to 187 per 100 000 people. Few studies have reliably investigated injuries involving isolated fractures of the distal fibula below the level of the ankle syndesmosis. Therefore, this study details on the patient-reported outcomes of nonoperatively managed isolated infrasyndesmotic fibula (ISF) fractures with a minimum 3-year follow-up.
Methods:
A retrospective population-based cohort study was undertaken across all emergency departments serving a major urban population. Among 159 consecutive patients meeting inclusion criteria, 108 agreed to participate. Clinical information, functional outcomes, and radiographic measurements were collected from electronic medical records and 3 validated outcome measures: the American Academy of Orthopaedic Surgeons (AAOS) Foot & Ankle Scale (FAS), the AAOS Shoe-Comfort Scale (SCS), and a general questionnaire.
Results:
An incidence of 22 ISF fractures per 100 000 people/year was found with FAS (91.2 ± 12.9) and SCS scores (76.8 ± 27.7), similar to reported population norms. Approximately 40% of patients (n = 43) reported continuing symptoms including pain (81.8%), stiffness (68.1%), and/or instability (39.0%). Less than 13% (n = 14) reported “severe” disabilities, and no patients required operative intervention within the follow-up period. Less-favorable outcomes were reported among work-related injuries, female patients, and “avulsion-type” fractures less than 10 mm in height (P < .01). No relationships were identified between age, degree of articular-incongruity, fracture-displacement, and self-reported outcomes.
Conclusions:
The majority of patients with nonoperatively managed ISF fractures reported good-to-excellent early functional outcomes. Less-favorable outcomes were reported among work-related injuries, female patients, and “avulsion-type” fractures.
Level of Evidence:
Level III, comparative series.
Keywords
Introduction
Ankle fractures are among the most common injuries encountered by orthopedic surgeons, with an incidence ranging from 71 to 187 per 100 000 people. 11,17 The majority arise from low-energy twisting injuries, but the resulting disability can be substantial when considering that trauma is the leading cause of early-onset ankle arthritis and degeneration. 6,9 Few studies have focused on injuries involving isolated fractures of the distal fibula below the level of the ankle syndesmosis or tibial plafond. 26,28,33 These injuries are best described as isolated infrasyndesmotic fibula (ISF) fractures, and include both avulsion fractures from ankle sprains, as well as larger malleolar fractures from ankle adduction injuries. Similarly, these injuries are also often classified by one of the 3 most commonly used ankle fracture classification systems: supination adduction type 1 fractures (SAD-1) of the Lauge-Hansen classification, type 44.A1 (OTA-44.A1) of the Orthopaedic Trauma Association / Arbeitsgemeinschaft für Osteosynthesefragen classification, and unimalleolar type A fractures of the Danis-Weber classification system. Although this fracture pattern is relatively common, there is very limited high-quality evidence within the scientific literature supporting the various treatment methods.
In general, ISF fractures account for 12% to 21% of all ankle fractures and typically arise from adduction and inversion forces acting on a plantigrade or plantarflexed foot. 26,46 This can give rise to a spectrum of injuries, of which the 2 most commonly encountered patterns are ligamentous injuries of the anterior talofibular ligament (ATFL) and osseous fractures of the lateral malleolus. 20,27,51 Because of the absence of established criteria, ligamentous avulsion-type fractures (ATFs) are difficult to radiographically distinguish from larger malleolar-type fractures (MTFs). However, this distinction is clinically relevant when considering the number of stabilizing structures originating from the distal fibula; diastasis of a larger MTF fragment may compromise a greater number of ligamentous and capsular structures than a smaller ATF fragment from a single ligament. 2,20,22,51 In either case, the current management of ISF fractures is generally nonoperative, with satisfactory outcomes expected among most patients. 1,26,36,49,52
However, the current evidence regarding ISF fracture management and outcomes is quite limited, with multiple case reports highlighting less-favorable outcomes among certain patients. 22,26,32,36,46,55 To date, only 1 study has reported on the outcomes of fibular ligamentous avulsion fractures, 38 and no published studies have reported on isolated ISF fractures. Likewise, several case reports describing residual joint instability and symptomatic malunions suggests that satisfactory patient outcomes may be less common than previously thought. 23,26,28 Thus, several authors have argued for early operative intervention among cases with expected poorer outcomes (eg, athletes, fragments with signs of impingement, etc). 5,12,16,20,31,38 A recent systematic review performed by Stufkens et al 47 failed to identify any reliable studies investigating ISF injuries and concluded that Danis-Weber type A fractures “do not show any better long-term outcomes than Danis-Weber-B Type fractures.” Overall, these findings underscore the need for additional research to provide reliable prognostic and outcome information on these commonly encountered injuries.
Therefore, this study was undertaken to investigate the early functional outcomes of isolated ISF fractures. Secondary objectives were to collect clinical information related to these injuries and to identify if specific clinical and radiographic factors were associated with poorer outcomes. Considering the current evidence, we hypothesized that the majority of patients sustaining ISF fractures would experience good to excellent short-term outcomes. 18,22,26,36,46
Methods
Design
A retrospective population-based cohort study of isolated ISF fractures was performed in 2014 with ethics approval. Provincial licensing agreements required all health care facilities to upload diagnostic images onto a central picture archiving communication system (IMPAX; AGFA Healthcare, version 5.2) and this allowed for identification of patients within a specified health care zone. 41 Potential participants were screened by reviewing consecutive images acquired within a 1-year period across all 7 emergency departments of a metro urban health region serving a population of approximately 782 000 people. 7
Selection Criteria
Radiographic images demonstrating evidence of an isolated ISF fracture were marked for study inclusion. Infrasyndesmotic fibula fractures were defined as a fracture of the distal fibula that did not extend above the level of the tibial plafond on either coronal or sagittal radiographic views. Images were systematically, consecutively, and independently reviewed for inclusion by 2 authors (K.A., A.D.), with cases requiring arbitration referred to the study’s principal investigator (A.S.). Inclusion criteria were applied using the following search parameters: “Location of acquisition” set to all emergency departments (ED) serving a metropolitan health region, “Date of acquisition” set to the 2010 year-period, “Body part” set to ankle, and “Age” set to patients 18 years or older to exclude skeletally immature patients. Participants were excluded if they demonstrated or reported any of the following: a non-isolated ISF fracture, inadequate or incomplete plain radiographs at the time of injury (ie, anteroposterior, mortise, and lateral ankle views), any subsequent ankle fracture or ligamentous injury, any radiographic signs of a medial osteoligamentous injury, a radiographic report of an os subfibulare or a nonacute fracture, any prior surgery to the ipsilateral foot or ankle, radiographic signs of chronic ankle arthritis, or any history of inflammatory arthropathy excluding osteoarthritis. Injury to the medial or syndesmotic osteoligamentous complexes were considered positive when radiographs demonstrated greater than 4 mm of medial tibiotalar clear space widening on anteroposterior radiographs, greater than 3 mm of tibiotalar translation or asymmetry on lateral or anteroposterior (AP) imaging, or greater than 6 mm of syndesmotic tibiofibular space widening measured at 1 cm above the joint line. 39,40,42,43
Data Collection and Outcome Measures
Eligible participants were initially contacted by mail and subsequently by telephone to complete 2 self-administered validated outcome measures the American Academy of Orthopaedic Surgeons Foot & Ankle Outcomes Scale (FAS) questionnaire (version 2.0, Rosemont, IL), and the AAOS Shoe-Comfort Scale (SCS) questionnaire (version 2.0). 25 In addition, participants completed a general questionnaire to collect demographic and injury-specific questions, as well as several questions to help identify confounding factors; a history of ankle reinjury requiring medical attention, any operative intervention of the lower limbs, physical therapy treatment, work-related injuries, current employment status, and any history of nonosteoarthritic inflammatory joint conditions. 25,44 The FAS and SCS instruments are both validated surveys that provide standardized and normative scores that allow for comparisons to the general adult population. 25 For graphic illustrations only, Likert scale results were transformed into 4 symptom categories: none (1), mild (2), moderate (3), and severe (4 and 5).
Radiographic characteristics of the ISF fracture were organized under the Danis-Weber classification. 26 The fracture fragment’s height, width, and articular displacement were only measured on the mortise ankle view for optimal assessment of the fibular joint line and to standardize measurements. The “fracture-gap,” or vertical displacement of the fragment from the fibula, was not measured owing to previous reports demonstrating the poor reliability of plain radiography for measuring vertical displacement of fibula fractures. 19 Therefore, only displacement along the fibular articular surface or step-off was measured. Based on the published anatomic literature of the ATFL fibular footprint demonstrating an average height of 8.2 mm and width of 5.4 mm, we proposed a novel radiographic distinction method between smaller ligamentous “avulsion-type” fractures (ATF) and larger “malleolar-type” fractures (MTF); fragments equal or greater than 10 mm in height were considered MTFs and those 9 mm or less were classified as ATFs (Figure 1). 4,48,51 Articular incongruity or displacement equal to or greater than 3 mm on the mortise views were considered “significant” based on biomechanical studies reporting increased contact pressures and poorer outcomes with greater than 2 mm of articular displacement or step-off. 20,34

(A) Mortise-view ankle plain radiographs demonstrating a larger malleolar-type fracture with approximately 1.5 mm of articular incongruity, and (B) an avulsion-type fracture with no displacement.
Analysis
Descriptive statistics were performed for study variables. Comparisons between groups were performed using independent sample t tests and logistic regression analysis. Pearson correlational analyses were performed to estimate the degree of linear association between interval independent variables and interval functional outcomes. Depending on the correlation coefficient, linear associations were categorized as no or little relation (0 to 0.25 [or –0.25]), fair (0.25 to 0.49 [or –0.25 to –0.49]), moderate (0.5 to 0.75 [or –0.5 to –0.75]), and good to excellent (greater than 0.75 (or –0.75 to –1.0]). 8 Statistical significance was set at an alpha level of 0.05. The data were analyzed using Statistical Package for the Social Sciences v22.0 (SPSS Inc, Chicago, IL).
Results
A total of 8048 consecutive images were reviewed to identify 1419 ankle fractures of which 1255 (88.5%) could be classified by the Danis-Weber System. The average patient age was 48.1 years (range,18-88) and no relationship was identified between age and outcome scores (r=0.08). Although the majority of these were Danis-Weber type B injuries (58.4%, n = 829), 191 were ISF fractures (ie, Danis-Weber type A fractures) of which 159 cases met the inclusion criteria. Among the 32 excluded cases, 12 demonstrated evidence of a concurrent osteoligamentous injury, 8 reported a history of inflammatory arthropathy, 8 had incomplete or inadequate radiographic imaging, 7 sustained a clinically significant reinjury of the same ankle, 3 had undergone prior or subsequent surgery to their ipsilateral foot or ankle, and 2 were deceased. Among patients who met our inclusion criteria, 5 (3.2%) declined participation and 46 patients (28.9%) could not be contacted. This provided us with a total of 108 patients consenting to participate (67.9%), with a reporting follow-up time frame of 3.3 to 4.6 years postinjury (average 3.7 years). Based on the city’s population consensus, an observed incidence of 22 ISF fractures per 100 000 people/year is reported, compared to a total ankle fracture incidence of 163 per 100 000 people/year. 7
In general, patients with conservatively managed ISF fractures reported good outcomes, with more than 60% (n = 65) denying any symptoms and less than 13% (n = 14) reporting any severe difficulties with either work- or life-related activities. The average FAS and SCS scores among all patients was 91.2 (SD = 12.9) and 76.8 (SD = 27.7), respectively (Table 1). No significant differences were found when comparing participants’ self-reported scores to that of the general population. Among patients who continued to report ankle symptoms, the most common complaints were pain (81.8%), followed by stiffness (68.1%) and instability (39.0%). Approximately two-thirds of symptomatic patients reported that their symptoms were mild in severity, with only a minority reporting any severe symptoms (27%) (Figures 2 and 3).
Descriptive and Statistical Analysis of Demographic and Dichotomous Patient Data.a
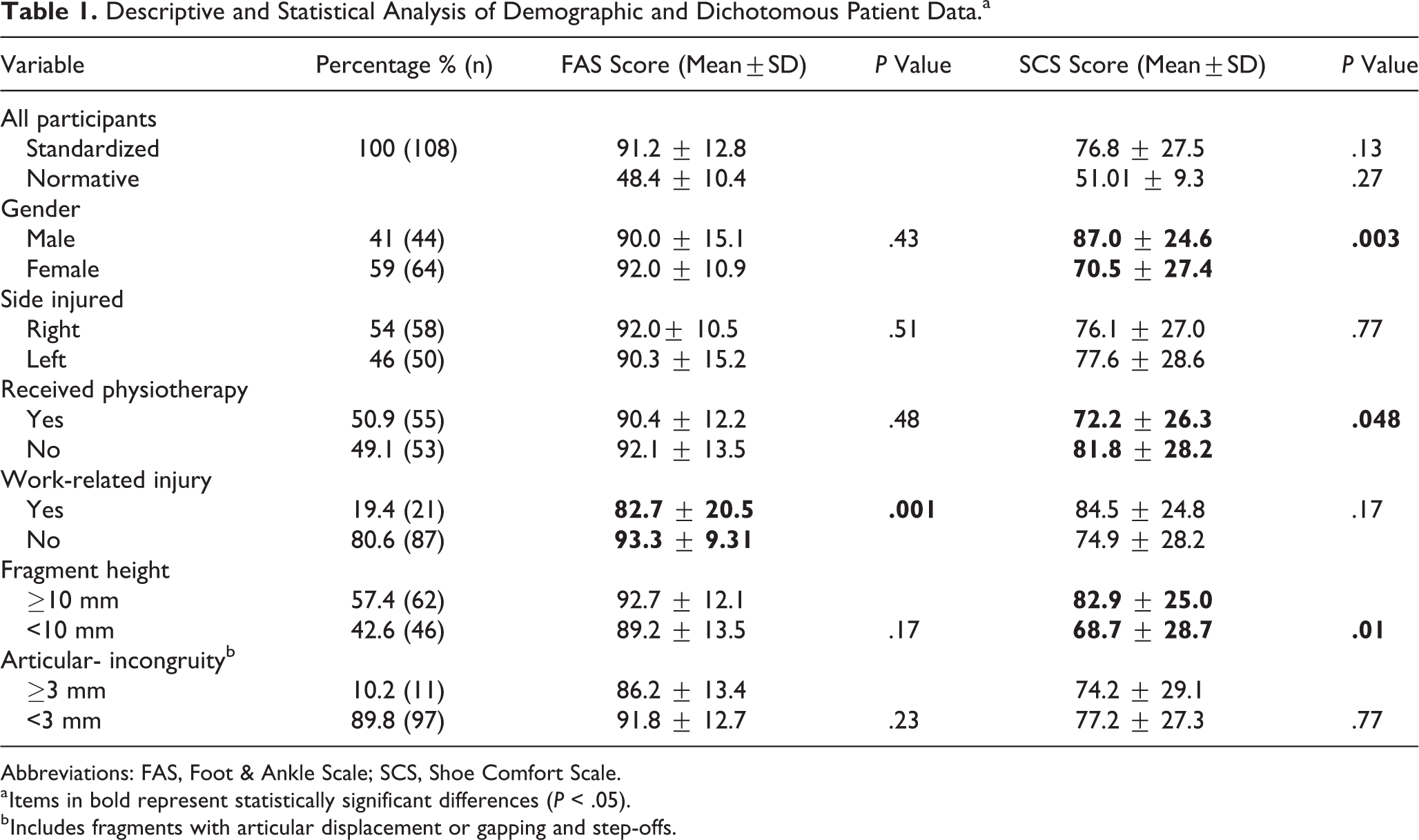
Abbreviations: FAS, Foot & Ankle Scale; SCS, Shoe Comfort Scale.
a Items in bold represent statistically significant differences (P < .05).
b Includes fragments with articular displacement or gapping and step-offs.

Graphic illustration of subjective responses to various survey questions. Likert-type 5-point scale responses transformed into 4 symptom categories for illustration purposes: none (1), mild (2), moderate (3) and severe (4 and 5).

Graphic illustration of subjective responses to various survey questions. Likert-type 5-point scale responses transformed into 4 symptom categories for illustration purposes: none (1), mild (2), moderate (3) and severe (4 and 5).
Ankle pain was most prevalent when walking on uneven surfaces or wearing formal dress-shoes (eg, platform or elevated heel shoes), and least prevalent when lying in bed, standing, or walking on flat surfaces. Regarding formal dress-shoe wear, 39% of participants reported some degree of discomfort, with instability being the most common complaint (51%). Participants reported similar SCS scores when wearing casual, sneaker, and prescription shoes (P > .05). The symptoms of pain (r = 0.54), ankle laxity (r = 0.51), and stiffness (r = 0.50), only moderately correlated with work- or life-related disability.
The average patient age of included participants was 48.1 (range,18-88) years; no relationship was identified between age and outcome scores (r = 0.08). Approximately 59% were females and no differences were reported between gender and either functional outcomes or fracture-fragment characteristics (P > .05). However, females reported lower SCS scores with specific limitations related to formal dress-shoe wear (P = .003). Participants who received physical therapy (PT) treatment reported lower SCS scores and more displaced fracture-fragments (P < .05), but no differences in reported functional or disability outcomes when compared to the general population. On the other hand, patients with work-related injuries reported normal SCS scores and fracture-fragment characteristics, but lower FAS scores and greater disability (P < .05). Although work-related injuries only accounted for 19% of patients, these participants were significantly younger (average 38 years vs 51 years, P = .003), predominantly male (71% vs 34%, P = .002), and reported significantly more symptoms during milder activities, including standing, walking on uneven surfaces, or walking on stairs (P < .01).
In terms of the radiographic characteristics, the majority of ISF fracture-fragments were displaced (60.2%, n = 65), although only 10% (n = 11) demonstrated an articular incongruity equal or greater to 3 mm. Approximately 57% (n = 62) of ISF fractures were of the ATF pattern, with an average height of 5.0 mm and a width of 8.9 mm. MTF fractures comprised 43% (n = 46) of all fractures, with an average height of 16.5 mm and a width of 17.4 mm. There was a significant difference in the displacement distance and proportion of displaced fragments between the 2 fracture patterns: many ATF fractures were displaced (58%, n = 38) with an average displacement distance of 1.5±1.2 mm, compared to MTF fragments where the majority were undisplaced (59.7%, n = 25), with an average displacement of 0.68±0.9 mm (P = .005). Based on our fragment height threshold of 10 mm, those with ATF injuries reported poorer SCS scores (P = .01) and had greater articular displacement (P = .005). However, no relationship was identified between patient-reported outcomes and either the fragment’s width (r = 0.12) or degree of articular displacement (r = –0.20). Likewise, no differences in reported FAS scores, ankle symptoms, or disabilities were identified between the 2 fracture patterns.
Discussion
This study presents the largest population-based investigation of ISF fractures, and the first to describe patient-reported functional outcomes at 3 years postinjury using validated outcome measures. Overall, the results confirm that the majority of conservatively managed isolated ISF fractures report good short-term outcomes with functional scores equivalent to the general population. However, over one-third of patients reported some degree of pain, stiffness, or instability, even though the majority considered these symptoms to be mild in severity. Likewise, smaller avulsion-type fracture patterns, as well as female patients and work-related injuries, all reported less-favorable outcomes. Specifically, patients with work-related injuries reported greater functional limitations, whereas female patients and those with fracture-fragment heights of <10 mm described greater symptoms and limitations with specific shoe wear. These findings suggest that further research and alternative management options may help improve outcomes among specific patient groups.
Previously published studies investigating isolated infrasyndesmotic fractures report comparable, albeit a wider, range of similar outcome findings: Kennedy et al reported on 12 cases of ISF fractures at 3-year follow-up with 81% good to excellent outcomes, Lash et al reported on 50 ISF cases at 2-year follow-up with 58% good to excellent outcomes, and Hughes et al reported on 36 ISF cases with an unspecified “early” follow-up period with 75% good to excellent outcomes. 22,26,28 On the other hand, more reliable comparisons can be made to ankle-sprain studies where as little as 15% of patients report any symptoms at 3-year follow-up. 53 This compares to 40% in our cohort and suggests that ISF fractures may represent a more severe pattern of injury than ligamentous ankle-sprain injuries. A recent study investigating ankle sprain injuries supports this finding where patients with a concomitant avulsion fragment demonstrated inferior outcomes compared with purely ligamentous injuries. 38
Several studies have investigated radiographic characteristics associated with inferior outcomes among ankle fractures and include the number of malleoli involved, the fracture grade, the presence of a posterior malleolar fragment, radiographic signs of syndesmosis or deltoid ligament injury, and the degree of articular congruity and reduction. 18,21,22,24,26,30,36,45 Similarly, our findings suggest that those with ATF injuries with fracture fragments less than 10 mm in height on the mortise view (ie, ATF fragments) are more likely to report greater instability symptoms (P = .006) and inferior SCS scores (P = .01) than those with larger MTF fragments. 3,37,39 We suspect that this may be due to several factors, such as differences in the force distributions between the 2 fracture patterns, the greater proportion of displaced fragments among the ATF cohort (61% ATF vs 40% MTF), the greater displacement of ATF fragments compared to MTF fragments (1.5 mm vs 0.7 mm, P = .004), and a theoretically higher likelihood of bony union among MTF injuries as a result of greater surface area contact. Moreover, we propose that among MTF injuries, the fracture absorbs the majority of traumatic forces with better reported outcomes due to sparing of the surrounding ligaments. In comparison, the ATFL sustains the majority of the forces in ATF injuries and becomes attenuated, rendering patients relatively more likely to report symptoms with specific shoe-wear (eg, high heels) and activities (eg, uneven-ground) because of ligamentous vs osseous pathology. Several biomechanical studies have highlighted the ankle’s sensitivity to instability where excessive tibial translations of greater than 1 mm have been shown to result in up to 40% loss of normal contact articulation. 42,50,54 These findings underscore the need to distinguish between ATF and MTF fracture patterns and may serve as a basis for future proposed studies to help optimize management decisions and outcomes.
In regard to the clinical factors evaluated, the poorer FAS scores reported among work-related injuries may be due to similar physical and psychosocial factors reported by other studies (eg, trauma-related anxiety, physical stressors, financial incentives, secondary gain, etc). 29,35,56 On the other hand, lower SCS scores reported among females were almost exclusively related to limitations in formal dress shoe wear, specifically high-heel and platform shoes. We suspect that the design of these shoes exacerbate any residual laxity or attenuation of the ATFL by simulating the ankle-drawer test because the ankle is held in approximately 20° of plantarflexion and the tibia is inclined to translate over the talus. 10 In regard to physical therapy (PT) treatment, contrary to the documented benefits of PT for ankle-sprains, patients who received PT in our cohort reported inferior SCS scores. 14 This may be due to confounding factors and selection bias; not only did the PT cohort demonstrate statistically greater fracture displacement (P < .038) but patients who continued to experience symptoms appeared to be selectively more likely to be referred for physical therapy. Overall, the inferior outcomes reported by these specific groups suggest that closer clinical attention and alternative management strategies could be considered to optimize outcomes.
The current indications for operative management of isolated ISF fractures remains controversial, with only a few published studies reporting on outcomes of operative interventions. 5,12,16,20,22,31,38,47 None of our study participants underwent operative intervention during the follow-up time frame, irrespective of their degree of displacement or fracture pattern. However, our institute does infrequently operate on these injuries, most commonly for failed conservative management with ongoing pain or signs of ligamentous instability. Unfortunately, the literature remains inconclusive regarding indications to guide operative intervention. A systematic review by Stufkens et al concluded that operatively managed Danis-Weber type A fractures did not demonstrate any better outcomes than operatively managed Danis-Weber type B fractures, and therefore, the benefits of operative intervention remain controversial. 47 Nevertheless, when considering the aforementioned patient groups with less-favorable outcomes, the potential benefits of alternative management options, including early operative intervention, may prove beneficial but requires further study.
Because of the retrospective nature of this study, several limitations are recognized. The small cohort and the use of self-reported evaluations limit the generalizability of some of the results. Likewise, comparisons among various management strategies could not be reliably performed because of a lack of standardization among both orthopedic and physical therapy services (eg, functional bracing vs casting; protected vs immediate weight-bearing; and timing, frequency, and duration of physical therapy). In addition, we relied on either radiographic imaging or the emergency physician’s medical note to confirm the integrity of the deltoid complex, which have both been shown to be unreliable. 13,15 Likewise, subjective patient reporting of stiffness and instability is not as reliable as objective measurements. Furthermore, by only reviewing plain radiographs, we could not confidently exclude associated injuries that include calcaneofibular ligament injuries, malrotated fragments, syndesmotic injuries, and occult fractures. In fact, the latter is reported to occur in up to 12% of ankle-sprain cases. 19,38 Despite these limitations, this study does provide reliable patient-reported outcomes using validated tools that found generally good outcomes among nonoperatively managed isolated ISF and identifies several subgroups that warrant closer clinical attention and consideration of alternative management options.
Conclusions
Patients with nonoperatively managed isolated ISF fractures reported good-to-excellent early functional outcomes similar to that of the general population. More than one-third of patients continued to report ankle symptoms; however, the majority considered them mild in severity, with less than 13% reporting any significant impact on their work- or life-related activities. Less-favorable outcomes were reported among work-related injuries, female patients, and avulsion-type fractures. No relationship was identified between reported outcomes and the patient’s age, degree of articular displacement, or the fragment’s width. These findings support closer clinical attention to specific patient populations and support the development of larger prospective studies.
Supplemental Material
Supplemental Material, FAO892227-ICMJE - Functional Outcomes of Isolated Infrasyndesmotic Fibula Fractures
Supplemental Material, FAO892227-ICMJE for Functional Outcomes of Isolated Infrasyndesmotic Fibula Fractures by Ashlee Dobbe, Lauren A. Beaupre, Khaled Ali Almansoori, Tak-Shing Fung and Angela V. Scharfenberger in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A research grant for this study has been offered from the Covenant Health Research Center (study no. 1344: Pro00026777).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.