
Abstract
Ankle fractures are one of the most common injuries treated by orthopedic surgeons worldwide. However, operative indications, techniques, and reported outcomes following operative fixation vary widely in the literature. This evidence-based review focuses on recent advances in the operative management of ankle fractures including arthroscopic-assisted surgery, deltoid ligament complex repair, expanded indications for posterior malleolus fixation, fibula intramedullary nailing, and dynamic syndesmosis repair.
Level of Evidence:
Level V, expert opinion.
Introduction
Ankle fractures are one of the most common orthopedic injuries in the world, with an incidence between 157 and 187/100 000 people reported in the literature. 13,17,51 Closed stable fractures with appropriate alignment of the ankle mortise and fracture displacement <2 mm can be treated nonoperatively with immobilization and protected weight bearing. Open unstable patterns, or those with significant articular malalignment, often require operative intervention to prevent malunion, nonunion, and early post-traumatic arthritis. Despite these general indications, a recent systematic review found that even in appropriately reduced ankle fractures, only 80% of operatively treated patients had good to excellent outcomes. Other predictors of poor outcomes include associated osteochondral lesions (OCLs), fracture pattern severity (including posterior malleolar involvement), syndesmotic malreduction, persistent medial ankle instability, and increased postoperative infection rates in diabetics and elderly individuals. 24,25,44,46,52,59
In recent years, operative management of ankle fractures has evolved to improve anatomic reduction of the ankle joint, address soft tissue injury around fracture fragments, prevent ankle subluxation, minimize operative incisions, and improve syndesmotic stability. This review will examine recent evidence regarding operative indications and operative management of ankle fractures with a focus on arthroscopic-assisted ankle open reduction internal fixation (ORIF), deltoid ligament complex repair, indications for posterior malleolar fracture fixation, fibula intramedullary nailing, and flexible syndesmotic fixation.
Arthroscopic-Assisted ORIF
Many patients who sustain ankle fractures continue to have persistent ankle pain and swelling months after surgery despite appropriate operative fixation. Fracture malreduction and/or OCLs can lead to altered contact forces and joint mechanics in the ankle resulting in early-onset post-traumatic arthritis. Contact pressures across the ankle joint have been shown to be up to 3.9 times body weight during heel rise and stance phase, and the average tibiotalar contact area is estimated to be 4.4 cm2. 47,48 Studies have demonstrated that as small as a 2-mm lateral talar shift decreases the contact surface area of the tibiotalar joint up to 56% and results in a load increase from 650 to 1590 N/cm2 for a 75-kg person. 37,48 Therefore, anatomic reduction of all ankle joint surfaces and fracture fragments is critical to achieving optimal clinical outcomes and minimizing persistent symptoms after surgery.
A recent systematic review of 1822 operatively treated ankle fractures identified 20% of patients who failed to achieve good to excellent outcomes despite anatomic fracture reduction. 54 One hypothesis to potentially explain the suboptimal outcomes in these patients is related to injury-associated traumatic OCLs and intra-articular loose bodies, which have been reported to occur in up to 20% to 79% of ankle fractures. 17,24,38 A significant correlation has been shown between ankle fracture severity and the incidence of talar OCLs. Patients with trimalleolar ankle fractures or ankle fracture-dislocations are at significantly increased risk of having an OCL compared to low-energy fractures. 49 Traumatic cartilage injuries have been shown to be an independent predictor of posttraumatic arthritis, especially when they occur in the talus and medial malleolus. 56
Ankle arthroscopy has been increasingly used as an adjunct to standard intraoperative ankle fracture fixation as a means to evaluate and manage traumatic intra-articular pathology. Although magnetic resonance imaging (MRI) is commonly used to evaluate cartilage injuries, traumatic edema and hematoma can significantly decrease the diagnostic utility of MRI in the setting of fractures. In addition, MRI is a static examination that does not provide dynamic evaluation of the bony and soft tissue injuries. 8,49 Arthroscopy allows for recorded direct visualization and evaluation of intra-articular pathology and ligamentous injury (Figure 1). Standard anteromedial and anterolateral portals are commonly used with a 30° small joint scope (2.7 mm). Diagnostic arthroscopy is performed before fracture fixation to evaluate the ankle cartilage and also remove intra-articular hematoma that contains inflammatory cytokines and matrix metalloproteinases that can contribute to early arthritis. Arthroscopy is generally kept brief in order to minimize fluid extravasation through the fracture sites and limit iatrogenic soft tissue edema.

(A) Anteroposterior and (B) lateral radiographs of a 24-year-old woman who sustained a closed, right trimalleolar ankle fracture-dislocation after a fall from height. (C) Intraoperative arthroscopy prior to fracture fixation shows a large full-thickness talar osteochondral lesion (OCL), (D) cartilaginous loose bodies from the OCL, and (E) syndesmotic disruption (yellow arrow) not seen on preoperative radiographs.
Studies have recommended that OCLs <150 mm2 be debrided to a stable border in the setting of a fracture whereas OCLs >150 mm2 be treated with debridement and microfracture. 27 For larger lesions not amenable to acute microfracture, arthroscopy can provide valuable prognostic information to surgeons to help plan for future potential osteochondral autograft or allograft transplantation or other future cartilage restoration surgeries. 65 An additional benefit of ankle arthroscopy is the ability to perform dynamic ligamentous stress examinations while directly visualizing the structures of interest. Valgus talar tilt and external rotation stress tests can be applied during arthroscopy to evaluate for dynamic instability of the deltoid ligament and syndesmosis, respectively. Intra-articular fracture fragments and loose bodies can also be identified and removed. 27
Following fracture fixation, arthroscopy can also be used to evaluate the quality of both articular and syndesmotic reduction, which can be difficult to assess with intraoperative fluoroscopy alone (Figure 2). Some surgeons have advocated for the use of intraoperative computed tomography (CT) as an alternative means to evaluate articular and syndesmotic reduction. However, a recent study showed no difference in the rate of syndesmotic malreduction with the use of intraoperative CT compared with standard intraoperative fluoroscopic views. 12 In addition, intraoperative CT is not commonly available in many operating rooms and has additional concerns of cost and increased radiation exposure to the patient and surgical staff.

(A) Ankle arthroscopy setup for the same patient as shown in Figure 1 using a thigh holder, noninvasive ankle strap, and distractor connected to the foot of the bed. Distraction can be applied to the ankle using manual traction through the L-shaped bar, fine-tuned traction through the hand turn knob, or by slowly lowering the foot of the bed. (B) Anteromedial and anterolateral portals to visualize the entire ankle joint surface using a 2.7-mm scope. (C) Direct visualization of the posterior malleolus fracture with probe in the fracture site to assist with debridement followed by (D) visualization of the articular reduction after screw fixation.
There have been 2 randomized controlled trials examining outcomes in arthroscopically assisted vs standard ankle fracture ORIF. Thordarson et al 60 demonstrated no difference in SF-36 and lower extremity scores at 21-month follow-up in a group of 19 patients randomized to treatment with and without arthroscopy. Meanwhile, Takao et al 58 showed significantly improved American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scores in patients treated with arthroscopically assisted ORIF vs those treated without, but the difference in AOFAS scores between groups was only 3.4 points. An ongoing randomized controlled trial in Germany that started in 2016 aims to examine the value of arthroscopically assisted ORIF in patients across a broad spectrum of ankle fracture injury severity. 8
The primary complication associated with ankle arthroscopy is iatrogenic neurovascular injury, specifically to the superficial peroneal nerve. Ferkel et al 14 found a 4.4% rate of iatrogenic neurologic injury related to portal placement and distractor pin placement in a series of 55 patients following ankle arthroscopy. A more recent review of ankle arthroscopy noted a neurovascular complication rate in up to 5.4% of cases, with particular risk to the dorsal intermediate cutaneous branch of the superficial peroneal nerve during creation of the anterolateral portal. 62 Although no definitive recommendations can be made at this time, current literature suggests that ankle arthroscopy has added benefit during ankle fracture fixation in cases of suspected intra-articular loose bodies, OCLs, and acute ligamentous instability.
In the authors’ opinion, ankle arthroscopy in the setting of ankle fractures provides valuable diagnostic and prognostic information that can significantly impact operative management and patient expectations after surgery. We recommend using noninvasive distraction, minimal sharp soft tissue dissection during anteromedial and anterolateral portal placement, and efficient hematoma lavage and joint inspection (<10-minute) in order to minimize soft tissue iatrogenic edema during subsequent fracture fixation.
Deltoid Ligament Complex Repair
Traditional management of bimalleolar-equivalent ankle fractures has consisted of fibular fixation, syndesmotic fixation as needed, and closed management of deltoid ligament injuries allowing the ligament to heal and scar in situ. 53,64 Older studies have suggested that closed management of deltoid ligament injury results in acceptable clinical outcomes. 4,7 A review of deltoid ligament injuries in supination external rotation–type ankle fractures found that the treatment of deltoid ligament lesions in ankle fractures was only necessary if there was soft tissue interposition in the medial gutter preventing adequate reduction of the fibular fracture. 55 However, these conclusions were based on 6 studies published more than 20 years ago, between 1980 and 1999.
More recent literature has demonstrated that failure to repair deltoid ligament disruption can be associated with persistent medial clear space widening despite fibular and syndesmotic fixation. 28,29,32 Patients typically report vague medial-sided ankle pain and swelling after surgery, in particular when going up and down stairs or performing rotational cutting maneuvers with athletics. Arthroscopic studies have found that up to 40% of ankle fractures have either partial or complete deltoid ligament disruption. 24 When a deltoid ligament injury is present in younger, active patients, it typically is associated with a significant syndesmotic injury, and the ligament itself avulses as a full-thickness sleeve off of its proximal attachments to the medial malleolus (Figure 3). 31 As a result, the deltoid ligament can become interposed within the medial gutter, preventing adequate reduction of the ankle mortise leading to healing in a nonanatomic position. 29
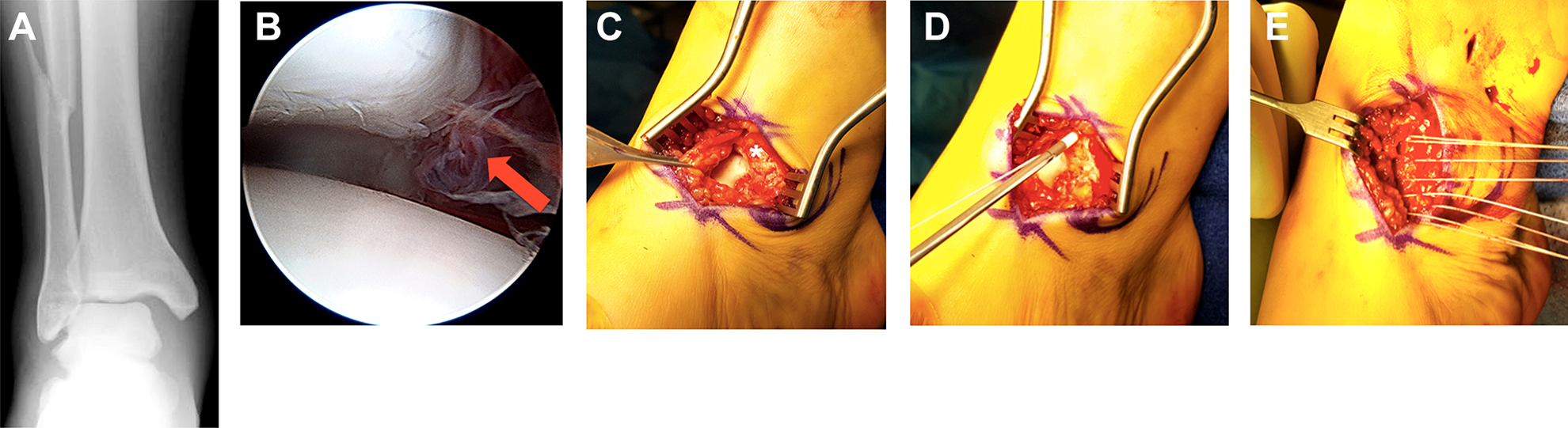
(A) Preoperative anteroposterior radiograph of a 19-year-old woman who sustained a closed, right fibula fracture with large medial clear space widening. (B) Arthroscopy demonstrated medial gutter hematoma and deltoid disruption (red arrow). (C) A small, curvilinear incision was made over the medial gutter and the deltoid ligament complex was found to be avulsed off the anterior aspect of the medial malleolus (asterisk). (D) Double-loaded 3-mm suture anchors (Suturetak, Arthrex Inc) were placed in the medial malleolus followed by (E) repair of the deltoid ligament using multiple horizontal mattress sutures back to bone.
In a series of 14 elite athletes, Hsu et al 29 reported that superficial deltoid ligament complex avulsion in elite athletes with associated syndesmotic injuries was a distinct injury pattern that benefited from operative repair with a high rate of return to play without complications. Prospective data have demonstrated that injury to the deltoid ligament can result in clinically significant chronic ankle instability and early ankle valgus deformity. 25 Retraction of the avulsed deltoid complex and healing in a nonanatomic position can lead to persistent anteromedial gutter pain, medial ankle instability, and functional loss. 26,34,39 Dynamic instability can lead to progressive chondral injury, chronic deltoid disruption, and early medial ankle arthritis. 18,23,25 A growing body of literature now advocates for routine open or arthroscopic evaluation of deltoid ligament integrity in ankle fractures followed by primary repair. 23,28,29
The diagnosis of deltoid ligament injury in the setting of an ankle fracture can be challenging without direct visualization. Medial skin dimpling on physical examination is sometimes present if the ligament has become completely interposed in the medial gutter. Manual or gravity external rotation stress radiographs may show evidence of medial clear space widening, or incongruity of the medial clear space relative to the distance between the tibial plafond and talar dome. Evaluation of medial ankle stability under live fluoroscopy may show signs of gross instability or laxity on valgus talar tilt testing. Direct arthroscopic or open visualization of the deltoid ligament are recommended for evaluation and diagnosis of deltoid ligament injuries and can be used to distinguish superficial from deep tears and partial tears from complete avulsions.
MRI has been shown to be sensitive and specific for detection of deltoid ligament tears, with one study demonstrating that the sensitivity and specificity of 1.5-tesla MRI for superficial deltoid ligament tears was 83.3% and 93.9%, respectively, whereas the sensitivity and specificity for deep deltoid ligament tears was 96.3% and 97.9%, respectively. 11 However, other recent studies have cautioned against using MRI as a predictor of ankle stability in the setting of deltoid ligament injury. One study found MRI evidence of deltoid ligament injury in all SER-type ankle fractures, including stable injuries with negative stress examinations. 43
Deltoid ligament repair in conjunction with ankle fracture ORIF is a relatively new concept, and limited objective data exist regarding outcomes following repair in this setting. However, initial outcomes following isolated deltoid ligament repair for medial-sided ankle instability are favorable, with few complications reported. One study of 51 patients treated with deltoid ligament reconstruction for ankle instability demonstrated excellent AOFAS functional scores at 4.4-year follow-up. Complications in this study included 1 wound infection and 2 patients with persistent paresthesia about the medial side of the ankle. 25
In operatively treated ankle fractures with significant widening of the medial clear space and syndesmosis on preoperative radiographs, the authors routinely make a small curved incision over the anteromedial aspect of the ankle centered over the medial gutter. The deltoid ligament complex is removed from the medial gutter, the medial malleolar bone is freshened to healthy bleeding bone using a small rongeur, and the ligament is provisionally fixed to the medial malleolus using one to two 3.0-3.5-mm suture anchors. The ligament is repaired with multiple horizontal mattress sutures at the end of the case after fibula and syndesmotic fixation is complete. The ankle is held in a slightly inverted position while the sutures are tightened and secured. The remaining suture from the anchors is used to imbricate the overlying tissue and reinforce the repair. 27
Expanded Indications for Posterior Malleolus Fixation
Controversy persists regarding operative indications and fixation of posterior malleolus fractures. The incidence of ankle fractures involving the posterior malleolus has historically varied from 7% to 44%, with more recent studies demonstrating involvement in up to 50% of operatively treated fractures. 10,30,57 The increasing incidence of these fractures is likely related to increased use of CT imaging to better evaluate and characterize fracture patterns, as well as an increased recognition of posterior malleolus fractures as important predictors of ankle fracture stability and long-term functional outcomes. Traditional indications for operative fixation are based largely on biomechanical data and radiographic outcomes and typically include any fracture involving greater than 25% of the tibial plafond articular surface. 20,21
Recent literature has demonstrated that fractures involving as little as 16% of the articular surface are associated with worse clinical outcomes at 2 years when treated nonoperatively. 59 This finding was further supported by a recent systematic review of 33 studies examining management of posterior malleolus fractures, which concluded that fracture size was a weak prognostic indicator, citing that most studies showed no association between fragment size and long-term outcomes. Instead, researchers noted that combined injuries involving the medial and lateral columns, fracture dislocations, articular surface incongruity, and residual talar subluxation were associated with poor outcomes, whereas isolated posterior malleolus fractures generally did well with conservative treatment even in fractures involving up to 47% of the articular surface. 44
Modern studies have recognized the posterior malleolus as an important contributor to syndesmotic stability and congruent ankle alignment. 15,22 Gardner et al created a pronation-external rotation fracture pattern with a posterior malleolar fragment in 10 lower extremity cadaver specimens. Relative to the intact specimens, stiffness was restored to 70% after fixation of the posterior malleolus alone compared with only 40% after traditional syndesmosis screw stabilization. The authors concluded that in posterior malleolus fractures with evidence of syndesmotic disruption, fixation of the posterior malleolus may be more important in restoring syndesmotic stability than traditional syndesmotic screw fixation because of restored stability of the posterior inferior tibiofibular ligament. 15
As a result of these recent findings, indications for operative fixation of posterior malleolus fractures are currently expanding. Updated indications place decreased emphasis on fracture size and increased emphasis on fracture pattern, posterior subluxation, comminution, and posterior pilon variants (Figure 4). 22,44,57 A recent survey of orthopedic surgeons found that the most frequently reported indication for operative fixation of posterior malleolus fractures was not fragment size but rather ankle stability, highlighting that current indications for fixation are much less clear-cut than the previous “25% rule.” 16

(A) Lateral radiograph of a 25-year-old man who sustained a bimalleolar ankle fracture with unstable posterior dislocation after a slide tackle injury. (B) Axial computed tomography cuts demonstrate a posterior rim fracture and distal fibula fracture (C) better seen on 3-dimensional reconstructed imaging. (D) A posterolateral approach was performed and the unstable posterior rim fracture was fixed using a 5-hole 2-mm plate to prevent persistent posterior joint subluxation along with a posterolateral fibula plate as seen on anteroposterior and (E) lateral intraoperative radiographs.
Haraguchi et al 19 classified posterior malleolus fractures as posterolateral oblique type, medial extension type, and small shell type based on CT imaging. Along with several other authors, they advocate for routine CT imaging for any ankle fracture involving the posterior malleolus to aid in operative decision making. 5,6,19 When associated injuries are identified or articular congruity is compromised, literature suggests that a more aggressive approach to ORIF of posterior malleolar fractures involving as little as 10% of the articular surface may improve long-term outcomes. 1,36,44
We routinely obtain a CT scan of all posterior malleolus fractures to determine size, orientation, comminution, and articular impaction. We prefer a prone posterolateral and/or posteromedial approach to the ankle to reduce the posterior fracture with mini-fragment lag screws and rim vs buttress plates (2.0/2.4 mm) depending on the individual fracture pattern (Figure 5). One may also use a 1/3 tubular plate as a buttress as well.

(A) Lateral radiograph of a 30-year-old woman who sustained a posterior malleolus fracture after a motor vehicle accident. (B) Axial computed tomography cuts show posterolateral and posteromedial fracture fragments with interposed articular comminution (C) confirmed on 3-dimensional reconstructed imaging. (D) A posterolateral approach was used to access both fragments that were fixed using two 2.4-mm buttress plates (E) followed by syndesmotic fixation using a 4-hole 1/3 tubular plate with 2 divergent TightRopes.
Limited-Incision Fibular Nailing
Intramedullary nail fixation of distal fibula fractures was first described by McLennan et al 40 in 1986. Since that time, significant advances in implant design and operative technique have led to a recent resurgence in the use of fibular nails. Although fixation with a lag screw and lateral neutralization plate construct is currently the most commonly used method of stabilization for distal fibula fractures, this method is associated with wound complication rates varying from 2% to 15%. Open injuries, soft tissue compromise, and patients with diabetes, peripheral vascular disease, and age >75 years have been identified as independent risk factors in predicting wound complications. 52 The goal of fibula intramedullary nailing is to minimize soft tissue dissection around the fracture site while providing a load-sharing implant for weight bearing (Figure 6).

(A) Anteroposterior and (B) lateral radiographs of a 65-year-old woman with diabetes who fell down a flight of stairs sustaining an open bimalleolar ankle fracture-dislocation with lateral soft tissue compromise and medial malleolar comminution. (C) Fixation was achieved using a 3×130-mm fibular nail (FibuLock, Arthrex Inc) along with 2.4-mm medial buttress plate, 3-mm cannulated lag screws, and a TightRope through the nail as seen on anteroposterior and (D) lateral intraoperative radiographs.
Tracey et al 61 retrospectively reviewed a series of 16 patients with bimalleolar and trimalleolar ankle fractures treated with fibula intramedullary nailing (FibuLock; Arthrex Inc, Naples, FL) for the lateral malleolus and reported a 100% union rate of the lateral malleolus with no wound infections despite 5 patients having diabetes and 1 being a smoker. Bugler et al 9 published a series of 105 patients with unstable ankle fractures treated between 2002 and 2010 with an alternative fibula rod (Acumed, Hillsboro, OR). In contrast to the series by Tracey et al, 61 the authors noted a 4.7% infection rate related to the distal fibula and failure of fibular fixation in 6.6% of patients. Seventy-six percent of their patients had major medical comorbidities, including ischemic heart disease (15%), diabetes (10.4%), chronic obstructive pulmonary disease or asthma (9.5%), and stroke (8.5%). They noted significantly increased incidence of fixation failure in patients with no interlocking screws or with only 1 distal interlocking screw. As a result, they recommended fixation with at least 1 distal interlocking screw and 1 syndesmotic screw. 9
In a prospective randomized controlled trial comparing lateral locked plating and the Epifisa nail (FH Orthopaedics, Mulhouse, France), Asloum et al 3 showed no difference in union rates, significantly decreased complication rates (7% vs 56%), and significantly better Olerud-Molander scores in patients treated with intramedullary nail fixation. Several technique papers have also described the utility of intramedullary fibular nailing in geriatric patients with poor skin quality and decreased tolerance for future operations for hardware removal. However, they emphasize the importance of an appropriate start point and reaming technique, as lateral cortical perforation with a rigid intramedullary device in the setting of poor bone quality is a potential risk. 2,50
In our opinion, expanded indications for fibula intramedullary nailing now include younger, healthier patients who desire limited incisions and early return to weight bearing through the load-sharing device. Currently, early results of modern intramedullary fibular nailing are promising, and consideration should be given to this technique in both high-risk patient populations and athletic patients.
Dynamic Syndesmotic Fixation
Several recent retrospective studies and randomized controlled trials have compared outcomes of TightRope suture button fixation (Arthrex Inc) to traditional syndesmotic screw fixation for the treatment of ankle fractures with associated syndesmotic injury. Naqvi et al 41 used postoperative CT imaging to evaluate the incidence of syndesmotic malreduction (defined as 2 mm of syndesmotic widening relative to the contralateral ankle) in 46 patients treated with either suture button fixation or syndesmotic screws. The authors found a 21.7% rate of malreduction in the screw cohort and a 0% rate of malreduction in the suture button cohort. However, despite this radiographic difference, they found no difference in AOFAS score or Foot and Ankle Disability Index score between groups. 41
Kortekangas et al 33 performed a similarly designed, prospective, randomized controlled trial and found no difference in rates of malreduction or postoperative patient-reported outcomes scores in the suture button cohort versus the syndesmotic screw cohort both immediately following surgery and at 2-year follow-up. In a multicenter randomized controlled trial, Laflamme et al 35 demonstrated significantly improved Olerud-Molander scores at 12 months in the suture button group and an 11.1% rate of loss of reduction in the syndesmotic screw group vs 0% in the suture button group. A meta-analysis of 5 randomized controlled trials totaling 280 patients comparing suture button fixation to syndesmotic screws found a statistically higher AOFAS score in the suture button group at 1-year follow-up. However, the authors concluded that this difference was unlikely to be clinically meaningful and found no statistically significant differences for any other parameters examined. 45
There have also been several cost analyses comparing suture button fixation to standard syndesmotic fixation. Neary et al 42 assumed a 20% rate of syndesmotic screw removal and a 4% rate of suture button removal and found the total cost of syndesmotic screw fixation to be $1482 greater than suture button fixation given a suture button cost of $880. In addition, the authors found that the screw removal rate would have to be less than 10% for syndesmotic screws to be more cost effective. 42 It should be noted that this analysis assumed fixation with only 1 suture button, whereas many surgeons emphasize the need for 2 divergent suture buttons to obtain adequate syndesmotic stability. A separate cost analysis by Weber et al 63 found that the screw removal rate would need to exceed 27% to make a single suture button more cost effective than a single syndesmotic screw. This number increased to 53% when 2 suture buttons were compared to 2 syndesmotic screws. 63
Overall, recent studies demonstrate a significant trend toward increased use and improved radiographic and clinical outcomes associated with suture button fixation for syndesmotic injuries compared with traditional syndesmotic screws. In cases of syndesmotic injury with low-energy distal fibula or bimalleolar ankle fractures, we typically use one TightRope device through a screw hole in the fibula plate to avoid creating a stress riser with the lateral button. For cases of isolated syndesmotic injury or Maisonneuve injury patterns, we routinely use a 2-hole buttress plate in combination with 2 divergent TightRopes to ensure increased rotation stability and fixation across the anterior and posterior aspects of the syndesmosis (Figure 7).

(A) Anteroposterior tibia radiograph of a 40-year-old man who sustained a ground-level fall with resultant right displaced, midshaft fibula fracture with (B) significant syndesmotic and medial clear space widening that is better seen on anteroposterior ankle radiograph. (C) The fibula shaft fracture was fixed using a lag screw and neutralization plate to ensure proper fibula length, alignment, and rotation and to assist with anatomic syndesmotic fixation. (D) A 2-hole buttress plate was used distally with 2 divergent TightRopes for syndesmotic fixation as seen on anteroposterior and (E) lateral postoperative radiographs. The superficial deltoid ligament complex was found to be avulsed off of the anterior aspect of the medial malleolus and flipped into the medial gutter. Therefore, the deltoid ligament was repaired directly back to bone using two 3-mm suture anchors before final tightening of the TightRopes.
Conclusions
There have been several significant advances in the operative management of ankle fractures in recent years. Current topics of interest include the use of ankle arthroscopy for ankle fractures, repair of the deltoid ligament complex, expanded indications for posterior malleolar fractures, minimally invasive fibula intramedullary nailing, and flexible syndesmotic fixation.
There is a modest amount of evidence to support the use of arthroscopy in the treatment of ankle fractures. Arthroscopically assisted ORIF offers an opportunity to evaluate and treat ligamentous and intra-articular pathology during the index procedure. Furthermore, it allows for direct evaluation of articular and syndesmotic reduction following fixation. Perhaps most importantly, it can inform discussions regarding long-term prognosis and help set appropriate patient expectations. There is some evidence to support repair of the deltoid ligament complex to aid in articular reduction and help prevent development of medial gutter pain, chronic medial ankle instability, resulting chondral injury, and functional loss.
In the setting of posterior malleolar fractures, recent literature suggests that fragment size is likely not as critical as previously thought. Instead, relatively large isolated posterior malleolar fractures with adequate articular congruity can be treated nonoperatively, although in the presence of associated bimalleolar, syndesmotic, or ankle fracture variant injuries, fractures involving as little as 10% of the articular surface should be treated more aggressively with formal ORIF.
Limited-incision intramedullary nail fixation of the distal fibula is emerging as an alternative to conventional lateral plate constructs in certain patient populations who require decreased soft tissue dissection and/or early weight bearing. Finally, recent studies comparing flexible syndesmotic fixation to conventional syndesmotic screw fixation suggest clinically equivalent outcomes in both groups with fewer complications and improved radiographic outcomes using suture button devices. Cost analyses favor suture button fixation in practices with high rates of syndesmotic screw removal, whereas screw fixation is more cost effective in practices with low screw removal rates.
The short- and long-term clinical benefits of these surgical advances remains unclear and require future prospective, randomized, controlled trials in order to determine potential differences in patient-reported outcomes between techniques. As ankle fracture surgery continues to evolve, research investigating minimal clinically important differences between modern operative techniques is critical to help determine additional areas of improvement that can be achieved with surgery.
Supplemental Material
Supplemental Material, FAO888505-ICMJE - Advances in the Surgical Management of Ankle Fractures
Supplemental Material, FAO888505-ICMJE for Advances in the Surgical Management of Ankle Fractures by David J. Wright, Jason T. Bariteau and Andrew R. Hsu in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew R. Hsu, MD, reports that he is a paid consultant for Arthrex, Inc., outside the submitted work. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.