
Abstract
This case report demonstrates a unique variant of a Chopart dislocation resulting in a plantar cuboid and navicular dislocation without concomitant fracture in a 48-year-old man. The mechanism of injury involved a low-energy plantarflexion moment from stepping off a small embankment. This report reviews the pertinent midfoot anatomy, discusses the proposed mechanism of injury, and demonstrates an effective method of treating these complex injuries with open reduction and internal fixation. Final results with 20 months of follow-up were excellent. This unusual midfoot dislocation is a complex injury that required open treatment for anatomic restoration. In complex Chopart dislocations, early open reduction should be strongly considered as the initial treatment to properly restore anatomy and function.
Introduction
Injuries involving fractures and dislocations of the Chopart joint are rare. 1,2,5,9,10 The Chopart joint, or transverse tarsal joint, involves 2 articulations: the calcaneocuboid joint and the talonavicular joint. It was named after Francois Chopart, a pioneer of urologic surgery who invented the amputation at the transverse tarsal joint in the late 1700s. 11 The Chopart joints rarely dislocate because of their intrinsic stability. 5,9 The first report of an isolated calcaneocuboid dislocation without fracture was described in 1969. 2 Partial or complete dislocation of either bone requires severe capsular and ligamentous injury and is typically a result of a high-energy mechanism. 1,2,5,8,10
The navicular is firmly seated between the cuboid laterally, the talus proximally, and the cuneiforms distally. It has extensive ligamentous stability conferred by plantar, dorsal, and interosseous ligaments with the surrounding tarsal bones and musculotendinous stability from the anterior and posterior tibial tendons. 9 The cuboid also has significant stability, with 5 bony articulations, stout ligamentous support, tendinous support from the peroneus longus, and its inherent shape and function within the lateral longitudinal arch. 5
Anatomic reduction of midfoot injuries is essential to provide optimal long-term functional results and to decrease the potential for future degenerative changes. 4,6,7,10 Definitive treatment of a Chopart dislocation with closed reduction is often unsuccessful as it can be difficult and possibly damaging to surrounding anatomic structures. Our case report presents a previously undescribed Chopart variant dislocation injury: plantar dislocation of the cuboid and navicular without concomitant fracture.
Case Report
A 48-year-old man (BMI of 31.8) with no history or examination findings of ligamentous laxity or neuropathy landed awkwardly on a plantar flexed foot after stepping off of a 3-foot smooth concrete embankment while wearing flexible-soled tennis shoes. The injury occurred during the day, and the patient was not intoxicated. He subsequently experienced severe pain and an inability to weightbear on his right foot. Initial clinical examination 8 hours after injury revealed ecchymosis, swelling, and pain over the medial aspect of his midfoot without a traumatic wound or neurovascular injury. Radiographs and computed tomographic (CT) scan of the right foot revealed plantar dislocations of the cuboid and navicular bones without fracture (Figures 1 and 2).

(A) Initial anteroposterior, (B) oblique, and (C) lateral injury radiographs demonstrating the Chopart variant cuboid and navicular dislocations.

Initial injury computed tomography scan demonstrating plantar dislocation of the cuboid and navicular in the (A) axial and (B) sagittal planes.
In the operating room 22 hours after injury, an unsuccessful attempt at closed reduction resulted despite being under full relaxation, with general anesthesia, intraoperative fluoroscopy, and external distraction. Open reduction commenced with a dorsal medial incision centered over the talonavicular and naviculocuneiform joints. The plantar and medial capsular and ligamentous structures of the navicular were disrupted and displaced into the naviculocuneiform joint (Figure 3). A “joystick” Kirschner wire (K-wire) was placed into the navicular as a reduction aid. The navicular injury showed translation inferiorly and medially with a rotational component, medially to plantar (Figure 4). Using an abduction and dorsally directed force with axial traction, the navicular was reduced within its anatomic articulations and provisionally fixed with multiple 1.6-mm K-wires. Next, a dorsolateral incision was made over the calcaneocuboid joint, which demonstrated significant lateral ligamentous disruption (Figure 5). In a similar fashion, a “joystick” K-wire was used in the cuboid as a reduction aide. With a dorsally directed force and axial traction, the cuboid was reduced, reestablishing its anatomic articulations and lateral column length (Figure 6).
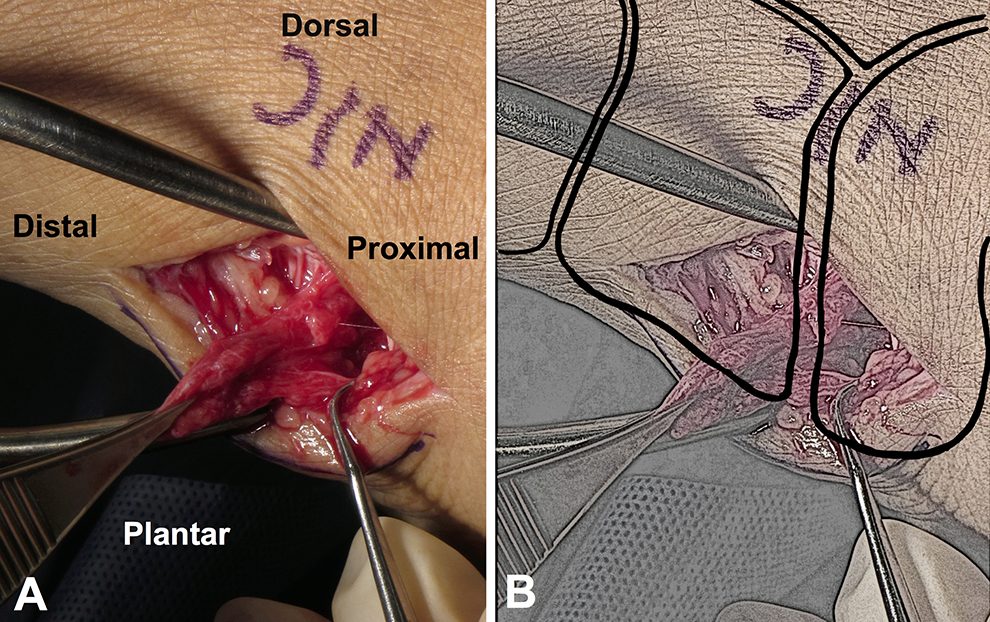
(A) Intraoperative image of the dorsal medial incision revealing plantar and medial naviculocuneiform joint capsule and interosseous ligamentous disruption. The soft tissues were displaced into the naviculocuneiform joint from the injury and removed from the joint intraoperatively to facilitate joint reduction. (B) Sketch of panel A including an idealized depiction of the bony anatomy in its proper anatomic location. Illustrated by Daniel Zieman.
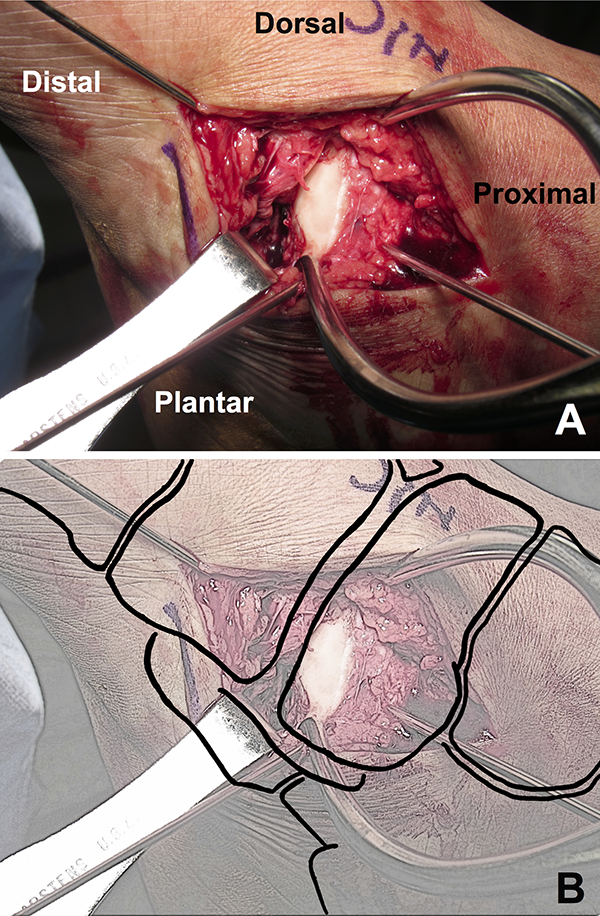
(A) Intraoperative image of the dorsal medial incision demonstrating substantial naviculocuneiform ligamentous disruption with plantar, medial, and rotational displacement of the navicular with respect to its cuneiform articulations. The “joystick” Kirschner wire in the navicular was used to achieve joint reduction. (B) Sketch of panel A including an idealized depiction of the bony anatomy in its proper anatomic location. Illustrated by Daniel Zieman.

(A) Intraoperative image of the dorsal lateral incision over the calcaneocuboid joint demonstrating substantial lateral calcaneocuboid ligamentous disruption and plantar dislocation of the cuboid (†) with respect to its calcaneal (*) articulation. The Kirschner wire is retracting the peroneal tendons. (B) Sketch of panel A including an idealized depiction of the bony anatomy in its proper anatomic location. Illustrated by Daniel Zieman.

(A) Intraoperative anteroposterior fluoroscopic image of the initial reduction using a calcaneocuboid external fixation distraction system as well as provisional talonavicular and naviculocuneiform Kirschner wire fixation. (B) Lateral fluoroscopic image of the provisional fixation of the Chopart joint complex with 1.6-mm Kirschner wires.
The dislocated joints were then fixed definitively. A 6-hole 2.7-mm plate was positioned medially over the talonavicular and naviculocuneiform joints and extra-articular screws were placed in the medial cuneiform, navicular, and talus. Through the lateral incision, an X-plate aligned the calcaneus and cuboid with extra-articular screws (Figure 7). A stable reduction of the Chopart joints was confirmed by manipulation using live fluoroscopy.

(A) Intraoperative anteroposterior and (B) lateral fluoroscopic images of the final fixation construct. A medial spanning plate was used over the naviculocuneiform and talonavicular joints and a lateral spanning X-plate was used over the calcaneocuboid joints. Note the anatomic restoration of the perinavicular and pericuboid joint spaces.
Postoperatively, the patient was made nonweightbearing and was placed into a short leg splint in neutral position. Sutures were removed at 3 weeks, and he was kept in a short leg cast for a total of 7 weeks with 3 cast changes in 2- to 3-week intervals. He remained compliant with his nonweightbearing status. He was then transitioned into a fixed-angle walking boot and remained nonweightbearing for an additional 4 weeks to “over-protect” the operative reconstruction. He was encouraged to remove the boot for daily range of motion exercises. At the 12-week follow-up visit, weightbearing radiographs demonstrated maintenance of anatomic reduction, and he was advanced to full weightbearing. Decreased swelling resulted in prominence of the medial plate. Hardware removal was planned at 6 months postoperatively because of eventual implant failure with the use of bridge plates spanning joints, but the patient ultimately elected not to have the surgery. Postoperative radiographs at the 13th month demonstrated maintained perinavicular and pericuboid joint spaces (Figure 8). During a 20-month telephone interview, he was able to return to work as a welder; however, he noted fatigue after prolonged standing at the end of the day. He was able to ambulate and climb stairs but was not able to run, and his shoe size has increased by a half size.

(A) Weight-bearing anteroposterior, (B) oblique, and (C) lateral radiographs at 13 months of postoperative follow-up. There was no hardware failure or collapse noted. The perinavicular and pericuboid joint spaces were well maintained.
Discussion
Chopart dislocations are rare injuries and are challenging to treat. 1,2,5,6,9,10 The surrounding bony articulations and ligamentous attachments of the navicular and cuboid create stable joints that are thought to require high energy to dislocate, typically accompanied by a concomitant fracture. 1,2,5,8,10 In our case, a Chopart dislocation without navicular or cuboid fracture was encountered from a low-energy fall onto a plantarflexed foot with subsequent rotation.
Chopart dislocations are uncommon because of the natural stability of the navicular and the cuboid. The navicular articulates with the talus proximally, the 3 cuneiforms distally, and the cuboid laterally. It has ligamentous support from the long and short plantar ligaments, the plantar calcaneonavicular “Spring” ligament, interosseous ligaments, intertarsal ligaments, and the bifurcate ligament that inserts both on the cuboid and the lateral surface of the navicular. 9 Medially, the posterior tibial tendon inserts on the navicular tuberosity and provides musculotendinous support.
The calcaneocuboid joint also has substantial inherent stability and is one of the least common joints in the foot to dislocate. 5 Its stability is conferred by its extensive soft tissue support. The soft tissues that contribute to the joint’s stability include ligamentous structures—long and short plantar ligaments, dorsal and plantar calcaneocuboid ligaments, the bifurcate ligament, interosseous ligaments, intertarsal, and tarsometatarsal ligaments—joint capsule, and lateral tendinous support from the peroneus longus tendon and its articulation with the cuboid via the peroneocuboid joint. 3,5
Our mechanism is similar to an incomplete variant of the navicular dislocation described by Pathria et al, in which forced plantarflexion resulted in disruption of the naviculocuneiform joint and the cuneiform bones impacted the plantar surface of the navicular, thus dragging the plantar naviculocuneiform joint capsule into the joint space as it returned to its natural position. 9 We postulate that the mechanism of injury required for this Chopart dislocation variant involved foot plantarflexion and eversion with a vector of energy originating from the naviculocuneiform and talonavicular joints and exiting laterally through the calcaneocuboid and cuboid-metatarsal joints. A concomitant eversion force was likely present resulting in the medial naviculocuneiform ligamentous disruption noted intraoperatively and resulting in a transfer of force through the Chopart joint laterally.
In our case, similar to previous reports of midfoot dislocations, open reduction was required for restoration of anatomic alignment. 1,4,5 Closed reduction is inherently difficult because surrounding soft tissue can become interposed into the Chopart joint, and the multidirectional force required to dislocate the cuboid or navicular requires a multidirectional reduction maneuver to restore a complex anatomic relationship between multiple surrounding bony articulations. 1
Not only is closed reduction difficult and frequently unsuccessful, but it also can be detrimental. It is difficult to adequately restore the complex anatomic relationship of the perinavicular and pericuboid articulations. It is also challenging to adequately assess anatomic reduction of the Chopart joint solely with plain radiographs. Open reduction allows for direct visualization of the restoration of anatomic alignment and for inspection of articular surface damage. The greatest predictor of long-term functional outcomes in midfoot dislocations is early anatomic reduction. 4,7,10 A single attempt at closed reduction is reasonable, although aggressive and repeated closed reduction maneuvers of midfoot dislocations can cause additional damage to both bony and soft tissue structures. The anterior tibial artery has an arterial branch that anastomoses with the deep plantar arterial circulation. A disruption of this anastomosis from repeated forceful reduction maneuvers could result in excessive bleeding and compartment syndrome. 10 Richter et al demonstrated that the highest postoperative functional scores of fractures and dislocations of the midfoot were those treated with early open reduction and fixation. 10 Therefore, we suggest that open treatment should be strongly considered early in all Chopart dislocations.
We present a case of a rare Chopart variant dislocation without concomitant fracture. Chopart dislocations are rare as the talonavicular and calcaneocuboid joints have substantial intrinsic anatomic stability. The mechanism of injury involves plantarflexion and midfoot rotation and can occur even with a low energy mechanism. The Chopart joint anatomy is complex, and restoration of proper anatomy requires intimate knowledge of the cuboid, the navicular, their bony articulations, and their network of ligamentous attachments. These injuries present a treatment challenge, and we recommend early open treatment as this may allow for more precise anatomic reduction and improved long-term functional outcomes.
Supplemental Material
Supplemental Material, FAO876262-ICMJE - The Chopart Variant Dislocation: Plantar Dislocation of the Cuboid and Navicular
Supplemental Material, FAO876262-ICMJE for The Chopart Variant Dislocation: Plantar Dislocation of the Cuboid and Navicular by M. Wesley Honeycutt and Mark D. Perry in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.