
Abstract
A select 10-30% of patients with recurrent lateral ankle sprains develop chronic ankle instability (CAI). Patients with chronic ankle instability describe a history of the ankle “giving way” with or without pathological laxity on examination. Evaluation includes history, identification of predisposing risk factors for recurrent sprains, and the combination of clinical tests (eg, laxity tests) with imaging to establish the diagnosis. There are a variety of nonoperative strategies to address chronic ankle instability, which include rehabilitation and taping or bracing to prevent future sprains. Patients who fail conservative treatment are candidates for surgery. The anatomic approaches (eg, modified Broström) are preferred to nonanatomic procedures since they recreate the ankle’s biomechanics and natural course of the attenuated ligaments. There is a growing interest in minimally invasive procedures via ankle arthroscopy that also address the associated intra-articular disorders. This article provides a review of chronic lateral ankle instability consisting of relevant anatomy, associated disorders, evaluation, treatment methods, and complications.
Level of Evidence:
Level V, expert opinion.
Keywords
Introduction
In the United States, ankle sprains occur frequently with a reported incidence of 2.15 per 1000 person-years. 61 Ankle sprains also account for a substantial amount of health care cost. 52,54 Because the most frequent mechanism is an inversion force on a plantarflexed foot, the lateral ankle ligaments are commonly sprained. 26,62 Regardless of initial treatment, approximately 10% to 30% of patients with acute lateral sprains can develop chronic ankle instability (CAI). 46
Currently, there is great heterogeneity regarding the exact definition of CAI. 31,33 In this review, CAI will be defined as recurrent ankle instability episodes occurring for a minimum of 1 year after an initial injury. 60 CAI has been traditionally classified as either mechanical or functional instability. 33 Mechanical instability may occur as a result of adverse anatomical changes such as ligamentous laxity and impaired arthrokinematics. 33 Functional instability may be a result of adverse neuromuscular changes such as impaired proprioception and neuromuscular control. 25,33 Functional instability has also been described as persistent symptoms without pathological laxity on examination. 20 However, it is now understood that mechanical and functional instability can coexist. 33
Most patients with CAI are initially treated conservatively via a rehabilitation program. However, those who do not respond favorably to conservative measures are candidates for surgical intervention. The purpose of this review is to describe the relevant anatomy, associated disorders, evaluation, treatment options, and complications of CAI.
Anatomy
The lateral ligaments of the ankle include the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL) (Figure 1). The ATFL is contiguous with the joint capsule and has a variable number of bands. 15,28 In a cadaveric study of the human lateral ankle ligaments, the authors found that 50% (7 of 14) of the specimens had a single-banded ATFL, with the remaining having 2 bands. 15 A single-banded ATFL’s origin is located on the fibula’s anterior margin approximately 13.8 mm from the lateral malleolus’s inferior tip. 15 The ATFL inserts just anterior to the lateral articular surface of the talus. 15 The CFL’s origin is approximately 5.3 mm anterior to the lateral malleolus’s inferior tip. 15 The CFL crosses both the subtalar and talocrural joint 15 and lies underneath the peroneal tendons. The CFL courses posteroinferiorly to insert onto the lateral aspect of the calcaneal body. 15,28,33 The PTFL’s origin is located approximately 4.8 mm superior to the lateral malleolus’s inferior tip on the medial aspect of the lateral malleolus, and its fibers spread onto the posterolateral aspect of the talus. 15

Intraoperative view of the lateral ankle ligaments (CFL and ATFL) along with the peroneal sheath and inferior extensor retinaculum (IER).
Ankle stability is conferred by passive ligamentous restraints, articular surface congruity, and active musculotendinous units. 33 The ATFL, CFL, and PTFL provide static restraint to the lateral aspect of the ankle. The ATFL is taut in plantarflexion and prevents anterior talar displacement and excessive plantarflexion. 28,33 Following an inversion injury of a plantarflexed foot, the ATFL is at risk of rupture. 28 It is also the weakest of the 3 ligaments. In a biomechanical study on the human ankle ligaments, the ATFL exhibited the lowest load to failure (138.9 N) compared to the CFL (345.7 N) and the PTFL (261.2 N). 3 In contrast, the CFL is taut in dorsiflexion; it prevents excessive subtalar and talocrural joint supination, excessive hindfoot inversion and internal rotation, and assists with subtalar joint stability. 28,33 The PTFL is also taut in dorsiflexion; however, it helps prevent excessive ankle internal rotation and inversion. 33,45 The PTFL is rarely affected, and it usually ruptures only after severe injuries such as ankle dislocation. 44
The inferior extensor retinaculum (IER) is an important secondary static stabilizer. It is composed of several bands (lateral, intermediate, and medial) and its characteristic shape secures the peroneus tertius and extensor digitorum longus tendon. 18 Similar to the CFL, the IER’s lateral band stabilizes the subtalar joint. 33
In contrast to the static stabilizers, the musculotendinous units provide stability via muscular contractions. 33 The peroneal muscles are important active stabilizers of the lateral ankle. During a sprain, the peroneal muscles serve as a major line of defense to counteract the excessive inversion force on the ankle. 34 A delayed peroneal reaction time is associated with CAI. There is some evidence that the ankle’s sensory fibers and mechanoreceptors are also damaged during a sprain. 34,38 This can potentially compromise the ankle’s proprioceptive reflex mechanism and lead to a disruption of peroneal reaction time. 34,38
Evaluation
Patients with CAI will report a history significant for prior or recurrent lateral ankle sprains. They will also complain of their ankle “giving way” without warning, and the sense of instability while ambulating on uneven ground and difficulty participating in sports. It is important to evaluate for generalized laxity as seen in inheritable disorders such as Ehlers-Danlos. The patient should also be evaluated for predisposing risk factors for recurrent sprain. Intrinsic or patient-related risk factors include an underlying foot deformity, diminished proprioception, postural imbalance, BMI, gender, and/or a history of a prior lateral ankle sprain. 60 Traditionally, a history of a prior sprain has been considered a more consistent risk factor for recurrent sprains. 19 However, most patients with a history of ankle sprain do not develop CAI. In a recent meta-analysis, a prior history of ankle sprain conferred a nonsignificant pooled relative risk of 1.44. 60 This discrepancy can be explained by several factors that can potentially influence the clinical outcomes after a sprain such as successful rehabilitation, the type of rehabilitation protocol, treatment compliance, and the type of associated injuries. 8
The physical examination should include inspection for alignment since varus tibia and hindfoot malalignment can lead to CAI (Figure 2). 39,58 The patient’s hindfoot alignment is assessed in standing position from the back, and normally the hindfoot is at 5 to 10 degrees of valgus. 39 However, clinical examination for alignment should be supplemented with radiography to increase its diagnostic accuracy and reliability. 49 The patient’s neurovascular status should be assessed. The superficial peroneal nerve should be evaluated since it is at risk of traction damage following a severe inversion injury. 43 Also, an ATFL sprain increases the ankle’s motion, which can then place the superficial peroneal nerve under a greater amount of strain and excursion. 43 This can lead to a loss of normal nerve function and potentially the loss of the ankle’s protective reflexes. 43

Image demonstrating hindfoot varus malalignment (black arrow).
The lateral ankle ligaments should be palpated for tenderness. Laxity should be assessed on examination and compared to the contralateral side as a reference. The anterior drawer test (ADT) should be performed to assess for ATFL laxity (Figure 3). ADT’s accuracy may be enhanced if performed with palpation and compared to the contralateral ankle. 17 The talar tilt (TT) or inversion stress test predominantly evaluates for CFL competence. In this test, the ankle is placed in dorsiflexion and the hindfoot is inverted. 33 Similar to the ADT, the TT test should not be used as a stand-alone test and should be used cautiously because mechanical laxity is not always present in patients with CAI. 48 Both the ADT and TT test have variable interobserver reliability and are also physician dependent. 35 Placing the patient in a prone position with the midshaft of the tibia positioned at the edge of the examination table and repeating the TT test can be helpful as the excursion of the hindfoot compared to the lateral fibula is easier to visualize with the patient prone. The addition of the prone position also acts as a reminder to perform a plantarflexion test to assess for posterior ankle impingement, and to palpate the peroneal tendons in order to assess for synovitis or a tear.

Image demonstrating the anterior drawer test (ADT) to evaluate for anterior talar displacement relative to the tibia.
The motor strength of the peroneal muscles should be evaluated for weakness. A single-leg balance test can be performed, which is especially useful for predicting future ankle sprains in the athletic patients. 57 In this test, the patient is asked to balance on one leg with the eyes open and closed, and then a positive test is reported if the patient complains of imbalance. 57
Bilateral weight-bearing radiographs of the ankle should be obtained since they allow for direct comparison to the contralateral side. 56 This is especially helpful for cases with more subtle malalignment. 39 The Saltzman view 49 can be used to supplement clinical examination because it objectively evaluates for hindfoot alignment in the coronal plane. Radiography will also demonstrate the presence of osteoarthritis, osteophytes, and/or subtalar joint pathology.
Stress radiography’s utility for diagnosing CAI has been evaluated. In this test, radiographic imaging is obtained while a clinical laxity test (eg, ADT and TT test) is also performed. The ADT stress test is evaluated in the lateral view, and then the anterior talar displacement is measured. 23 The TT stress test is evaluated in the anteroposterior view, then the angle between the dome of the talus and tibial plafond is measured. 23,35 Traditionally, an ADT greater than 10 or 5 mm side-to-side difference, or TT greater than 10 degrees (Figure 4) or 5 degrees side-to-side difference, has been considered diagnostic of ankle instability. 35 However, the major criticisms surrounding stress radiography include underestimating both the anterior talar translation and the TT angles, variable reference ranges, and whether mechanical devices versus manual stress should be applied during the laxity tests. 23,35

Positive talar tilt on radiographic imaging.
Other imaging modalities include ultrasonographic (US) and magnetic resonance imaging (MRI) (Figure 5). In a recent meta-analysis evaluating efficacy of several imaging methods for diagnosis of CAI, US was more sensitive (pooled sensitivity of ∼0.90) than MRI in detecting both chronic ATFL and CFL injuries. 11 The accuracy of MRI was mostly limited to diagnosing chronic ATFL injuries (pooled sensitivity of 0.83). 11 These findings suggest that imaging alone is insufficient to diagnose CAI. However, MRI is still valuable to assess for talar or tibial osteochondral damage (Figure 6A) if a patient continues to have persistent ankle pain after conservative treatment. 60

Coronal T2-weighted magnetic resonance imaging demonstrating a calcaneofibular ligament tear (blue arrow).
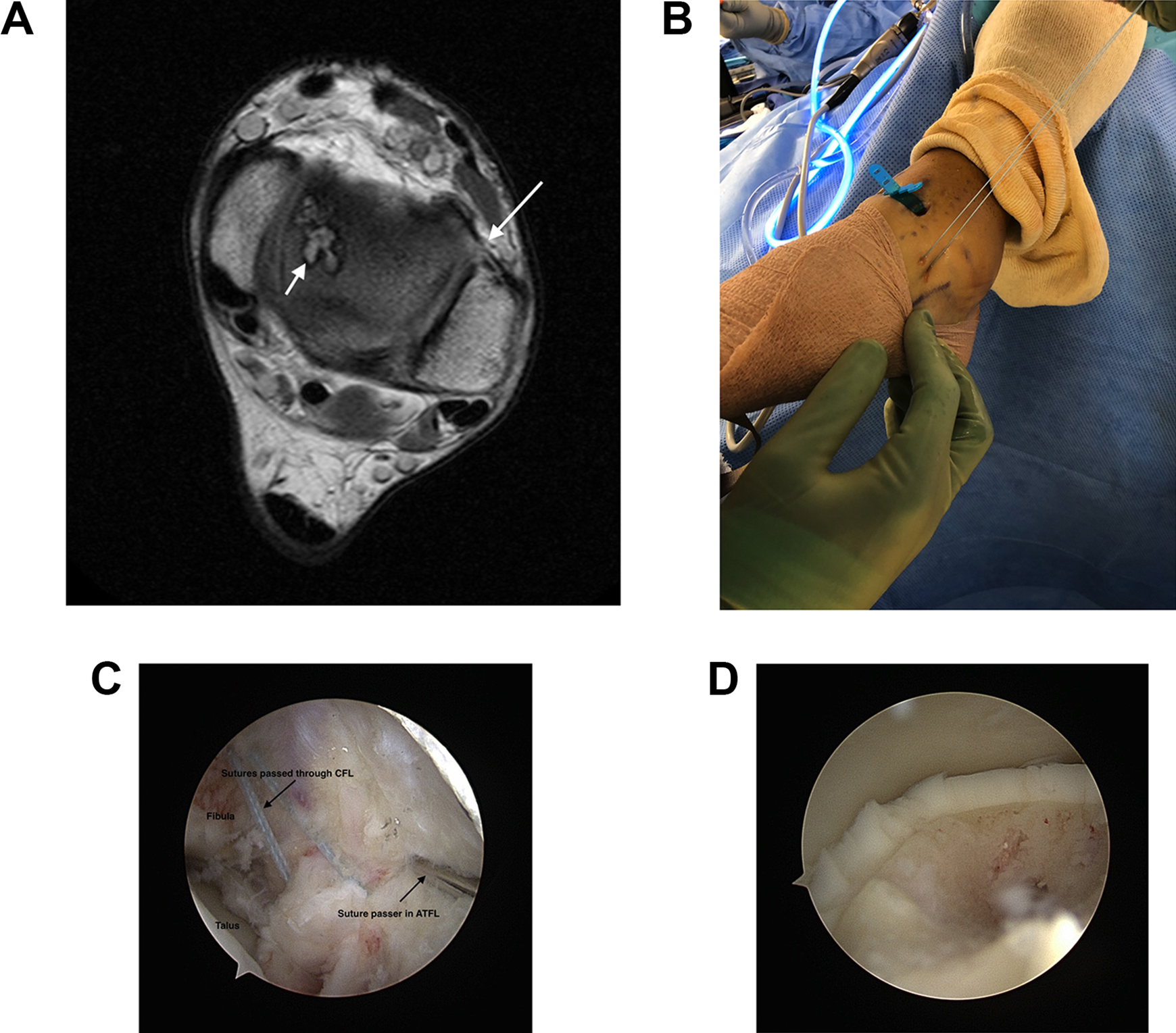
(A) Axial T1-weighted magnetic resonance image demonstrating a chronic ATFL tear (large white arrow) and a medial osteochondral defect of the talus (small white arrow). (B) Intraoperative view of the sutures passed via arthroscopic approach. (C) Arthroscopic view of the lateral ligament repair demonstrating sutures passed through the CFL and the suture passer device for the ATFL. (D) Arthroscopic view of an osteochondral defect treated concomitantly during arthroscopic lateral ligament stabilization.
Associated Pathology
Concomitant disorders include bony and soft tissue ankle impingement, osteochondral lesions of talus (OLT), loose bodies, peroneal tenosynovitis, and peroneus brevis tears. 22 It is suggested that certain disorders predict unsatisfactory outcomes following surgery. 14 However, a more recent retrospective case series (Level IV) revealed that the reoperation rate was actually lower in patients with peroneal pathology compared with others (8.7% vs 27.5%, P = .032) which was attributed to a more comprehensive initial surgery. 2 The senior authors routinely perform ankle arthroscopy at the time of ligamentous stabilization because of the high rate of intra-articular lesions in this patient population, including OTLs and soft-tissue or bony impingement.
Another condition commonly associated with CAI is known as subtalar joint instability (STJI) which occurs in approximately 10% to 30% of patients who have CAI. 45 The subtalar joint has an extensive amount of ligamentous support from the interosseous talocalcaneal ligament, cervical ligament, deltoid ligament’s tibiocalcaneal fascicle, CFL, and the lateral root of the IER. 5,33,45 Although an ATFL and CFL injury primarily compromises the stability of the talocrural joint, 33 a CFL injury can also present as STJI. 37 As a result, STJI and CAI present very similarly where patients complain of their ankle “giving way” in the setting of recurrent sprains. 45
Traditionally, stress radiography has been used to delineate CAI from STJI by objectively evaluating both the talocrural and talocalcaneal joints. 37,45 The Broden projection is a popular subtalar stress view and a nonparallelism between the talus and calcaneus is suggestive of STJI. 53 However, its utility has since been questioned because it only evaluates the posterior facet of the subtalar joint. 53 Thus, little is known about effective diagnostic methods to clinically differentiate STJI from CAI.
A potential sequela of CAI is osteoarthritis and hindfoot varus or valgus malalignment. In a case series (Level IV) evaluating posttraumatic ankle osteoarthritis, 13% were attributed to a ligamentous lesion, with the majority involving the lateral ligaments. 58 Notably, the time span for developing arthritis was shorter in those with a single severe sprain compared to chronic lesions (mean latency of 25.7 vs 38.0 years, P < .05). 58 The authors also found that approximately 67% of patients with chronic lateral ankle instability had varus malalignment. The varus malalignment was attributed to progressive degenerative changes on the medial ankle’s cartilaginous surface as a result of peroneal muscle dysfunction and abnormal ankle kinematics. 58
Treatment Methods
Nonoperative Intervention
After a sprain, patients are initially treated conservatively. An individualized rehabilitation program for at least 3 months is an important component of nonoperative intervention, because it addresses each patient’s exercise needs accordingly. 1,41 The rehabilitation program for CAI is composed of a functional and a preventative component. 1 During both phases, the patient performs multidirectional strengthening exercises with an emphasis on proprioceptive training, peroneal muscle strengthening, and sport-specific training for athletes. 1,41
Addressing risk factors for recurrent sprains (eg, proprioception deficits) are important for both preventive and treatment strategies. 60 The use of either bracing or taping is also effective in preventing recurrent sprains. 60 In a randomized controlled study (Level I) evaluating the preventive role of a brace alone to neuromuscular training and combination of the two, the authors found that a brace alone was superior to neuromuscular training in decreasing the incidence but not the severity of the sprains. 36 Compared to the neuromuscular training group, the patients who received a combination of the 2 methods had a lower incidence of recurrence; however, it was not statistically significant. 36 In another study (Level I), the authors evaluated the effect of a semirigid orthosis on the incidence of ankle sprains in soccer players. 55 They found a significantly lower incidence of recurrent sprains in the orthotic group. However, the use of a semirigid orthosis did not affect the incidence in patients without history of sprain. 55 The authors suggested that orthosis provides both proprioception and mechanical support to an ankle with a prior history of sprain. 55 Preventive programs have also been found to reduce the rate and recurrence of ankle sprains. 42
Operative Intervention
There are several surgical options for patients who do not respond to rehabilitation. 6 These techniques are broadly categorized into nonanatomic versus anatomic approaches. Nonanatomic approaches do not re-create the ligaments’ normal anatomic insertion points; these procedures predominantly rely on local grafts (eg, peroneus brevis tendon autograft) in order to reconstruct the attenuated ligaments. 6 Nonanatomic procedures have several clinical disadvantages, such as the sacrifice of a normal tendon to use as a graft, impaired ankle range of motion, and long-term degenerative changes. 4,7 In contrast, anatomic procedures are preferred as they attempt to re-create the normal ankle’s biomechanics, 6,12 and these procedures will be described here.
A direct lateral structure repair depends on the quality of the ligamentous tissue. In the 1960s, Broström 9,10 first described an anatomic technique that directly repaired the ATFL and CFL. In this technique, the ends of the attenuated ATFL are oversewn and tightened using continuous sutures. However, this was later modified with the Gould technique, which involves reinforcing the repair by suturing the IER to the fibula. 29,30,40
The open Broström-Gould anatomic repair is one of the most common techniques used for lateral ankle instability. However, an alternative anatomic technique involving the use of an autograft or allograft is occasionally necessary, usually in the setting of revision surgery, longstanding instability, and generalized ligamentous laxity. 16,40 In a comparative (Level III) study evaluating clinical outcomes following Broström repair versus anatomic reconstruction with allograft tendons, the 2 groups had similar function and activity levels at a minimum of 2 years follow-up, which suggests that reconstruction is a reliable option for those at risk of failure with a standard anatomic repair. 40 However, it is unclear which anatomical procedure is most appropriate for CAI due to study heterogeneity and limited high-quality studies. 12
The use of a suture tape and/or suture anchor augmentation for lateral ligament reinforcement has also been evaluated. In a cadaveric study comparing the traditional Broström repair to suture anchor and suture anchor with tape augmentation, the authors found that the tape augmentation group was biomechanically superior to the others. 51 The addition of a suture tape material may be particularly useful in cases where a standard Broström repair has a higher risk of failure, such as connective tissue disorders, revision surgery, or generalized ligamentous laxity. In a prospective case series (Level IV) of 28 patients with generalized ligamentous laxity treated with suture tape augmentation (mean follow-up of 35.8 months), the authors found significantly improved Foot and Ankle Outcome Scores and Foot and Ankle Ability Measure scores from baseline. 13 Only 1 subject in the series experienced recurrence of CAI. 13 This suggests that suture tape augmentation is an effective adjuvant to the modified Broström repair.
In the past decade, there has been an increased interest in arthroscopic surgery because of its minimally invasive nature and its potential to decrease patients’ recovery time and morbidity. 24 Arthroscopic intervention also allows the surgeon to concurrently diagnose and treat intra-articular disorders while addressing the damaged ligaments (Figure 6B-D). 24 In a randomized controlled study (Level I) comparing an “all-inside” arthroscopic modified Broström to the open technique, at 1 year after surgery there was no difference in clinical or radiologic outcomes. 63 In another study (Level IV), the authors compared clinical outcomes of the open Broström-Gould repair to an all-inside arthroscopic Broström. 47 The data showed no observable differences between the 2 approaches with respect to pain, American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot Score, and Karlsson-Peterson scores. 47 However, compared to the open procedure, the authors found that the arthroscopic group exhibited earlier time to ambulation (12 vs 22 days). 47 In a case series (Level IV) of patients treated with an “all-inside” arthroscopic knotless suture-anchor technique, not only did all the patients report subjective improvement in their ankle stability and ability to return to their normal activities but the technique also avoided the suture knot prominence that is often associated with postoperative neuritis. 59
Arthroscopic procedures also have their disadvantages. The suture anchors’ knots can entrap nearby structures such as the extensor tendons, superficial peroneal nerve, and peroneus tertius. 24,32 Although a recent systematic review comparing open to arthroscopic techniques showed higher complication rates for arthroscopic studies, the review was mostly limited to level IV studies and by statistical heterogeneity. 32 The complications did not impact patients’ functional scores. 32
Surgical Technique
The authors’ preferred operative technique includes the use of diagnostic arthroscopy to address any concomitant intra-articular lesions, and an open lateral ligament reconstruction with suture anchors. The patient is placed in the lateral position with the affected ankle lateral side up using an axillary roll (Figure 7A). The lateral positioning permits the surgeon to address concomitant disorders (eg, peroneal tendinopathy) simultaneously. This can also be performed in the supine position with a bump under the hip, if preferred. A diagnostic arthroscopy is performed through the anteromedial and anterolateral ankle portals with the hip externally rotated placing the leg on leg holder (Figure 7B). After the intra-articular pathology is addressed, a curvilinear incision (Figure 8A) is made along the distal margin of the lateral malleolus and dissection is performed down to the fibular periosteum and extensor retinaculum. The ligaments and IER are dissected free. After the creation of a fibular periosteal flap, a pair of suture anchors (Figure 8B to 8D) are placed into the ATFL’s and/or CFL’s fibular insertion points. The ligaments and IER are then sutured using a modified Mason-Allen technique in order to capture the tissue with 1 locking suture limb and 1 sliding suture limb. With the ankle in slight eversion, the sutures are tensioned and tied. The limbs are then brought back through the periosteum in order to create a “pants over vest” repair. If desired, 1 suture limb from each can be reanchored into the lateral fibula to create a double-row repair and mat down the suture knots.

(A) Preoperative lateral positioning, the operative limb elevated with extra-blankets. (B) Preoperative positioning, hip externally rotated prior to ankle arthroscopy.

(A) Intraoperative view showing a curvilinear skin incision along the fibula. (B) Intraoperative view of the distal fibula with proper drill hole placement for the suture anchors. (C) Intraoperative view of the lateral ligament repair and identification of the CFL (black arrow). (D) Intraoperative view of the lateral ligaments (ATFL and CFL) and the IER suture anchors.
The authors prefer immediate weight-bearing as tolerated in a stirrup brace postoperatively as it allows for a quick return of the ankle’s proprioception and range of motion without compromising the repair. A report of this rehabilitation protocol and surgical technique in 6 patients with mean follow up of 2.5 years showed satisfactory AOFAS scores. 27 A more recent study has also reported satisfactory outcomes using immediate unrestricted weight-bearing after lateral ligament stabilization. 21 However, the weight-bearing status can be adjusted to take into account the surgeon’s preference and the type of ligamentous stabilization and/or concomitant procedure performed.
Complications
Postoperative complications can occur after open or arthroscopic approaches. Complications of both approaches include superficial wound infection, local nerve injury, delayed wound healing, residual instability, and venous thromboembolic events. 32,50 Portal site irritation is specific to arthroscopic procedures. 32 As previously described, the results of a systematic review revealed that arthroscopic interventions had a greater overall postoperative complication rate (15.27%) compared to open (7.92%). 32 In this review, the authors found that the most common postoperative complications were superficial peroneal neuritis and superficial wound infections in arthroscopic and open procedures, respectively. 32
Conclusion
CAI is the result of recurrent lateral ankle sprains that compromise the static stabilizers of the ankle joint. Not all patients who sustain a single or recurrent ankle sprain may develop CAI. Adverse anatomical and/or neuromuscular changes can occur after a sprain. CAI can also exist with several associated disorders such as STJI or OLTs. A thorough evaluation is paramount in order to appropriately address the associated disorders. Accurate diagnosis involves careful combined assessment of history, examination findings, and imaging findings. The preferred initial treatment includes pain control, activity restriction, bracing, and functional rehabilitation. Physiotherapy includes proprioceptive training with balance and postural control exercises. The open modified-Broström anatomic repair is one of the most commonly performed technique with good results reported in the literature, although select patients may require augmentation with other methods. Although an arthroscopic approach provides several advantages, further study is warranted.
Supplemental Material
Supplemental Material, FAO846938-ICMJE - Lateral Ankle Sprain and Chronic Ankle Instability
Supplemental Material, FAO846938-ICMJE for Lateral Ankle Sprain and Chronic Ankle Instability by Aida K. Sarcon, Nasser Heyrani, Eric Giza and Christopher Kreulen in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eric Giza, MD, reports Arthrex, Inc., fellowship support. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.