
Abstract
Background:
Talar body osteonecrosis can be a difficult condition to treat. Recent reports highlight a high rate of failure with the use of femoral head allograft. Additionally, higher rates of failure have been reported in diabetics and smokers. Our institution attempted a novel technique utilizing fresh allograft talus in attempt to improve on a reported 50% nonunion rate.
Methods:
Five patients who underwent tibiotalocalcaneal (TTC) fusion utilizing fresh talar allograft were clinically and radiographically reviewed to evaluate fusion rates and functional outcomes.
Results:
Our case series of 5 patients had a 100% union rate, including 2 former smokers and 2 diabetic patients. There were no infections or complications. Functional outcomes also improved in our series of patients postoperatively as noted by their FAAM and SF-36 scores.
Conclusion:
TTC fusion using fresh allograft talus has a higher union rate than reported with femoral head allograft. This case series requires further study to evaluate whether this technique can be used beyond patients with osteonecrosis of the talus.
Level of Evidence:
Level IV, case series.
Introduction
Techniques for treating talar osteonecrosis with collapse often involve arthrodesis, which typically requires removal of nonviable talar bone and subsequent structural grafting. Specific surgical options include tibiotalar fusion, tibiocalcaneal fusion, tibiotalocalcaneal (TTC) fusion utilizing femoral head or talar allograft, TTC fusion utilizing fibular autograft, or trabecular metal augments (Unite3D Bridge Fixation System; Zimmer Biomet, Warsaw, IN). 2,4,5,8,10 These surgeries are often complicated by nonunion, limb shortening, or graft failure. Fresh or frozen femoral head allograft is commonly used for structural grafting during TTC arthrodesis. However, one study found a 50% nonunion rate using this technique. 6 It is unclear whether the nonunion rate is different when fresh allograft are used compared to frozen as both have been used in previous studies. 6 In response to these suboptimal outcomes, we recently developed a technique using a fresh allograft talus rather than femoral head to achieve TTC fusion for osteonecrosis of the talus. 3 The talus may be better suited biomechanically to resisting compressive forces at the ankle than femoral head, though no biomechanical studies exist to confirm this.
The goal of this study was to evaluate the outcome of patients with talar osteonecrosis treated with a fresh allograft talus TTC arthrodesis, specifically evaluating fusion rate, complications, and functional outcomes. We hypothesized that the use of a fresh talar allograft would increase the rate of successful fusion compared to that of other structural allografts as reported in the literature.
Methods
Institutional review board approval was obtained prior to study initiation. We retrospectively identified 6 patients with osteonecrosis of the talus who had undergone TTC arthrodesis with fresh allograft talus prior to October 2016. Patients were included if they had undergone TTC arthrodesis with fresh allograft talus due to the diagnosis of osteonecrosis of the talus. Patients were excluded if they had previous infection as the cause of their osteonecrosis. Five of the 6 eligible patients gave consent to participate in the study. Functional, radiographic, and clinical variables were retrospectively reviewed from 6 weeks, 12 weeks, 6 months, and 9 or 12 months postoperatively.
All patients had plain radiographs as well as an MRI preoperatively to confirm the extent of talar osteonecrosis (Figures 1 and 2). Patient’s history, demographics, postoperative adverse events, radiographic fusion, and patient-reported outcomes were recorded (Table 1). Patient-reported outcomes included RAND Short Form–36 (SF-36) and Foot and Ankle Ability Measure (FAAM). 7,9 Additionally, a resting 100-point visual analog pain scale (VAS) was recorded pre- and postoperatively.

(A) Anteroposterior and (B) lateral preoperative radiograph demonstrates patient with talar osteonecrosis.

Preoperative magnetic resonance imaging showing talar body osteonecrosis with collapse.
Demographic Data for study Patients.
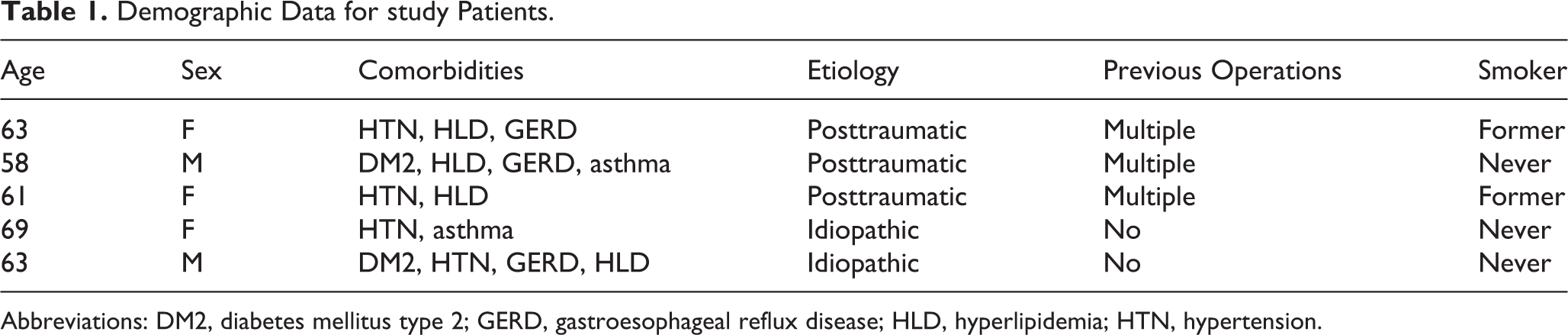
Abbreviations: DM2, diabetes mellitus type 2; GERD, gastroesophageal reflux disease; HLD, hyperlipidemia; HTN, hypertension.
Plain radiographs were obtained postoperatively to monitor incorporation of the allograft talus; if there was clinical concern for a nonunion, a CT scan was obtained. Union was defined as bony apposition with no intervening radiolucent lines covering more than 50% of the arthrodesis sites 6 (Figure 3). Patient variables such as smoking status and medical comorbidities, including diabetes, were recorded. Two of the 5 patients were former smokers but had abstained from tobacco use at least 1 month prior to surgery. Two of the 5 had diabetes requiring insulin for treatment. The cohort was composed of 3 women and 2 men. The average age at time of surgery was 63 years (range, 58-69), and the minimum follow-up was 9 months (range, 9-45).

(A) Mortice, and (B) lateral postoperative ankle radiograph demonstrating graft incorporation and tibiotalocalcaneal arthrodesis.
Operative Procedure
The operative technique for the allograft talus TTC arthrodesis had been previously descibred. 3 In brief, a lateral approach to the ankle was undertaken and the fibula removed and milled for additional graft. Avascular talar bone was excised, maintaining as many vascular attachments to healthy talar head and neck as possible. Remaining tibiotalar and subtalar joints were then prepared for arthrodesis in standard fashion. A laterality-matched fresh-frozen allograft talus was utilized for structural graft. The graft was denuded of cartilage at both the tibial and calcaneal articulations and prepared for arthrodesis in the standard fashion. It was then soaked in autologous stem cells obtained from the ipsilateral iliac crest to aid in graft incorporation. The graft was positioned and a TTC fusion nail is utilized to stabilize both the tibiotalar and subtalar arthrodesis sites. Compression screws were also utilized across both fusion sites and through the native talar head and neck into the graft. Postoperatively, patients were immobilized and remained nonweight bearing for 12 weeks. Patients were then advanced to progressive weight bearing 12 weeks after surgery in a pneumatic boot and allowed to be full-weight bearing at 16 weeks after surgery.
Statistical Analysis
Functional outcomes for the FAAM pre- and postoperatively were analyzed for differences using a paired Student t test. Statistical significant was defined as a P value of <.05.
Results
All 5 of the patients in the cohort (100%) achieved successful fusion after surgery based on clinical symptoms and plain radiographs. There were no infections. One patient required removal of hardware due to proximal stress reaction and pain, but there were no other unplanned returns to the operating room. Four of the 5 patients had radiographic union within 6 months of surgery. One diabetic patient required more than 6 months to unite, but at 12 months healing of his nonunion was confirmed with CT scan. The mean time to fusion for the cohort was 7.2 months. The patient with nonunion required a CT scan because of clinical concern for nonunion. This demonstrated incorporation at the tibiotalar and subtalar arthrodesis sites.
There was improvement in both SF-36 and FAAM scores postoperatively in all areas except for the physical functioning subscale of the SF-36. SF-36 scores improved the greatest in physical limitation and general health, improving from preoperative scores of 16.7 and 41.7, respectively, to 50 and 81.3 postoperatively (Figure 4). Improvements in FAAM scores were most pronounced in activities of daily living, increasing from 29.3 on average to 55.7 (Figure 5). The differences in outcomes scores were not statistically significant (P = .06). Two of the 5 patients had a VAS of 0 at final follow-up, 2 others had rest pain of 20 on a 100-point scale, and 1 patient had continued rest pain of 60 measured by VAS.

Includes SF-36 subscores preoperation (dark) versus postoperation (light). The scores indicate improvements in all domains: RL-PH/EP (role limitations—physical health/emotional problems), EF (energy/fatigue), EWB (emotional well-being), SF (social functioning), P (pain), GH (general health) except for PF (physical functioning).

Demonstrates improvements in FAAM scores postoperatively.
Discussion
Osteonecrosis with collapse of the talus is a difficult problem to manage because of the need to remove nonviable bone and then address the resultant defect. The operative techniques described for this problem have demonstrated variable outcomes with high failure rates, especially in smokers and diabetics. In particular, studies of TTC arthrodesis with femoral head allograft have a reported union rate of only 48% to 50%. 1,6 Our experience with TTC arthrodesis was similar and was the driving force behind the development of this new technique.
The theoretical benefit of using allograft talus rather than femoral head is that the talus is more suited to accommodate compressive forces of the ankle joint. We speculate that the progressive loss of graft height with use of femoral head allograft is secondary to mal-orientation of the trabecular bone, making the femoral head less suited to withstand compressive forces at the ankle when weight bearing is initiated. 6 We did not observe any talar graft collapse in this cohort postoperatively though our short-term follow-up of only 12 months limits our ability to detect late collapse.
Smoking and diabetes correlate with nonunion in the treatment of talar osteonecrosis. 1,6 This study included 2 diabetics who obtained successful fusions. Notably, one of the diabetic patients did require advanced imaging to confirm arthrodesis and also required more than 6 months for radiographic healing of his nonunion. We recommend encouraging smoking cessation and optimizing glucose control prior to surgery in smokers and diabetics.
In contrast to previous studies of TTC arthrodesis for the treatment of osteonecrosis, our cohort had a 100% fusion rate, including 2 former smokers and 2 insulin-dependent diabetics. Four of 5 patients had fusion within 6 months, and 1 diabetic patient experienced a nonunion that eventually united after 6 months to within 1 year. The exact time to fusion cannot be discerned as union was demonstrated with a CT scan that was obtained 1 year after surgery. In addition, our cohort experienced improvement in functional outcome measures postoperatively including FAAM, SF-36, and VAS. The singular SF-36 domain (physical function) that did not show improvement includes joint range of motion in activities such as jumping (Figures 4 and 5). Because TTC arthrodesis sacrifices motion at the tibiotalar and subtalar joints, there is an expected loss of mobility postoperatively and a subsequent decrease in the SF-36 physical functioning domain.
This study has several limitations, most notably the small size of the cohort. The study included fewer patients than previously published series using femoral head allograft. Our cohort also did not include Charcot, failed arthroplasty, or patients with previous infection. Thus, our results may not translate to these populations. Additionally, our study used only plain radiographs to determine fusion, which may not have adequately detected delayed union or nonunion at the subtalar arthrodesis site because of its oblique orientation. Given that this is a retrospective study and because patients were doing well clinically, a CT scan was obtained in only 1 of the 5 patients. Similar to TTC fusion techniques that use trabecular metal grafts, the allograft talus TTC technique has substantial associated costs and preoperative planning time. A fresh allograft talus costs on average $7000, as compared to $800 for a frozen femoral head allograft. There is the additional concern of disease transmission as well when using a fresh graft rather than a frozen one. Additionally, there is typically an increased time required to obtain a size- and side-matched fresh allograft talus.
Conclusion
In conclusion, allograft talus TTC fusion for treatment of talar osteonecrosis has a high rate of fusion, with few complications observed in this small case series. Furthermore, the patients in this cohort were noted to have improvements in functional outcomes after surgery. Additional study is needed to determine if this technique may be useful in treating bone loss caused by other conditions such as failed total ankle arthroplasty or Charcot neuroarthropathy.
Supplemental Material
Supplemental Material, FAO834541-ICMJE - Case Series: Allograft Tibiotalocalcaneal Arthrodesis Utilizing Fresh Talus
Supplemental Material, FAO834541-ICMJE for Case Series: Allograft Tibiotalocalcaneal Arthrodesis Utilizing Fresh Talus by Joshua Vaughn, Kenneth W. DeFontes, Cornelia Keyser, Eric M. Bluman and Jeremy T. Smith in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.